Embed Size (px)
Citation preview
Orthognathic Surgery Page 1 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
Aetna Better Health® 2000 Market Street, Suite 850 Philadelphia, PA 19103
AETNA BETTER HEALTH®
Clinical Policy Bulletin: Orthognathic Surgery
Revision: March 2015
Number: 0095
Policy
Certain jaw and cranio-facial deformities may cause significant functional
impairment. These deformities include apertognathia (either lateral or anterior not
correctable by orthodontics alone), significant asymmetry of the lower jaw,
significant class 2 and class 3 occlusal discrepancies, and cleft palate. Aetna
considers orthognathic surgery medically necessary for correction of the following
skeletal deformities of the maxilla or mandible when it is documented that these
skeletal deformities are contributing to significant dysfunction, and where the
severity of the deformities precludes adequate treatment through dental
therapeutics and orthodontics alone:
I. Maxillary and/or Mandibular Facial Skeletal Deformities Associated with
Masticatory Malocclusion
Aetna considers orthognathic surgery medically necessary for correction of
skeletal deformities of the maxilla or mandible when it is documented that
these skeletal deformities are contributing to significant masticatory
dysfunction, and where the severity of the deformities precludes adequate
treatment through dental therapeutics and orthodontics:
A. Antero-posterior discrepancies
1. Maxillary/mandibular incisor relationship: overjet of 5
millimeter (mm) or more, or a 0 to a negative value (norm 2
mm),
2. Maxillary/mandibular antero-posterior molar relationship
discrepancy of 4 mm or more (norm 0 to 1 mm).
Note: These values represent 2 or more standard deviations
(SDs) from published norms.
B. Vertical discrepancies

Orthognathic Surgery Page 2 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
1. Presence of a vertical facial skeletal deformity which is 2 or
more SDs from published norms for accepted skeletal
landmarks
2. Open Bite
a. No vertical overlap of anterior teeth greater than 2 mm
b. Unilateral or bilateral posterior open bite greater than 2
mm
3. Deep overbite with impingement or irritation of buccal or
lingual soft tissues of the opposing arch
4. Supraeruption of a dento-alveolar segment due to lack of
opposing occlusion creating dysfunction not amenable to
conventional prosthetics.
C. Transverse discrepancies
1. Presence of a transverse skeletal discrepancy which is 2 or
more SDs from published norms.
2. Total bilateral maxillary palatal cusp to mandibular fossa
discrepancy of 4 mm or greater, or a unilateral discrepancy of
3 mm or greater, given normal axial inclination of the
posterior teeth.
D. Asymmetries
1. Antero-posterior, transverse or lateral asymmetries greater
than 3 mm with concomitant occlusal asymmetry.
II. Facial Skeletal Discrepancies Associated with Documented Sleep Apnea,
Airway Defects, and Soft Tissue Discrepancies
Aetna considers orthognathic surgery medically necessary in cases where
it is documented that mandibular and maxillary deformities are contributing
to airway dysfunction, where such dysfunction is not amenable to non-
surgical treatments, and where it is shown that orthognathic surgery will
decrease airway resistance and improve breathing.
For example, studies demonstrate that persons with vertical hyperplasia of
the maxilla have an associated increase in nasal resistance, as do persons
with maxillary hypoplasia with or without clefts. Following orthognathic
surgery, such individuals routinely demonstrate decreases in nasal airway
resistance and improved respiration.
Aetna considers orthognathic surgery medically necessary for members
with underlying craniofacial skeletal deformities that are contributing to
obstructive sleep apnea. See CPB 0004 - Obstructive Sleep Apnea in
Adults. Before surgery, such individuals should be properly evaluated to
determine the cause and site of their disorder and appropriate non-surgical
treatments attempted when indicated.
Orthognathic Surgery Page 3 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
III. Temporomandibular Joint Pathology
Aetna considers orthognathic surgery for correction of temporomandibular
joint disease or myofascial pain dysfunction experimental and
investigational because its effectiveness for these indications has not been
established. See CPB 0028 - Temporomandibular Disorders.
IV. Speech Impairments
Aetna considers orthognathic surgery medically necessary for treatment of
speech impairments accompanying severe cleft deformity. Orthognathic
surgery may help to reduce the flattening of the face that is characteristic of
severe cleft deformity. By using osteotomy techniques along with bone and
cartilage grafts, the upper and lower jaws and facial skeletal framework are
moved and appropriately reconstructed. Pre-surgical orthodontic treatment
is usually recommended.
Aetna considers other orthognathic surgeries experimental and
investigational for correction of articulation disorders and other impairments
in the production of speech because there is inadequate evidence from
prospective clinical studies in the peer-reviewed published medical
literature of the effectiveness of orthognathic surgery for this indication.
Aetna considers orthognathic surgery for correction of distortions within the
sibilant sound class or for other distortions of speech quality (e.g., hyper-
nasal or hypo-nasal speech) not medically necessary as these distortions
do not cause functional impairment.
V. Unaesthetic Facial Features and Psychological Impairments
Orthognathic surgery is considered cosmetic for correction of unaesthetic
facial features.
Mentoplasty or genial osteotomies/ostectomies (chin surgeries) are always
considered cosmetic when performed as an isolated procedure to address
genial hypoplasia, hypertrophy, or asymmetry, and may be considered
cosmetic when performed with other surgical procedures.
No benefits are available for orthognathic surgery performed primarily for
cosmetic purposes. See Aetna CPB 0031 - Cosmetic Surgery.
VI. Aetna considers the use of condylar positioning devices in orthognathic
surgery experimental and investigational because their effectiveness in
orthognathic surgery has not been established.
VII. Aetna considers orthognathic surgery experimental and investigational for
all indications other than those listed above because their effectiveness for
indications other than the ones listed above has not been established.
VIII. Aetna considers three-dimensional virtual treatment planning of
orthognathic surgery experimental and investigational because its
effectiveness has not been established.
Orthognathic Surgery Page 4 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
Note: Precertification requests or claims for orthognathic surgery are subject to
review by Aetna's Oral and Maxillofacial Surgery Unit.
Orthodontic Treatment Prior to Orthognathic Surgery
Note: Expenses associated with the orthodontic phase of care (both pre- and post-
surgical) are considered dental in nature and are not covered under Aetna's
medical plans. See CPB 0082 - Dental Services and Oral and Maxillofacial
Surgery: Coverage Under Medical Plans.
Orthodontic treatment may be needed prior to orthognathic surgery to position the
teeth in a manner that will provide for an adequate occlusion following surgical
repositioning of the jaws. For plans that require precertification, orthognathic
surgery must be precertified prior to pre-surgical orthodontic treatment. The
interim occlusion that is achieved by orthodontic treatment may be dysfunctional
prior to the completion of the orthognathic surgical phase of the treatment plan.
Therefore, all requests for orthognathic surgery must be reviewed/precertified by
an the Aetna Oral and Maxillofacial Surgery Unit prior to the initiation of pre-
surgical orthodontic care. Failure to obtain precertification of orthognathic surgery
prior to orthodontic care may result in the denial of benefits.
Documentation Requirements
Note: Orthognathic surgery may be subject to precertification review in plans that
include precertification requirements. The following documentation should be
forwarded to Aetna's Oral and Maxillofacial Surgery Unit for review: a written
explanation of the member's clinical course, including dates and nature of any
previous treatment; physical evidence of a skeletal, facial or craniofacial deformity
defined by study models and pre-orthodontic imaging; and a detailed description of
the functional impairment considered to be the direct result of the skeletal
abnormality.
See also CPB 0082 - Dental Services and Oral and Maxillofacial Surgery:
Coverage Under Medical Plans.
Background
Orthognathic surgery is the revision by ostectomy, osteotomy or osteoplasty of the
upper jaw (maxilla) and/or the lower jaw (mandible) intended to alter the
relationship of the jaws and teeth. These surgical procedures are intended (i) to
correct skeletal jaw and cranio-facial deformities that may be associated with
significant functional impairment, and (ii) to reposition the jaws when conventional
orthodontic therapy alone is unable to provide a satisfactory, functional dental
occlusion within the limits of the available alveolar bone. Congenital or
developmental defects can interfere with the normal development of the face and
jaws. These birth defects may interfere with the ability to chew properly, and may
also affect speech and swallowing. In addition, trauma to the face and jaws may
create skeletal deformities that cause significant functional impairment. Functional
deficits addressed by this type of surgery are those that affect the skeletal

Orthognathic Surgery Page 5 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
masticatory apparatus such that chewing, speaking and/or swallowing are
impaired.
There is limited evidence of the effectiveness of orthognathic surgery on
temporomandibular disorders. Abrahamsson et al (2007) examined if orthognathic
surgery does affect the prevalence of signs and symptoms of temporomandibular
disorders (TMDs). A literature survey in the PubMed and Cochrane Library
electronic databases was performed and covered the period from January 1966 to
April 2006. The inclusion criteria were controlled, prospective or retrospective
studies comparing TMDs before and after orthognathic surgery in patients with
malocclusion. There were no language restrictions, and 3 reviewers selected and
extracted the data independently. The quality of the retrieved articles was
evaluated by 4 reviewers. The search strategy resulted in 467 articles, of which 3
met the inclusion criteria. Because of few studies with unambiguous results and
heterogeneity in study design, the scientific evidence was insufficient to evaluate
the effects that orthognathic surgery had on TMD. Moreover, the studies had
problems with inadequate selection description, confounding factors, and lack of
method error analysis. The authors concluded that to obtain reliable scientific
evidence, additional well-controlled and well-designed studies are needed to
determine how and if orthognathic surgery alters signs and symptoms of TMD.
Lindenmeyer et al (2010) performed a systematic review of the best available
research literature investigating the relation of oral and maxillofacial surgical
procedures to the onset or relief of chronic painful TMD. A comprehensive review
of the databases CINAHL, Cochrane Library, Embase, Medline, NHS Evidence--
Oral Health, PsycINFO, Web of Knowledge, and MetaLib was undertaken by 2
authors up to June 2009 using search terms appropriate to establishing a relation
between orofacial surgical procedures and TMD. The search was restricted to
English-language publications. Of the 1,777 titles reviewed, 35 articles were
critically appraised, but only 32 articles were considered eligible. These were
observational studies that fell into 2 groups; 9 were seeking to establish a surgical
cause for TMD. Of these, only 2 of a series of 3 claimed that there was a
significant link, but this claim was based on weak data (health insurance records)
and was abandoned in a subsequent report. Twenty-three studies were seeking
to achieve relief by orthognathic surgical intervention. These were also negative
overall, with 7 articles showing varying degrees of mostly non-significant
improvement, whereas 16 showed no change or a worse outcome. No published
report on the putative effect of implant insertion was found. The authors
concluded that these apparently contradictory approaches underline a belief that
oral surgical trauma or gross malocclusion has a causative role in the onset of
TMD. However, there was no overall evidence of a surgical causal etiology or
orthognathic therapeutic value. This review emphasized that it is in the patients'
best interest to carry out prospective appropriately controlled randomized trials to
clarify the situation.
In a Cochrane review, Luther et al (2010) examined the effectiveness of
orthodontic intervention in reducing symptoms in patients with TMD (compared
with any control group receiving no treatment, placebo treatment or reassurance)
and investigated if active orthodontic intervention leads to TMD. The Cochrane
Oral Health Group's Trials Register, CENTRAL, MEDLINE and EMBASE were
searched. Hand-searching of orthodontic journals and other related journals was

Orthognathic Surgery Page 6 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
undertaken in keeping with the Cochrane Collaboration hand-searching program.
No language restrictions were applied. Authors of any studies were identified, as
were experts offering legal advice, and contacted to identify unpublished trials.
Most recent search was April 13, 2010. All randomized controlled trials (RCTs)
including quasi-randomized trials assessing orthodontic treatment for TMD were
included. Studies with adults aged equal to or above 18 years old with clinically
diagnosed TMD were included. There were no age restrictions for prevention
trials provided the follow-up period extended into adulthood. The inclusion criteria
required reports to state their diagnostic criteria for TMD at the start of treatment
and for participants to exhibit 2 or more of the signs and/or symptoms. The
treatment group included treatment with appliances that could induce stable
orthodontic tooth movement. Patients receiving splints for 8 to 12 weeks and
studies involving surgical intervention (direct exploration/surgery of the joint and/or
orthognathic surgery to correct an abnormality of the underlying skeletal pattern)
were excluded. The outcomes were: how well were the symptoms reduced,
adverse effects on oral health and quality of life. Screening of eligible studies,
assessment of the methodological quality of the trials and data extraction were
conducted in triplicate and independently by 3 review authors. As no 2 studies
compared the same treatment strategies (interventions) it was not possible to
combine the results of any studies. The searches identified 284 records from all
databases. Initial screening of the abstracts and titles by all review authors
identified 55 articles that related to orthodontic treatment and TMD. The full
articles were then retrieved and of these articles only 4 demonstrated any data
that might be of value with respect to TMD and orthodontics. After further analysis
of the full texts of the 4 studies identified, none of the retrieved studies met the
inclusion criteria and all were excluded from this review. The authors concluded
that there are insufficient research data on which to base clinical practice on the
relationship of active orthodontic intervention and TMD. There is an urgent need
for high quality RCTs in this area of orthodontic practice.
There is a lack of evidence to support the use of condylar positioning devices in
orthognathic surgery. Costa et al (2008) stated that in the past few years, many
devices have been proposed for preserving the pre-operative position of the
mandibular condyle during bilateral sagittal split osteotomy. The authors stated
that accurate mandibular condyle re-positioning is considered important to obtain a
stable skeletal and occlusal result, and to prevent the onset of TMD. Condylar
positioning devices (CPDs) have led to longer operating times, the need to keep
inter-maxillary fixation as stable as possible during their application, and the need
for precision in the construction of the splint or intra-operative wax bite. The
authors reviewed the literature concerning the use of CPDs in orthognathic
surgery since 1990 and their application to prevent skeletal instability and contain
TMD since 1995. They concluded that there is no scientific evidence to support
the routine use of CPDs in orthognathic surgery.
Stokbro et al (2014) stated that numerous publications regarding virtual surgical
planning protocols have been published, most reporting only 1 or 2 case reports to
emphasize the hands-on planning. None had systematically reviewed the data
published from clinical trials. This systematic review analyzed the precision and
accuracy of three-dimensional (3D) virtual surgical planning of orthognathic
procedures compared with the actual surgical outcome following orthognathic
surgery reported in clinical trials. These researchers performed a systematic

Orthognathic Surgery Page 7 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
search of the current literature to identify clinical trials with a sample size of more
than 5 patients, comparing the virtual surgical plan with the actual surgical
outcome. Search terms revealed a total of 428 titles, out of which only 7 articles
were included, with a combined sample size of 149 patients. Data were presented
in 3 different ways: intra-class correlation coefficient, 3D surface area with a
difference less than 2mm, and linear and angular differences in 3D. Success
criteria were set at 2 mm mean difference in 6 articles; 125 of the 133 patients
included in these articles were regarded as having had a successful outcome.
Due to differences in the presentation of data, meta-analysis was not possible. The
authors concluded that virtual planning appears to be an accurate and reproducible
method for orthognathic treatment planning; a more uniform presentation of the
data is necessary to allow the performance of a meta-analysis. Moreover, they
stated that currently the software system most often used for 3D virtual planning in
clinical trials is SimPlant (Materialise); more independent clinical
trials are needed to further validate the precision of virtual planning.
Adolphs et al (2014) stated that within the domain of craniomaxillofacial surgery,
orthognathic surgery is a special field dedicated to the correction of dentofacial
anomalies resulting from skeletal malocclusion. Generally, in such cases, an inter-
disciplinary orthodontic and surgical treatment approach is needed. After initial
orthodontic alignment of the dental arches, skeletal discrepancies of the jaws can
be corrected by distinct surgical strategies and procedures in order to achieve
correct occlusal relations, as well as facial balance and harmony within
individualized treatment concepts. To transfer the pre-operative surgical planning
and re-position the mobilized dental arches with optimal occlusal relations, surgical
splints are typically used. For this purpose, different strategies have been
described which use 1 or more splints. Traditionally, these splints are
manufactured by a dental technician based on patient-specific dental casts;
however, computer-assisted technologies have gained increasing importance with
respect to pre-operative planning and its subsequent surgical transfer. In a pilot
study of 10 patients undergoing orthognathic corrections by a 1-splint strategy, 2
final occlusal splints were produced for each patient and compared with respect to
their clinical usability. One splint was manufactured in the traditional way by a
dental technician according to the preoperative surgical planning. After performing
a CBCT scan of the patient's dental casts, a second splint was designed virtually
by an engineer and surgeon working together, according to the desired final
occlusion. For this purpose, RapidSplint, a custom-made software platform, was
used. After post-processing and conversion of the datasets into .stl files, the
splints were fabricated by the PolyJet procedure using photo polymerization.
During surgery, both splints were inserted after mobilization of the dental arches
then compared with respect to their clinical usability according to the occlusal
fitting. Using the workflow described above, virtual splints could be designed and
manufactured for all patients in this pilot study. Eight of 10 virtual splints could be
used clinically to achieve and maintain final occlusion after orthognathic surgery.
In 2 cases virtual splints were not usable due to insufficient occlusal fitting, and
even two of the traditional splints were not clinically usable. In five patients where
both types of splints were available, their occlusal fitting was assessed as being
equivalent, and in one case the virtual splint showed even better occlusal fitting
than the traditional splint. In 1 case where no traditional splint was available, the
virtual splint proved to be helpful in achieving the final occlusion. The authors
Orthognathic Surgery Page 8 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
concluded that the findings of this pilot study demonstrated that clinically usable
splints for orthognathic surgery can be produced by computer-assisted
technology. Virtual splint design was realized by RapidSplint®, an in-house
software platform which might contribute in future to shorten pre-operative
workflows for the production of orthognathic surgical splints. The preliminary
findings from this pilot study need to be validated by well-designed studies.
Swennen (2014) evaluated the timing for 3D virtual treatment planning of
orthognathic surgery in the daily clinical routine. A total of 350 consecutive patients
were included in this study. All patients were scanned following the standardized
"Triple CBCT Scan Protocol" in centric relation. Integrated 3D virtual planning and
actual surgery were performed by the same surgeon in all patients. The authors
concluded that although clinically acceptable, still software improvements
especially toward 3D virtual occlusal definition are mandatory to make 3D virtual
planning of orthognathic surgery less time-consuming and more user-friendly to the
clinician.
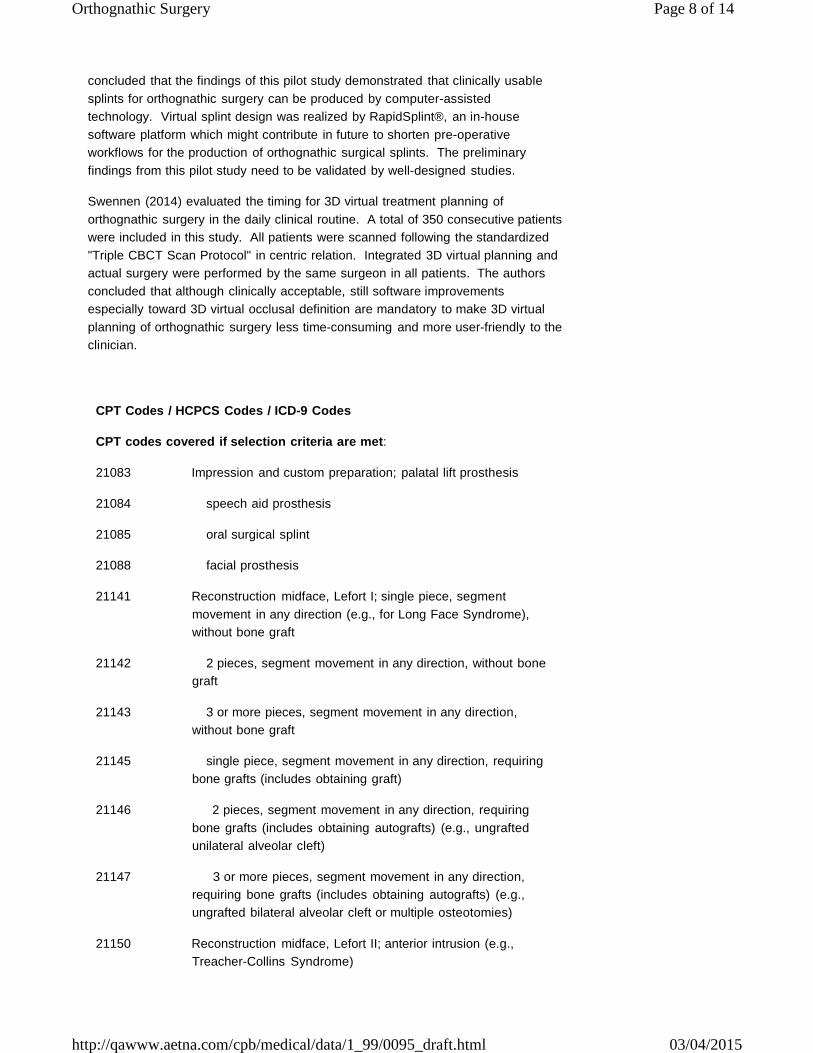
CPT Codes / HCPCS Codes / ICD-9 Codes
CPT codes covered if selection criteria are met:
21083 Impression and custom preparation; palatal lift prosthesis
21084 speech aid prosthesis
21085 oral surgical splint
21088 facial prosthesis
21141 Reconstruction midface, Lefort I; single piece, segment
movement in any direction (e.g., for Long Face Syndrome),
without bone graft
21142 2 pieces, segment movement in any direction, without bone
graft
21143 3 or more pieces, segment movement in any direction,
without bone graft
21145 single piece, segment movement in any direction, requiring
bone grafts (includes obtaining graft)
21146 2 pieces, segment movement in any direction, requiring
bone grafts (includes obtaining autografts) (e.g., ungrafted
unilateral alveolar cleft)
21147 3 or more pieces, segment movement in any direction,
requiring bone grafts (includes obtaining autografts) (e.g.,
ungrafted bilateral alveolar cleft or multiple osteotomies)
21150 Reconstruction midface, Lefort II; anterior intrusion (e.g.,
Treacher-Collins Syndrome)

Orthognathic Surgery Page 9 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
21151 any direction, requiring bone grafts (includes obtaining
autografts)
21154 Reconstruction midface, Lefort III (extracranial), any type,
requiring bone grafts (includes obtaining autografts); without
Lefort I
21155 with Lefort I
21159 Reconstruction midface, Lefort III (extra and intracranial) with
forehead advancement (e.g., mono bloc), requiring bone grafts
(includes obtaining autografts): without Lefort I
21160 with Lefort I
21181 Reconstruction by contouring of benign tumor of cranial bones
(e.g., fibrous dysplasia), extracranial
21182 Reconstruction of orbital walls, rims, forehead, nasoethmoid
complex following intra- and extracranial excision of benign
tumor of cranial bone (e.g., fibrous dysplasia) with multiple
autografts (includes obtaining grafts); total area of bone
grafting less than 40 sq cm
21183 total area of bone grafting greater than 40 sq cm but less
than 80 sq cm
21184 total area of bone grafting greater than 80 sq cm
21188 Reconstruction midface, osteotomies (other than Lefort type)
and bone grafts (includes obtaining autografts)
21193 Reconstruction of mandibular rami, horizontal, vertical, C, or L
osteotomy; without bone graft
21194 with bone graft (includes obtaining graft)
21195 Reconstruction of mandibular rami and/or body, sagittal split;
without internal rigid fixation
21196 with internal rigid fixation
21198 Osteotomy, mandible, segmental;
21199 with genioglossus advancement
21206 Osteotomy, maxilla, segmental (e.g., Wassmund or
Schuchard)
21208 Osteoplasty, facial bones; augmentation (autograft, allograft, or
prosthetic implant)
21209 reduction

Orthognathic Surgery Page 10 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
21210 Graft, bone; nasal, maxillary or malar areas (includes obtaining
graft)
21215 mandible (includes obtaining graft)
21230 Graft; rib cartilage, autogenous, to face, chin, nose or ear
(includes obtaining graft)
21235 ear cartilage, autogenous, to nose or ear (includes obtaining
graft)
21240 Arthroplasty, temporomandibular joint, with or without autograft
(includes obtaining graft)
21242 Arthroplasty, temporomandibular joint, with allograft
21243 Arthroplasty, temporomandibular joint, with prosthetic joint
replacement
21247 Reconstruction of mandibular condyle with bone and cartilage
autografts (includes obtaining grafts) (e.g., for hemifacial
microsomia)
21255 Reconstruction of zygomatic arch and glenoid fossa with bone
and cartilage (includes obtaining autografts)
21270 Malar augmentation, prosthetic material
21275 Secondary revision of orbitocraniofacial reconstruction
21295 Reduction of masseter muscle and bone (e.g., for treatment of
benign masseteric hypertrophy); extraoral approach
21296 intraoral approach
42200 -
42281
Repair of palate
CPT codes not covered for indications listed in the CPB:
21125 Augmentation, mandibular body or angle; prosthetic material
21127 with bone graft, onlay or interpositional (includes obtaining
autograft)
Other CPT codes related to the CPB:
21110 Application of interdental fixation device for conditions other
than fracture or dislocation, includes removal
21120 -
21123
Genioplasty
HCPCS codes covered if selection criteria are met:

Orthognathic Surgery Page 11 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
D5954 -
D5959
Palatal augmentation and lift prosthesis
D7940 -
D7955
Other repair procedures
Other HCPCS codes related to the CPB:
D8010 -
D8999
Orthodontics
ICD-9 codes covered if selection criteria are met:
524.00 -
524.29
Major anomalies of jaw size and dental arch relationship
524.4 -
524.59
Malocclusion and dentofacial functional abnormalities
749.00 -
749.04
Cleft palate
749.20 -
749.25
Cleft palate with cleft lip
327.23 Obstructive sleep apnea (adult) (pediatric) [associated with
facial skeletal deformities]
ICD-9 codes not covered for indications listed in the CPB:
524.60 -
524.69
Temporomandibular joint disorders
V50.1 Other plastic surgery for unacceptable cosmetic appearance
Other ICD-9 related to the CPB:
784.5 Other speech disturbance
786.00 -
786.09
Dyspnea and respiratory abnormalities [associated with
obstructive airway defects]
The above policy is based on the following references:
1. McCarthy JG, Stelnicki EJ, Grayson BH. Distraction osteogenesis of the
mandible: A ten-year experience. Semin Orthod. 1999;5(1):3-8.
2. Baker NJ, David S, Barnard DW, et al. Occlusal outcome in patients
undergoing orthognathic surgery with internal fixation. Br J Oral Maxillofac
Surg. 1999;37(2):90-93.
3. Bennett ME, Phillips CL. Assessment of health-related quality of life for
patients with severe skeletal disharmony: A review of the issues. Int J Adult
Orthodon Orthognath Surg. 1999;14(1):65-75.
Orthognathic Surgery Page 12 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
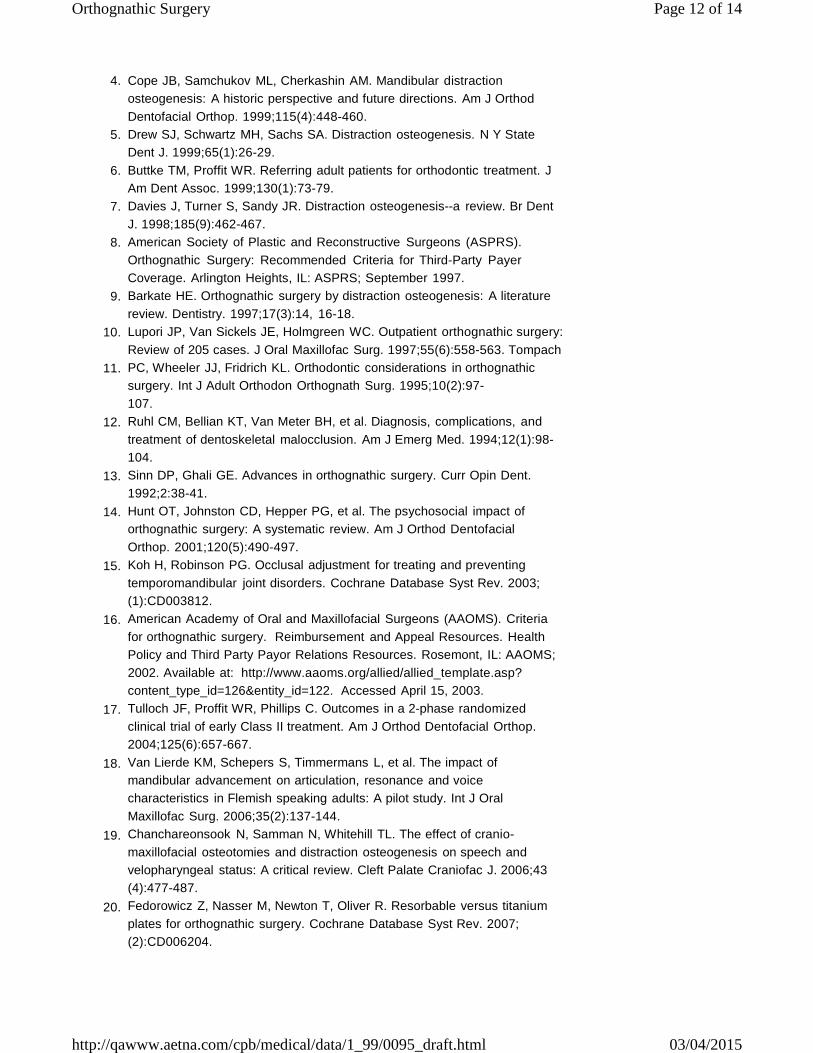
Cope JB, Samchukov ML, Cherkashin AM. Mandibular distraction
osteogenesis: A historic perspective and future directions. Am J Orthod
Dentofacial Orthop. 1999;115(4):448-460.
Drew SJ, Schwartz MH, Sachs SA. Distraction osteogenesis. N Y State
Dent J. 1999;65(1):26-29.
Buttke TM, Proffit WR. Referring adult patients for orthodontic treatment. J
Am Dent Assoc. 1999;130(1):73-79.
Davies J, Turner S, Sandy JR. Distraction osteogenesis--a review. Br Dent
J. 1998;185(9):462-467.
American Society of Plastic and Reconstructive Surgeons (ASPRS).
Orthognathic Surgery: Recommended Criteria for Third-Party Payer
Coverage. Arlington Heights, IL: ASPRS; September 1997.
Barkate HE. Orthognathic surgery by distraction osteogenesis: A literature
review. Dentistry. 1997;17(3):14, 16-18.
Lupori JP, Van Sickels JE, Holmgreen WC. Outpatient orthognathic surgery:
Review of 205 cases. J Oral Maxillofac Surg. 1997;55(6):558-563. Tompach
PC, Wheeler JJ, Fridrich KL. Orthodontic considerations in orthognathic
surgery. Int J Adult Orthodon Orthognath Surg. 1995;10(2):97-
107.
Ruhl CM, Bellian KT, Van Meter BH, et al. Diagnosis, complications, and
treatment of dentoskeletal malocclusion. Am J Emerg Med. 1994;12(1):98-
104.
Sinn DP, Ghali GE. Advances in orthognathic surgery. Curr Opin Dent.
1992;2:38-41.
Hunt OT, Johnston CD, Hepper PG, et al. The psychosocial impact of
orthognathic surgery: A systematic review. Am J Orthod Dentofacial
Orthop. 2001;120(5):490-497.
Koh H, Robinson PG. Occlusal adjustment for treating and preventing
temporomandibular joint disorders. Cochrane Database Syst Rev. 2003;
(1):CD003812.
American Academy of Oral and Maxillofacial Surgeons (AAOMS). Criteria
for orthognathic surgery. Reimbursement and Appeal Resources. Health
Policy and Third Party Payor Relations Resources. Rosemont, IL: AAOMS;
2002. Available at: http://www.aaoms.org/allied/allied_template.asp?
content_type_id=126&entity_id=122. Accessed April 15, 2003.
Tulloch JF, Proffit WR, Phillips C. Outcomes in a 2-phase randomized
clinical trial of early Class II treatment. Am J Orthod Dentofacial Orthop.
2004;125(6):657-667.
Van Lierde KM, Schepers S, Timmermans L, et al. The impact of
mandibular advancement on articulation, resonance and voice
characteristics in Flemish speaking adults: A pilot study. Int J Oral
Maxillofac Surg. 2006;35(2):137-144.
Chanchareonsook N, Samman N, Whitehill TL. The effect of cranio-
maxillofacial osteotomies and distraction osteogenesis on speech and
velopharyngeal status: A critical review. Cleft Palate Craniofac J. 2006;43
(4):477-487.
Fedorowicz Z, Nasser M, Newton T, Oliver R. Resorbable versus titanium
plates for orthognathic surgery. Cochrane Database Syst Rev. 2007;
(2):CD006204.

Orthognathic Surgery Page 13 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
Hassan T, Naini FB, Gill DS. The effects of orthognathic surgery on speech:
A review. J Oral Maxillofac Surg. 2007;65(12):2536-2543.
Abrahamsson C, Ekberg E, Henrikson T, Bondemark L. Alterations of
temporomandibular disorders before and after orthognathic surgery: A
systematic review. Angle Orthod. 2007;77(4):729-734.
Lye KW. Effect of orthognathic surgery on the posterior airway space
(PAS). Ann Acad Med Singapore. 2008;37(8):677-682.
Won CH, Li KK, Guilleminault C. Surgical treatment of obstructive sleep
apnea: Upper airway and maxillomandibular surgery. Proc Am Thorac Soc.
2008;5(2):193-199.
Costa F, Robiony M, Toro C, et al. Condylar positioning devices for
orthognathic surgery: A literature review. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod. 2008;106(2):179-190.
Kang SH, Yoo JH, Yi CK. The efficacy of postoperative prophylactic
antibiotics in orthognathic surgery: A prospective study in Le Fort I
osteotomy and bilateral intraoral vertical ramus osteotomy. Yonsei Med J.
2009;50(1):55-59.
Danda AK, Wahab A, Narayanan V, Siddareddi A. Single-dose versus
single-day antibiotic prophylaxis for orthognathic surgery: A prospective,
randomized, double-blind clinical study. J Oral Maxillofac Surg. 2010;68
(2):344-346.
Dan AE, Thygesen TH, Pinholt EM. Corticosteroid administration in oral
and orthognathic surgery: A systematic review of the literature and meta-
analysis. J Oral Maxillofac Surg. 2010;68(9):2207-2220.
Garg M, Cascarini L, Coombes DM, et al. Multicentre study of operating
time and inpatient stay for orthognathic surgery. Br J Oral Maxillofac Surg.
2010;48(5):360-363.
Lindenmeyer A, Sutcliffe P, Eghtessad M, et al. Oral and maxillofacial
surgery and chronic painful temporomandibular disorders -- a systematic
review. J Oral Maxillofac Surg. 2010;68(11):2755-2764.
Luther F, Layton S, McDonald F. Orthodontics for treating
temporomandibular joint (TMJ) disorders. Cochrane Database Syst Rev.
2010;(7):CD006541.
Pineiro-Aguilar A, Somoza-Martín M, Gandara-Rey JM, Garcia-Garcia A.
Blood loss in orthognathic surgery: A systematic review. J Oral Maxillofac
Surg. 2011;69(3):885-892.
Danda AK, Ravi P. Effectiveness of postoperative antibiotics in orthognathic
surgery: A meta-analysis. J Oral Maxillofac Surg. 2011;69(10):2650-2656.
Mattos CT, Vilani GN, Sant'Anna EF, et al. Effects of orthognathic surgery
on oropharyngeal airway: A meta-analysis. Int J Oral Maxillofac Surg.
2011;40(12):1347-1356.
Stokbro K, Aagaard E, Torkov P, et al. Virtual planning in orthognathic
surgery. Int J Oral Maxillofac Surg. 2014;43(8):957-965.
Adolphs N, Liu W, Keeve E, Hoffmeister B. RapidSplint: Virtual splint
generation for orthognathic surgery - results of a pilot series. Comput Aided
Surg. 2014;19(1-3):20-28.
Swennen GR. Timing of three-dimensional virtual treatment planning of
orthognathic surgery: A prospective single-surgeon evaluation on 350
consecutive cases. Oral Maxillofac Surg Clin North Am. 2014;26(4):475-
485.

Orthognathic Surgery Page 14 of 14
http://qawww.aetna.com/cpb/medical/data/1_99/0095_draft.html 03/04/2015
Copyright Aetna Inc. All rights reserved. Clinical Policy Bulletins are developed by Aetna to assist in
administering plan benefits and constitute neither offers of coverage nor medical advice. This Clinical Policy
Bulletin contains only a partial, general description of plan or program benefits and does not constitute a
contract. Aetna does not provide health care services and, therefore, cannot guarantee any results or
outcomes. Participating providers are independent contractors in private practice and are neither
employees nor agents of Aetna or its affiliates. Treating providers are solely responsible for medical advice
and treatment of members. This Clinical Policy Bulletin may be updated and therefore is subject to change.
CPT only copyright 2008 American Medical Association. All Rights Reserved.