Embed Size (px)
Citation preview
Clinical Case Discussion: Considering Conventional and Integrative
Approaches to Anxiety
Amy Locke, M.D.Associate Professor
Department of Family and Preventive Medicine University of Utah School of Medicine
Stephen Warnick, M.D.Assistant Professor
Department of Family Medicine and Department of PsychiatryUniversity of Michigan Medical School
Objectives
• Provide patients with informed information about risks and benefits of common supplements and herbal products, as well as possible non-pharmacologic therapies, including nutritional advice, role of physical activity, importance of sleep and personal connection with others.
• Prescribe effective pharmacologic treatment and recommend evidence-based therapies for anxiety disorders.
Disclosures
• None
Case
35 yo woman with anxiety presents to discuss her care. She has a history of frequent benzodiazepine use that her previous physician found to be concerning. She has tried several antidepressants in the past and has had sexual side effects. She wants to know if Kava is a good option. She also may be interested in starting a family in next 1-2 years.
Anxiety: Scope of the Problem
• 19.1% of US adults in past year with ANY anxiety disorder
– Women 23.4%, Men 14.3 %
• 31.1% of US adults experience ANY anxiety disorder in their lifetime
• Generalized Anxiety Disorder –higher in adolescents, women 2-3 times more likely than men
• Specific phobias most common, followed by panic disorder1.Harvard Medical School, 2007. National Comorbidity Survey (NCS). (2017, August 21). Retrieved from https://www.hcp.med.harvard.edu/ncs/index.php.
2.Data Table 2: 12-month prevalence DSM-IV/WMH-CIDI disorders by sex and cohort.3.Harvard Medical School, 2007. National Comorbidity Survey (NCS). (2017, August 21). Retrieved from https://www.hcp.med.harvard.edu/ncs/index.php.
4. Data Table 1: Lifetime prevalence DSM-IV/WMH-CIDI disorders by sex and cohort.
Conventional Treatments - Therapy
• Cognitive Behavioral Therapy (CBT) – MOST DATA– Studied individually, groups, books, online modules, virtual reality– Virtually all are effective in some format for most anxiety disorders– 6-7 sessions can even be effective!– Panic DO – CBT likely MORE effective than medications– GAD- CBT likely equally efficacious as medications– Includes exposure therapies
• Acceptance and Commitment Therapy (ACT) – MIXED DATA• Psychodynamic Psychotherapy – LIMITED DATA• Therapy benefits likely last for 1-3 years post treatment!
Conventional Treatments - Medications
• Medication recommendations vary slightly by type of anxiety condition.
• Generalized Anxiety Disorder:
– First line SSRI/SNRI, pregabalin [CANMET and NICE] (Level 1)
– Second Line: Quetiapine (not first line due to SE profile; Level 1), Buspirone (due to limited efficacy in some patients), hydroxyzine (Level 1), BDZ (not first line due to substance use concerns; Level 1), Bupropion XL (Level 2)[CANMET – NICE recommends against BDZ]
Depping AM, Komossa K, Kissling W, Leucht S. Second-generation antipsychotics for anxiety disorders. Cochrane Database of Systematic Reviews 2010, Issue 12. Art. No.: CD008120. DOI: 10.1002/14651858.CD008120.pub2
Conventional Treatments – Cochrane
• Antidepressants (SSRI, TCAs) had NNT of 5.5 in Cochrane review compared to placebo
• All therapy with Risk Ratio of 0.48-0.78 compared to weight list
• Cochrane review showing hydroxyzine effective compared to placebo, higher SE burden
• Quetipaine effective compared to other antipsychotics but SE burden
• Buspirone effective but not if prev treated with BDZ
Flynn CA, Chen YC. Antidepressants for generalized anxiety disorder. Am Fam Physician. 2003 Nov 1;68(9):1757-8.Hunot V, Churchill R, Teixeira V, Silva de Lima M. Psychological therapies for generalized anxiety disorder. Cochrane Database of Systematic Reviews 2007, Issue 1.
Art. No.: CD001848. DOI: 10.1002/14651858.CD001848.pub4.
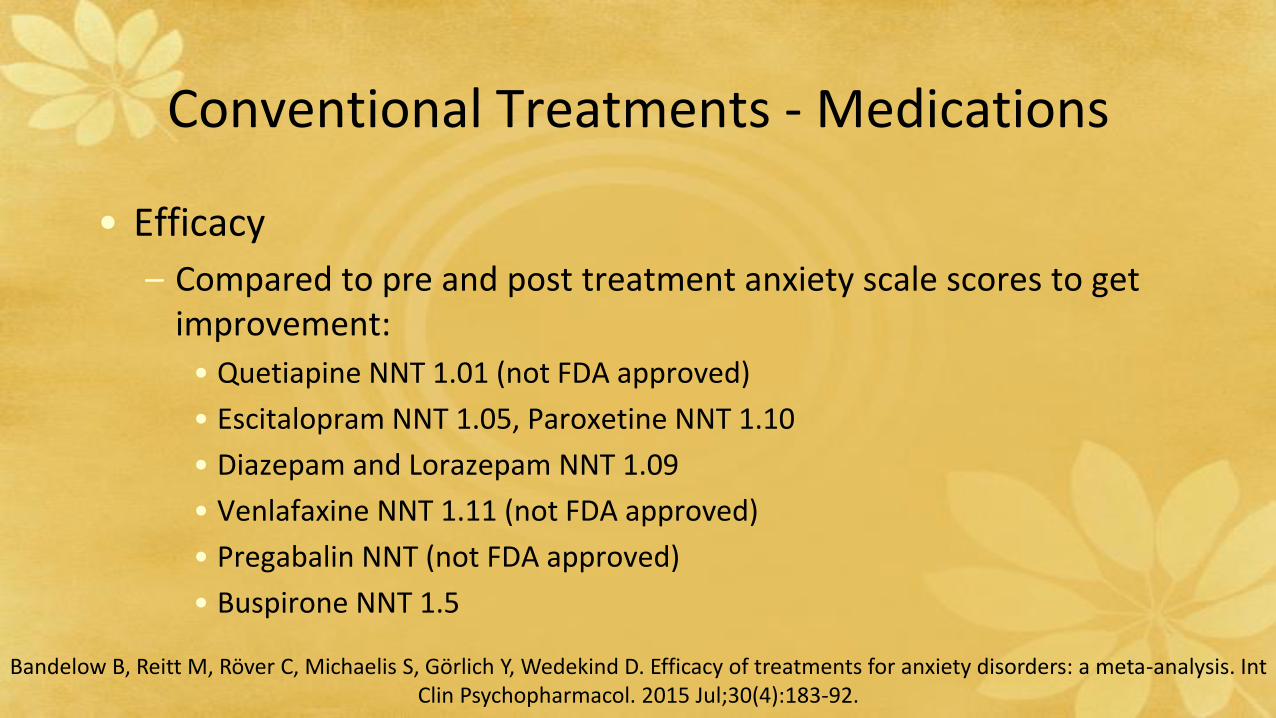
Conventional Treatments - Medications
• Efficacy
– Compared to pre and post treatment anxiety scale scores to get improvement:
• Quetiapine NNT 1.01 (not FDA approved)
• Escitalopram NNT 1.05, Paroxetine NNT 1.10
• Diazepam and Lorazepam NNT 1.09
• Venlafaxine NNT 1.11 (not FDA approved)
• Pregabalin NNT (not FDA approved)
• Buspirone NNT 1.5
Bandelow B, Reitt M, Röver C, Michaelis S, Görlich Y, Wedekind D. Efficacy of treatments for anxiety disorders: a meta-analysis. Int Clin Psychopharmacol. 2015 Jul;30(4):183-92.
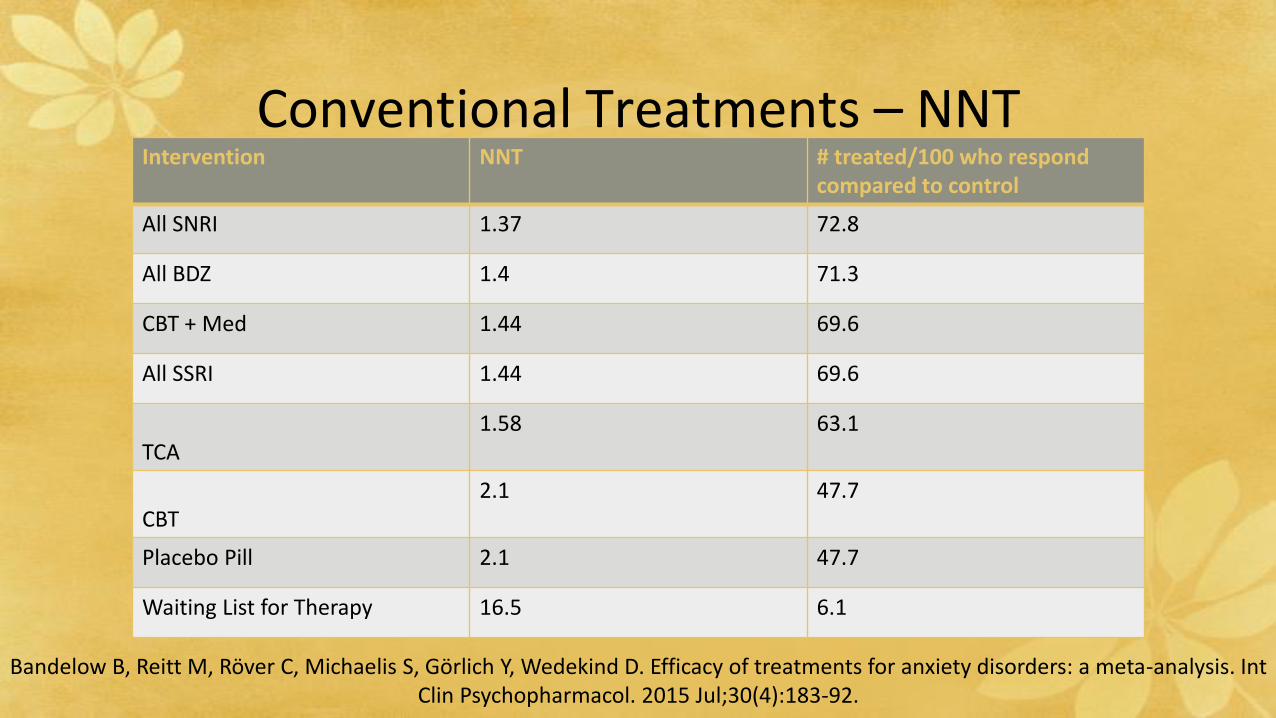
Conventional Treatments – NNT
Bandelow B, Reitt M, Röver C, Michaelis S, Görlich Y, Wedekind D. Efficacy of treatments for anxiety disorders: a meta-analysis. Int Clin Psychopharmacol. 2015 Jul;30(4):183-92.
Intervention NNT # treated/100 who respond compared to control
All SNRI 1.37 72.8
All BDZ 1.4 71.3
CBT + Med 1.44 69.6
All SSRI 1.44 69.6
TCA 1.58 63.1
CBT2.1 47.7
Placebo Pill 2.1 47.7
Waiting List for Therapy 16.5 6.1
Anxiety in Women
• Higher prevalence than men except in social anxiety disorder
• High comorbidity with depression and bulimia (and lower substance use, ADHD, intermittent explosive disorder compared to men)
• Significantly higher rate of more than one anxiety disorder compared to men
• Women more likely to go to ER/urgent care/doctor for anxiety than men– BUT less likely to go to mental health professional!
• Women with anxiety have more missed work days per month than men
McLean CP, Ansari A, Litz BT, Hofmann SG. Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and
burden of illness. J Psychiatr Res. 2011 Aug;45(8):1027-35.
Anxiety in Pregnancy and Lactation
• Evidence on depression in perinatal period is convincing on maternal and infant morbidity
• Untreated anxiety disorders peripartum increase risk of postpartum depression
• SSRIs and SNRIs generally safe to use in pregnancy– General consensus – if severe symptoms, medication effects
outweigh risk, especially if comorbid depression
– SSRI – possible increased low birth weight and preterm birth; other findings inconsistent
Marchesi C, Ossola P, Amerio A, Daniel BD, Tonna M, De Panfilis C. Clinical management of perinatal anxiety disorders: A systematic review. J Affect Disord. 2016 Jan 15;190:543-550.
Anxiety in Pregnancy and Lactation
• BDZ traditionally discouraged during pregnancy– Fetal defect risk may not be as great as once thought
• Quetiapine (not FDA approved) generally safe in pregnancy but high SE burden (used often in bipolar DO, not in anxiety)
• Therapy with no SE burden during pregnancy
• Consensus: CBT first line, SSRI another first line strategy in pregnancy and breastfeeding
• NIH LactMed
Marchesi C, Ossola P, Amerio A, Daniel BD, Tonna M, De Panfilis C. Clinical management of perinatal anxiety disorders: A systematic review. J Affect Disord. 2016 Jan 15;190:543-550.
Case Discussion
• Kava in pregnancy?
• Many medication alternatives to BDZ and SSRI that do not cause sexual side effects or dependence
• Therapy is an option as well
Case Revisited - Integrative
35 yo woman with anxiety presents to discuss her care. She has a history of frequent benzodiazepine use that her previous physician found to be concerning. She has tried several antidepressants in the past and has had sexual side effects. She wants to know if Kava is a good option. She also may be interested in starting a family in next 1-2 years.

Integrative Approach
• Foundations of Health
– Nutrition
– Physical activity
– Sleep
– Connection with others
• Specific nutrition recommendations
• Supplements
• Botanicals
• Medications
• Mind-Body Techniques
• Other therapies
– Manual Medicine
– Movement
– Acupuncture
– Energy work
– Psychotherapy
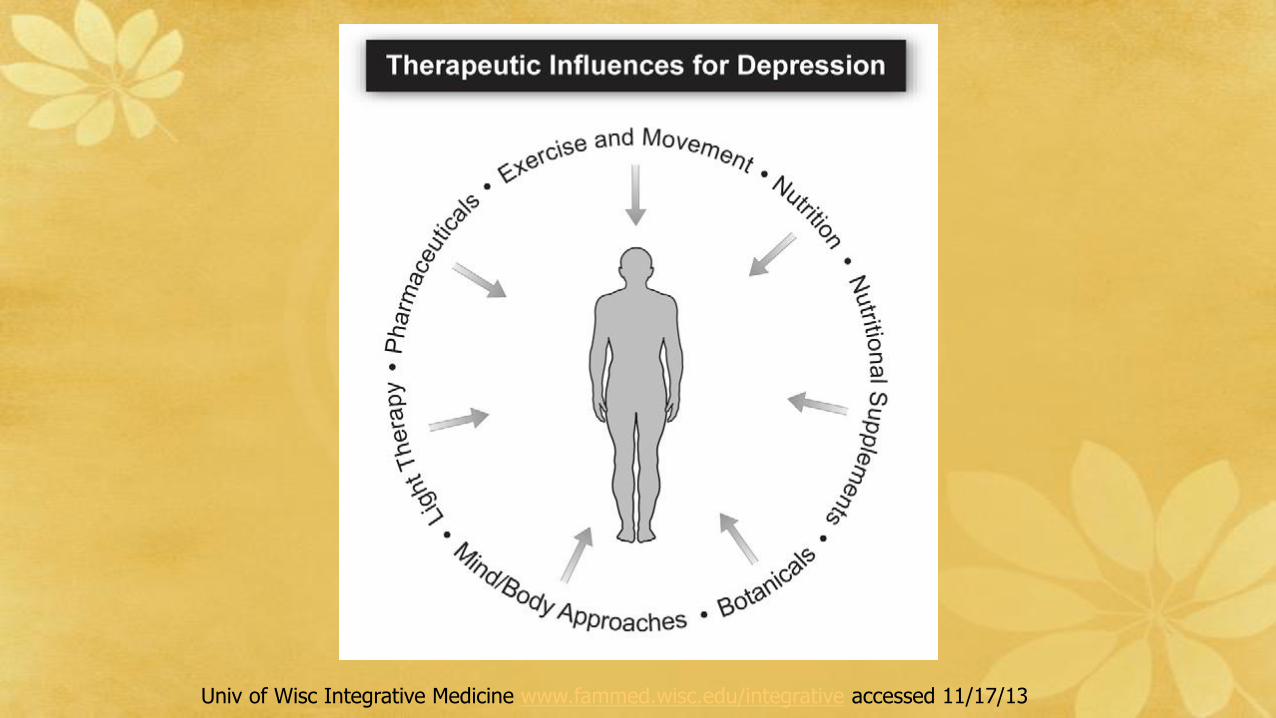
Univ of Wisc Integrative Medicine www.fammed.wisc.edu/integrative accessed 11/17/13
Lifestyle Approaches
• Mediterranean Diet
– Caution with caffeine
• Smoking cessation
• Physical Activity
– Aerobic
– Yoga
• Sleep quality and quantity
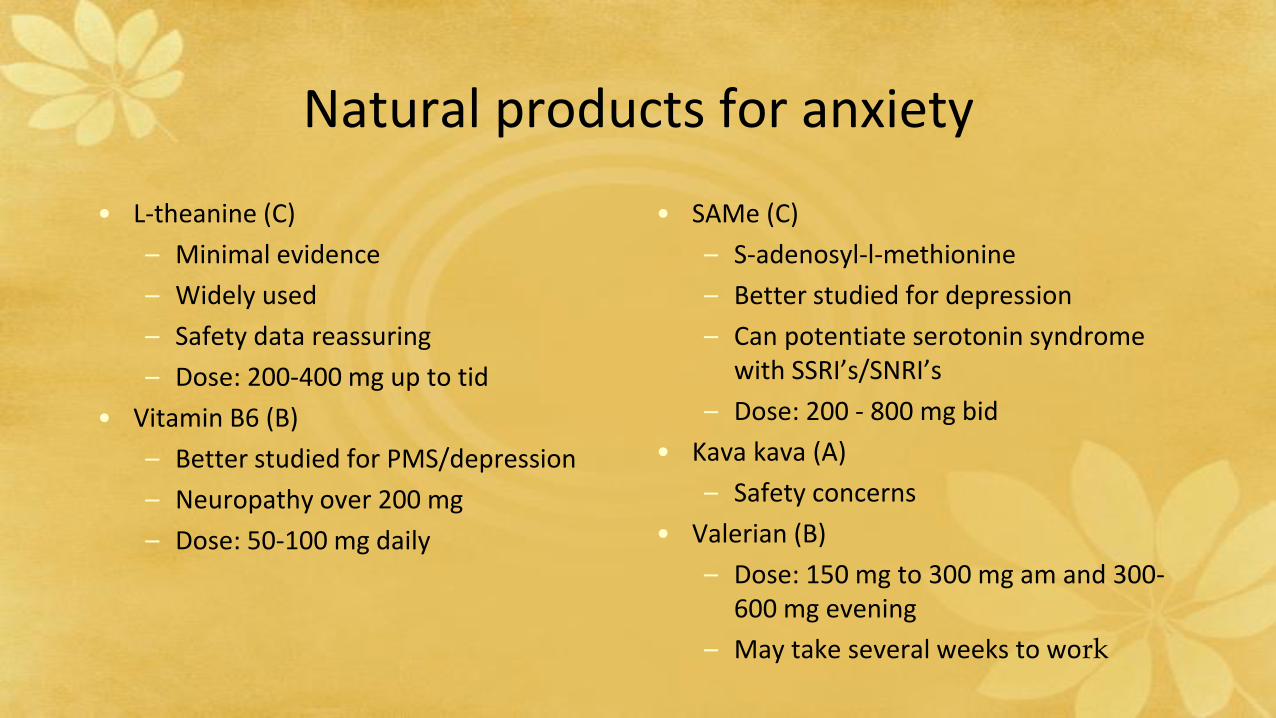
• L-theanine (C)
– Minimal evidence
– Widely used
– Safety data reassuring
– Dose: 200-400 mg up to tid
• Vitamin B6 (B)
– Better studied for PMS/depression
– Neuropathy over 200 mg
– Dose: 50-100 mg daily
Natural products for anxiety
• SAMe (C)
– S-adenosyl-l-methionine
– Better studied for depression
– Can potentiate serotonin syndrome with SSRI’s/SNRI’s
– Dose: 200 - 800 mg bid
• Kava kava (A)
– Safety concerns
• Valerian (B)
– Dose: 150 mg to 300 mg am and 300-600 mg evening
– May take several weeks to work
SAMe
• S-Adenosyl-L-Methionine
• Better studied for depression
• Affects levels of:
– Dopamine
– Norepinephrine
– Serotonin
• Rapid onset
• Dose 400mg to 1600mg daily
– Start 200-400mg daily
• Concerns:
– Expensive
– Serotonin syndrome with SSRI’s
Poll Question
What advice can you give about the use of Kava for anxiety?
A. Kava has evidence for treatment of anxiety
B. Kava is safer than medication for treatment of anxiety
C. Kava has significant safety concerns
D. Kava is not widely available which limits its use
E. A and C
Kava kava (Piper methysticum)
• Number of trials for generalized anxiety
• CNS depressant
• Benzodiazepine receptors
• Metabolized via P450 system
• Often used socially
– Kava bars
– Beverages
• At your local grocery
• May cause hepatic failure
– Banned from many countries
– Not considered safe
Issues related to botanicals
• Identification of plant
• Part used
• How made
– Extract
– Crude plant
– Tea/infusion
• Growing conditions
• Dose
• Certification
– USP (United States Pharmacopeia)• Voluntary testing
• Verify contents and dose
• Consumer Labs
– Independent testing

Other treatments
• Homeopathy
– Rescue Remedy
• Therapeutic Touch
• Aromatherapy
– Essential oils
• Lavender
• Lemon Balm
• Passionflower
• Acupuncture vs. counseling vs. usual care1
– RCT of 755 depressed pts in primary care
– Intervention groups had better PHQ-9 at three months
• Acupuncture vs. IM care vs. conventional2
– RCT of 120 pts with depression and anxiety
– Intervention better at 4 and 8 months
• Both depression and anxiety
Acupuncture
1. MacPherson et al PLoS Med Sept 20132. Arvidsdotter et al BMC Complement Altern Med Nov 2013
• Breathing exercises
• Meditation
– Mindfulness1
• Guided Imagery
• Progressive Muscle Relaxation
• Journaling
• Biofeedback
Mind-Body Techniques
1. Khoury et al. Clin Psychol Rev 2013
• Teaching of Jon Kabat-Zinn
• Widely available
• Similarly effective to CBT
• Evaluated for:
– Depression
– Anxiety
– Psychological Distress
– Pain
Mindfulness Based Stress Reduction
Marchand J Pyschiatr Pract 2012
• Cardiac rehab1
– Meditation more effective than relaxation and control
– Reduced depression, anxiety, HR and BP
• Breast cancer2
– Improved anxiety, fatigue and QOL but not depression
Meditation
1. Delui et al. Open Cardiovasc Med 20132. Kim et al. Complement Ther Med 2013
Bringing it all together
References
• NICE Guidelines (https://www.nice.org.uk/guidance/CG113)• Katzman MA, Bleau P, Blier P, Chokka P, Kjernisted K, Van Ameringen
M; Canadian Anxiety Guidelines Initiative Group on behalf of the Anxiety Disorders Association of Canada/Association Canadienne des troubles anxieux and McGill University, Antony MM, Bouchard S, Brunet A, Flament M, Grigoriadis S, Mendlowitz S, O'Connor K, RabheruK, Richter PM, Robichaud M, Walker JR. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders. BMC Psychiatry. 2014;14 Suppl 1:S1
• Bandelow B, Michaelis S, Wedekind D. Treatment of anxiety disorders. Dialogues Clin Neurosci. 2017 Jun;19(2):93-107.
References- – Cochrane Reviews
• Flynn CA, Chen YC. Antidepressants for generalized anxiety disorder. Am Fam Physician. 2003 Nov 1;68(9):1757-8.
• Depping AM, Komossa K, Kissling W, Leucht S. Second-generation antipsychotics for anxiety disorders. Cochrane Database of Systematic Reviews 2010, Issue 12. Art. No.: CD008120. DOI: 10.1002/14651858.CD008120.pub2
• Hunot V, Churchill R, Teixeira V, Silva de Lima M. Psychological therapies for generalized anxiety disorder. Cochrane Database of Systematic Reviews 2007, Issue 1. Art. No.: CD001848. DOI: 10.1002/14651858.CD001848.pub4.
• Chessick CA, Allen MH, Thase ME., Batista Miralha da Cunha AABC, Kapczinski FFK, Silva de Lima M, dos Santos Souza JJSS. Azapirones for generalized anxiety disorder. Cochrane Database of Systematic Reviews 2006, Issue 3. Art. No.: CD006115. DOI: 10.1002/14651858.CD006115
• Guaiana G, Barbui C, Cipriani A. Hydroxyzine for generalised anxiety disorder. Cochrane Database of Systematic Reviews 2010, Issue 12. Art. No.: CD006815. DOI: 10.1002/14651858.CD006815.pub2
References
• Bandelow B, Reitt M, Röver C, Michaelis S, Görlich Y, Wedekind D. Efficacy of treatments for anxiety disorders: a meta-analysis. Int Clin Psychopharmacol. 2015 Jul;30(4):183-92.
• Marchesi C, Ossola P, Amerio A, Daniel BD, Tonna M, De Panfilis C. Clinical management of perinatal anxiety disorders: A
systematic review. J Affect Disord. 2016 Jan 15;190:543-550
• McLean CP, Asnaani A, Litz BT, Hofmann SG. Gender differences in anxiety disorders: prevalence, course of illness, comorbidity
and burden of illness. J Psychiatr Res. 2011 Aug;45(8):1027-35.