Embed Size (px)
Citation preview

DOI: 10.1542/peds.2011-1545; originally published online July 9, 2012; 2012;130;315Pediatrics
Shalea J. Piteau, Michelle G.K. Ward, Nick J. Barrowman and Amy C. PlintNonabusive Head Trauma: A Systematic Review
Clinical and Radiographic Characteristics Associated With Abusive and
http://pediatrics.aappublications.org/content/130/2/315.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2012 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Dartmouth College Library on August 6, 2014pediatrics.aappublications.orgDownloaded from at Dartmouth College Library on August 6, 2014pediatrics.aappublications.orgDownloaded from

Clinical and Radiographic CharacteristicsAssociated With Abusive and NonabusiveHead Trauma: A Systematic Review
abstractBACKGROUND AND OBJECTIVE: To systematically review the literatureto determine which clinical and radiographic characteristics are as-sociated with abusive head trauma (AHT) and nonabusive head trauma(nAHT) in children.
METHODS:We searched MEDLINE, EMBASE, PubMed, conference proceed-ings, and reference lists to identify relevant studies. Two reviewers in-dependently selected studies that compared clinical and/or radiographiccharacteristics including historical features, physical exam and imagingfindings, and presenting signs or symptoms in hospitalized children#6years old with AHT and nAHT.
RESULTS: Twenty-four studies were included. Meta-analysis wascomplicated by inconsistencies in the reporting of characteristicsand high statistical heterogeneity. Notwithstanding these limitations,there were 19 clinical and radiographic variables that could bemeta-analyzed and odds ratios were determined for each variable.In examining only studies deemed to be high quality, we found thatsubdural hemorrhage(s), cerebral ischemia, retinal hemorrhage(s),skull fracture(s) plus intracranial injury, metaphyseal fracture(s),long bone fracture(s), rib fracture(s), seizure(s), apnea, and no adequatehistory given were significantly associated with AHT. Epiduralhemorrhage(s), scalp swelling, and isolated skull fracture(s) weresignificantly associated with nAHT. Subarachnoid hemorrhage(s),diffuse axonal injury, cerebral edema, head and neck bruising, anybruising, and vomiting were not significantly associated with eithertype of trauma.
CONCLUSIONS: Clinical and radiographic characteristics associatedwith AHT and nAHT were identified, despite limitations in the literature.This systematic review also highlights the need for consistent criteriain identifying and reporting clinical and radiographic characteristicsassociated with AHT and nAHT. Pediatrics 2012;130:315–323
AUTHORS: Shalea J. Piteau, MD, MSc,a Michelle G.K. Ward,MD,b Nick J. Barrowman, PhD,c and Amy C. Plint, MD, MScb,d
aDepartment of Pediatrics, Queen’s University, Kingston, Ontario,Canada; Departments of bPediatrics and dEmergency Medicine,University of Ottawa, Ottawa, Ontario, Canada; and cClinicalResearch Unit, Children’s Hospital of Eastern Ontario ResearchInstitute, Ottawa, Ontario, Canada
KEY WORDSabusive head trauma, head injury, children, abuse, systematicreview
ABBREVIATIONSAHT—abusive head traumaCI—confidence intervalnAHT—nonabusive head traumaOR—odds ratio
Drs Piteau and Plint conceived and designed the study;Drs Piteau and Ward screened literature search results andidentified articles for retrieval, reviewed full papers forinclusion, and extracted data for meta-analysis; Dr Barrowmananalyzed the data; and all authors interpreted the data, criticallyrevised the draft, and gave final approval of the version to bepublished. Dr Piteau is the guarantor for the study.
www.pediatrics.org/cgi/doi/10.1542/peds.2011-1545
doi:10.1542/peds.2011-1545
Accepted for publication Apr 9, 2012
Address correspondence to Shalea Piteau, MD, MSc, Departmentof Pediatrics, Kingston General Hospital, Queen’s University, 76Stuart St, Kingston, Ontario, Canada K7L 2V7. E-mail:[email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: No external funding.
COMPANION PAPER: A companion to this article can be found onpage 347, and online at www.pediatrics.org/cgi/doi/10.1542/peds.2012-1442.
PEDIATRICS Volume 130, Number 2, August 2012 315
REVIEW ARTICLE
at Dartmouth College Library on August 6, 2014pediatrics.aappublications.orgDownloaded from

Abusive head trauma (AHT) is the mostcommon cause of traumatic death inchildren younger than 1 year1 and is themost common cause of death due tochild abuse.1 Survivors of AHT are leftwith significant morbidity, with 45%having permanent neurologic sequelaecompared with 5% of nonabuse cases.2
While the annual incidence of AHT isestimated at ∼24 to 34 per 100 000children younger than 1 year,3–5 this islikely an underestimate because manycases are not brought to medical at-tention and others are not recognizedas abuse. AHT in children can be diffi-cult to diagnose because the symptomsare nonspecific, the history is often in-accurate, and the victim is often pre-verbal. In 1 study, physicians missedthe diagnosis on initial presentation inone-third of cases and this resulted inrepeated trauma, increased morbidity,and death.6 As there is no gold stan-dard diagnostic test for child abuse,the diagnosis relies on clinical andradiographic features as well as sup-porting social and child welfare infor-mation. AHT may be recognized in partby historical features (eg, no history oftrauma, a low-impact trauma history,a changing or inconsistent history, ora history incompatible with the injuriesor incompatible with the child’s develop-mental stage), certain types of intra-cranial injuries (eg, diffuse subduralhemorrhages), and associated injuries(eg, retinal hemorrhages, metaphysealfractures, and patterned bruising).6–12
We planned a systematic review tosummarize the best available evidencecomparing the clinical and radiographiccharacteristics of AHT and nonabusivehead trauma (nAHT) in hospitalized chil-dren. By identifying these features wehope to help front-line clinicians in thedifficult task of distinguishing betweenAHT and nAHT trauma. Such informationmay improve outcomes for the victimsof abuse and their siblings through theearly identification of child abuse.
METHODS
Wefollowedaprotocol for this review, inwhich all eligibility criteria, outcomes,and analyses were specified a priori(available from authors on request).
Search Strategy
The main search strategy (Supplemen-tal Information 1) was developed by anexperienced librarian and includedMEDLINE (1950 to November, week 2,2010) and EMBASE (1980 to week 45,2010); both searches were executedthrough the Ovid interface. Other searchstrategies included searches of relevantconference proceedings (American Acad-emy of Pediatrics, Canadian PediatricSociety, Pediatric Academic Societies,Society for Academic Emergency Medi-cine, Canadian Association of Emer-gency Physicians, American College ofEmergency Physicians) for 1999–2009,contact with the primary author of rele-vant studies, and review of the referencelists of included studies and relevantreviews. There was no restriction onyear, language, or publication status.Studies identified as eligible were usedas seed articles for a PubMed-relatedarticle search conducted on November18, 2010 (Supplemental Information 1).The first 50 related articles (ranked byrelevance) not previously identified bythe subject search were retained andscreened.
Study Selection
Studieswere included if they comparedhistorical features, physical examina-tion or imaging findings, or presentingsigns or symptoms of AHT and nAHTin hospitalized children #6 years old.Head trauma was defined as skullfracture on computed tomography, MRI,or plain radiography or at least 1 of thefollowing on computed tomographyor MRI: subdural hemorrhage, epiduralhemorrhage, subarachnoid hemorrhage,intraparenchymal hemorrhage, braincontusion, diffuse axonal injury, cerebral
edema, and hydrocephalus. Exclusioncriteria included duplicate publications,review articles, opinion pieces, consen-sus statements, studies evaluating abu-sive injury exclusive of head trauma,noncomparative studies evaluating AHT,studies evaluating nonhospitalized chil-dren, studies examining only clinicaloutcomes, management or postmorteminvestigations, or studies judged to bemethodologically weak owing to signifi-cant bias. Studies were judged to havesignificant bias if the same variableswere applied in both the diagnosis andthe characterization of abuse; for exam-ple, the pattern of head trauma was theprimary factor used to define abuse andthenwas analyzed as a variable of abuse.
Two reviewers (S.J.P. and M.G.K.W.) in-dependently reviewed the titles andabstracts generated by the search toidentifypotentially relevant articles. The2reviewers then independently assessedthe full article by using a standardizedform with eligibility criteria establisheda priori. Disagreementswere resolved byconsensus or by a third reviewer (A.C.P.)as necessary. The third reviewer (A.C.P.)additionally reviewed the eligibility of allstudies deemed eligible by both review-ers (S.J.P. and M.G.K.W.), and disagree-ments were resolved by consensus.Authors were asked for clarification whenit was unclear whether all children in thestudy met our definition of head trauma.
Assessment of MethodologicalQuality
Two independent reviewers (S.J.P. andM.G.K.W.) assessed study quality anddisagreements were resolved by con-sensus or by the third reviewer (A.C.P.).Reviewerswerenotblinded toauthororother publication details. Study qualitywas assessed according to the ability toaccurately categorize the etiology ofhead trauma as abusive or nonabusivebased on a priori criteria. In the absenceof a gold standard diagnostic test forchild abuse, the quality of the a priori
316 PITEAU et al at Dartmouth College Library on August 6, 2014pediatrics.aappublications.orgDownloaded from

criteria was assessed based on its abilityto be free of bias and circular logic toarrive at a diagnosis of child abuse.Specifically, we applied the previouslypublished 5-point scale, “ranking criteriafor the definition of abuse,” to categorizestudies as high (score of 1 or 2) or lowquality (score of 3–5) (Table 1).7,13–17
Data Extraction
Two reviewers (S.J.P. and M.G.K.W.) in-dependently extracted data to a stan-dardized form and entered it intoMicrosoft Excel (Microsoft Corp, Red-mond, WA). Only consensus data wereused in the review. Extracted data in-cluded: (1) characteristics of the study(design, year of publication, etc), (2)description of study populations (age,number of participants, etc), (3) stand-ards used to determine abusive andnonabusive nature of injury, (4) type ofhead trauma (subdural hemorrhage,epidural hemorrhage, subarachnoidhemorrhage, intraparenchymal hem-orrhage, skull fracture plus intracranialinjury, isolated skull fracture, cerebralischemia, cerebral edema, and diffuseaxonal injury), and (5) other clinicalvariables. Other clinical variables in-cluded historical features (no adequatehistory, history of low-impact trauma,inconsistent history, the injury wasblamed on home resuscitative effortsor on siblings, or delay in seeking careafter an injury), presenting signs andsymptoms (seizures at orwithin 24hours
of presentation, vomiting, apnea at pre-sentation, lethargy, abnormal neurologicstatus such as cranial nerve palsy orparesis), other physicalfindings (such asscalpswelling,retinalhemorrhage(s), ribfracture(s), long bone fracture(s), meta-physeal fracture(s), any bruising, headand neck bruising, other organ injury,cardio-respiratory compromise, andGlasgow Coma Scale score on admis-sion), and operative interventions. Wherestudies included a category of headtrauma of indeterminate etiology, thesecases were excluded. Where studies in-cluded children with injuries that did notmeet our definition of head trauma alongwith thosethatdidmeetourdefinition,weextracted data for eligible children only,and if data could not be extracted for onlythese children, the study was excluded.
Data Analysis
Data were expressed as pooled oddsratios (ORs) with 95% confidenceintervals (CIs). For ORs.1, the variableis associated with AHT and for ORs,1, the variable is associated withnAHT. Data were pooled by usingthe Dersimonian-Laird random effectmethod by using the empirical OR withinverse variance weighting exceptwhen at least 1 cell in a 2 3 2 tablewas 0, in which case 0.5 was added toall the cells in the table before com-puting the empirical OR and variance.Heterogeneity was examined by usingthe I2 statistic. Significance was deter-mined by a P value,.05. Analyses wereconducted by using custom programswritten by using R version 2.10.18
Due to the inconsistency in the specificclinical and radiographic variables re-ported between studies and in themanner of reporting these variablesbetween studies, we limited our meta-analysis to 19 variables.19 These vari-ables were chosen because they wereconsidered clinically relevant, werereported in at least 2 studies, andcould be dichotomized into present and
absent. These variables were subduralhemorrhage(s), epidural hemorrhage(s),subarachnoid hemorrhage(s), retinalhemorrhage(s), skull fracture(s) co-occurring with intracranial injuries, iso-lated skull fracture(s), cerebral ischemia,cerebral edema, diffuse axonal injury,scalp swelling (defined as either soft tis-sue swelling or subgaleal hematoma),metaphyseal fracture(s), long bonefracture(s), rib fracture(s), any bruis-ing, head and neck bruising (distin-guished from other signs of externalhead trauma), apnea at presentation,seizure(s) at presentation or within 24hours of presentation, vomiting, and noadequate history (such as no history oftrauma).
Clinical and radiographic variableswere analyzed in 2 separate groups: (1)all studies that reported a given vari-able and (2) high-quality studies only(rank 1 or 2). Given that the most com-mon age group affected by abuse ischildren ,3 years old, we had a prioriplanned a subgroup analysis by age(children#3 and$3 years of age). Thisanalysis was, however, not possiblegiven the manner in which data werepresented within included studies. Whenpossible, the mean age of children in the2 cohorts was compared. A Wilcoxonsigned rank test tested the hypothesisthat the abused children were youngerthan those not abused, accounting forthe pairing within studies of childrenidentified as abused and not abused. Weexpanded our a priori analysis plan byexamining this hypothesis for studiesthat included only children up to 24 and36 months old, respectively.
During data extraction, it became clearthat studies could be grouped into3 categories by the manner in whichthey reported clinical and radiographiccharacteristics, and this resulted in theneed to expand our a priori analysis planto consider missing data. For example,in reporting retinal hemorrhages,some studies clearly stated that all
TABLE 1 Ranking of Criteria Used to DefineAbuse17
Ranking Criteria Used to Define Abuse
1 Abuse confirmedat case conferenceor civil,family, or criminal court proceedingsor admitted by perpetrator
2 Abuse confirmed by stated criteriaincluding multidisciplinary assessment
3 Diagnosis of abuse defined by statedcriteria
4 Abuse stated as occurring, but nosupporting detail given as to how itwas determined
5 Abuse stated simply as “suspected”; nodetails on whether it was confirmed
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 2, August 2012 317 at Dartmouth College Library on August 6, 2014pediatrics.aappublications.orgDownloaded from

children in each cohort had fundoscopicexams,15,20,21 some studies reportedthis variable for only the subset ofchildren in each cohort who hadfundoscopic exams,10,22–24 while others(mainly retrospective cohort studies)reported the number of retinal hem-morhages as if all children in eachcohort had a fundoscopic exam, but indetailed review, it was clear that thiswas highly unlikely.2,11,24–28 We deter-mined that of the 19 variables reportedin this review, retinal hemorrhages andrib, long bone, and metaphyseal frac-tures were most likely to be affected byinformative missing data,29 and thesevariables required a sensitivity anal-ysis. These variables were chosen asspecific investigations (skeletal surveyor bone scan) or a specialized physicalexam skill (fundoscopic examination)would be needed to rule out thesefindings and that these investigationsand exams were much more likely to becompleted for children in whom abu-sive trauma was suspected. For thesensitivity analysis, we considered allstudies, as well as high-quality studiesalone, and examined (1) those studies inwhich all children had the relevant in-vestigation or examination and (2) thosestudies in which either all children hadthe relevant investigation or examinationdone and/or studies in which the pro-portion of the children having the in-vestigation or examination done wasclearly stated. We chose not to imputemissing values (eg, we did not assumethat unexamined children in the non-abuse cohort had the finding typicallyassociatedwith abuse) given that inmanyof the retrospective studies we could notdetermine how many children had theinvestigation or examination done.
RESULTS
Description of Studies
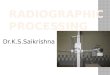
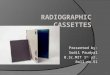
Figure 1 shows the flow of studiesthrough the selection process. Five hun-dred ninety-six studies were identified;
85 were deemed possibly relevant onscreening and full text publicationswere obtained, and of these, 24 met in-clusion criteria (Fig 1).2,8–12,15–21,26–28,30–38
Two included studies37,38 were identifiedby reviewing reference lists of relevantreviews.17 One study2 appeared to reportdata for 40 children that were also in-cluded in a second35 publication; onlyvariables with no overlap were included.Table 2 describes the included studies.Twenty-one studies were deemed highquality (rank 1 or 2), and 3 studiesweredeemed low quality (rank 3, 4, or 5).
Clinical and Radiographic Variables
There was a wide range of clinicalcontent in the included studies with82 variables reported overall. Studiesreported 1 to 35 variables, with a meanof 15 variables. Subdural hemorrhagewas the most commonly reported var-iable, being reported in 15 studies. Thefollowingcharacteristicswerereported inat least 10 studies: retinal hemorrhages,
subarachnoid hemorrhage, epiduralhemorrhage, seizure, and the injurymechanisms of motor vehicle accidents,falls, and admitted/witnessed assault.
Inconsistency in the definition and re-porting of clinical and radiographicvariables as well as high statistical het-erogeneitypresentedchallenges tometa-analysis. For example, subdural hemor-rhage was reported as total, unilateral,bilateral, mixed density, interhemi-spheric, or subdural hemorrhage plusother injuries.2,8–12,15,21–23,25–28,31–35,37,38
Skull fracture was reported as simple,complex, multiple, bilateral, depressed,nonparietal, diastatic fractures .3mm, or fractures crossing suturelines.8,9,11,12,15,22,24–26,28,31–38 By selectingvariables that were clinically relevant,reported in at least 2 studies, and thatcould be dichotomized into present orabsent, we were able to individuallymeta-analyze 19 clinical and radiographicvariables. Table 3 provides a summary ofthe results of the meta-analysis for each
FIGURE 1Study flow.
318 PITEAU et al at Dartmouth College Library on August 6, 2014pediatrics.aappublications.orgDownloaded from

individual characteristic, and Supplemen-tal Information 2 shows forest plots forthese characteristics. The degree ofstatistical heterogeneity variedmarkedlybetween the variables and ranged fromlow to high (Table 3). Of note, a high ORdoes not directly correlate with a highpositive predictive value for a given fea-ture since this depends on the prevalenceof abuse in the individual studies.
Variables Associated With AHT
When examining all studies, subduralhemorrhage(s), cerebral ischemia, cere-bral edema, retinal hemorrhage(s), skullfracture(s) co-occurringwith intracranialinjury,metaphyseal fracture(s), longbonefractures(s), rib fracture(s), any bruising,seizure(s) at or within 24 hours of pre-sentation, apnea at presentation, and noadequate history were individually sig-nificantly associated with AHT (Table 3).Including only high-quality studies, cere-bral edema and any bruising were nolonger significantly associated with AHT.
Variables Associated With nAHT
When examining all studies, epiduralhemorrhage(s), isolated skull fracture(s), scalp swelling, and head and neckbruising were significantly associatedwith nAHT (Table 3). When analysis waslimited to high-quality studies, head andneck bruising was no longer signifi-cantly associated with nAHT.
Variables Not SignificantlyAssociated With AHT or nAHT
When examining all studies and onlyhigh-quality studies, subarachnoid hem-orrhage(s), diffuse axonal injury, andvomitingwerenotsignificantlyassociatedwith AHTor nAHT. Head andneck bruising,any bruising, and cerebral edema werenot significantly associated with AHT ornAHT in only high-quality studies.
Sensitivity Analysis
We performed a sensitivity analysisfor 4 variables: retinal hemorrhages
and long bone, metaphyseal, and ribfractures (Supplemental Information3 and 4). While retinal hemorrhagesremained significantly associated withAHT, long bone and rib fractures didnot, and there were no studies exam-ining metaphyseal fractures to includein the analysis. The small number ofstudies also limited the analyses for riband long bone fractures.
Age
Fourteen studies contributed data tothe age analysis. Seven studies did notreport the mean age of the individualcohorts,12,25,26,30,32,34,36 3 studies repor-ted the mean age for both cohorts butwe extracted data only for childrenmeeting our eligibility criteria and wecould not extract the correspondingage data,11,12,24 and 1 article reportedmean age35 but this overlapped withdata reported in another article.2 In allexcept 1 study,8 the mean age of chil-dren identified as abused was lowerthan the mean age of children identi-fied as not abused (P , .0004). Therange of mean ages reported was 2.1to 22 months in the abuse cohort and5.64 to 43 months in the nonabuse co-hort. Among the abuse cohort, themean age was,12 months in 12 (86%)studies and ,6 months in 6 (43%)studies. Among the nonabuse cohort,the mean age was ,12 months in 7(50%) studies and,6months in 1 (7%)study. When the analysis was re-stricted to the 11 studies that includechildren ,36 months old and to the 6studies that include children ,24months old, the mean age of the chil-dren identified as abused remainedlower than the mean age of childrenidentified as not abused (P = .003 andP = .03, respectively).
DISCUSSION
Principal Findings of the Review
DistinguishingbetweenAHTandnAHTcanbe challenging. Negative consequences
TABLE 2 Characteristics of Included Studies (N = 24)
FirstAuthor
Year ofPublication
Country Age, mo SampleSizea
Type ofStudy
Study QualityRank
Bechtel9 2004 US 0–24 82 Prospective 1 and 2Billmire24 1985 US 0–12 70 Retrospective 1 and 2Datta35 2005 UK 0–24 52 Retrospective 1 and 2Duhaime12 1992 US 0–24 68 Prospective 1 and 2Ettaro25 2004 US 0–36 377 Retrospective 1 and 2Ewing-Cobbs2 1998 US 0–72 40 Prospective 1 and 2Ewing-Cobbs35 2000 US 0–72 60 Prospective 1 and 2Feldman22 2001 US 0–36 54 Prospective 1 and 2Hettler10 2003 US 0–36 163 Retrospective 1 and 2Hobbs36 1984 UK 0–24 89 Retrospective 1 and 2Hoskote37 2002 UK 0–24 16 Retrospective 4Hymel8 2007 US 0–36 41 Prospective 1 and 3Ichord31 2007 US 0–36 52 Prospective 1 and 2Keenan26 2004 US 0–24 152 Prospective 1 or 2Kelly28 2004 New Zealand 0–24 64 Retrospective 4McKinney30 2008 US 0–36 32 Retrospective 1 and 2Myhre32 2007 Norway 0–36 52 Retrospective 2Reece11 2000 US 0–36 179 Retrospective 1 and 2Ruppel38 2001 US 0–72 13 Prospective 5Shugerman27 1996 US 0–36 87 Retrospective 2Tzioumi23 1998 Australia 0–24 36 Retrospective 1 and 2Vavilala33 2007 US 0–60 10 Prospective 1 and 2Vinchon21 2005 France 0–24 150 Prospective 1 and 2Vinchon15 2009 France 0–24 84 Prospective 1
High-quality studies = 1–2; low-quality studies = 3–5 as based on the criteria used to determine the etiology of head injury.a Sample size reported is that of children in each included study that met our definition of head trauma and for whom datarelevant to the review could be extracted. The Duhaime,12 McKinney,32 Reece,11 and Billmire26 studies included children whodid not meet our definition of head trauma and the sample size reported is for only those children that meet our definition.
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 2, August 2012 319 at Dartmouth College Library on August 6, 2014pediatrics.aappublications.orgDownloaded from

including re-injury and death havebeen shown to occur when the di-agnosis has been missed.6 There canalso be negative consequences to thechild and family with an incorrectdiagnosis of abusive injury. For these
reasons, accurate diagnoses mustbe made. From our systematic reviewwe were able to highlight some clin-ical and radiographic characteristicsassociated with AHT and nAHT inchildren.
We found that each of subdural hemor-rhage(s), cerebral ischemia, skull frac-ture(s) in conjunction with intracranialinjury, retinal hemorrhage(s), long bonefracture(s), rib fracture(s), metaphysealfracture(s), seizure(s) at presentation orwithin 24 hours, apnea at presentation,and no adequate history were indi-vidually significantly associated withAHT when only high-quality studieswere meta-analyzed. Epidural hemor-rhage(s), scalp swelling, and isolatedskull fracture(s) were each signifi-cantly associated with nAHT whenhigh-quality studiesweremeta-analyzed.Although we recognize that patternsof injuries are of key importance inmaking a diagnosis of abuse ornonabuse, limitations in the data,as well as the manner in which itwas presented, prevented us fromexamining whether variables wereassociated with abusewhen found incombination.
Comparison With Other Studies
In 1962, Kempe described “batteredchild syndrome” as the combination ofsubdural hemorrhage, skeletal inju-ries, and bruises.39 Since then, manystudies have supported the associationof subdural hemorrhage with childabuse,6,40,41 the association of epiduralhemorrhage with nAHT, and the asso-ciation of subarachnoid hemorrhagewith both mechanisms of injury.2,27,35
Our study provides evidence that ayounger age is associated with AHT,and this may support the hypothesizedtemporal association between AHT andcrying patterns in infants within thefirst 3 months of life.42 This finding mayalso reflect the physiologic and anatomicdifferences in younger children that mayalter the susceptibility to head injurywith a given mechanism or force.43–45
Maguire et al13 recently published asystematic review addressing a similarquestion as our review. Similar to ourstudy, they found that apnea, retinal
TABLE 3 Clinical and Radiographic Characteristics Associated With ABT and nABT
Characteristic No. ofStudies
OR (95% CI); OR .1Favors Abuse; OR ,1Favors Nonabuse
I2, % P
Subdural hemorrhage(s)All studies 15 8.92 (6.77–11.74) 0 ,.001High-quality studies 14 8.90 (6.75–11.73) 0 ,.001
Epidural hemorrhage(s)All studies 10 0.15 (0.08–0.29) 0 ,.001High-quality studies 9 0.13 (0.06–0.26) 0 ,.001
Subarachnoid hemorrhage(s)All studies 13 1.42 (0.67–3.0) 76 .36High-quality studies 11 1.31 (0.58–3.0) 80 .52
Cerebral edemaAll studies 9 2.17 (1.06–4.45) 54 .03High-quality studies 7 2.05 (0.82–5.10) 65 .12
Cerebral ischemiaHigh-quality studies 4 4.79 (1.84–2.46) 29 .001
Diffuse axonal injuryAll studies 6 1.47 (0.26–8.32) 61 .66High-quality studies 4 0.83 (0.06–2.46) 72 .89
Skull fracture(s) + intracranial injuryHigh-quality studies 4 7.76 (1.06–57.08) 88 .04
Isolated skull fracture(s)High-quality studies 2 0.01 (0.003–0.04) 0 ,.001
Long bone fracture(s)All studies 8 4.234 (2.50–7.19) 0 ,.001High-quality studies 6 4.344 (2.52–7.49) 0 ,.001
Metaphyseal fracture(s)All studies 2 11.76 (2.18–63.41) 0 .004High-quality studies 1 1 5.06 (1.93–117.72) Single estimate ,.001
Rib fracture(s)All studies 7 8.89 (4.04–7.19) 1 ,.001High-quality studies 6 9.84 (4.42–21.90) 0 ,.001
Retinal hemorrhage(s)All studies 14 27.12 (15.70–46.84) 24 ,.001High-quality studies 12 28.24 (15.37–51.90) 35 ,.001
Any bruisingAll studies 5 4.77 (1.62–14.05) 15 .005High-quality studies 3 5.35 (0.91–31.41) 0 .06
Head and neck bruisingAll studies 3 0.42 (0.19–0.94) 26 .03High-quality 2 0.65 (0.27–1.57) 0 .34
Scalp swellingHigh-quality studies 7 0.12 (0.05–0.32) 65 ,.001
ApneaAll studies 4 5.31 (2.34–12.05) 0 ,.001High-quality studies 3 4.89 (2.08–11.49) 0 ,.001
Seizure(s)All studies 10 7.25 (3.04–17.27) 77 ,.001High-quality studies 9 11.24 (7.30–17.29) 0 ,.001
VomitingHigh-quality studies 3 0.89 (0.02–4.88) 83 .89
No adequate historyAll studies 9 46.94 (12.91–170.63) 69 ,.001High-quality studies 8 52.72 (12.79–217.33) 72 ,.001
320 PITEAU et al at Dartmouth College Library on August 6, 2014pediatrics.aappublications.orgDownloaded from

hemorrhage, rib fractures, long bonefractures, skull fractures associatedwith intracranial injury, and seizureswere associated with abuse.13 The re-view also found head and neck bruis-ing was associated with nAHT. Someimportant differences exist, however,between these 2 reviews, includingthe definition of head trauma, articlesincluded, characteristics analyzed, stati-stical methodology, and data represen-tation. Specifically, our review includedexamination of historical features andthe type of intracranial injury. We believethat the type of intracranial injury asso-ciated with injury mechanism is critical,as these may be the initial data availableto front-line clinicians who must makea preliminary determination around in-jury mechanism. We included only stud-ies of admitted patients to focus onmoreseriously injured patients, andwe limitedour study population to a younger age tofocus on the primary age group at riskfor AHT. We included more studies in oursystematic review, although 3 studies inMaguire et al’s 2009 review did not meetour inclusion criteria. We also chose toexamine statistical heterogeneity be-tween studies and to examine all studies,as well as only high-quality studies, toaddress the robustness of our data.Interestingly, when low-quality studieswere excluded from analysis, only 3variables were no longer significantlyassociated with either AHT or nAHTsuggesting our conclusions are fairlyrobust. We dealt with informativemissing data in a different manner. TheMaguire et al 2009 review imputed in-formative missing data when onlya proportion of the children in eachcohort had the investigations. Wechose not to use this approach for oursensitivity analysis since we could notdetermine the proportion of children ineach cohort that had the given in-vestigation or exam performed. Thesmall number of studies accuratelyreporting missing data limited oursensitivity analysis.
Two other reviews of characteristicsassociated with AHT and nAHT havebeen recently published. One, by Kempet al, reviewed neuroradiologic fea-tures in 21 studies of children hospi-talized with head trauma. This study’sfinding that subdural hemorrhage andhypoxic ischemic injury were signifi-cantly associated with AHT46 was inagreement with our results. The authorsalso found that cerebral edema wasassociated with AHT. The second study,a patient-level meta-analysis from 6 co-hort studies, examined the positive pre-dictive values of a combination of 6clinical features (head and neck bruis-ing, rib fracture, skull fractures, longbone fractures, retinal hemorrhage,seizures, and apnea) in conjunctionwithintracranial injury.47 It reported that anycombination of $3 features yieldeda positive predictive value for AHT of85%. Given the limitations of the articlesincluded in our review, an analysis ofcombined features was not possible inour study.
Limitations of the Review
The meta-analysis for this review wasmade difficult by inconsistencies in thecriteria used to determine the etiologyfor head trauma, inconsistencies indefining and reporting clinical and ra-diographic variables, andamoderate tohigh degree of statistical heterogeneitybetween studies. As there are no stan-dardized criteria for the definition ofabuse, most authors developed theirown criteria, and many of these arefraught with circular reasoning. The di-agnosis of AHT relies on historical fea-tures, clinical findings, and radiologicinterpretations, and it is these samecriteria that are used to categorize headtrauma as abusive or nonabusive. Weattempted to address this limitation byusing a published scale to rank thequality of the criteria used for defin-ing abuse7,13,16,17 and examined our re-sults for all eligible studies, as well asfor those using high-quality criteria.
However, for features that have beentraditionally associatedwith abuse (suchas subdural hemorrhage and retinalhemorrhage), this ranking scale doesnot compensate well for circularity andthus our results must be interpretedcautiously.
Significant variability in the definitionand description of clinical and radio-graphic variables in the includedstudies made meta-analysis difficult.This variability highlights the need forthe standardization of definitions anddescriptions of characteristics to ac-curately compare data between stud-ies or combine data for meta-analysis.Ultimately, such standardization couldadvance the development of accuratediagnostic criteria for AHT. The highdegree of heterogeneity among stud-ies may reflect this lack of standard-ization, somewhat weakening theclinical interpretability of the reviewfindings.
All studies included in this reviewwere,as expected, observational studies. Se-lection, informational, and confoundingbias are limitations to these studies. Theretrospective studies were limited withrespect to reporting missing data. Manystudies reported data around charac-teristics (eg, retinal hemorrhages) as ifall children in both cohorts had un-dergone the necessary investigation orexamination (eg, fundoscopy) to lookfor the characteristic in question; how-ever, a detailed review of the datarevealed this to be unlikely. While weperformed a sensitivity analysis toexamine this issue, our results need tobe interpreted cautiously. The retro-spective studies in this review werealso limited by recall bias; for exam-ple, the low-quality studies relied onmedical record coding for the diag-nosis of abuse, without reviewing sup-porting detail as to how abuse wasdetermined. By limiting the review tostudies of admitted children, onlyserious head injurieswouldhavebeen
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 2, August 2012 321 at Dartmouth College Library on August 6, 2014pediatrics.aappublications.orgDownloaded from

included, but children who died be-fore presentation would have beenexcluded. As well, children with lesssevere abusive injuries may be lesslikely to be brought to the hospitalafter an abusive event. Thus, a se-lection bias may occur for chil-dren with more severe injuries andsymptoms in the abusive cohortbeing brought to the hospital com-pared with those in the nonabusivecohort.
CONCLUSIONS
Clinical and radiographic variables as-sociated with AHT and nAHT in childrenwere identified, despite important limi-tations in the existing literature. Thissystematic review highlights the need forconsistent criteria in identifying andreporting the historical, physical, andradiographic variables associated withabusive and nonabusive head injuries. Afuture multicenter prospective trial eval-uating AHT and nAHT by using standard
criteria for both the categorization ofetiology and for the examination andreporting of characteristics of headtrauma would allow for more definitivefindings.
ACKNOWLEDGMENTSThe authors gratefully acknowledge thefollowing individuals for their contribu-tions to this project: Margaret Sampson,MLIS, PhD, AHIP (search services), andErin Crouchman, MSc (article retrieval).
REFERENCES
1. Duhaime AC, Christian CW, Rorke LR, et al.Nonaccidental head trauma in infants—the“shaken baby syndrome.”. N Engl J Med.1999;338:1822–1829
2. Ewing-Cobbs L, Kramer L, Prasad M, et al.Neuroimaging, physical, and developmentalfindings after inflicted and noninflictedtraumatic brain injury in young children.Pediatrics. 1998;102(2 pt 1):300–307
3. Barlow KM, Minns RA. Annual incidence ofshaken impact syndrome in young chil-dren. Lancet. 2000;356(9241):1571–1572
4. Minns RA, Jones PA, Mok JY. Incidence anddemography of non-accidental head injuryin southeast Scotland from a national da-tabase. Am J Prev Med. 2008;34(suppl 4):S126–S133
5. Keenan HT, Runyan DK, Marshall SW, NoceraMA, Merten DF, Sinal SH. A population-based study of inflicted traumatic braininjury in young children. JAMA. 2003;290(5):621–626
6. Jenny C, Hymel KP, Ritzen A, Reinert SE, HayTC. Analysis of missed cases of abusivehead trauma. JAMA. 1999;281(7):621–626
7. Kemp AM, Dunstan F, Harrison S, et al.Patterns of skeletal fractures in childabuse: a systematic review. BMJ. 2008;337:a1518
8. Hymel KP, Makoroff KL, Laskey AL, ConawayMR, Blackman JA. Mechanisms, clinical pre-sentations, injuries, and outcomes frominflicted versus noninflicted head traumaduring infancy: results of a prospective,multicentered, comparative study. Pediat-rics. 2007;119(5):922–929
9. Bechtel K, Stoessel K, Leventhal JM, et al.Characteristics that distinguish accidentalfrom abusive injury in hospitalized youngchildren with head trauma. Pediatrics. 2004;114(1):165–168
10. Hettler J, Greenes DS. Can the initial historypredict whether a child with a head in-jury has been abused? Pediatrics. 2003;111(3):602–607
11. Reece RM, Sege R. Childhood head injuries:accidental or inflicted? Arch Pediatr Ado-lesc Med. 2000;154(1):11–15
12. Duhaime AC, Alario AJ, Lewander WJ, et al.Head injury in very young children: mech-anisms, injury types, and ophthalmologicfindings in 100 hospitalized patients youn-ger than 2 years of age. Pediatrics. 1992;90(2 pt 1):179–185
13. Maguire S, Pickerd N, Farewell D, Mann M,Tempest V, Kemp AM. Which clinical featuresdistinguish inflicted from non-inflicted braininjury? A systematic review. Arch Dis Child.2009;94(11):860–867
14. Geddes JF, Hackshaw AK, Vowles GH, NickolsCD, Whitwell HL. Neuropathology of inflictedhead injury in children. I. Patterns of braindamage. Brain. 2001;124(pt 7):1290–1298
15. Vinchon M, de Foort-Dhellemmes S, DesurmontM, Delestret I. Confessed abuse versus wit-nessed accidents in infants: comparison ofclinical, radiological, and ophthalmologicaldata in corroborated cases. Childs NervSyst. 2010;26(5):637–645
16. Maguire S, Moynihan S, Mann M, Potokar T,Kemp AM. A systematic review of the fea-tures that indicate intentional scalds inchildren. Burns. 2008;34(8):1072–1081
17. Maguire S, Mann MK, Sibert J, Kemp A. Arethere patterns of bruising in childhood whichare diagnostic or suggestive of abuse? Asystematic review. Arch Dis Child. 2005;90(2):182–186
18. R Development Core Team. R: A Languageand Environment for Statistical Computing.Vienna, Austria: R Foundation for StatisticalComputing; 2009
19. Higgins JP, Thompson SG, Deeks JJ, AltmanDG. Measuring inconsistency in meta-analyses.BMJ. 2003;327(7414):557–560
20. Bechtel K, Berger R. Inflicted traumaticbrain injury: making the diagnosis in theemergency department. Clin Pediatr EmergMed. 2006;7:138–142
21. Vinchon M, Defoort-Dhellemmes S, DesurmontM, Dhellemmes P. Accidental and nonacci-dental head injuries in infants: a prospec-tive study. J Neurosurg. 2005;102(suppl 4):380–384
22. Feldman KW, Bethel R, Shugerman RP,Grossman DC, Grady MS, Ellenbogen RG.The cause of infant and toddler subduralhemorrhage: a prospective study. Pediat-rics. 2001;108(3):636–646
23. Tzioumi D, Oates RK. Subdural hematomasin children under 2 years. Accidental or in-flicted? A 10-year experience. Child AbuseNegl. 1998;22(11):1105–1112
24. Billmire ME, Myers PA. Serious head injuryin infants: accident or abuse? Pediatrics.1985;75(2):340–342
25. Ettaro L, Berger RP, Songer T. Abusive headtrauma in young children: characteristics andmedical charges in a hospitalized population.Child Abuse Negl. 2004;28(10):1099–1111
26. Keenan HT, Runyan DK, Marshall SW, NoceraMA, Merten DF. A population-based com-parison of clinical and outcome charac-teristics of young children with seriousinflicted and noninflicted traumatic braininjury. Pediatrics. 2004;114(3):633–639
27. Shugerman RP, Paez A, Grossman DC, Feld-man KW, Grady MS. Epidural hemorrhage: isit abuse? Pediatrics. 1996;97(5):664–668
28. Kelly P, Hayes I. Infantile subdural haema-toma in Auckland, New Zealand: 1988-1998.N Z Med J. 2004;117(1201):U1047
322 PITEAU et al at Dartmouth College Library on August 6, 2014pediatrics.aappublications.orgDownloaded from

29. Little J, Rubin D. Statistical Analysis withMissing Data. 2nd ed. NJ: Wiley and Sons,Inc; 2002
30. McKinney AM, Thompson LR, Truwit CL,Velders S, Karagulle A, Kiragu A. Unilateralhypoxic-ischemic injury in young chil-dren from abusive head trauma, lackingcraniocervical vascular dissection orcord injury. Pediatr Radiol. 2008;38(2):164–174
31. Ichord RN, Naim M, Pollock AN, Nance ML,Margulies SS, Christian CW. Hypoxic-ischemic injury complicates inflicted andaccidental traumatic brain injury in youngchildren: the role of diffusion-weightedimaging. J Neurotrauma. 2007;24(1):106–118
32. Myhre MC, Grøgaard JB, Dyb GA, Sandvik L,Nordhov M. Traumatic head injury in in-fants and toddlers. Acta Paediatr. 2007;96(8):1159–1163
33. Vavilala MS, Muangman S, Waitayawinyu P,et al. Neurointensive care; impaired cere-bral autoregulation in infants and youngchildren early after inflicted traumatic braininjury: a preliminary report. J Neurotrauma.2007;24(1):87–96
34. Datta S, Stoodley N, Jayawant S, RenowdenS, Kemp A. Neuroradiological aspects of
subdural haemorrhages. Arch Dis Child.2005;90(9):947–951
35. Ewing-Cobbs L, Prasad M, Kramer L, et al.Acute neuroradiologic findings in youngchildren with inflicted or noninflicted trau-matic brain injury. Childs Nerv Syst. 2000;16(1):25–33, discussion 34
36. Hobbs CJ. Skull fracture and the diagnosisof abuse. Arch Dis Child. 1984;59(3):246–252
37. Hoskote A, Richards P, Anslow P, McShane T.Subdural haematoma and non-accidentalhead injury in children. Childs Nerv Syst.2002;18(6-7):311–317
38. Ruppel RA, Kochanek PM, Adelson PD, et al.Excitatory amino acid concentrations inventricular cerebrospinal fluid after severetraumatic brain injury in infants and chil-dren: the role of child abuse. J Pediatr.2001;138(1):18–25
39. Kempe CH, Silverman FN, Steele BF,Droegemueller W, Silver HK. The battered-child syndrome. JAMA. 1962;181:17–24
40. Caffey J. The whiplash shaken infant syn-drome: manual shaking by the extremitieswith whiplash-induced intracranial and in-traocular bleedings, linked with residualpermanent brain damage and mental re-tardation. Pediatrics. 1974;54(4):396–403
41. Guthkelch AN. Infantile subdural haematomaand its relationship to whiplash injuries.BMJ. 1971;2(5759):430–431
42. Barr RG, Trent RB, Cross J. Age-related in-cidence curve of hospitalized Shaken BabySyndrome cases: convergent evidence forcrying as a trigger to shaking. Child AbuseNegl. 2006;30(1):7–16
43. Bylski DI, Kriewall TJ, Akkas N, Melvin JW.Mechanical behavior of fetal dura materunder large deformation biaxial tension.J Biomech. 1986;19(1):19–26
44. Kriewall TJ, Akkas N, Bylski DI, Melvin JW,Work BA Jr. Mechanical behavior of fetaldura mater under large axisymmetric in-flation. J Biomech Eng. 1983;105(1):71–76
45. Galford JE, McElhaney JH. A viscoelasticstudy of scalp, brain, and dura. J Biomech.1970;3(2):211–221
46. Kemp AM, Jaspan T, Griffiths J, et al. Neu-roimaging: what neuroradiological featuresdistinguish abusive from non-abusive headtrauma? A systematic review. Arch Dis Child.2011;96(12):1103–1112
47. Maguire SA, Kemp AM, Lumb RC, FarewellDM. Estimating the probability of abusivehead trauma: a pooled analysis. Pediatrics.2011;128(3). Available at: www.pediatrics.org/cgi/content/full/128/3/e550
FEEDING FRENZY: We often think of the ecosystem from the bottom up: single-celled organisms capture energy from the sun and are at the bottom of the foodchain. Larger animals feed on smaller ones culminating with the top predatorthat is preyed upon by no other species. We all know that if the algae were to die,the entire food chain would collapse. However, what happens if the predators, orthose near the top of the food chain, disappear? Now, more data suggest thecritical role that top predators play in managing food chains and ecosystems. Asreported in The New York Times (Environment: June 12, 2012), salt marshesacross Cape Cod are disintegrating. The reason for their destruction is that theSesarma crab population has exploded. Juvenile and adult crabs are eaten bymany different animals, but the key predators of the inch-long Sesarma crab areblue crabs, striped bass, and cod. The problem is that in areaswhere there is a lotof recreational fishing and shellfishing, the populations of these predators havebeen decimated. With fewer predators, the Sesarma crab population has in-creased dramatically. As the Sesarma crabs eat marsh grasses, vast areas ofthe salt marshes have become denuded of grass that is essential for the de-velopment of fish nurseries, filtering water, and prevention of erosion. Hence, theloss of the marsh grass has many detrimental effects. All ecosystems requirebalance. Removing either the foundation or the top predator from a food chainhas profound untoward effects. At least there is something we can do for the saltmarshes in Cape Cod: release any fish caught in these areas.
Noted by WVR, MD
REVIEW ARTICLE
PEDIATRICS Volume 130, Number 2, August 2012 323 at Dartmouth College Library on August 6, 2014pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2011-1545; originally published online July 9, 2012; 2012;130;315Pediatrics
Shalea J. Piteau, Michelle G.K. Ward, Nick J. Barrowman and Amy C. PlintNonabusive Head Trauma: A Systematic Review
Clinical and Radiographic Characteristics Associated With Abusive and
ServicesUpdated Information &
mlhttp://pediatrics.aappublications.org/content/130/2/315.full.htincluding high resolution figures, can be found at:
Supplementary Material
3/peds.2011-1545.DCSupplemental.htmlhttp://pediatrics.aappublications.org/content/suppl/2012/07/0Supplementary material can be found at:
References
ml#ref-list-1http://pediatrics.aappublications.org/content/130/2/315.full.htat:This article cites 44 articles, 19 of which can be accessed free
Citations
ml#related-urlshttp://pediatrics.aappublications.org/content/130/2/315.full.htThis article has been cited by 3 HighWire-hosted articles:
Rs)3Peer Reviews (PPost-Publication
http://pediatrics.aappublications.org/cgi/eletters/130/2/315
R has been posted to this article: 3One P
Subspecialty Collections
e_neglect_subhttp://pediatrics.aappublications.org/cgi/collection/child_abusChild Abuse and Neglectthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2012 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Dartmouth College Library on August 6, 2014pediatrics.aappublications.orgDownloaded from