Embed Size (px)
Citation preview

A R T I C L E
Clinical Phenotype and Mutations in Connexin 26(DFNB1/GJB2), the Most Common Cause ofChildhood Hearing LossEDWARD S. COHN AND PHILIP M. KELLEY*
Mutations in the gene for connexin 26, GJB2, are the most common cause of hearing loss in American andEuropean populations, with a carrier rate of about 3%—a rate similar to that for cystic fibrosis. A singlemutation, 35delG, is responsible for most of this autosomal recessive hearing loss, DFNB1. A broad spectrumof mutations in GJB2 has been found to be associated with hearing loss, including another deletionmutation, 167delT, which has a carrier rate of about 4% in the Ashkenazi Jewish population. Mutations inGJB2 have also been found to be associated with dominant nonsyndromic hearing loss, DFNA3. Clinicalstudies have shown that the recessive hearing loss can vary from mild to profound, even within the samesibship. This type of hearing loss is nonsyndromic and is accompanied by normal vision, vestibular re-sponses, and no malformations of the inner ear detectable by computed tomography scanning. Progressiveand asymmetrical hearing loss has been noted in some cases, but it accounts for fewer than one-third ofthe cases of this type of hearing loss. The discovery of mutations in GJB2 that cause hearing loss hasprofound implications in the early diagnosis of hearing loss in general. The relative ease of diagnosis bygenetic testing of Cx26 permits early identification of children with GJB2/DFNB1 hearing loss. This testing,coupled with hearing loss diagnosed by infant auditory brainstem response audiometry, will ensure thathearing-impaired children and their parents receive proper medical, audiologic, genetic, and educationalcounseling. Am. J. Med. Genet. (Semin. Med. Genet.) 89:130–136, 1999. Q 2000 Wiley-Liss, Inc.
KEY WORDS: gap junction; 35delG; variable hearing loss; deafness; recessive
INTRODUCTION
Recessive nonsyndromic hearing loss(RNSHL) accounts for approximate-ly 40% of all childhood hearing loss[van Camp et al., 1997]. Twenty-fiveRNSHL loci have been reported, but asingle locus, DFNB1, accounts for at
least 50% of this type of hearing loss[Maw et al., 1995; van Camp andSmith, 1998]. Recently, the gene re-sponsible for DFNB1 was identified asGJB2, encoding the gap junction pro-tein connexin 26 [Kelsell et al., 1997].The single base deletion mutation,35delG, is responsible for 80% ofDFNB1 hearing loss in European andAmerican populations [Denoyelle et al.,1997; Zelante et al., 1997; Kelley et al.,1998]. It is the cause of one of the mostcommon human genetic disorders,with an incidence similar to that of cys-tic fibrosis [Green et al., 1999]. Thehigh incidence of this type of hearingloss and the ease with which it can nowbe diagnosed by molecular methodspromise to dramatically change thepractice of hearing loss diagnosis.
DFNB1 IS THE MOSTCOMMON SINGLE CAUSEOF HEARING LOSS INEUROPEAN POPULATIONS
In 1994 Guilford et al. mapped a neu-rosensory RNSHL, DFNB1, to chro-
mosome 13q12 in two consanguineousTunisian families. This hearing loss wasdescribed as bilateral and profound.Maw et al. [1995] tested 18 New Zeal-and families and one Australian familywith nonsyndromic hearing loss forlinkage to chromosome 13q12. Thefamilies tested showed recessive inher-itance, with at least two affected chil-dren. Nine of 18 families showed co-segregation of haplotype markers, withhearing loss compatible with linkage to13q12. These results were the firstsuggestion that the source of DFNB1
might be a major contributor to non-syndromic hearing loss. Phenotypic
Dr. Cohn is an Associate Professor in thedepartment of Otolaryngology and Hu-man Communications at Creighton Uni-versity Medical School. He is also StaffOtolaryngologist at the Boys Town Na-tional Research Hospital and is affiliatedwith the BTNRH Genetics department.He studies the clinical features and natu-ral history of hereditary hearing loss. Dr.Kelley is an Assistant Professor in the de-partment of Otolaryngology and HumanCommunications at Creighton UniversityMedical School. He is a Staff Scientist andResearch Associate in the Center for He-reditary Communications Disorders atthe Boys Town National Research Hospi-tal. His research focuses on the identifi-cation of hearing loss genes by positionalcloning.
Contract grant sponsor: NIH-NIDCD;Contract grant number: P01 DC01813-05.
*Correspondence to: Center for theStudy of Hereditary Communication Dis-orders, Boys Town National ResearchHospital, 555 North 30th Street, Omaha,NE 68131. E-mail: [email protected]
Mutations in the gene forconnexin 26, GJB2, are the
most common cause ofhearing loss in American
and European populations.
AMERICAN JOURNAL OF MEDICAL GENETICS (SEMIN. MED. GENET.) 89:130–136 (1999)
© 2000 Wiley-Liss, Inc.

variation of hearing loss within familieswas also noted. In a very large consan-guineous Bedouin family with pro-found bilateral RNSHL, the loss wasalso linked to the 13q12 locus [Scott etal., 1995], but in a study of 27 consan-guineous Pakistani families, only onecase was found to link to DFNB1[Brown et al., 1996]. These resultssuggested that DFNB1 might not ac-count for the major proportion ofRNSHL in at least some non-Europeanpopulations. Gasparini et al. [1997] ana-lyzed 48 Mediterranean families (30Italian and 18 Spanish) and found anabsence of linkage to DFNB1 in ap-proximately 21% of the Mediterraneanfamilies. This study supported earlierfindings that DFNB1 was the majorcause of hearing loss in European popu-lations. Chaib et al. [1994] mapped anonsyndromic neurosensory dominanthearing loss, DFNA3, to the identical13q12 region in a single large Frenchfamily. This dominant hearing loss wasprelingual, bilateral, and symmetrical.Although some members of the familyhave moderately progressive hearingloss, at least 50% are profoundly deaf.
DFNB1-INDUCED HEARINGLOSS IS CAUSED BYMUTATIONS IN GJB2/CX26
During the study of a family with au-tosomal dominant palmoplantar kera-toderma (PPK) and hearing loss, Kelsellet al. [1997] discovered a missense mu-tation (M34T) in CX26 that segregatedas an autosomal dominant mutationwith hearing loss but not with PPK.Upon analysis of CX26 in three con-sanguineous families with autosomalRNSHL that mapped to the same re-gion (13q11-12), two nonsense muta-tions (W24X and W77X) were found.
THE MUTATION 35DELG ISRESPONSIBLE FOR MOSTDFNB1 HEARING LOSS INAMERICAN ANDEUROPEAN POPULATIONS
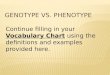
The most common mutation associatedwith DFNB1 hearing loss is a deletionof a guanine from a series of six gua-nines in the coding region of the con-
nexin 26 gene, GJB2 (Fig. 1). This leadsto a frameshift and a resulting stopcodon at position 13. The mutation ispredicted to result in the synthesis of atruncated 12-amino-acid polypeptideinstead of the normal 226-amino-acidpolypeptide. Zelante et al. [1997] firstreported this common connexin 26mutation. They found this mutation in34 of 54 Italian families, six of 12 Span-ish families, and two of four Israelifamilies with RNSHL. Carrasquillo[1997] found the same mutation intwo inbred Israeli-Arab kindreds withhearing loss mapping to 13q11-12. De-noyelle [1997] found 62 mutant allelesin 39 of 65 RNSHL families. About70% of the CX26 mutant alleles were35delG. This population was reportedas white. Most of the families werefrom the United Kingdom and NewZealand, but the group includedfamilies from Tunisia, France, Leb-anon, Algeria, and Portugal. Of 82RNSHL families (51 Italian and 31Spanish), Estivill et al. [1998] found that49% had mutations in CX26. Most hadthe most common mutant allele,35delG. They also found that 27% offamilies with hearing loss linked to
DFNB1 did not have mutations in thecoding region of GJB2, suggesting thatmutations might have been missed inthe promoter for GJB2 or that a secondgene causing RNSHL might be closelylinked to GJB2.
Isolated cases of CX26-associatedhearing loss also have been reportedfrom northern and central Africa[Brobby et al., 1998; Lench et al.,1998]. Among 58 American familiesdiagnosed with RNSHL, 20 familieswere found to have mutations in bothalleles of CX26 [Kelley et al., 1998].The two most common alleles were35delG and the 167delT. Thirty-three35delG mutant al leles and nine167delT mutant alleles were found.Among 96 controls without hearingloss, two individuals were heterozy-gous for 35delG, but no occurrencesof 167delT were noted. The preva-lence of the 35delG mutation in theAmerican population is approximately2.8% [Kelley et al., 1998]. In a studyof an Ashkenazi Jewish populationwith RNSHL, both 35delG and167delT were found [Morell et al.,1998]. The prevalence of the 167delTmutant allele in the normal Ashkenazi
Figure 1. Electropherogram of CX26 (GJB2) sequence from a patient homozygous forthe 35delG mutation and a normal control. The sequence was derived from polymerasechain reaction–amplified genomic DNA, as previously described [Kelley et al., 1998].
ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS (SEMIN. MED. GENET.) 131

Jewish population was found to be4.03%, while that of the 35delGwas 0.73%. A survey of 32 JapaneseRNSHL families found no 35delG mu-tation but did find a new mutation,235delC, that was relatively commonin the Japanese population [Usami etal., 1999].
The high carrier rate (2.5%)[Green et al., 1999] of the 35delG mu-tation in the normal population raisesquestions of the origin of the mutationand why it is present at such a highlevel. Haplotype analysis indicates thatthis mutation arose independentlymany times and is not the result of asingle founder [Carrasquillo et al.,1997; Morell et al., 1998]. The 35delGmutation occurs at a site that shares ho-mology with a putative mutational hotspot, except for a single base [Krawczakand Cooper, 1991]. The sequenceTG(A/G(A/G) (G/T)(A/C) is thoughtto be an arrest site for DNA polymerasealpha and to be especially prone toframeshift mutations. A single base in-sertion, 35insG, and another deletion,31-68del(38), have also been found atthis site (Table I).
HEARING LOSS INPATIENTS HOMOZYGOUSFOR THE CONNEXIN 2635DELG MUTATIONVARIES FROM MILD-MODERATETO PROFOUND
The phenotype of CX26-induced hear-ing loss has proved to be remarkablyvariable in the extent of hearing loss.Part or all of this variability may be dueto the apparent progression of hearingloss that has been documented, but thiswill certainly require further study.Comparing variability in hearing loss isdifficult, because the qualitative termsdescribing it, such as mild, moderate,severe, and profound, and overlappingcategories, such as severe-profound,have been defined and reported differ-ently by different researchers. Similarly,such terms as asymmetry and progres-sion may be defined in varying ways,making comparison difficult. Accep-tance of the definitions proposed by theEuropean Workshop on Genetic Hear-ing Loss would help standardize the re-sults and allow for more meaningfulcomparisons between studies [http://hear.unife.it/].
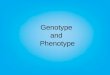
Cohn et al. [1999] examined 46 in-dividuals in 24 families that were eitherhomozygous or compound heterozy-gous for CX26 mutations. A subset ofthese patients was examined for vestib-ular function, otoacoustic emissions,auditory brain-stem response, thyroidfunction, and pleiotropic manifestationsand by temporal bone computed to-mography, electrocardiography, andurinalysis. No other symptoms werefound to be associated with hearingloss. Hearing loss varied in severityfrom mild-moderate to profound, andasymmetry was also observed in 18 of46 individuals. Figure 2 shows the au-diographic results from three patients,illustrating the variability typical of thistype of hearing loss. About one-third ofthe individuals with CX26 mutationsand adequate data on serial audiogramshad progressive hearing loss. Half ofthose with progression (five of ten)were 167delT homozygotes or com-pound heterozygotes. Most of the pa-
tients studied were homozygous forCX26 35delG. The study was unable toshow whether specific mutations couldbe correlated with severity, but therewas a suggestion that the 167delT mu-tation was more severe.
Denoyelle et al. [1999] studied theclinical phenotype in 104 families withtwo affected children but parents withnormal hearing and 47 patients withsporadic hearing loss. As they had re-ported earlier, 35delG homozygoteshad varying degrees of hearing loss.Asymmetrical hearing loss in theirpopulation was rare. Denoyelle et al.and Cohn et al. used different criteriafor asymmetrical hearing loss. Theyfound no vestibular defects and no in-ner ear malformations by computed to-mographic scanning. Of 16 childrenwho were tested after 10 years, twoshowed evidence of progression (1.5 dBper year), and three showed mild hear-ing loss change (0.5–1.0 dB per year).
Combining the clinical data fromCohn et al. and Denoyelle et al., a con-sistent picture of hearing loss caused bymutations in GJB2 is beginning toemerge. All individuals with CX26mutations in both alleles have a signifi-cant prelingual hearing loss. Hearingloss associated with 35delG is variable,ranging from mild-moderate to pro-found. Other mutations are generallyassociated with more severe or pro-found hearing loss. The loss is trulynonsyndromic, since other symptoms,including vestibular defects, are not ap-parent. Children reportedly walk at anormal age. Most cases are bilateral,with profound or severe-profoundhearing loss, and at least two-thirds ofcases do not progress.
A BROAD SPECTRUM OFMUTATIONS HAVE BEENFOUND IN GJB2/DFNB1ASSOCIATED WITHHEARING LOSS
More than 40 mutations have been de-scribed for connexin 26 (Table I). Asingle splice site mutant has been de-tected (Denoyelle et al., 1999; Green etal., 1999). Three single base insertion/
The relative ease of adiagnosis by genetic testing
of CX26 permit earlyidentification of children
with GJB2/DFNB1hearing loss. This testingcoupled with hearing loss
diagnosed by infantauditory brainstem response
audiometry, will ensurethat hearing-impaired
children and their parentsreceive proper medical,audiologic, genetic, andeducational counseling.
132 AMERICAN JOURNAL OF MEDICAL GENETICS (SEMIN. MED. GENET.) ARTICLE

frameshift mutants and 10 small dele-tions have been recognized. One of thedeletion mutations was an in-framethree-base deletion. Seven nonsensemutants and 16 missense mutationshave been discovered. One of the mis-sense mutations occurs at codon 1, re-sulting in conversion of the initiatingmethionine codon to a valine codon.The three missense mutations found inthe first transmembrane domain, M1,and the first extracellular domain, E1,have been characterized as dominantmutations (M34T, W44C, R75W).Codon 34 is methionine in GJB1 andGJB2, though other connexins gener-ally have leucine at this position. Mu-tations W44C and R75W occur at in-variant codons, where no change isapparently tolerated. Four silent muta-tions have been discovered. Four mis-sense mutations in unaffected individu-als have been recognized. Two of themresult in conservative changes from va-line to isoleucine in the first membranedomain. A third missense variant con-verts phenylalanine to leucine at codon83 in the second membrane domain. Afourth change converts glycine to serineat codon 160 in the second extracellulardomain. Because they have not yetbeen associated with any pathologiccondition, they are assumed to be nor-mal variants.
MUTATIONS IN GJB2 HAVEBEEN FOUND TO BEASSOCIATED WITHDOMINANTNONSYNDROMICHEARING LOSS
The M34T mutation was originally de-scribed as causing dominant hearing loss(DFNA3) but has since been found inseveral individuals with normal hearing.Scott et al. [1998b] found the M34Theterozygote once in a control popula-tion of 100 individuals with normalhearing. Kelley et al. [1998] found threeof 96 unrelated individuals with normalhearing who were heterozygous forM34T. Two RNSHL families hetero-zygous for M34T were also reported. Inone family the mutation did not segre-gate with the hearing loss. In the secondfamily the mutation segregated as a re-cessive allele associated with hearingloss when coupled with a second mis-sense mutation, V95M [Kelley et al.,1998]. To complicate this puzzle fur-ther, White et al. [1998] have charac-terized the M34T mutation in an invitro functional assay using the Xenopuslaevis oocyte system. In this assay, CX26with the M34T mutation acts as a dom-inant inhibitor of wild-type CX26.However, the M34T allele appears tobe present in human populations at ahigh enough rate that if it is pathoge-netic as a dominant allele for hearing
loss by itself, it would be a major causeof hearing loss. Furthermore, no homo-zygous M34T individuals with hearingloss have been detected. The highprevalence (four of 196 controls) of thisallele in the normal population and theabsence of homozygous individualswith hearing loss suggest that this allelemay not even be a recessive mutationbut simply a normal variant. Alterna-tively, such an allele might be embry-onic lethal in the homozygous state.The variation in phenotype among in-dividuals who are homozygous for therecessive allele 35delG and the paradoxof the M34T phenotype in vivo and invitro suggest that the role of CX26 ismore complex. Several connexins areknown to be expressed in the cochlea,including CX26, CX30, and CX31.The interaction of these different con-nexins might be key to unraveling thispuzzle.
Two additional dominant muta-tions in CX26 have been reported. De-noyelle et al. [1998] reported a missensemutation, W44C, in a French familythat segregated with hearing loss as anautosomal dominant allele. This muta-tion was not found in 190 unrelatedcontrols. Richard et al. [1998] found amissense mutation, R75W, in an Egyp-tian family in whom both hearing lossand PPK co-segregated. This allele waspresent in one of 154 Egyptian controls
Figure 2. Audiograms from three unrelated patients homozygous for GJB2 35delG. The audiogram for 1586-2 was taken at age 9 years,for 748-7 at age 20.5 years, and for 1560-1 at age 7 years.
ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS (SEMIN. MED. GENET.) 133

who had no evidence of a hereditaryskin disorder. The allele was also testedin the Xenopus laevis oocyte system andgave results similar to those of theM34T allele.
In a study of Ashkenazi Jewish in-dividuals with RNSHL, those hetero-zygous for CX26 mutations were foundto have subtle differences in otoacousticemissions, suggesting a semidominanteffect [Morell et al., 1998]. Audio-graphic data, such as that presented byBrobby et al. [1998], suggest that spe-cific missense mutations, such asR143W, that result in profound hear-ing loss in the homozygous state mightalso have an effect in the heterozygousstate. Such a semidominant effect mightinfluence sensitivity to noise-inducedhearing loss or presbycusis. Further stud-ies of hearing loss in individuals carryingCX26 recessive alleles is warranted.
THE DISCOVERY OFMUTATIONS IN GJB2CAUSING HEARING LOSSHAS SIGNIFICANTIMPLICATIONS IN THEEARLY DIAGNOSIS,MANAGEMENT, ANDGENETIC COUNSELING OFHEARING LOSS
Coupling CX26 testing for newbornswith hearing loss established by diag-nostic Auditory Brainstem Responseaudiometry should have significant util-ity for the parents and professionals car-ing for these children. Although the ge-notype will not predict the hearing in aspecific child, a significant number ofchildren (30–57%) will have profoundhearing loss, and another 26–30% areexpected to have severe hearing loss.Knowledge of genotype will allow phy-sicians, audiologists, educators, and ge-neticists to counsel parents more appro-priately. Genetic counseling of parentswith sporadic patients with CX26 hear-ing loss allows accurate statement of riskthat a subsequent child might havesimilar hearing loss. Audiologists fol-lowing a child who fails newborn diag-nostic screening and shows positive re-sults for a mutation may track moreclosely the progress of the child usingamplification.
TABLE I. Mutations in GJB2: The Gene Encoding Human Connexin 26*
Codon location Nucleotide Mutation type Disease association
IVS1 IVS1 + 1G > A Splice sitea,b RecessiveM1V 1A > G Missense/initiation codonc Recessive10 35delG Deletion/frameshiftd–g Recessive10 31-68del(38) Deletion/frameshifte Recessive10 35insG Insertion/frameshiftc RecessiveW24X 74G > A Nonsenseg,h RecessiveV27I 79G > A Missensei NoneI30I 90T > A/C Silentf NoneM34T 101T > C Missenseh ?r
V37I 109G > A Missensei NoneW44C 132G > C Missensej DominantE47X 139G > T Nonsensec,e Recessive56 167delT Deletion/frameshifta,c,f RecessiveQ57X 169C > T Nonsensek RecessiveY65X 195C > G Nonsensec RecessiveR75W 223C > T Missensel Dominants
W77R 229T > C Missensed RecessiveW77X 231G > A Nonsenseh Recessive78 235delC Deletion/frameshiftm RecessiveF83L 249C > G Missenseg NoneV84L 250G > C Missensei RecessiveL89L 267C > A Silentf None89 267insT Insertion/frameshiftn RecessiveL90P 269T > C Missenseo RecessiveV95M 283G > A Missensei RecessiveR98Q 293G > A Missensen RecessiveH100Y 298C > T Missensen Recessive104 310-323del14 Deletion/frameshiftp Recessive105 314-327del(14) Deletion/frameshifti Recessive111 333-334del(AA) Deletion/frameshifti RecessiveS113R 339T > G Missensej Recessive120 358del(GAG) Deletion/in framee RecessiveK122I 365A > T Missensen RecessiveQ124X 370C > T Nonsenseg RecessiveR127H 380G > A Missensec RecessiveI128I 384C > T Silentf NoneY136X ? Nonsensej,m RecessiveR143W 427T > C Missensej,q,m RecessiveG160S 478G > A Missenseg NoneF161S 482T > C Missenseo RecessiveP173R 518C > G Missenseo Recessive170 510insA Insertion/frameshiftb RecessiveV182V 546G > C Silentg NoneR184P 551G > C Missensee,o Recessive191 572delT Deletion/frameshiftk,l RecessiveS199F 596C > T Missensen Recessive211 631-632del(GT) Deletion/frameshifti Recessive
*Mutations are identified as suggested by the Nomenclature working Group (Anto-narakis, 1998).aMorell et al., 1998.bDenoyelle et al., 1999.cEstivill et al., 1998.dCarrasquillo et al., 1997.eDenoyelle et al., 1997.fZelante et al., 1997.gScott et al., 1998a.hKelsell et al., 1997.iKelley et al., 1998.jDenoyelle et al., 1998.kKelley, unpublished observations.lMurgia et al., 1999.mUsami et al., 1999.nGreen et al., 1999.oRabionet et al., 1999.pMueller et al., 1999.qBrobby et al., 1998.rDisease association with M34T is the subject of controversy (see text).sThis mutation was also found in the control population (see text).
134 AMERICAN JOURNAL OF MEDICAL GENETICS (SEMIN. MED. GENET.) ARTICLE

Some children who do not learn speechwith amplification will be taught signlanguage. Others may have the oppor-tunity to consult with a cochlear im-plant team, depending on the commu-nities in which they reside, economicconsiderations, availability of cochlearimplant devices and teams, and parentalchoice. Children diagnosed and suc-cessfully treated with amplification be-fore age 6 months will have a muchgreater chance of developing normalspeech and language [Yoshinaga-Itanoet al., 1998].
Testing for DFNB1 most likelywill become the first step in determin-ing the cause of hearing loss. A positiveresult for biallelic mutations in theGJB2/DFNB1 gene should eliminatethe need for expensive tests, such aselectroretinography and tests using ra-diation (computed tomography of theinner ear or perchlorate washout studiesfor Pendred syndrome). No longer willthere be a need for deep sedation orgeneral anesthesia of children for manyof these tests. In states where there areuniversal newborn hearing screeningprograms and difficulty with the logis-tics of follow-up after failed diagnosticauditory brain-stem response testing,confirmation of the CX26 mutationmay help prioritize follow-up, becausea significant number of these children(37–57%) are expected to have pro-found hearing loss. The parents whowant to know the source and recur-rence risk of their child’s hearing losswill receive an answer.
ACKNOWLEDGMENTS
This work was supported in part byNIH-NIDCD grant P01 DC01813-05to Dr. William J. Kimberling, BoysTown National Research Hospital.
REFERENCES
Antonarakis SE. 1998. Recommendations for anomenclature system for human gene mu-tations. Nomenclature Working Group.Hum Mutat 11:1–3.
Brobby GW, Muller-Myhsok B, HorstmannRD. 1998. Connexin 26 R143W mutationassociated with recessive nonsyndromicsensorineural deafness in Africa [Letter]. NEngl J Med 338:548–550.
Brown KA, Janjua AH, Karbani G, Parry G,Noble A, Crockford G, Bishop DT, New-ton VE, Markham AF, Mueller RF. 1996.Linkage studies of non-syndromic recessivedeafness (NSRD) in a family originatingfrom the Mirpur region of Pakistan mapsDFNB1 centromeric to D13S175. HumMol Genet 5:169–173. [Published erratumappears in Hum Mol Genet 1996;5(5):710.]
Carrasquillo MM, Zlotogora J, Barges S,Chakravarti A. 1997. Two different con-nexin 26 mutations in an inbred kindredsegregating non-syndromic recessive deaf-ness: implications for genetic studies in iso-lated populations. Hum Mol Genet 6:2163–2172.
Chaib H, Lina-Granade G, Guilford P, PlauchuH, Levilliers J, Morgon A, Petit C. 1994. Agene responsible for a dominant form ofneurosensory non-syndromic deafness mapsto the NSRD1 recessive deafness gene in-terval. Hum Mol Genet 3:2219–2222.
Cohn ES, Kelley PM, Fowler TW, Gorga MP,Lefkowitz DM, Kuehn HJ, Schaefer GB,Gobar LS, Hahn FJ, Harris DJ, KimberlingWJ. 1999. Clinical studies of families withhearing loss attributable to mutations in theconnexin 26 gene (GJB2/DFNB1). Pediat-rics 103:546–550.
Denoyelle F, Lina-Granade G, Plauchu H, Bruz-zone R, Chaib H, Levi-Acobas F, Weil D,Petit C. 1998. Connexin 26 gene linked toa dominant deafness [Letter]. Nature 393:319–320.
Denoyelle F, Marlin S, Weil D, Moatti L, Chau-vin P, Garabedian EN, Petit C. 1999. Clini-cal features of the prevalent form of child-hood deafness, DFNB1, due to a connexin-26 gene defect: implications for geneticcounseling. Lancet 353:1298–1303.
Denoyelle F, Weil D, Maw MA, Wilcox SA,Lench NJ, Allen-Powell DR, Osborn AH,Dahl HH, Middleton A, Houseman MJ,Dode C, Marlin S, Boulila-ElGaied A,Grati M, Ayadi H, BenArab S, Bitoun P,Lina-Granade G, Godet J, Mustapha M,Loiselet J, El-Zir E, Aubois A, Joannard A,Petit C. 1997. Prelingual deafness: highprevalence of a 30delG mutation in theconnexin 26 gene. Hum Mol Genet 6:2173–2177.
Estivill X, Fortina P, Surrey S, Rabionet R, Mel-chionda S, D’Agruma L, Mansfield E, Rap-paport E, Gasparini P, Estivill X, Volpini V,Totaro A, Castellvi-Bel S, Govea N, MilaM, Della MM, Ventruto V, De BenedettoM, Stanziale P, Zelante L, Mansfield ES,Sandkuijl L, Surrey S, Fortina P. 1997.Linkage of DFNB1 to non-syndromic neu-rosensory autosomal-recessive deafness inMediterranean families. Eur J Hum Genet5:83–88.
Govea N, Mila M, Zelante L, Gasparini P. 1998.Connexin-26 mutations in sporadic and in-herited sensorineural deafness. Lancet 351:394–398.
Green GE, Scott DA, McDonald JM, Wood-worth GG, Sheffield VC, Smith RJ. 1999.Carrier rates in the midwestern UnitedStates for GJB2 mutations causing inheriteddeafness. JAMA 281:2211–2216.
Guilford P, Ben Arab S, Blanchard S, Levilliers J,Weissenbach J, Belkahia A, Petit C. 1994.
A non-syndrome form of neurosensory, re-cessive deafness maps to the pericentro-meric region of chromosome 13q. NatureGenet 6:24–28.
Kelley PM, Harris DJ, Comer BC, Askew JW,Fowler T, Smith SD, Kimberling WJ. 1998.Novel mutations in the connexin 26 gene(GJB2) that cause autosomal recessive(DFNB1) hearing loss. Am J Hum Genet62:792–799.
Kelsell DP, Dunlop J, Stevens HP, Lench NJ,Liang JN , Parry G, Mueller RF, Leigh IM.1997. Connexin 26 mutations in hereditarynon-syndromic sensorineural deafness. Na-ture 387:80–83.
Krawczak M, Cooper DN. 1991. Gene deletionscausing human genetic disease: mechanismsof mutagenesis and the role of the localDNA sequence environment. Hum Genet86:425–441.
Lench NJ, Markham AF, Mueller RF, KelsellDP, Smith RJ, Willems PJ, Schatteman I,Capon H, Van De Heyning PJ, van CampG. 1998. A Moroccan family with autoso-mal recessive sensorineural hearing losscaused by a mutation in the gap junctionprotein gene connexin 26 (GJB2). J MedGenet 35:151–152.
Maw MA, Allen-Powell DR, Goodey RJ, Stew-art IA, Nancarrow DJ, Hayward NK, Gard-ner RJ. 1995. The contribution of theDFNB1 locus to neurosensory deafness in aCaucasian population. Am J Hum Genet57:629–635.
Morell RJ, Kim HJ, Hood LJ, Goforth L, Fri-derici K, Fisher R, van Camp G, Berlin CI,Oddoux C, Ostrer H, Keats B, FriedmanTB. 1998. Mutations in the connexin 26gene (GJB2) among Ashkenazi Jews withnonsyndromic recessive deafness. N Engl JMed 339:1500–1505.
Mueller RF, Nehammer A, Middleton A,Houseman MJ, Lench NJ. 1999. Non-syndromal sensorineural hearing impair-ment/deafness: genotype–phenotype stud-ies in autosomal recessive familes, sibs andsporadically affected individuals analysed forconnexin 26 mutations [Abstract]. Am JHum Genet 63:A375.
Murgia A, Polli R, Leonardi E, Martella M, Vi-nanzi C , Orzan E. 1999. Genotype–phenotype correlations in Cx26 deafness[Abstract]. Am J Hum Genet 63:A376.
Rabionet R, Melchionda S, D’Agruma L,Zelante L, Gasparini P, Estivill S. 1999.Mutations in the connexin-26 gene (GJB2)in Italian and Spanish patients with congen-ital deafness [Abstract]. Am J Hum Genet63:A381.
Richard G, White TW, Smith LE, Bailey RA,Compton JG , Paul DL, Bale SJ. 1998.Functional defects of Cx26 resulting from aheterozygous missense mutation in a familywith dominant deaf-mutism and palmo-plantar keratoderma. Hum Genet 103:393–399.
Scott DA, Carmi R, Elbedour K, Duyk GM,Stone EM, Sheffield VC. 1995. Nonsyn-dromic autosomal recessive deafness islinked to the DFNB1 locus in a large inbredBedouin family from Israel [Letter]. Am JHum Genet 57:965–968.
Scott DA, Kraft ML, Carmi R, Ramesh A, El-bedour K, Yairi Y, Srisailapathy CR,
ARTICLE AMERICAN JOURNAL OF MEDICAL GENETICS (SEMIN. MED. GENET.) 135

Rosengren SS, Markham AF, Mueller RF,Lench NJ, van Camp G, Smith RJ, Shef-field VC. 1998a. Identification of mutationsin the connexin 26 gene that cause autoso-mal recessive nonsyndromic hearing loss.Hum Mutat 11:387–394.
Scott DA, Kraft ML, Stone EM, Sheffield VC,Smith RJ. 1998b. Connexin mutations andhearing loss [Letter]. Nature 391:32.
Usami S, Abe S, Shinkawa H, Weston MD, Kel-ley PM, Kimberling WJ. 1999. Prevalentmutations in connexin 26 gene in sporadicand recessive non-syndromic deafness in
Japanese population. Association for Re-search in Otolaryngology Abstract 40(http://www.aro.org).
van Camp G, Smith RJ. 1998. Hereditary Hear-ing Loss Homepage. World Wide Webhttp://hgins.uia.ac.be/dnalab/hhh/.
van Camp G, Willems PJ, Smith RJ. 1997. Non-syndromic hearing impairment: unparal-leled heterogeneity. Am J Hum Genet 60:758–764.
White TW, Deans MR, Kelsell DP, Paul DL.1998. Connexin mutations in deafness [Let-ter]. Nature 394:630–631.
Yoshinaga-Itano C, Sedey AL, Coulter DK,Mehl AL. 1998. Language of early- andlater-identified children with hearing loss.Pediatrics 102:1161–1171.
Zelante L, Gasparini P, Estivill X, Melchionda S,D’Agruma L, Govea N, Mila M, MonicaMD, Lutfi J, Shohat M, Mansfield E, Del-grosso K, Rappaport E, Surrey S, Fortina P.1997. Connexin 26 mutations associatedwith the most common form of non-syndromic neurosensory autosomal reces-sive deafness (DFNB1) in Mediterraneans.Hum Mol Genet 6:1605–1609.
136 AMERICAN JOURNAL OF MEDICAL GENETICS (SEMIN. MED. GENET.) ARTICLE