Embed Size (px)
Citation preview

Department of RadiologyLausanne University Hospital
Switzerland
Clarisse Dromain
Imagerie de la carcinose péritonéale

Department of RadiologyLausanne University Hospital
Switzerland
Clarisse Dromain
Imagerie des métastasespéritonéales

Peritoneal tumor imaging
• High spatial resolution: small volume of implants
• High contrast resolution: – Similar attenuation to small bowel wall or
other normal tissue
– No significant enhancement
• Minimization of motion artifacts: MRI, PET-CT
A technical challenge

Peritoneal tumor imaging
– Low inter-reader variability
– Low confidence of presence: high frequency of doubtful lesions
– Too many of PM are seen only in retrospect
An interpretation challenge

• Diagnostic
• Sélection des patients pour la chirurgie
– Extension intrapéritonéale +++ • Distribution dans l’abdomen et le pelvis
– Localisations invisibles en laparoscopie
– Les atteintes nécessitant une chirurgie d’expertise
– Les atteintes associées à une faible probabilité d’obtenir une cytoréduction complète
– Les atteintes extrapéritonéales
Sugarbaker PH, De Bree E., J Surg Oncol, 2004
Rôle du radiologue

• Sensitivity – Per patient 82 à 93%– Per lesion 25 à 93%
• Depends on– Localisation of implants
• Epigastrium, subphrenic space, péri ombilical• Pelvis, mesentery, visceral peritoneum, R subphrenic
space
– Implants size– Primary tumor– Radiologist expertise *
• Warde : 3 readers, sens 30-73%
• Coakley : k = 0.35-0.50 for peritoneal thickening
k = 0.12-0.25 for small bowel involvement
*de Bree E, JSO2004; Kim SJ Radiology 2009; Warde P Am J Med Sci 1987; Coakley FV, Radiology 2002
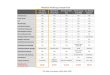
CT: Imaging of reference
Sens. > 1cm < 0,5 cm
Jacquet 1993 79% 28%
Davies 1997 71%
De Bree 2004 > 5cm59-67%
9-24%
Koh 2009 60% 11%
Kim 2009 28,3%
Marin 2010 75% 43%


PM detection: how to improve !
• Analyze the peritoneum as an own organ: – The toblerone effect …

PM detection: how to improve !
• Use multiplanar reconstruction
• To know the different types of lesion
Peritonealthickening
Fat standingNodules

• Look at not only intraperitoneal cavity but also peritoneal fat folds – Ligaments
– Mesenteries
– Omenta
Morisson pounch
Pelvic pounch
Subprhrenic space
Spenic pounch
Round lgt
Falciform lgtLesser omentum
Coronary lgt
Triangular lgt
Mesentery
Mesocolon
PM detection: how to improve !

Améliorer la détection de la CP au TDM
• Connaitre les signes indirects de CP– Métastases ovariennes
– Dilatation urétérale
– Métastase ombilicale : nodule de sœur Mary Joseph (cancer gastrique)
– Ganglion cardiophrénique CPALN
*Koves I, et al 1993 Eur J Surg**Goéré D et al Eur J Surg Oncol. 2008;34(12):1335.

utérus
tumeur
annexe droite
annexe gauche
abcès
abcès
abcès
utérus
tumeur
annexe droite
annexe gauche
abcèsabcès
abcès
65 ansAdénocarcinome du sigmoïde opéré il y 6 mois
Abcès tubo ovarien sur carcinose péritonéale
Carcinose
Trompe dilatée

• CPALN chain : major relay stations both for– The entire peritoneal surface– The diaphragm
• 550 patients with CRC treated by surgerywith complete peritoneal exploration
• CPALN in 245 patients (45%) on CT images
• CPALN only imaging feature associatedwith PM on multivariate analysis
• The nature (malignant or benign) of the CPALN is still unknown
CPALN
PM(n = 165) 30%
No PM(n = 385)
CPALN (%)
Yes 123 (75 %) 122 (32 %)
No 42 (25 %) 263 (68 %)
Sens Spe PPV NPV
75% 68% 50% 86%

PM for a MINEC tumor

Recurrent PM after HIPEC
May 2016After Folfiri + beva
Dec 2015
CSR + HIPEC + CPALN dissection : tumoral lymph
node involvement

Perihepatic and perisplenic ascites
CPLN
Thickenings of parietalperitoneum
Dissection of the CPLN
Signet ring cellcarcinoma

Digestive NET: Comparison MR and F-DOPA PET

PM mimickers Sigmoïd diverticulum
Spenosis implant
Mesenteric lymph nodes
Post-therapeutic fibrous nodules• Post-operative CT 2 months after surgery is helpful to dicrease FP
on CT exams
DiverticulumResidual fibrous
nodule after HIPEC
Mesenteric LN
Slenosis implant

Ganglion du mésosigmoïde
Nodule de carcinose
PM vs lymph node

• Male 51 years
• Caecal adenocarcinoma
3 months after surgery
Epiploic fat necrosis

Desmoïd tumors• Male 55 years
• Surgery for colon cancer 2 years ago

No PM:Inflammatory peritoneal
reaction
• Male 55 years
• Stenotic colon cancer

• Male 78 years, laotian origin, many trips
• Weight loss (-6Kg)
• Hemochromatosis since 1997
• Colonoscopy with colic perforation in 2008
• Laparoscopic cholecystectomy in 2014
Inflammatory granuloma : Lost intraperitoneal stones afterlaparoscopic cholecystectomy
An FDG uptake on PET CT images doesn’t mean cancer

Post-operative CTafter intra-abdominal
collection drainage
6 -months FU CT
Mme T, 64 yoPM from colon cancerCSR + HIPEC (oxaliplatine) complicated with intra-abdominal collections

• CT-PCI– Underestimation 96% of patients*
• ≥ 4 area 33,2%• small lesions, adherences **
– Overestimation less frequently : infiltration of fat
** Esquivel JSO 2010, Sala Radiology 2010
Quantitative assessment of PM distribution
• High CT-PCI is a reliable • If the CT images tumor nodules, they are almost
always present
• A low CT-PCI has a more limited prognostic• Laparoscopy ?
Meandifference
CT vs surgery (%)
PET vs surgery (%)
-2 0 7.1
-1 3.3 0
0 26.6 14.3
1 16.6 14.3
2 6.6 7.1
3 13.3 10.7
4 16.6 17.8
5 10 7.1
6 0 3.5
7 6.6 7.1
8 0 3.5
9 0 7.1
* Dromain C et al, Abdo Imaging 2008

Standardization of scoringWeb application
www.e-promise.org
www.psmss.net

Qualitative assessment of PM distribution
Radiologic features associated with high risk of incomplete surgery
• Clumped bowel
– Strong predictor of diffuse involvement of visceral peritoneum by a tumor of high grade histology
• Pluri-segmental bowel obstruction
• Involvement of the hepato-duodenal ligament
• Extensive pelvic disease, vesical trigone or 2 ureters
• Extensive peri-gastric disease
• CT-PCI > 20 (excluding PMP, cystic mesothelioma and low malignant ovarian tumors)
Sugarbaker P, C Dromain et al, Int J Hyperthermia 2017, Chamdramohan Br J Radiol 2017

Standardized reportkey imaging features that a radiology report should include
1. Description of PM
2. Distribution:□Localized □Plurifocal □Diffuse
3. Ascites– Volume: □Low □Lntermediate □High
– Type: □ Libre □ Cloisonnée □ Bloody
4. CT-PCI– Common cut-off for surgery CT-PCI < 20 (Excluding PMP and cystic
mesothelioma)
– Should take into account the primary tumor and the general status of the patient

4. High risk features for incomplete surgery:– Plurifocal bowel obstruction □No □Yes – Mesentery involvement □No □Yes – Portal hepatis infiltration and/or bile duct obstruction □No □Yes – Hydroureter □No □Yes – Psoas muscle invasion □No □Yes – Gastric outlet obstruction □No □Yes – Tumor ≥ 5cm in lesser omentum or subpyloric space □No □Yes – Tumor ≥ 5cm in jejunal regions □No □Yes – Mesenteric and retroperitoneal lymphadenopathy □No □Yes – Pleural effusion in the absence of extensive ascites □No □Yes – Pelvis sidewall invasion □No □Yes – Bladder involvement □No □Yes
5. Lesion requiring complexe surgery– Diaphragmatic involvement □No □Yes – Extensive perihepatic involvement □No □Yes – Pancreatic involvement □No □Yes – Perivascular involvement □No □Yes
6. Extraperitoneal metastases□No □Yes If yes, location:

PAUSE Criteria
• P Primary tumor and PCI
• A Ascites and abdominal wall involvement
• U Unfavorable site of involvement
• S Small bowel and mesenteric involvement
• E Extraperitoneal disease
Chandramohan a et al, Clin Radiol 2017;72:972-980
• P 16
• A 1 (ascites)
• U 1 (hep-duodenal lig.)
• S 0
• E 0

Benefits of MRI
• Increased detection of small implants – High contrast resolution with DW images
• Malignant ascites– Increased conspicuity of some tumoral implant by the suppression
of SI of ascitis fluid
• High sensitivity for some anatomic site such as subdiaphragmatic space and pelvis
• High sensitivity for mucinous PM ( PET-scan)
• Post-operative recurrent disease
• Limitation: inter-reader reproducibility < PET-CT*
*Soussan Eur radiol 2012; Satoh AJR 2011

IRM: technique

Normal CT
• Male 38 yo
• PM from sigmoïd adenocarcinoma treated by
CRS + HIPEC 10 months ago
MRI: Recurrence in the spermatic cord

T2FS PETdiffusion
Mucinous PM and retroperitoneal LN

Recurrent pseudomyxoma

Follow up of PMP

Problem solving tool in pelvis

Indication of MRI for PM detection and staging
• Current recommandation (in addition to CT)
– Staging and FU of mucinous peritoneal carcinomatosis including PMP
– Problem solving tool ( pelvis ++)
– Increased markers with normal CT (vs PET-CT)
• Option
– Pré-operative staging of peritoneal metasases

DW-MRI Limites• T2 Shine –Through : hypersignal persistant des structures à fort T2
(composante liquidienne): faux positifs– Images d’ADC
– Comparaison aux images morphologiques
• Tumeurs à faible densité cellulaire– T séreuses et mucineuses : aspect hétérogène, valeur élevée de l’ADC
– T calcifiées (ovaire) hyposignal T2 et T2 diffusion.

DWI b= 0 DWI b= 0
ADC

Take home message
• Accurate interpretation with knowledge of direct and indirect signs may significantly improved the per-site detection of PM
• Standardization of CT reports with description of high risk lesions is crucial for selection of patient suitable HIPEC and cytoreduction surgery or PIPAC– Will also facilitate multicenter clinical trials– Will facilitate to follow longitudinal studies of response to
therapy
• MRI is useful in staging and FU of mucinousperitoneal carcinomatosis including PMP and problem solving

Thank you for your attention [email protected]