Embed Size (px)
Citation preview
CLINICAL & APPLIED ANATOMY OF THE RESPIRATORY SYSTEM
DR. AJELETI A. O.
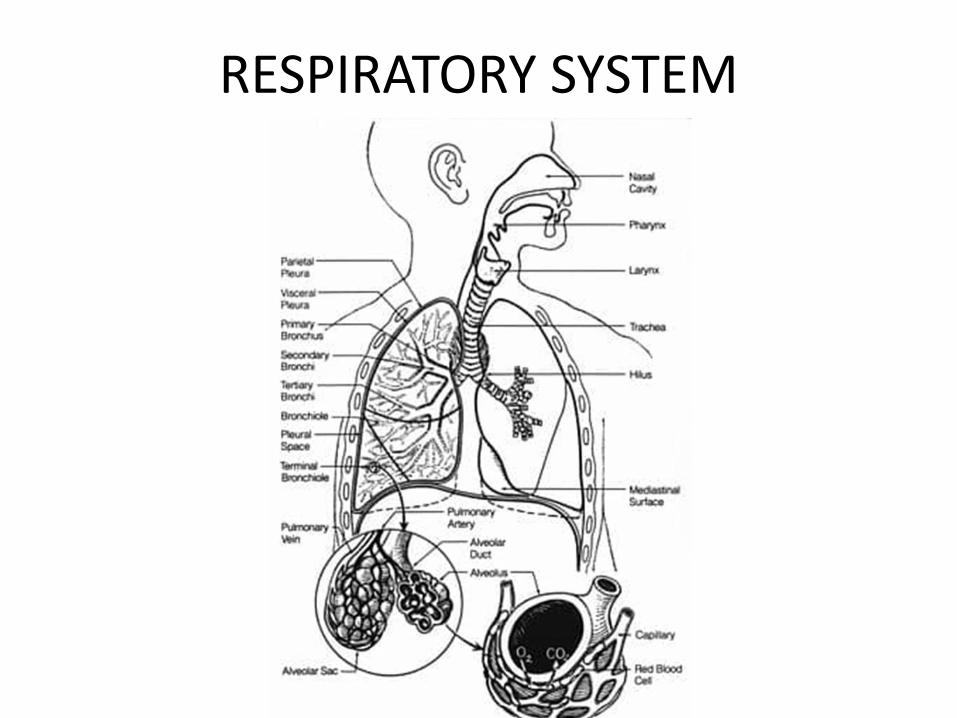
RESPIRATORY SYSTEM
STRUCTURAL DIVISION
• The upper respiratory tract
Nose
Pharynx
Larynx.
• The lower respiratory tract Trachea
Lungs: bronchi, bronchioles, alveolar ducts and alveoli
FUNCTIONAL DIVISION
• CONDUCTING Nose
Pharynx
Larynx
Trachea
Bronchi
Terminal bronchioles
• RESPIRATORY Respiratory bronchioles
Alveolar duct & Alveoli.
RESPIRATORY SYSTEM
FUNCTIONS
• Gaseous exchange
• Olfaction (smelling)
• Vocalization(phonation)
• Breathing(pulmonary ventilation)
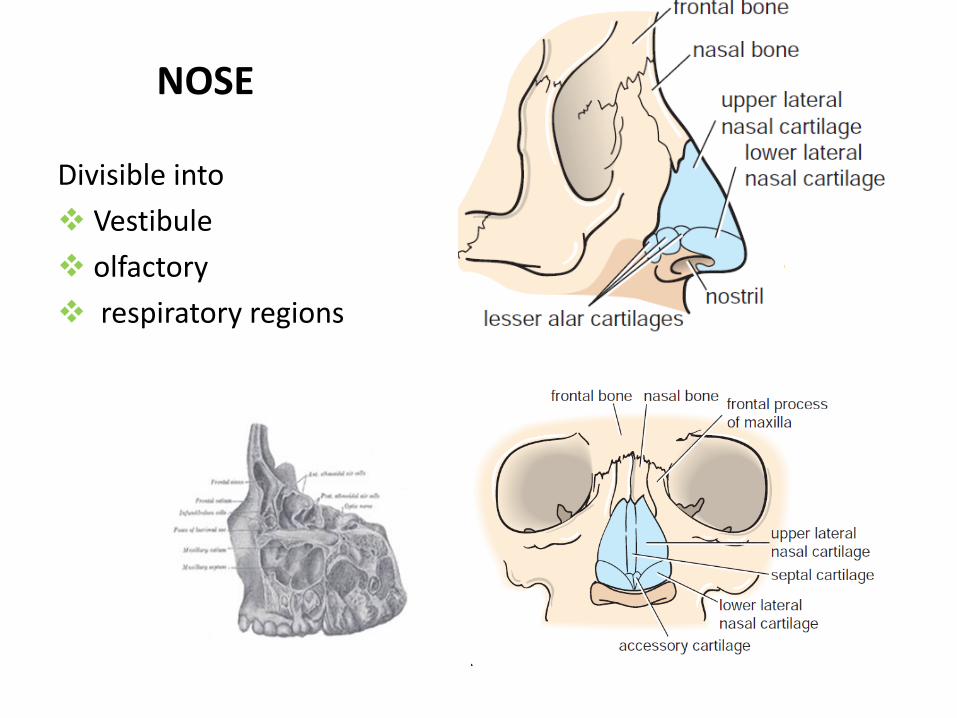
NOSE
Divisible into
Vestibule
olfactory
respiratory regions
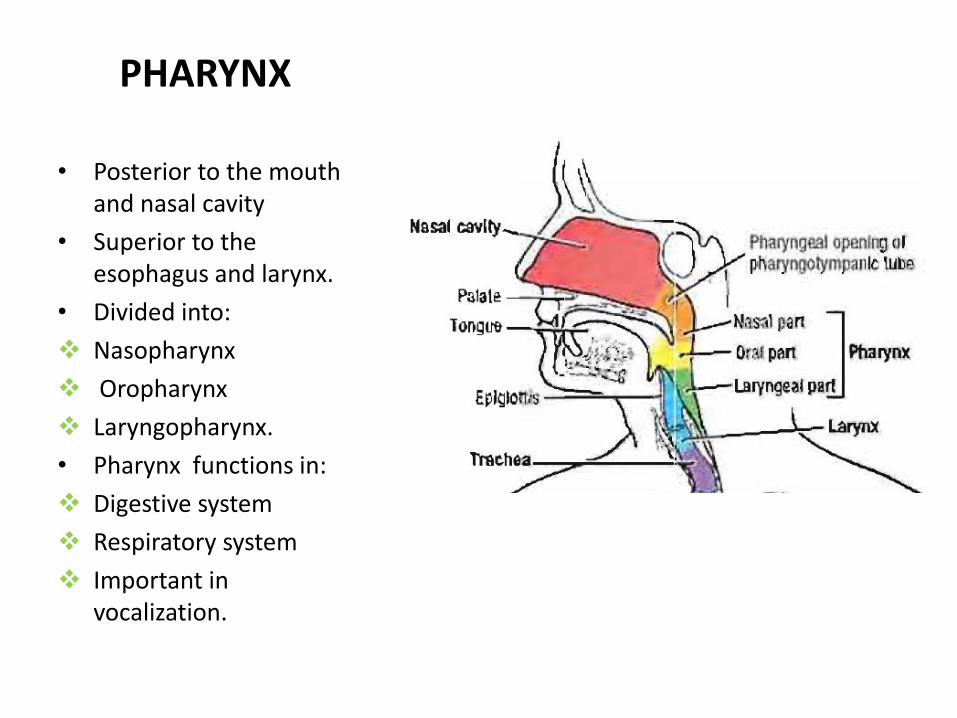
PHARYNX
• Posterior to the mouth and nasal cavity
• Superior to the esophagus and larynx.
• Divided into:
Nasopharynx
Oropharynx
Laryngopharynx.
• Pharynx functions in:
Digestive system
Respiratory system
Important in vocalization.
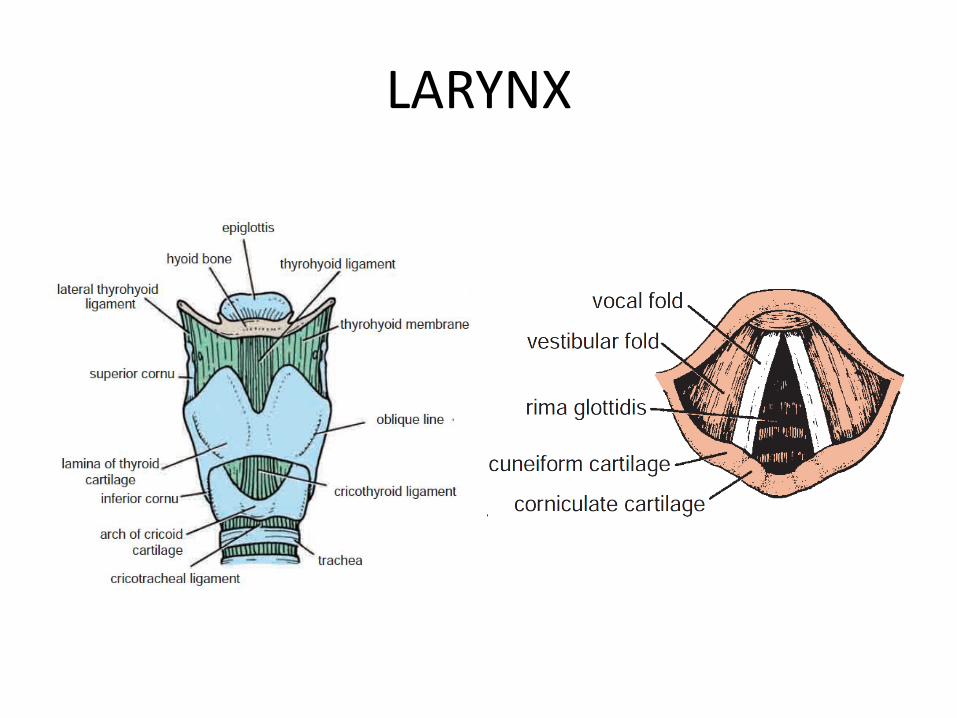
LARYNX

LARYNX
• Organ of voice, a hollow, tubular structure inferior to pharynx and connected to the top of the trachea
• It forms the lower part of the anterior wall of the pharynx
• Has mucous lining of that cavity; on either side of it lie the great vessels of the neck
• Larynx is formed by a rigid framework of bones, cartilages, muscles and ligaments..
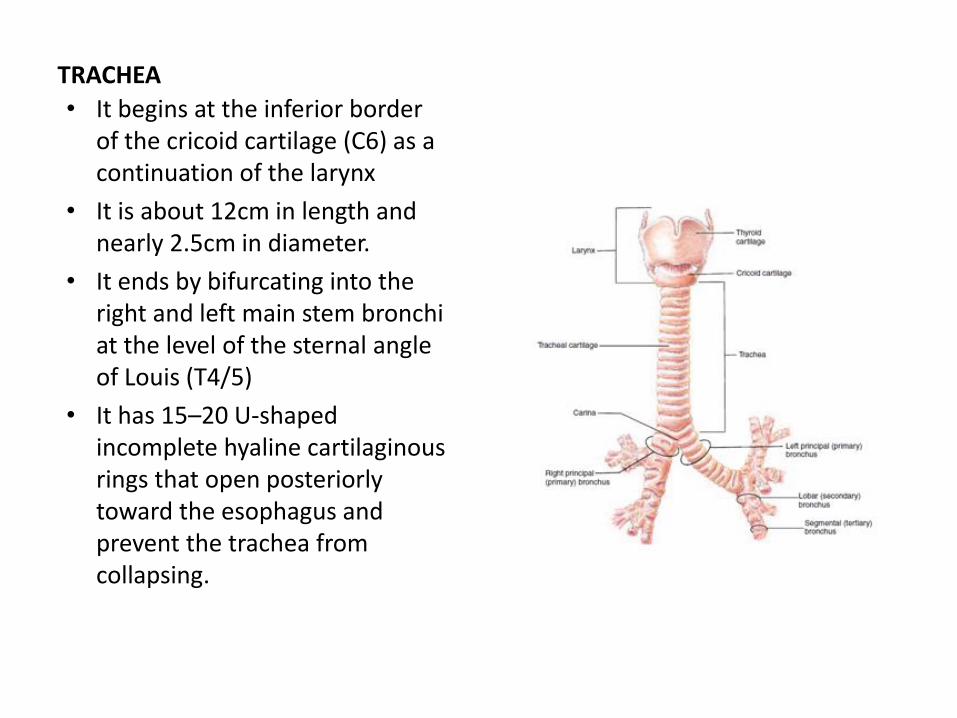
TRACHEA
• It begins at the inferior border of the cricoid cartilage (C6) as a continuation of the larynx
• It is about 12cm in length and nearly 2.5cm in diameter.
• It ends by bifurcating into the right and left main stem bronchi at the level of the sternal angle of Louis (T4/5)
• It has 15–20 U-shaped incomplete hyaline cartilaginous rings that open posteriorly toward the esophagus and prevent the trachea from collapsing.
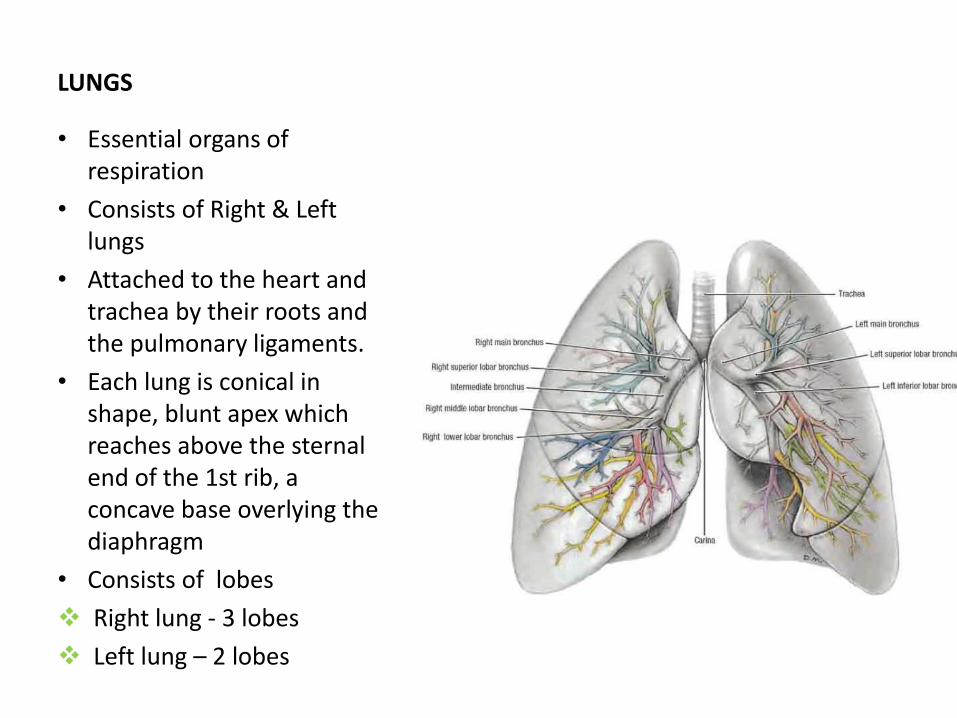
LUNGS
• Essential organs of respiration
• Consists of Right & Left lungs
• Attached to the heart and trachea by their roots and the pulmonary ligaments.
• Each lung is conical in shape, blunt apex which reaches above the sternal end of the 1st rib, a concave base overlying the diaphragm
• Consists of lobes
Right lung - 3 lobes
Left lung – 2 lobes
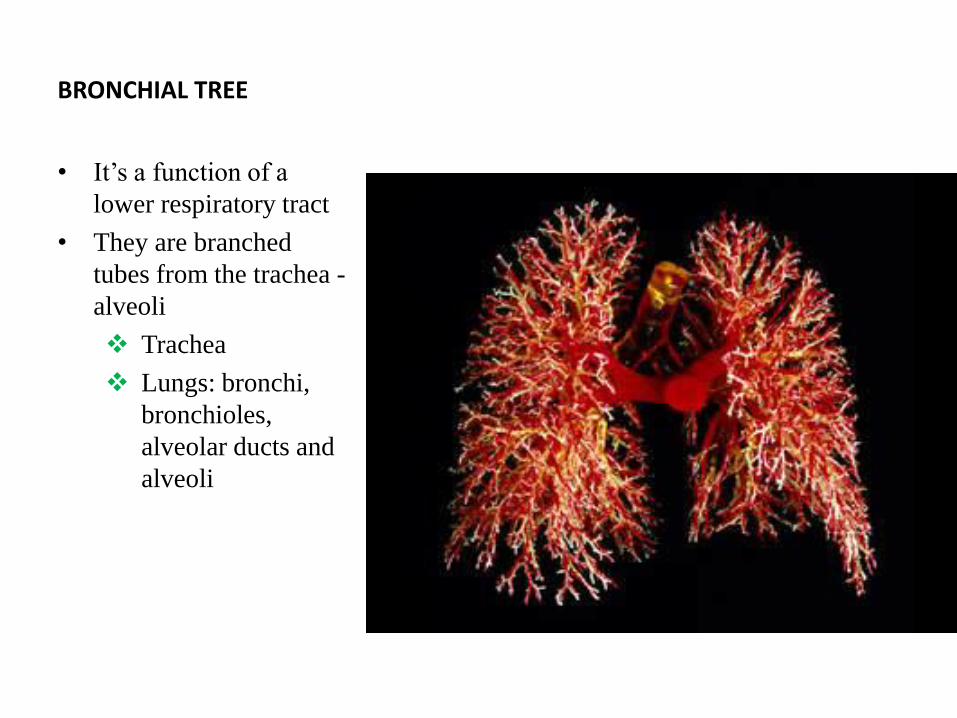
BRONCHIAL TREE
• It’s a function of a
lower respiratory tract
• They are branched
tubes from the trachea -
alveoli
Trachea
Lungs: bronchi,
bronchioles,
alveolar ducts and
alveoli
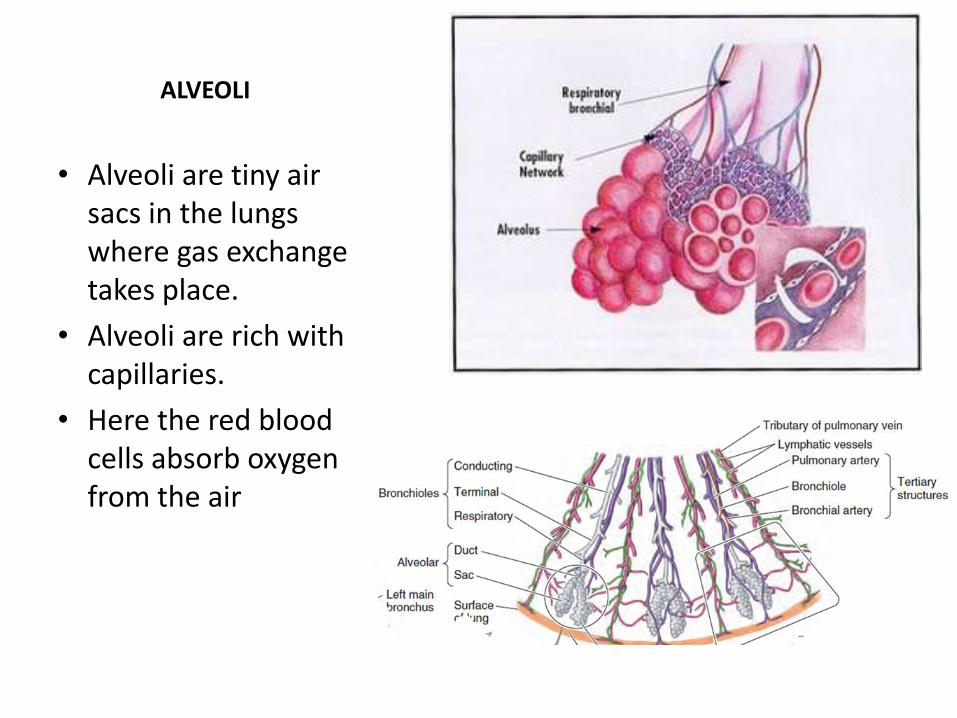
ALVEOLI
• Alveoli are tiny air sacs in the lungs where gas exchange takes place.
• Alveoli are rich with capillaries.
• Here the red blood cells absorb oxygen from the air
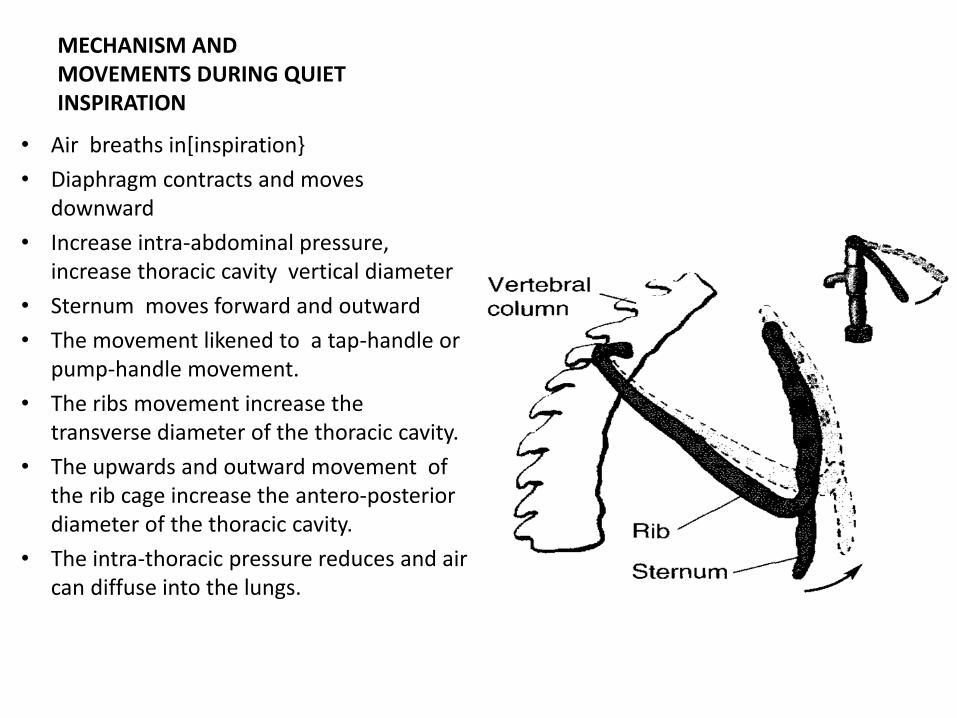
MECHANISM AND MOVEMENTS DURING QUIET INSPIRATION
• Air breaths in[inspiration}
• Diaphragm contracts and moves downward
• Increase intra-abdominal pressure, increase thoracic cavity vertical diameter
• Sternum moves forward and outward
• The movement likened to a tap-handle or pump-handle movement.
• The ribs movement increase the transverse diameter of the thoracic cavity.
• The upwards and outward movement of the rib cage increase the antero-posterior diameter of the thoracic cavity.
• The intra-thoracic pressure reduces and air can diffuse into the lungs.
ANOMALIES & DISEASES OF RESPIRATORY SYSTEM
• AGENESIS OF LUNGS
• TRACHEO-OESOPHAGEAL FISTULA
• BRONCHIAL ASTHMA
• CYSTIC FIBROSIS
• INFANT RESPIRATORY DISTREESS
• EMPHYSEMA
• PLEURAL EFFUSION
• BRONCHOGENIC CARCINOMA
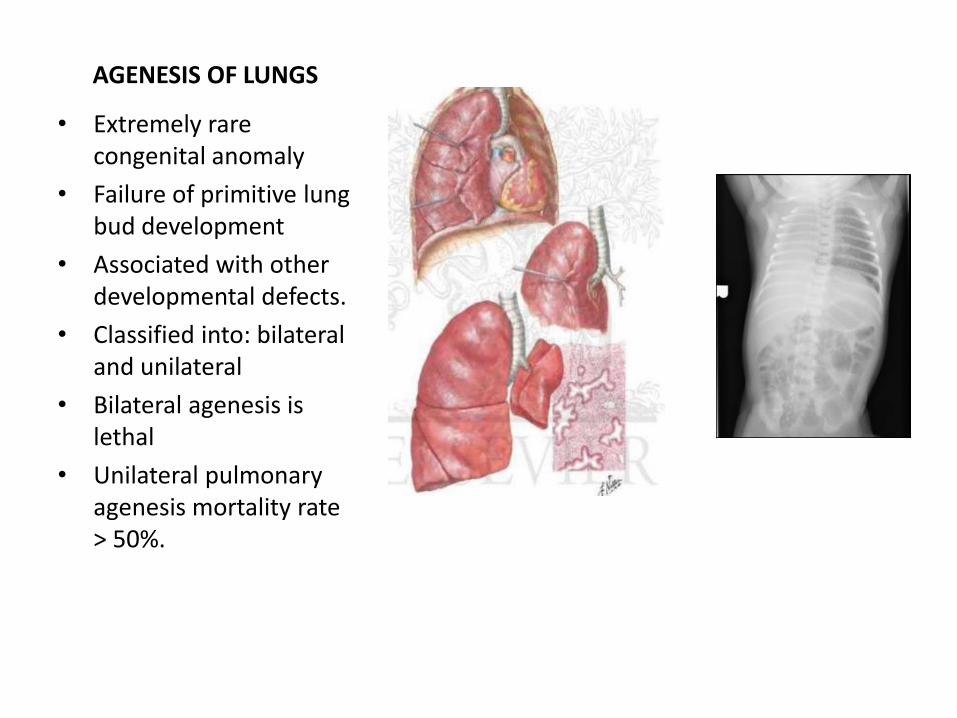
AGENESIS OF LUNGS
• Extremely rare congenital anomaly
• Failure of primitive lung bud development
• Associated with other developmental defects.
• Classified into: bilateral and unilateral
• Bilateral agenesis is lethal
• Unilateral pulmonary agenesis mortality rate > 50%.
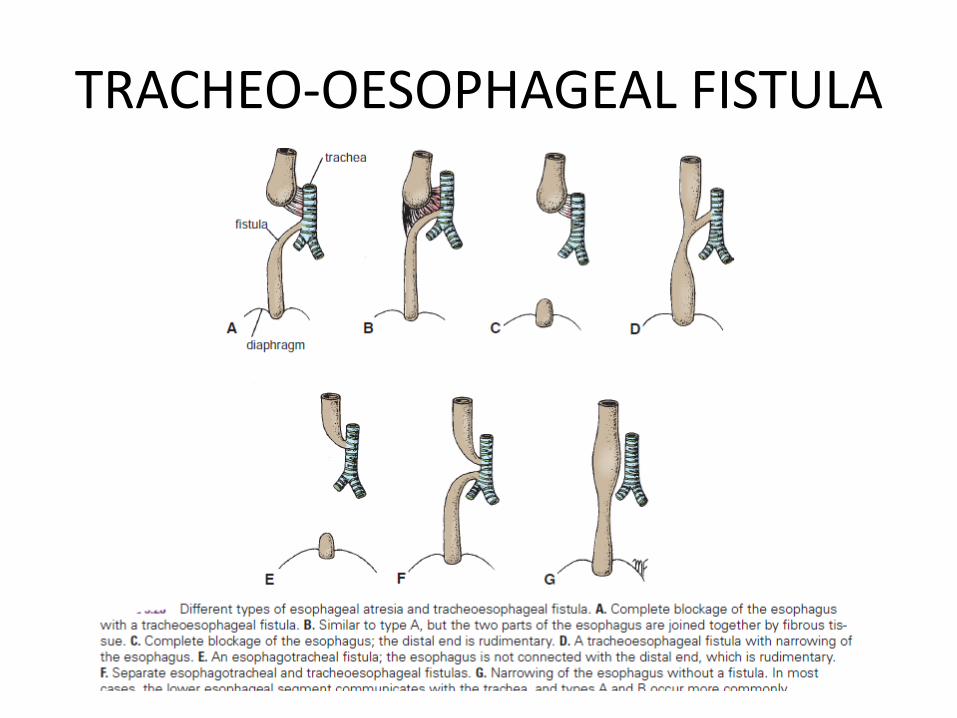
TRACHEO-OESOPHAGEAL FISTULA
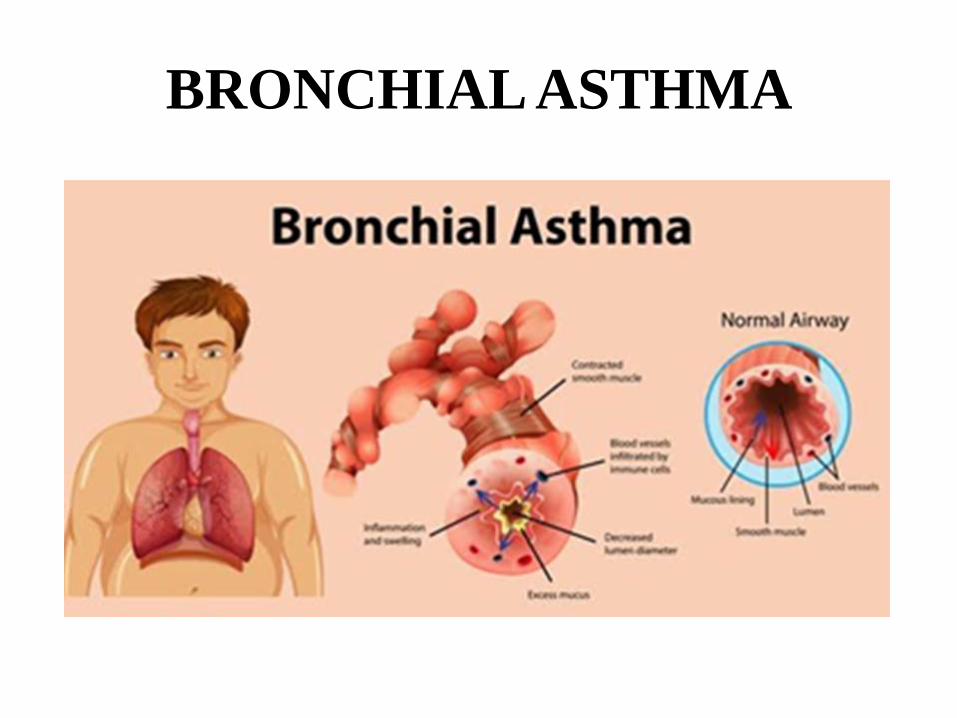
BRONCHIAL ASTHMA
• Spasm of the smooth muscle in the wall of the bronchioles as a result of inflammation from allergic reactions.
• Classification base on frequency and severity of the signs
mild intermittent: about two days a week and two nights a month
mild persistent: > two times a week, not more than once in a day
moderate persistent: once a day and more than one night a week
Severe persistent: throughout the day on most days and frequently at night.
• Signs and symptoms:
Wheezing and shortness of breath.
Lungs becomes distended
Thoracic cage is enlarged forming the so-called barrel chest.
Increased mucus production
Edema of bronchial walls.
BRONCHIAL ASTHMA
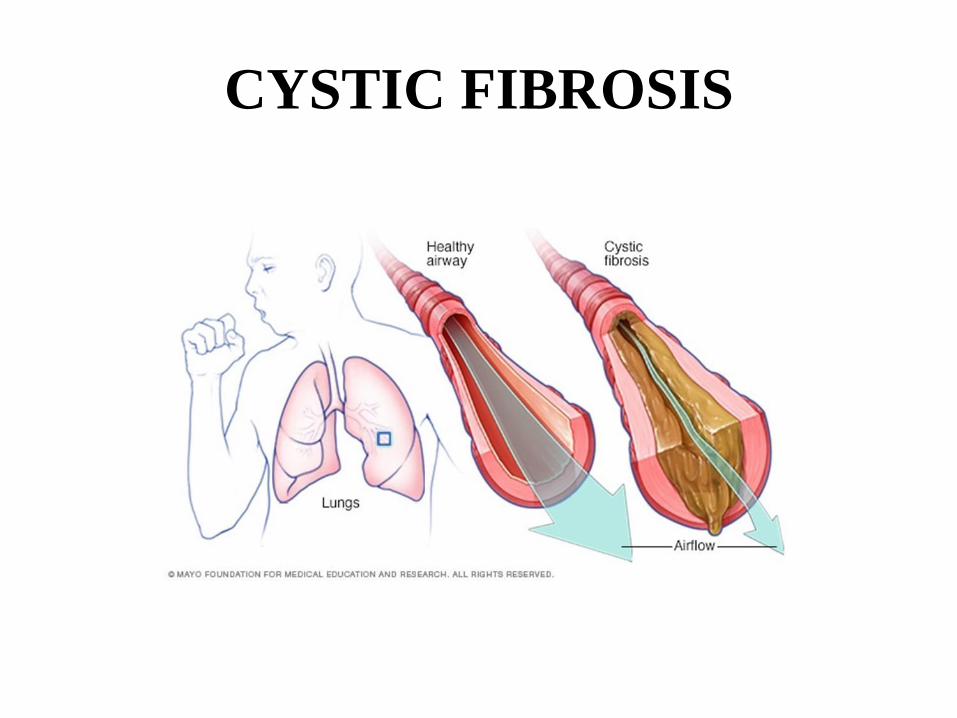
CYSTIC FIBROSIS
• Congenital metabolic disorder in which the secretions of exocrine glands are abnormal in the lungs
• Na+ and water move out of airways, leaving their other secretions sticky.
• Over time the mucus builds up in the airways of the patient and makes it hard to breathe
• Infection from the trapped germs hence formation of cysts and fibrotic tissue
• Signs and symptoms:
Respiratory: wheezing or trouble breathing,
frequent lung infections.
Non- respiratory: trouble with bowel movements infertility(in men)
trouble gaining weight.
CYSTIC FIBROSIS
LUNG DISEASES AFFECTING ALVEOLI:
INFANT RESPIRATORY DISTREESS
• Lung disease due to incomplete differentiation of the type II alveolar cells
• Resultant deficit in the surfactant production
• Occurs in babies born before the 28th week of gestation
• Incompatible with life.
• Signs and symptoms:
difficulty in breathing
inability to expand the lungs.
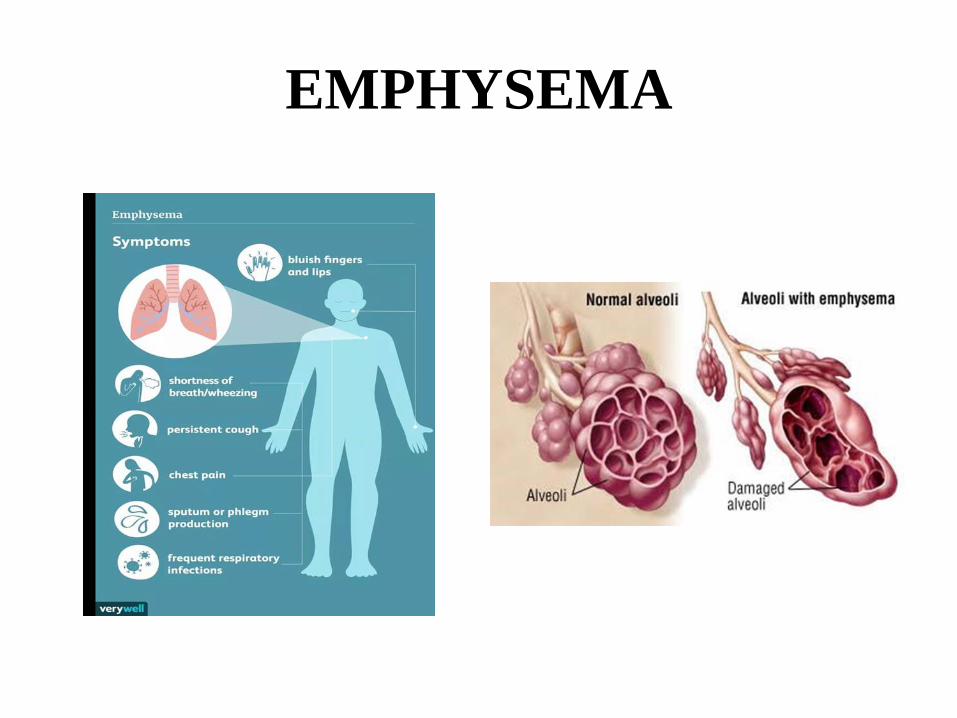
EMPHYSEMA
• Lung condition that causes shortness of breath due to the damage of the air sacs
• Over time the inner walls of the air sacs weaken and rupture thereby creating larger air spaces rather than small, numerous ones reducing the surface area of the lungs
• It is also associated with chronic bronchitis
• Smoking is the leading cause of emphysema.
• Signs and symptoms: shortness of breath
EMPHYSEMA
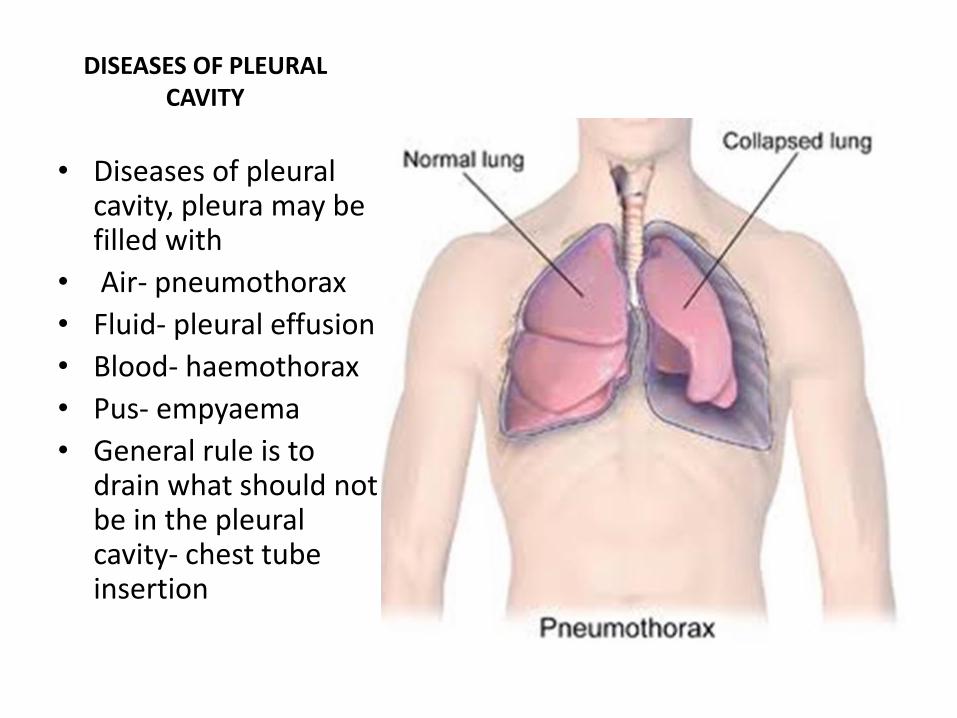
DISEASES OF PLEURAL CAVITY
• Diseases of pleural cavity, pleura may be filled with
• Air- pneumothorax
• Fluid- pleural effusion
• Blood- haemothorax
• Pus- empyaema
• General rule is to drain what should not be in the pleural cavity- chest tube insertion
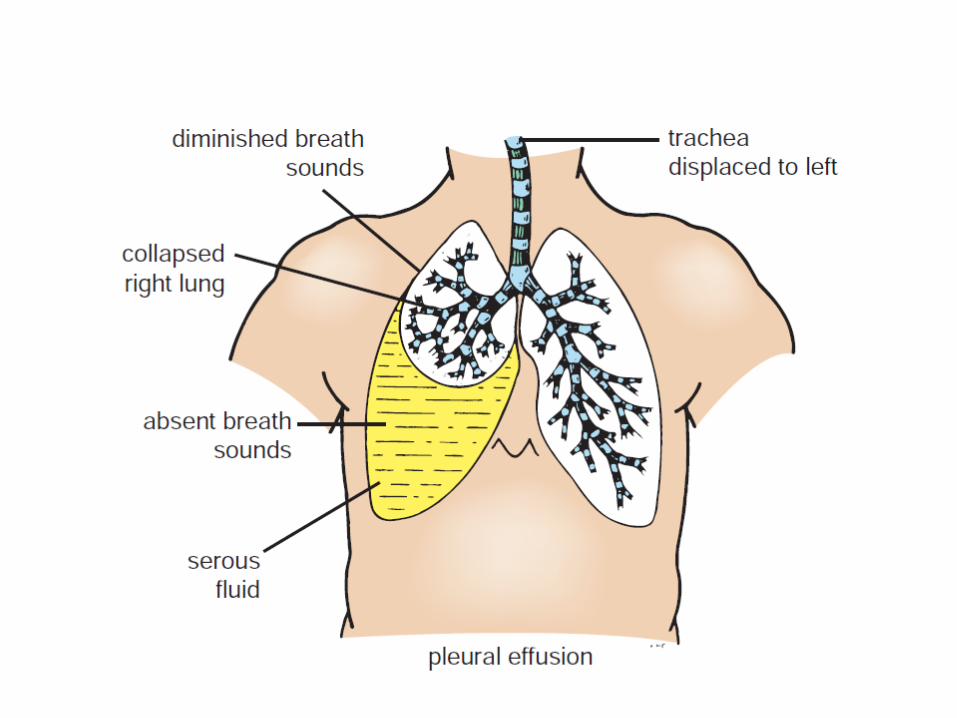
PLEURAL EFFUSION
• Pleural effusion is an unusual amount of fluid in the lungs. The lung is normally invested in a pleural cavity that contains pleural fluid. However, there could be accumulation of excess pleural fluid called pleural effusion
• Causes: leakage from other organs, autoimmune conditions, pulmonary embolism, cancer, infections etc.
• Signs and symptoms: shortness of breath, chest pain, fever, cough.
• Diagnosis: computed tomography, chest x-ray, ultrasound.
• Classification: transudative & exudative
• Treatment: tube thoracostomy, pleural drain, plerual decortication, pleurodesis.
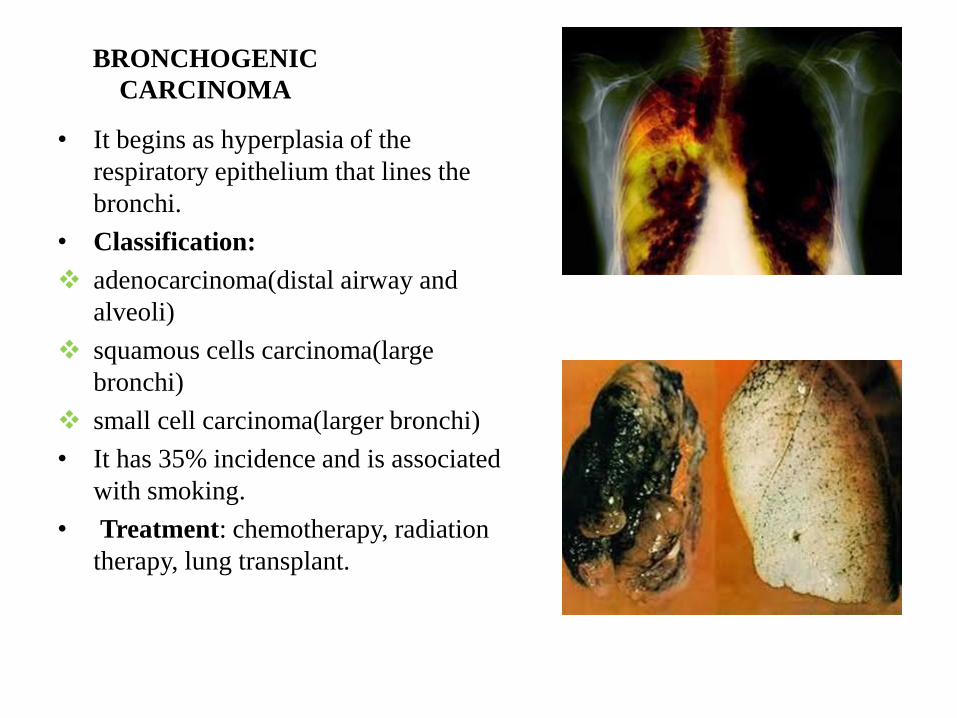
BRONCHOGENIC
CARCINOMA
• It begins as hyperplasia of the
respiratory epithelium that lines the
bronchi.
• Classification:
adenocarcinoma(distal airway and
alveoli)
squamous cells carcinoma(large
bronchi)
small cell carcinoma(larger bronchi)
• It has 35% incidence and is associated
with smoking.
• Treatment: chemotherapy, radiation
therapy, lung transplant.
ASPIRATION OF FOREIGN
BODIES
• When a strange object is aspirated in a child
for example, it most likely enters the right
main bronchus due to its width and
(less)obliquity.










![Anatomy and Physiology Respiratory System [Tab 2] Respiratory System](https://img.pdfslide.net/doc/110x75/56649ebd5503460f94bc631f/anatomy-and-physiology-respiratory-system-tab-2-respiratory-system.jpg)