Embed Size (px)
Citation preview

Cognitive-Behavioral Therapies,
Part II
PSYC 4500: Introduction to Clinical Psychology
Brett Deacon, Ph.D.
November 29, 2012

Questions for Herbert et al. (2000) response paper, due Tuesday 12/3
• 1. Why do think EMDR has become so popular among therapists?
• 2. What can be concluded about EMDR from the observation that component studies generally find that imagery without eye movements is as effective as standard EMDR?
• 3. Which one of the FiLCHeRS (essential features of science) do you find most troublesome about EMDR?

From Last Class
• CBT, theory and practice
• Behavior and cognitive modification techniques
• A →B →C model
• Albert Ellis with Gloria

REBT
• Video of Albert Ellis with Gloria
• Pay attention to A-B-C model, identifying, and disputing beliefs
• What’s it like to be a patient in REBT?
• What’s it like to be a therapist in REBT?
• A disclaimer about Albert Ellis

Basics of CBT
• Determine cognitive and behavioral factors that are contributing to the problem
• Develop cognitive and behavioral strategies to address them

Cognitive Techniques
• By definition, anxiety disorders involve fears that
are at least somewhat irrational
• Therapist teaches clients how to think
accurately about feared stimuli so they will only
be as afraid as the facts warrant
• Thinking is most useful when it is believable and leads to a more realistic appraisal of danger and the ability to cope with feared stimuli

Accurate vs. Positive Thinking
• Actual quote from a therapist in a patient’s
medical chart:• “The importance of cognitive interventions was also discussed. In this
regard, the patient was encouraged to develop a working list of positive
cognitions to draw upon when beginning to feel and think anxiously. She
cited initial examples of enjoying thinking about movies, spending time with
her mother, or being at home. She was encouraged to expand upon these
topics, including specifics, e.g. specific movie scenes, places in the home,
etc. The patient was encouraged to write down her list of alternative
cognitions and thoughts to keep with her, and to utilize and refer to when
feeling more anxious, e.g. at school.”
• Is this a helpful cognitive therapy technique?

CBT for Anxiety Disorders
• Basic clinical strategies in CBT for anxiety
• Education
• Cognitive modification techniques
• Behavior modification techniques: exposure and fading of safety behaviors
• Integrating these: “behavioral experiments”

Cognitive Techniques
• I know nothing bad will happen when I _____
(encounter feared stimuli), but…..
• “Head” vs. “gut”-level understanding
• Simply talking about probabilities of danger is not
as convincing as direct evidence from personal
experience
• Are cognitive techniques necessary?

Basic Methods of Conducting Exposure
• Systematic desensitization (SD):• Relaxation training• Constructing a fear hierarchy• Relaxing while imagining each step in the
hierarchy
• Why SD is rarely used anymore
• Graduated exposure in vivo (graduated real-life exposure)
• Flooding (ungraduated real-life exposure)

Types of Exposure
• In vivo exposure - confronting feared stimuli in the environment (situations and objects)
• Imaginal exposure - confronting feared mental stimuli such as thoughts, worries, and memories
• Interoceptive exposure - confronting feared body sensations
• Some examples will follow in video clips

Exposure Hierarchy for a Patient Afraid of Acquiring Cancer
Exposure Situation Estimated SUDS
Thinking about having a deadly disease 95
Reading articles/watching TV about deadly diseases 90
Touching objects in public restrooms 85
Riding crowded elevators with medical patients 75
Touching objects in emergency room waiting area 70
Smoking a cigarette 60
Handling pets 55
Running 50
Hyperventilation 50

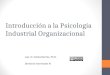
Exposure Hierarchy for a Patient Afraid of Negative Evaluation
Exposure Situation Estimated Anxiety
Ask a woman out on a date 95
Take dance lessons 95
Go to a bar 80
Online dating 50
Write letters/emails to friends/family 55
Work out in crowded gym 25
Committing social mishaps 20
Asking friends to get together 10

Exposure Hierarchy for a Patient Afraid of Panic-Related Body Sensations
Exposure Situation Estimated Anxiety
Hyperventilation 90
Breathing through a straw 85
Running in place 85
Shaking head from side to side 80
Spinning in chair 80
Swallowing rapidly 70

Exposure Therapy for Snake Phobia video clip
• http://www.youtube.com/watch?v=zKTpecooiec
• Look for educational, cognitive, and behavioral techniques
• What it’s like to be a therapist using this approach?
• What it’s like to be a patient in this therapy?
• Is it torture?

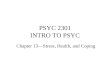
Pediatric OCD Treatment Study (POTS I):
Penn, Duke, & Brown
CBT +SER
n = 28
CBT
n = 28
SER
n = 28
PBO
n = 28
12 Week Treatment Phase
16 Week Follow-up Phase for Treatment Responders

0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
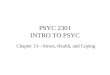
SER CBT COMB
Penn
Duke
Pediatric OCD Treatment Study Team (2004). JAMA
Site x Treatment Interaction

Psychotherapist Outcomes for CBT: Pre- and Post-TX CY-BOCS
0
5
10
15
20
25
30
35
40
1 6 5 3 7
Pre-Tx CY-BOCS
Post-TX CY-BOCS
Therapists account for 8.0% of variance within CBT, NS