Embed Size (px)
Citation preview
COMBATING S CO G OSEVERE COAGULOPATHY
Piya SamankatiwatyRamathibodi hospital
Haemostasis Haemostasis
MechanismsEndothelium and Vascular functionPl t l t t d f tiPlatelet amount and functionCoagulation factorsCoagulation factorsFibrinolysis y
Vascular functionVascular function
Endothelial responseVasoconstrictionM di t Mediators
Platelet functionPlatelet function
Adequate amount of plateletPlatelet activation and adhesionPl t l t tiPlatelet aggregationStimulation of coagulation factors Stimulation of coagulation factors through platelet factor
Coagulation factorsCoagulation factors
Intrinsic pathwayExtrinsic pathway
Current concept on haemostasis byCurrent concept on haemostasis by coagulation factors
Substrates:Vascular injury: exposure of tissue factorContact of tissue factor and factor VIIaActivation of plateletsActivation of factor VIIProthrombinFibrinogen
Thrombin burstThrombin burst
C t t f Current concept of coagulationcoagulation
Initiation phaseAmplification phaseP ti hPropagation phase
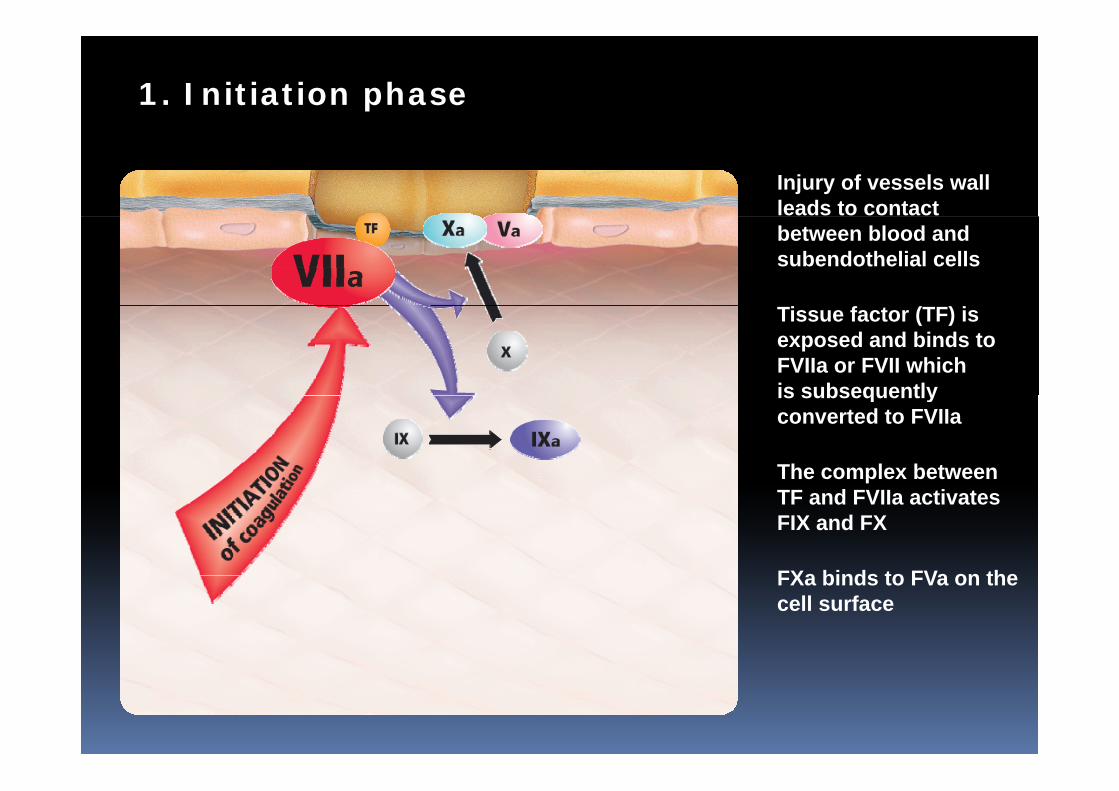
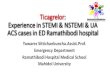
1. Initiation phase
Injury of vessels wallleads to contact between blood and subendothelial cells
Tissue factor (TF) isexposed and binds toFVIIa or FVII whichis subsequently
The complex between
is subsequently converted to FVIIa
FXa binds to FVa on the
TF and FVIIa activates FIX and FX
FXa binds to FVa on thecell surface
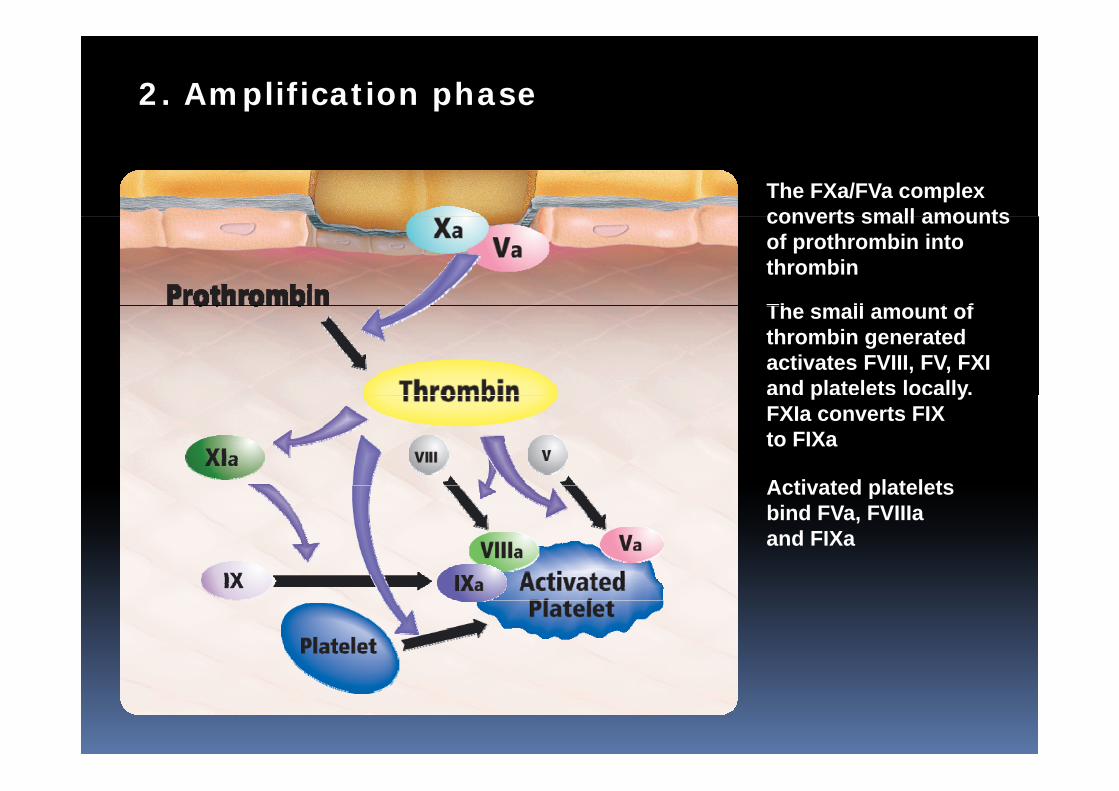
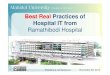
2. Amplification phase
The FXa/FVa complexconverts small amountsconverts small amountsof prothrombin intothrombin
Th ll t fThe small amount ofthrombin generatedactivates FVIII, FV, FXIand platelets locally.p yFXIa converts FIX to FIXa
Activated plateletsActivated plateletsbind FVa, FVIIIaand FIXa
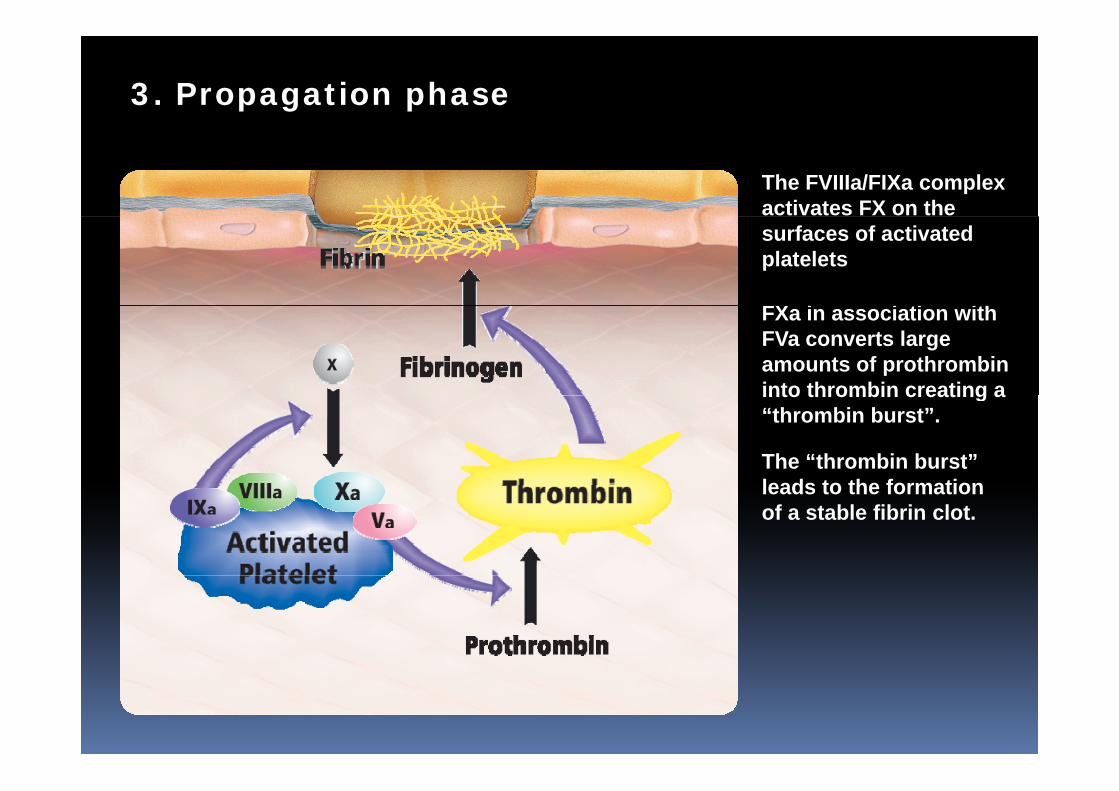
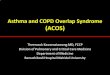
3. Propagation phase
The FVIIIa/FIXa complexactivates FX on thesurfaces of activatedplatelets
FX i i ti ithFXa in association withFVa converts largeamounts of prothrombininto thrombin creating ainto thrombin creating a “thrombin burst”.
The “thrombin burst”leads to the formationleads to the formationof a stable fibrin clot.
Summary of haemostasisSummary of haemostasis
Endothelium and vascular functionPlatelet amount and functionSti l ti f l ti f tStimulation of coagulation factors
Coagulopathy Coagulopathy
DefinitionClotting (coagulation) disorderAb lit f h t iAbnormality of haemostasis
CausesCauses
Acquired: liver failure, usage of lanticoagulant, etc
Autoimmune cause of acquired Autoimmune cause of acquired disorder: antiphospholipid p p psyndromeGenetics: abnormal production of clotting factors e g haemophiliaclotting factors e.g. haemophilia
Bl di di d Bleeding disorder Platelet disordersCoagulation disordersCoagulation disordersHyperfibrinolysis Medication‐induced coagulopathyAnaemia; severeAnaemia; severe
Coagulopathyg p yThrombocytopaenia and purpura
Nonthrombocytopaenic purpura: Henoch Schönlein purpuraNonthrombocytopaenic purpura: Henoch‐Schönlein purpuraThrombocytopaenic purpura: ITP (Evans syndrome)TM (TTP)( )Heparin‐induced thrombocytopenia ∙May‐Hegglin anomaly
Platelet functionadhesion (Bernard‐Soulier syndrome) ∙aggregation (Glanzmann's thrombasthenia)platelet storage pool deficiency (Hermansky Pudlakplatelet storage pool deficiency (Hermansky‐Pudlaksyndrome,Gray platelet syndrome)
Clotting factorgHemophilia (A/VIII, B/IX, C/XI)Von Willebrand diseaseH th bi i /II XIIIHypoprothrombinemia/II ∙XIII
Platelet disordersPlatelet disordersHereditary platelet dysfunctionHereditary platelet dysfunction
Disorder of adhesionBernard‐Soulier Syndrome: a deficiency on the surface of the platelet in an area called Glycoprotein Ib/IX platelet in an area called Glycoprotein Ib/IX
Disorder of aggregationGlanzmannThrombasthenia: life‐threatening. a deficiency of a protein on the surface of the platelet called Glycoprotein protein on the surface of the platelet, called Glycoprotein IIb/IIIa
Disorder of secretion:Delta storage pool deficiencyDelta storage pool deficiencyGray platelet syndrome
Disorder of platelet procoagulant activityScott syndromeScott syndrome
Combination of disorder of number and activity: May‐HegglinAnomaly Alport Syndrome Alport Syndrome Wiskott‐Aldrich Syndrome.
Platelet disordersPlatelet disordersAcquired platelet disorders in number and functions:q pThrombocytopaenia: immune thrombocytopaenic purpura (ITP)Platelet function can be affected by common drugs.
Aspirin (ASA) and other drugs containing aspirin p g g pNon‐steroidal anti‐inflammatory drugs like indomethacin, ibuprofen and naproxen Ticlopidine
Other drugs can also affect platelet function These include: Other drugs can also affect platelet function. These include: Some antibiotics Cardiovascular drugs Antidepressants A th tiAnaestheticsAntihistamines
Platelet function returns to normal when these medications are stopped. ppCertain medical conditions can cause abnormal platelet function.
Chronic kidney disease Cardiopulmonary bypass surgery S f f l k iSome forms of leukemiaRare causes: cardiac tumour
Coagulation factor disordersCoagulation factor disorders
Hereditary coagulation disorders:Haemophilia AHaemophilia AHaemophilia BHaemophilia CHaemophilia CVon‐Willebrand’s diseaseSerum prothrombin conversion accelerator (SPCA) Serum prothrombin conversion accelerator (SPCA) deficiency
HypoprothrombinaemiaHypoprothrombinaemiaDisseminated intravascular coagulation
Drug induced haemostatic Drug‐induced haemostatic disordersdisorders
Anti‐platelet therapyAspirinClopidogrel (Plavix®)Glycoprotein (GP) IIb/IIIa inhibitors
Anticoagulants t coagu a tsHeparin and LMWHOral anticoagulant: warfarinOral anticoagulant: warfarin
Thrombolytic agents: streptokinase/ urokinase
Effects of CPB on coagulationEffects of CPB on coagulation
Heparin effectHeparin reboundHeparin‐induced thrombocytopaenia (HIT I & II)Consumption of platelets and clotting factorsHyperfibrinolysisHypothermiaHaemodilution Systemic inflammatory response
Perioperative evaluation ofPerioperative evaluation of coagulopathycoagulopathy
History and physical examination
History of medications
Complete blood countComplete blood count
Evaluation of platelet function
Evaluation of coagulating factor
Evaluation of fibrinolysisy
Preoperative evaluation ofPreoperative evaluation of coagulopathyg p y
History and physical examination
Reliable and increases sensitivity and specificity of haemostasis testsSimple systematic questionnaire
A simple screening questionnairep g q
have you ever bled for a long time or developed a swollen tongue or mouth after cutting or biting your tongue, cheek or lip?g g y g pdo you develop bruises larger than «a silver dollar» without being able to remember when or how you injured yourself ? If so, how big was the largest of these bruises?ho man times ha e o had teeth p lled and hat as the how many times have you had teeth pulled and what was the longest time that you bled after an extraction? Has bleeding ever started up again the day after extraction?what operations have you had, including minor surgery such as skin p y , g g ybiopsies? Was bleeding after surgery ever hard to stop ? Have you ever developed unusual bruising in the skin around an area of surgery or injury?have you had a medical problem within the past 5 yr requiring a have you had a medical problem within the past 5 yr requiring a doctor’s care? If so, what was its nature?what medications including aspirin or any other remedies for headaches, cold, menstrual cramps or other pains have you taken i hi h d ?
p p ywithin the past 7‐9 days?has any blood relative had a problem with unusual bruising or bleeding after surgery? Were blood transfusions required to control this bleeding?this bleeding?
Preoperative evaluation ofPreoperative evaluation of coagulopathyg p y
Complete blood countHaematocritHaematocrit
Evaluation of platelet number and functionPlatelet countPlatelet countBleeding time
Evaluation of coagulating factorsEvaluation of coagulating factorsProthrombin time (PT)Partial thromboplastin time (PTT)Partial thromboplastin time (PTT)
Evaluation of fibrinolysis
IntraIntra‐‐opertiveopertiveppmanagement of bleedingmanagement of bleeding
Intraoperative monitoring of Intraoperative monitoring of haemostasis
A large prospective trial in cardiac surgery used two bed‐side monitors at the same time : the Coaguchek® g(APTT,PT) and the T 540® (PC) to set up an algorithm for platelet concentrates and fresh frozen plasma infusion. The use of the products was guided by the instantaneous p g yresults provided by the monitors. Received significantly less intraoperative fresh frozen plasma (0.4±1.1 U vs 2.4±2.8 U)p ( 4 4 )Shorter operation times and less mediastinal chest tube drainage in the early perioperative timeAlso received fewer platelets (1 6±5 9) vs 6 4±8 2 U) and Also received fewer platelets (1.6±5.9) vs 6.4±8.2 U) and red blood cell transfusions after the operation.
Despotis GJ et al : Prospective evaluation and clinical utility of on‐site monitoring of coagulation in patients undergoing cardiac operations. J Thorac Cardiovasc Surg 1994; 107: 271‐279
Intra operative managementIntra‐operative management
Prevention:Meticulous surgical technique and haemostasis is g qthe most important.Pharmacologic method: aprotinin, transexamic a.g p ,Mechanical: heparin‐coated circuitSIRS: leucocyte‐reduction filterSIRS: leucocyte‐reduction filter
Intra operative managementIntra‐operative management
h iTherapeutic:Addition doses of protamineAprotininAntifibrinolytics: Tranexamic acid, epsilon‐y , paminocaproic acid Recombinant factor VIIaeco b a t acto aLocal haemostats: Floseal®, Coseal®, oxidised cellulose (Surgicel®), Gelfoam®, Bio‐glue® and cellulose (Surgicel ), Gelfoam , Bio glue and fibrin glue
ProtamineProtaminePolycationic peptide isolated from sperm of Polycationic peptide isolated from sperm of salmonCounteract the effects of heparin and is usually Counteract the effects of heparin and is usually given in a 1:1 (1.3‐1.5 : 1) mg/mg ratio to return the ACT to baseline.Despite complete neutralisation of heparin, the ACT may remain elevated in patients with significant thrombocytopenia or coagulopathy significant thrombocytopenia or coagulopathy. Moderate thrombocytopenia has not been shown to increase the ACT in patients with s o to c ease t e C pat e ts tnormally functioning platelets, it does seem to increase it when associated with platelet dysfunction after bypassdysfunction after bypass.
AprotininAprotininSerine proteases inhibitor Polypeptide molecule F l b d i h i i f i Forms complex bond with active serine of various protease molecules e.g. trypsin, kallikrein, plasminThe most potent antifibrinolytic agent: The most potent antifibrinolytic agent: Aprotinin 4 µmol/L can inhibit "intrinsic" fibrinolysisof activated kallikrein and can inhibit plasmin from
f l b“extrinsic" or activation of plasminogen by tissue plasminogen activator (tPA)Also exhibit anti inflammatory effects Also exhibit anti‐inflammatory effects Remark: withdrawn from FDA due to serious complicationsp
AprotininAprotinin
(1) High dose: 2 million KIU prior to heparinisationp p2 million KIU in pump prime0.5 million KIU/h5
(2) Low dose: half of above(3) Weight adjusted: (3) Weight adjusted:
3.5 mg/kg IV bolus i l d70 mg pump prime load
3.5 mg/kg/h for 1 hour /k /h ti i f i1 mg/kg/h continuous infusion
Tranexamic acid and epsilon‐aminocaproicid ( )acid (EACA)
Th i t d i f t i id i t The appropriate dosing of tranexamic acid is not well defined. 10 mg/kg over 20 minutes followed by a 1 mg/kg/h 10 mg/kg over 20 minutes followed by a 1 mg/kg/h Infusion1 g bolus followed by an infusion of 400 mg/h with 500 mg in the pump prime500 mg in the pump prime.Another study showed that one dose of 100 mg/kg given before CPB was very effective in reducing g y gbleeding. For EACA ft th i d ti f th i 5 g after the induction of anesthesia, 5 g on pump,
and 1 g/h during the procedure. Giving a 5–10‐g dose only at the time of Giving a 5 10 g dose only at the time of heparinization for bypass also reduces blood loss.
PostopertivePostopertive management management pp ggof bleedingof bleeding
Causes of excessive bleeding Causes of excessive bleeding after cardiac surgeryg y
Inadequate surgical haemostasisProlonged bypass timeProlonged bypass timePlatelet dysfunction or consumption (dilutional thrombocytopenia)Excessive hemostatic activationcess e e ostat c act at oExposure to long‐acting antiplatelet or antithrombotic agentsantithrombotic agents.
Levy JH, Tanaka KA, Steiner ME.
Evaluation and management of bleeding during cardiac surgery.
Curr Hematol Rep. 2005 Sep;4(5):368-72.
“Excessive bleeding after cardiac surgery occurs because of alterations in the occurs because of alterations in the hemostatic system pertaining to dilutional thrombocytopenia excessive hemostatic thrombocytopenia, excessive hemostatic activation, and exposure to long‐acting
ti l t l t tith b ti t ” antiplatelet or antithrombotic agents.”
Recognition of bleeding disorder: Testsg f g
Platelet function: bleeding time, platelet function analyser (PFA)function analyser (PFA)
Coagulogram: PT, aPTTBlood level of coagulation factors
Fibrinolytic activity testsb o y c ac y es s
Post operative assessmentPost‐operative assessment
Clinical evaluationConventional haemostatic assessment
Complete blood count with platelet countCoagulogram: PT, PTT, TT and INRAdditional tests(if required): D‐dimer, FDP, fibrinogen level
P i t f Point‐of‐care Activated clotting time (ACT)HHepconPFA‐100Thromboelastography (TEG)Thromboelastography (TEG)
ThromboelastographyThromboelastography
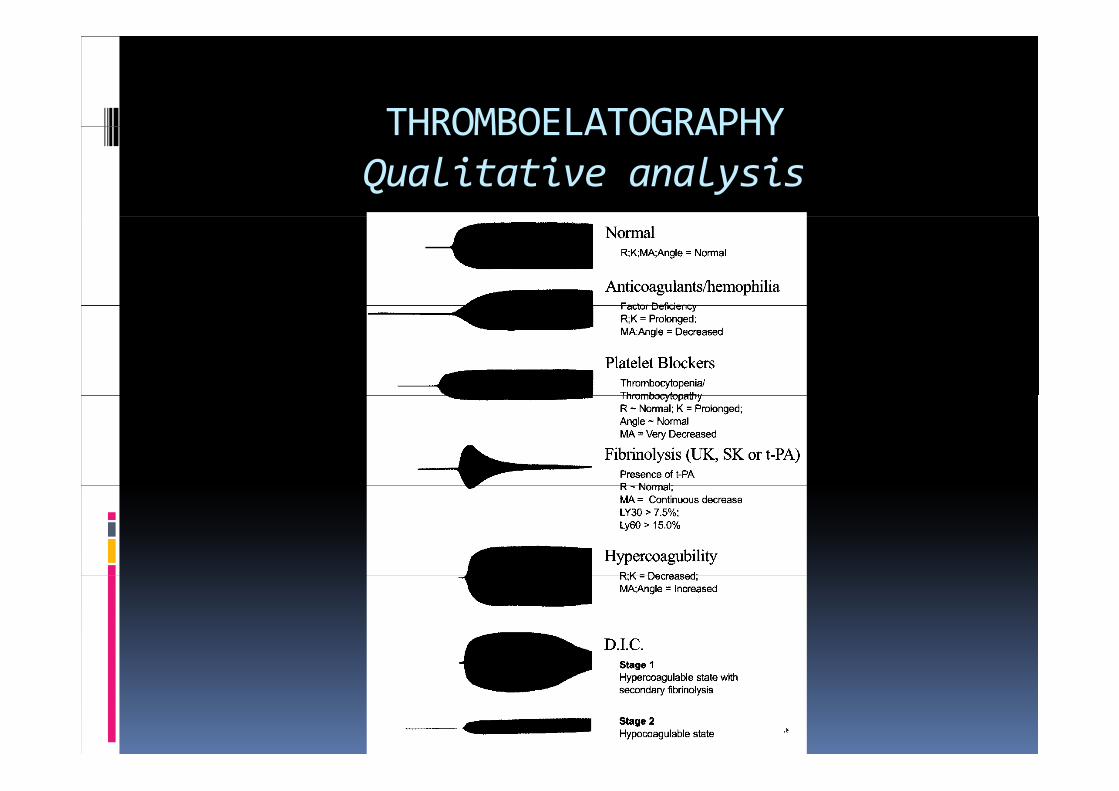
THROMBOELATOGRAPHYTHROMBOELATOGRAPHYQualitative analysis
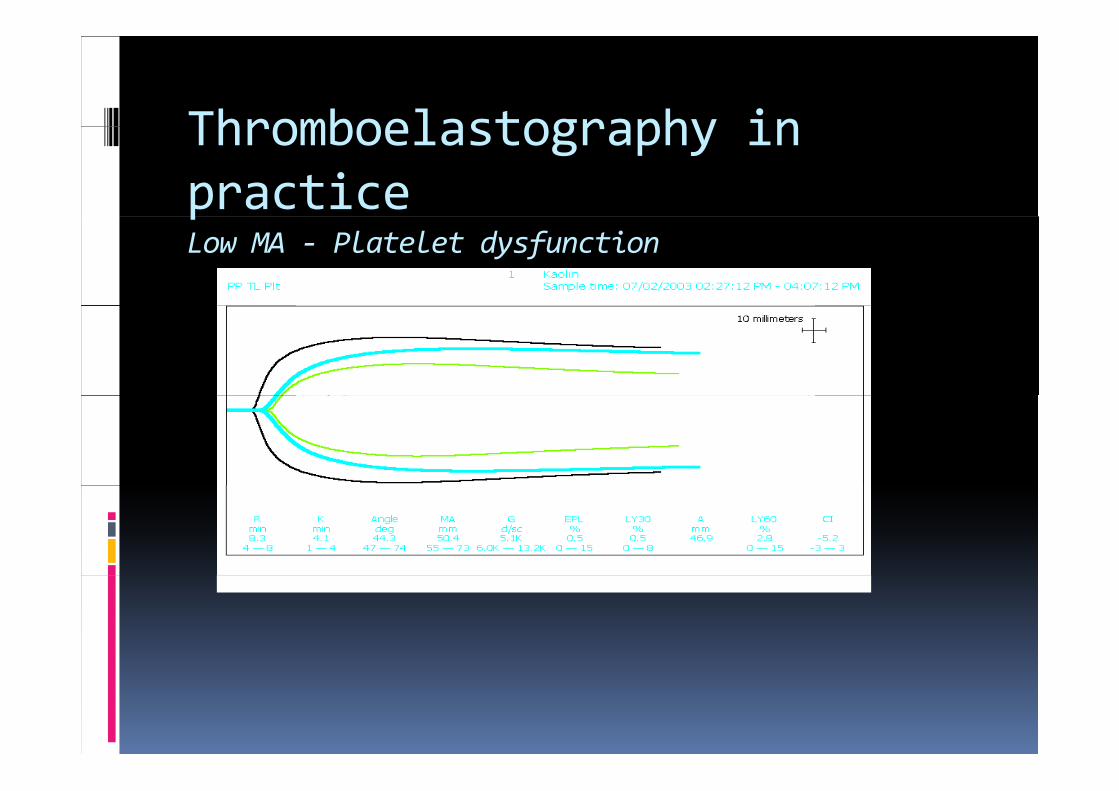
Thromboelastography in Thromboelastography in practicepLow MA ‐ Platelet dysfunction
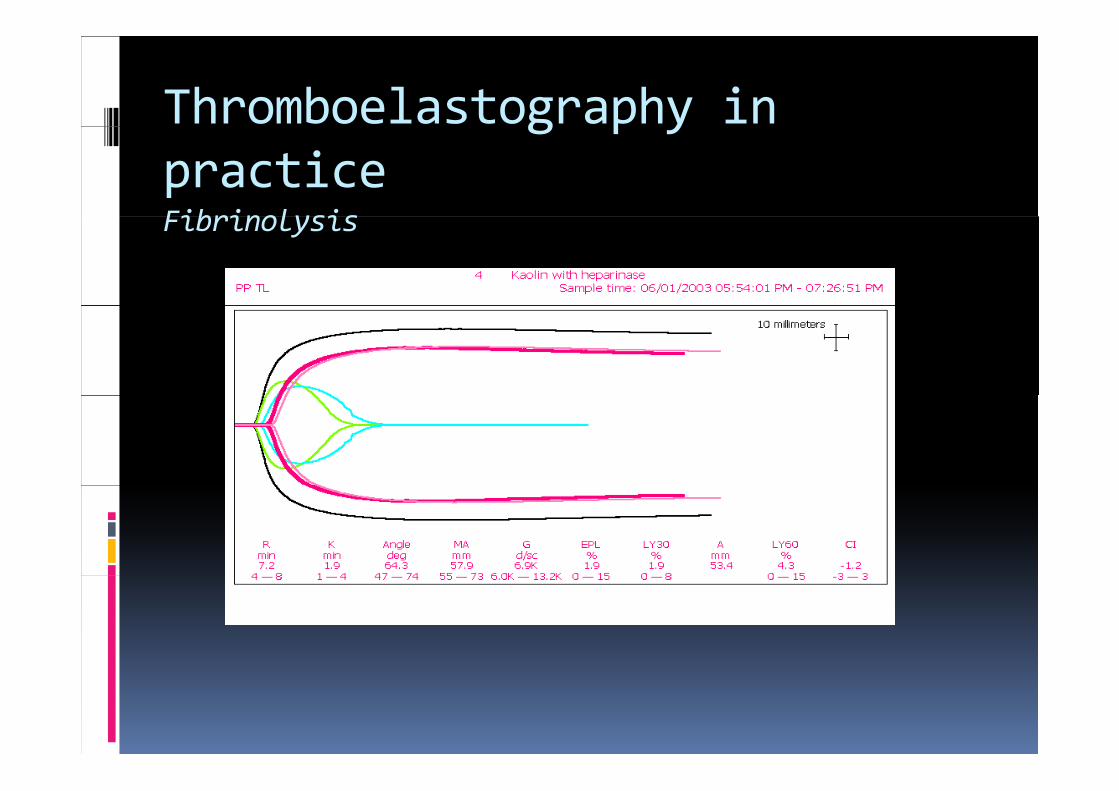
Thromboelastography in g p ypracticeFibrinolysisFibrinolysis
Advantages of TEG over conventional Advantages of TEG over conventional coagulation monitoring
It is dynamic, giving information on entire l i h h i l dcoagulation process, rather than on isolated
part
It gives information on areas which it is normally difficult to study easily – fibrinolysis and platelet function in particular
Near‐patient testing means results are rapid p g pfacilitating appropriate intervention
It is cost effective compared to conventionalIt is cost effective compared to conventional tests
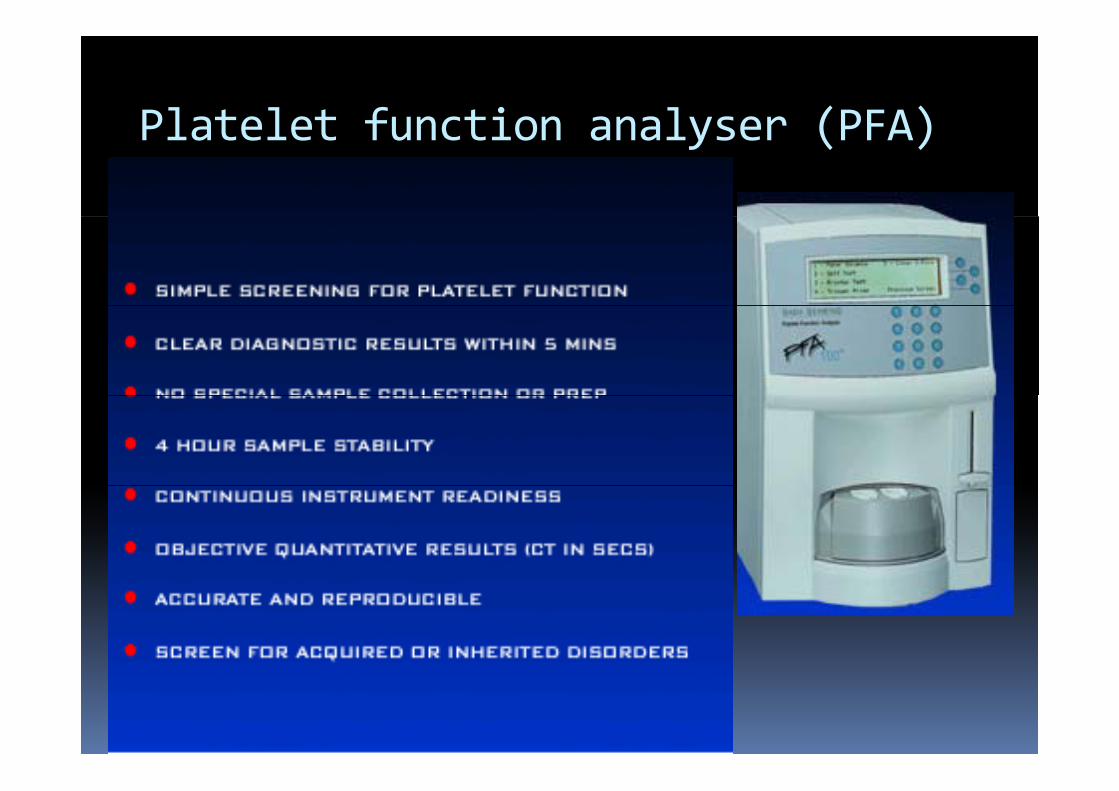
Platelet function analyser (PFA)Platelet function analyser (PFA)
Comparison of structured use of routine laboratory tests or near‐p ypatient assessment with clinical judgement in the management of bleeding after cardiac surgery
210 patients allocated in one of 3 groupsLaboratory guide algorithm (LGA n 51)Laboratory‐guide algorithm (LGA, n=51)Point‐of‐care (POC, n=51)Clinician discretion (n=108)Blood loss transfusion of blood and blood Blood loss, transfusion of blood and blood components
Avidan MS, Alcock EL, Da Fonseca J et al. BJA 2004, 92(2): 178‐86
Comparison of structured use of routine laboratory tests or near‐p ypatient assessment with clinical judgement in the management of bleeding after cardiac surgery
210 patients allocated in one of 3 groupsIn clinician discretion group had unnecessary In clinician discretion group had unnecessary transfusion although degree of blood loss was not different among groups.was not different among groups.In LAG and POC groups, algorithm was equally effective In contrast POC group had equally effective. In contrast, POC group had significantly less blood component use in previous studies previous studies.
Avidan MS, Alcock EL, Da Fonseca J et al. BJA 2004, 92(2): 178‐86
Point of care testsPoint‐of‐care tests
Targeting blood‐component therapy according to identified abnormalities in coagulation systemIdentifying patients who could benefit from pharmacologic interventionsIdentifying patients who have a surgical source of bleeding can be expedited if coagulation tests reveal relatively normal results in the setting of
i bl diexcessive bleeding.
Current therapeutic strategyCurrent therapeutic strategy
Fluid replacement to maintain adequate cardiac outputA id h th iAvoid hypothermiaAdequate haematocrit concentrationC l ti f t d l t l tCoagulation factors and plateletsPharmacological agents e.g. aprotinin, tranexamic acid (Transamin ®) epsilon‐aminocaproic acidacid (Transamin ), epsilon‐aminocaproic acid (EACA, amicar ®)Recombinant activated factor VII (rFVIIa,Recombinant activated factor VII (rFVIIa, NovoSeven ®)
HypothermiaHypothermia
Reversible reduction in platelet count and functionfunctionAltered coagulationEnhanced fibrinolysis At 25‐29 C, patients developed more t 5 9 C, pat e ts de e oped o eextensive bleeding than at normothermia.Prolonged bleeding time PT andPTTProlonged bleeding time, PT andPTT
Adequacy of haematocritAdequacy of haematocrit
Keep Hct at the level of 35 % (Hb 11 gm/dl)An adequate haematocrit is required for q qoptimum haemostasis. Red blood cells (RBC) have an established role in arterial thrombosis formation Escolar et al studied the effect of formation. Escolar et al. studied the effect of RBC and platelet count on the interaction of platelets with the subendothelium, using the p , gBaumgartner perfusion technique.Platelet aggregation was impaired when h t it d d t % d thi haematocrit was decreased to 20% and this was independent of platelet count.
Escolar G, Garrido M, Mazzara R, Castillo R, Ordinas A : Experimental basis for the use of red cell transfusion in the management of anemic‐thrombocytopenic patients. Transfusion 1988;
28 : 406‐411.
Roles of red blood cell in Roles of red blood cell in clot formation
Rheologic role: in living blood circulation, red blood cells circulate in the central flow while l t l t i th i h El ti platelets in the periphery. Elevating
haematocrit promotes the transport of platelets towards the vessel wall.platelets towards the vessel wall.Source of adenosine diphosphate (ADP) enhance platelet degranulationp gContain multiple cryptic adhesion receptorsCatalyse phosphatidylserine exposure needed y p p y pfor activation of coagulation cascadeMay express antithrombotic properties
Coagulation factors and Coagulation factors and plateletsp
Platelet concentrate 0.2 Unit/KgFFP 10 ml/KgFFP 10 ml/KgCryoprecipitate 0.2 Unit/Kg
Pharmacologic agentsPharmacologic agents
ProtamineAprotinin (Trasylol®)Aprotinin (Trasylol®)Tranexamic acidEpsilon‐aminocaproic acid
ProtamineProtamine
Additional dose will be given in case of prolonged ACT or PTTprolonged ACT or PTT1 mg/kg/dose intravenously
Tranexamic acid and epsilonTranexamic acid and epsilon‐aminocaproic acidp
In first‐time coronary revascularisationEACA and tranexamic acid decreased total EACA and tranexamic acid decreased total exposure to allogenic blood productsJustifying the routine use of synthetic antifibrinolyticsDose: 1‐4 mg/kg/dose
Hardy JF, Belisle S, Dupont C et al. Prophylactic tranexamic acid and epsilon‐aminocaproic acid for primary myocardial revascularization. Ann Thorac Surg 1998; 65
371‐6
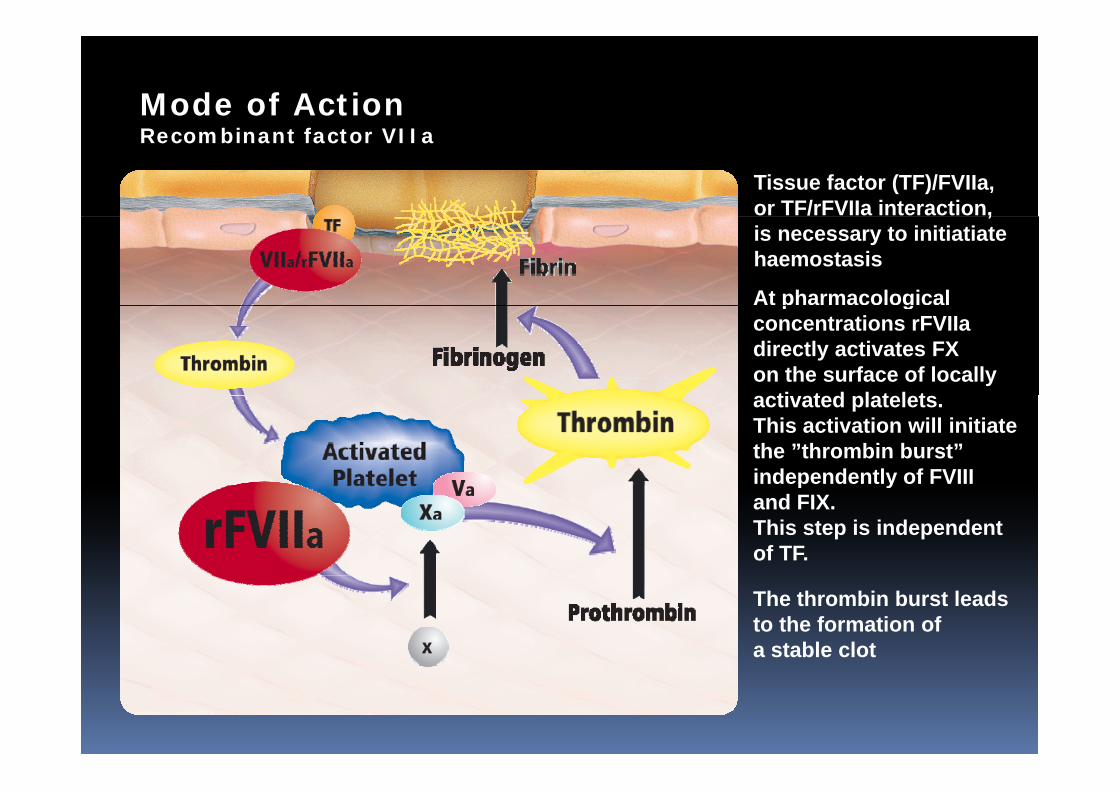
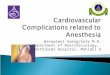
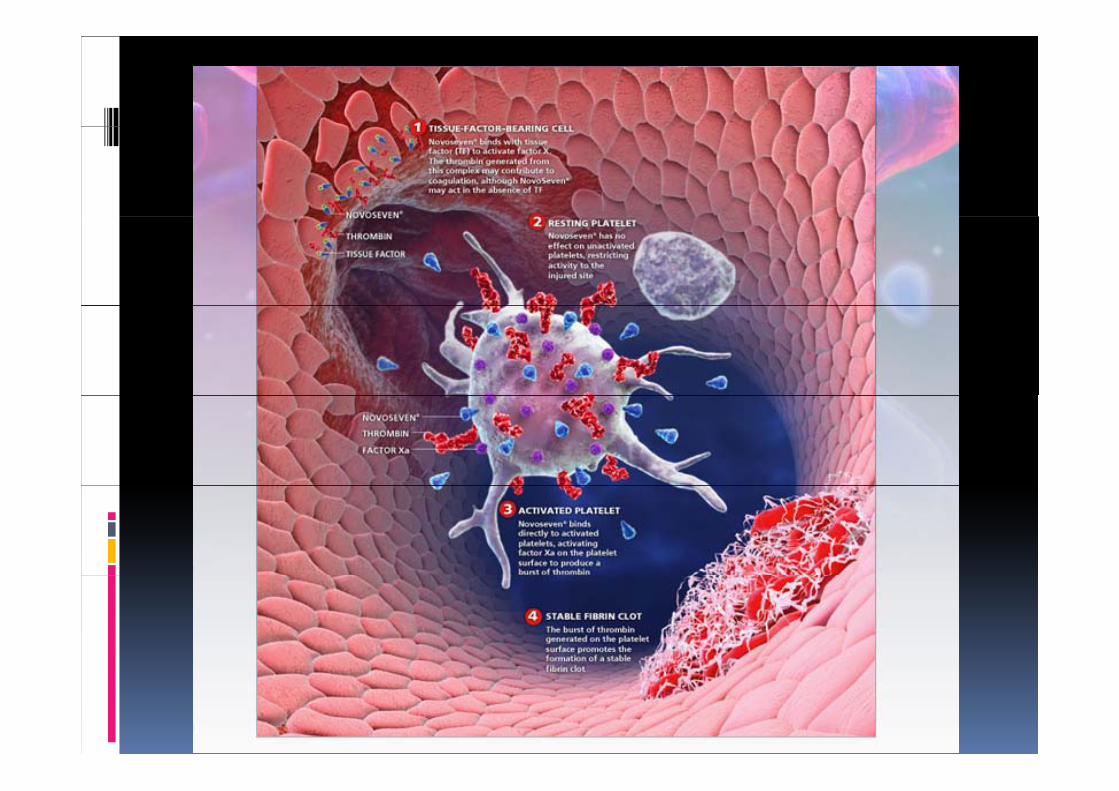
Mode of ActionRecombinant factor VIIa
Tissue factor (TF)/FVIIa,or TF/rFVIIa interaction,,is necessary to initiatiate haemostasis
At pharmacological p gconcentrations rFVIIa directly activates FX on the surface of locally
ti t d l t l tactivated platelets.This activation will initiatethe ”thrombin burst”independently of FVIII p yand FIX. This step is independent of TF.
The thrombin burst leads to the formation of a stable clot
Consider re opening if:Consider re‐opening if:
bleeding >200 ml/hr for 3‐4 hours or more than 5 % of blood volume per hourthan 5 % of blood volume per hourbleeding >400 ml/hr in 1 hour total loss > 1500‐2000 ml
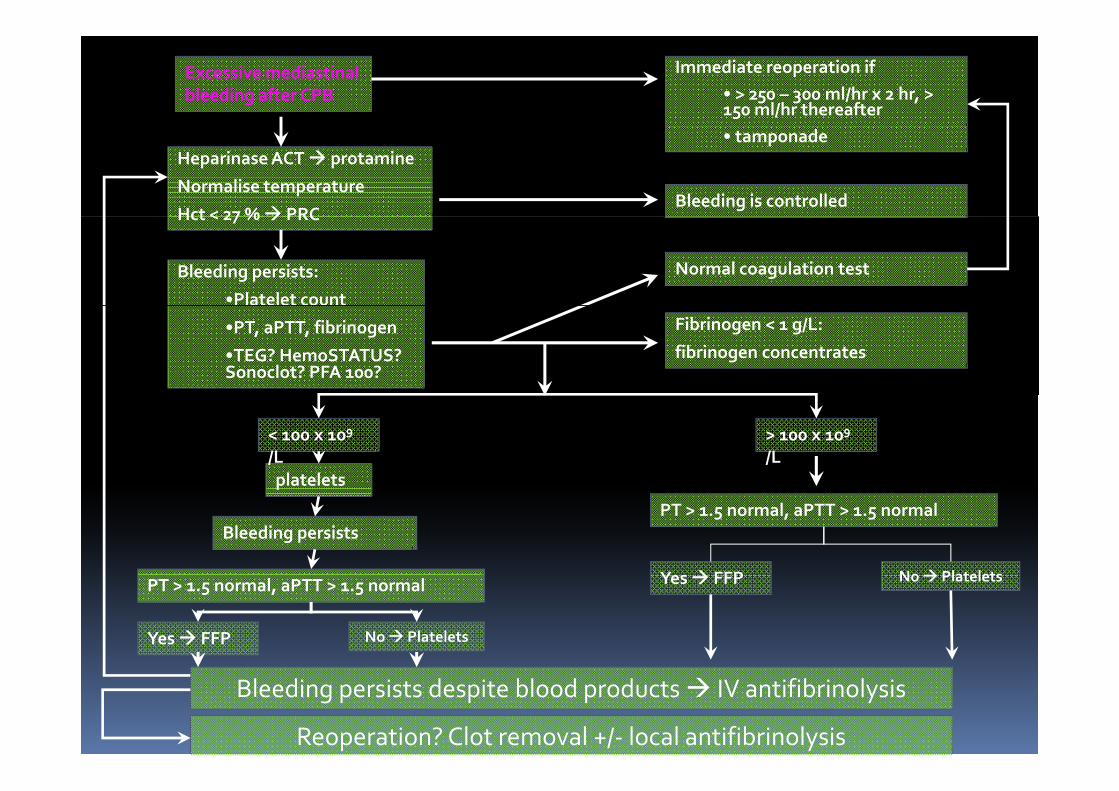
Excessive mediastinal bleeding after CPB
Immediate reoperation if• > 250 – 300 ml/hr x 2 hr, > 150 ml/hr thereafter
Heparinase ACT protamine
Normalise temperature
Hct < 27 % PRCBleeding is controlled
• tamponade
Bleeding persists:
•Platelet count
Hct < 27 % PRC
Normal coagulation test
•PT, aPTT, fibrinogen
•TEG? HemoSTATUS? Sonoclot? PFA 100?
Fibrinogen < 1 g/L:
fibrinogen concentrates
platelets
< 100 x 109
/L> 100 x 109
/Lplatelets
Bleeding persists
Yes FFP No Platelets
PT > 1.5 normal, aPTT > 1.5 normal
PT > 1.5 normal, aPTT > 1.5 normal
Yes FFP No Platelets
Yes FFP No Platelets
Bleeding persists despite blood products IV antifibrinolysis
Reoperation? Clot removal +/‐ local antifibrinolysis
Complications of blood transfusionComplications of blood transfusion
Immune‐mediated transfusion reactionsAcute H l iHaemolysisFebrile nonhaemolytic transfusion reaction (FNHTR)Acute lung injury (TRALI) leads to ARDSUrticariaAnaphylaxis
Delayede ayedAlloimmuneHaemolysisGraft‐versus‐host disease (GVHD)Graft‐versus‐host disease (GVHD)Platelet‐refractory
Prevention is the most crucial way in order to minimise transfusion complications.
Complications of blood transfusionComplications of blood transfusion
Non‐immune mediated transfusion reactionsAcute HaemolysisHaemolysisEmbolicMetabolic disorder: citrate toxicity, coagulopathy, hypothermia, hyperkalaemia hypocalcaemiahyperkalaemia, hypocalcaemiaCirculatory overload
DelayedMetabolic iron overloadInfection: viral, bacteria, parasite
Prevention is the most crucial way in order toPrevention is the most crucial way in order to minimise transfusion complications.

ConclusionConclusion
Simple methods for example history taking andSimple methods, for example history taking and systematic questionnaire, are crucial in preoperative evaluation of coagulopathy.preoperative evaluation of coagulopathy.Thorough surgical haemostasis remains the most important measure to reduce postoperativeimportant measure to reduce postoperative bleeding in cardiac surgeryApplication of a structured approach has beenApplication of a structured approach has been reported in terms of reduction in unnecessary blood transfusion.Aggressive postoperative haemostasis management is significant in prevention of transfusion complications
ConclusionConclusionProperly manage the bleeding problem.p y g g pReduce unnecessary blood and blood component transfusion.component transfusion.Minimise transfusion reactions and transfusion‐related complicationstransfusion‐related complications.Identify patients at risk and high risk operationsS i l bl di b l d dSurgical bleeding must be excluded.Use of the right test, right component (medicine) at the right time