Embed Size (px)
Citation preview
Cognitive-behavioral and attachment based family therapy for anxious children and adolescents
ADAA, March 2008Lynne Siqueland, Ph.D.
Children’s Center for OCD and AnxietyGuy Diamond, Ph.D.
Center for Family Intervention Science/CHOPUniversity of Pennsylvania Medical School
Interplay anxiety and adolescence
Adolescence is a time of recalibrating the balance of attachment and autonomy.
Anxiety complicates this normal process. Anxiety reinforces avoidance and dependency which
undermines the exploration of independence and competency
Parents to find balance between challenging and helping
Goals of ABFT for depression
Depression in adolescence is characterized by interpersonal problems in cohesion, responsiveness, criticism, conflict
• Once adolescents are able to express their attachment related feelings and demands in more directly and in a regulated manner, and parents respond in caring, respectful manner, this process can generalize to issues beyond the attachment relationship.
• Parents are then positioned to support, guide and protect their adolescents re: dating, peer relations, school, etc.
Role of family intervention
• Not necessary for all families- assess and address as relevant
• Other targets of treatment above symptom relief not always addressed by CBT but important for
development
• Interactional processes that impede CBT treatment
Cognitive-Behavioral Skills
1. Identify physical symptoms of anxiety and relaxation training
2. Identify and modify anxious or depressive self-talk- cognitive restructuring
3. Problem-solving vs. avoidance
4. Self evaluation and reward
5. In vivo practice with anxiety hierarchy
Education and engagement
• Explain what anxiety is (body’s alarm system backfiring)
• Give it a name, draw a picture of it
• Think about what you hate about it
• Think about what you want to be doing instead.
Chansky, T. Freeing your child from anxiety
Case conceptualization
• Presenting problem– Physiological symptoms– Mood– Behavior – Cognition– Interpersonal
Case conceptualization
• History and development
• Cultural context
• Cognitive structures and predispositions
• Behavioral antecedents and consequences
Session structure
• Mood or symptom check in
• Homework review
• Agenda setting
• Session content
• Homework assignment
• Eliciting feedback
Basic Techniques
• Relaxation training• Coping modeling• Role play• Contingent reward• Individualized
performance-based practice (in vivo exposure)
• Graduated sequence of tasks
• Repetition to mastery• Pleasant event
scheduling• Homework
Modifications for adolescents:cognitive formulation
• Be specific about cognitive formulation or model
• Review in first session with parents and adolescent.
• 3 components physical, cognitive and behavior
• Be clear about the reason for introduction of each skill with adolescent
Physiological reactions to anxiety and relaxation techniques
Identifying physical reactions
facial & bodily expressions- identification and errors
monitoring through daily log and observation
Techniques for relaxation
diaphragmatic breathing, calming counts
progressive muscle relaxation- personalize music or tape
visualization- candles, stairs, falling leaf
Strategies for identifying thoughts
• Daily diary and 3 column technique
• Cartoons, stories about other teens, imaginal exposure about things you tell yourself
• Cognitive replay- review of past situation
• Cognitive forecasting- imagining future events
• Offering hypotheses
• Down arrow technique- emotional significance- then what?
from Wilkes, Belsher, Rush, Frank & Assoc. Cognitive therapy for depressed adolescents
Situation Thought Feeling Action
Anxious and depressive thinking
Anxiety• Overestimate likelihood of bad outcome• Overestimate how terrible would be if happened• Focus on danger (safety, criticism, embarrassment)DepressedThink in self critical ways (worthless, helpless)See lives in negative ways and believe situations cannot
changeNegative view of future- always this way and never get
better
Anxiety Tricks
• Their first reaction self-talk is typically about the most awful thing instead of most likely that could happen in a situation
• Being in danger vs. feeling afraid• Always think twice- don’t trust 1st reaction-is that your final
answer• Feelings vs. facts• “what ifs” vs. “what elses”• Future vs. present
Chansky, T. Freeing your child from anxiety
Socratic dialogueGoal: to promote understanding of beliefs
1. Elicit & identify automatic thought
2. Tie automatic thought to feeling and behavior
3. Link thought-feel-beh sequence together with an empathic response
4. Obtain collaboration from child on 1-3 and agree to go forward
5. Socratically test the belief
Discussion of thinking errors1. Identification types of errors
2. Explore and label themes
(safety or threat, focus on self, evaluation by others)
3. Double standard technique
4. Pro-con evaluation
5. Contradictory evidence
6. Logical analysis- identify inconsistencies
7. Time projection- consequences of thoughts over timefrom Wilkes, Belsher, Rush, Frank & Assoc. Cognitive therapy for depressed adolescents
Cognitive challengesAre you expecting the worst? Or making it worse than it is
Are you sure this is really going to happen?- how likely?
Are you jumping to conclusions?- what is the evidence?
Are there other ways to look at the situation?
Is this thought helpful?
Can you expect to be perfect in everything you do?
How horrible would it be if the worst thing happened? Best outcome? Most likely outcome?
So what?
Challenging thought content
• Decatastrophizing
• Test of evidence
• Advantages/disadvantages
• Reattribution– Responsibility pie
Problem solving steps
1. Identify the problem
2. Brainstorm possible solutions or responses
3. Think about consequence of each response especially inappropriate response
4. Identify your goal
5. Evaluate and choose the best 1-2 solutions
6. Evaluate the results of solution
FEAR acronym
1. FFeeling frightened
2. EExpecting bad things to happen
3. AActions and ideas that will help
4. RResults and reward
Depression related interventions
• Pleasant activity scheduling
• Activation vs. withdrawal• Think can’t but can
• Improve mood
• Assertiveness
• Family conflict
Tolerating affect
• Surfing anxiety*• Learning to tolerate strong affect instead of fearing it• Don’t fight it• This is only a feeling• Identify what you are meant to be doing• Internal to external (interpersonal or grounding)*Chilled: The Cool Kids Anxiety and Depression Program Schnieing, Lyneham, Wignall
and Rapee (2006). Center for Emotional Health, Macquarie University Sydney, Australia.
Strategies into action
• Behavioral experiments- generate and test predictions
• Problem solving what can and cannot change
• Understand problem (who and what)
• How could I change the situation
• Change my reaction for what cannot change (teacher you hate)
Core beliefs
• Not trying fear of failure or disappointment• Letting people walk all over you• Not looking after yourself• Withdrawing from others or not trying to make friends• Not taking risks due to low self confidence• Giving up on things• Being too dependent or needy with others
• Chilled: The Cool Kids Anxiety and Depression Program Schnieing, Lyneham, Wignall and Rapee (2006). Center for Emotional Health, Macquarie University Sydney, Australia.
Two types of exposures
o Facing fears in a step by step fashion to test out the accuracy of thoughts and the ability to cope with possible anxiety experienced.
o The family also provides a context for expressing one’s views and feelings, dealing with conflict, negotiating relationships, and self assertion.
Social skills
Anxiety gets in the way of demonstrating good social skills or person under-estimates their skills
• reduce anxiety
• address perceptions and cognitionsAnxiety partly related to social skills deficits (trouble reading social cues, opportunities for practice)
• affective education
• role play, coaching, and progressive steps
Modifications CBT for adolescents
Often more resistant to homework- focus in session
Use language of choice
Distinguish personality style from anxiety
Discuss avoidance or “fake” quality of role play
Hierarchy established by adolescent more out of session
Focus on goals for independence in future
Modifications for adolescents: using the language of choice
• “right now you do not have a choice- in some ways you are controlled or limited by your way of thinking- consider alternatives so you have some control or choice in the matter.”
• “Would you like to be able to choose when you think about things rather than thinking or obsessing all the time? Try new way you can always go back to the old .”
• “You could make your own choices, to better define who you are, rather than be defined by anxiety”
Modifications for adolescents:language of choice
• “Alternative thoughts may be easier to both conjure up or hold on to when calm.”
• “Let’s figure out how to resolve this when you are calm. Right now we know who wins in the moment- the old familiar thoughts.”
• You can always keep the old way in back pocket. Instead you can experiment- notice the conflicts, as you challenge them you may be able to integrate more.
Modifications for adolescents:separating anxiety & personality
Be aware of not challenging the adolescent’s uniqueness unnecessarily
While it is helpful to normalize some feelings or experiences, many adolescents feel their situation, feelings and thoughts are different.
Therapist should tentatively offer alternatives and suggestions – what about, could it be, is it possible
Modification for adolescents: separating personality and anxiety
• “Challenging things is really interesting and is something that you enjoy but challenging is different from being stuck in the repetitive old patterns or concerns.”
• “Your personality is to care about other people and to value their opinion. This is one of your strengths- your personality is not to be anxious or self-conscious. Don’t want to change your sense of caring or sensitivity to others because these are positive qualities which you value. We want to address discomfort that holds you back or keeps you from your goals and interests”
Modifications for adolescents:avoidance of analysis
• Many adolescents are avoidant to the point of hesitancy to practice skills in session. Focus on how being unwilling to practice leaves you unprepared for situations which raises your anxiety. Role play as in vivo
• Avoidance sabotages the likelihood that it will go well.• Avoid anxiety by not wanting to review past
experiences. “It’s over, I don’t want to dwell on it. Now is time I feel fine and want to have fun. Again can’t learn from experiences
Modifications for adolescents: Homework compliance
Hesitant to commit thoughts to paper because it
• makes the thoughts seem “more real”
• worry about getting it right
• complain the task is too analytical compared to living in the moment
Can use diary format or tape recorder instead
Modifications for adolescents:Homework compliance
• Wilkes et al (1994) suggest making homework assignments brief and simple and then completing the rest in session.
• have adolescent jot down once each day situation, emotion and automatic thought
• therapist and adolescent in session, label the distortion and generate alternative thoughts.
Modifications for adolescents:Establishing in vivos
• Adolescent as an active collaborator and take the lead on setting manageable goals or steps.
• Adolescents are less motivated by rewards. • The adolescent may be even more hesitant about
doing an in vivo with the therapist • Most relevant in-vivos are naturally occurring
(being invited to a party, a trip to mall) or can be created (e.g. adolescent agrees to call a friend on the phone, chat with a classmate in homeroom).
Risk for disorder
Children of parents with an anxiety disorder are at risk. • 7 times more likely to have disorder than control• 2 times than depressed parents• emotional distress, poor social adjustment, anxiety
and fears• 65% of children (18-59 months) were behaviorally
inhibited & somatic problems - early precursors (Manassis et al., 1995)
Why add family based treatment?Why add family based treatment?
Risk for disorder
Children with anxiety disorders are likely to have parents who suffer with anxiety disorders
83% lifetime (40%)
57% current (20%)
Why add family based treatment?Why add family based treatment?
Observation of family interactionObservation of family interaction
Family Enhancement of Avoidant ResponsesFamily Enhancement of Avoidant ResponsesFEAR effect (Barrett et al., 1996)FEAR effect (Barrett et al., 1996)
Children with anxiety disorders• children and parents perceived more threat to
ambiguous situations • generated more avoidant responses • avoidant responses increased following discussion with
parents
Family treatment approaches
Barrett et al (1996) treatment involves teaching parents:
• To reward courageous and coping behavior• To extinguish excessive anxious behavior • Coping skills for their own anxiety• Communication and problem-solving skills
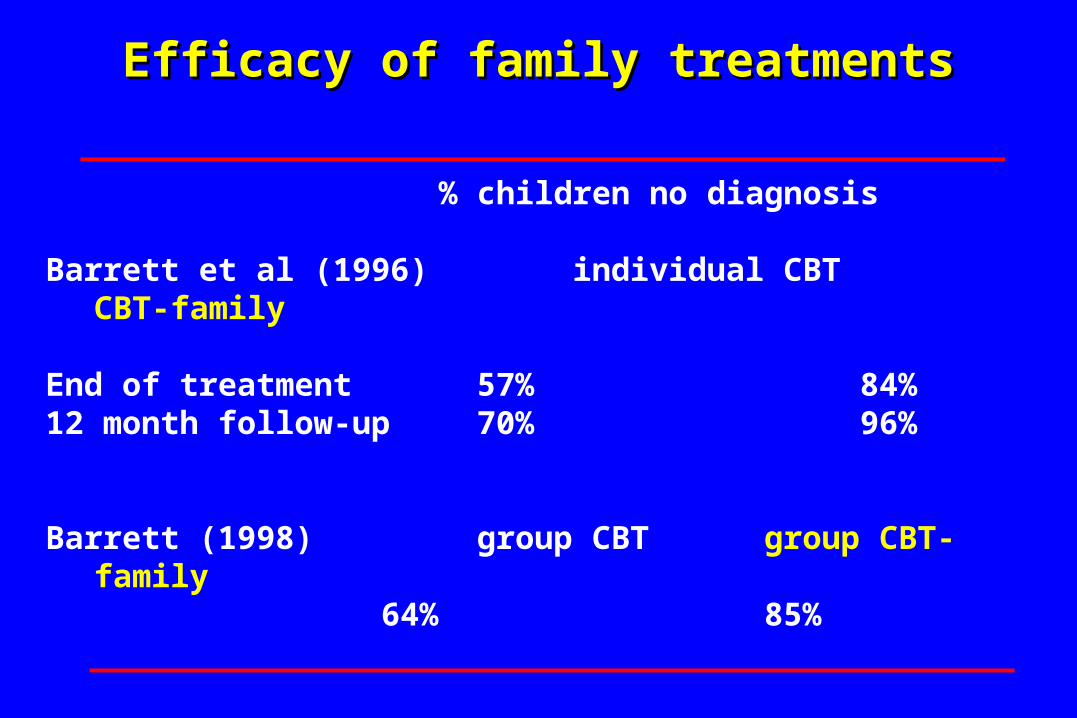
% children no diagnosis
Barrett et al (1996) individual CBT CBT-family
End of treatment 57% 84%12 month follow-up 70% 96%
Barrett (1998) group CBT group CBT-family
64% 85%
Efficacy of family treatmentsEfficacy of family treatments
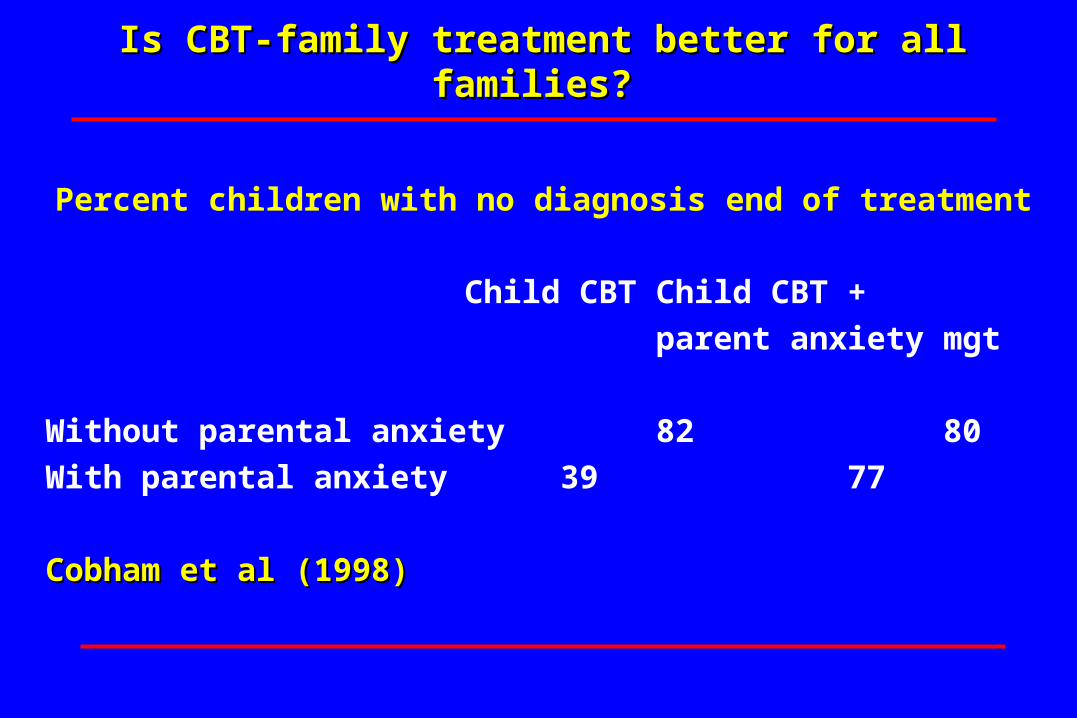
Is CBT-family treatment better for all families? Is CBT-family treatment better for all families?
Percent children with no diagnosis end of treatment
Child CBT Child CBT +
parent anxiety mgt
Without parental anxiety 82 80
With parental anxiety 39 77
Cobham et al (1998)Cobham et al (1998)
Psychological autonomyPsychological autonomy
• solicits child's opinion, not simply a reaffirmation of parents' opinion
• tolerates differences of opinion• acknowledges and demonstrates respect for
child's views• avoids judgmental or dismissive reactions to
child's views• encourages child to think independently • uses explanation and other inductive
techniques
Children with anxiety disorders and control families (Siqueland et al., 1996)
• Children reported less warmth or acceptance
• Rated by observers as less granting of autonomy
• No differences by parent report
Observation of family interactionObservation of family interaction
Treatment structure of CBT + family
Session 1 - parents & adolescent - focus on family interaction styleSession 2 - adolescent alone- alliance & goals Sessions 3- 6 alone with adolescentCognitive behavioral techniques (relaxation, cognitive restructuring & problem-solving)
Session 3-6- concurrent parents alone – beliefs, parenting & marital conflict
Sessions 8-16 adolescent, parents or conjoint- focus in vivo exposure & family interaction
Family targets of treatment
• Modeling anxious behavior
• Encouraging avoidance
• Modeling anxious interpretations of events
• Autonomy and competence
• Expression of conflict or differences
Attachment
Working internal models of self, world and particularly relationships
• Self as competent• Family as a secure base• Family as able to tolerate independent exploration• Family can tolerate potential conflict, independence and
affect• At adolescence, more often negotiated around goal
conflicts and through conversation (Kobak)
Family component
Assess and address as relevant1. helping parents to encourage adolescent's coping and mastery rather than allowing avoidance, taking over for, or directing.
2. modifying parents' expectations of adolescent's ability to function independently in academic, social and interpersonal arenas.
3. identify and discuss the role of parent's own anxiety or depressive symptoms may have on helping adolescent
Family component
4. encouraging increased tolerance for the expression of different viewpoints, feelings and experiences within the family, especially negative affect of anger and sadness
5. focus on problem-solving and open negotiation of conflict rather than avoidance
6. if marital conflict involves major differences in parenting- working with parents alone to negotiate a compromise position on managing anxious behavior
Family issues in adolescent depression
• Adolescent feels not listened or specifically criticized
• Adolescent feels not understood or accepted in own right
• Ongoing anger and unresolved conflict
• Past attachment rupture that has not been talked about or addressed.
Reattachment Task
• Adolescent disclosure of core conflicts
• Parental acknowledgement and respect
• Mutual responsibility and commitment to change
Reattachment: Expanded Model
• Therapist initiates• Adolescent anger/explore details • Adolescent vulnerable emotions• Adolescent attributional assessment• Parent confides own role• Adolescent ambivalence• Relational reframing• Forgiveness
Session 1 interventionsSession 1 interventions
• Ask each family member’s view of the problem-philosophy about the reason for anxiety
• Ask how each member feels and what each member does when child is anxious
• What works and what does not work• How does child feel about the parent’s reaction
Session 1 interventionsSession 1 interventions
• If it arises in session, can ask parent about their own anxiety or depression and how they cope or do not cope with it.
• Provide rationale for CBT and skills to be taught• Introduce dilemma for parents of knowing how much
to push and how much to help• At end of session try and summarize theme of family
interaction
Establishing goals for family treatment
• Parents balance helping and challenging
• To teach the adolescent to self soothe
• To develop the adolescent’s self & social competence
• Need for change for current development and future
Engaging families
• Join with parents about difficulty of parenting anxious child
• Normalize experience and discuss other families
• Be aware families are hesitant to admit difficulties or frustrations
• Identify impact of anxious child on family functioning
• Clarify should have same expectations of this child with modifications
Engaging parents
• Identify dilemma of accommodating to child and then getting angry
• Okay to want change for themselves
• Discuss child’s need for structure and consequences
• Check if family gives child independence or responsibility (chores)
Session alone Adolescent
• What do you want from and for your life?• What wishes and dreams do you have for yourself?• It’s time to take responsibility for where your life is
going. It’s okay to feel afraid• You need to show your parents how to do it or help• What gets in the way of you being independent?
Set individual and family oriented goals
Family targets
• Family beliefs
• Family behaviors
• Family interaction
Parent session
Ask parents beliefs about parenting:
• Match child’s emotional style and own
• What do you think good parent is?
• How do you decide how to parent?
• How were you (parent) parented?
• How does how you were parented affect how you parent your child?
Family of origin issues
• Own parents as good or bad model
• If parent was anxious as child, how did their parent help or hinder coping
• Legacy from parents about expression or management of emotions
• Elucidate message being sent by parent actions in present family
Parental fears
• Anxiety is threatening and to be avoided
• It is terrible to upset my child
• My child is too fragile to expect much or to push
• Expectation that parent has to fix situation
Various points of interventionVarious points of intervention
• first session – explanation of anxiety or family pattern identified
• parent session- parenting beliefs
• helping create new conversations/interactions
• “sabotage” of or no support of in-vivo exposure
• parental psychopathology
• marital conflict
Family targets for intervention
Family beliefs/behavior Technique
ideas of safety and threat awareness
encourage avoidance challenge
promote perfectionism cognitive restructuring
limit autonomy or difference indiv tx/ inter
limit expression of emotion enactment
Adolescent’s contributionAdolescent’s contribution
• Do you like that your parents take over for you?
• Do you like when your parent handle things for you so you don’t have to?
• Do you sometimes act as if you can’t do things for yourself when you can?
• I wonder if you could do it with a little help
• Do you want to be able to do it yourself?
Psychological autonomy
Concerns about autonomy are often concerns about expression of feelings
• Don’t upset your mother or father
• Going to be out of control- messy
• Going to dwell in it
• To ask for help, to be needy is weak
Psychological autonomy
Concerns about autonomy are often concerns about relationships
• expression of differences or conflict in the family will damage or lead to the loss of their intimate relationships
• open negotiation and communication is blocked • physical and psychological independence is perceived
as a threat to closeness
Parent-adolescent conversation
• Prepare adolescent- to tell parent what needs and does not need in a respectful way
• Prepare parent- to elicit input and listen
• Enactment of a different type of conversation and different kind of help
Autonomy and competence task• Encourage the adolescent to take the risk and express what he or
she wants or needs in terms of a change from parents. • Coach the adolescent to stand up for him or herself and not
acquiesce or sacrifice him or herself in order to protect their parents.
• Or if the adolescent is not ready to assert his or her independence more directly, we encourage the adolescent to share with the parents his or her fears or worries about independence
• The main shift for parents is to focus on a different kind of
parenting: from over protecting to promoting competency. We help parents give permission for autonomy and tolerate expressions of differences, conflict and independence.
Psychological autonomyPsychological autonomy
• Look for clinical examples in session or examples from home
• Model different way of interacting- ask adolescent first, validate their view
• Gently note and challenge examples of taking over
• Look at language used and give feedback about how might be perceived
• Or ask adolescent to help give feedback- hard to speak up or try
Psychological autonomy Problems arise during in vivos
• Parents may question adolescent’s motivation or ability
• May suggest concerns about danger, safety or failure
• Parent doesn’t find time or is unable to complete in vivo
• Parent may not be able to do in vivo because of own discomfort or adolescent’s
Defining helpDefining help
• Let adolescent ask for help
• Adolescent can define kind of help needed
• Different kind of help – adolescent coping CBT skills
• What do you think you could do or say that would help you feel calmer
Defining helpDefining help
• Therapist can help parents sit with adolescent in distress
• Wait until adolescent calms self
• Best help is not helping- faith in adolescent’s ability
• Make sure request not dropped or avoided
Parent psychopathologyParent psychopathology
Parent identifies with adolescent because of similar distress
Parent unable to reassure adolescent that world is safe
Parent feels overwhelmed by own anxiety- anxiety is too painful and to be avoided
Parent physically unable to do the in vivo because of own limitations- no model for adolescent
Parents issues dominate session or family life
Parent psychopathologyParent psychopathology
• Frame for parent what need to be able to do for adolescent
• Start from place may be able to overcome concern to help adolescent
• Therapist and spouse as support
• Evidence that parental difficulty impeding adolescent
Parent psychopathologyParent psychopathology
• Treatment for parent to help adolescent
• Treatment for parent for self because deserves less pain & better life
• Parent as model to adolescent of taking care of self and family
• Adolescent treatment as model for how treatment works and possible recovery
Marital conflictMarital conflict
• Need for an agreed upon way of managing anxiety that both can feel comfortable with
• Often one parent identifies with adolescent
• Discuss issues of polarization to compensate for other spouse
• Can have stronger parent take lead with other’s support
Marital conflictMarital conflict
• Need for parents to be united in goals and consequences
• Parents cannot agree on parenting because don’t agree on anything
• Difficulty compromising with spouse
• Adolescent and problem serves purpose of uniting couple or keeps parents apart