Embed Size (px)
Citation preview

212
Cognitive Behavioral Group Treatment for Physically Abused Children
Cynthia Cupi t Swenson, Medical University of South Carolina Elissa J. Brown, New York University Child Study Center
The purpose of this case study was twofold: to assess the feasibility of implementing a multiple-module, 16-week cognitive behavioral group treatment program for physicaUy abused children; and to evaluate preliminary data from this group treatment program de- signed to address the multiple sequelae common to school-aged physically abused children (i.e., aggression and other behavioral prob- lems, social shills deficits, and trauma-related symptoms). Results indicate that the multiple components of this group treatment pro- gram were implemented successfully and allowed for flexibility across children, even within a group format. Preliminary data show decreases on self-report measures of trauma-related emotional symptoms targeted by the group treatment. Increases were evident in par- ent ratings of children's internalizing and externalizing behaviors. Interpretations of these findings and future research recommenda- tions are discussed.
C HILD PHYSICAL ABUSE (CPA) has been defined as in- jury to a child by a parent or other caregiver after
intentional physical contact (Starr, Dubowitz, & Bush, 1990). National surveys reveal an incidence of approxi- mately 1% to 10% of children in the United States (e.g., Finkelhor & Dziuba-Leatherman, 1994; Gallup, 1995; Na- tional Center on Child Abuse and Neglect, 1996; Wolfner & Gelles, 1993). Regardless of their age at the time of the abuse, CPA victims may experience a variety of mental health problems throughout childhood, such as aggres- sion, social skills deficits, depression, and poor self- esteem (e.g., Finkelhor & Dzuiba-Leatherman; Kolko, 1992; Pelcovitz et al., 1994).
In their most recent survey, the National Center for Child Abuse and Neglect (1996) reported that children in their middle-childhood years (ages 6 to 14) have the greatest risk of experiencing CPA. School-aged CPA vic- tims commonly display several behavior problems, in- cluding aggression and other externalizing behaviors, so- cial skills deficits, and trauma-related symptoms. Parents and teachers consistently rate physically abused children as more oppositional, aggressive, and coercive with peers, siblings, and adults than nonabused agemates (e.g., Has- kett & Kistner, 1991; Kolko, 1992; Lahey, Conger, Atke- son, & Treiber, 1984; Lane & Davis, 1987; Prino & Peyrot, 1994). They are also less socially competent than their nonabused peers, initiating fewer positive interactions with peers and adults and avoiding peers more often than comparison children (Howes & Espinosa, 1985; Kaufman & Cicchetti, 1989; Prino & Peyrot).
Cognitive and Behavioral Practice 6, 2 1 2 - 2 2 0 , 1999 1077-7229/99/212-22051.00/0 Copyright © 2000 by Association for Advancement of Behavior Therapy. MI rights of reproduction in any form reserved.
Continuing Education Quiz located on p. 297.
With regard to trauma-specific symptoms, school-aged CPA victims experience various affective symptoms, such as general anxiety, depression, hopelessness, and low self- esteem (Kazdin, Moser, Colubus, & Bell, 1985; Kinard, 1982; Kolko, 1992). The rates of posttraumatic stress dis- order (PTSD) vary tremendously across studies, from 11% to 90% (Deblinger, McLeer, Atkins, Ralphe, & Foa, 1989; Famularo, Fenton, & Kinscherff, 1993; Kiser, Heston, Millsap, & Pruitt, 1991; Pelcovitz et al., 1994). Al- though studied less often, adjustment disorder is fre- quently associated with CPA (e.g., Brown, Swenson, & Kirk, 1996) as well.
Longitudinal studies indicate that the three clusters of symptoms (aggression, social skills deficits, and trauma- specific sequelae) may persist into adolescence and man- ifest in adulthood as violent and nonviolent criminal behaviors, substance abuse, self-injurious and suicidal be- haviors, anxiety and depression, interpersonal problems, and /o r academic and vocational difficulties (Malinosky- Rummell & Hansen, 1993; McCord, 1988). Although CPA victims may experience multiple, long-term conse- quences, most intervention efforts have focused almost exclusively on the abusing parent (Wolfe & Wekerle, 1993). Interventions aimed solely at parents may be help- ful in reducing parental risk for reabuse but fail to fully address the multifaceted symptoms of the child victim.
The small number of treatment-outcome studies for CPA victims and their families have typically been re- stricted to preschoolers and fall into two groups: either specific interventions that address only one area, such as social skills (Fantuzzo, Stovall, Schachtel, Goins, & Hall, 1987; Fantuzzo et al., 1988), or broad interventions focus- ing on cognitive and social development, such as day treatment programs (Culp, Little, Let ts ,& Lawrence, 1991; Culp, Richardson, & Heide, 1987; Gabel, Swanson, & Shindledecker, 1990). Although these studies indicate

Child Physical Abuse 213
some promise, limitations (e.g., absence of randomiza- tion to treatment condition, inclusion of victims of other forms of abuse and neglect) prevent generalizability of the findings to other samples of CPA victims (Oates & Bross, 1995).
In spite of the fact that they are an age group at high risk of CPA, only one randomized clinical trial has been conducted with school-aged victims. Kolko (1996) com- pared individual cognitive behavioral therapy (CBT) conducted with children and their parents (i.e., separate but parallel protocols), family therapy, and routine com- munity services. Both CBT and family therapy were asso- ciated with decreases in victims' externalizing and inter- nalizing behaviors and parent-to-child violence. Although trauma-specific approaches (e.g., safety planning, relax- ation training) were used only in the individual CBT with children, trauma-related symptoms decreased signifi- can@ across the treatment conditions.
Given the importance of peer relationships for school- aged children, social support for trauma victims, and cost efficiency in this managed-care era, group therapy may be a valuable approach to the treatment of CPA victims. A number of authors have argued that trauma-focused group treatment should be an effective method for ad- dressing the sequelae of child sexual abuse (Berliner & Ernst, 1984; Mandell et al., 1989; Steward, Farquahar, Glick, & Martin, 1986). The rationale is that group treat- ment provides the opportunity for education, correction of distortions, and positive interactions with peers who share similar experiences (Berliner & Ernst). In a metaanalytic review, Hoag and Burlingame (1997) found that group treatment is an effective method for children and adolescents, regardless of diagnosis. Uncontrolled studies on group treatment of sexually abused children have shown reductions in distress (Nelki & Watters, 1989) and fear and depression (Hoier & Inderbitzen-Pisaruk, 1989). However, this modality has not been evaluated for school-aged victims of CPA.
A number of cognitive behavioral techniques have em- pirical support for the type of problems CPA victims ex- perience. These techniques include anger and aggres- sion management (Feindler, Ecton, Kingsley, & Dubey, 1986; Goldstein, Sprafkin, Gershaw, & Klein, 1980; Loch- man, 1992; Lochman & Curry, 1986; Stern & Fodm, 1989), social skills training (Michelson, Sugai, Wood, & Kazdin, 1983; Michelson & Wood, 1980), and trauma- focused treatment (Deblinger & Herin, 1996; Deblinger, Lippman, & Steer, 1996; Deblinger, McLeer, & Henry, 1990; Stauffer & Deblinger, 1996). Many of these ap- proaches have been conducted in a group format with populations other than CPA victims.
The chief aim of this study was to develop a cognitive behavioral group treatment program for school-aged vic- tims of CPA, based on empirically validated techniques.
Further, this study aimed to assess the feasibility of imple- menting such a group and to present preliminary results from the application of this program.
Method
Participants Six children (four female and two male) were initially
enrolled in the cognitive behavioral group treatment (CBGT). Of the initial six participants, four children (completers) completed the entire 16-week program, one attended four sessions, and the other child attended eight sessions. The latter two children are considered partial participants. Parents and caregivers completed pre- and posttreatment measures on three of the group completers and two of the partial participants. Posttreat- ment measures were not obtained on the fourth com- pleter. Each child, except the group completer with miss- ing data, is described briefly below. Pseudonyms are used for each child participant.
Completers Samantha. Samantha, an 8-year-old Caucasian female,
was physically abused by her mother. The abuse consisted of being hit with objects, such as a belt or paddle, and punched with a fist, resulting in a black eye and bruises on her leg and arm. Samantha was placed with her grand- mother and maintained su- pervised visitation with her mother at the time of treat- ment. Samantha and her mother attended family treat- ment with another agency.
Randy. Randy, an 8-year- old Caucasian male, was phys- ically abused by his mother and an older brother. When she was angry, his mother hit him with objects, such as a short board, and his older sib- ling threw him against the wall, hitting and pinching him. The abuse left him with bruises and lacerations that
Interventions
aimed solely at parents may be helpful in reducing parental risk for reabuse but fail to fully address the multifaceted symptoms of the child victim.
required stitches. At the time of treatment, Randy was liv- ing with the family members who maltreated him. The family signed a safety plan with the child protection ser- vice agency agreeing to not use physical discipline and was attending family treatment at another agency.
Marva. Marva, a lO-year-old Caucasian female, was physically and verbally abused by her mother. The abuse consisted of being struck with objects, such as a belt, wooden spoon, and stick, and name calling. The abuse resulted in bruising to her legs, arms, and back. Marva

Z14 Swenson & Brown
lived with her mother at the time of treatment. The mother signed a safety plan with the child protection agency agreeing not to commit further physical abuse. Marva and her mother were enrolled in family treatment in another agency.
CBGT is o r g a n i z e d
in to t h r e e m o d u l e s :
t r a u m a - s p e c i f i c
w o r k ; a n g e r
m a n a g e m e n t ;
a n d soc i a l skil ls
t r a i n i n g .
Partial Participants Janie. Janie, a 12-year-old Caucasian female, was physi-
cally and sexually abused by her stepfather. The physical abuse consisted of being hit with his hand and objects, such as a belt buckle and extension cord. The stepfather was in prison due to burglary charges and Janie had no contact with him during group treatment. She attended four sessions of CBGT and then dropped out due to a change of foster care placement. Janie's family was not receiving treatment.
Evelyn. Evelyn, a 12-year-old Caucasian female, was physically abused by her father. The abuse consisted of being struck by a belt and other objects. She is consid-
ered a partial participant be- cause she missed sessions throughout the 16-week pro- gram, attending a total of eight sessions and receiving partial instruction in each module (i.e., orientation, three trauma-specific sessions, two anger-management sessions, two social skills sessions). Eve- lyn had regular supervised contact with her father but lived with another family mem-
ber during the first quarter of group. She attended four consecutive sessions prior to returning to live with her father. After her return to the father, which occurred dur- ing week 5 of CBGT, she attended four additional ses- sions, albeit not consecutively. On those days, her case worker was instrumental in getting her to group. Al- though Evelyn's father had severe difficulties with sub- stance abuse, he was not in treatment at the time Evelyn attended group.
Procedure Group participants were recruited from county men-
tal health centers, child protective services, and a local child advocacy center. Therapists and caseworkers were notified about the program by an announcement mailed and faxed to local agencies. Inclusion criteria were (a) children between the ages of 8 and 12, and (b) physical abuse substantiated by a child protective services (CPS) agency. Prior to enrolling a child for group treatment, therapists obtained information from CPS and the par- ent or caregiver regarding specifics of the abuse. Cases were not included when CPS was unclear if the abuse had
occurred. Caregivers of all referred children were con- tacted by the group leaders, given a brief description of the program, and invited to complete an intake (i.e., pre- treatment) assessment. At the intake, CBGT was de- scribed to the caregiver and an informed consent was signed. The assessment included both child victims and their caregivers; however, children completed both the clinical interview and standardized self-report measures separately from their caregivers.
Assessment Measures Child behavior problems. The Child Behavior Checklist
(CBCL; Achenbach, 1991), completed by the caregiver, consists of 113 behavior-problem items and has strong va- lidity and reliability. Results are organized into three broad behavior problem scales: internalizing, externaliz- ing, and total behavior problems.
Trauma-related emotional symptoms. The Trauma Symp- tom Checklist-Children's Form (TSCC; Briere, 1996), completed by the child, consists of 54 items that assess six domains: anxiety, depression, anger, posttraumatic stress, dissociation, and sexual concerns or preoccupation. Reli- ability studies have found moderate to high internal con- sistency (.77 to .89) for the clinical scales. The Children's Depression Inventory (CDI; Kovaks, 1992) is comprised of 27 items that provide a global index of depression in youth ages 7 years to 17 years. The scale is completed by the child and has demonstrated strong reliability (Smucker, Craighead, Craighead, & Green, 1986).
Treatment Program CBGT involved 16 weekly, 1-hour sessions conducted
at an outpatient clinic that specializes in treatment of child and adult victims of traumatic events. Therapists were a doctoral-level, licensed psychologist and a pre- doctoral clinical psychology intern.
M1 sessions were based on a cognitive behavioral model and included interventions that have received em- pirical support with other populations (Berliner & Saun- ders, 1996; Deblinger & Herin, 1996; Deblinger et al., 1996; Feindler et al., 1986; Michelson et al., 1983; Michel- son & Wood, 1980). CBGT is organized into three mod- ules: trauma-specific work; anger management; and so- cial skills training. Modules were conducted in this order; however, specific skills were reviewed and practiced throughout the group. For example, problem solving was modeled and reinforced in each session. The format for each session is detailed in a treatment manual (Swenson, 1996). Below is a summary of the orientation session and subsequent treatment modules.
Orientation Prior to beginning Module 1, a brief orientation was
presented to group members. First, rules and confi- dentiality limits were discussed. Group members were

Child Physical Abuse 215
in fo rmed of the difference between private and secret.
This was impor t an t due to the secrecy that of ten accom-
panies abuse.
In g roup we will be talking abou t things that have h a p p e n e d to each of you. What we talk about here is private bu t no t a secret. [Leader asks if g roup
members know the difference.] If g roup were a secret, I can ' t tell and you can ' t tell what we do here. But that 's not how group works. Group is pri- vate. That means ne i the r you no r I can tell anyone
what o the r kids in g roup say. But you can tell any- one you want what our activity was or what you said. BUT, if anyone in g roup tells me you are th inking about hur t ing yourself or someone else or that someone has hu r t you, that informat ion will not be
kept private. Just r e m e m b e r that if you tell me about abuse of you that has a l ready been repor ted ,
I will not r epor t it again.
The above s ta tement reflects an effort to he lp chil-
d ren unde r s t and that they would no t have to go th rough ano the r forensic process for disclosing known mater ia l in
the group. Second, steps for p rob l em solving were p resen ted (see
Table 1) to be used in a weekly exercise known as "How Was Your Week?" This problem-solving structure was used at the beg inn ing of all subsequent groups to assist chil- d ren with conflicts and concerns that occur red dur ing
the pr io r week. Third, an overview of the group was p resen ted and
chi ldren were in fo rmed that their physical abuse ex- per ience(s) would be discussed in the group. As in all
subsequent sessions, the final activity was snack time. Group members were assigned tasks to work on toge ther (e.g., one holds cup, o the r pours drink) to foster pee r re- lations and group cohesion. Outside of the group, al- though all parents were a t t end ing family therapy at an- o the r agency, CBGT therapists were available to discuss specific issues with the parents and to communica te with the family therapist .
Module 1 (Trauma-Specific Work, Six Sessions) Module 1 focused on issues specific to physical abuse
and its emot iona l impact . First, CPA was def ined by group member s and all possible defini t ions though t of
Table 1 Problem Solving Steps
Step One: Step Two: Step Three: Step Four: Step Five:
What is the problem? What do I/we want? What are the solutions? (brainstorm, don't evaluate) What are the consequences of each solution? Pick one to try
by group members were listed on a large flip chart. Care
was taken to avoid placing any child in a loyalty conflict. The mal t rea t ing caregiver 's behavior was f ramed as "against the rules" ra ther than as a personal flaw.
Next, feelings all kids exper ience and then feelings kids exper ience about physical abuse were el ici ted and discussed. These were listed on a large flip char t and
group members had the oppor tun i ty to select which feelings they had exper ienced and which ones re la ted to
the abuse. This activity was helpful in demons t ra t ing sim- ilarities in chi ldren 's feelings in an a t t empt to normal ize feelings.
Affect regula t ion was then in t roduced using a meta- pho r of a television set with three "channels": thinking, feel- ing, and behavior. Using a paper model of three television
sets, r epresen t ing thinking, feeling, and doing, the poten- tial for changing the channe l
(i.e., changing thoughts, feel- ings, actions) was i l lustrated (Berl iner & Saunders, 1996).
Examples of conflict or upset- t ing scenarios were then elic-
i ted and used to identify the effects on others of changing the channe l (e.g., talking in- stead of f ighting might result
in less anger) . The television
Using a paper model of three television sets, representing thinking, feeling, and doing, the potential for changing the channel was illustrated.
exercise was used in subsequent sessions to show the rela-
t ionship among thinking, feeling, and behavior (e.g., if he changes the th inking channel from 'T l l kill them" to "I jus t need to let it go," his do ing will be different) .
The fourth task in Module 1 involved teaching anxiety and stress management . Cont ro l led b rea th ing and a vari- ety of re laxat ion skills were demons t ra ted and then the chi ldren pract iced each skill with their g roup peers. Each
group m e m b e r was asked to blow up a bal loon that repre- sented the stomach. They were asked to note that as air came into the bal loon it got b igger ("like your s tomach
does when you i n h a l e / b r e a t h in") and as air went out of the bal loon it got smaller ("like your s tomach does when
you e x h a l e / b r e a t h out"). This act ion was c o m p a r e d to the s tomach when cont ro l led b rea th ing is be ing used. To aid chi ldren in slowing the rate of inhal ing and exhaling, leaders slowly verbalized the phrase "bal loon out" for inhal ing and "balloon in" for exhaling. Chi ldren were in- s t ructed to inhale as the leader said "bal loon out" and ex- hale as the l eader said "bal loon in." After initial instruc- tion, group members prac t iced lying on a mat with a pape r cup on their s tomach, testing whether they could inhale slowly and make the cup rise and exhale slowly and make the cup go down.

116 Swenson & Brown
The final task in Module 1 involved exposure and ad- dressing any thinking errors regarding the abuse (e.g., self-blame). Using paints, string, and a paper bag, each child made a puppet of the person who abused him or her. In cases where there were multiple abusers, multiple puppets were made. Once the puppets were complete, each child had the opportunity to have the puppet tell
Each ch i ld m a d e a
p u p p e t o f t h e
p e r s o n w h o
a b u s e d h i m or her.
Each ch i ld h a d t h e
o p p o r t u n i t y t o
h a v e t h e p u p p e t
tell t h e s t o r y o f
w h a t h e o r s h e d i d
t o t h e ch i ld t h a t
w a s p h y s i c a l l y
a b u s i v e .
the story of what he or she did to the child that was physically abusive. Children were taught to apply coping skills, such as the controlled breathing, or cognitions to abuse-related anxiety (i.e., change the think- ing or doing channel). After the puppet told of his or her behavior, each group member expressed feelings about the abuse to the puppet. In this particular group, the expo- sure activities continued over three sessions. One child was unable to have her puppet tell about the abuse. As an alter- native, she selected a group member who spoke for the
puppet as the target child whispered instructions in her ear. Assistance from a peer enabled this child to get her story out in the open.
Module 2 (Anger Management, Five Sessions) The aim of Module 2 was for group members to exam-
ine how they manage anger, develop alternative manage- ment skills, and practice new skills. Initially, the group ad- dressed the issue of pride and violence. Managing anger was compared to fishing. Group members were asked to take the leaders through the process of fishing. The inter- action between the group leaders and members was simi- lar to the following:
First you take a pole and put bait on the hook. Then you throw the hook in the water. The fish comes along and nibbles at the hook and you jerk your pole up and hook the fish. How is this like anger? What happens when the fish takes the hook? What happens to you when you take the hook?
Leaders compared throwing out the hook to ver- bal provocation and taking the hook as losing con- trol, letting other kids get the best of you. Not taking the hook was recognized as winning, keep- ing your cool.
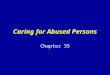
To determine types of events or verbalizations that provoke anger in group members, the "what makes me hookable" worksheet was used in session (see Figure 1).
WHAT MAKES ME HOOKABLE
I can't stand it when another student says to me:
I can't stand it when my parents say to me:
I can't stand it when my teacher says to me:
I can keep my cool until another person:
I usually get in a fight when the other person:
Figure 1. What Makes Me Hookable Worksheet
Next, using Feindler and colleagues' (1986) model as a guide, group members identified physiological and cog- nitive anger cues and then external anger cues, including provocative statements or actions by others. Group mem- bers were presented a worksheet labeled INSIDE CUES on the top half of the page and OUTSIDE CUES on the bottom half of the page and asked to develop lists for each. For example, for inside cues, group members listed physio- logical cues such as increased heartbeat, watering eyes, and cognitions, such as, "He's dissin' me and nobody disses me."
Coping skills, including relaxation, thought stopping, and cognitive substitution, were taught and practiced through role-play. Group members were prompted to substitute a coping skill for aggression at the first sign of anger (the physiological or cognitive cue).
Module 3 (Social Skills Training, Four Sessions) Throughout CBGT, therapists modeled appropriate
social skills and, through verbal praise, reinforced the children's use of appropriate social skills. Ongoing op- portunities were created to practice sharing, turn taking, and complimenting through buddy assignments, struc- tured group activities, and unstructured snack time. In a more structured format, Module 3 involved instruction in social skills such as assertiveness, managing derogatory statements from others, appropriate complaining, and managing complaints from others. These specific skills were modeled and practiced through games and role-

Child Physical Abuse 217
play. For example, in one game a group member was pre-
sented with a scenario. Three group members drew a card from a stack of cards. On the card was a description
of a possible reaction. Dyads of group members role-
played the scenario and each reaction. Then the entire
group had to determine which reaction would br ing
about the most favorable consequence. U p o n the com-
plet ion of social skills training, each child developed a so-
cial support and safety plan (Kolko, 1996). The strengths
and progress of each group member were then discussed
and chi ldren de te rmined how they would say good-bye to
their group peers.
R e s u l t s
I m p l e m e n t a t i o n
Each of the three modules was implemented success- fully across 16 weeks. No difficulties were evident with the
sequencing of the modules. The active pace and hands-
on activities engaged the chi ldren in instruction and
practice of skills. Engaging the parents by talking with
them before or after group seemed ins t rumental in the
children's regular at tendance. Children whose place-
men t changed dur ing the course of the group partially
completed the CBGT. For those children, barriers to par-
ticipation included the absence of transportation, new
caregiver's awareness that the child was enrol led in
group, and, caregiver's commi tmen t to the child's partic- ipation. Treatment was nei ther mandated by CPS for
these chi ldren nor required by other agencies/ individu- als involved with the family.
P r e l i m i n a r y D a t a
The pre- and post t reatment scores from caregiver- and
child-report measures for each group completer (n = 3)
are shown in Tables 2 and 3. At pretreatment , caregivers
reported subclinical internalizing and externalizing
behavior-problem scores; for each completer, the CBCL
scores increased over the course of the group.
On measures of trauma-related emotional symptoms
(Table 3), completers self-reported reductions on anger,
posttraumatic stress symptoms, fantasy dissociation, sex-
ual concerns, and sexual preoccupation. Two completers,
Samantha and Marva, experienced decreases in sexual
distress. Randy and Marva also reported reductions on
anxiety and depression. In fact, Randy's CDI score
dropped markedly. Samantha exhibited increases on
anxiety, depression, and dissociation.
The pre- and post t reatment measures for group par-
tial participants (n = 2) are shown in Tables 4 and 5. Par-
ent reports varied between the two children. For Janie,
internal izing and externalizing behavior problems in-
Table 2 Standard Scores for
Parent-Report Measures-Group Completers
Samantha Randy Marva
Scale Pre Post Pre Post Pre Post
CBCL internalizing 48 57 46 65 52 59 CBCL externalizing 53 60 48 60 50 58
Table 3 Standard Scores for
Child Self-Report Measures-Group Completers
Scale
Samantha Randy Marva
Pre Post Pre Post Pre Post
CDI TSCC
Anxiety 61 Depression 48 Anger 50 PTS 53 Dissociation 43 Overt dissoc. 40 Fantasy dissoc. 52 Sexual concerns 82 Preoccupation 81 Sexual distress 69
- - 59 47 47 47
69 47 ~35 59 ~35 55 43 -<35 67 -<35 44 48 37 51 -<35 49 41 38 47 ~35 45 54 -<35 51 ~35 48 54 37 54 37 42 52 43 47 37 62 50 42 67 52 73 54 43 50 43 43 44 44 78 6l
Table 4 Standard Scores for
Parent-Report Measures-Group Partial Participants
Janie Evelyn
Scale Pre Post Pre Post
CBCL internalizing 76 87 69 62 CBCL externalizing 74 80 79 69
Table 5 Standard Scores for
Child Self-Report Measures-Group Partial Participants
Janie Evelyn
Scale Pre Post Pre Post
CDI 68 85 56 49 TSCC
Anxiety 52 49 -<35 -<35 Depression 65 77 -<35 39 Anger 53 57 59 44 Posttraumatic stress 67 58 --<35 38 Dissociation 49 63 37 42 Overt dissoc. 48 62 40 48 Fantasy dissoc, 52 62 37 37
Sexual concerns 82 57 57 57 Sexual preoccupation 73 50 66 66 Sexual distress 78 61 43 43

218 Swenson & Brown
creased. Ratings by Evelyn's caregiver showed reductions in both types of problems. Results also varied on mea- sures of trauma-related emotional symptoms. Like Randy, Evelyn reported reductions in anger and CDI scores. Janie, who attended only four group sessions, reported a sharp increase in CDI score, as well as increases in TSCC depression, anger, and dissociation scales. She exhibited reductions on TSCC anxiety, posttraumatic stress, and sexual concerns.
Factors Related to Successful Implementation
The goal of the present case study was to examine the feasibility of implementing and evaluating a 16-week CBGT that addressed the multiple sequelae common to school-aged, physically abused children. We found that each of the modules was feasible, and the children re- sponded positively to the structure of the group and activ- ities. The main barriers to completion of the group were
Children, w h i l e
l i v ing w i t h a
m a l t r e a t i n g
caregiver, are able
to participate in treatment that directly addresses the abusive experiences and talk openly about the experience.
transportation and problems associated with change of placement. Regular commu- nication with the child's case worker is essential.
One important lesson learned from implementing this group treatment is that children, while living with a maltreating caregiver, are able to participate in treat- ment that directly addresses the abusive experiences and talk openly about the experi- ence. To facilitate acknowl- edgment and recapitulation of the abuse, therapists must work to avoid placing the
child in a loyalty conflict regarding the therapist's opin- ion of the abuse and the caregiver's behavior. The value of peer support in facilitating abuse disclosure also ap- peared to be valuable and, in one case, directly facilitated a child's participation in an exposure exercise.
Measuring Outcomes
Given the emphasis on showing that clients are bene- fiting from treatment, using pre- and posttreatment mea- sures is essential. When doing so, providers should use measures from multiple sources (e.g., caregiver, child, teacher) that relate to the focus and goals for treatment. Measuring outcomes from one source only may lead pro- riders to erroneously conclude that the client did or did not benefit from treatment.
In the current study, results from the pre-post assess-
ment indicate that children who completed the group showed reductions in the symptoms targeted in CBGT (e.g., anger, posttraumatic symptoms). The child who completed only four sessions evinced increases in depres- sion, anger, and dissociation and lower reductions on caregiver-reported behavior problems.
Although not in the clinical range, parent ratings of completers indicated increases in internalizing and ex- ternalizing behavior problems. This finding was surpris- ing, considering parents' anecdotal comments about their children's improvements; parents of all completers verbally reported that their children enjoyed the group, felt they made friends, and had shown positive improve- ments in their behavior. This discrepancy between verbal- and questionnaire-report may relate to a number of factors. Caregivers may have initially minimized their chil- dren's behavior problems and, as treatment progressed, may- have been more comfortable reporting the severity- of problems. Alternatively, the reduction in depressive symptomatology and increase in (adaptive) assertiveness may have been viewed negatively by the caregivers. The reduction in child-reported posttraumatic symptoms may have been manifested as improved mood and activity level and, thus, viewed as an increase in behavioral diffi- culties. Lastly, the children's improvements through the CBGT process may have had more impact on peer rela- tions than on caregiver-child relationships. Regardless of the specific explanation, given the inconsistent findings in the present study and the knowledge that physically abusive caregivers tend to view their children's behaviors in a negative light relative to nonabusive caregivers (Brad- ley & Peters, 1991), a critical modification to the extant treatment program would be to include caregivers as ac- tive members in parallel and /o r family treatment.
Future Directions
In light of the small sample size and methodological weaknesses (e.g., no random assignment, no control group, participants were all Caucasian), the current data can only be considered preliminary. We cannot deter- mine whether the positive self-report outcomes for group completers or negative parent-report outcomes are due to the group treatment or to other factors. Controlled re- search is needed to further assess the efficacy of CBGT with physically abused children. Adding caregivers, sib- lings, and other key family members to the child's treat- ment may be a more effective way to lower future risk for these children. Moreover, future research should include children from multiple ethnic and cultural backgrounds.
The current case study is the first to examine CBGT with physically abused children. We have demonstrated that the modules are feasible and the structured compo- nents of this group treatment program can be imple-

Child Physical Abuse 219
mented with flexibility to meet the needs of the child par- ticipants. The strength of this abuse-focused group treatment is that children can disclose abusive experi- ences, be supported by peers and adult leaders, and have the opportunity for normalization of thinking, feelings, and behaviors related to physical abuse.
R e f e r e n c e s
Achenbach, T. M. (1991). Manual of the child behavior checklist and 1991 profile. Burlington: University of Vermont.
Berliner, L., & Ernst, E. (1984). Group work with pre-adolescent sexual assault victims. In I. Stuart &J. Geer (Eds.), Victims ofsexualaggres- sion: Treatment of children, women, and men (pp. 105-126). New York: Van Nostrand Reinhold.
Berliner, L., & Saunders, B. E. (1996). Treating fear and anxiety in sex- ually abused children: Results of a controlled 2-year follow-up study. Child Maltreatment, 1, 294-309.
Bradley, E.J., & Peters, R. D. (1991 ). Physically abusive and nonabusive mothers' perceptions of parenting and child behavior. American Journal of Orthopsyehiatry, 61, 455-460.
Briere, J. (1996). Trauma symptom checklist for children professional man- ual. Odessa, FL: Psychological Assessment Resources.
Brown, E. J., Swenson, C. C., & Kirk, L. C. (1996,June). The impact of physical abuse on children. Poster presented at the annual meeting of the American Professional Society on the Abuse of Children, Chicago, IL.
Culp, R. E., Little, V, Letts, D., &Lawrence, H. (1991). Maltreated chil- dren's self-concept: Effects of a comprehensive treatment pro- gram. American Journal of Orthopsychiatry, 61, 114-121.
Culp, R. E., Richardson, M. T., & Heide, J. S. (1987). Differential devel- opmental progress of maltreated children in day treatment. National Association of Social Workers, 497-499.
Deblinger, E., & Heflin, A. H. (1996). Treating sexually abused children and their nonoffending parents: A cognitive behavioral approach. Thou- sand Oaks, CA: Sage.
Deblinger, E., Lippman, J., & Steer, R. (1996). Sexually abused chil- dren suffering postta-aumatic stress symptoms: Initial treatment outcome findings. Child Maltreatment, 1, 310-321.
Deblinger, E., McLeer, S. V., Atkins, M. S., Ralphe, D., & Foa, E. (1989). Post-tramnatic stress in sexually abused, physically abused, and nonabused children. Child Abuse and Neglect, 13, 403-408.
Deblinger, E., McLeer, S. V., & Henry, D. (1990). Cognitive behavioral treatment for sexually abused children suffering post-traumatic stress: Preliminary findings.Journal of the Ameriean Academy of Child and Adolescent Psychiatry, 29(5), 747-752.
Famularo, R., Fenton, T., & Kinscherff, R. (1993). Child maltreatment and the development of posttraumatic stress disorder. American Journal of the Diseases of Children, 147, 755-760.
Fantuzzo, J. W., Jurecic, L., Stovall, A., Hightower, A. D., Goins, C., & Schachtel, D. (1988). Effects of adult and peer social initiations on the social behavior of withdrawn, maltreated preschool chil- dren. Journal of Consulting and Clinical Psychology, 56, 34-39.
Fantuzzo, J. W., Stovall, A., Schachtel, D., Goins, C., & Hall, R. (1987). The effects of peer social initiations on the social behavior of with- drawn maltreated preschool children. Journal of Behavior Therapy and Experimental Psychiatry, 18(4), 357-363.
Feindler, E. L., Ecton, R. B., Kingsley, D., & Dubey, D. R. (1986). Group ange~control training for institutionalized psychiatric male ado- lescents. Behavior Therapy, 17, 109-123.
Finkelhor, D., & Dziuba-Leatherman, J. (1994). Children as victims of violence: A national survey. Pediatrics, 94, 413-420.
Gabel, S., Swanson, A. J., & Shindledecker, R. (1990). Aggressive chil- dren in a day treatment program: Changed outcome and possible explanations. Child Abuse & Neglect, 14, 515-523.
The Gallup Organization. (1995). GaUup nationwide poll. Washington, DC: U.S. Government Printing Office.
Goldstein, A. E, Sprafkin, R. E, Gershaw, N. J., & Klein, E (1980). Skill streaming the adolescent. Champaign, IL: Research Press Company.
Haskett, M. E., & Kismer, J. A. (1991). Social interactions and peer per- ceptions of young physically abused children. Child Development, 62, 979-990.
Hoag, M. J., & Burlingame, G. M. (1997). Evaluating the effectiveness of child and adolescent group treatment: A meta-analytic review. Joun*al of Clinical Child Psychology, 26, 234- 246.
Hoier, T., & Inderbitzen-Pisaruk, H. (1989). Shert-term cognitive-behav- ioral group treatment of victims of sexual abuse. Unpublished manu- script. West Virginia University, Morgantown.
Howes, C., & Espinosa, M. E (1985). The consequences of child abuse for the formation of relationships with peers. Child Abuse and Neglect, 9, 397-404.
Kaufman, J., & Cicchetti, D. (1989). Effects of mahreatment on school- age children's socioemotional development: Assessments in day- camp setting. DevelopmentalPsyehology, 25(4), 516-524.
Kazdin, A. E., Moser, J., Colubus, D., & Bell, R. (1985). Depressive symptoms among physically abused and psychiatrically disturbed children. Journal of Abnormal Psychology, 94(3), 298- 307.
Kinard, E. M. (1982). Experiencing child abuse: Effects on emotional adjustment. American Journal of Orthopsyehiatr); 52, 82-91.
Kiser, L. J., Heston, J., Millsap, E A., & Pruitt, D. B. (1991). Physical and sexual abuse in childhood: Relationship with post-traumatic stress disorder. Journal of the American Academy of Child and Adoles- cent Child Psyehiatry, 30, 776-783.
Kolko, D. J. (1992). Characteristics of child victims of physical vio- lence.Journal of Interpersonal Violence, 7, 244-276.
Kolko, D. J. (1996). Individual cognitive behavioral treatment and family therapy for physically abused children and their offending parents: A comparison of clinical outcomes. Child Maltreatment, 1, 322-342.
Kovaks, M. (1992). The Children's Depression Invento U. North Tonawanda, NY: Multihealth Systems.
Lahey, B. B., Conger, R. D., Atkeson, B. M., & Treiber, E A. (1984). Parenting behavior and emotional status of physically abusive mothers. Journal of Consulting and Clinical Psychology, 52, 1062- 1071.
Lane, T. W., & Davis, G. E. (1987). Child maltreatment and juvenile delinquency: Does a relationship exist? In J. D. Burchard & S. N. Burchard (Eds.), Prevention of delinquent behavior (pp. 122-138). Newbury Park, CA: Sage.
Lochman, J. E. (1992). Cognitive-behavioral intervention with aggres- sive boys: Three-year follow-up and preventive effects. Journal of Consulting and Clinical Psychology, 60, 426-432.
Lochman, J. E., & Curry, J. E (1986). Effects of social problem-solving training and self-instruction training with aggressive boys.Journal of Clinical Child Psychology, 15, 159-164.
Malinosky-Rummell, R., & Hansen, D. J. (1993). Long-term conse- quences of childhood physical abuse. Psychological Bulletin, 114, 68-79.
MandelI, J. G., Damon, L., Castaldo, E C., Tauber, E. S., Mortise, L., & Larsen, N. E (1989). Group treatment for sexually abused children. New York: Guilford Press.
McCord, J. (1988). Parental aggressiveness and physical punishment in long-term perspective. In G. T. Hotaling, D. Finkelhor, J. T. Kirkpatrick, & M. A. Straus (Eds.), Family abuse and its consequences (pp. 91-98). Newbury Park, CA: Sage.
Michelson, L., Sugai, D. E, Wood, R. E, & Kazdin, A. E. (1983). Social skills assessment and t~z~ining with children. New York: Plenum Press.
Michelson, L., & Wood, R. A. (1980). Social skills assessment and train- ing with children and adolescents. In M. Hersen, R. M. Eisler, & E Miller (Eds.), Progress in behavior modification (Vol. 9). New York: Academic Press.
National Center for Child Abuse and Neglect. (1996). Study findings: Study of national incidence and prevalence of child abuse and neglect. Washington, DC: U.S. Government Printing Office.
Nelki, J., &Watters, J. (1989). A group for sexually abused children: Unraveling the web. Child Abuse and Neglect, 13, 369-378.
Oates, R. K., & Bross, D. C. (1995). What have we learned about treat- ing child physical abuse? A literature review of the last decade. Child Abuse and Neglect, 19, 463-473.
Pelcovitz, D., Kaplan, S., Goldenberg, B., Mandel, E, Lehane, J., & Guarrera, J. (1994). Post-traumatic stress disorder in physically

220 Swenson & Brown
abused adolescents. Journal of American Academic Child and Adoles- cent Psychiatry, 33(3), 305-312.
Prino, C. T., & Peyrot, M. (1994). The effect of child physical abuse and neglect on aggressive, withdrawn, and prosocial behavior. Child Abuse and Neglect, 18, 871-884.
Smucker, M. R., Craighead, E., Craighead, L., & Green, B.J. (1986). Normative and reliability" data for the Children's Depression Inventory.Journal of Abnormal Child Psychology, 14, 25-39.
Start, R. H., Dubowitz, H., & Bush, B. A. (1990). The epidemiology of child maltreatment. In R. T. Ammerman & M. Hersen (Eds.), Chil- dren at risk: An evaluation of factors contributing to child abuse and neglect (pp. 23-53). NewYork: Plenum.
Stauffer, L. B., & Deblinger, E. (1996). Cognitive behavioral groups for nonoffending mothers and their young sexually abused children: A preliminary treatment outcome study. Child Maltreatment, 1, 65-76.
Stern, J. B., & Fodor, I. G. (1989). Anger control in children: A review of social skills and cognitive behavioral approaches to dealing with aggressive children. Child and Family Behavior Therapy, 11, 1-20.
Steward, M., Farquahar, L., Glick, D., & Martin, E (1986). Group ther- apy: A treatment of choice for young victims of child abuse. Inter- national Journal of Group Psychotherapy, 36, 261-271.
Swenson, C. C. (1996). Group treatmevtt for physically-abused children: Ther- apist's manual. Medical University of South Carolina, Charleston, SC.
Wolfe, D. A., & Wekerle, C. (1993). Treatment strategies for child phys- ical abuse and neglect: A critical progress report. Clinical Psychol- ogy Review, 13, 473-499.
Wolfner, G. D., & Gelles, R.J. (1993). A profile of violence toward chil- dren: A national study. ChildAbuse & Neglect, 17, 197-212.
The authors wish to thank C. Hope Cunningham for her assistance on this project.
Address correspondence to Cynthia Cupit Swenson, Ph.D., Family SmMces Research Center, Department of Psychiatry and Behavioral Sciences, Medical University of South Carolina, 67 President St., Suite CPP, EO. Box 250861, Charleston, SC 29425; e-mail: swensocc@musc. edu.
Received: November25, 1997 Accepted: June 10, 1998