Embed Size (px)
Citation preview

Support Care Cancer (2004) 12:669–673DOI 10.1007/s00520-004-0643-0 O R I G I N A L A R T I C L E
Elizabeth A. BarnesEdward ChowLou AnderssonCharles HayterAndrew LoblawDavid LeeLori HoldenGrace ChanCyril Danjoux
Communication with referring physiciansin a palliative radiotherapy clinic
Received: 21 November 2003Accepted: 7 April 2004Published online: 11 May 2004� Springer-Verlag 2004
E. A. Barnes ()) · E. Chow ·L. Andersson · C. Hayter · A. Loblaw ·L. Holden · G. Chan · C. DanjouxRapid Response Radiotherapy Program,Department of Radiation Oncology,Toronto-Sunnybrook Regional CancerCentre, University of Toronto,2075 Bayview Avenue, Toronto, Ontario,M4 N 3M5, Canadae-mail: [email protected].: +1-416-4804998Fax: +1-416-2171338
D. LeeDepartment of Clinical Trialsand Epidemiology,Toronto-Sunnybrook Regional CancerCentre, University of Toronto,Toronto, Ontario, Canada
Abstract Goals: The rapid responseradiotherapy program (RRRP) atToronto-Sunnybrook Regional Can-cer Center (TSRCC) provides quickaccess to palliative radiotherapy forpatients with a life expectancy of lessthan 12 months. Patients then returnto their referring physician for con-tinued oncologic management. Afterthe initial RRRP consultation, we faxan interim consultation report to thereferring physician. The purpose ofthis study was to assess how usefulreferring physicians perceive thisinterim report and whether this reportneeds to be modified to meet theirinformation needs. Methods: Physi-cians who referred patients to theRRRP and who were faxed an inter-im consultation report were identi-fied over a 4-month period. Thesephysicians were then faxed a ques-tionnaire that asked how useful theinterim report was in patient man-agement, about their satisfaction withthe information provided, to cri-tique the report format, and whetherthe RRRP physician and nurse wereeasily accessible by telephone.
Main results: Forty physicians re-ferred patients to the RRRP clinicover the 4-month study period. Theresponse rate to our survey was58% (23/40). The vast majority ofphysicians (95%) stated that the in-terim consultation report was usefulin patient management. They feltthat treatment details were ade-quately discussed in the report. Thereport format was perceived to beclear and concise. Referring physi-cians wished to be informed aboutany medication changes. RRRPphysicians and nurse were perceivedto be easily accessible by telephoneif needed. Conclusions: Resultsshowed that referring physiciansfound the faxed interim consultationreport useful in patient management.Suggestions were made on how toimprove the report, and they will beused to further enhance physiciancommunication and ultimately pa-tient care.
Keywords Survey · Palliative care ·Radiotherapy · Physiciancommunication
Introduction
Prompt and effective physician communication is vital toensure quality patient care. Several studies have shownthat communication between referring physicians/familyphysicians and specialists is suboptimal in many ways [8,9, 7, 2, 1]. Referring physician letters may not state thereason for referral or provide appropriate information, and
specialists may not send consultation reports in a timelyfashion or indeed at all. Referring physicians have alsofound the content of these consultation letters inadequate.
The Rapid Response Radiotherapy Program (RRRP) atToronto-Sunnybrook Regional Cancer Center (TSRCC)provides quick access to palliative radiotherapy for pa-tients with a life expectancy less than 12 months. InCanada, radiation oncology departments are localized in

670
larger centers, so that two large centers—TSRCC andPrincess Margaret Hospital (PMH)—provide radiotherapyservices to the Greater Toronto area with a population ofover 3 million. The demand for radiotherapy exceeds re-sources, and the long waiting list for consultation andtreatment led to the formation of the RRRP is at TSRCCin 1996. Five radiation oncologists see patients in 5 half-day clinics per week, and approximately 700 new patientsare seen a year. Radiotherapy treatment is generally de-livered over 1–5 days, after which patients return to their
referring physician, usually a community medical oncol-ogist, for follow-up care.
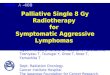
A survey of physicians referring to the RRRP wascarried out in 1999, and these physicians identified rapidcommunication as being essential in order to convey theexpected benefits and side effects of radiotherapy forthese patients with limited prognosis [3]. In responseto this need, we devised a short, semistructured, interimconsultation report, which is faxed to the referring phy-sician the same day the patient is seen in clinic (Fig. 1).This is followed by a full consultation letter, which is
Fig. 1 Interim ConsultationReport

671
mailed within 2 weeks of the initial consult. The purposeof this study was to obtain feedback as to how usefulreferring physicians perceive this faxed report, includingtimeliness and content, and how this report can be im-proved to meet their information needs.
Methods
When patients are seen in consultation in the RRRP at TSRCC, astandardized, one-page, interim consultation report is completed bythe radiation oncologist and faxed to the referring physician thesame day (Fig. 1). The report template prompts the radiation on-cologist to summarize the consultation and details of radiotherapy.The phone number for the nurse coordinator is given, and the reportstates that routine follow-up has not been arranged, although repeatconsultations are welcome.
We identified all referring physicians to whom we sent thisreport over a 4-month period from February to May 2003. In June2003, a cover letter and questionnaire were faxed to this populationof referring physicians. A follow-up cover letter and questionnairewere faxed to all nonresponders 10 days after the initial fax.Physicians referring more than one patient during this study periodwere sent only one questionnaire and were asked to complete this inreference to the last interim consultation report they received.
The questionnaire consisted of nine questions plus an additionalfour questions to collect demographic data. Physicians were askedwhether they had received the faxed interim consultation reportand, if so, whether sufficient treatment-related information wasprovided, what additional information would be useful, to critiquethe report format, and if the radiation oncologist and nurse coor-dinator were easily accessible by phone. Responses were recordedeither on a five-point Likert scale (1=strongly disagree and5=strongly agree) or as yes/no/nonapplicable.
Data analysis included descriptive statistics focusing on fre-quencies, means, medians, and ranges. The response to the Likertscale was categorized as “disagree” (scores 1 or 2, strongly disagreeor disagree) and “agree” (score 4 or 5, agree or strongly agree).
Results
Forty physicians were identified over the 4-month studyperiod and mailed questionnaires. The response rate to thequestionnaire was 57.5% (23/40) with 15 physicians re-sponding to the initial fax and eight to the reminder fax.Demographic data for responding physicians are sum-marized in Table 1. Nearly three quarters of the referringphysicians were community medical oncologists, withfamily physicians and surgeons making up the remainder.Almost all (96%) worked in an urban setting.
The results for the questionnaire responses are sum-marized in Tables 2 and 3. Most of the responding physi-cians (20/23; 87%) stated that they had received the faxedinterim consultation report, and of these, 95% agreed orstrongly agreed that it was useful in patient management.At least 90% of referring physicians agreed or stronglyagreed that the report adequately discussed the consul-tation details, apart from the issue of treatment-relatedside effects, an area in which they wished to have moreinformation. Medical oncologists were more likely than
surgeons or family physicians to feel that the radiationtreatment plan and goals of treatment had been adequatelydiscussed (p value for Fisher’s exact test=0.067). Physi-cians wanted to be informed of any medication changesbut were less likely to want details on information relayedto the patient on treatment outcome or prognosis, and
Table 1 Demographic data on 23 responding physicians. RRRPrapid response radiotherapy program
No. of physicians (%)
Medical SpecialtyMedical oncologyFamily practiceSurgery
17 (74%)3 (13%)3 (13%)
Practice locationUrbanRural
22 (96%)1 (4%)
No. years in practiceMedianRange
181–30
No. patients referred to RRRP per yearMedianRange
211–100
Table 2 Physician’s opinions on faxed interim consultation reportdetailsa
Issue Agreement thatadequately discussedb
Main symptoms 19/20 (95%)Radiation treatment plan 18/20 (90%)Goals of treatment 18/20 (90%)Anticipated treatment-related sideeffects
15/20 (75%)
Recommendations 19/20 (95%)a Results based on the 20 physicians who stated they received theinterim consultation reportb Agreement=score of 4 or 5 (agree or strongly agree) on a scale of1= strongly disagree and 5=strongly agree
Table 3 Physicians’ opinions on communication issues
Agreementa
Report received in a timely fashionReport useful in patient managementItems that may be useful addition to interim
reportInformation discussed with patientMedication changesTreatment site-specific information sheet
90%95%64%95%55%
Report format clear and concise 100%Prefer alternate report format 0%Radiation oncologist easily accessible bytelephone if needed
93%
Nurse coordinator easily accessible by telephoneif needed
100%
a Agreement=score of 4 or 5 (agree or strongly agree) on a scale of1=strongly disagree and 5=strongly agree

672
they were ambivalent on the inclusion of a treatmentsite-specific information sheet. Referring physicians werepleased with the report format, which consists of a shortsemistructured template, and did not want this changed toan alternate format, i.e., tick boxes. The RRRP physicianand nurse were felt to be easily accessible if needed toclarify the report details.
Discussion
This study used a questionnaire to investigate the effec-tiveness of a faxed interim consultation report in com-munication with referring physicians regarding patientsreferred for palliative radiotherapy. We found that refer-ring physicians perceived the faxed interim consultationreport to be useful in patient management. Our surveyresulted in suggestions on how to improve the interim re-port, including more reporting of potential treatment sideeffects and inclusion of any medication changes. TheRRRP staff were perceived to be readily accessible ifneeded to clarify issues in the report.
Limitations of this study included the small number ofresponders, with 23 of the 40 physicians surveyed re-turning the questionnaire. This response rate (58%) whilelow, is in keeping with the 50% response rate typicallyseen with mail questionnaires. We sent a follow-up ques-tionnaire to nonresponders to increase the response rate,and this resulted in eight additional questionnaires beingreturned, accounting for 35% (8/23) of the total responses.Physicians pleased with the services provided by theRRRP may be more likely to return the questionnaire,therefore biasing the results. However, with more than 50referring physicians to the RRRP per year [3], and the factthat physicians in this survey reported referring a medianof 21 patients a year, we feel that their feedback offers arepresentative view of RRRP-referring physicians.
This study was done in follow-up to a satisfactionsurvey of physicians referring patients to the RRRP con-ducted several years ago [3]. At that time, major weak-nesses of the program were found to include difficultycontacting the radiation oncologist, poor communicationof treatment information, and the lengthy time for dictatedconsultation notes to arrive. Patients are generally notseen in follow-up in the RRRP; therefore, communicationof all information needed to provide optimal continuedcare is important. In addition, given the limited life ex-pectancy of these patients, rapid communication of thisinformation is vital.
Letters have been the traditional means of physiciancommunication [8]. The length of time for consultationletters to reach referring physicians and family physicianshas been reported as a concern in the past. Information isoften lacking, and issues physicians believe to be im-portant are not discussed [8, 9, 7, 2, 1]. Therefore, westarted faxing an interim consultation report to referring
physicians the same day their patient was seen in con-sultation. A previous study found the use of handwritten,faxed, discharge summaries to be an acceptable method ofcommunication by family physicians [6]. Faxing wasthought to be preferable to giving patients a copy of thereport, as the report would not be received until the nextphysician visit and may be lost by the patient. However,13% (3/23) of physicians responding to this survey deniedreceiving the faxed report, which indicates that thismethod of communication is not without limitations. Al-ternatively, as there may have been an interval of up to 5months between receiving the faxed report and the ques-tionnaire, physicians may have forgotten seeing the reportor it may have been filed by their office staff.
In response to the 1999 satisfaction survey where re-ferring physicians requested more treatment information[3], a template for the interim consultation report was de-vised with headings specific for treatment details, such astreatment site, dose and fraction, and the start date ofradiation. Goals of treatment and potential side effectswere also included in the template (Fig. 1). From the sur-vey results presented here, referring physicians agreedthat apart from potential side effects, the treatment detailswere now adequately addressed. Not reporting potentialtreatment side effects was previously identified as aproblem during a review of letters sent to family physi-cians after patients were discharged to their care follow-ing palliative radiotherapy [1]. That study, as well as theRRRP survey from 1999, both reported physicians ashaving difficulty contacting the radiation oncologist [1,3]. This was not confirmed in our more recent survey. Itmay be that by providing the faxed interim report, thereferring physician no longer needs to contact the radia-tion oncologist directly for treatment information. Thefaxed interim report also contains the phone number forthe nurse coordinator, so this method of accessing infor-mation may be a useful alternative.
Referring physicians agreed that it was important forthem to be informed of medication changes made at thetime of the RRRP consultation. Many patients are referredto the RRRP to palliate pain arising from bony metastasesor tumor-mass effect. We previously found that at thetime of RRRP consultation for bone metastases, 80% ofpatients complained of moderate to severe pain, and ofthese, 38% were either not taking any analgesics or onlynonopioids or weak opioids [4]. Informing the physicianresponsible for patient follow-up of changes made in theRRRP to the analgesic regime, such as the addition ofopioids or dose adjustment, is important for optimal con-tinued care. A previous communication study found 85%of family physicians wanted the letter from the radiationoncologist after palliative radiotherapy to mention painmedications, but this was only seen in 5% of letters [1].Medications may also be prescribed for other disease-related symptoms or as prophylaxis for radiotherapy-in-

673
References
1. Barnes EA, Hanson J, Neumann CM,Nekolaichuk C, Bruera E (2000) Com-munication Between Primary CarePhysicians and Radiation OncologistsRegarding Patients with Cancer Treatedwith Palliative Radiotherapy. J ClinOncol 18:2902–2907
2. Bourguet C, Gilchrist V, McCord G(1998) The consultation and referralprocess. A report from NEON. North-eastern Ohio Network Research Group.J Fam Pract 46:47–53
3. Chow E, Wong R, Vachon M, et al(1999) Referring physicians’ satisfac-tion with the rapid response radiother-apy programme. Support Care Cancer8:405–409
4. Chow E, Connolly R, Franssen E, etal (2001) Prevalence of under-dosageof analgesics for cancer bone pain inpatients referred for palliative radio-therapy, and its potential implicationsin radiotherapy trials. Annals RCPSC34:217–222
5. Haddad P, Soban F, Williams D, et al(2003 How helpful is prompt commu-nication about a palliative radiotherapyvisit? A survey on our interim consul-tation report. Support Care Cancer11:422 (abstract)
6. Paterson JM, Allega RL (1999) Im-proving communication between hos-pital and community physicians. Feasi-bility study of a handwritten, faxedhospital discharge summary. Dis-charge Summary Study Group. CanFam Physician 45:2893–9
7. Stalhammar J, Holmberg L, SvardsuddK, et al (1998) Written communicationfrom specialists to general practitionersin cancer care: What are the expecta-tions and how are they met? Scand JPrim Health Care 16:154–9
8. Tattersall MHN, Griffin A, Dunn SM etal (1995) Writing to referring doctorsafter a new patient consultation: Whatis wanted and what was contained inletters from one medical oncologist?Aust N Z J Med 25:479–482
9. Wood ML (1993) Communication be-tween cancer specialists and familydoctors. Can Fam Physician 39:49–57
duced side effects such as nausea, vomiting, diarrhea, orskin erythema.
PMH has conducted a survey to assess the satisfactionof their interim consultation report faxed after patients areseen in consultation in the palliative radiation oncologyprogram (PROP) [5]. The PROP report template differsfrom the RRRP at TSRCC by including patients’ ECOGperformance status, recommended changes to medications,whether the patient was entered into a clinical trial, furtherinterventions, and if any referrals were made. They foundvirtually all referring physicians (93%) considered the re-port necessary, 84% stated they read the report the sameday, 92% thought the length was just right, and only 15%considered some important information missing. This mis-sing information mainly consisted of the rationale under-lying treatment decisions. Both the RRRP and PMH in-terim report surveys therefore suggest that physicians re-ceive and read the faxed reports in a timely fashion and thatthese reports are useful in patient management. Medicationchanges are routinely mentioned in the PROP report, andreferring physicians stated that this would be a useful ad-dition to the RRRP report. Only half of RRRP-referringphysicians were interested in receiving a treatment-specificinformation sheet. This may be due to treatment informa-tion being adequately discussed in the interim report and/orthat most (74%) physicians are medical oncologists whorefer many patients (median=21 annually) to the RRRPand may therefore be familiar with treatment information.PROP does not send such information sheets, and no physi-cians requested such information in their survey. PROP
faxes their interim report to the family physician and otherphysicians involved in patient care in addition to the re-ferring physician. This may be a policy for RRRP to adopt,as it ensures all physicians are aware of the patients’ cur-rent medical status and treatment plan, facilitating bettercommunication and ultimately patient care.
The interim report can also serve as a means of pro-viding education on the role of palliative radiotherapy. Asurvey of family physicians found that knowledge of theindications and effectiveness of palliative radiotherapywas limited [1]. Deficits in knowledge may mean thatpatients with symptoms amenable to treatment may not bereferred for radiotherapy. While the majority (74%) ofreferring physicians were medical oncologists and shouldbe aware of the role of palliative radiotherapy, this cannotbe assumed. By providing rapid feedback on the clinicalscenarios where palliative radiotherapy is useful, the in-terim report can provide useful information for all refer-ring physicians and physicians involved in patient caresuch as family physicians.
In summary, this survey showed that referring physi-cians found the faxed interim consultation report useful inpatient management. We will continue to fax the interimreport to referring physicians the same day as patientconsultation. To improve communication and enhancepatient care consideration, radiation oncologists will beencouraged to emphasis anticipated treatment related sideeffects and report medication changes, and considerationwill be given to faxing the report to other members of thepatients health care team.