Embed Size (px)
Citation preview

1
CLINICAL and EMPIRICAL FINDINGS ABOUT COLLEGE
STUDENT SUICIDE
Morton M. Silverman, M.D.Senior Advisor, SPRC
Medical Consultant, The Jed FoundationColumbia University/NYSPI/AFSP Conference
New York, NYApril 21, 2005

2
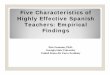
HIVDiabetes MellitusCongenital
AnomaliesCerebrovascularCerebrovascular
SuicideCerebrovascularCerebrovascularHIVSepticemia
LiverDisease
LiverDisease
Diabetes MellitusChronic Low. Respiratory Dis.
Chronic Low. Respiratory Dis.
Chronic Low. Respiratory Dis.HomicideHIV
CongenitalAnomalies
Heart Disease
DiabetesMellitus
HIVHeart DiseaseHeart
DiseaseSuicide
CerebrovascularSuicideMalignant
NeoplasmsMalignant
NeoplasmsHomicide
UnintentionalInjuries
Heart Disease
HomicideSuicideCongenitalAnomalies
Heart Disease
MalignantNeoplasmsSuicideHomicide
MalignantNeoplasms
MalignantNeoplasms
UnintentionalInjury
UnintentionalInjury
UnintentionalInjuries
UnintentionalInjuries
Age Groups5 - 14 15-24 25-34 45-64
Suicide Among Leading Causes of DeathsSuicide Among Leading Causes of DeathsUnited States United States -- 20022002
35-44
9
8
7
6
5
4
3
2
1

3
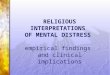
Suicide Rates by Ethnicity and Age GroupUnited States, 1995-1999
0
5
10
15
20
25
30
35
Age Group in Years
Rat
e pe
r 100
,000
pop
ulat
ion
Eur-Amer Non-LatinoAfr-Amer Non-LatinoNative AmericanAsian-PILatino
0-4 5-9 10-14
15-19
20-24
25-29
30-34
35-39
40-44
45-49
50-54
55-59
60-64
65-69
70-74
75-79
80-84 85
+

4
The U.S. College and The U.S. College and University PopulationUniversity Population
More teenagers and young adults die from suicide than from all medical illnesses combined
Approx. 14 million students currently attend over 4,500 American colleges and universities.
An estimated 8 million college/university students are between ages 18-24 (representing over one-quarter of all 18-24 year-old in the U.S.)
Students’ health-risk behaviors, including suicidal behavior, have been only partially documented.
College and university students constitute an important, but in many respects underserved, population for public health interventions.
Why the Rise?Why the Rise?
Earlier identification and referral (high school)Improved treatment optionsDecreased stigma (high school & college)Increased accessibility/availabilityGreater parity with physical healthDecreased 3rd party coverage & reimbursementIncreased perturbation and uncertainty in worldCohort effect?

5
Evidence for Rise in Psychological DistressEvidence for Rise in Psychological Distress
Big 10 Universities Student Suicide Study (1980-1990)CDC’s YRBS (2001; 2003)CDC’s NCHRBS (1995)ACHA Spring 2000 NCHAAUCCCD’s Annual SurveysPublished literatureChickering Insurance Company figures
Percentage of High School Students Who Felt Percentage of High School Students Who Felt Sad or Hopeless,* 1999 Sad or Hopeless,* 1999 -- 20032003
* Felt so sad or hopeless almost every day for > 2 weeks in a row that they stopped doing some usual activities during the 12 months preceding the survey1 No change over time
National Youth Risk Behavior Surveys, 1999 – 2003
28.3 28.3 28.61
0
20
40
60
80
100
1999 2001 2003
Perc
ent

6
Percentage of High School Students Who Seriously Percentage of High School Students Who Seriously Considered Attempting Suicide,* 1991 Considered Attempting Suicide,* 1991 -- 20032003
* During the 12 months preceding the survey1 Significant linear decrease and quadratic effect, p < .05
National Youth Risk Behavior Surveys, 1991 - 2003
29.024.1 24.1
20.5 19.3 16.9119.0
0
20
40
60
80
100
1991 1993 1995 1997 1999 2001 2003
Perc
ent
Percentage of High School Students Who Percentage of High School Students Who Made a Suicide Plan,* 1991 Made a Suicide Plan,* 1991 -- 20032003
* During the 12 months preceding the survey1 Significant linear decrease, p < .05
National Youth Risk Behavior Surveys, 1991 - 2003
18.6 19.0 17.7 15.7 14.5 16.5114.8
0
20
40
60
80
100
1991 1993 1995 1997 1999 2001 2003
Perc
ent

7
Percentage of High School Students Who Actually Percentage of High School Students Who Actually Attempted Suicide,* 1991 Attempted Suicide,* 1991 -- 20032003
* One or more times during the 12 months preceding the survey1 No change over timeNational Youth Risk Behavior Surveys, 1991 - 2003
7.3 8.6 8.7 7.7 8.3 8.518.8
0
20
40
60
80
100
1991 1993 1995 1997 1999 2001 2003
Perc
ent
Percentage of High School Students Percentage of High School Students Whose Suicide Attempt Required Whose Suicide Attempt Required Medical Attention,* 1991 Medical Attention,* 1991 -- 20032003
* During the 12 months preceding the survey1 No change over time
National Youth Risk Behavior Surveys, 1991 - 2003
1.7 2.7 2.8 2.6 2.6 2.912.6
0
20
40
60
80
100
1991 1993 1995 1997 1999 2001 2003
Perc
ent

8
ECA STUDYECA STUDY

9

10
BIG 10 UNIVERSITIES STUDENT SUICIDE BIG 10 UNIVERSITIES STUDENT SUICIDE STUDYSTUDY
BIG 10 UNIVERSITIES STUDENTSUICIDE STUDY
1980 - 1990

11

12

13

14

15

16

17
NCHA vs. NCHRBS FindingsNCHA vs. NCHRBS Findings
68 (1.5%)
39 (1.4%)
29 (1.7%)
Attempted Suicide
469 (10.0%)
302 (10.4%)
167 (9.3%)
Seriously Considered Attempting Suicide
NCHRBS 1995(N=4,609)
214 (1.5%)
126 (1.4%)
88 (1.6%)
Attempted Suicide
1,374 (9.5%)
893 (9.9%)
481 (8.7%)
Seriously Considered Attempting Suicide
TotalFemaleMaleNCHA Spring 2000(N=15,977)
AUCCCD 2003 Survey AUCCCD 2003 Survey
81.4% report seeing more students with serious psychological problems than 5 years ago. This is the #1 service provision concern (772%) and the #1 administrative concern (49.5%)
40.7% of clients have severe psychological problems
Utilization of services: 9.8% is average (goes up to 40%) for entire campus per year
160 suicides in 2002-03, but only 31 were current or former counseling center clients

18

19

20
FACTS AND FIGURESFACTS AND FIGURES
Upwards of 20% of students use antidepressants at some point in their college yearsAUCCCD reports 18% of students seeking help at counseling centers received psychotropic meds –up from only 7% in 19921.6 million incoming freshmen experience episodes of depression
Jed Foundation/NMHA estimate 1088 suicides/year on college campuses
CoCo--MorbidityMorbidity
7-10% with MDD die from suicide
60% completed suicides have an MDD diagnosis
8-10% with bipolar disorder die from suicide
over 50% of suicides have alcohol or other drugs in their system

21
CoCo--MorbidityMorbidity
a sleep disturbance is a symptom of depression, anxiety, and/or stress
perceived stress can be a symptom of depression
alcohol is often used to self-medicate for anxiety, stress, or depression
impulsivity, aggressive behavior, and irritability are associated with suicidal behavior
Overlap of spheres of influence for Overlap of spheres of influence for suicidal behaviorsuicidal behavior
Individual Administration
School CommunityHealth/
Mental Health Svcs.

22

23

24
Prevent Suicide and Promote Mental Health
Awareness & Well-BeingLeadership: President’s Office
Training of Mental Health Service (MHS) Providers to:
• Identify and treat depression, threats of suicide, and other emotional disorders
• Refer cases as appropriate• Lead: Suicide prevention experts• Target: MHS, community resources,
local hospitalsLife Skills Development (Protective
Factors) to:• Improve students’ management of
the rigors of college life• Equip students with tools to
recognize and manage triggers and stressors
• Lead: VP of Student Affairs, Deans of Students, MHS, Faculty & Staff, Advisors, Residential Life
• Target: Students
Educational Programs to:• Train gatekeepers and students to:
(1) identify signs of individuals in distress; (2) take the steps that get them help
• Lead: Provost, VP Student Affairs• Target: Students and gatekeepers
(Deans of Students, Faculty & Staff, Advisors, Residential Life, Student Gov’t, Student & Greek Orgs., Athletic Dept., Dining Services, Public Safety, Chaplainry)
Pre-Enrollment Survey to:• Identify high-risk and potentially
high-risk students• Provide snapshot of incoming class• Proactively work (programs,
treatment) with identified students• Lead: Admission Office or Freshman
Dean with MHS and the Health Service• Target: Incoming first-year students
Social Network Promotion to:• Reduce student isolation and
promote feeling of belonging• Encourage the development of
smaller groups within the larger campus community
• Lead: Deans of Students, Faculty & Staff, Residential Life, Student Gov’t, Student & Greek Orgs., Chaplainry
• Target: Students
Social Marketing to:• Stimulate campus-wide cultural
change that de-stigmatizes mental health, removes barriers, and encourages help-seeking behavior
• Target both high-risk students and general campus community
• Lead: VP Student Affairs, Deans of Students, MHS, Marketing Department, Campus Media
• Target: Entire campus community
Draft 8-8-03
Crisis Management to:• Establish policies and implement
programs (including medical leave and re-entry) that respond to suicide attempts and high-risk behavior
• Respond with comprehensive postvention program
• Lead: VP Student Affairs, MHS• Target: Students; gatekeepers (with
implementation responsibility)
Means Restriction to:• Limit access to lethal means• Lead: Buildings & Grounds, Public
Safety, Residential Life, Chemistry Dept., Athletic Dept.
• Target: Entire campus community

25
UlifelineUlifeline
Schools can join the Ulifeline NetworkTool that helps students cope with the stress of everyday college lifeEmpowers students to help one another and themselves
• Self E-Valuator• Q&A
Free serviceStudent-friendlyConnects students to the counseling services available to them on campus
Internal resources of a university can be used to create an effective awareness of Ulifeline
Ulifeline.org
Ulifeline.org leverages the anonymity of the internet to provide students with anon-threatening link to their counseling centers as well as important mental health information

26
For more information:
See: www.jedfoundation.org
See: www.ulifeline.org
E-mail: [email protected]
Contact SPRCContact SPRC
Phone: 877-GET-SPRC (438-7772)TTY: 617-964-5448Web: www.sprc.orgEmail: [email protected]: Suicide Prevention Research Center55 Chapel StreetNewton, MA 02158-1060