Embed Size (px)
DESCRIPTION
Daniel Castellanos, MD Founding Chair, Department of Psychiatry & Behavioral Health Professor of Psychiatry & Behavioral Health and Pediatrics Herbert Wertheim College of Medicine, Florida International
Citation preview

Common Behavioral Health Disorders
of Children
& Adolescents
Daniel Castellanos, MDFounding Chair, Department of Psychiatry & Behavioral Health
Professor of Psychiatry & Behavioral Health and PediatricsHerbert Wertheim College of Medicine, Florida International University

Disclosures
No relevant financial disclosures
Castellanos FIU/HWCOM Intl Med Congress 2015
Objectives
Identify the most common psychiatric disorders in children and adolescents
Recognize the appropriate pharmacologic management of the common psychiatric disorders:
ADHD
Disruptive Behavior Disorders
Anxiety Disorders
Major Depressive Disorder (maybe if time permits)
NOTE: Focus of this presentation will be on identifying behavioral health issues in primary care
Castellanos FIU/HWCOM Intl Med Congress 2015

Adults lifetime
prevalence
Source: Kessler, et al, National Comorbidity Survey, 2005
Any substance use disorder
14.6%
Any anxiety disorder
28.8%
Major depression16.6%
ADHD8.1%
Castellanos FIU/HWCOM Intl Med Congress 2015
PTSD6.8%
Bipolar Disorder
3.9%OCD1.6%
An estimated 15 million children have a mental disorder.
Castellanos FIU/HWCOM Intl Med Congress 2015

Children aged
3-17 yrscurrently
had:
Source: MMWR, 2013
ADHD 6.8%
Behavioral or conduct
disorder 3.5%
Anxiety3.0%
Depression2.1%
Castellanos FIU/HWCOM Intl Med Congress 2015

Lifetime Prevalence of Mental Disorders Adolescents
Source: Meriknagas,et al, 2010
Castellanos FIU/HWCOM Intl Med Congress 2015
ADHD
Behavior Disorders (Oppositional Defiant Disorder, Conduct Disorder)
Anxiety Disorders Depressive Disorders (Major Depressive Disorder and
Persistent Depressive Disorder/ FKA Dysthymic Disorder)
Substance Use Disorders (mainly adolescents). Schizophrenia is not commonly found in childhood.
Most Common
Behavioral Health
DisordersChildren
& Adolescent
Castellanos FIU/HWCOM Intl Med Congress 2015

What makes a
mental health problem clinical
(need for treatment)?
ImpairmentSeverity
Castellanos FIU/HWCOM Intl Med Congress 2015

Levels of Scientific Evidence
Randomized controlled trials
Non-randomized controlled trials; large
meta-analysis
Observational studies with controls
Observational studies w/o controls; case series
Case reports; anecdotal reports; clinical consensus
Source: Adapted from US Dept of Health and Human Services; http://www.ahrq.gov/
Highest
Lowest
Castellanos FIU/HWCOM Intl Med Congress 2015
Attention-Deficit/Hyperactivity
Disorder(ADHD)
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015

Age of onset raised from 7 years to 12 years Studies indicate later detection/identification Onset criterion has been changed from “symptoms that caused
impairment were present before age 7 years” to “several inattentive or hyperactive-impulsive symptoms were present prior to age 12”
Slight modification of criteria to accommodate Adult ADHD Five or more of 9 inattention and/or >5/9 hyperactivity
symptoms (instead of >6/9)
Cross-situational requirement has been strengthened to “several” symptoms in each setting
Castellanos FIU/HWCOM Intl Med Congress 2015
ADHD

Specifiers: Subtypes have been replaced with presentation
specifiers that map directly to the prior subtypes: Combined Predominantly Inattentive Predominantly Hyperactive
Severity: based on # and severity of symptoms, and impact on function: mild/moderate/severe
If in partial remission
A comorbid diagnosis with autism spectrum disorder is now allowed
Castellanos FIU/HWCOM Intl Med Congress 2015
ADHD

A. A persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development as characterized by (1) and/or (2):
1.Inattention
2.Hyperactivity and Impulsivity
Castellanos FIU/HWCOM Intl Med Congress 2015
ADHD

1. Inattention: Six or more symptoms of inattention for children up to age 16, or five or more for adolescents 17 and older and adults; symptoms of inattention have been present for at least 6 months, and they are inappropriate for developmental level:
a. Often fails to give close attention to details or makes careless mistakes in schoolwork, at work, or with other activities.
b. Often has trouble holding attention on tasks or play activities.
c. Often does not seem to listen when spoken to directly.
d. Often does not follow through on instructions and fails to finish schoolwork, chores, or duties in the workplace (e.g., loses focus, side-tracked).
e. Often has trouble organizing tasks and activities.
f. Often avoids, dislikes, or is reluctant to do tasks that require mental effort over a long period of time (such as schoolwork or homework).
g. Often loses things necessary for tasks and activities (e.g. school materials, pencils, books, tools, wallets, keys, paperwork, eyeglasses, mobile telephones).
h. Is often easily distracted
i. Is often forgetful in daily activities.Castellanos FIU/HWCOM Intl Med Congress 2015
ADHD
2. Hyperactivity and Impulsivity: Six or more symptoms of hyperactivity-impulsivity for children up to age 16, or five or more for adolescents 17 and older and adults; symptoms of hyperactivity-impulsivity have been present for at least 6 months to an extent that is disruptive and inappropriate for the person’s developmental level:
a. Often fidgets with or taps hands or feet, or squirms in seat.
b.Often leaves seat in situations when remaining seated is expected.
c. Often runs about or climbs in situations where it is not appropriate (adolescents or adults may be limited to feeling restless).
d.Often unable to play or take part in leisure activities quietly.
e. Is often “on the go” acting as if “driven by a motor”.
f. Often talks excessively.
g. Often blurts out an answer before a question has been completed.
h.Often has trouble waiting his/her turn.
i. Often interrupts or intrudes on others (e.g., butts into conversations or games
Castellanos FIU/HWCOM Intl Med Congress 2015
ADHD

B. Several inattentive or hyperactive-impulsive symptoms were present before age 12 years.
C. Several symptoms are present in two or more setting, (e.g., at home, school or work; with friends or relatives; in other activities).
D. There is clear evidence that the symptoms interfere with, or reduce the quality of, social, school, or work functioning.
E. The symptoms do not happen only during the course of schizophrenia or another psychotic disorder. The symptoms are not better explained by another mental disorder (e.g. Mood Disorder, Anxiety Disorder, Dissociative Disorder, or a Personality Disorder).
Castellanos FIU/HWCOM Intl Med Congress 2015
ADHD

Groups:
Stimulants: Usually first line/choice meds Controlled substances Amphetamine basedMethylphenidate
Non-stimulant medications:NOT controlled substancesAtomoxetine (Strattera®)Clonidine, clonidine ER (Kapvay®) & guanfecine,
guanfecine ER (Intuniv®)Others (typically off label)
Medications Used
to Treat
ADHD
Castellanos FIU/HWCOM Intl Med Congress 2015

FDA Max FDA Approved for ADHD
Generic Name Brand Name® per day Children & Adol Adults
Mixed Amphetamine salts Adderall 40 mg Yes No
Mixed Amphetamine salts XR Adderall XR 30 mg Yes Yes
Clonidine Catapres * 0.4 mg No No
Methylphenidate Daytrana Patch 30 mg Yes No
Methylphenidate ER
Concerta
Metadate CD
Ritalin LA
Quillivant XR
72 mg
60 mg
60 mg
60 mg
Yes Yes
Dextroamphetamine Dexedrine 40 mg Yes No
Dexmethylphenidate Focalin 20 mg Yes No
Dexmethylphenidate XR Focalin XR 30 mg Yes Yes
Guanfecine ER Intuniv 4 mg Yes No
Clonidine ER Kapvay 0.4 mg Yes No
Methylphenidate Ritalin; Methylin 60 mg Yes No
Atomoxetine Strattera 100 mg Yes Yes
Guanfecine Tenex * 4 mg No No
Lisdexamphetamine Vyvanse 70 mg Yes Yes
Bupropion Wellbutrin SR/XL* 300 mg No No
Meds Used to Treat ADHD
Castellanos FIU/HWCOM Intl Med Congress 2015* Off label use for ADHD

Meds Used to Treat ADHD - Duration of Effect
Castellanos FIU/HWCOM Intl Med Congress 2015

Time (hours)
05 10
0
15
20
Mean
pla
sma
leve
ls(n
g/
mL
)
Absorption &
Duration
5
10
MethylphenidateMethylphenidate ER (Concerta®)Mixed amphetamine salts (Adderall XR®)Lisdexamphetamine (Vyvanse®)
Effective concentration
Castellanos FIU/HWCOM Intl Med Congress 2015
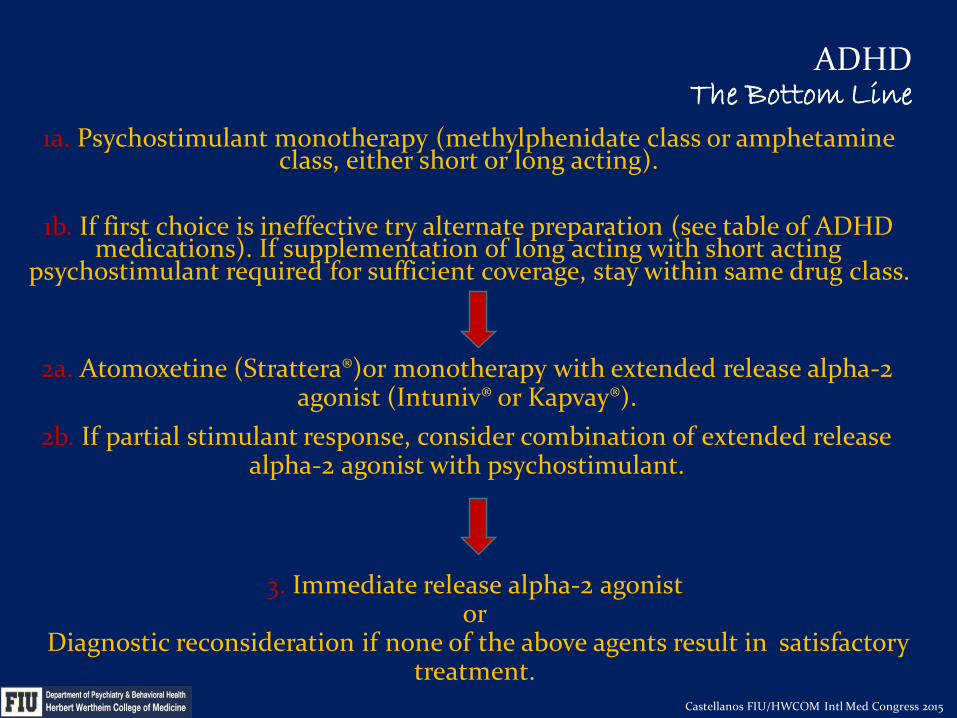
ADHDThe Bottom Line
1a. Psychostimulant monotherapy (methylphenidate class or amphetamine class, either short or long acting).
1b. If first choice is ineffective try alternate preparation (see table of ADHD medications). If supplementation of long acting with short acting
psychostimulant required for sufficient coverage, stay within same drug class.
2a. Atomoxetine (Strattera®)or monotherapy with extended release alpha-2 agonist (Intuniv® or Kapvay®).
2b. If partial stimulant response, consider combination of extended release alpha-2 agonist with psychostimulant.
3. Immediate release alpha-2 agonist or
Diagnostic reconsideration if none of the above agents result in satisfactory treatment.
Castellanos FIU/HWCOM Intl Med Congress 2015
All Medication Guidelines
can be
accessed at:
http://medicaidmentalhealth.org/
Castellanos FIU/HWCOM Intl Med Congress 2015

Disruptive Behavior
Disorders
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015

Oppositional Defiant Disorder
Conduct Disorder
Disruptive Behavior
Disorders
Castellanos FIU/HWCOM Intl Med Congress 2015

Oppositional Defiant
Disorder
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015
Symptoms grouped into three types: angry/irritable mood argumentative/defiant behavior vindictiveness.
Frequency: ODD behaviors occur commonly in normally developing
youth. Frequency of behaviors is important to determine if they are symptomatic of the disorder.
Severity: Degree of pervasiveness of symptoms across settings is
an important indicator of severity.

Conduct Disorder
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015
More serious behavioral problems than ODD.
Addition of a conduct disorder specifier called “with limited prosocial emotions”Applies to those with conduct disorder who show a callous
and unemotional interpersonal style across multiple settings and relationships. Based on research showing that individuals with conduct
disorder with limited prosocial emotions tend to have a relatively more severe form of the disorder and a different treatment response.
Oppositional Defiant Disorder &Conduct Disorder --
No known medications to address the core pathology.
Meds can be helpful with associated symptoms (eg, severe aggression).
Disruptive Behavior
DisordersThe Bottom Line
Castellanos FIU/HWCOM Intl Med Congress 2015

Anxiety Disorders
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015

Most common are fear based anxiety disorder ---
Separation Anxiety Disorder
Social Anxiety Disorder (FKA Social Phobia)
Generalized Anxiety Disorder
Specific Phobias
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015
Anxiety Disorders

Anxiety Disorders
The Bottom Line
1. Sertraline (Zoloft®) or Fluoxetine (Prozac®)
2. Switch to one above not used-Fluoxetine (Prozac®) or sertraline (Zoloft®)
3. Switch to citalopram (Celexa®) or escitalopram (Lexapro®)
No current meds are FDA approved for treatment of anxiety disorders in children
Castellanos FIU/HWCOM Intl Med Congress 2015

Anxiety Disorders
Castellanos FIU/HWCOM Intl Med Congress 2015

Substance Use
Disorders
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015

High School Students Who Reported Current Alcohol Use, 2011
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015
Source: National Youth Risk Behavior Survey, 2011
* Had at least one drink of alcohol on at least 1 day during the 30 days before the survey.

Substance Use
Disorders
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015
Nonmedical use
of prescription
drugs
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015
The 2011 National Youth Risk Behavior
Survey (YRBS) found that 1 in 5 high
school students in the US have ever taken a
prescription drug, such as OxyContin,
Percocet, Vicodin, Adderall, Ritalin, or
Xanax, without a doctor’s prescription.
Source: www.cdc.gov/yrbss

Percentage of High School Students Who Ever Took Prescription Drugs Without a Doctor's Prescription,* by Type of
Grades Earned , 2009
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015
Source: United States, Youth Risk Behavior Survey, 2009

Major Depressive
Disorder
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015
Most of this area will be covered by subsequent presentation by Aramys Barzaga, MD
A few points to highlight will follow
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015
Major Depressive Disorder

Diagnostic Criteria:
Essentially unchanged except removal of the “bereavement exclusion.” Allows clinicians to now exercise their professional
judgment as to whether someone with a major depressive disorder and grieving should be diagnosed with MDD. The 2-month timeframe required by DSM-IV suggests an
arbitrary time course to bereavement that is inaccurate. Individuals experiencing both conditions can benefit
from treatment but are excluded from diagnosis under DSM-IV.
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015
Major Depressive Disorder
Diagnostic Criteria:
Added:Persistent Depressive Disorder
Disruptive Mood Deregulation DisorderSpecifiers:
“With anxious distress”
Meds Used to Treat
Major Depression
FIU
Psychotropic Medications
Training
Castellanos FIU/HWCOM Intl Med Congress 2015
Major Depressive Disorder
Major Depression
The Bottom Line
1a. Fluoxetine (Prozac®) or 1b. escitalopram (Lexapro®)
2. Switch to one not used- escitalopram (Lexapro®) or Fluoxetine (Prozac®)
3. Refer to psychiatrist or
Switch to sertraline (Zoloft®), bupropion (Wellbutrin®) or venlafaxine (Effexor®)
Castellanos FIU/HWCOM Intl Med Congress 2015

A thorough evaluation- it all starts here:
Ensure an appropriate evaluation before beginning psychopharmacological interventions.
This usually implies meeting the criteria for a disorder (not just being a anxious or sad).
Severity & Impairment: As a general rule, meds are indicated for disorders with moderate to severe symptoms and impairment.
Use meds with the strongest evidence base.
Caution with extrapolating from adult literature to justify the use in children.
Take Home Points
Castellanos FIU/HWCOM Intl Med Congress 2015

Typically begin with meds that are FDA approved for that indication or have the strongest evidence base:
ADHD: Multiple
Anxiety Disorders: Sertraline (Zoloft®) or
fluoxetine (Prozac®)
Insomnia: Melatonin
Major depression: Fluoxetine (Prozac®) or
escitalopram (Lexapro®)
Take Home Points
Castellanos FIU/HWCOM Intl Med Congress 2015

Parting Thoughts
“If you want happiness for an hour, take a nap.If you want happiness for a day, go fishing.
If you want happiness for a month, get married.If you want happiness for a year, inherit a fortune.If you want happiness for a lifetime, help others.“
Anonymous Chinese Proverb
Castellanos FIU/HWCOM Intl Med Congress 2015





























