Embed Size (px)
Citation preview

CNS Neoplasia
Presented By:
Joseph S. Ferezy, D.C.

Primary Tumors
80% of All CNS Tumors

Primary Brain Tumors:
Arise from cells originating in the tissue of the brain and skull.
Rarely spread to other areas of the body, but they can spread to other parts of the brain and to the spinal cord.
Prognoses determined by histologic type (cell type) grade of malignancy extent of the tumor patient's age, the performance status, and the
duration of symptoms.

Primary Tumors: Astrocytoma
Gliomas (Non-neuronal Tissue) 45% Histological classification for adult brain
tumors: Glial tumors: Gliomas constitute the most
common primary central nervous system (CNS) tumors. Of the gliomas, astrocytomas of variable malignancy are the most prevalent. Cerebral astrocytomas are subdivided into categories (grades) based on the degree of tumor anaplasia and the presence or absence of necrosis.

Primary Tumors: Astrocytoma
Astrocytic tumors noninfiltrating - These astrocytomas are
relatively slow-growing tumors such as juvenile pilocytic and subependymal astrocytomas, which occur most frequently in children but can occur in adults.
juvenile pilocytic subependymal

Primary Tumors: Astrocytoma
infiltrating - These tumors are more infiltrative than the juvenile pilocytic and subependymal astrocytomas but are still relatively slow-growing tumors.
well-differentiated mildly and moderately anaplastic astrocytoma
anaplastic astrocytoma - These tumors are highly anaplastic with obvious vascular abnormalities. This grade III astrocytoma grows more rapidly than the more differentiated astrocytomas.

Primary Tumors: Summary -Astrocytoma
Benign Commonest in Children May Become Malignant (Glioblastoma Multiform)
at Any Time Peak Incidence @ 30-40 Yrs. Or Child Usually Frontal Unilateral HA or Generalized Skull Films Show Displaced Calcified Pineal
Gland, CT Scan Cerebral or Cerebellar

Astrocytoma

Astrocytoma: Optic Nerve

Astrocytoma: Gross


Primary Tumors: Astrocytoma

Primary Tumors
Glioblastoma Multiforme (Grade IV Astrocytoma) Most Common
in Adult Usually 50-60
Yrs. Malignant Rapid
Progression

GBM

GBM Case Study
Clinical History: 61-year-old RH white male with history of multiple CVAs with new onset of right sided hemiparesis of one week duration.
Diagnosis: Bifrontal butterfly S-shaped lesion consistent with glioblastoma multiforme.

GBM Case Study
Axial post Gadolinium T1 W1 of the brain reveals a large necrotic butterfly mass involving the corpus callosum with enhancing borders.
There is no evidence of herniation.

GBM Case Study
Discussion: A butterfly lesion is a lesion which infiltrates across the corpus callosum. Thus this pathological process spreads from one hemisphere to another.
The differential diagnosis of a butterfly lesion includes: glioblastoma multiforme (GBM), lymphoma, and demyelinating process.

GBM Case Study
Symptoms can range from seizures to focal neurologic deficits to symptoms associated with increased intracranial pressure (headaches, nausea, vomiting, decreased visual acuity).
Once a mass lesion is suspected, then an MRI with Gadolinium should be performed.
This will usually show the classic ring enhancing (associated with angiogenesis occurring at the periphery of the tumor) lesion.
However, definitive diagnosis is based on surgical biopsy.

GBM Case Study
GBM tumors are treated with surgical resection and post-operative radiation. Nonetheless, this malignant process has a poor prognosis with the median survival being 8-10 months. The 1, 2, and 5-year survival rates are 30-44%, 8-12%, and 2.5-5%. The most common cause of death is reoccurrence of tumor at the original site.

GBM Case Study
References:Grossman R, Loftus C. Principles of Neurosurgery. Lippincott-Raven, Philadelphia; 1999.
Submitted by:Robert Lee, M.D.Aditya PandeyC. F. Lanzieri, M.D.

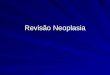
GBMT1W MR after Gadolinium infusion reveals a thalamic mass lesion. Characterized by irregular ring-enhancement surrounding a central non-enhancing region of necrosis. Note the shaggy inner-margin of the ring, and the variation in its thickness. The small foci of internal enhancement represent islands of living tumor within the regions of necrosis.

Primary Tumors - Oligodendrogliomas
Uusually found in the cerebral hemispheres of middle aged adults
Comprise about 5% of neuroectodermal tumors.
Grow fairly slowly and there is a mean 5-year survival rate.
May appear more circumscribed than astrocytomas.
30-40 Yrs. Chronic Ha & Seizures Maybe Only Symptoms

Primary Tumors – Oligodendrogliomas

Primary Tumors – Epenymoma
ependymomas are predominantly tumors of childhood and adolescence and account for 6% of all neuroectodermal tumors.
Survival usually does not exceed a few years. They arise most frequently in the fourth ventricle and
may cause hydrocephalus by blocking off the normal flow of CSF.
However, they can occur anywhere in relation to the ventricular system or central canal and are the most common glioma in the spinal cord and filum terminale.
In the spinal cord, they are somewhat well circumscribed and can sometimes be "shelled out" surgically.

Primary Tumors – Epenymoma
A Slow Growing, Calcific, Ventricular Wall Tumor (Usually 4th Ventricle), Occurring Most Often in Children.
Signs and Symptoms of Increased Intracranial Pressure – Short Average Survival
Increase Intracranial Pressure = Nausea, Vomiting, Papilledema

CSF Flow

Primary Tumors – Epenymoma Case
Clinical History: 19-month-old female with enlarging head circumference and gross motor delay.

Primary Tumors – Epenymoma Case
Radiologic Findings: large posterior fossa mass on a nonenhanced CT. Prominent features shown are obstructive hydrocephalus, obliteration of the fourth ventricle, and marked internal calcifications.

Primary Tumors – Epenymoma Case
Images two and three are T1 and T2 weighted MR axial scans prior to contrast.
These confirm the presence of a mass lesion and elicit several internal flow voids suggesting encasement of at least the right superior cerebellar artery.
The mass extends laterally through the right foramen of Luschka.

Primary Tumors – Epenymoma Case
Images four and five are also T1 weighted MR scans, now following gadolinium administration and shown in axial and sagittal planes.
These demonstrate heterogeneous enhancement and clearly show marked mass effect on the medulla as well as complete compromise of the foramen magnum.
Following emergent ventricular decompression, the patient was taken for operative resection.

Primary Tumors – Epenymoma Case
The final image shows the gross intraoperative appearance with the tumor fungating out the foramen of Magiendie beneath the cerebellar hemispheres.

Primary Tumors – Epenymoma Diagnosis: Differential diagnostic considerations for
fourth ventricular masses in children include pilocytic astrocytoma, medulloblastoma, ependymoma, brainstem glioma, and choroid plexus papilloma. Pathologic evaluation diagnosed an ependymoma.
Intracranially sixty percent are infratentorial, and of these the vast majority occur in the fourth ventricle.
Typically they present in children less than five. A smaller number appear in thirty to forty year olds. The tumors are slow growing and lobulated. They tend to fill the ventricle and can extend out the
exiting foramina.

Primary Tumors – Epenymoma
About one half will present with calcifications.
Often they will be cystic when supratentorial. These tend to be isodense on CT, iso/hypointense on T1, and iso/hyperintense on T2. Enhancement is heterogeneous and moderate. Prognosis is moderate as many will die from recurrence or progression.

Primary Tumors – Epenymoma
References: Furie, DM and Provenzale, JM: Supratentorial Ependymomas and Subependymomas: CT and MR Appearance, J Comp. Asst. Tomo. 19:518-526.
Osborne, AG: Diagnostic Neuroradiology, Mosby, pp566-571. Tortori-Donati, P, et al.: Ependymomas of the posterior cranial
fossa: CT and MRfindings, Neurorad. 37:238-243, 1995.
Willing, SJ, Atlas of Neuroradiology, Saunders, pp 200-204.
Submitted by:Jeffrey L. Sunshine, M.D.Neuroradiology

Primary Tumors - Choroid Plexus Papilloma
Related to ependymoma papilloma
Benign, although choroid plexus carcinomas do exist.
Rare & Found in Children
Associated Hydrocephalus

Primary Tumors – Medulloblastoma
2nd Most Common in Child
Usually in Cerebellar Vermis
Highly Malignant Male:female 2-3:1 Ataxia and Cerebellar
Vermis Syndrome

Primary Tumors – Medulloblastoma
Tumors of neuronal origin are rare and the only important intracranial tumor of this group is the medulloblastoma (neuroblastoma). The term medulloblastoma is a misnomer, since a medulloblast has never been isolated, but the name is too well entrenched to be eradicated.
Most think that these tumors arise from identical cells in one of two sites.
First, from migrating neuroblasts which have become arrested in the roof of the fourth ventricle (anterior medullary vellum). This would account for the midline location of many of the tumors.
Second, from the external granular layer of the cerebellum. The migrating cells form this layer in the immature cerebellum before entering the deep cerebellar cortex (granular layer). The external granular layer disappears (through inward migration) by the second year of life.
Because of its origin from immature cells, it is not surprising that the majority of medulloblastomas are seen during the first decade of life. However, there is another peak in young adulthood. These tend to be more laterally placed and have a better prognosis. The fact that some medulloblastomas may simultaneously differentiate along astrocytic lines is another reason that some pathologists retain the name "medulloblastoma."

Primary Tumors
Pinealoma In Area of Pineal
Gland Increased Intracranial
Pressure

Primary Tumors - Pituitary Adenoma Pituitary adenomas make up approximately 8% of all
intracranial tumors. They predominate in adolescence and young
adulthood. They are usually benign and grow slowly. Historically, they have been divided into
chromophobe, eosinophilic and basophilic varieties, depending on their tinctorial properties.
The adenomas are thought to be derived from one of these normal cell types.
Previously, it was taught that basophilic adenomas produced ACTH, that eosinophilic adenomas produced growth hormone and that chromophobe adenomas produced no hormone at all.
Hormone Secretion or Hypopituitaryism Caused by Compression

Primary Tumors Arising from Coverings of the Brain, from Peripheral Nerve, from Blood Vessels, or from Blood Cells
Meningioma Approximately 15% of all intracranial
neoplasms. Greatest incidence in middle age and in
women. However, they occur at all ages and are common in men.
Almost always benign and slow growing, though aggressive examples are sometimes encountered. Malignant transformation occurs very rarely.

Meningiomas
Majority arise from arachnoidal cells in the dura mater, particularly in areas adjacent to the sagittal sinus, Sylvian fissure, and bony ridges of the base of the skull
Compete with Schwannomas as the most common tumor of the spinal canal. Others may sometimes arise in the leptomeninges and the ventricles.
On gross inspection, are well encapsulated. They tend to push into, but not invade the brain (image below, arrow) and frequently, they can be excised.

Meningiomas

Primary Tumors
Neurilemomas (Neurinoma, Schwannoma)
A Slow Growing, Benign Tumor of Mesodermal Origin
About 7% of all intracranial neoplasms
Like meningiomas, they have their highest incidence in middle age and in women.
Rarely malignant. Usually on CN VIII (Acoustic
Neurinoma) Tinnitus, Hearing Loss,
Vertigo, CN V and VII Signs, and Finally, As It Fills the Cerebellopontine Angle, Cerebellar Signs Develop.

False Neuromas
There Are Two Types of Nerve Tumors: True Neuromas
These Are Very Rare and Are Composed of Actual Nerve Tissue. They Are Associated With the Sympathetic System, and Often Multiple.
False Neuromas Arise From the Connective Tissue of the Nerve Trunk. Often in Multiple Numbers Along the Spinal Nerves. Examples Include, Neurofibromatosis and Plexiform Neuromas.
These peripheral nerve tumors resemble Schwannomas and are differentiated from the latter by histological criteria that are not always distinct.

Primary Tumors
During embryogenesis, epithelial and mesodermal tissues can be trapped inside the skull and spinal canal. These tissues, along with residual embryonal tissues that have failed to differentiate, may all give rise to tumors. As representatives of this group we will discuss craniopharyngiomas and chordomas. However, lipomas, dermoid cysts, epidermoid cysts, disgerminomas, teratomas and others are also encountered.

Primary Tumors
CRANIOPHARYNGIOMAS account for about 3% of all intraranial tumors.
They are most frequently seen in children and adolescents.
These tumors are suprasellar in location and it is thought that they arise from epithelial remnants of Rathke's pouch that are trapped in the stalk of the pituitary gland.

Primary Tumors - Craniopharyngioma
Grossly, the tumor appears partially solid and partially cystic and compresses the optic chiasm in front, the pituitary below, and the third ventricle above
Congenital Usually Detected by
Age 30 Male:female 3:2 Increase ICP

Primary Tumors: Hemangioblastoma About 1% of intracranial tumors often associated with von Hippel-Lindau disease, a
familial condition characterized by retinal angiomas, pancreatic cysts, and kidney tumors.
typically found in the cerebellum as a mural nodule within a cystic cavity whose appearance is much like that of the cystic cerebellar astrocytoma and can often be totally excised.
Many hemangioblastomas appear to cause polycythemia because of the presence of erythropoietin-like material in the cyst fluid.
Microscopically, numerous capillaries are seen coursing through a matrix of cells with foamy cytoplasm. This picture may closely resemble a renal cell carcinoma.

Primary Tumors: Hemangioblastoma Case
Clinical History: This is a 39 year old female who presents with severe headaches.
Findings: Image #1 is a contrast-enhanced axial CT of the head demonstrating an approximately 2 cm. ring enhancing lesion within the left cerebellum. There is significant associated edema with obliteration of the fourth ventricle.
Image #2 is a T2 weighted MR image of the head demonstrating an approximately 2 cm. region of increased signal within the left cerebellum with surrounding edematous changes.

Primary Tumors: Hemangioblastoma Case
Image #3 is a T1 weighted MR image in the same region demonstrating this lesion to be of low signal intensity on T1 weighted images.
Image #4 is a post Gadolinium enhanced T1 weighted sagittal image through the same region demonstrating this lesion to have a cystic center with irregular peripheral enhancement with more dense enhancement posteriorly near the pial surface.
Diagnosis: Hemangioblastoma.

Hemangioblastoma Discussion: Hemangioblastomas are rare, benign, generally solitary tumors of the
central nervous system most commonly identified within the posterior fossa. These lesions are most often found in the cerebellum, and although they may be solid, the majority are cystic. In addition, the majority of hemangioblastomas will demonstrate a densely enhancing peripheral nodule. In addition to the cerebellar hemispheres, the vermis and medulla are other potential sites of origin of hemangioblastomas. Between 4 and 20% of patients with hemangioblastomas of the cerebellum or spinal cord have von Hippel-Lindau disease. Histologically, these tumors are characterized by a fine hypervascularity mesh in a stroma of polygonal cells without evidence for mitotic activity. These lesions are always superficial in location most often located within the periphery of the cerebellar hemisphere. The nidus of the tumor always abuts the pial surface. The vascular supply to a hemangioma is derived from the pia. The characteristic radiologic findings of a hemangioblastoma on both CT and MR include a peripherally located cerebellar lesion with central cystic region with peripheral enhancing nodule. The signal intensity of the cystic portion of the hemangioma may be brighter than that of cerebral spinal fluid. In summary, the findings of a peripheral cystic structure with bright signal intensity on T2 weighted images located within the posterior fossa with an associated densely enhancing mural nodule is virtually pathognomonic for hemangioblastoma.
References: Lee Seung. Posterior Fossa Hemangioblastomas: MR Imaging. Radiology 1989;171:463-468.
Osborn Anne. Diagnostic Neuroradiology. Mosby, St. Louis. 1994. Submitted by:
Vincent Keiser, M.D.Charles Lanzieri, M.D.

Hemangioblastoma Summary
Usually Cerebellar Vermis or Cord Syrinx 30-40 Yrs. Males With Cysts and Tumors of Liver, Pancreas and
Kidneys Is Termed Lindau’s Syndrome - With Additional Retinal Angioma = Von-hipple-lindau Syndrome

Lymphoma
These tumors of the CNS are identical with lymphomas elsewhere. These tumors include large- and small-celled varieties (principally of B cell type), Hodgkin's disease, and multiple myeloma, etc. The latter is largely confined to the dura mater and bony coverings of the CNS. Newer classifications and nomenclature for lymphomas are constantly emerging.
Lymphomas may arise as primary CNS tumors, but are more frequently seen in association with lymphomas elsewhere in the body, unless the patient is immunosuppressed. Primary (and secondary) CNS lymphomas are being seen with increasing frequency as a result of immunosuppression for organ transplantation and the current AIDS epidemic.
If primary, they tend to be within the substance of the brain, and if secondary, the spinal canal is more frequently involved. Here, the tumors usually present as epidural masses which arise from the vertebrae. However, intracranial vascular and meningeal involvement is also common in secondary lymphomas and this may be accompanied by mild infiltration of the brain parenchyma.

Primary Tumors: Colloid Cysts of the 3rd Ventricle
A rare, congenital tumor formerly thought to be related to ependymoma or choroid plexus is the colloid cyst of the third ventricle.
Electronmicroscopy has shown that in some specimens the cyst lining most closely resembles bronchial mucosa which suggests a derivation from displaced bronchial cleft tissue.
In any case , this benign tumor can kill if it obstructs the foramina through which CSF passes from lateral to third ventricle. This will suddenly raise intracranial pressure causing severe headache and possible death.
Since the tumor is often on a stalk, it may intermittently obstruct the passage of CSF, depending upon the exposition of the patients head. Therefore positional, severe headache is an important clue to this potentially life threatening but curable condition.

Primary Tumors
Dermoid & Epidermoid Cysts (Pearly Tumors)

Primary Tumors
Chordoma (Notochord) Although, chordoma may appear anywhere in the spinal
column, it's more likely to appear at the ends of the spine at the occipital cervical junction or in the sacrococcygeal region.
Chordoma is rare. Sacrococcygeal chordoma appears more often in males and usually develops during middle ages, but can develop any time.
Although imaging studies such as x-rays and MRIs may be suspicious, the diagnosis of chordoma is established by biopsy of the tumor.
Treatment is surgical resection of the tumor. The overall prognosis for the tumor depends on the size, extent of skeletal involvement, and other factor
30-70 Yrs. 2:1 Males

Primary Tumors
Sacrococcygeal or Clivus Arachnoid Cysts
CSF Cysts in Arachnoid Space Common in Infants or Young Child May Be Bulging

Metastatic Neoplasms
Usually Carcinomas Spread From the Lungs or Breast, Less Frequently From the Thyroid or Gastrointestinal System. Metastasis to the CNS Comprises Only 20% of All Intracranial Masses. Metastasis to the Vertebra (Osteoblastic or Osteolytic) Is Much More Common Due to the Increased Venous Vascularity. 20% of All Intracranial Neoplasms Most Common From Lung (35%), Breast (20%), Melanomatous
(10%), Gastrointestinal (10%), Kidney (5%) Genitourinary and Endocrine
40-70 Yrs. Usually Through Arterial System Usually Middle Cerebral Artery

Metastatic Disease
The spine and it surrounding elements have a generous blood supply, draining many of the structures of the lower abdominal cavity via a system of veins called Batson's Plexus. This venous plexus is felt to be the reason that certain intra-abdominal and pelvic tumors have a tendency to spread to the spine.
The spread or metastasis of tumors from elsewhere in the body to the spine may occur after a cancer has been growing in another part of the body for a long time. Tumors that have spread to the spine usually cause a significant amount of pain. If they are large enough, they may put pressure on the spinal cord, which causes increasing pain and loss of normal functioning in the bowel, bladder, and legs.
Metastatic cancer may not be curable, but the treatment goals are usually directed at relief from pain, decompression of the neural elements (removing the pressure on the spinal cord and nerves), and preserving the patient's quality of life as much as possible. Surgery, chemotherapy, and localized radiation therapy all play a role in reducing the pain associated with cancers that have spread to the spine from other sites.

Other Spinal Cancers
Myeloma is the most common primary malignant tumor of bone. It typically affects adults greater than 40 years of age. It tends to be generalized, involving multiple bones, but back pain and involvement of the spine is the most common presenting complaint. Treatment is palliative; meaning that disease can be controlled, but not completely cured. Chemotherapy is used to control the pain and slow the progression of the disease. Surgery may be required if pathological fractures develop or there is compression of the spinal cord.

Other Spinal Cancers
Osteosarcoma is the second most common primary malignant tumor of bone. There are two age groups that can often develop this type of cancer. It typically affects adolescents and young adults, with a second peak of incidence in older adults. It is very rare in the spine. Modern advances in imaging, chemotherapy, and surgical treatment of osteosarcomas have significantly improved the 5-year survival to greater than 80 percent. This is an amazing accomplishment, since 20 years ago, this disease was almost always fatal.

Other Spinal Cancers
Leukemia: Leukemia, in its many forms, may present with back pain, which can be caused by the cancer growing in the bone marrow of the vertebral body. However, the more common symptoms of leukemia, such as fevers, fatigue, easy bruiseability, excessive bleeding and anemia are usually noticed well before back pain occurs.

Meningeal Carcinomatosis
Least Common Usually Breast or Lung Carcinoma

Spinal Canal Tumors
Tumors of the spinal cord, like tumors of the brain are both benign and malignant in nature and their growth similar to brain tumors will cause symptoms and signs in the level at which the nerve tissue is compressed.

Cord Tumors
Cord tumors can be extramedullary or outside the cord but within the neural canal. schwannoma or nerve sheath tumors will grow along the
openings of the neural canal where the nerve roots exits. Surgery for all tumors involving the spinal cord are
difficult due to the potential injury to the nerves and possible resulting nerve injury or paralysis.
In some cases of malignant tumors a needle biopsy can be done and radiation or other treatments can be started.
Tumors of the spine can often press on to the spinal cord and require surgical decompression. This type surgery will then often require spinal fusion to reconstruct the spine.

Vertebral Canal
May Be Benign or Malignant. Spinal Canal Tumors Are Usually Classified As:
Extradural (Outside the Meninges) Intradural (Inside the Meninges).
Extramedullary (Not Intrinsically Involving the Spinal Cord) (Intramedullary (Intrinsically Involving the Spinal Cord).

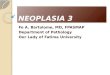
Spinal Canal Tumors
This picture shows a intramedullary tumor or tumor within the cord itself

Spinal Canal Tumors
All but Intramedullary Tumors Have the Same Features of Root Involvement and Positive Intrathecal Signs. Compression Causes Radicular Pain As Well As Loss of Neurologic Function Below the Level of the Lesion, Including Progressive Spastic Paraparesis, Paresthesias, and Bladder And/or Bowel Involvement. With Intramedullary Tumors, Sensation Is Lost Early (Especially Pain and Temperature), and Intrathecal Tests Are Often Negative.

Spinal Canal Tumors
Extradural Carcinomas and Sarcomas From Metastasis or Adjacent
Vertebrae; As Well As Lipomas, Fibromas, Neurinomas, Chondromas, Angiomas and Hematomas Also Occur.
Intradural Extramedullary
Usually Benign Tumors Arising From the Pia or Arachnoid Mater, or From Nerve Root Sheaths. Neurinomas, Meningiomas and Rarely, Sarcomas Have Been Described.
Intramedullary Ependymomas Commonly, Hemangiomas and Lipomas Rarely.

Spinal Canal Tumors
NOTE: Bilateral or Unilateral Radicular Pain at the Site of the Lesion And/or Paresthesias Are Common Findings.
Intrathecal Tests Are Usually Positive. Check Associated Cord Function BELOW the Level of the Lesion.
Check Carefully for Signs of Bowel or Especially Bladder Dysfunction
(Incontinence, Dribbling, Ect.,)

Treatment
Surgery: Surgical removal of brain tumors is generally recommended for most types of brain tumors. The location and size determines both the pre-operative and post-operative symptoms associated with the tumor and the resection. Surgery should be as complete as possible but neurologic function should be preserved. Diagnosis by Stereotaxic biopsy can be used for lesions that are difficult to reach and resect.
Other Treatments: Radiation therapy has a major role in the treatment of most tumor types and
can increase the cure rate or prolong disease-free survival. Chemotherapy may prolong survival in some tumor types. Gliadel wafers (TM) are sometimes used to apply chemotherapy directly to the resected tumor bed.
Wholistic: Diet, nutritional supplementation (vitamins, minerals, herbs, Homeopathic, etc.), exercise, manual therapies, Meridian Therapy, acupuncture, spiritual.
Relative contraindication to local manual manipulation. Other treatments include radiosensitizers, hyperthermia, or interstitial
brachytherapy used in conjunction with external-beam radiation therapy.