Embed Size (px)
Citation preview

Early Human Development, 1978, 2/1,73-80 o Elsevier/North-Holland Biomedical Press
73
Clinical assessment of gestational age at birth: the effects of sex, birthweight, and weight for length of gestation*
M.K. OUNSTED' , CA. CHALMERS’ and P.L. YUDKIN’
Departments of ’ Paediatrics and z Obstetrics of the University of Oxford, John Radcliffe Hospital, Headington, Oxford, United Kingdom
Accepted for publication 13 December 1977
SUMMARY
During studies on different aspects of fetal growth rate infants who were small-for-dates (SFD) large-for-dates (LFD) or within the normal range of birthweight for length of gestation (AFD) were examined within 48 h of birth. Gestational age was clinically assessed by the Dubowitz method.
Among 140 AFD infants boys had higher mean values than girls for total and external scores, but there was no difference in neurological scores. Multiple regression of the score for external criteria on gestation, bithweight and sex, showed a significant contribution for birthweight and sex in addi- tion to gestation; whereas gestation was the only significant explanatory variable in the regression of the score for neurological criteria.
When infants in the three weight groups were matched for length of gestation and sex, the SFD group had significantly lower mean total and ex- ternal scores than the AFD group. The mean scores for the LFD group were not significantly higher than the AFD group. The neurological scores did not differ in the three groups.
Maturation of external characteristics is related to weight as well as ge- station. When assessment is made after birth by a clinical examination which includes these characteristics, the length of gestation of some SFD infants will be underestimated. The sex of the infant should also be borne in mind.
neonate; small-for-dates; large-for-dates; gestational age assessment; external criteria; neurological criteria
INTRODUCTION
During the past 10 years many methods have been produced to evaluate by clinical means the gestational age of infants at birth. Two sets of criteria are
*This work is supported by a Medical Research Council grant.
74
commonly used comprising items related to external (superficial) and neuro- logical features. Some workers favour assessments using external criteria [ 10, 11,161. while others use neurological characteristics alone [1,3,5,6,17].
In 1970 Dubowitz et al. [8] published their method of assessment which incorporates both external and neurological characteristics. Twenty-one dif- ferent observations are made on each infant. A score is given for each item, the total score is set against a graph, and the gestational age estimated. This scoring system has now been widely used in many countries. Indeed in South Africa, because of the lack of sophistication in the population and the un- reliability of information regarding the last menstrual period, this estimate of the length of gestation is the one used when plotting individual infants on birthweight-for-gestation charts [ 191.
There is a suggestion that maturation of some external features may be influenced by birthweight, [ 121. Thus assessment made on these criteria alone would underestimate the gestational age of small-for-dates neonates. From 36 wk gestation onwards boys are heavier than girls [4] , and their gestational age might be overestimated by this clinical assessment. It there- fore seemed important to explore these relationships in greater depth.
PATIENTS AND METHODS
During the course of studies on factors associated with slow and fast fetal growth rate and their outcome, small-fordates (SFD) and large-for-dates (LFD) infants were identified at birth. The criteria for selection were that their birthweights should be 2 standard deviations (SD) or more below and above the mean respectively for length of gestation and sex [4]. Mother-- infant pairs in the beds adjacent to SFD and LFD probands were invited to join the study as a random sample of the hospital population. The .birth- weights of these infants were all within 2 SD of the mean for length of gestation and sex (AFD).
The mothers were all interviewed personally and their infants examined by members of a small research team who periodically checked their metho- dology to minimize inter-observer bias. All the patients in this study were sure of the date of their last menstrual period (LMP). They had a regular cycle of 26--31 days, and had had at least one normal period since with- drawal from the pill. Their uterine size was reported as equivalent to their dates at an examination before 16 wk gestation. Clinical assessment of gestational age according to the Dubowitz method was made on all infants within 48 h of birth.
There were 140 infants in the AFD series, 76 male and 64 female. The total, external and neurological Dubowitz scores of the males and females were compared. Multiple regression analyses were made of the total Dubo- witz score on birthweight, gestation and sex. These were repeated for the external and neurological scores, separately.
75
93 SFD, AFD and LFD infants (53 male and 40 female) were then matched for length of gestation and sex. Analyses were made by paired t-tests on the total Dubowitz scores, and the scores for external and neurological charac- teristics separately. The total, external and neurological scores for boys and girls within the SFD and LFD groups were also compared.
RESULTS
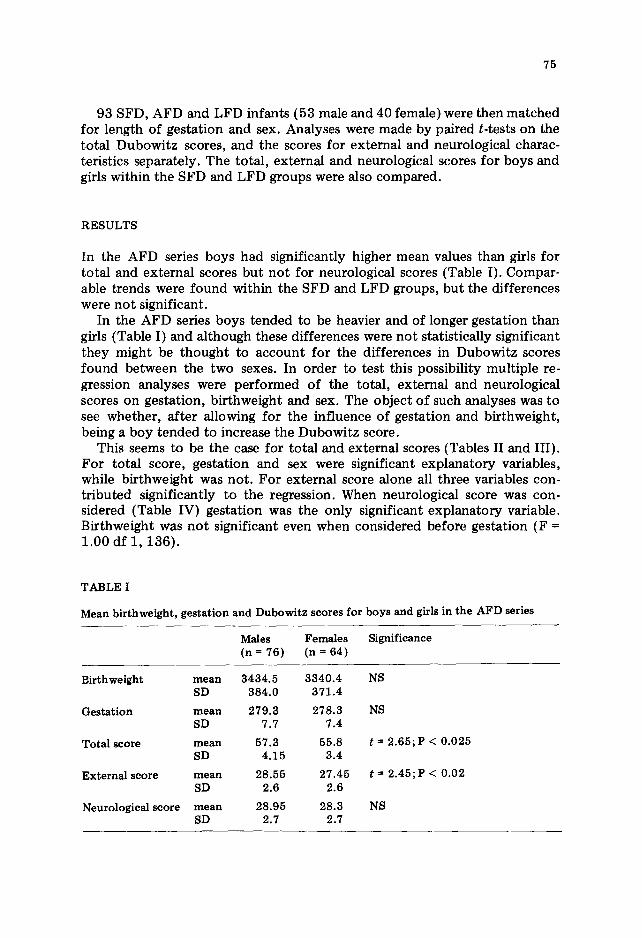
In the AFD series boys had significantly higher mean values than girls for total and external scores but not for neurological scores (Table I). Compar- able trends were found within the SFD and LFD groups, but the differences were not significant.
In the AFD series boys tended to be heavier and of longer gestation than girls (Table I) and although these differences were not statistically significant they might be thought to account for the differences in Dubowitz scores found between the two sexes. In order to test this possibility multiple re- gression analyses were performed of the total, external and neurological scores on gestation, birthweight and sex. The object of such analyses was to see whether, after allowing for the influence of gestation and birthweight, being a boy tended to increase the Dubowitz score.
This seems to be the case for total and external scores (Tables II and III). For total score, gestation and sex were significant explanatory variables, while birthweight was not. For external score alone all three variables con- tributed significantly to the regression. When neurological score was con- sidered (Table IV) gestation was the only significant explanatory variable. Birthweight was not significant even when considered before gestation (F = 1.00 df 1, 136).
TABLE I
Mean birthweight, gestation and Dubowitz scores for boys and girls in the AFD series
Males Females Significance (n = 76) (n = 64)
Birthweight mean 3434.5 3340.4 NS SD 334.0 371.4
Gestation mean 279.3 278.3 NS SD 7.7 7.4
Total score mean 57.3 55.8 f = 2.65; P < 0.025 SD 4.15 3.4
External score mean 28.55 27.45 t = 2.45;P < 0.02 SD 2.6 2.6
Neurological score mean 28.95 28.3 NS SD 2.7 2.7

76
TABLE II
Multiple regression of total score on gestation, birthweight and sex (AFD series only)
Source ss
Total 2113.61 Regression 823.65 Residual 1289.95
Gestation 746.41 Birthweight
after gestation 15.63
Sex after birthweight and gestation 61.58
MS df F P
15.21 139 274.55 3 28.95 -Co.001
9.49 136
1 78.69 <O.OOl
1 1.65 NS
1 6.49 -CO.025
-
r2 = 0.390
By criterion there were large weight differences between the SFD, AFD and LFD groups (Table V). Although there were a few preterm babies in each of the original series it was not possible to match them for gestational age and so they were excluded. Length of gestation in the matched groups ranged from 259 to 295 days.
The SFD group had significantly lower mean total and external scores compared with the AFD group (Table VI). The comparable values for LFD babies were marginally higher than AFD babies but the differences were not significant. The SD for total and external scores was the same in the AFD and LFD groups, but in the SFD group it was larger, showing greater variabi- lity. The mean values and SDS for neurological scores did not differ in the three groups.
TABLE III
Multiple regression of external score on gestation, birthweight and sex (AFD series only)
Source ss MS df D P
Total 977.11 7.03 139 Regression 296.37 98.79 3 19.74 < 0.001 Residual 680.74 5.01 136
Gestation 240.29 1 47.96 <O.OOl Birthweight
after gestation 33.28 1 6.64 <0.025
Sex after birthweight and gestation 22.80 1 4.55 -Co.05
r-2 = 0.303

77
TABLE IV
Multiple regression of neurological score on gestation, birthweight and sex (AFD series only)
Source ss MS df F P
Total 1015.22 7.30 139 Regression 152.27 50.76 3 8.00 <O.OOl Residual 862.95 6.35 136
Gestation 138.26 1 21.79 <O.OOl Birthweight
after gestation 3.78 1 0.60 NS
Sex after birthweight and gestation 10.23 1 1.61 NS
rz = 0.150
TABLE V
Birthweight and length of gestation in the three groups (n = 93 in each group)
SFD AFD LFD -
Birthweight mean 2251.4 3375.85 4508.6 (g) SD 263.1 451.4 207.4
Gestation mean 277.1 277.1 277.2 (days) SD 7.0 7.0 6.9
TABLE VI
Dubowitz scores in the three groups (n = 93 in each group)
SFD AFD LFD
Total score mean 53.9* 56.3 56.5 SD 5.0 3.8 3.8
External score
mean SD
26.5** 27.9 28.4 3.8 2.6 2.35
Neurological mean 27.85 28.4 28.1 score SD 2.45 2.6 2.4
*Significantly lower than AFD; t = 3.96; P <O.OOl. **Significantly lower than AFD; t = 4.2O;P <O.OOl.
78
DISCUSSION
Our findings on a large group of babies whose birthweights were within 2 SD of the mean for length of gestation clearly show that when external factors alone are considered the maturational score is influenced by weight inde- pendently of gestation. SFD neonates had a lower external score than AFD neonates of the same gestational age. This again suggests an association between the maturation of at least some of these characteristics and weight gain. Thus the gestational age of SFD babies would be underestimated when calculated according to a clinical examination which relied on external characteristics.
As is so often found when extreme groups are ascertained by a statistical criterion, the LFD infants did not show a mirror-image effect [ 151; although there was a general tendency for higher external scores in this group. Finn- strijm [14] compared the external scores of SFD, AFD and LFD infants. His total numbers were small, and the criterion for SFD infants (more than 2 SD below the mean) was more extreme than that for LFD infants (above the 90th centile). But again, the difference between the scores for SFD and AFD in- fants was great, whereas that for LFD infants was almost identical with AFD infants.
The influence of sex on external score in the AFD group appeared to be independent of birthweight and gestation. Parkin et al. [16] found no systematic differences between males and females when data on individual items in their assessment were analysed. However, Finnstrom [14] noted pronounced differences between male and female scores for external geni- talia. Although non-comparability in scoring this item for boys and girls may contribute towards our finding, it is unlikely to be the only feature in- volved since the maximum score for either sex is only 2.
Neurological score in the AFD series was associated with gestation, but not with birthweight or sex. Moreover, no differences were found between the neurological scores for SFD, AFD and LFD groups. It thus appears that unlike external criteria, maturation of the neurological characteristics ex- amined here is unaffected by the size of the baby or his sex. Schulte et al. 1181 demonstrated consistent abnormal motor behaviour in SFD neonates, and considered that examination by their technique was unsuitable for gestational age assessment. The babies in their study were all born to tox- aemic mothers; and many of the items used were not included in the Dubo- witz assessment. The same may be said of Finnstram’s neurological examina- tion [ 131 which seemed to be aimed at demonstrating differences in neuro- logical status rather than maturational features as such. SFD infants, by his assessment, had lower mean scores than AFD infants. On the other hand Dubowitz et al. [9] have observed that neurological criteria of gestational age tend to be influenced in the other direction (from external criteria) in SFD infants, suggesting advanced neurological maturation.
The infants in our study were all of gestational ages over 37 wk. Matura- tion of external and neurological characteristics during the third trimester

79
may not progress at a steady pace. Our findings cannot necessarily be extra- polated to earlier periods of gestation. When a baby is sick and in an in- cubator assessment by neurological means may be difficult. Even if the ex- amination is practicable, hypotonia associated with the infant’s immediate condition may result in a lower score. Nevertheless, it is clear from our data that the effect of weight on the external score is considerable; and even when both external and neurological characteristics are taken into account, the total score will give a biased estimate of gestational age in SFD infants.
Assessment ,of gestational age by means of nerve conduction velocity [2,7] may give a more accurate estimate in sick and SFD infants. But this method is impracticable for universal use. Among clinical techniques it is unlikely that much improvement can be made on the Dubowitz assessment. In experienced hands it takes very little time, and reduction of the number of items is unnecessary.
Rate of maturation is a biological variable which, like somatic growth, is not uniform. Fetuses, like children, would not be expected to mature all at the same rate. The standard deviation of neonatal maturity (which will vary according to the organs or system involved), has not been precisely defined. But it is unlikely to be much smaller than the confidence limits of the op- timal methods of assessment now available. If this is so, even the most sensitive techniques will not equate maturity with gestational age in every patient, 5% of whom would be at least 2 wk more or less ‘mature’ than their chronological age. Our data suggest that when gestational age is calculated from a score based on a clinical examination which includes external cha- racteristics, a girl of low birthweight will often appear to be less mature than expected for her length of gestation.
ACKNOWLEDGEMENTS
We are grateful to the other members of MKO’s research team for clinical assistance.
REFERENCES
1 Amiel-Tison, C. (1968): Neurological examination of the maturity of newborn in- fants. Arch. Dis. Child., 43,39.
2 Blom, S. and Finnstrom, 0. (1971): Studies on maturity in newborn infants. V Motor conduction velocity. Neuropiidiatrie, 3, 129-139.
3 Brett, E.M. (1965): The estimation of fetal maturity by the neurological examina- tion of the neonate. In: Gestational Age, Size and Maturity. Editors: M. Dawkins and B. MacGregor. Clinics in Developmental Medicine, N. 19, Spastics Society with Heinemann, London.
4 Butler, N.R. and Alberman, E.D. (1969): Perinatal Problems. E. and S. Livingstone, Edinburgh, London.
5 Dargassies, Sainte-Anne S. (1955): La maturation neurologique des prematures. Etud. Neo-Natales, 4, 71.

6 Dargassies, Sainte-Anne S. (1962): Le nouveau ne B terme: aspecte neurologique. Biol. Neonat., 4, 174.
7 Dubowitz, V., Whittaker, G.F., Brown, B.H. and Robinson, A. (i968): Nerve con- duction velocity. An index of neurological maturity of the newborn infant. Dev. Med. Child Neurol., 10, 741-749.
8 Dubowitz, L.M.S., Dubowitz, V. and Goldberg, C. (1970): Clinical assessment of gestational age in the newborn infant. J. Pediatr., 77.1.
9 Dubowitz, L.M.S., Dubowitz, V., Goldberg, C. and Keith, I. (1976): Rapid assess- ment of gestational age at birth. Arch. Dis. Child., 51, 12,986-987.
10 Farr, V., Mitchell, R.G., Neligan, G.A. and Parkin, J.M. (1966a): Dev. Med. Child Neurol., 8,5,507-511.
11 Farr, V., Kerridge, D.F. and Mitchell, R.G. (1966b): Dev. Med. Child Neurol., 8, 657-660.
12 Farr, V. and Mitchell, R.G. (1967): The effect of birthweight on maturity scoring. Dev. Med. Child Neurol., 9, 745-748.
13 Finnstrom, 0. (1971): Studies on maturity in newborn infants, iii Neurological examination. Neuropldiatrie, 3, 72-96.
14 Finnstrom, 0. (1972): Studies on maturity in newborn infants. ii External characte- ristics. Acta Paediatr. Stand., 61, 24-32.
15 Ounsted, M. and C. (1973): On Fetal Growth Rate. Clinics in Developmental Medi- cine No. 46, Spastics International Medical Publications, Heinemann, London.
16 Parkin, J.M., Hey, E.N. and Clowes, J.S. (1976): Rapid assessment of gestational age at birth. Arch. Dis. Child., 51, 4, 259-263.
17 Robinson, R.J. (1966): Assessment of gestational age by neurological examination. Arch. Dis. Child., 41,437.
18 Schulte, F.J., Schrempf, G. and Hinze, G. (1971): Maternal toxaemia, fetal malnu- trition and motor behaviour of the newborn. Pediatrics, 48,6,871-882.
19 Stein, H. and Ellis, V. (1974): The low birthweight African baby. Arch. Dis. Child., 49,2,156-159.