Embed Size (px)
Citation preview
Patologia sistematica V
Gastroenterologia Prof. Stefano Fiorucci
Harrison’s Principles of Internal Medicine – 18° Ed. 2012
Colon polyps
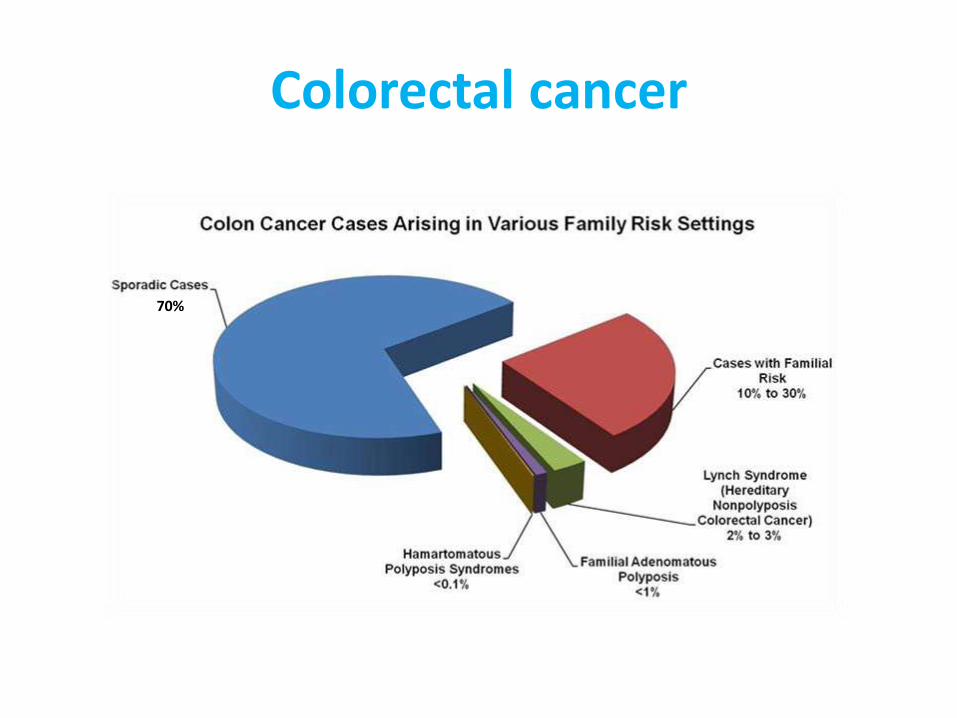
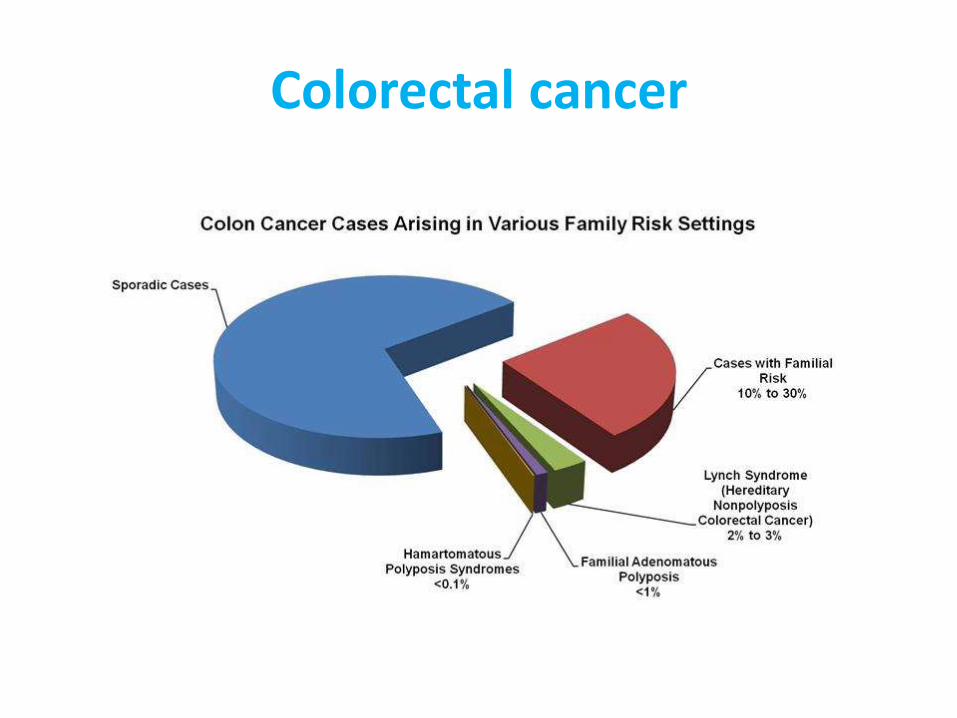
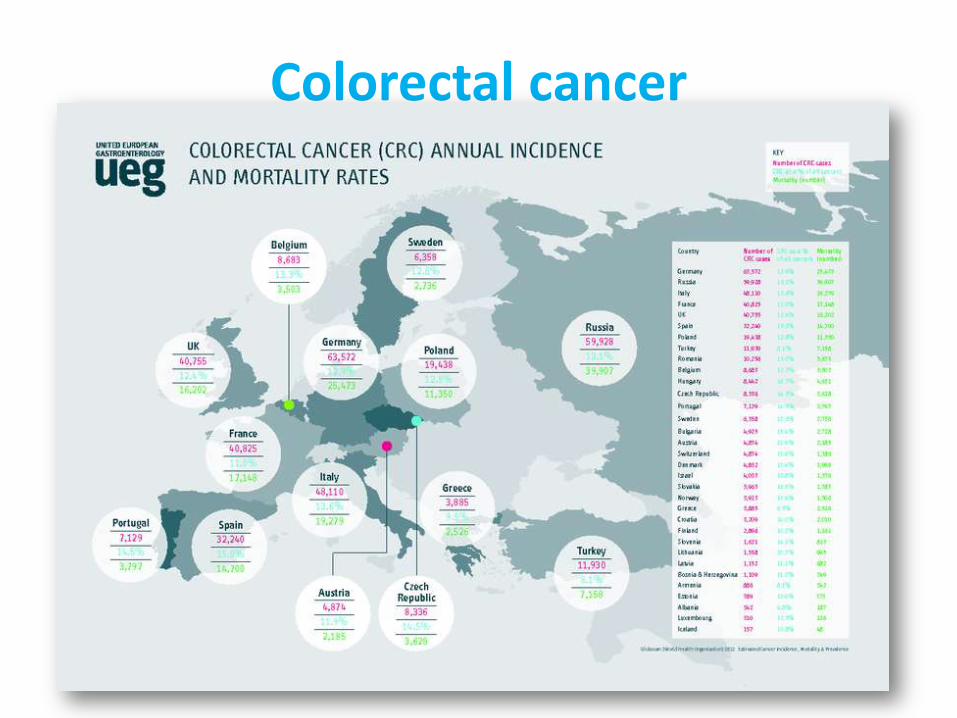
Colorectal cancer
Colorectal cancer
CRC and colon polyps
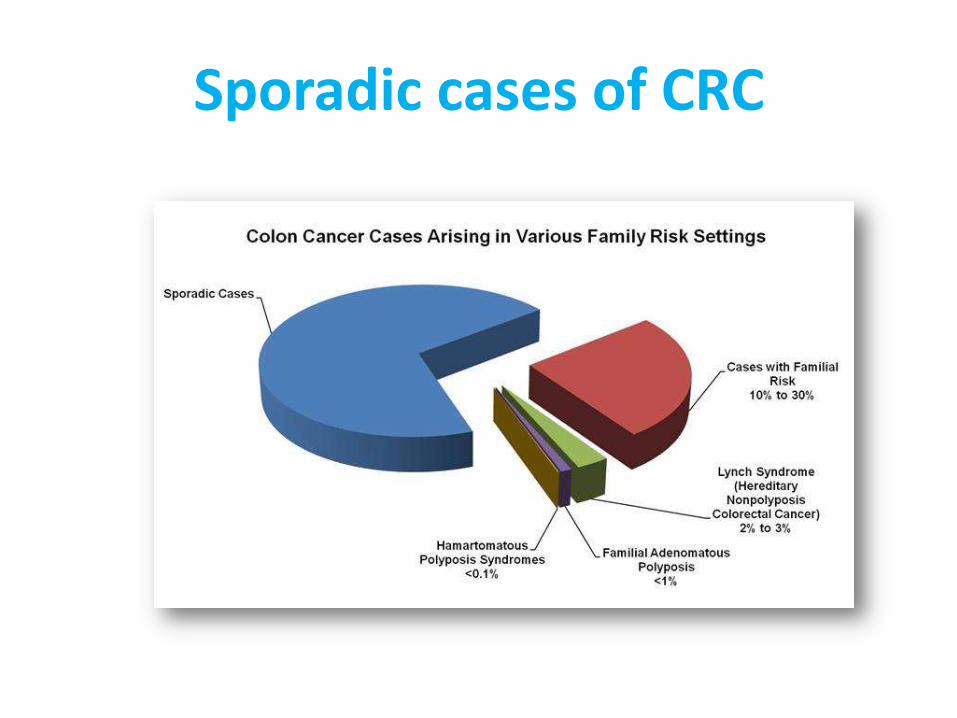
• Most colorectal cancers, regardless of etiology, arise from adenomatous polyps.
• A polyp is a grossly visible protrusion from the mucosal surface and may be classified pathologically as a non-neoplastic hamartoma (juvenile polyp), a hyperplastic mucosal proliferation (hyperplastic polyp), or an adenomatous polyp.
• Only adenomas are clearly premalignant, and only a minority of such lesions becomes cancer.
• Adenomatous polyps may be found in the colons of ~30% of middle-aged and ~50% of elderly people; however, <1% of polyps ever become malignant. Most polyps produce no symptoms and remain clinically undetected.
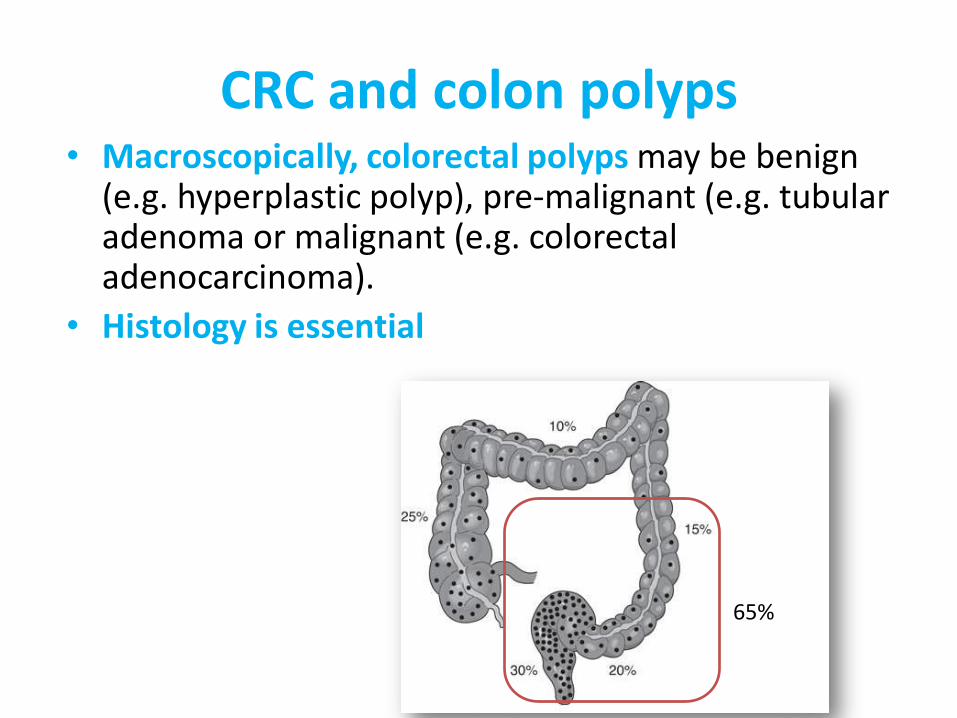
CRC and colon polyps • Macroscopically, colorectal polyps may be benign
(e.g. hyperplastic polyp), pre-malignant (e.g. tubular adenoma or malignant (e.g. colorectal adenocarcinoma).
• Histology is essential
65%
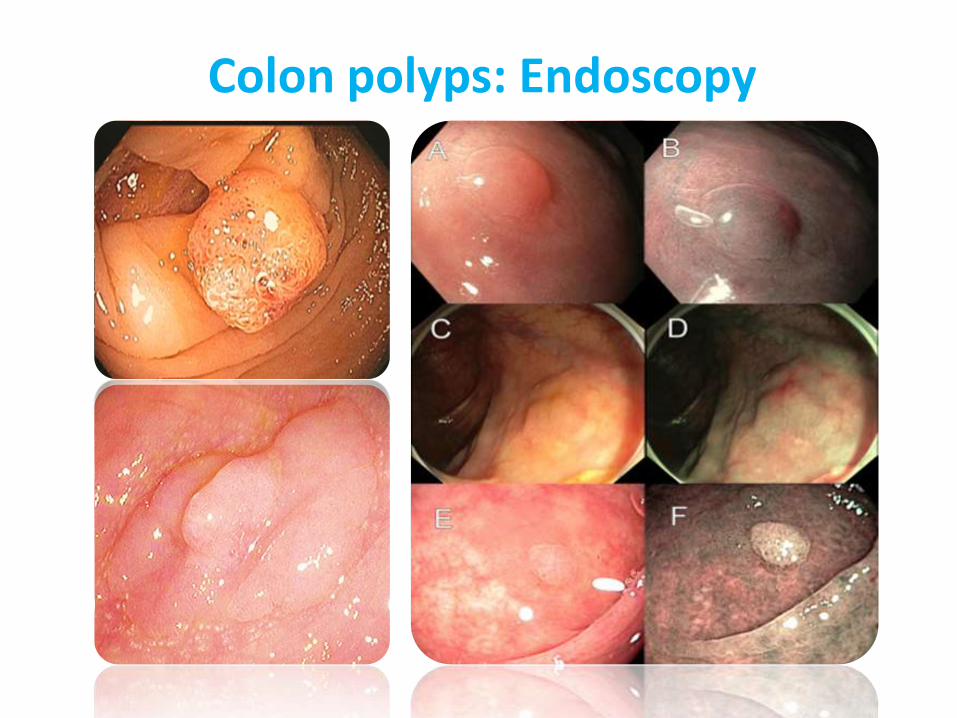
Colon polyps: Endoscopy

Malignant potential is associated with degree of dysplasia and lesion size
Type of polyp (e.g. vilous adenoma): Tubular Adenoma: 5% risk of cancer Tubulovillous adenoma: 20% risk of cancer Villous adenoma: 40% risk of cancer Serrated*
Size of polyp and number
<1 cm =<2% risk of cancer
1 cm=10%risk of cancer 2 cm=15%risk of cancer
A polyp which is greater than 0.5 cm needs to be treated
Colon polyps: risk for CRC
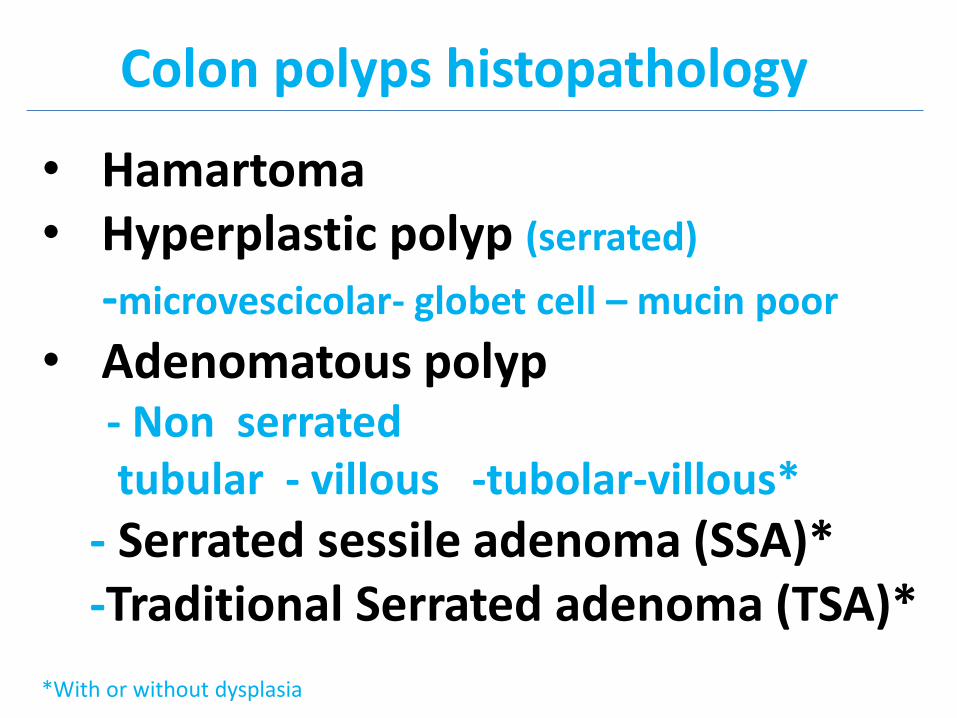
• Hamartoma • Hyperplastic polyp (serrated)
-microvescicolar- globet cell – mucin poor
• Adenomatous polyp - Non serrated tubular - villous -tubolar-villous*
- Serrated sessile adenoma (SSA)* -Traditional Serrated adenoma (TSA)*
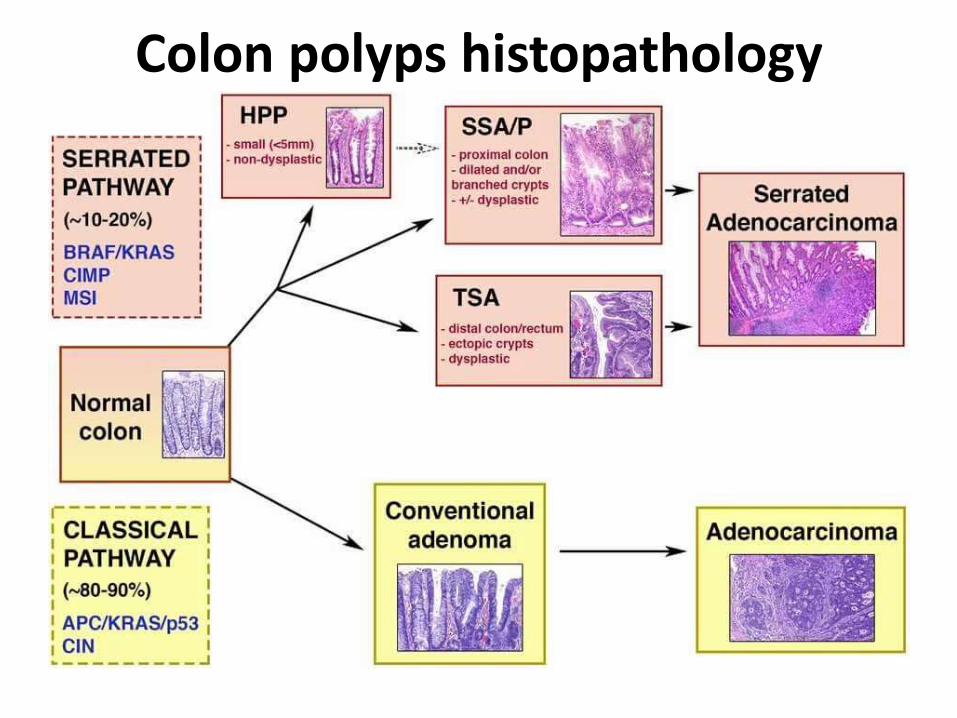
Colon polyps histopathology
*With or without dysplasia
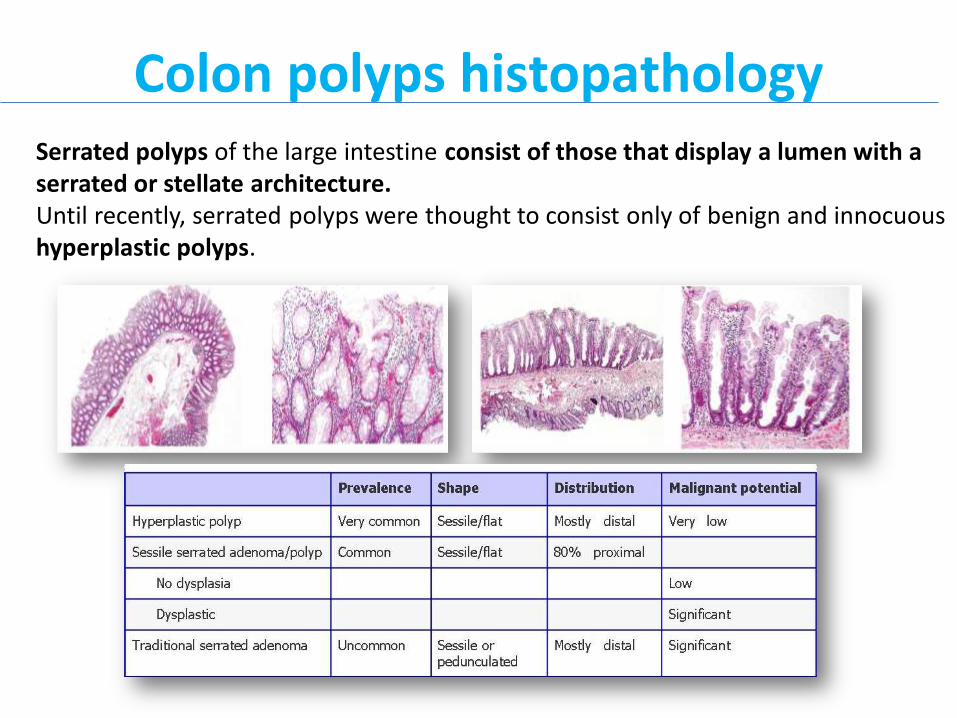
Colon polyps histopathology Serrated polyps of the large intestine consist of those that display a lumen with a serrated or stellate architecture. Until recently, serrated polyps were thought to consist only of benign and innocuous hyperplastic polyps.
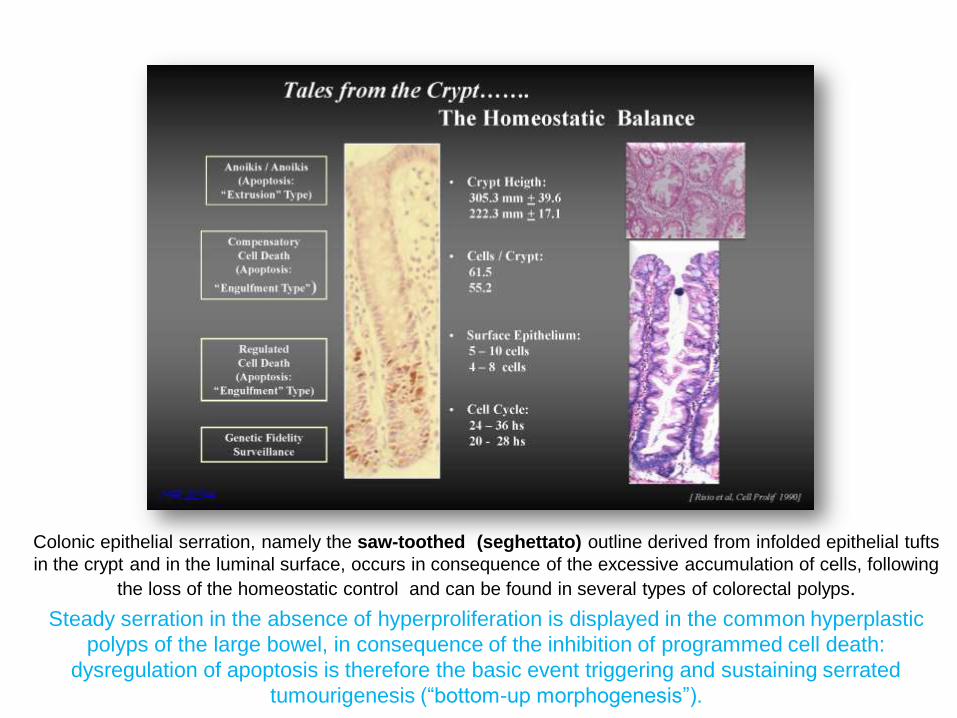
Colonic epithelial serration, namely the saw-toothed (seghettato) outline derived from infolded epithelial tufts
in the crypt and in the luminal surface, occurs in consequence of the excessive accumulation of cells, following
the loss of the homeostatic control and can be found in several types of colorectal polyps.
Steady serration in the absence of hyperproliferation is displayed in the common hyperplastic
polyps of the large bowel, in consequence of the inhibition of programmed cell death:
dysregulation of apoptosis is therefore the basic event triggering and sustaining serrated
tumourigenesis (“bottom-up morphogenesis”).
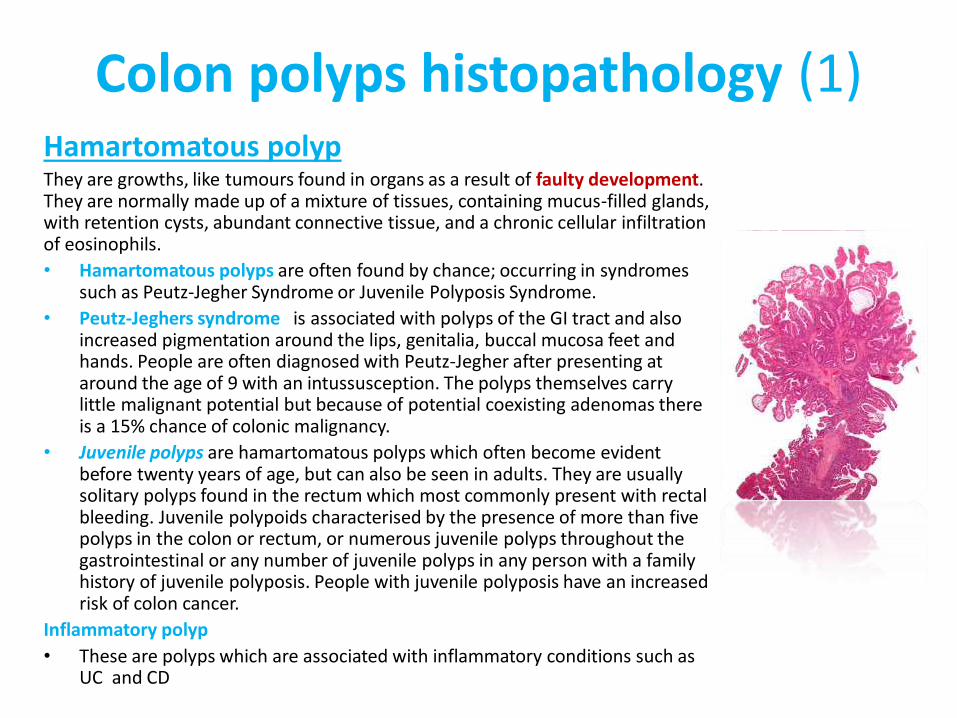
Colon polyps histopathology (1) Hamartomatous polyp They are growths, like tumours found in organs as a result of faulty development. They are normally made up of a mixture of tissues, containing mucus-filled glands, with retention cysts, abundant connective tissue, and a chronic cellular infiltration of eosinophils.
• Hamartomatous polyps are often found by chance; occurring in syndromes such as Peutz-Jegher Syndrome or Juvenile Polyposis Syndrome.
• Peutz-Jeghers syndrome is associated with polyps of the GI tract and also increased pigmentation around the lips, genitalia, buccal mucosa feet and hands. People are often diagnosed with Peutz-Jegher after presenting at around the age of 9 with an intussusception. The polyps themselves carry little malignant potential but because of potential coexisting adenomas there is a 15% chance of colonic malignancy.
• Juvenile polyps are hamartomatous polyps which often become evident before twenty years of age, but can also be seen in adults. They are usually solitary polyps found in the rectum which most commonly present with rectal bleeding. Juvenile polypoids characterised by the presence of more than five polyps in the colon or rectum, or numerous juvenile polyps throughout the gastrointestinal or any number of juvenile polyps in any person with a family history of juvenile polyposis. People with juvenile polyposis have an increased risk of colon cancer.
Inflammatory polyp
• These are polyps which are associated with inflammatory conditions such as UC and CD
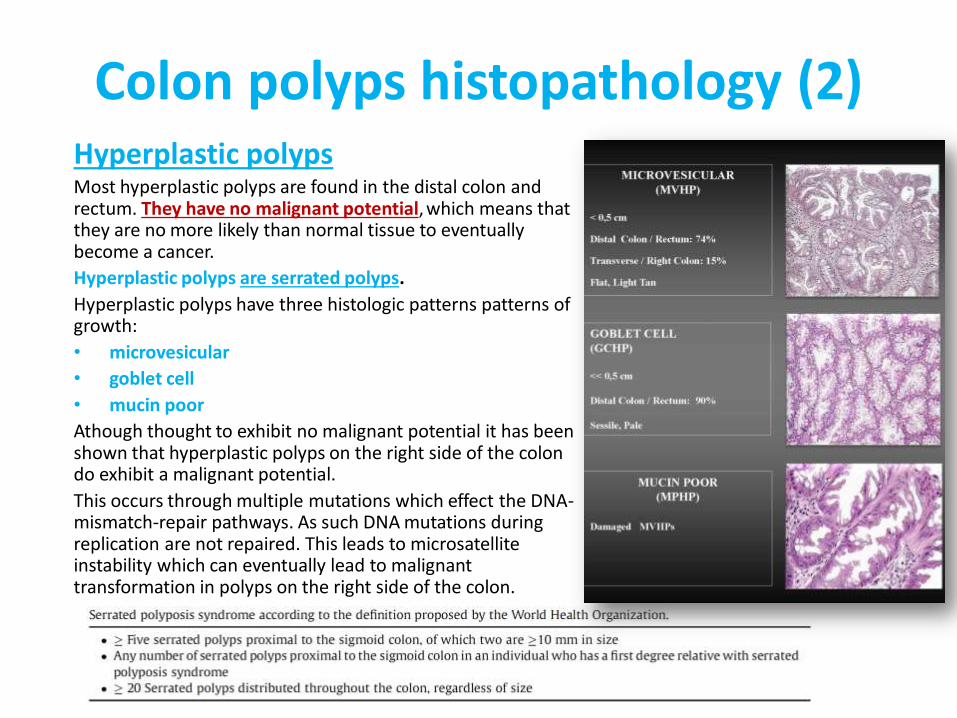
Colon polyps histopathology (2) Hyperplastic polyps Most hyperplastic polyps are found in the distal colon and rectum. They have no malignant potential, which means that they are no more likely than normal tissue to eventually become a cancer.
Hyperplastic polyps are serrated polyps.
Hyperplastic polyps have three histologic patterns patterns of growth:
• microvesicular
• goblet cell
• mucin poor
Athough thought to exhibit no malignant potential it has been shown that hyperplastic polyps on the right side of the colon do exhibit a malignant potential.
This occurs through multiple mutations which effect the DNA-mismatch-repair pathways. As such DNA mutations during replication are not repaired. This leads to microsatellite instability which can eventually lead to malignant transformation in polyps on the right side of the colon.
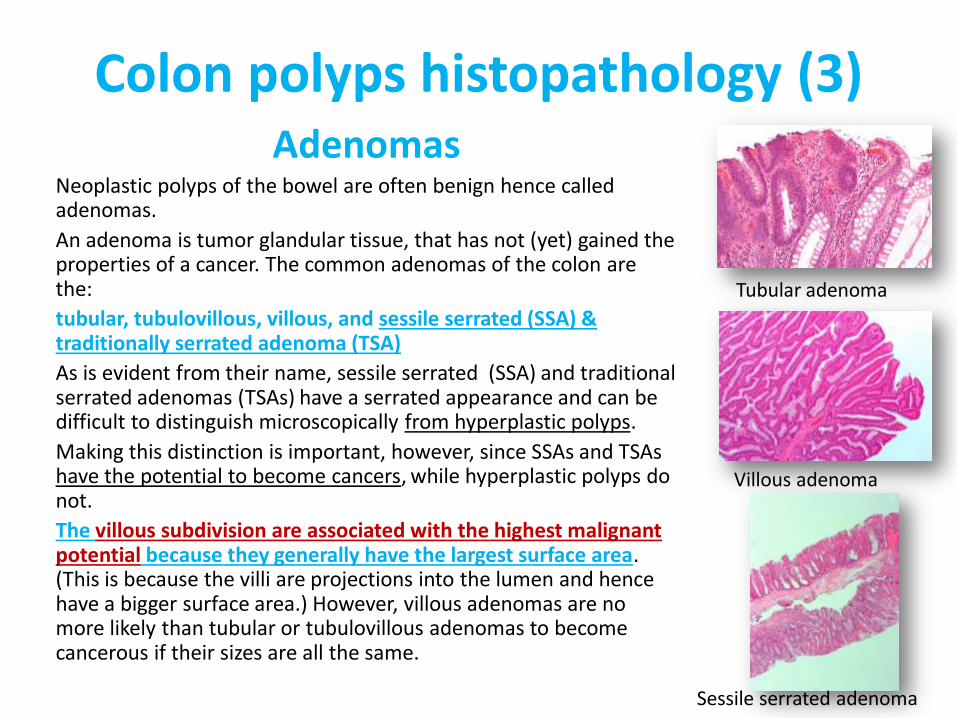
Colon polyps histopathology (3) Adenomas
Neoplastic polyps of the bowel are often benign hence called adenomas.
An adenoma is tumor glandular tissue, that has not (yet) gained the properties of a cancer. The common adenomas of the colon are the:
tubular, tubulovillous, villous, and sessile serrated (SSA) & traditionally serrated adenoma (TSA)
As is evident from their name, sessile serrated (SSA) and traditional serrated adenomas (TSAs) have a serrated appearance and can be difficult to distinguish microscopically from hyperplastic polyps.
Making this distinction is important, however, since SSAs and TSAs have the potential to become cancers, while hyperplastic polyps do not.
The villous subdivision are associated with the highest malignant potential because they generally have the largest surface area. (This is because the villi are projections into the lumen and hence have a bigger surface area.) However, villous adenomas are no more likely than tubular or tubulovillous adenomas to become cancerous if their sizes are all the same.
Villous adenoma
Tubular adenoma
Sessile serrated adenoma
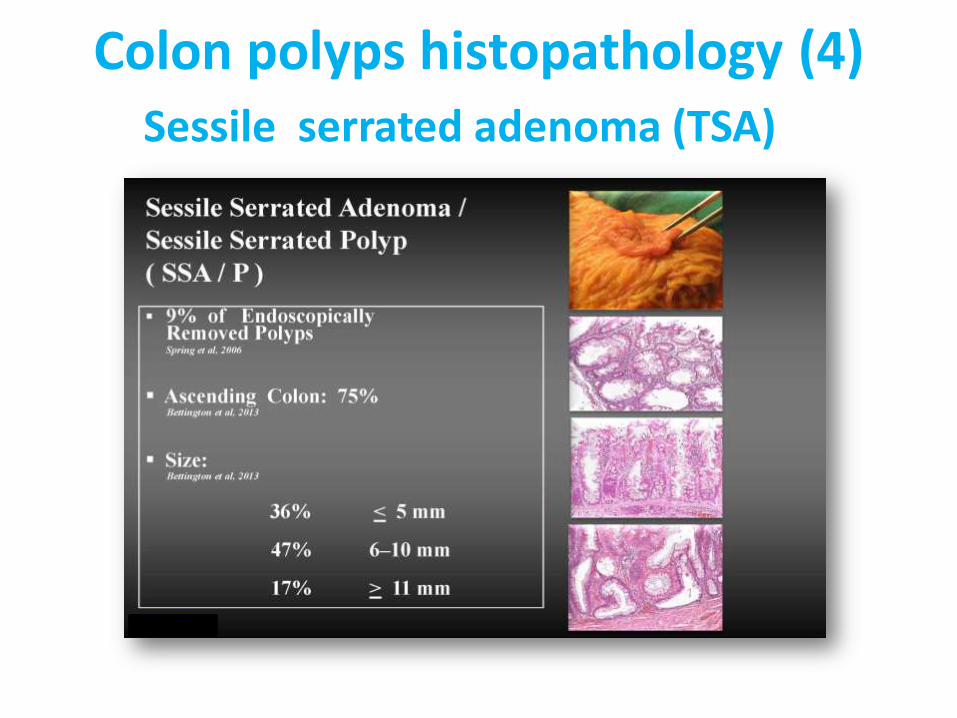
Colon polyps histopathology (4) Sessile serrated adenoma (TSA)
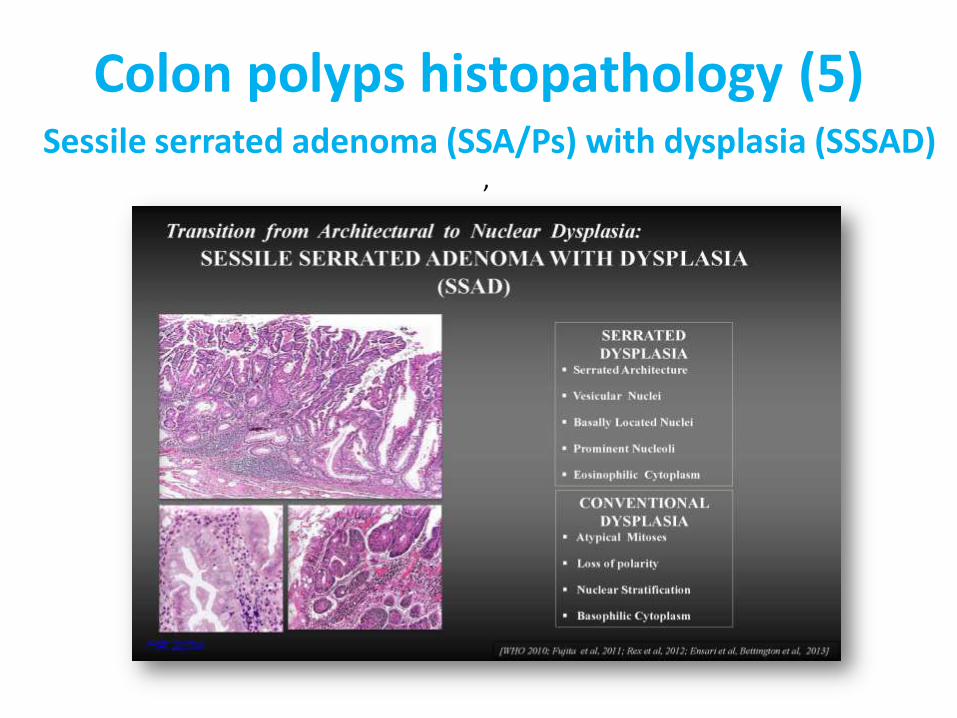
Colon polyps histopathology (5)
Sessile serrated adenoma (SSA/Ps) with dysplasia (SSSAD) ,
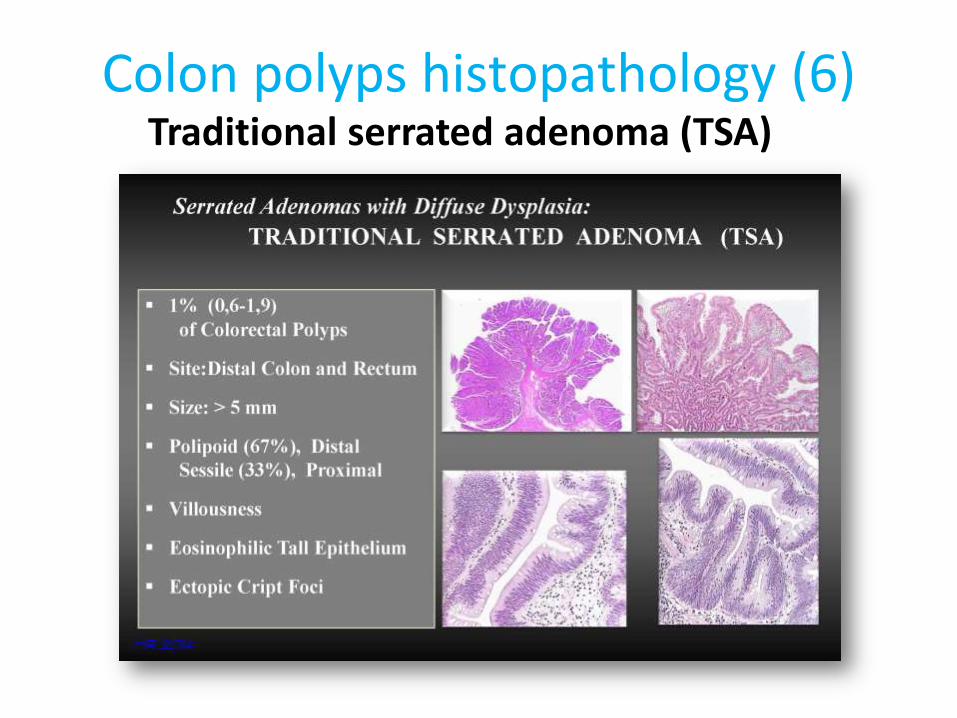
Colon polyps histopathology (6) Traditional serrated adenoma (TSA)
Colon polyps histopathology
Colon polyps symptoms
In the large majority of cases colon polyps cause no symptoms.
Sometimes, however, there may be signs and symptoms
such as:
• Rectal bleeding
• Occult bleeding (anemia)
• Changes in the bowel habit (constipation, diarrhea or narrowing of the stool).
• Pain or obstruction (rare)
Colon polyps diagnosis
Nearly all colon cancers develop from polyps, but the polyps grow slowly, usually over a period of years.
Screening tests play a key role in detecting polyps before they become cancerous.
These tests can also help find colorectal cancer in its early stages, when you have a good chance of recovery.
• Fecal blood tests.
• Colonoscopy (flexible sigmoidoscopy)
• Barium enema.
• Computerized tomographic colonography (virtual colonoscopy).
• Stool DNA testing.
• Genetic testing.
Endoscopic removal of colon polyps
• Polipectomy (Polipectomia endoscopica)
• Endoscopic Mucosal Resection (Mucosectomia Endoscopica)
• Endoscopic Submucosal Dissection (Dissezione sottomucosa endoscopica)
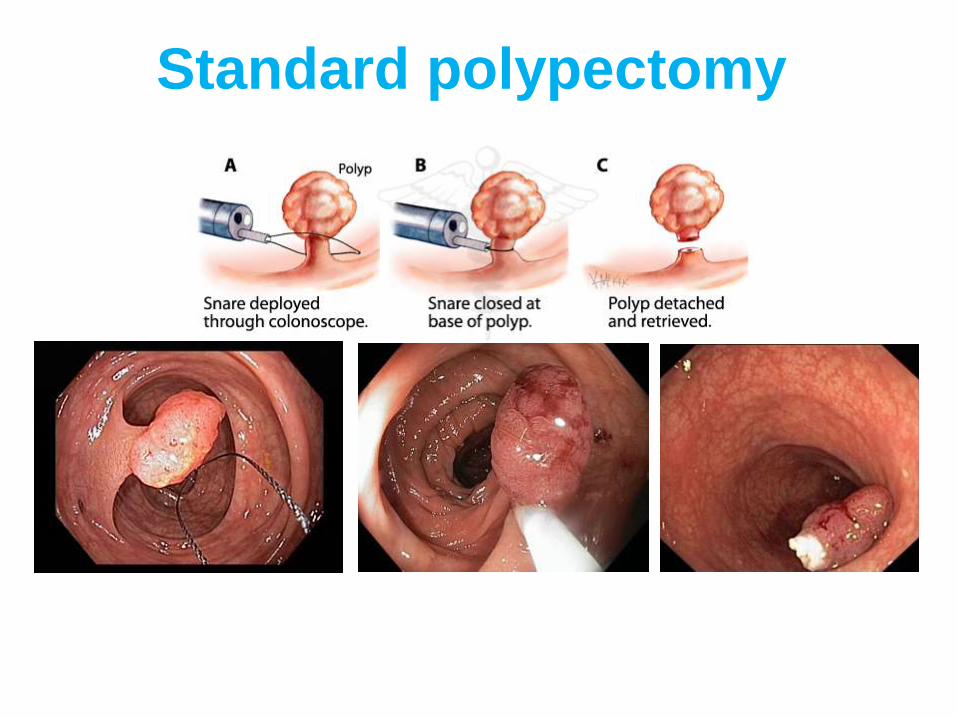
Standard polypectomy
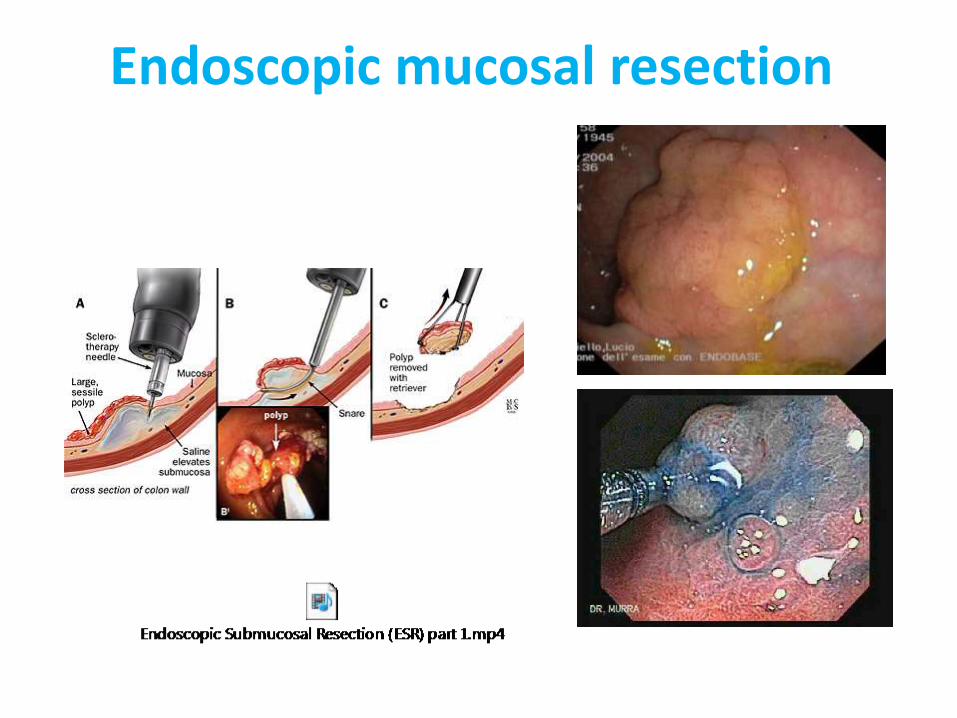
Endoscopic mucosal resection
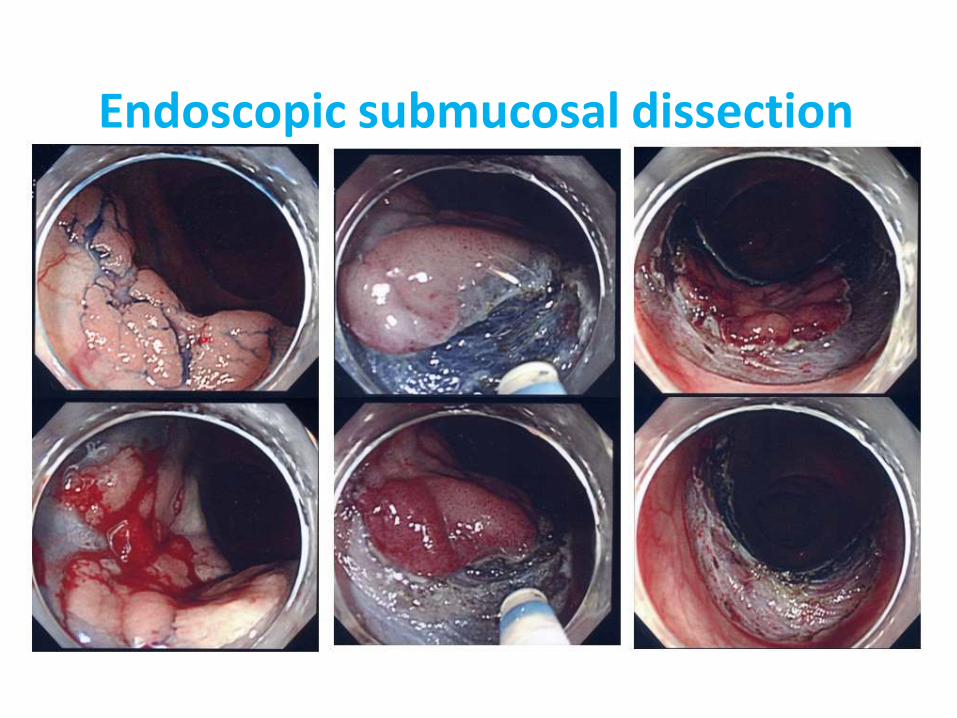
Endoscopic submucosal dissection
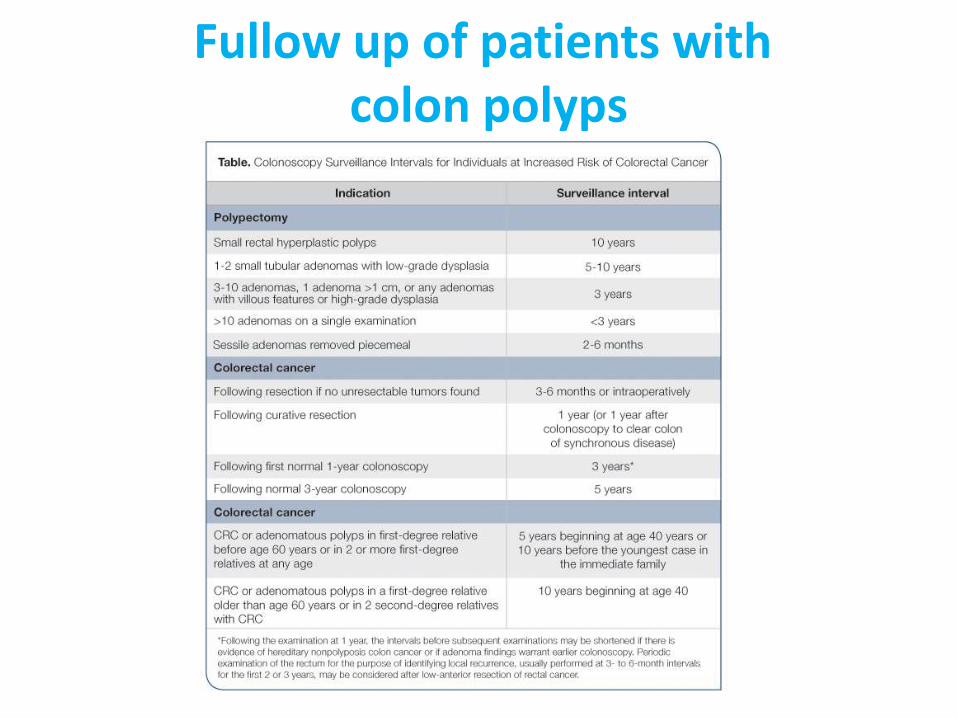
Fullow up of patients with colon polyps
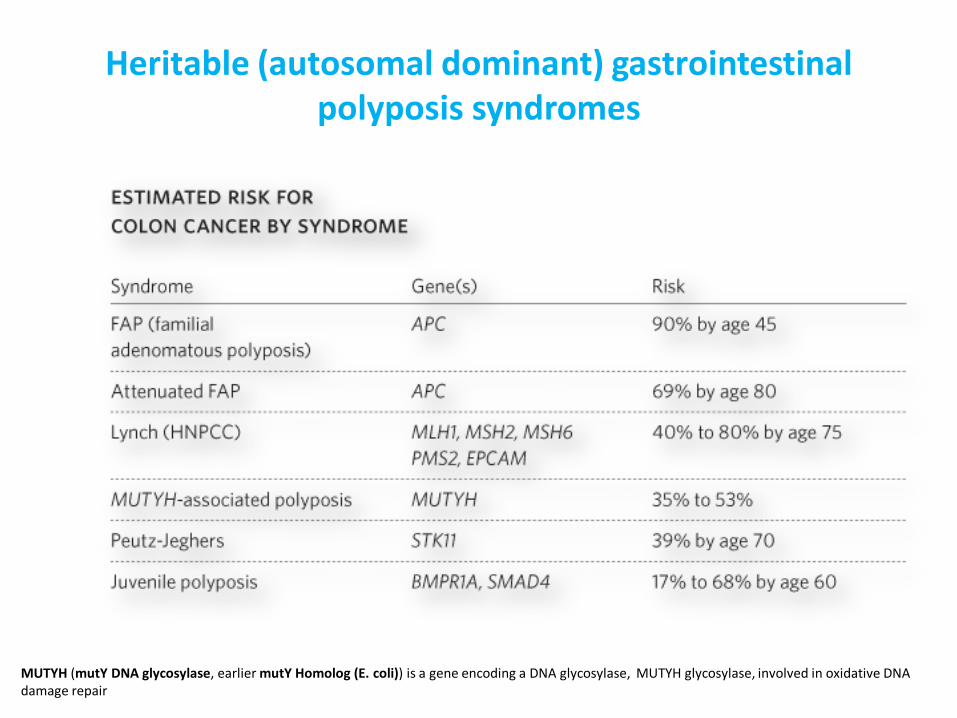
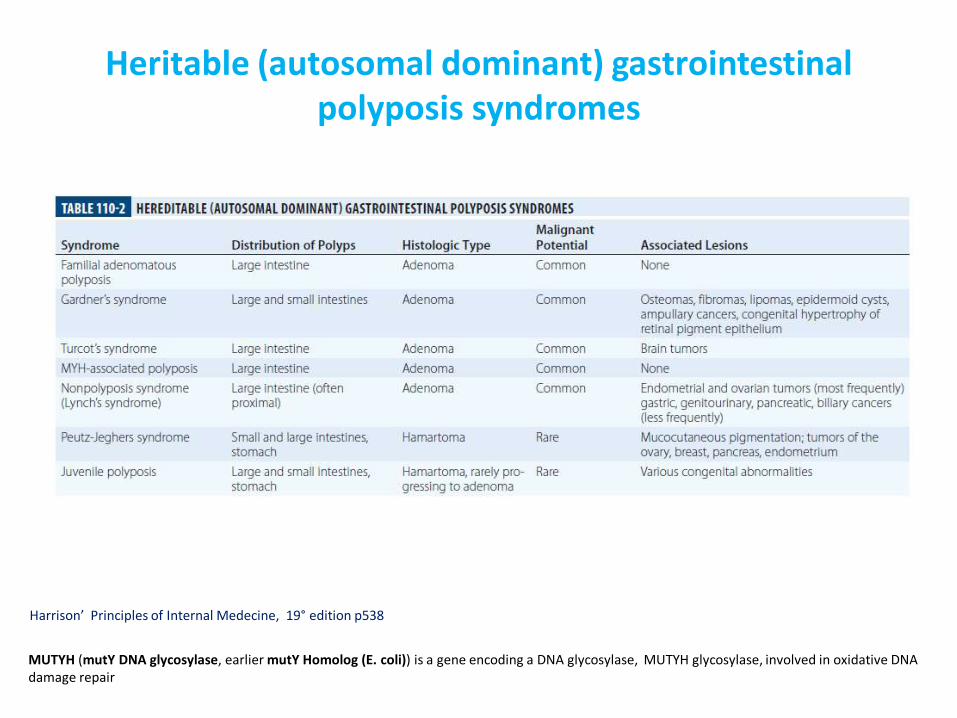
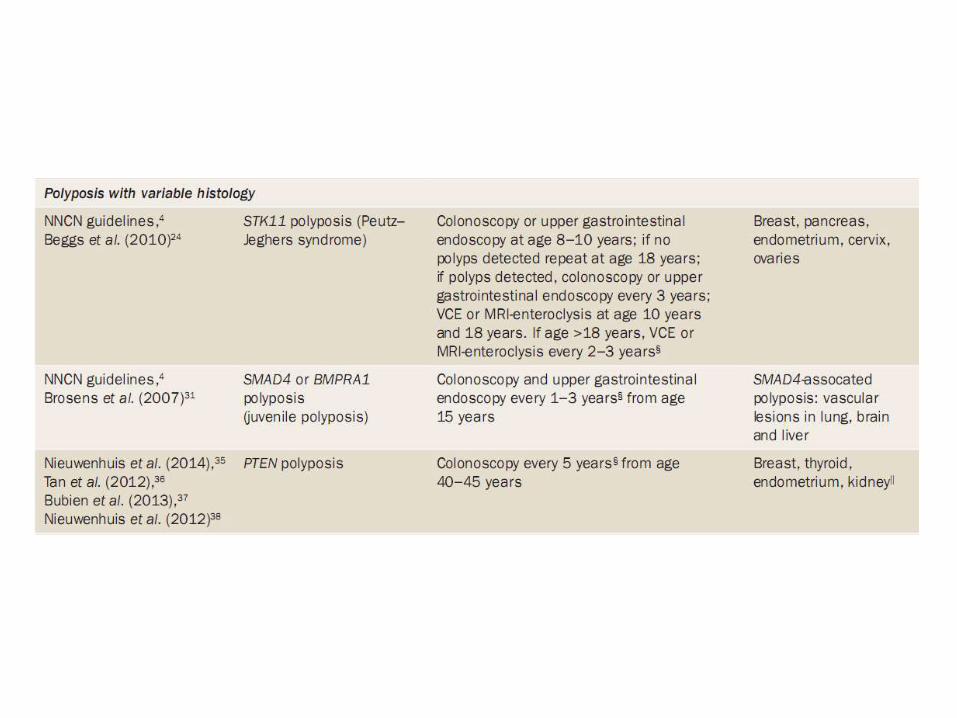
Heritable (autosomal dominant) gastrointestinal polyposis syndromes
MUTYH (mutY DNA glycosylase, earlier mutY Homolog (E. coli)) is a gene encoding a DNA glycosylase, MUTYH glycosylase, involved in oxidative DNA damage repair
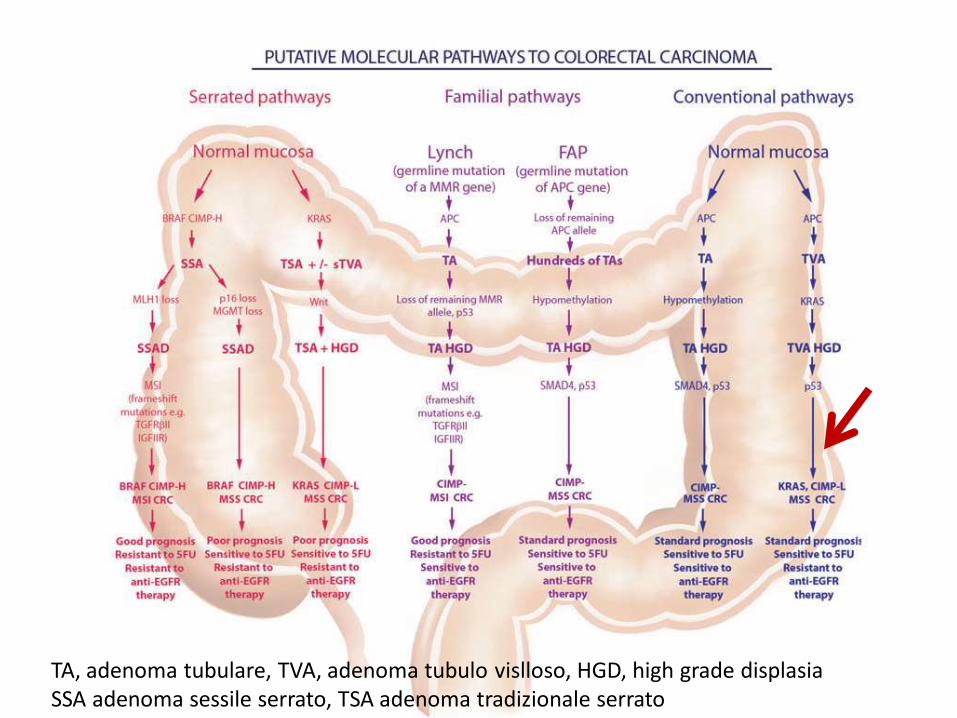
TA, adenoma tubulare, TVA, adenoma tubulo vislloso, HGD, high grade displasia SSA adenoma sessile serrato, TSA adenoma tradizionale serrato
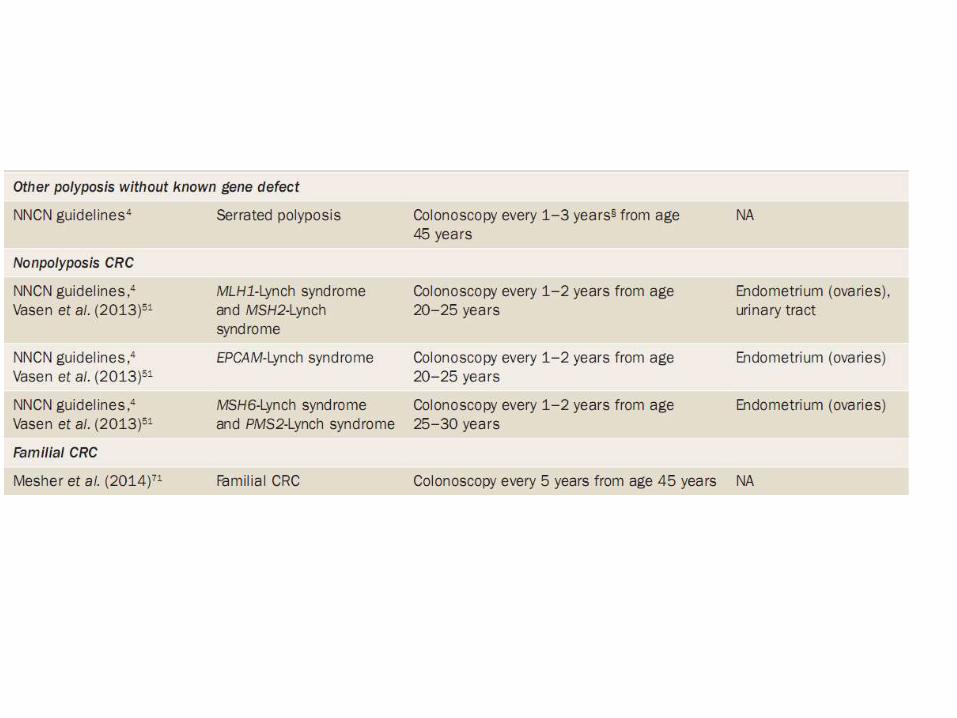
Heritable (autosomal dominant) gastrointestinal polyposis syndromes
MUTYH (mutY DNA glycosylase, earlier mutY Homolog (E. coli)) is a gene encoding a DNA glycosylase, MUTYH glycosylase, involved in oxidative DNA damage repair
Harrison’ Principles of Internal Medecine, 19° edition p538
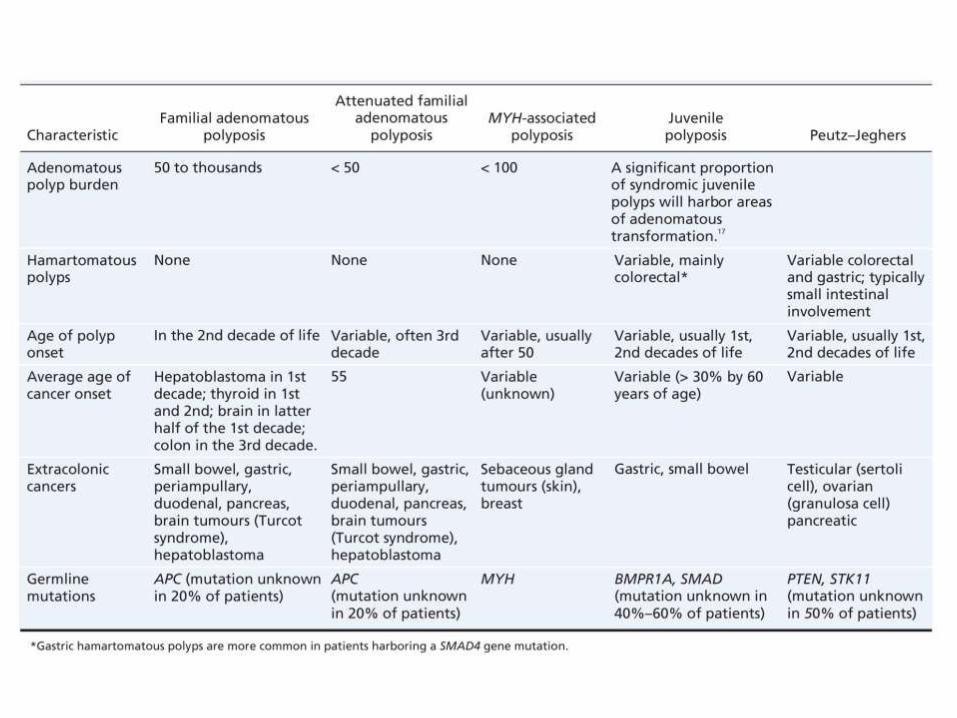

FAP autosomal dominant
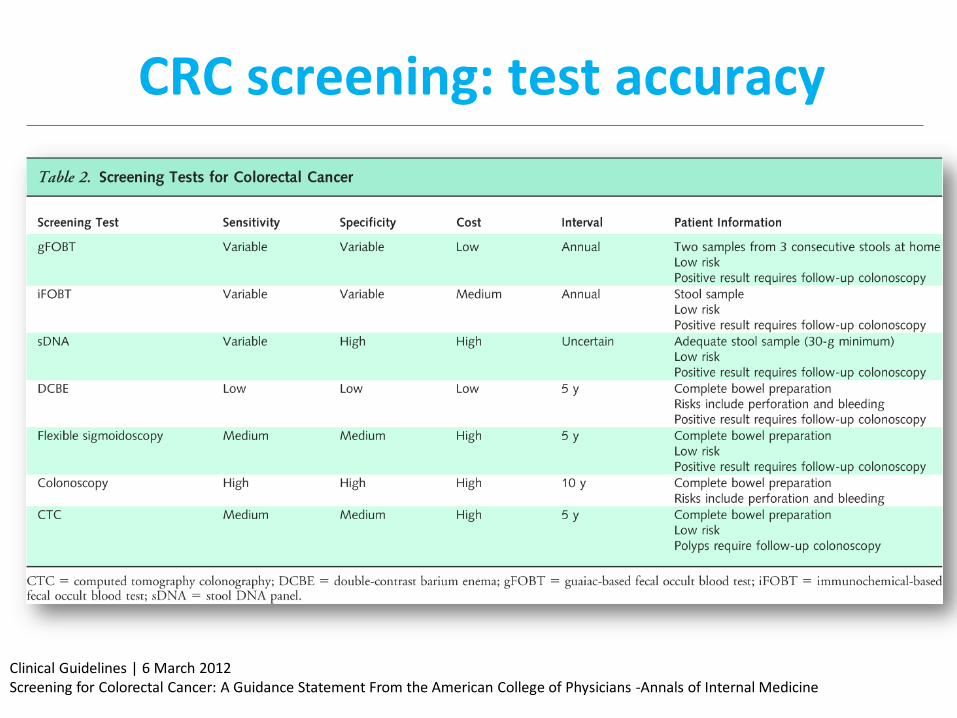
CRC screening: test accuracy
Clinical Guidelines | 6 March 2012 Screening for Colorectal Cancer: A Guidance Statement From the American College of Physicians -Annals of Internal Medicine
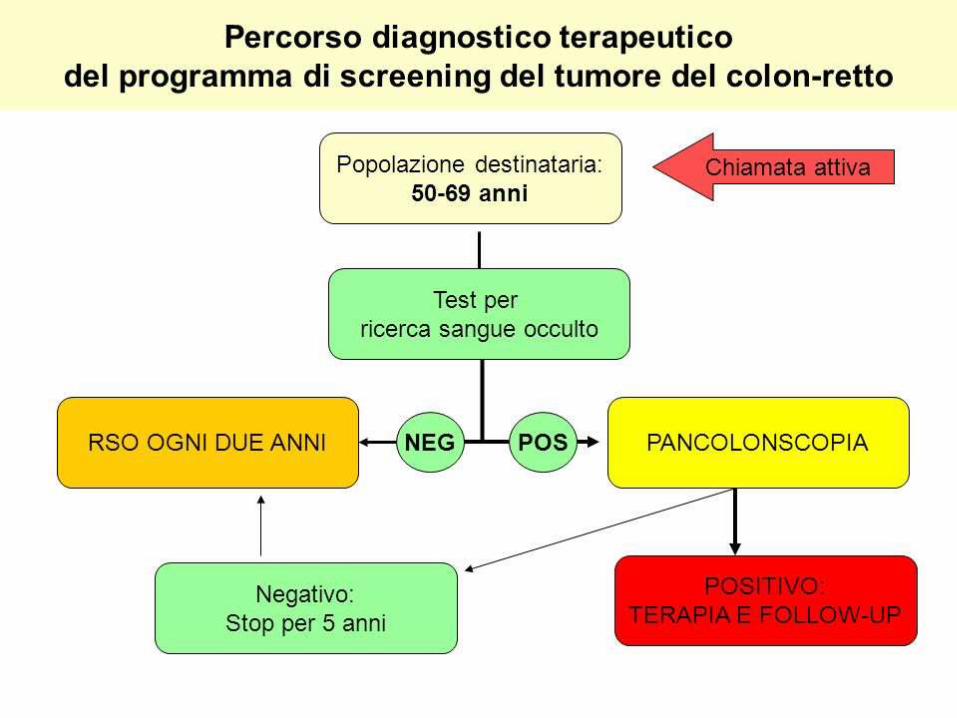
CRC screening Programmi di screening del cancro del colon-retto (8)
Rischio normale medio (età >50 anni, assenza di altri fattori di rischio) ricerca sangue occulto annuale, rettosigmoidoscopia con strumento flessibile o
Colonscopia ogni 5 anni
Rischio moderato
- Storia di adenoma: colonscopia
- parenti di primo grado con CRC: colonscopia all'età di 40 anni, o 10 anni prima se familiari hanno presentato il tumore in giovane età
- parenti di primo grado con adenoma prima di 60 anni: colonscopia all'età di 40 anni
Rischio elevato
- poliposi familiare: colonscopia a dieci anni di età e valutazione genetica
- cancro in poliposi non familiare: colonscopia a 20 anni e valutazione ogni 2 anni; dopo 40 anni, colonscopia ogni anno; valutazione genetica
- malattie infiammatorie del colon: colonscopia ogni 2 anni in RCU o Crohn-colite estese a tutto il colon, della durata 8 anni; se colite ulcerosa o Crohn-colite sono
limitate al colon sinistro, dopo 12 anni
CRC primary prevention ASA and NSAIDs
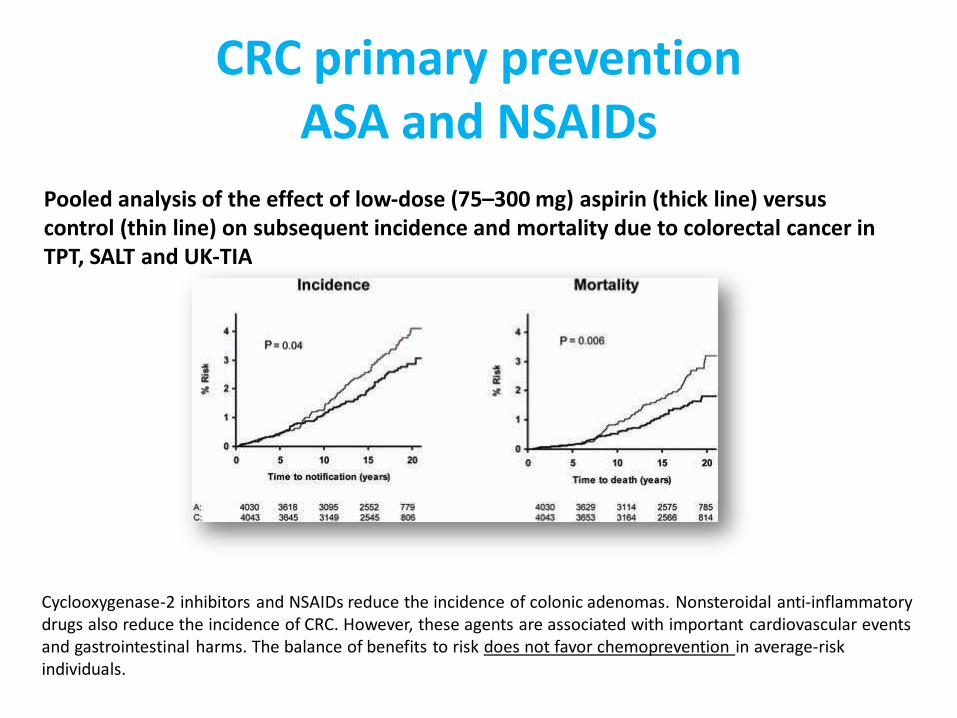
Pooled analysis of the effect of low-dose (75–300 mg) aspirin (thick line) versus control (thin line) on subsequent incidence and mortality due to colorectal cancer in TPT, SALT and UK-TIA
Cyclooxygenase-2 inhibitors and NSAIDs reduce the incidence of colonic adenomas. Nonsteroidal anti-inflammatory drugs also reduce the incidence of CRC. However, these agents are associated with important cardiovascular events and gastrointestinal harms. The balance of benefits to risk does not favor chemoprevention in average-risk individuals.
CRC presenting symptoms Symptoms depend on the anatomic location of the tumor
• Cancer in right colon usually become larger than cancer in the left colon and
synptoms are less specific (fatigue, anemia, weight loss, intermittent bleeding) • Cancer in the left colon are more commonly linked to stool obstruction,
abdominal pain & rectal bleeding • Cancer from rectosigmoidal location might have hematochezia, tenesmus,
narrowing of stool caliber. Anemia is less frequent. Rectal bleeding is common.
• In general abdominal pain is seen in 44% of patients, change in bowel habits in 43%, blood in the stools or dark stools in 40%, weakness in about 20%, Iron deficiency anemia in 10% and weight loss in about 5%.
• Symptoms can be of gradual onset or sudden such as when the tumor causes intestinal obstruction or perforation (a hole in the bowel wall).
• About 20% of patients will have disease already spread to the liver at the time of diagnosis. .
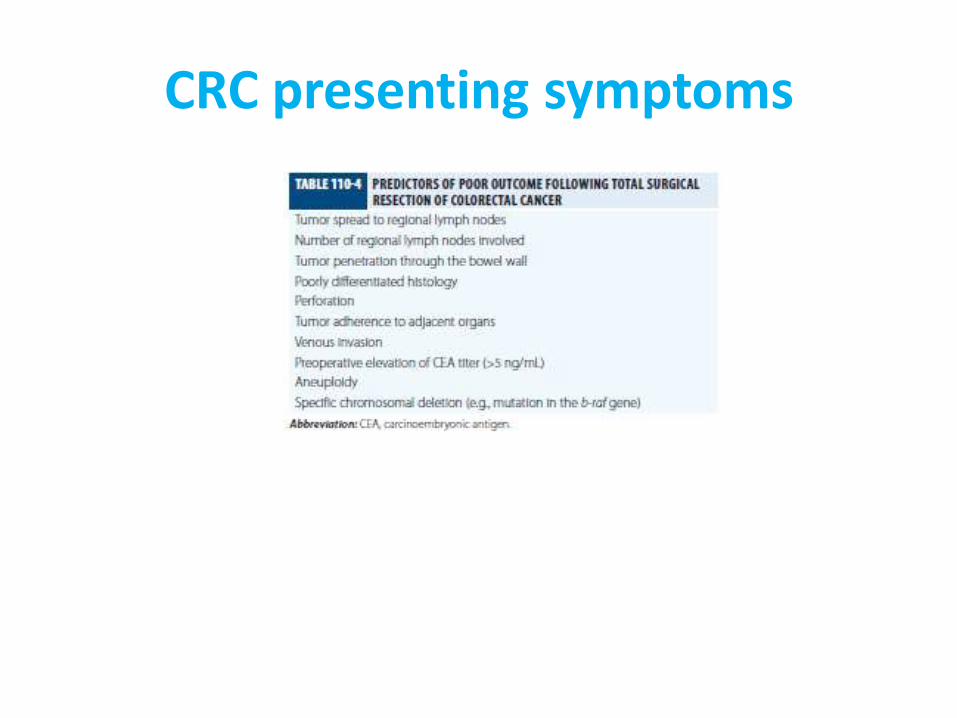
CRC presenting symptoms
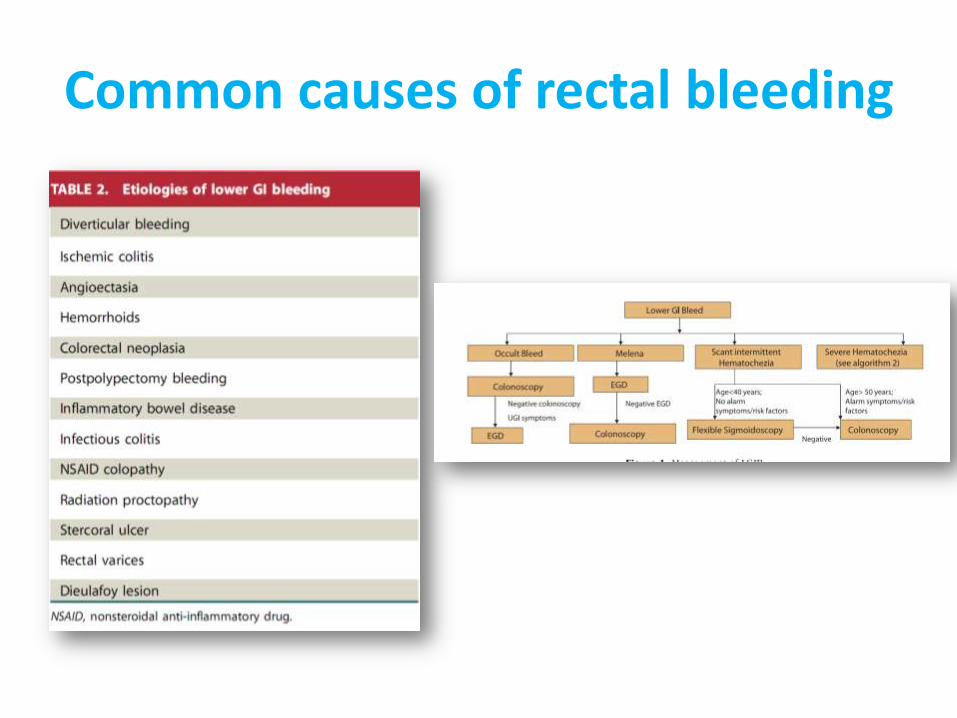
Common causes of rectal bleeding
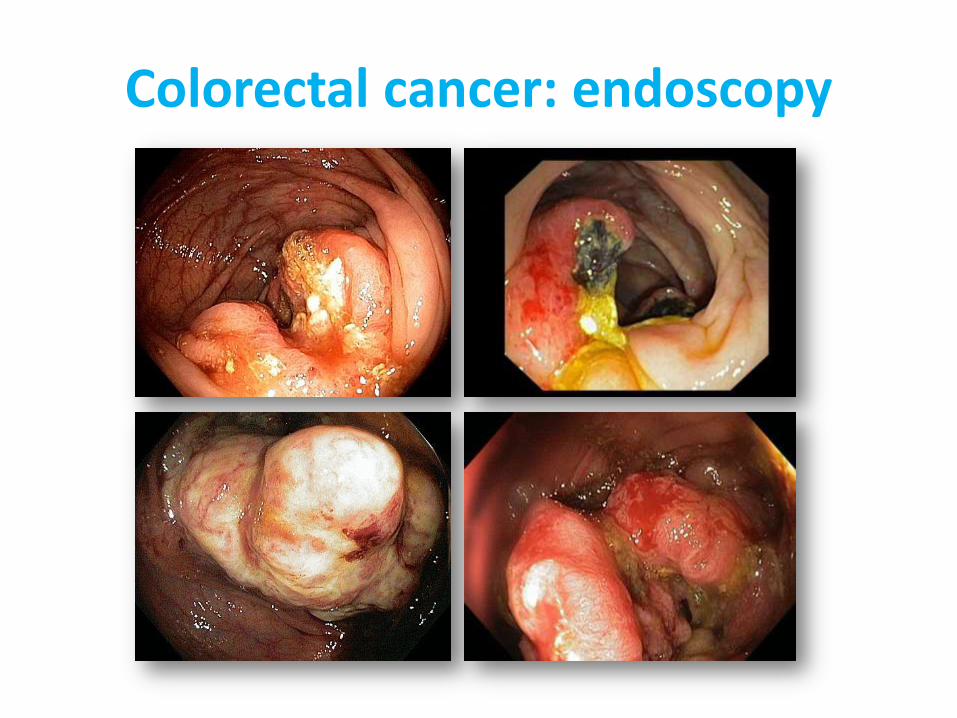
Colorectal cancer: endoscopy
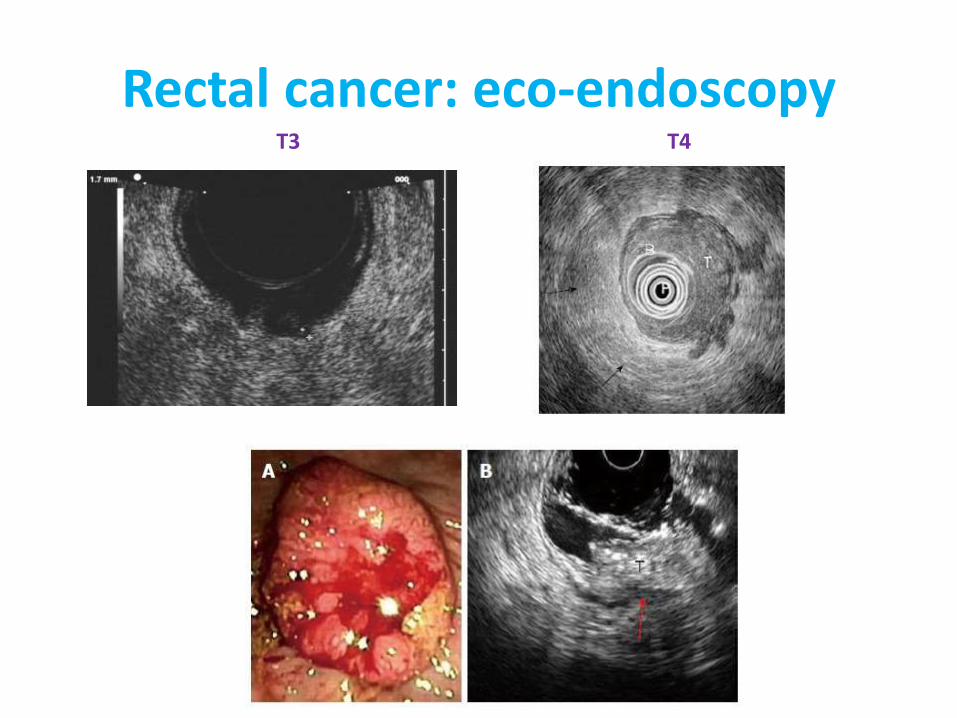
Rectal cancer: eco-endoscopy T3 T4
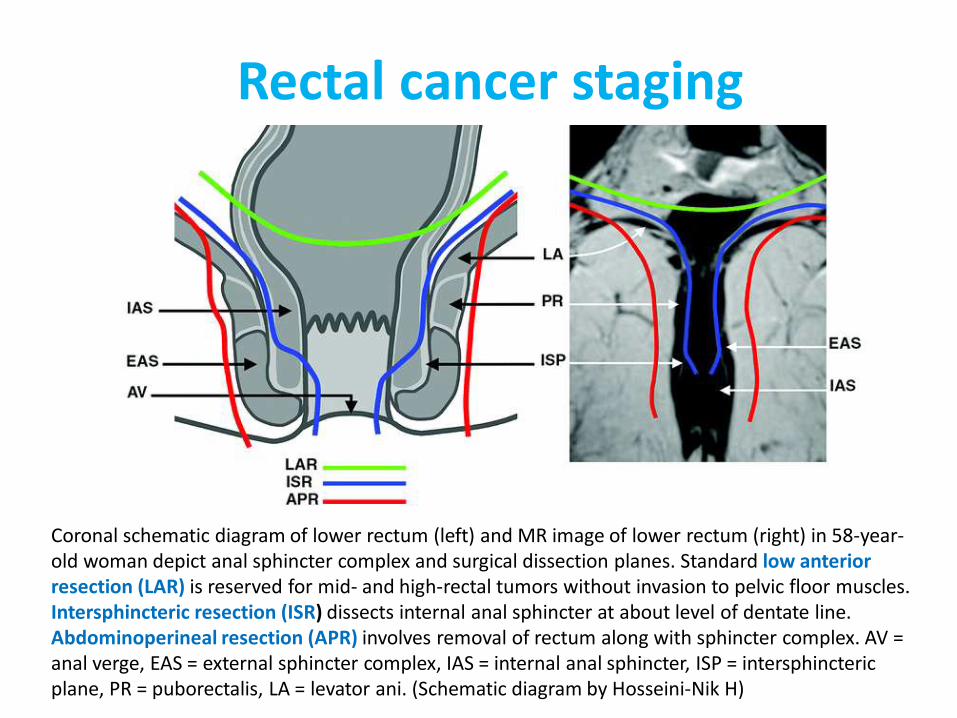
Rectal cancer staging
Coronal schematic diagram of lower rectum (left) and MR image of lower rectum (right) in 58-year-old woman depict anal sphincter complex and surgical dissection planes. Standard low anterior resection (LAR) is reserved for mid- and high-rectal tumors without invasion to pelvic floor muscles. Intersphincteric resection (ISR) dissects internal anal sphincter at about level of dentate line. Abdominoperineal resection (APR) involves removal of rectum along with sphincter complex. AV = anal verge, EAS = external sphincter complex, IAS = internal anal sphincter, ISP = intersphincteric plane, PR = puborectalis, LA = levator ani. (Schematic diagram by Hosseini-Nik H)
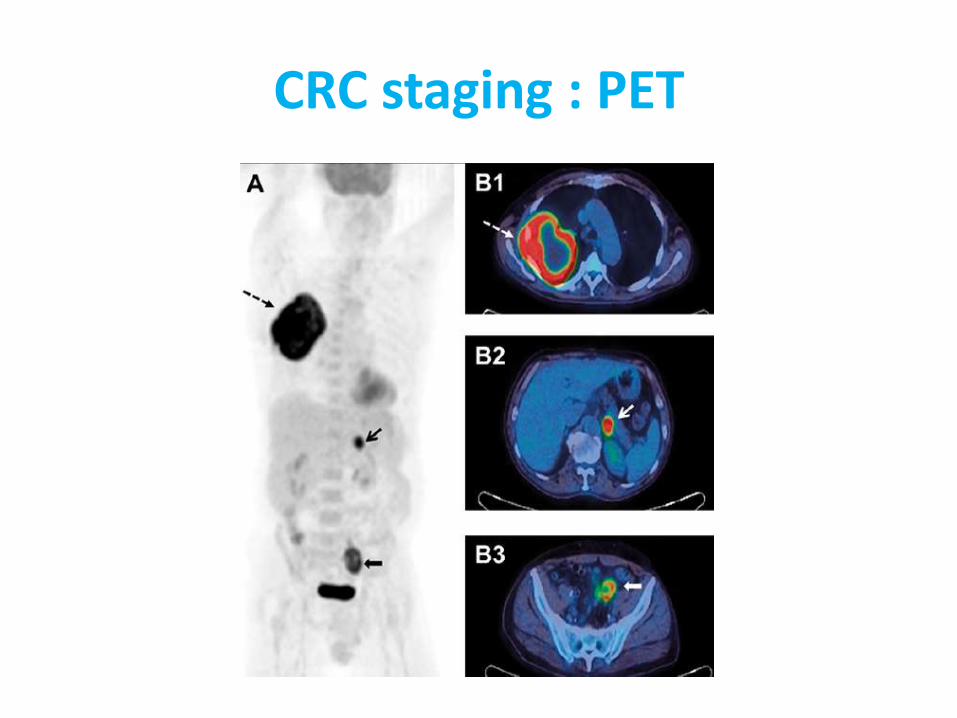
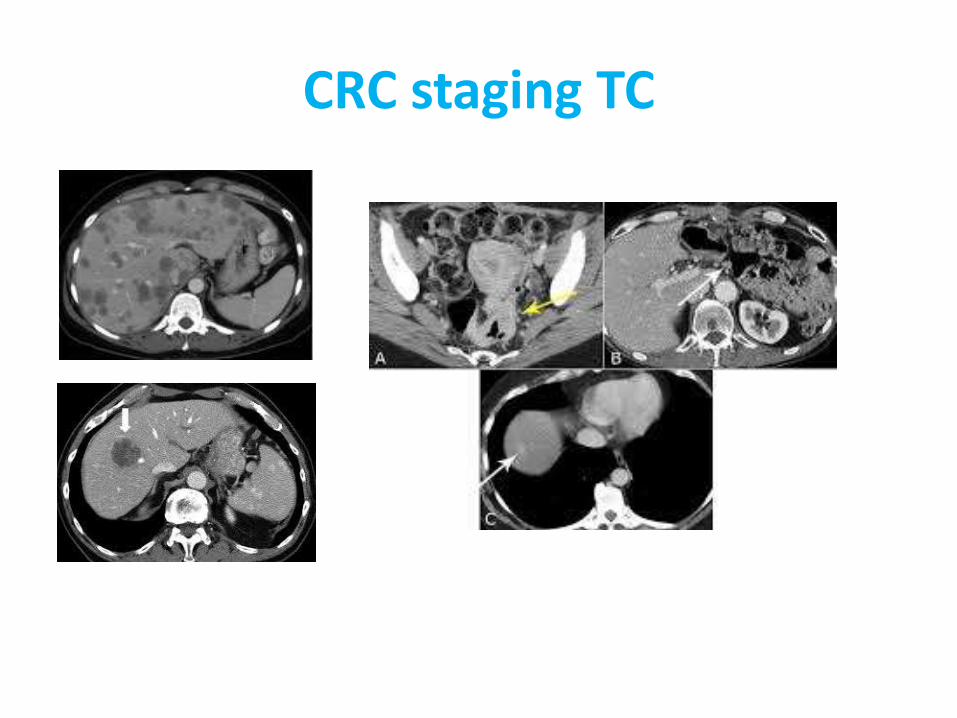
CRC staging : PET
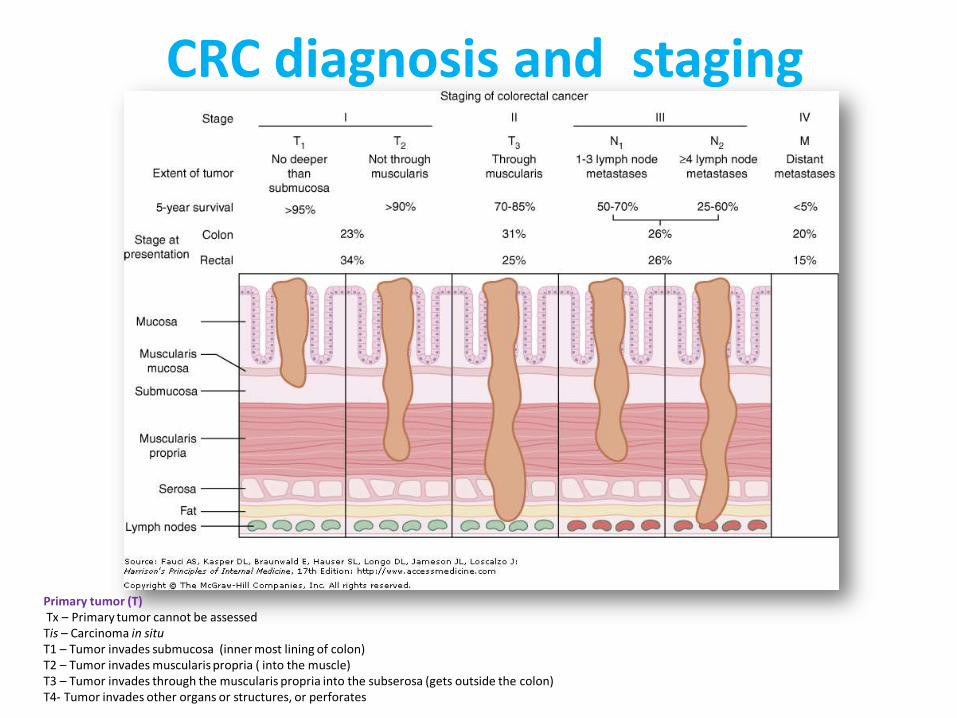
CRC diagnosis and staging
Primary tumor (T) Tx – Primary tumor cannot be assessed Tis – Carcinoma in situ T1 – Tumor invades submucosa (inner most lining of colon) T2 – Tumor invades muscularis propria ( into the muscle) T3 – Tumor invades through the muscularis propria into the subserosa (gets outside the colon) T4- Tumor invades other organs or structures, or perforates
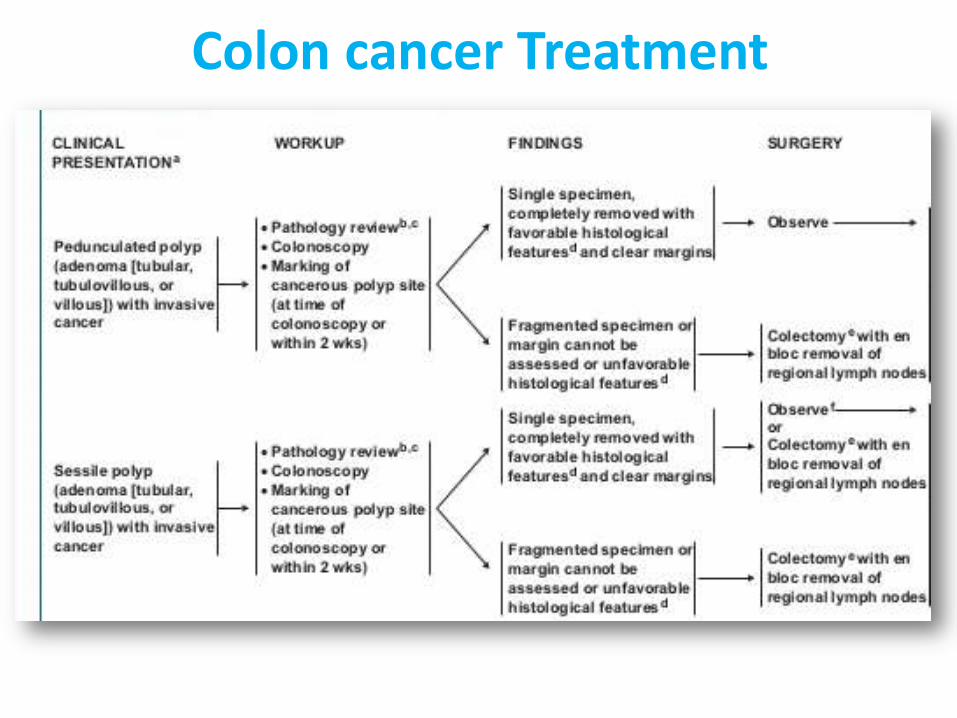
Colon cancer Treatment
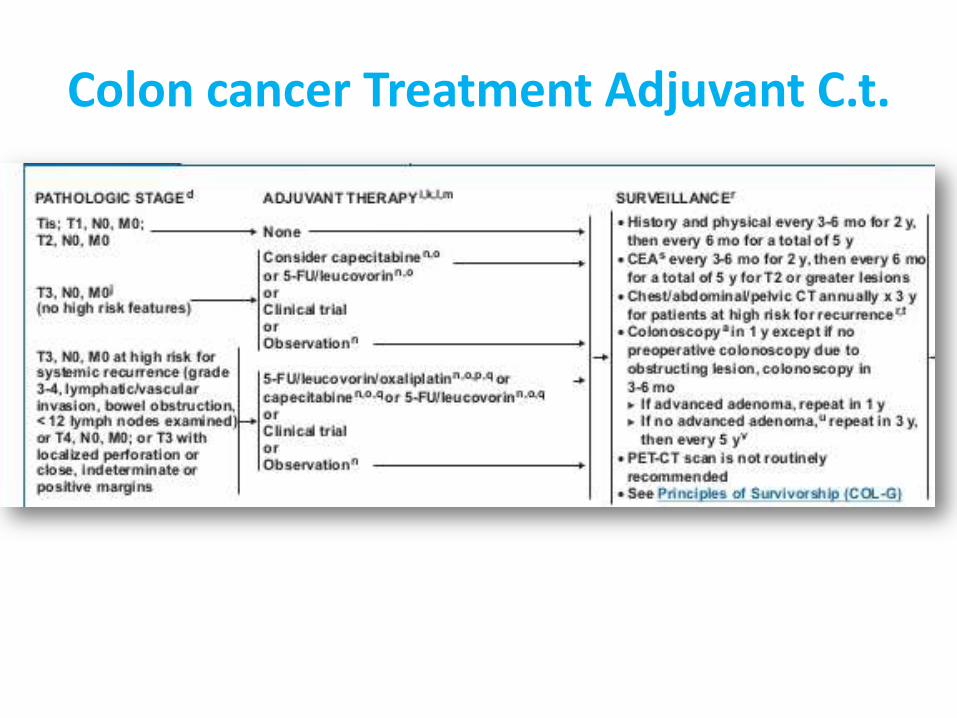
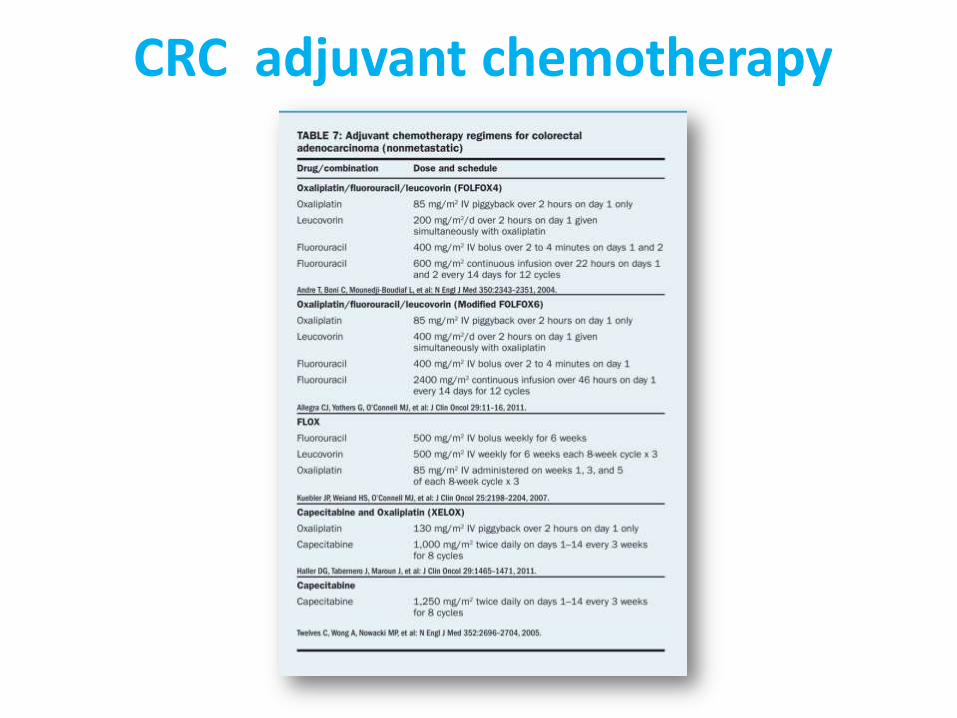
Colon cancer Treatment Adjuvant C.t.
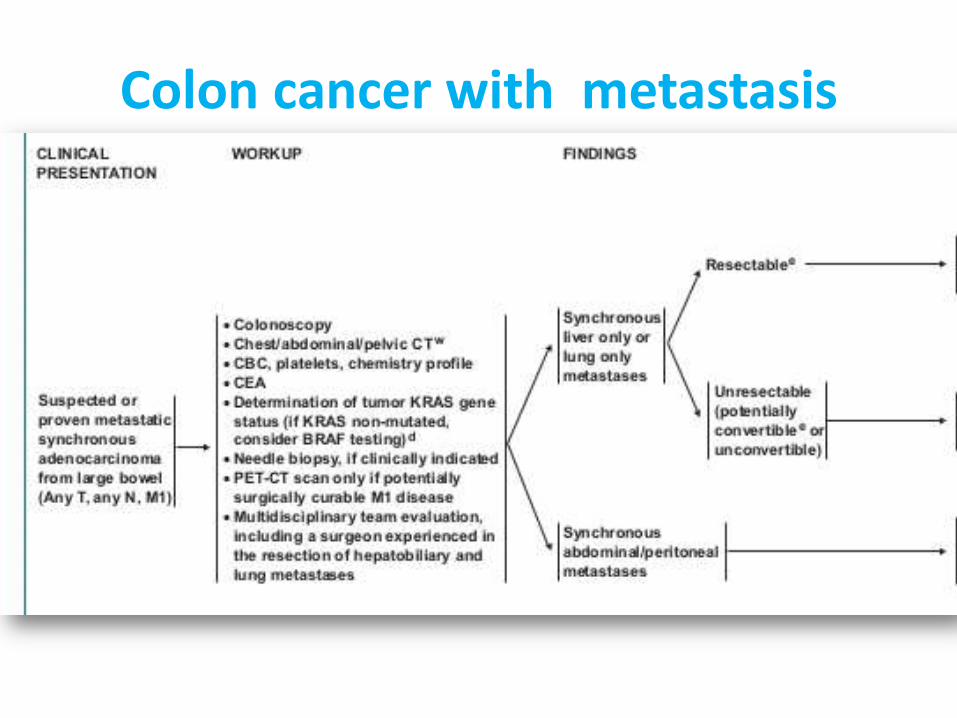
Colon cancer with metastasis
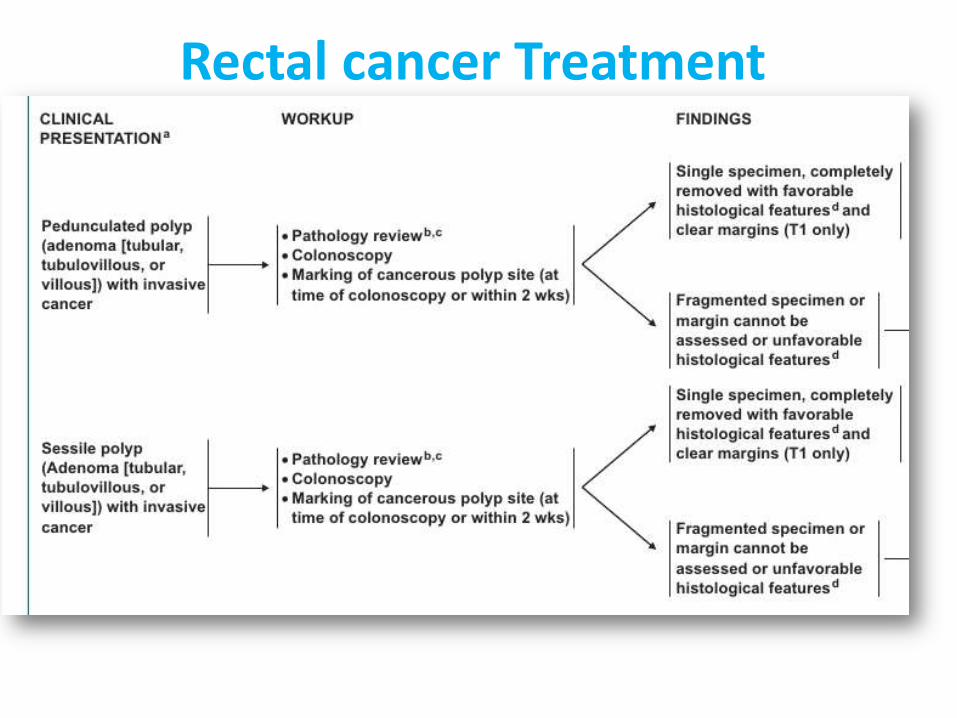
Rectal cancer Treatment
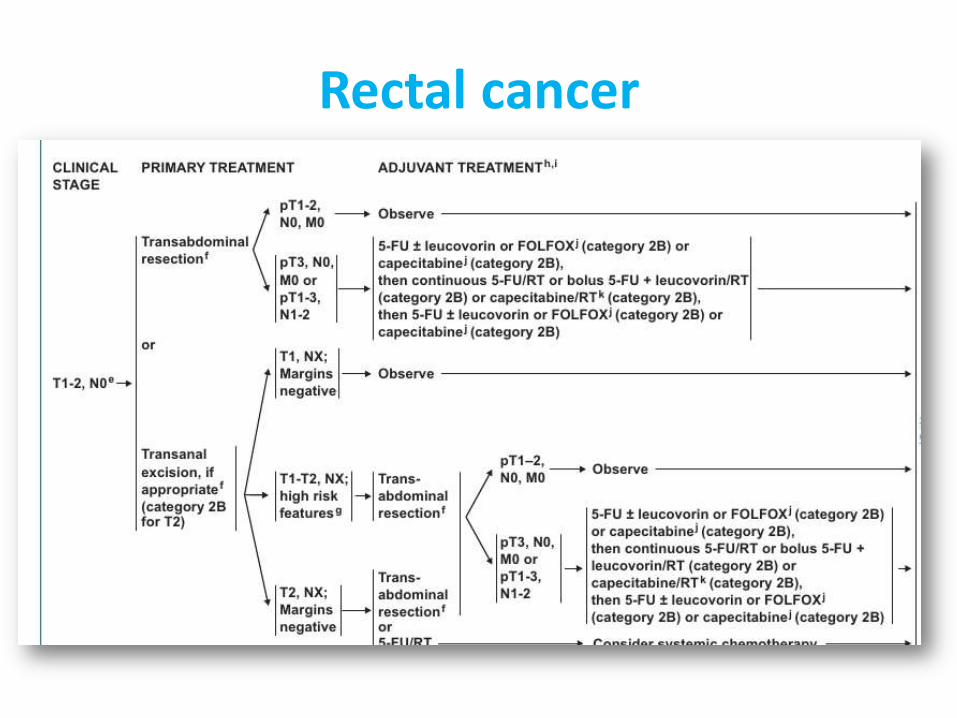
Rectal cancer
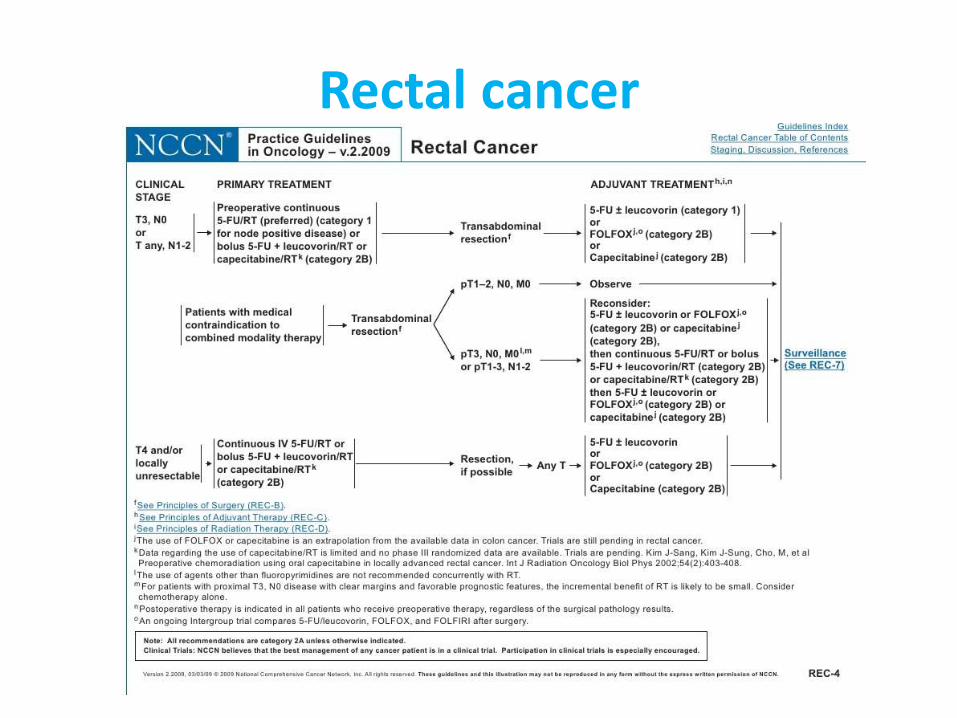
Rectal cancer
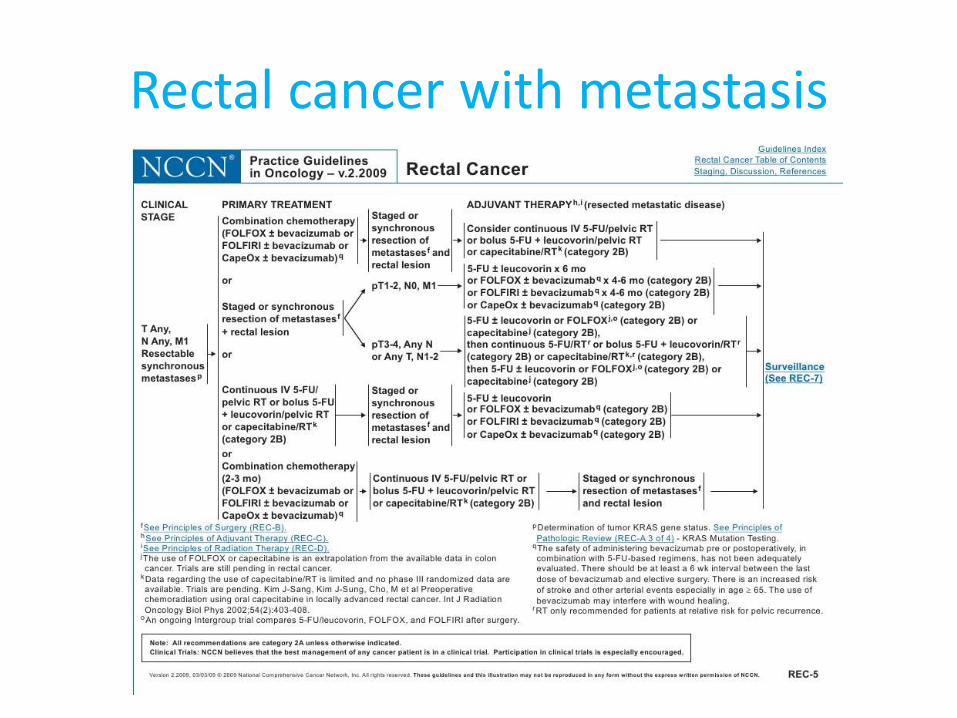
Rectal cancer with metastasis
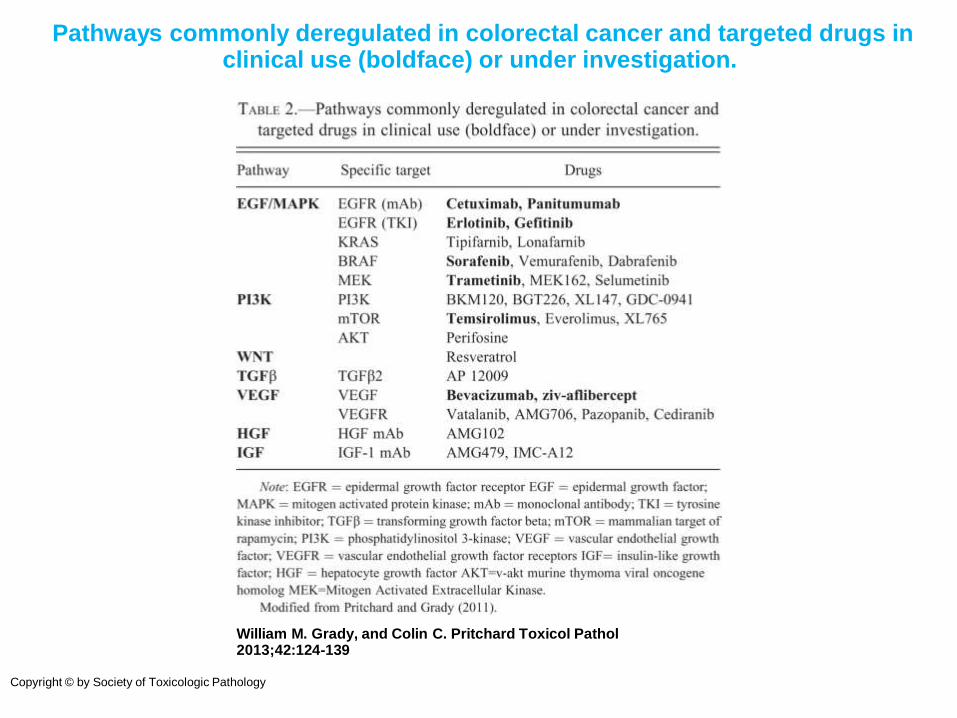
Pathways commonly deregulated in colorectal cancer and targeted drugs in clinical use (boldface) or under investigation.
William M. Grady, and Colin C. Pritchard Toxicol Pathol 2013;42:124-139
Copyright © by Society of Toxicologic Pathology
Anti EGFR and VEGF • Cetuximab (Erbitux) and panitumumab (Vectibix) are directed against the
epidermal growth factor receptor (EGFR), a transmembrane glycoprotein involved in signaling pathways affecting growth and proliferation of tumor cells.
• Both cetuximab and panitumumab, when given alone, have been shown to benefit a small proportion of previously treated patients, and cetuximab appears to have therapeutic synergy with such chemotherapeutic agents as irinotecan, even in patients previously resistant to this drug;
• Bevacizumab (Avastin) is a monoclonal antibody directed against the vascular endothelial growth factor (VEGF) and is thought to act as an anti-angiogenesis agent.
• The addition of bevacizumab to irinotecan-containing combinations and to FOLFOX improves the outcome observed with the chemotherapy alone. The use of bevacizumab can lead to hypertension, proteinuria, and an increased likelihood of thromboembolic events.
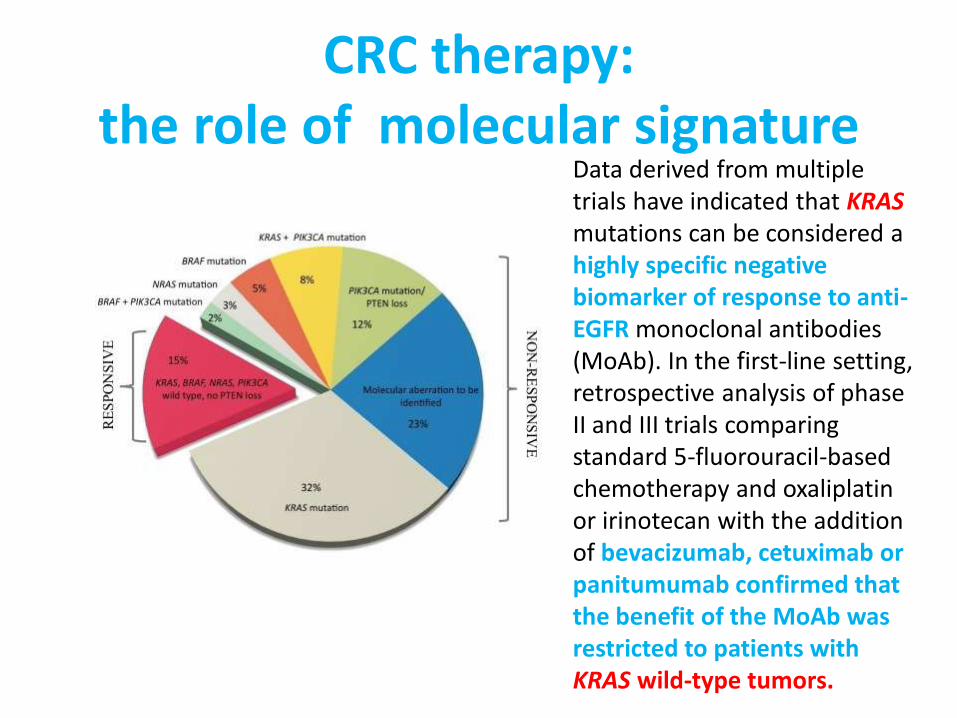
CRC therapy: the role of molecular signature
Data derived from multiple trials have indicated that KRAS mutations can be considered a highly specific negative biomarker of response to anti-EGFR monoclonal antibodies (MoAb). In the first-line setting, retrospective analysis of phase II and III trials comparing standard 5-fluorouracil-based chemotherapy and oxaliplatin or irinotecan with the addition of bevacizumab, cetuximab or panitumumab confirmed that the benefit of the MoAb was restricted to patients with KRAS wild-type tumors.
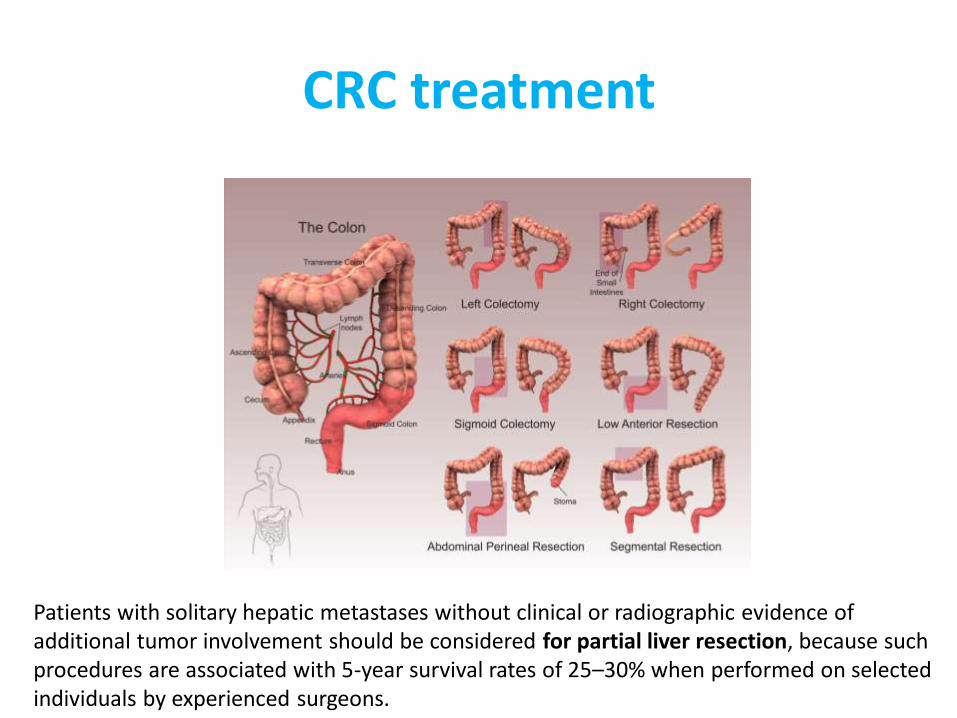
CRC treatment
Patients with solitary hepatic metastases without clinical or radiographic evidence of additional tumor involvement should be considered for partial liver resection, because such procedures are associated with 5-year survival rates of 25–30% when performed on selected individuals by experienced surgeons.

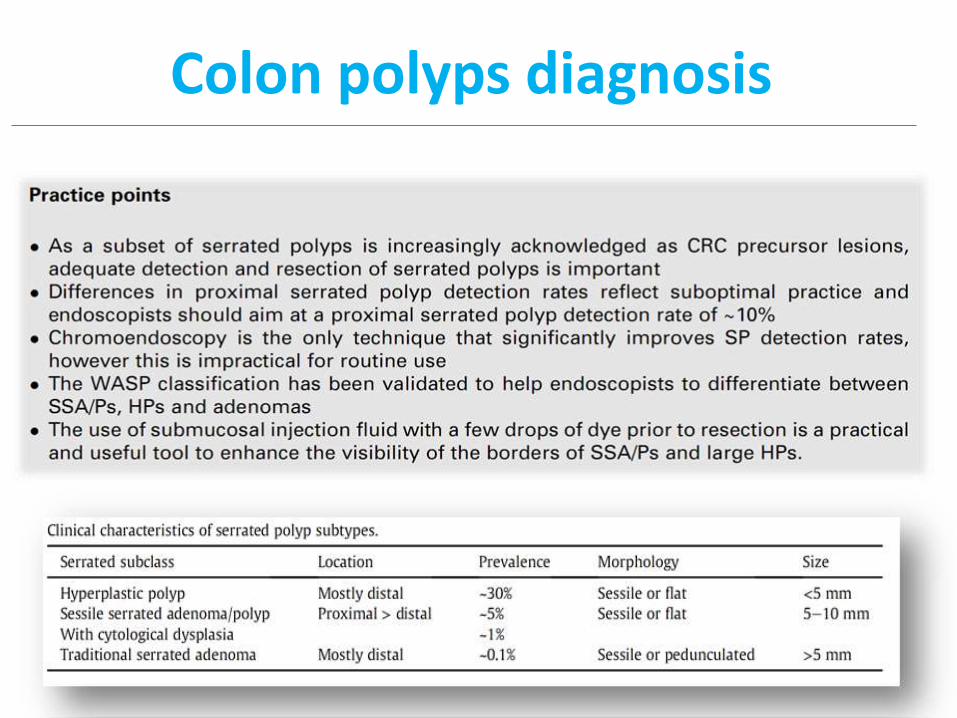
Colon polyps diagnosis
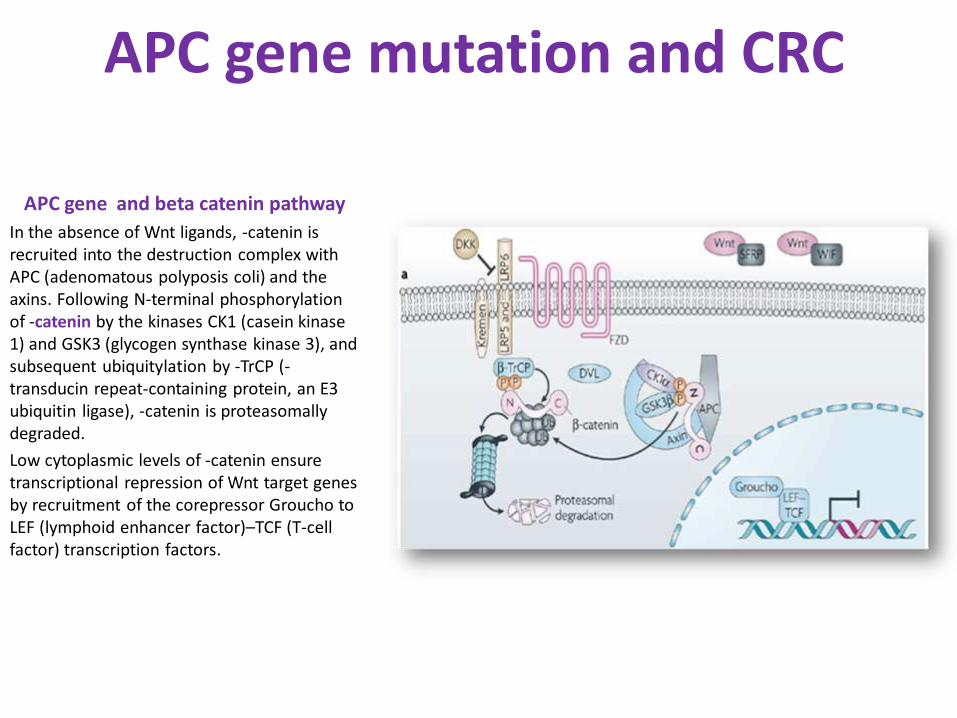
APC gene and beta catenin pathway
In the absence of Wnt ligands, -catenin is recruited into the destruction complex with APC (adenomatous polyposis coli) and the axins. Following N-terminal phosphorylation of -catenin by the kinases CK1 (casein kinase 1) and GSK3 (glycogen synthase kinase 3), and subsequent ubiquitylation by -TrCP (-transducin repeat-containing protein, an E3 ubiquitin ligase), -catenin is proteasomally degraded.
Low cytoplasmic levels of -catenin ensure transcriptional repression of Wnt target genes by recruitment of the corepressor Groucho to LEF (lymphoid enhancer factor)–TCF (T-cell factor) transcription factors.
APC gene mutation and CRC
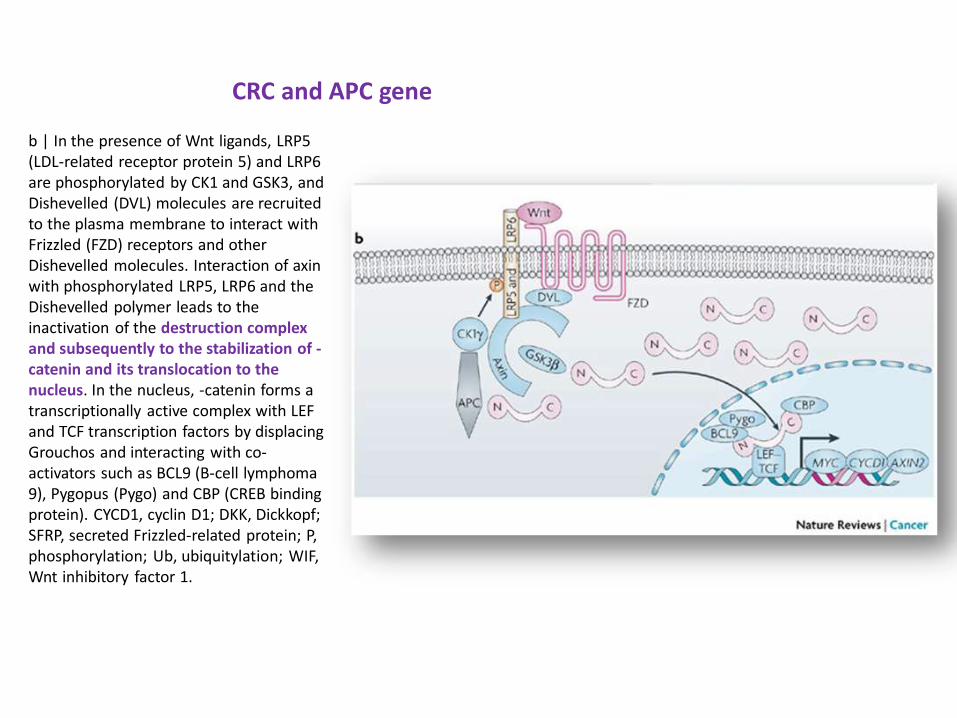
CRC and APC gene
b | In the presence of Wnt ligands, LRP5 (LDL-related receptor protein 5) and LRP6 are phosphorylated by CK1 and GSK3, and Dishevelled (DVL) molecules are recruited to the plasma membrane to interact with Frizzled (FZD) receptors and other Dishevelled molecules. Interaction of axin with phosphorylated LRP5, LRP6 and the Dishevelled polymer leads to the inactivation of the destruction complex and subsequently to the stabilization of -catenin and its translocation to the nucleus. In the nucleus, -catenin forms a transcriptionally active complex with LEF and TCF transcription factors by displacing Grouchos and interacting with co-activators such as BCL9 (B-cell lymphoma 9), Pygopus (Pygo) and CBP (CREB binding protein). CYCD1, cyclin D1; DKK, Dickkopf; SFRP, secreted Frizzled-related protein; P, phosphorylation; Ub, ubiquitylation; WIF, Wnt inhibitory factor 1.
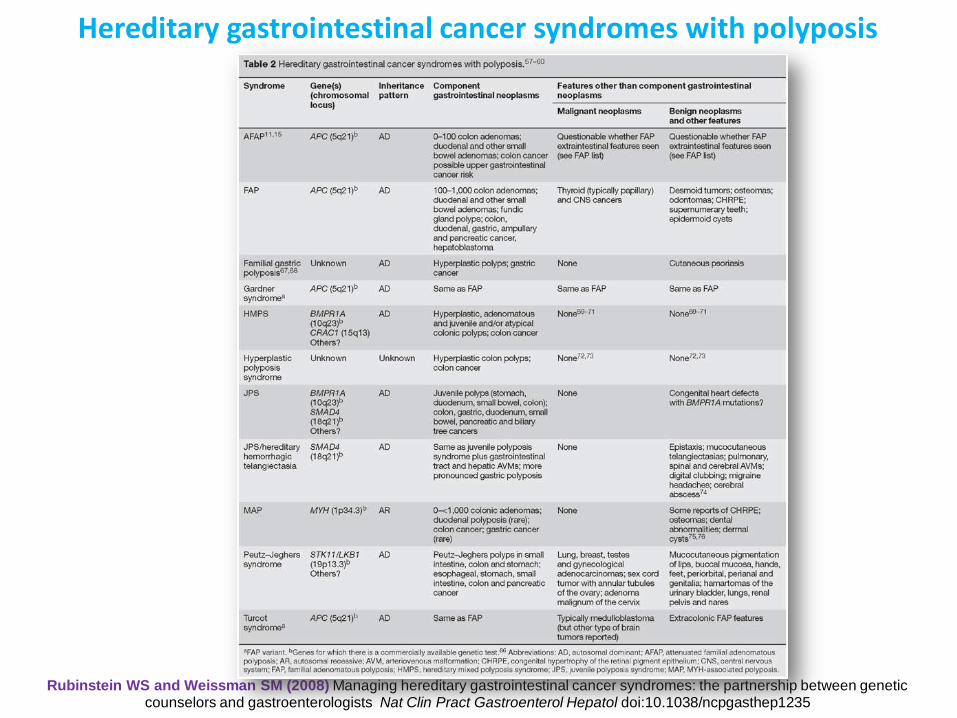
Rubinstein WS and Weissman SM (2008) Managing hereditary gastrointestinal cancer syndromes: the partnership between genetic counselors and gastroenterologists Nat Clin Pract Gastroenterol Hepatol doi:10.1038/ncpgasthep1235
Hereditary gastrointestinal cancer syndromes with polyposis
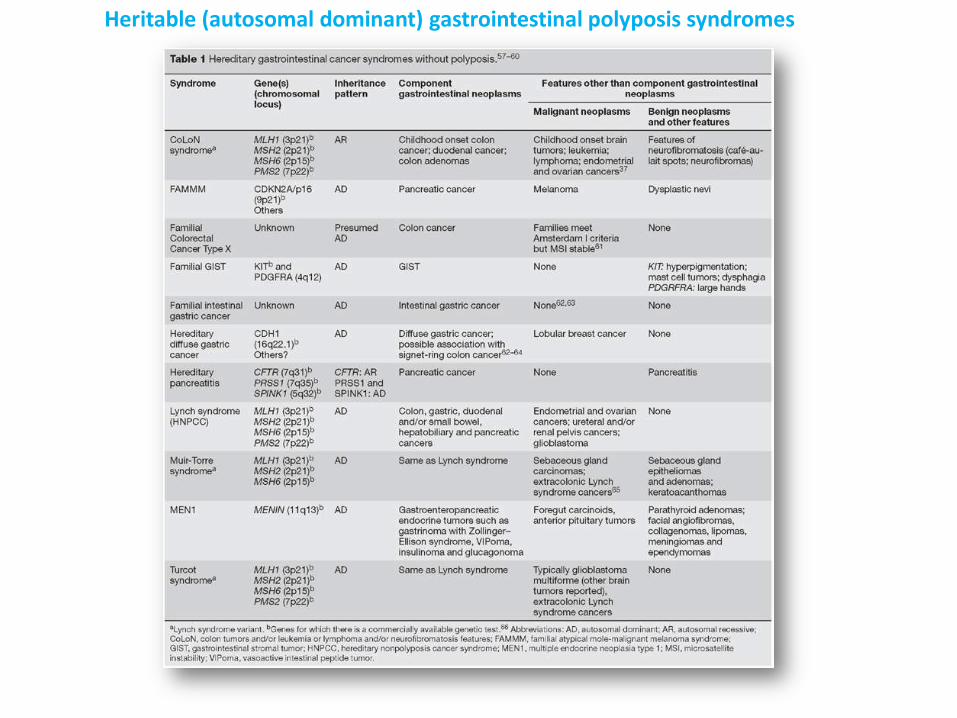
Heritable (autosomal dominant) gastrointestinal polyposis syndromes





![Prevalence of Colorectal Polyps: A Retrospective Study to …€¦ · to be an average of 10 years [3, 4]. The detection and removal of . polyps early in the polyp-cancer sequence](https://img.pdfslide.net/doc/110x75/5f4d8b0668593756d475d0c6/prevalence-of-colorectal-polyps-a-retrospective-study-to-to-be-an-average-of-10.jpg)