Embed Size (px)
Citation preview

1Classification of Thoracolumbar Spine
InjuriesGuillem Saló Bru
IMAS. Hospitals del Mar i de l’Esperança.ICATME. Institut Universitari Dexeus USP.UNIVERSITAT AUTÒNOMA DE BARCELONA

Objectives of classification� Information about the severity of the given injury.� Guide for further treatment:
� Which injuries are stable ??� Which injuries benefit from spinal cord decompression ??� Which injuries require surgical stabilization ??
� Prediction of clinical outcome.

Historical ClassificationSystems
Only for conservative treatFirst Classification1938Watson-Jones
Nonspecific for everyday use
Punctuate for each part of
Vertebrae broken.1977Louis & Goutallier
1983
1968
1963
1949
Year
The middle column is the primary determinant of mechanical stability.
Development of the three-column modelDenis
Classification guides treatment of neurologic deficit
Refines the two-column modelKelly & Whitesides
Fails to appreciate some burst fracture instabilities
Modifies previous classification systems to include the mechanisms of injury and two-column theory
Holdsworth
Foundation for subsequent classification systems
Differentiates stable from unstable fracturesNicoll
CommentsSummaryAuthor

Historical ClassificationSystems
Involves the vertebral body as it relates to kyphosis.
Suggests a posterior component, anterior component and body component
1994Gertzbein
Cumbersome, nonspecific for everyday use
Combines work done by Denis and McAfee; mechanistic classification to clarify patterns of thoracolumbar injury
1984Ferguson and Allen
1994
1994
1983
Year
Strong inter-observer reliabilityDeveloped in response to poor patient outcomes; grades injury based on amount of damage to vertebral body, the spread of fragments in fracture site and amount of corrected kyphosis
McCormack(Load-Sharing)
Moderate inter-observer reliabilityClassifies types of fractures into A, B, or C and into subcategories subsequentlyMagerl/AO
Easily communicated type of injury with patients
Based on CT appearance; classifies injuries into 6 categoriesMcAfee
CommentsSummaryAuthor

Denis Classification
� 1983� Based on the review of 412 thoracolumbar
injuries, CT scans of 53 patients and surgical notes from 120 cases.
� Primarily based on pathologic anatomy of different types of spinal injuries, each of which was based on a different mechanism of injury.
� Supported on a three-columns concept of spine.
Denis F. Spine. 1983

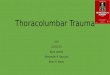
Anterior column- formed by the anterior longitudinal ligament, the anterior annulus, and the anterior portion of the vertebral body
Middle column- the critical feature.Very important to spinal stability; consists of posterior longitudinal ligament, the posterior portion of the annulus, and the posterior aspect of the vertebral body
Posterior column- includes the neural arch, facet joints and capsules, ligamentum flavum, and remaining ligamentous complex
Denis: Three -column model
Denis F. Spine. 1983

Denis Classification.
� Studies have supported the three-column theory and found that the middle column is the primary determinant of mechanical stability of the thoracolumbar region of the spine.
Panjabi, MM. Spine, 1995.

� Basic modes of failure of the columns in the four major types of spinal Injuries.
V. MINOR INJURIES: 17% (transverse, articular, spinous process, pars interarticularis,…)
16
5
15
47
%
DISTRACTION ROTATION/
SHEAR
DISTRACTION/ ROTATION/
SHEAR
COMPRESSIÓNROTATION/
SHEAR
IV. FRACTURE-DISLOCATION
DISTRACTIONDISTRACTIONNONE / COMPRESSION
III. SEAT-BELT
NONECOMPRESSIONCOMPRESIÓNII. BURST
NONE/DISTRACTION
NONECOMPRESSIONI. COMPRESSION
POSTERIORMIDDLEANTERIOR
Denis: Three -column model
Denis F. Spine. 1983

� I-A Anterior:� A: Failure of both end plates
and vertebral body (16 %).� B: Failure of the upper end-
plate (62%).� C: Failure of the inferior end-
plate (6%).� D: Failure of the central
vertebral body without end-plate fracture (15%).
� I-B Lateral:
Denis: Compression fractures (47%)
A B C D

• II-A. Failure of both end plates (24% axial compression).
• II-B. Failure of the upper end-plate (49% axial compression & flexion).
• II-C. Failure of the upper end-plate (7% axial compression & flexion)..
• II-D. Burst-rotation (15% axial compression & rotation).
• II-E. Burst-lateral flexion (5% axial compression & lateral flexion).
Denis: Burst fractures (15%)

Denis: Burst fracturesBurst Fracture Type IIA
Burst Fracture Type IIC

LigamentsBoneOne-level injuries:• III-A. Bony injury (Chance
fracture) (47%).• III-B. Ligamentous injury (10%).
Two-level injuries:• III-C. Through bone middle
column (26%).• III-D. Through ligamentous
middle column (16%).
Denis: Seat-Belt fractures (5%)

Seat-belt fracture III-A.
Denis: Seat-Belt fractures (5%)Seat-belt fracture III-B.
Seat-belt fracture III-C. Seat-belt fracture III-D.

Denis: Fracture Dislocations (16%)
IV-A. Flexion-rotation (13%).IV-B. Shear type (1%).IV-C. Flexion distraction (1%).

Denis: Fracture Dislocations (16%)
Fracture Dislocation IV-A. Fracture Dislocation IV-B.
Fracture Dislocation IV-C.

Load Sharing Classification� Created system in response to poor patient outcomes
when the vertebral body sustained a disproportionately severe injury.
� Load-Sharing Classification: a straight-forward way to describe the amount of bony comminution in a spinal fracture.
McCormack et al. Spine, 1994

Load Sharing Classification
� Classification system grades:� Amount of damaged vertebral
body.� Spread of the fragments in the
fracture sight.� Amount of corrected kyphosis.
� Three degrees of severity for each item.
� Failure of posterior short-segment fixation correlates with a total injury severity point value ≥ 7.
McCormack et al. Spine, 1994

Load Sharing Classification
� System can be used pre-operatively to:1. Predict screw breakage when short segment,
posteriorly placed pedicle screw implants are being used
2. Describe any spinal injury for retrospective studies
3. Select spinal fractures for anterior reconstruction with strut graft
McCormack et al. Spine, 1994

Load Sharing Classification
Reliability� Dai and Jin (2005): Inter-observer and intra-observer
reliability of the Load Sharing system was evaluated by 5 observes on 2 occasions.� Analysis found high levels of agreement when Load
Sharing Classification was used to assess thoracolumbar burst fractures.
� Concluded that the system could be applied with excellent reliability.
� But this system classification fails to consider:� Ligamentous injury.� Injury of the neural elements.
Dai LY, Jin WJ. Spine, 2005.

AO Classification
� Revision of 1445 consecutive thoracolumbar injuries
� Primarily based on pathomorphological criteria.
� Supported on a two-columns concept of spine.� Categories based on:
� Main mechanism of injury� Pathomorphological uniformity� Prognostic aspects regarding healing potential
Magerl et al. Eur Spine J. 1994.

AO Classification
� Classification reflects progressive scale of morphological damage by which the degree of instability is determined
� Consists of a 3-3-3 grid for sub-grouping injuries into three types:� A, B and C� Every type has three groups, each of which contains
three subgroups with specifications.
Magerl et al. Eur Spine J. 1994.

AO Classification
� Types have a fundamental injury pattern which is determined by the three most important mechanisms acting on the spine
1. Compression2. Distraction3. Axial torque
Magerl et al. Eur Spine J. 1994.
3
3
2
1
1

AO Classification - A, B, C ’s
� Type A:� Vertebral body compression- injury patterns of the
vertebral body� Posterior elements remain intact.
� Type B: � Anterior and posterior element injuries with
distraction, characterized by transverse disruption either anteriorly or posteriorly
� B.1 & B.2 hyperflexion mechanism.� B.3 Hiperextension.
� Type C: � Anterior and posterior injuries with rotation or
translation injury patters resulting from axial torque.� C1: A+rotation.� C2: B+ rotation.� C3: translation.
Magerl et al. Eur Spine J. 1994.

AO Classification
� Groups and subgroups.
Magerl et al. Eur Spine J. 1994.

AO Classification
C3.2
A3.3
B1.2
B2.2

Reproducibility studies
Onner et al: Studied the interobserver and intra-observer reproducibility of the Magerl (AO) in comparison with the Denis classification.�The agreement was better with the Denis classification, but the variance was higher due to the difficulty of finding proper categories for some injury patterns. �Although the AO classification allows proper registration of all kinds of injury, the reproducibility, especially at the type level, is fair with CT scans and moderate with MRI.�In spite of this, the authors recommend the use of the Magerl (AO) classification because it allows categorization of injuries to all relevant parts of the spine.

Reproducibility studies
� Blauth el al: interobserver reliability of AO classification system.� 22 hospitals evaluated 14 radiographs and CT scans. � The mean interobserver agreement for all fourteen cases was found to
be 67% (41±91 %),when only the three main types (A, B, C) were used. � The reliability decreased by increasing the categories.
Orthopade, 1999; NASS, 2004

Reproducibility studies
� Wood, et al: 31 CT scans and radiographs of acute traumatic fractures of the thoracolumbar spine evaluated by 19 observers.
� Classified according to both AO and Denis classification system.� Only moderate reproducibility and repeatability among well-trained spine
surgeons using AO and Denis classification systems
Wood JBJS 2005

Reproducibility studies
� To assess the inter-observer reliability and intra-observer reproducibility of standard radiographic evaluation of 150 thoraco-lumbar fractures using the AO-classification (A,B,C). 6 observers, 2 sessions.
� The infuence of clinical information on agreement levels was also evaluated.
� The overall inter-observer agreement was rated as fair (0.291) in the first session and moderate (0.403) in the second.
� The increased level of agreement in the second session was attributed to the value of additional clinical information Eur Spine J, 2006

Thoracolumbar Injury Classification and Severity Score - TLICS (2005).
� Three variables were identified by authors as critical to clinical decision-making in thoracolumbar trauma:
1. The morphology of injury as determined by reviewing the pattern of disruption on available imaging studies.
2. The integrity of the posterior ligamentous complex (PLC).
3. The neurologic status of the patient. Vaccaro et al. Spine 2005.

Thoracolumbar Injury Classification and Severity Score - TLICS (2005).
� Morphology: Fracture pattern
Vaccaro et al. Spine 2005.

Thoracolumbar Injury Classification and Severity Score - TLICS (2005).
� Integrity of the posterior ligamentous complex (supraspinous ligament, interspinous ligament, ligamentum flavum, and the facet joint capsules).
� Neurologic status.
Vaccaro et al. Spine 2005.
� Score ≤ 3 : nonoperative injury.� Score = 4 might be handled conservatively or surgically.� Score ≥ 5: surgical intervention may be considered.

Thoracolumbar Injury Classification and Severity Score - TLICS (2005).
� Surgical Approach:� Integrity of the PCL.� Neurologic status of the patient.
Vaccaro et al. Spine 2005.

Reproducibility studies
� The TLICS has good reliability and compares favorably to other contemporary thoracolumbar fracture classification systems.
� Studies from the same group of authors
� Short-term experience.

What classification is more used today?
� Review of the literature.� Indexed articles about thoracolumbar fractures
published in the last 10 years (1997-2007): 195.� Using a classification system: 59.
0
5
10
15
20
25
30
35
Denis 1983 Gertzbein1994
Load Sharing1994
Magerl/AO1994
TLICS 2005
Last 5 years5 to 10 years

Summary
� Currently no classification system that has achieved global clinical utility and universal acceptance.
� The attempts to develop all-inclusive schemes are highly divided and not truly useful for physician communication, nor are they reproducible in their ability to repeatedly classify injuries.
� Few studies have evaluated the effectiveness of the different systems.
� More recent classification system needs a long-term follow-up to know its clinical utility.