Embed Size (px)
Citation preview

CNS UPDATE 2: DIFFUSE GLIOMAS AND PA
Arie Perry, M.D. Director, Neuropathology

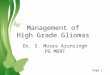
Distribution of Childhood Primary Brain and CNS Tumors by Histology and Age (Ages 0-14) (N = 15,398), CBTRUS Statistical Report: NPCR and SEER, 2006-2010.
Ostrom Q T et al. Neuro Oncol 2013;15:ii1-ii56
© The Centers for Disease Control and Prevention. Published by Oxford University Press on behalf of the Society for Neuro-Oncology in cooperation with the Central Brain Tumor Registry 2013.

• Disease entities should be defined as narrowly as
possible in order to establish highly biologically
uniform groups (i.e., as previously undertaken by
the hematopathology community)
• Molecular information will be incorporated into the
definitions of some diagnostic entities
• For some diagnostic entities, histology will remain
the basis for definition and diagnosis
ISN-Haarlem conclusions (1)

• Grade will reflect natural history and will be
based on histological findings; for some
diagnoses, avoiding a histological grade may be
preferable
• Some pediatric tumor types will require the
creation of entities independent of their adult
histological “look-alikes”
1. ‘Pediatric GBM’
2. ‘Pediatric oligodendroglioma’
ISN-Haarlem conclusions (2)

School of Medicine
ASTROCYTOMAS
• Diffuse
– Fibrillary
– Gemistocytic
– Giant Cell
– Small Cell
– Granular Cell
– Others
• Circumscribed / Favorable
– Pilocytic
– PXA
– SEGA
– DIA

School of Medicine
DIFFUSE ASTROCYTOMAS

School of Medicine
DIFFUSE ASTROCYTOMA GRADING
Atypia
Mitoses
Endothelial Proliferation (MVP, EH)
Necrosis
WHO II=A; III=A+M; IV=A+M+(E or N)

School of Medicine
ASTROCYTOMA (WHO GRADE II)


School of Medicine
ANAPLASTIC ASTROCYTOMA, WHO III
School of Medicine
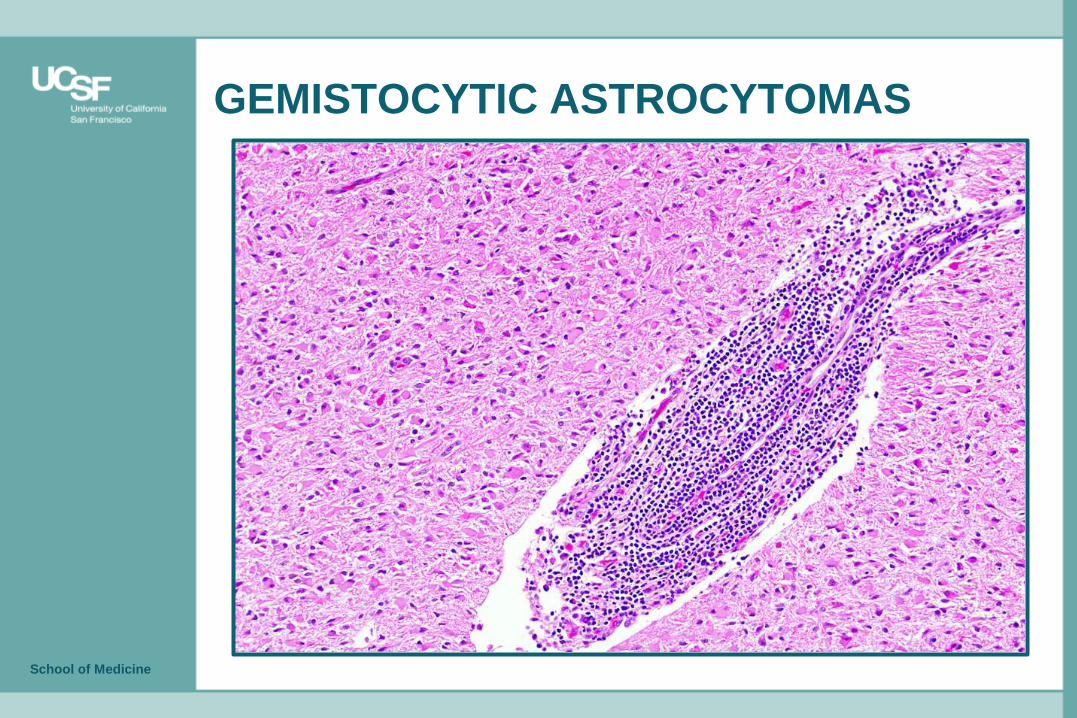
GEMISTOCYTIC ASTROCYTOMAS

p53

School of Medicine
GLIOBLASTOMA (GBM), WHO GRADE IV
• WHO dropped “multiforme” in 2000
• Rapid onset and progression
• Rim (or ring)-enhancing, but can be less clear in kids
• Survival ~1-year, but highly variable
• More often brainstem and thalamus in kids, but also cerebral hemispheres

School of Medicine
GBM, WHO IV

School of Medicine
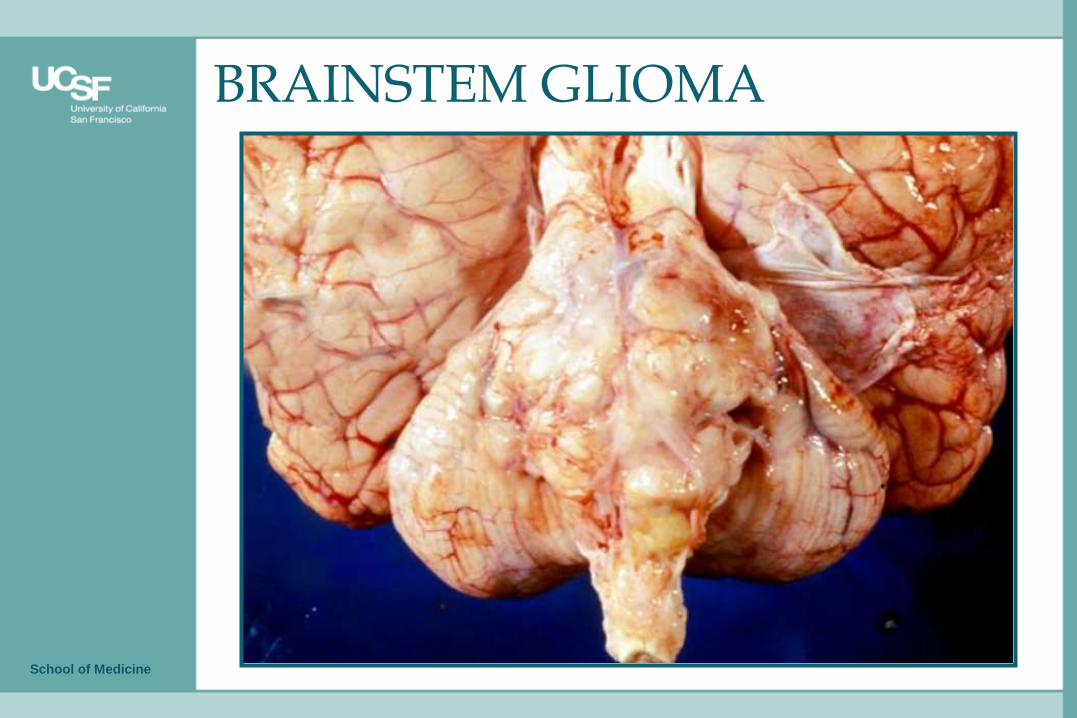
BRAINSTEM GLIOMA

School of Medicine
‘BRAINSTEM GLIOMA’
• Diffuse intrinsic pontine glioma (DIPG): malignant
• Dorsal, exophytic cervicomedullary astrocytoma (pilocytic)
• Focal tectal glioma (pilocytic)
• NF1-associated (pilocytic)




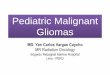
H3.3 K27M

Brain Pathology 23 (2013) 565-73

PDGFRα CEP4

IDH1R132H mutant GBM maybe further subdivided based
upon PDGFRA amplification
Log-rank test, p<0.05

Nat Genet 46: 462-466, 2014

School of Medicine
GBM VARIANTS / PATTERNS
• Fibrillary (Classic)
• Gemistocytic
• Giant Cell
• Gliosarcoma
• Adenoid / Epithelioid / Metaplastic
• Lipidized
• Inflammation-rich
• Granular Cell
• Small Cell
• GBM with an oligodendroglial component
• GBM with PNET-like foci
• Rhabdoid / Epithelioid

School of Medicine
GIANT CELL GBM

GFAP

School of Medicine
GIANT CELL GBM
19p13
19q14

School of Medicine
GIANT CELL GBM/GS
• ~1-5% of GBMs and gliosarcomas
• Clinical DDx: Meningioma, pleomorphic sarcoma, or metastasis
• Pathology DDx: PXA (EGBs; BRAF V600E)
• Less infiltrative
• Clinically a primary GBM, but younger patients, TP53 mutations common and EGFR-AMP rare; Mostly IDH1-R132H-neg
• Small subset with better prognosis
• May be overrepresented in Turcot disease

19: 81-90, 2009


GFAP
Neu-N SYN
NSE

p53 MIB-1

School of Medicine
GBM with PNET-like Features
PTEN DMBT1

School of Medicine
GBM with PNET-like Features
CEP2 N-myc



School of Medicine
GBM/GS WITH A PNET COMPONENT
• <1% of diffuse gliomas
• DDx: CNS PNET, lymphoma, metastatic small cell carcinoma
• Behaves locally like a GBM, but many develop CSF dissemination
• Can be either a primary or secondary GBM: PTEN-del in most cases, MYCN-AMP or MYCC-AMP in PNET-like area in >40%; IDH1-R132H in 16%
• Misdiagnosed CNS PNETs in kids?
AJSP 2010; 34:341-54
AJSP 2013; 37:658-98



SOX2 GFAP

BRAF-V600E

School of Medicine
RHABDOID/EPITHELIOID GBM
• Younger patients
• Superficial and circumscribed
• -22 in more rhabdoid cases?
• Focal INI1 loss?
• IDH1-neg
• BRAF V600E in more epithelioid cases
• Subset with better survival

Sturm et al.,
Cancer Cell
2012;22:425-437

School of Medicine
• Rare in kids (2-3% of gliomas)
• Oligo mimics more common: DNT, pilocytic astrocytoma, central neurocytoma, clear cell ependymoma
• Series with long followup rare since often transfer care as adults
• Same biology as adults?
• Genetics appear to be different
OLIGODENDROGLIOMA

School of Medicine
OLIGODENDROGLIOMA, WHO GRADE II

GFAP

GFAP

School of Medicine
ANAPLASTIC OLIGODENDROGLIOMA
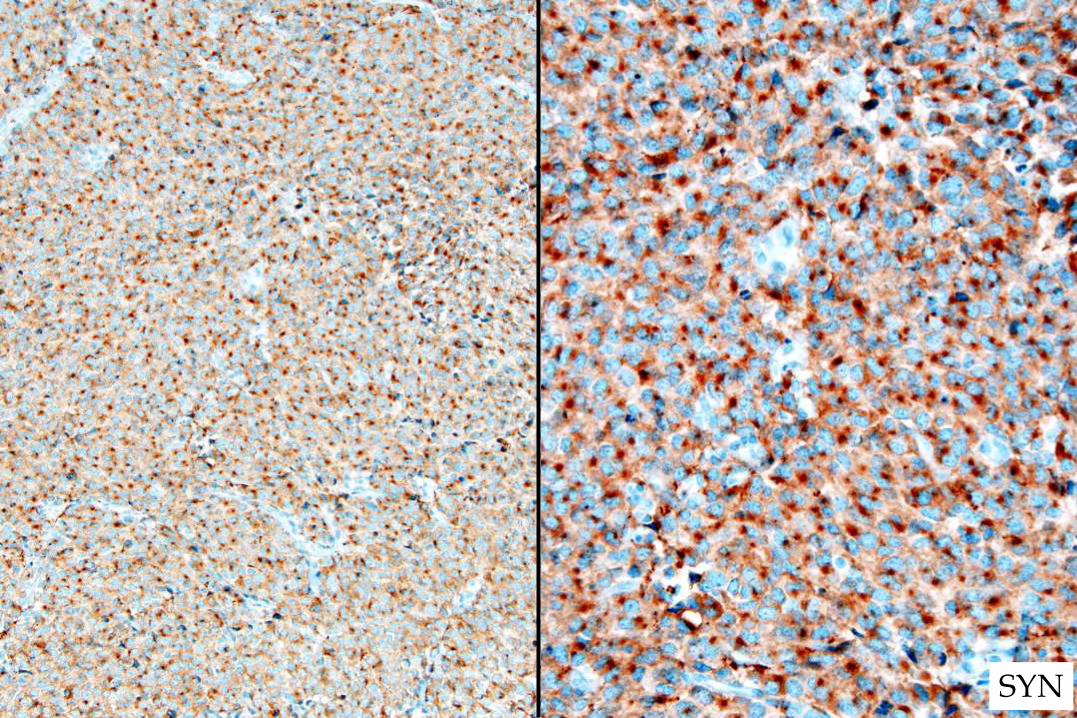
SYN

IDH1-R132H
ADULT TYPE OLIGODENDROGLIOMA

School of Medicine
1p32
1q42
19p13
19q13
ADULT TYPE OLIGODENDROGLIOMA


School of Medicine
Raghavan et al. JNEN 62:530, 2003

Oligodendroglioma phenotype
Astrocytoma phenotype
Glioblastoma phenotype
Diffuse glioma, indeterminate, “mixed” or ambiguous phenotype
Histologic
diagnosis
Grade II, III, IV, ungraded
IDH, ATRX, 1p/19q IDH, ATRX, 1p/19q
Grade II, III, IV, ungraded
1) Histology and molecular concordant: Diagnosis, grade, molecular findings
2) Indeterminate or mixed histology: Diagnose and grade based on molecular profile
3) Histology and molecular discordant: Diffuse glioma, histologic phenotype, molecular profile
4) Molecular testing not performed: Histologic diagnosis, NOS
Integrated Diagnosis
Molecular
information
Adult (some teenagers) Diffuse Glioma

ADULT TYPE ASTROCYTOMA
IDH1 p53 ATRX

Integrated diagnosis:
Oligodendroglioma, WHO grade II, IDH-
mut, 1p/19q codeleted
Histological classification:
Diffuse glioma, oligodendroglioma phenotype
WHO grade:
Grade II
Molecular information:
IDH-mut, 1p/19q codel, ATRX intact
Adult Type Oligodendroglioma

Histologic classification
Diffuse astrocytoma Oligodendroglioma “Oligoastrocytoma” or ambiguous
histology
IDH-mut, 1p/19q-
nondel, ATRX loss
Diffuse astrocytoma, ATRX loss of
expression
Diffuse glioma (oligodendroglioma
phenotype), 1p/19q non-deleted,
ATRX loss of expression
Diffuse astrocytoma, ATRX loss of
expression
info
rma
tio
n
IDH-mut, 1p/19q-codel,
ATRX intact
Diffuse glioma (astrocytoma phenotype),
1p/19q-codeleted
Oligodendroglioma, 1p/19q-
codeleted Oligodendroglioma, 1p/19q-codeleted
Mole
cula
r
IDH wild type Diffuse astrocytoma, IDH wild type* Diffuse glioma (oligodendroglioma
phenotype), IDH wild type Diffuse astrocytoma, IDH wild type*
Testing not performed Diffuse astrocytoma, NOS Oligodendroglioma, NOS “Diffuse glioma, NOS”

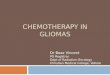
Pediatric AA/GBM
Primary GBM
Pilocytic astrocytoma
PXA
IDH1-mutated infiltrating adult gliomas
Diffuse astrocytoma Oligodendroglioma
Anaplastic astrocytoma,
GBM
Anaplastic oligodendroglioma
H3F3A, DAXX TP53, ATRX
EGFR, PDGFRA PTEN, TP53 CDKN2A/B, NF1 TERT promoter
BRAF
IDH1,2
TP53 ATRX
1p/19q CIC, FUBP1 TERT promoter
RB1,CDK4 CDKN2A, MDM2, PTEN
Neural
Progenitor
Cell
RB1,CDK4 CDKN2A
Courtesy of Dr. Dan Brat
PILOCYTIC ASTROCYTOMA
• Child / young adult
• Cerebellum, hypothalamus/3rd v., optic pathway, spinal cord
• NF1-associated OPG
• Insidious onset / slow growth
• Surgically “curable” (WHO I)
• 20-year survival = 80%

PILOCYTIC ASTROCYTOMA

PILOCYTIC ASTROCYTOMA






OPG-JPA


Nat Genet 45: 927-932, 2013
MAPK pathway

BRAF KIAA1549

LOWER-GRADE GLIOMA GENETICS
• BRAF-KIAA1549 duplication/fusion
– pilocytic astrocytomas (~70% in cerebellum; less in other locations)
– PMA (1/3rd to ½)
– MEK inhibitors?
• BRAF V600E mutation:
– PXA (~67%), GG (20-50%), DNET (20-30%), PA (~10%), GBM (5-10%)
– BRAF inhibitors, especially in recurrent or disseminated cases?
VIRTUALLY ‘ALL’ PEDIATRIC BRAIN TUMORS
Pediatric Neuro-Oncologist Pediatric Pathologist/Neuropathologist
Did you order BRAF testing? On this???
Really??


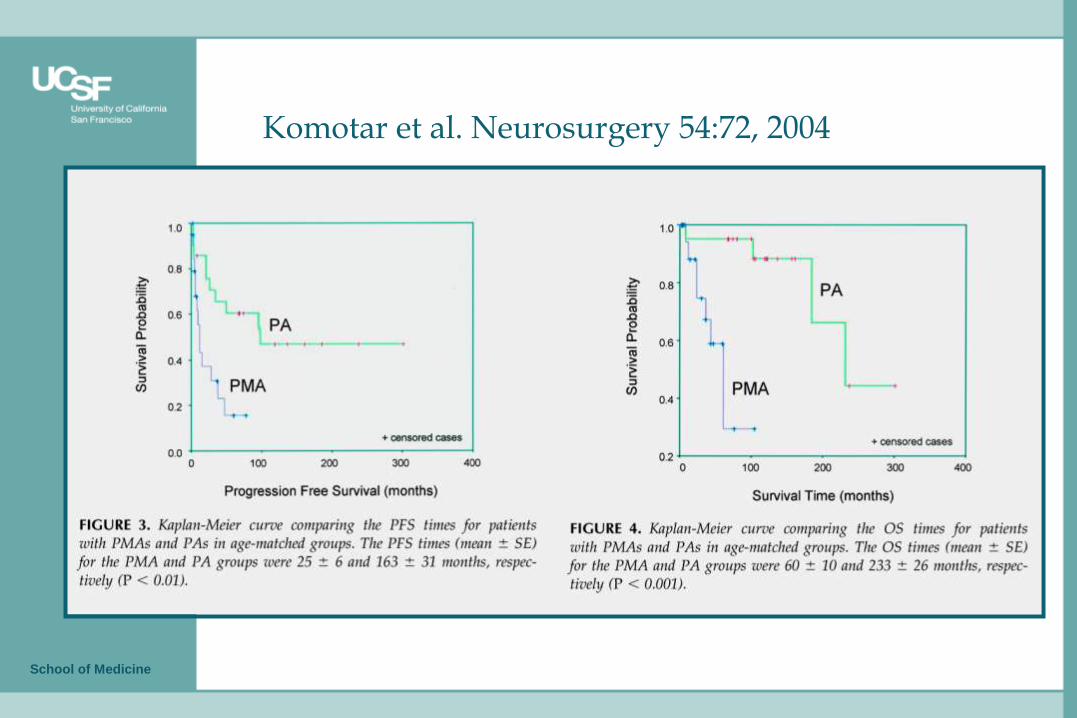
PILOMYXOID ASTROCYTOMA, WHO II

School of Medicine
Komotar et al. Neurosurgery 54:72, 2004


QUESTIONS?