Embed Size (px)
Citation preview

Community Care Physicians Community Care Physicians Quality of Care Initiatives Quality of Care Initiatives
20062006
Bridges to ExcellenceBridges to ExcellencePerformance Improvement ProjectsPerformance Improvement ProjectsEMR ImplementationEMR Implementation

Bridges to Excellence Status Bridges to Excellence Status ReportReport
17 Practices representing 84 Physicians achieved recognition17 Practices representing 84 Physicians achieved recognitionImproved patient outcome and responseImproved patient outcome and responseQuality brandingQuality brandingSignificant monetary reward: >$470,000 and counting from Significant monetary reward: >$470,000 and counting from the collaborativethe collaborativeAn additional $188,000 anticipated by yearAn additional $188,000 anticipated by year’’s ends end~ $500,000 received in related incentives (~ $500,000 received in related incentives (HealthplansHealthplans))Corporate Application in progress with EMR implementationCorporate Application in progress with EMR implementation

BTE Related ActivitiesBTE Related Activities
Diabetes Care InitiativeDiabetes Care Initiative
Diabetes Case Management ProgramDiabetes Case Management Program
Diabetes Self Management Education ProgramDiabetes Self Management Education Program
ProCareProCare
EMREMR

DCIDCIDiabetes Care InitiativeDiabetes Care Initiative
Diabetes Performance Measurement and ImprovementDiabetes Performance Measurement and Improvement
-- Develop Diabetic registry Develop Diabetic registry -- Conduct process audit Conduct process audit -- Provide benchmarking dataProvide benchmarking data-- Develop interventions and implementDevelop interventions and implement-- ReRe--measuremeasure
Phase 1 conducted at 5 Practices involving 40 Practitioners Phase 1 conducted at 5 Practices involving 40 Practitioners and 3000 patientsand 3000 patients
Phase 2 expanded to total of 10 Practices, 60 PractitionersPhase 2 expanded to total of 10 Practices, 60 Practitioners4500 patients4500 patients

Areas of Opportunity and InterventionsAreas of Opportunity and Interventions
Tobacco screeningTobacco screening-- Staff education on Diabetic patient prep and Tobacco screeningStaff education on Diabetic patient prep and Tobacco screeningScheduling of followScheduling of follow--up visitsup visits-- Process changes in the way we schedule patients Process changes in the way we schedule patients Comprehensive foot careComprehensive foot care-- Diabetes Tool Kits filled with tools for the provider and the pDiabetes Tool Kits filled with tools for the provider and the patient atient –– to to facilitate foot examsfacilitate foot examsAnnual dilated retinal examAnnual dilated retinal exam-- Documentation Tools: flow sheets, standing order sets etc. Documentation Tools: flow sheets, standing order sets etc. Nephropathy testingNephropathy testing-- Educational information on nephropathy testing Educational information on nephropathy testing Self Management EducationSelf Management EducationADA Certified Diabetes Self Management Education ProgramADA Certified Diabetes Self Management Education Program

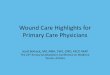
Relationship of # of Visits per Year to A1C LevelsSelected CCP Practices (2004)
6
6.1
6.2
6.3
6.4
6.5
6.6
6.7
6.8
6.9
7
1 1.5 2 2.5 3 3.5 4 4.5
Number of Visits/Year
A1C
Lev
els
Practice ExperienceLinear (Practice Experience)
Practice 1
Practice 2 Practice 3
Practice 4
Practice 5
Note: Demographics of each practice - including age, sex, geographic location
and insurance all very similar.

Diabetes Case Management ProjectDiabetes Case Management Project
CDPHP Health Plan CDPHP Health Plan and and
Community Care Physicians Community Care Physicians Diabetes Case ManagementDiabetes Case Management
2004 2004 -- 20052005

The Collaborative ProjectThe Collaborative Project
Patients were included in the project if their Patients were included in the project if their HbA1c was >9.0% (Case Management Trigger)HbA1c was >9.0% (Case Management Trigger)CDPHP Case Managers worked with patients on CDPHP Case Managers worked with patients on lifestyle modifications, medication and diabetes lifestyle modifications, medication and diabetes management and provided general diabetes management and provided general diabetes disease education.disease education.The Case Manager sent a followThe Case Manager sent a follow--up report to the up report to the patientpatient’’s physician documenting the intervention.s physician documenting the intervention.The Provider incorporated the intervention into the The Provider incorporated the intervention into the plan of care thereby reinforcing the message.plan of care thereby reinforcing the message.

Average A1c - Case Management
10.138
8.676
7.5
8
8.5
9
9.5
10
10.5
# of Lab Draws
A1c
Val
ue
Last Draw
First Draw

Average A1c Without Case Management - 2005
9.459.96
0
2
4
6
8
10
12
Average A1c for the First Draw Average A1c for the Second Draw

Case Management Results Case Management Results
1.651748.410.05
Combined 2004 2005
1.5768.610.12005
1.8988.2102004
ChangeNAverage A1c Post-Case
ManagementAverage A1c Pre-Case
ManagementYear

Diabetes Self Management Education Diabetes Self Management Education ProgramProgram
ADA certified ADA certified
Multiple sites, times, group and individual classes Multiple sites, times, group and individual classes --accessaccess
Improve patient outcome by providing a previously Improve patient outcome by providing a previously unun--reimbursable form of patient intervention.reimbursable form of patient intervention.
Promote continuum of carePromote continuum of care

DSME OutcomesDSME Outcomes
9.75%
6.93%
0%
2%
4%
6%
8%
10%
12%
Pre DSME Program HbA1c 6-month Post DSMEProgram HbA1c
*Mean difference between HbA1c pre and post DSME Program was -2.8% (95% CI -2.09 to -3.55)
* p≤.001

Post DMSE HbA1c DistributionPost DMSE HbA1c Distribution
18%
23%
41%
18%
>8.0%7.0-7.9%6.0-6.9%5.0-5.9%
*68.18% of patients who participated in the DMSE Program achieved a HbA1c≤7.0%


Disease Management Disease Management ““ProPro--CareCare””
Systematic method of identifying patients in need of care and Systematic method of identifying patients in need of care and contacting them for follow upcontacting them for follow up
Evidenced based management of chronic illnessEvidenced based management of chronic illness
Utilizes data mining of internal and external information Utilizes data mining of internal and external information sourcessources
Improves Provider payor profiles by Improves Provider payor profiles by ““cleaningcleaning”” claims dataclaims data

ProCare ROI ProCare ROI -- 5 Practices5 PracticesPilot Project 2Pilot Project 2ndnd half 2005half 2005
Using Using ““3 Most Prevalent Conditions3 Most Prevalent Conditions””
# of Pts Identified # of Pts Identified -------------------------- 23512351# of Visits scheduled # of Visits scheduled -------------------- 677677Success rate Success rate ------------------------------------------ 28%28%Total charges Total charges -------------------------------------- $151,367$151,367Expenses Expenses -------------------------------------------------- $4,158$4,158

EMR ROICOST SAVINGSCOST SAVINGS
CHARTS CHARTS –– SUPPLIES, PAPER, FORMS, SUPERBILLS, FOLDERS, SCRIPT PADSSUPPLIES, PAPER, FORMS, SUPERBILLS, FOLDERS, SCRIPT PADSCHART AVAILABILITY CHART AVAILABILITY –– ALL THE TIME IN MULTIPLE PLACESALL THE TIME IN MULTIPLE PLACESCHART PULLS CHART PULLS –– TIMETIMECHART PREP CHART PREP –– TIMETIMETRANSCRIPTION TRANSCRIPTION –– COSTS (50 COSTS (50 –– 90%)90%)SCANNED EOBsSCANNED EOBsDIRECT CHARGE ENTRYDIRECT CHARGE ENTRYREDUCED CALL BACKSREDUCED CALL BACKSSTREAMLINED ePRESCRIBINGSTREAMLINED ePRESCRIBINGDECREASE OVERTIME DECREASE OVERTIME
REVENUE ENHANCEMENTSREVENUE ENHANCEMENTSPAY FOR PERFORMANCE PAY FOR PERFORMANCE –– e.g. Bridges to Excellencee.g. Bridges to ExcellenceBETTER CODING BETTER CODING –– BETTER DOCUMENTATION (5 BETTER DOCUMENTATION (5 –– 15 %)15 %)CLINICAL RESEARCH CAPABILITIESCLINICAL RESEARCH CAPABILITIESENHANCED INCENTIVES FROM PAYERSENHANCED INCENTIVES FROM PAYERS
REDUCED MEDICAL ERRORREDUCED MEDICAL ERRORENHANCED SPACE UTILIZATIONENHANCED SPACE UTILIZATIONIMPROVED QUAILTY CAREIMPROVED QUAILTY CARE
LEGIBILITYLEGIBILITYDISEASE MANAGEMENTDISEASE MANAGEMENTREFERRAL TRACKINGREFERRAL TRACKINGHIGH RISK TRACKINGHIGH RISK TRACKINGPREVENTIVE MANAGEMENTPREVENTIVE MANAGEMENTDECISION SUPPORT TOOLSDECISION SUPPORT TOOLS

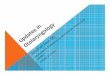
EMR Improvement on EMR Improvement on Documentation of CareDocumentation of Care
Network Comparison: November 2004 vs November 200598
.11%
89.5
8%
70.7
7%
65.2
6%
51.2
7%
63.0
7%
43.2
6%
28.1
1%
52.9
1%
37.3
0%
36.0
5%
10.9
4%
0.00
%
96.6
0%
87.4
8%
79.2
5%
74.2
4%
70.4
8%
62.7
9%
56.5
3%
50.6
3%
49.7
3%
42.7
5%
31.4
8%
12.8
8%
11.0
9%
99.8
1%
98.3
0%
94.7
0%
83.3
3%
79.3
6%
72.9
2%
72.9
2%
62.5
0%
69.7
0%
54.9
2%
36.5
5%
39.5
8%
18.1
8%
12.6
9%99.6
6%10
0.00
%
0.00%
20.00%
40.00%
60.00%
80.00%
100.00%
120.00%
Bloo
d Pr
essu
re
Med
Rev
iew
Lipi
d
Glu
cose
Toba
cco
Scre
en Die
t
Follo
w U
p Vi
sit
Exer
cise
Foot
Exa
m
Mic
roal
bum
in
ASA
Use
Eye
Exam
MN
T w
/RD
Smok
er
Jan 04 thru Sept 04
November 2004
November 2005