Embed Size (px)
Citation preview

Common Congenital AnomaliesCarolyn O’Donnell, MD, PGY-3
Newborn Exam
Head Enlarged fontanelle Hair- swirls/white forelock Eyes- congenital cataracts, extra folds,
hyper/hypotelorism, upslant/downslant Choanal atresia Ear pits/tags, position/rotation Cleft palate/lip Prominent frenula/tongue tie
Red Reflex
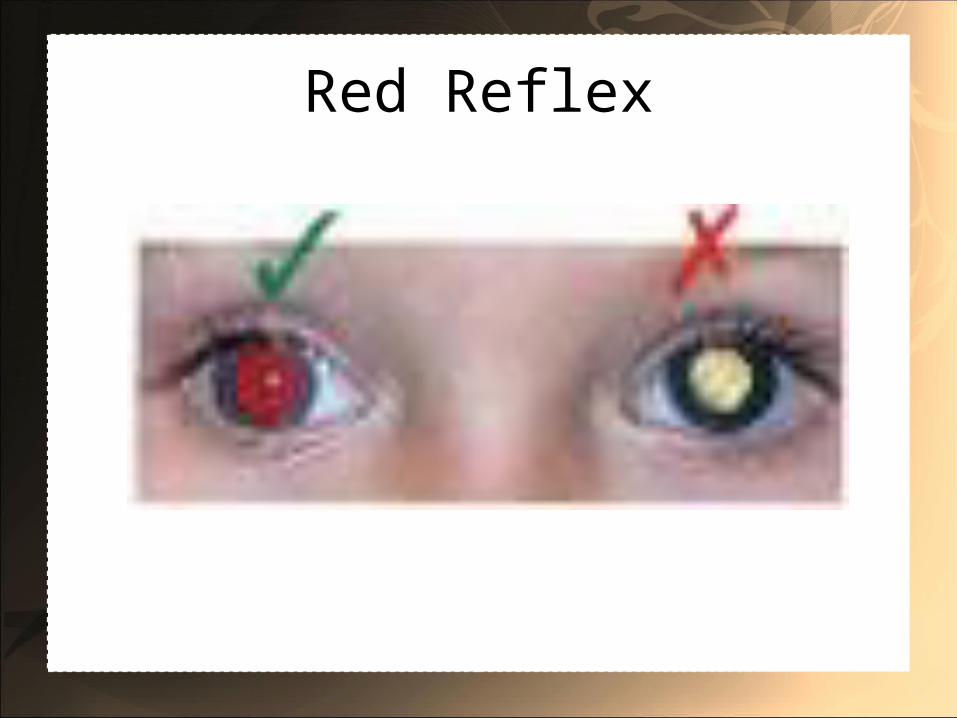
• Rule out opacities between the cornea and the retina
• Congenital glaucoma: can see large eyes, excess tearing and cloudy corneas. This condition can be clinding
• An infant with consistently white pupils might have a retinoblastoma tumor
Red Reflex
Tongue Tie (Ankylogossia)
Neck and Chest
• Cystic hygroma• Thyroglossal duct cyst• Branchial cleft cyst• Pectus excavatum• Extra mamillary tissue (3rd nipple)• Heart murmur- congenital heart disease
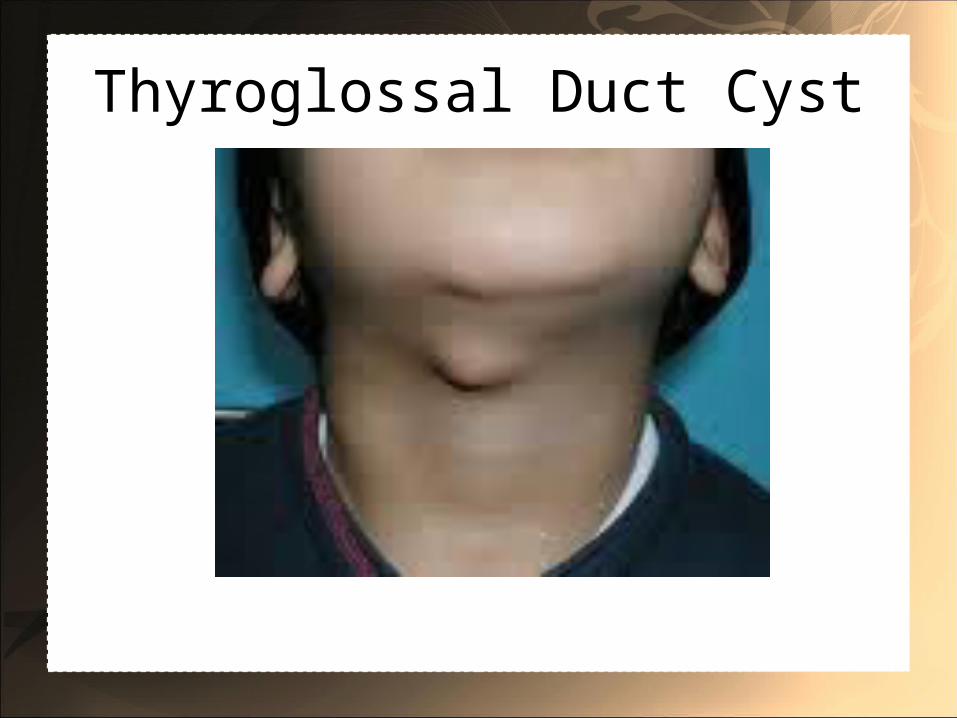
Thyroglossal Duct Cyst
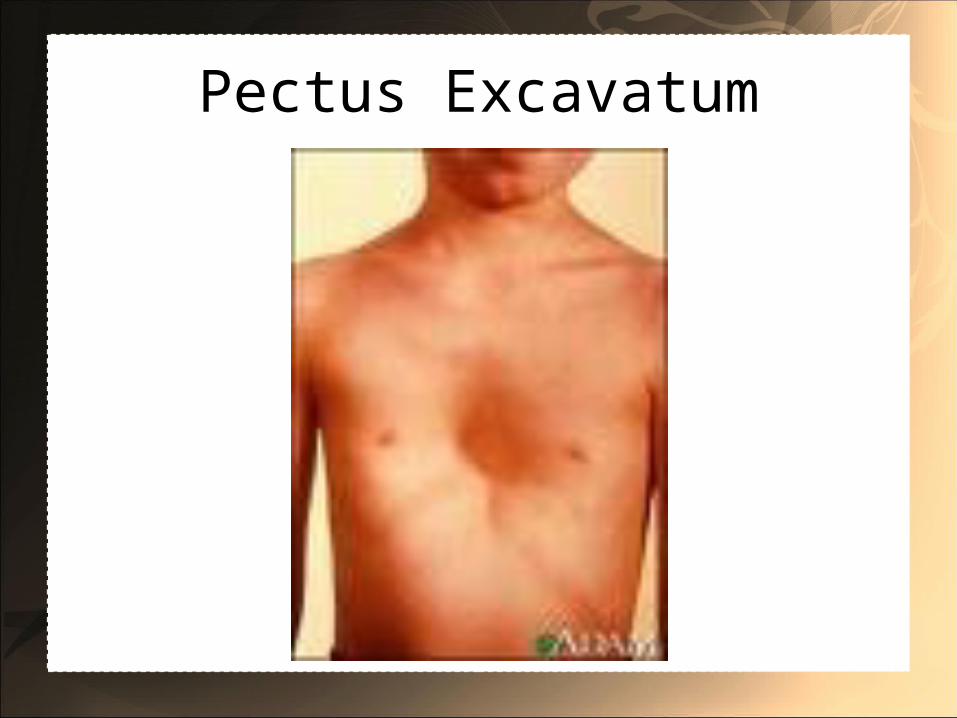
Pectus Excavatum
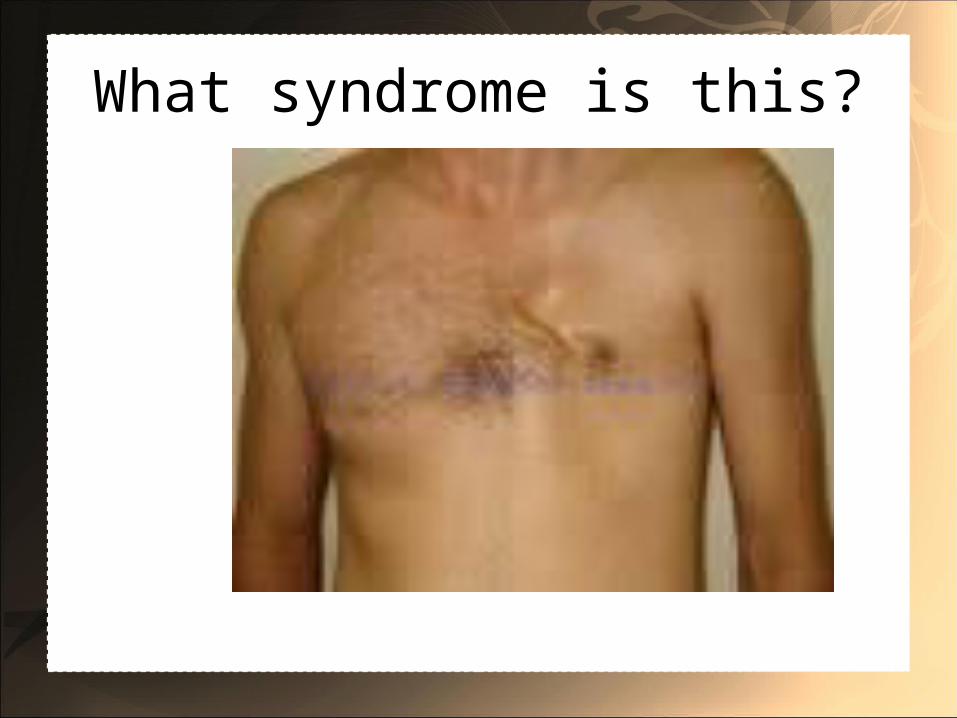
What syndrome is this?

Extranumerary nipple
Abdomen and GU
• Omphalocele/gastroschesis/umbilical hernia• Scaphoid abdomen- ?congenital diaphragmatic
hernia• Femoral pulses- aortic coarctation• Undescended testes• Virilized female• Fistulas, hypospadia/epispadias, imperforate
anus, Hirschprung’s• Posterior urethral valves (no urinating)

Imperforate Anus
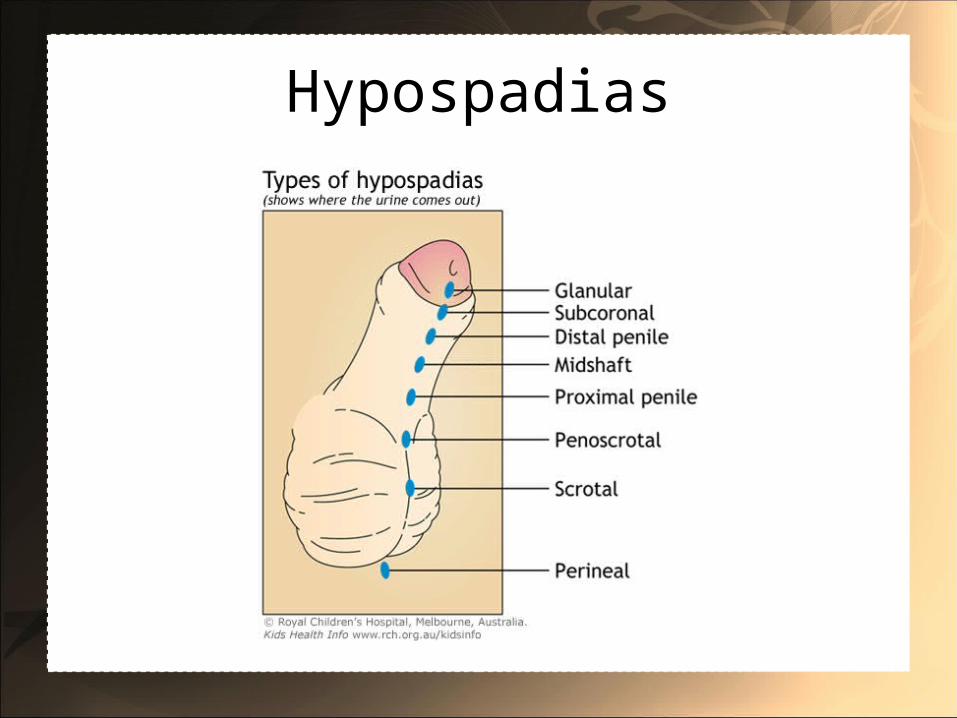
Hypospadias

Virilized female
Extremities and Skin
• Congenital Hip dysplasia• Extra digits• Single palmar crease• Clubbed foot• Congenital nevi• Hemangiomas
Club Foot
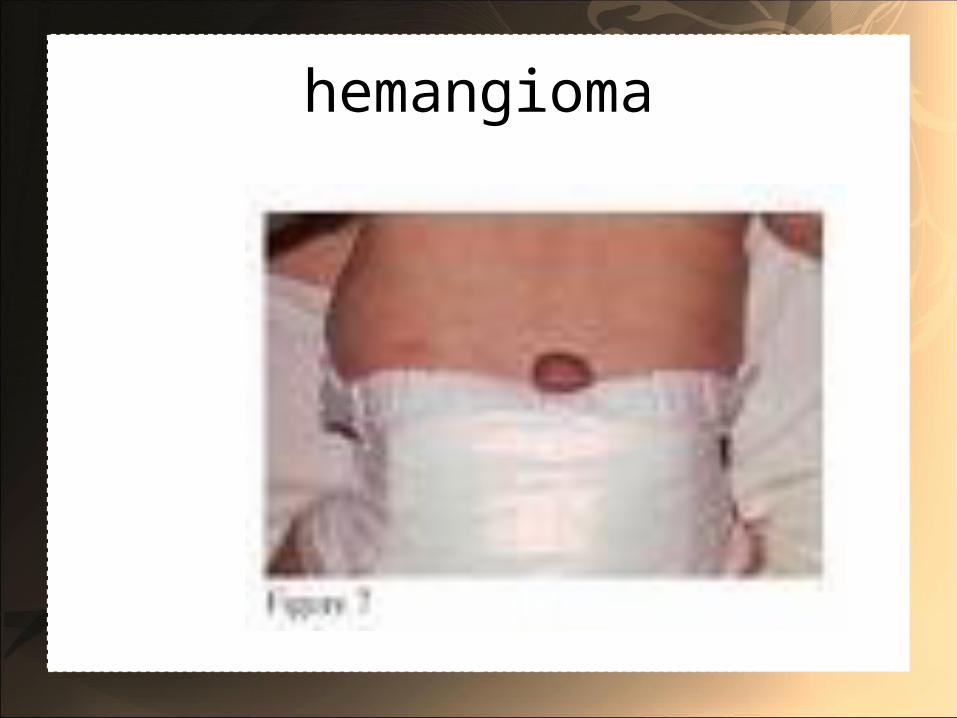
hemangioma
Cleft lip/palate
• Incidence: about 1 in 600 live births• Cleft lip with or without cleft palate• Syndromic: associated with another syndrome.
Syndromic cleft lip/palate is more common in males
• Nonsyndromic: isolated finding, not associated with any particular syndrome. Non syndromic tends to be equal between males and females.
• Consider submucous cleft palate with bifid uvula
Causes
• Multifactorial: combination of hereditary and environmental factors involved in growth and development
• Interference with normal development- within the 1st few months of development
• Medications such as phenytoin, steroids, retinoids (Vitamin A derivatives)
• Alcohol, hypoxia and dietary deficiencies have been implicated
• Both single and multiple genes
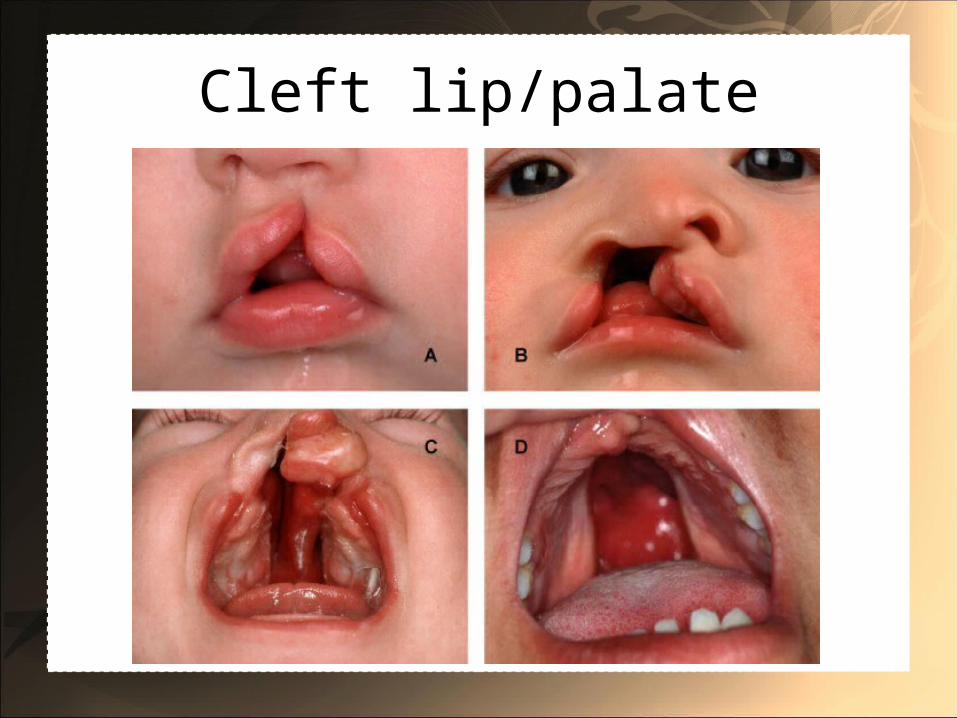
Cleft lip/palate
Syndromes
• DeGeorge/velocardiofacial/22q deletion• Pierre Robin malformation sequence• Apert syndrome• Crouzon syndrome• Treacher-Collins
Complications
• Feeding problems• Eustacian tube dysfunction secondary to
abnormal muscle placement -> serous otitis/middle ear disease/chronic ear infections -> hearing problems
• Speech problems• Dental problems• Team approach needed: medical/surgical,
dental, speech and hearing
Treatment
• Surgical repair- usually by plastic surgery- can affect maxillofacial growth pattern
• Timing of surgery controversial- often in 2 stages. One commonly used plan involves early soft palate repair at age 6 months, followed by hard palate repair at age 6 years. Others involve complete repair at a later age.
• Involvement with ENT, speech therapy, following hearing tests, dental/orthodontic specialists, social supports.
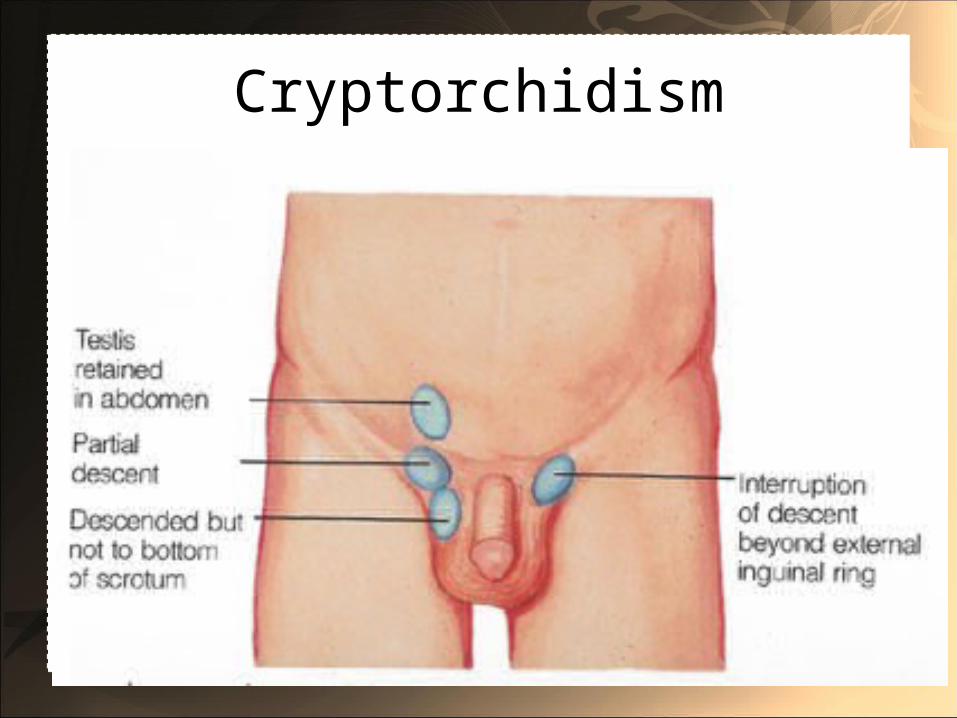
Undescended Testicle (cryptorchidism)
• Occurs in 3-4% of full term newborns• More common in premature infants- transinguinal
migration occurs at 28-40 weeks gestation (under hormonal control)
• Often the testicle will descend by the time the infant is 9 months old- prevalence is 1% at 1 year of age
• If there’s no descent by 1 year of age, this warrants further workup
• One can ask the family to check at home in a warm bath due to retractile testis (due to cremasteric reflex)
Causes
• Increased incidence in prematurity• Increased risk with:• Small for gestational age• Low birth weight• Maternal exposure to estrogen early in pregnancy• Twin• Sibling with cryptorchidism• Conditions associated with low intra-abdominal
pressure
Cryptorchidism
Cryptorchidism• Complications-• Infertility (increased risk with time in abdomen)• Increased risk for testicular cancer- approximately
40x normal• If neither testicle palpable, endocrine and genetic
testing warranted to determine true sex• Ultrasound may be helpful to identify the location
of the testicle- sometimes not present at all• If partially descended, exam should be followed
closely to make sure fully descends
Treatments• Often surgical (orchiopexy) though some medical
treatments have been tried including testosterone and HCG
• Surgery performed by general surgeon or urologist- usually between 6 and 12 months of age
• Surgical correction many decrease the risk of cancer though it is still significantly elevated.
• Another benefit of surgery is more easily identifiable if tumor/mass. Also decreased infertility.
Ear pits and tags
• There is an association between ear anomalies and hearing loss. Audiologic evaluation is recommended for any ear anomaly
• Multiple ear anomalies may suggest a kidney problem as well as there is an association and many syndromes contain anomalies in both systems.
• Renal Ultrasound is not recommended if isolated pit or tag
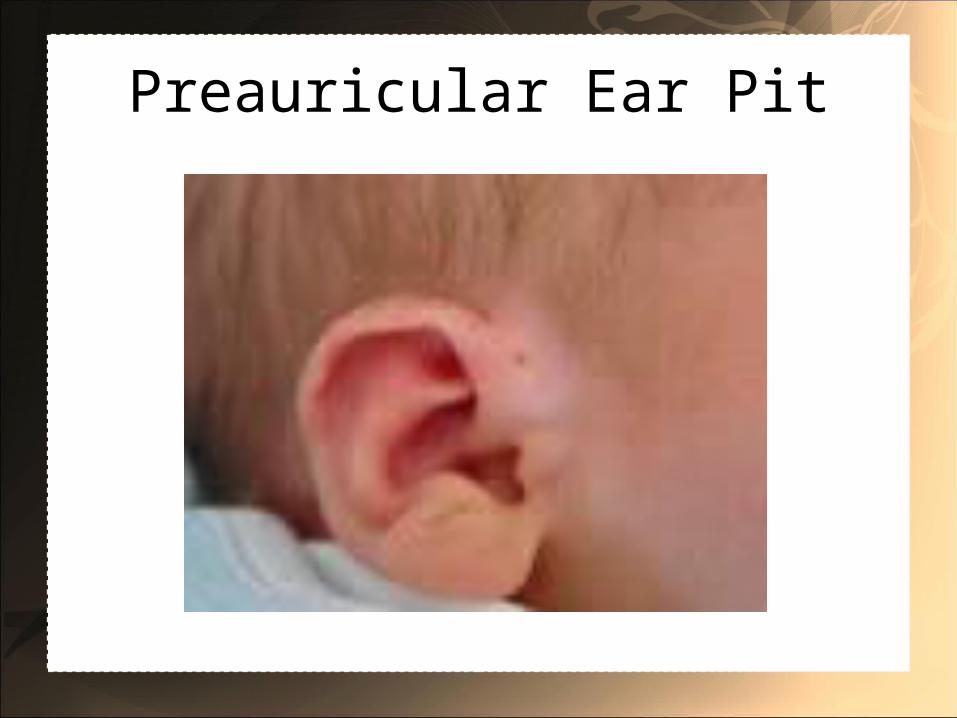
Preauricular Ear Pit
Ear Tag
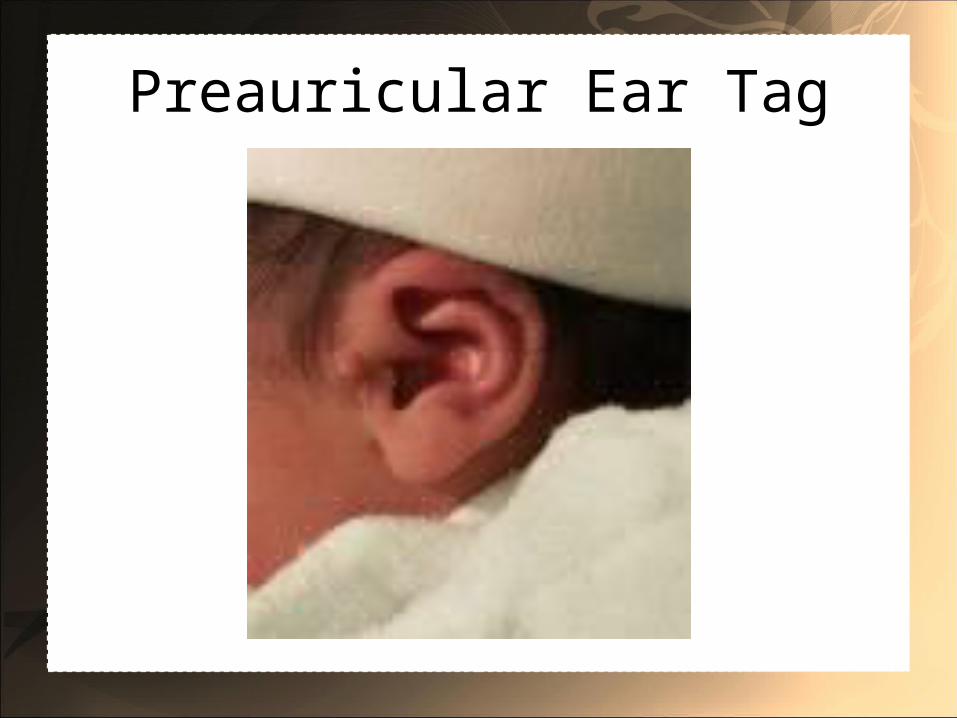
Preauricular Ear Tag