Embed Size (px)
Citation preview

Community Partnerships
to Reduce Readmissions
Part 1May 2, 2012
Objectives for Today
► Discuss how the GHA Hospital Engagement Network (HEN) and Alliant | GMCF are partnering with providers to reduce readmissions
► Illustrate the need to work with hospitals and nursing homes in your community to improve care transitions and reduce readmissions
Georgia QIO: Alliant | GMCF
The Quality Improvement Organization Program has evolved:►Bold improvement goals►Transformation at the systems level►Patient-centered approach►All improvers welcome►Everyone teaches and learns (“All teach, all learn”)►August 1, 2011 through July 31, 2014
3
4
Driving Improvement
CMS contracts with QIOs to improve health and health care for Medicare beneficiaries, utilizing three broad aims as the foundation:
Better health
Better care for people and communities
Affordable care through lowering costs by improvement
Aligned with National Priorities
QIO improvement initiatives support the:National Quality Strategy► Six priorities: safer care, coordinated care, person-
and family-centered care, preventive care, community health, making care more affordable
Partnership for Patients
► QIO initiatives can support your commitment
► Adverse drug events, CAUTI, CLABSI, patient and family engagement, reducing readmissions
5
QIOs Seek Improvement Synergies
6
Partnership Partnership for for
PatientsPatients
Regional Regional ExtensionExtensionCentersCenters
HospitalHospitalEngagementEngagement
NetworksNetworks
National National PrioritiesPriorities
PartnershipPartnership
Institute for Institute for Healthcare Healthcare
ImprovementImprovement
Aligning Aligning Forces for Forces for
QualityQuality
Quality Improvement Organizations
Four QIO Program Aims
►Make Care Beneficiary and Family Centered
►Improve Individual Patient Care
►Improve Health for Populations and Communities
►Integrate Care for Populations and Communities to Reduce Readmissions
7
Georgia PartnershipJoint Letter of Cooperatation
8
Georgia Partnership
9
1) Align effort to maximize resources
2) Decrease provider burden
3) Convene cross-setting groups
4) Monthly partnership meetings
5) Learning and Action Network - Collaborate on monthly webinars and face to face meetings
6) On-site technical assistance by QIO
Lessons learned from the QIO 9th SOWCare Transitions Initiative
► Importance of community collaboration– Providers talking, visiting each other, sharing
► Tailor solutions to fit community priorities– Community needs and leaders determine change
► Include patients and families– Incorporate beneficiaries when they are sick and
healthy
► Public outreach activities– Storytelling to support data
Results from the 9th SOW
11
► Hospital readmissions work also reduces hospital admissions
► Population-based measures of readmission going down
► Population-based measures of admission also going down
► Nursing Home and Home Health utilization has increased slightly; while 30-day readmission rates from Nursing Home and Home Health have decreased
► Promising measures of cost-savings
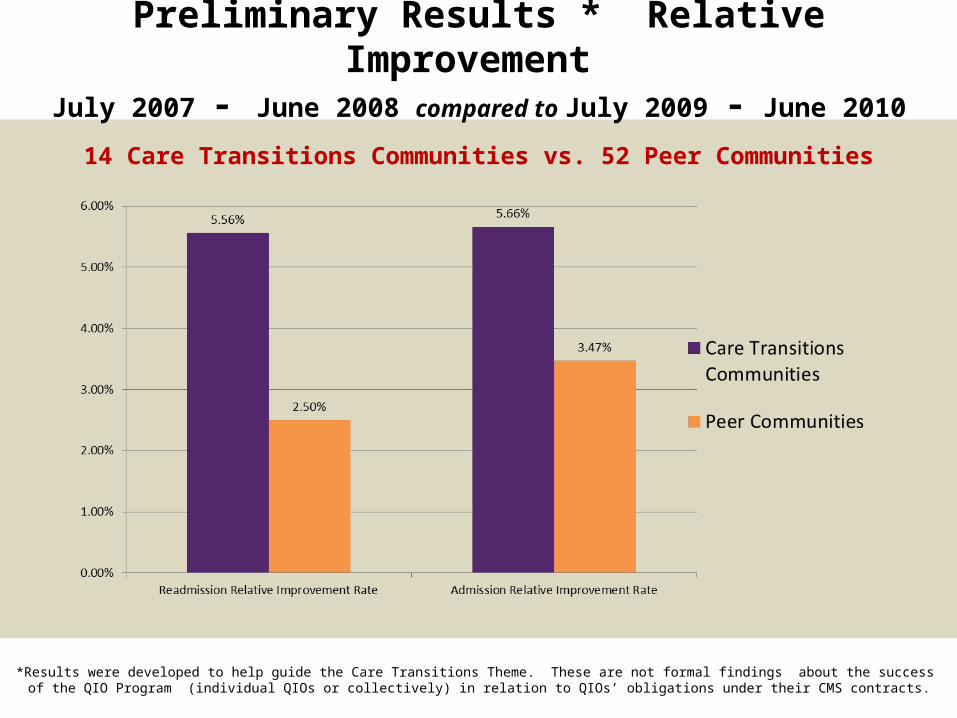
Preliminary Results * Relative Improvement July 2007 - June 2008 compared to July 2009 - June 2010
*Results were developed to help guide the Care Transitions Theme. These are not formal findings about the success of the QIO Program (individual QIOs or collectively) in relation to QIOs’ obligations under their CMS contracts.
14 Care Transitions Communities vs. 52 Peer Communities
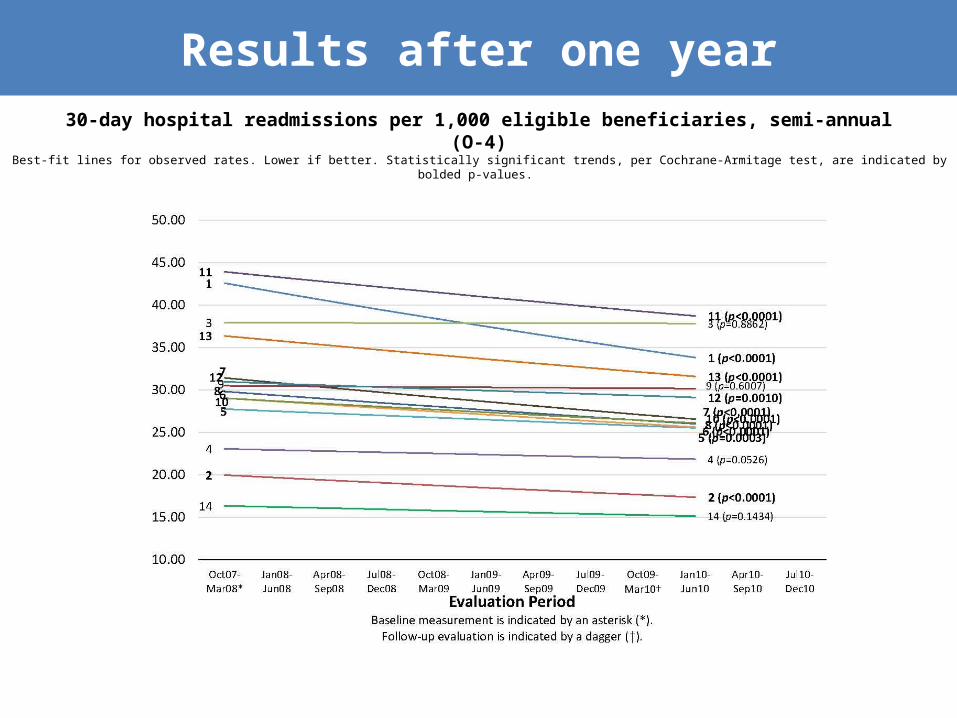
Results after one year30-day hospital readmissions per 1,000 eligible beneficiaries, semi-annual
(O-4)Best-fit lines for observed rates. Lower if better. Statistically significant trends, per Cochrane-Armitage test, are indicated by bolded p-values.
Recurring themes in successful communities
► Community cohesiveness
► Provider activation/will
► Strategic partners
► Cross-setting work
► Coaching as an intervention
► Strong community leadership (e.g., physician champions)
August 2011 – July 2014
15
Integrating Care for Populations & Communities Aim:
► Form effective care transitions coalitions
► Improve the quality of care for Medicare beneficiaries as they transition between providers
► Reduce 30-day hospital re-admissions (nationally) by 20% within 3 years
► Build capacity to qualify for funding through Section 3026 of the Affordable Care Act
The Strategy
16
► Define a community
► Identify service patterns associated with readmission
► Recruit and convene providers & partners
► Reduce unplanned 30d hospital readmissions for the community
► Using evidence-based interventions and tools
Why are readmissions a community problem?
Poor provider-patient interface medication management, no effective patient engagement strategies, unreliable f/u
Unreliable system support Lack of standard and known processes Unreliable information transfer Unsupported patient activation during transfers
No community infrastructure for achieving common goals

Why engage a community?
► Every readmission begins with hospital discharge
→ Every transition has 2 sides
► The problem of home
→ Patients are people, too► Isolated information is not safe medical management
→ Inevitably need to share► Visibility to drive improvement and mission
→ Providers are people, too
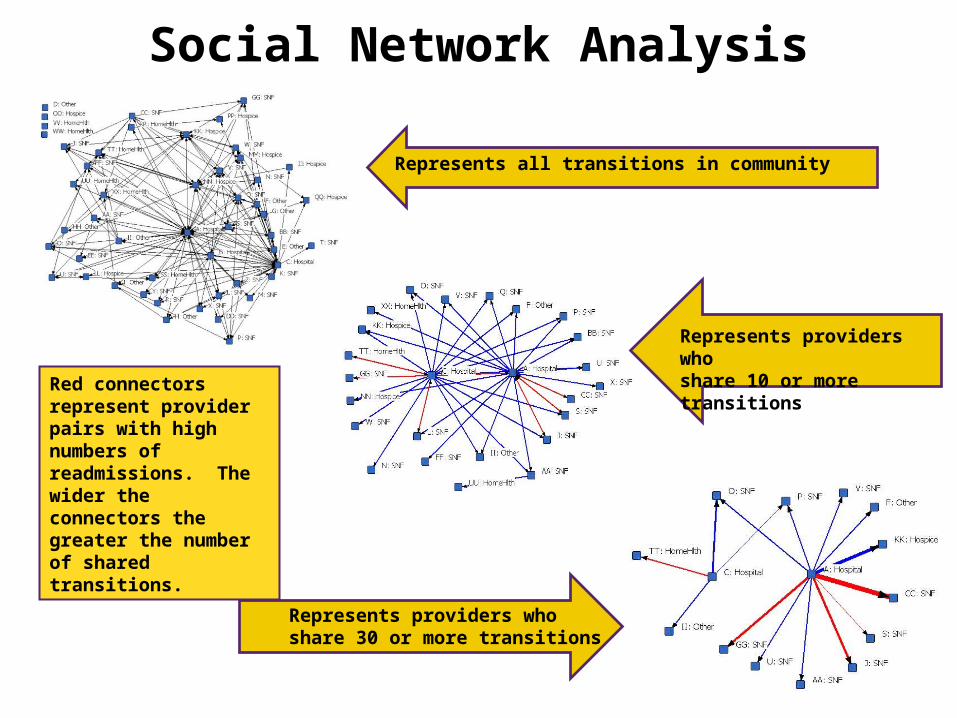
Represents all transitions in community
Represents providers who share 10 or more transitions
Represents providers who share 30 or more transitions
Red connectors represent provider pairs with high numbers of readmissions. The wider the connectors the greater the number of shared transitions.
Social Network Analysis
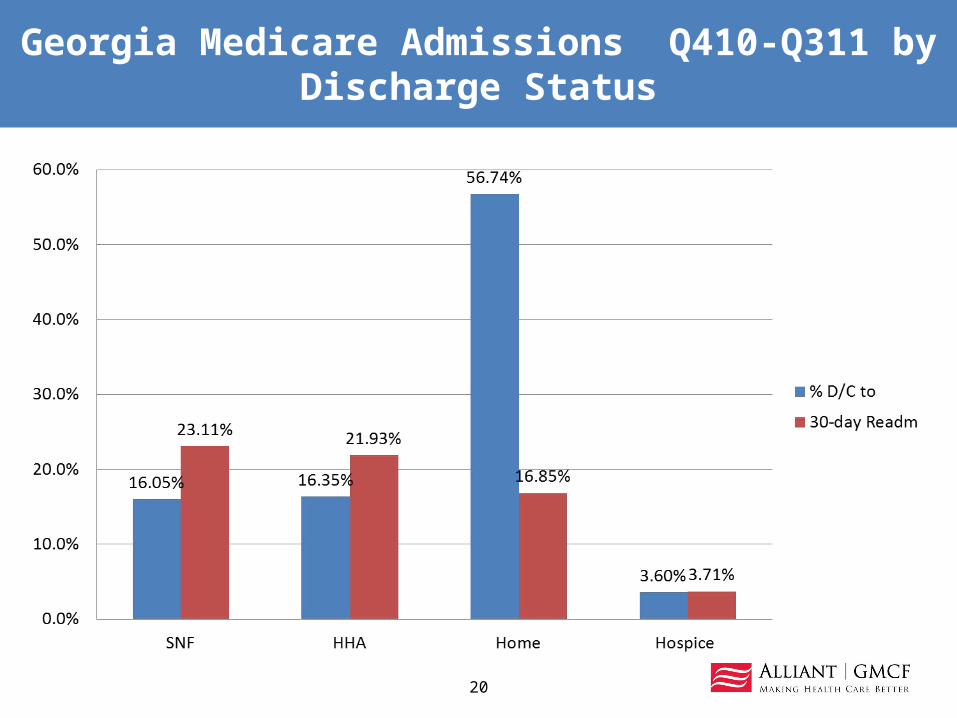
Georgia Medicare Admissions Q410-Q311 by Discharge Status
20
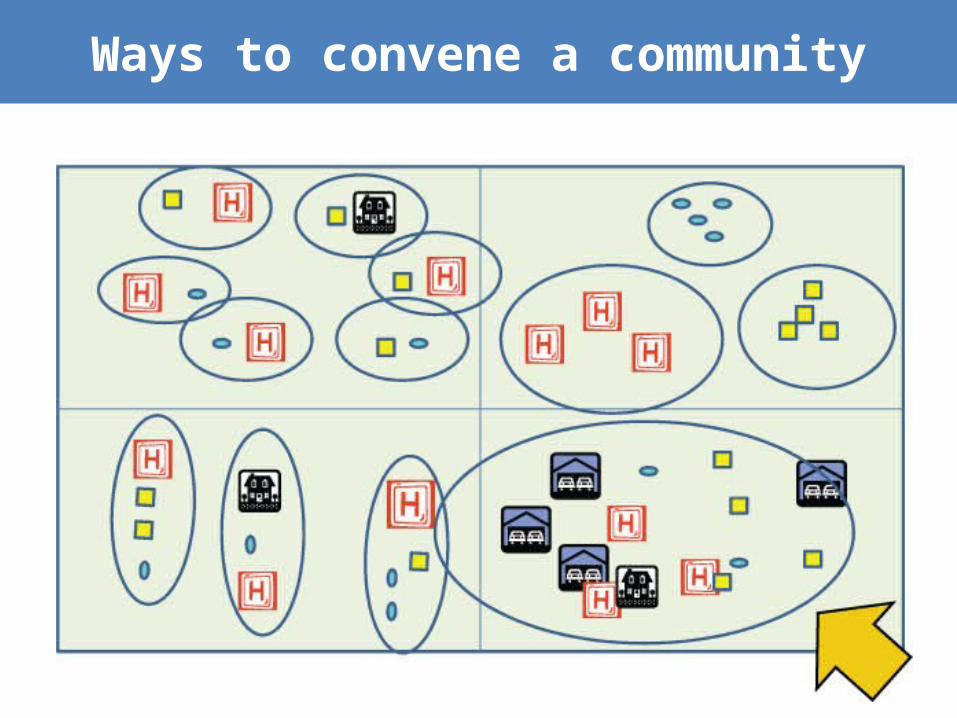
Ways to convene a community
Healthy Conversations for Safer Healthcare
22

Community Healthcare Connection Meetings
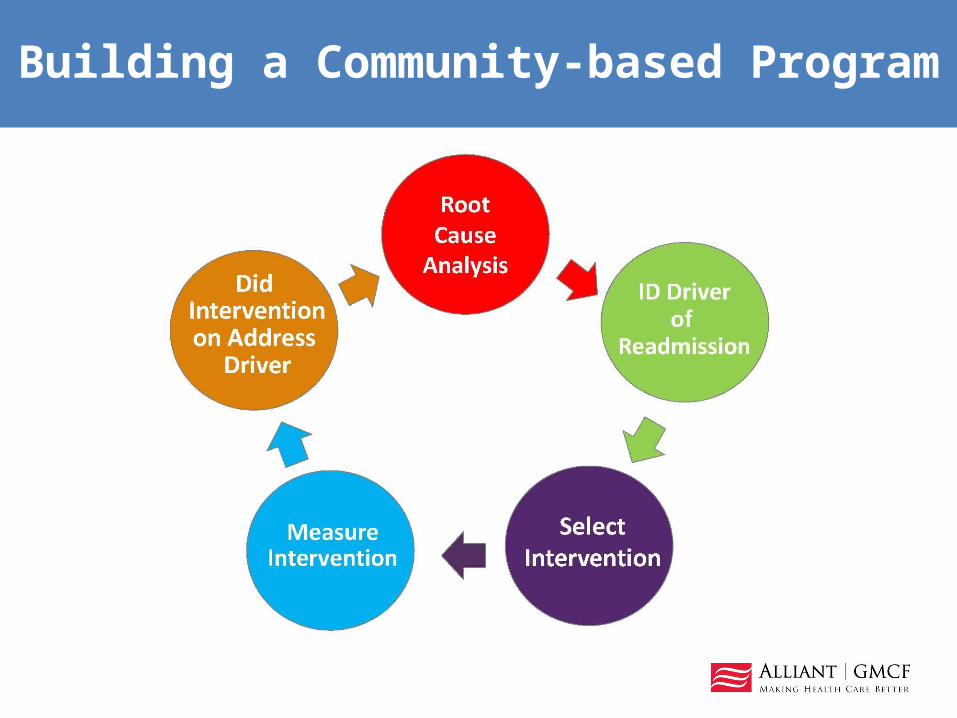
Building a Community-based Program
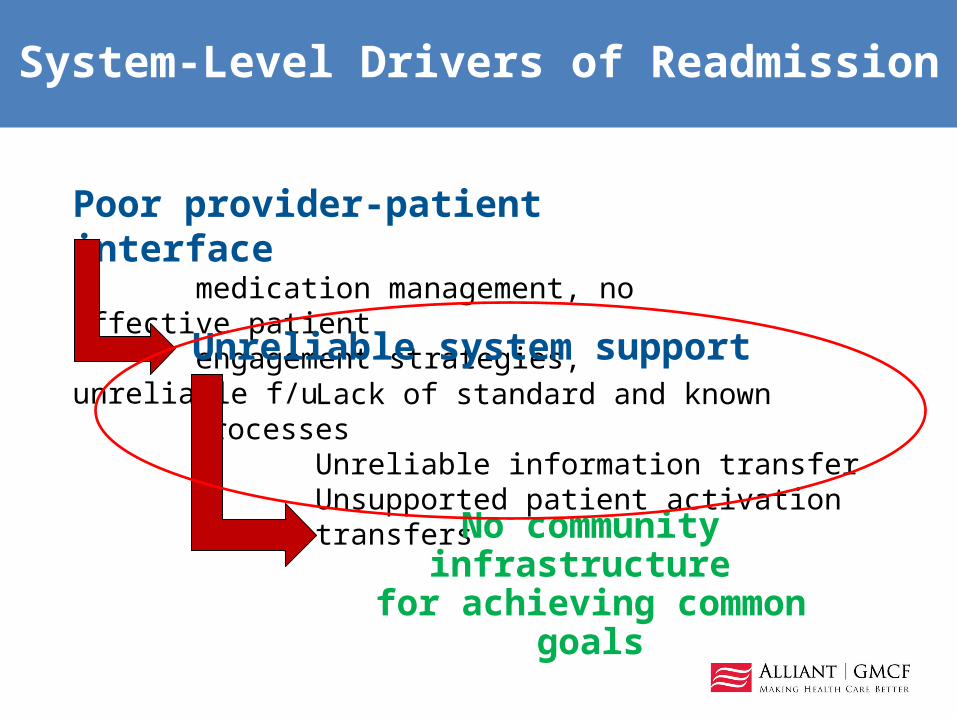
System-Level Drivers of Readmission
Poor provider-patient interface medication management, no effective patient engagement strategies, unreliable f/u
Unreliable system support Lack of standard and known processes Unreliable information transfer Unsupported patient activation during transfers
No community infrastructure for achieving common goals
Intervention Selection & Implementation Plan
26
► Results from the community-specific root cause analysis
► Existing local programs and resources
► Sustainability
► Community preferences
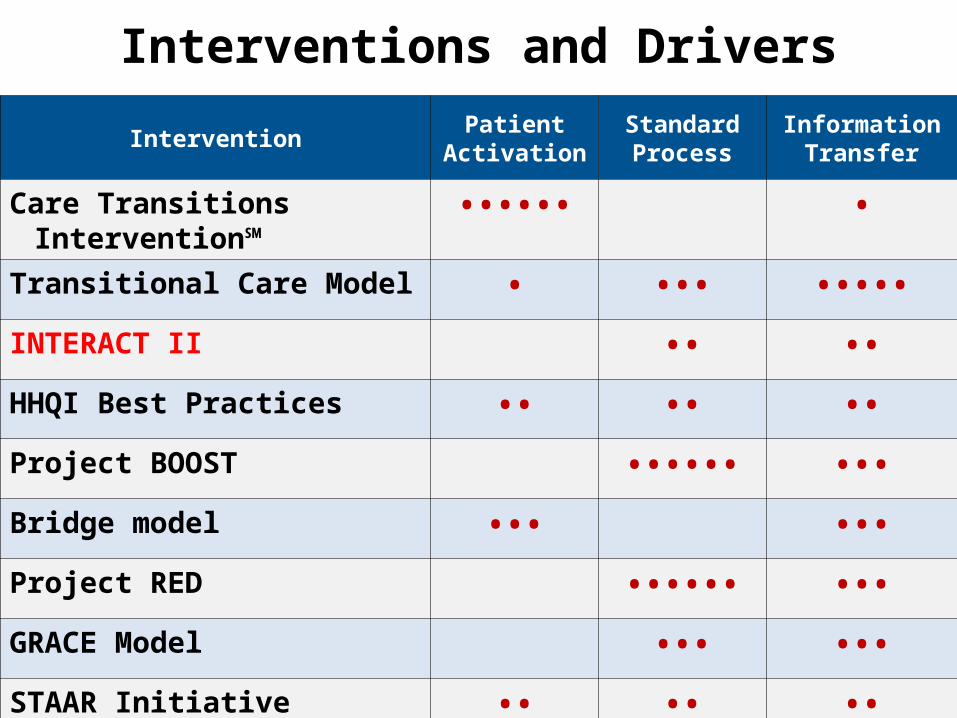
Interventions and Drivers
Intervention Patient Activation
Standard Process
Information Transfer
Care Transitions Intervention℠ •••••• •
Transitional Care Model • ••• •••••
INTERACT II •• ••
HHQI Best Practices •• •• ••
Project BOOST •••••• •••
Bridge model ••• •••
Project RED •••••• •••
GRACE Model ••• •••
STAAR Initiative •• •• ••
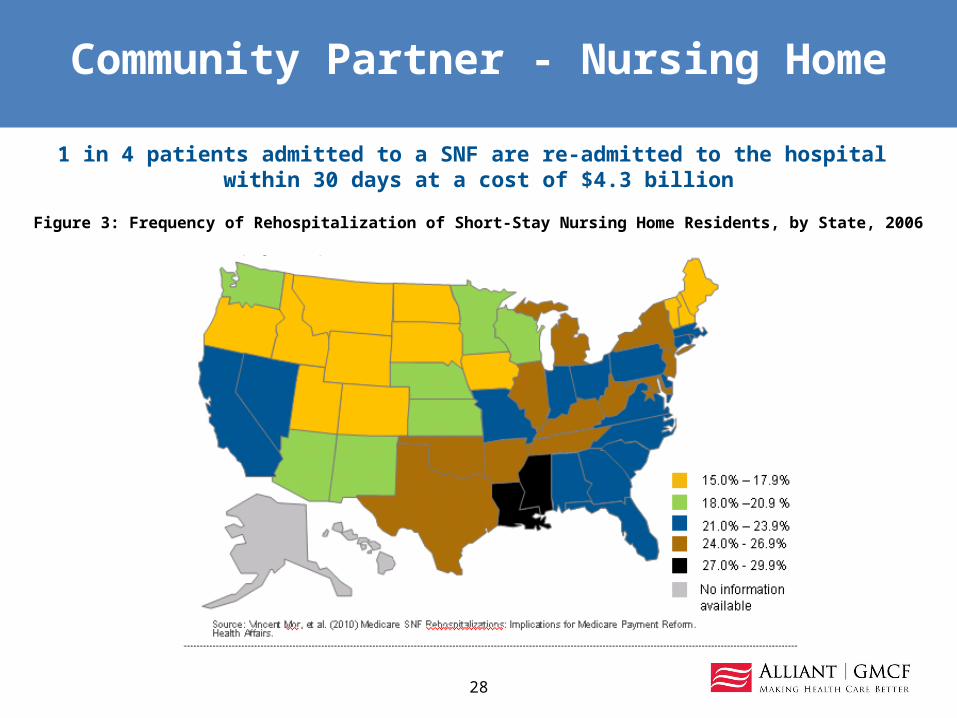
Community Partner - Nursing Home
28
1 in 4 patients admitted to a SNF are re-admitted to the hospital within 30 days at a cost of $4.3 billion
Figure 3: Frequency of Rehospitalization of Short-Stay Nursing Home Residents, by State, 2006

Community PartnerNursing Home Interventions
29
(“Interventions to Reduce Acute Care Transfers”)
Is a quality improvement program designed to improve the care of nursing home residents with
acute changes in condition
Nursing Home Interventions
► includes evidence and expert-recommended clinical practice tools, strategies to implement them and related educational resources
http://interact2.net
Nursing Home Interventions Why does this matter?
31
1) Hospital transfers are common and often result in complications in older NH residents
2) Some hospital transfers are preventable; some are not
3) Care can be improved, resulting in fewer complications and reduced cost
4) Cost savings to Medicare can be shared with NHs to further improve care
5) Financial and regulatory incentives are changing
Nursing Home InterventionsHospitalizations can cause many complications:
32
► Distress and discomfort for the resident and family► Delirium ► Polypharmacy► Falls► Incontinence and catheter use► Hospital acquired infections► Unintentional weight loss and poor nutrition► Immobility, de-conditioning, pressure ulcers
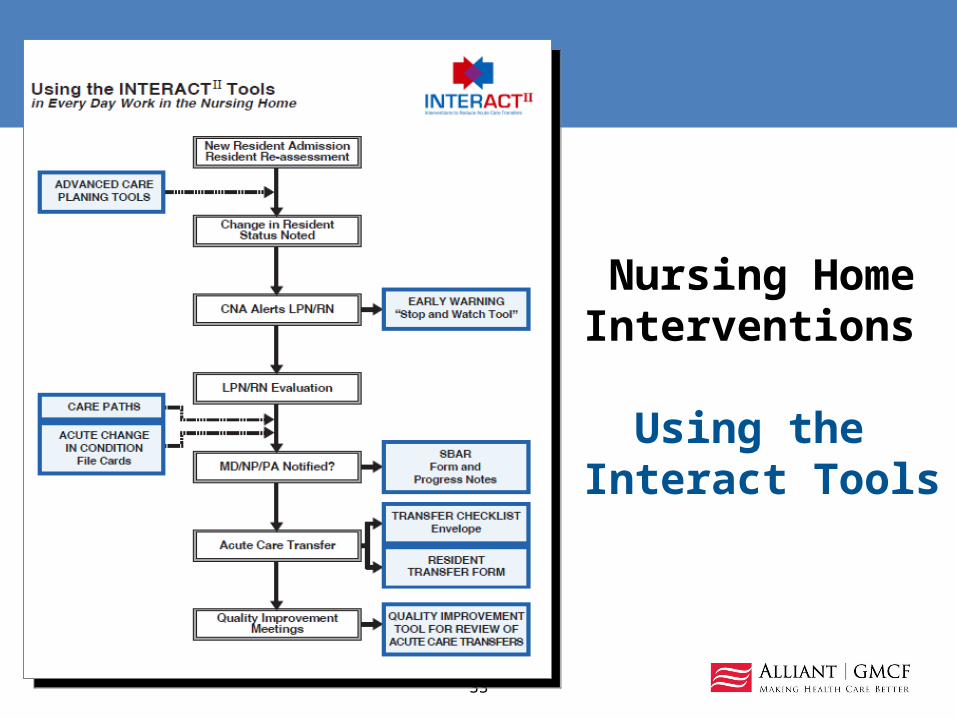
Nursing Home Interventions
Using the Interact Tools
33

Nursing Home 2012 Quality Goals
34
Interacting with your local hospitals► Schedule in-person meetings
– Offer a tour of your facility– Create an agenda
► Start with who staff you already interact with on a regular basis
– ED staff– Case Managers
► Emphasize 2-way communication
► Set mutual expectations
Interacting with your hospitals
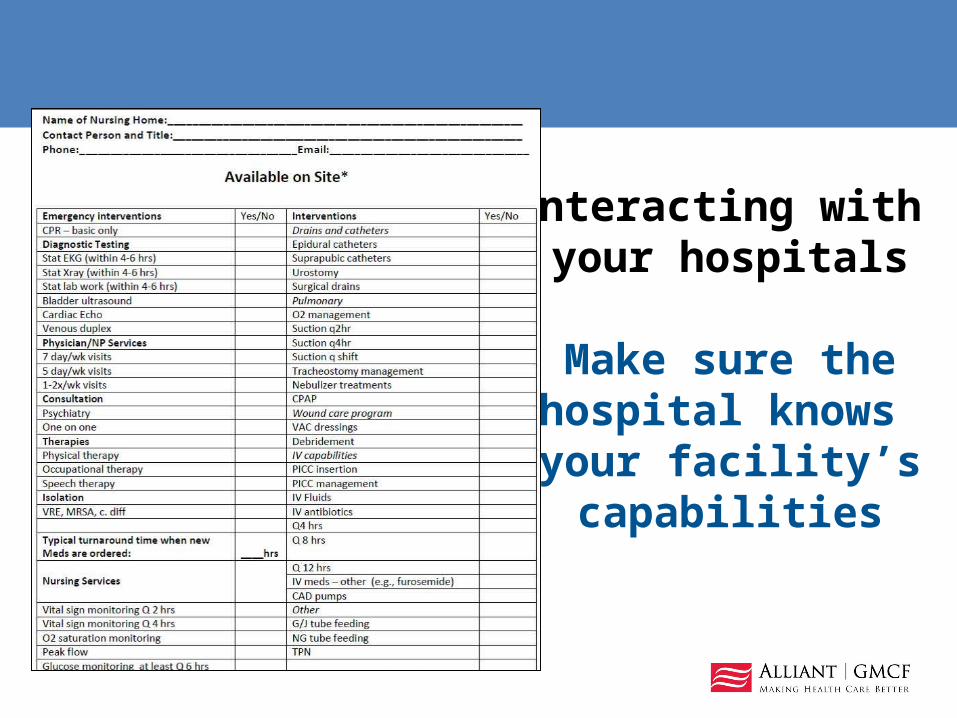
Interacting with your hospitals
Make sure the
hospital knows your facility’s capabilities
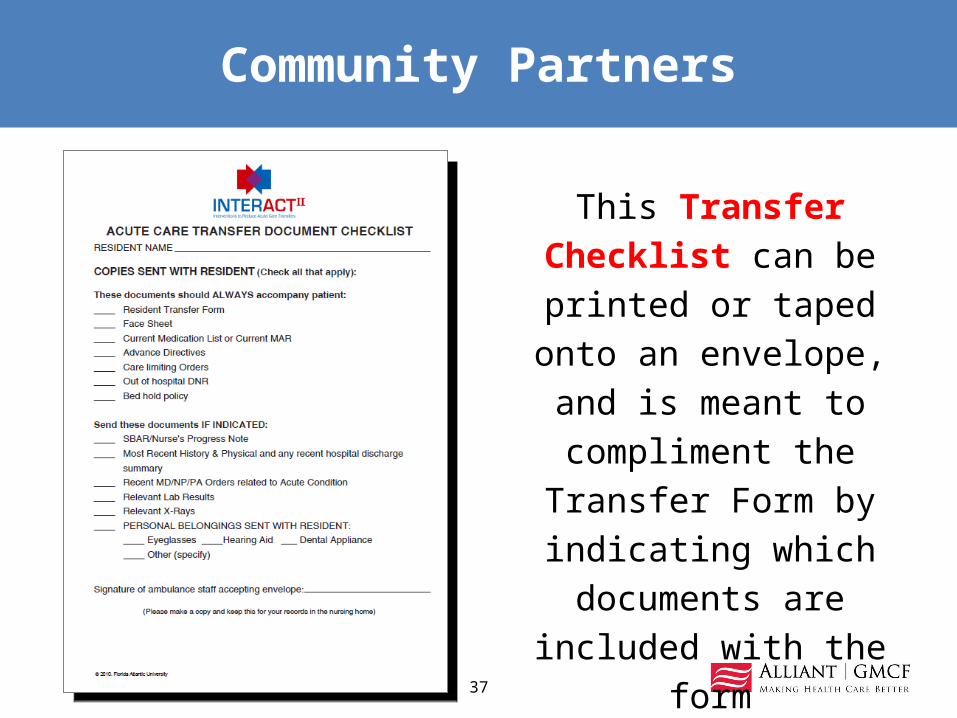
Community Partners
37
This Transfer
Checklist can be
printed or taped onto
an envelope, and is
meant to compliment
the Transfer Form by
indicating which
documents are
included with the form
Community Partners- Hospital
38
Hospital Interventions► Risk screen for post hospital needs and readmission
► Provide patient / caregiver with effective education prior to discharge
► Implement the Teach Back method
► Schedule outpatient follow-up appointment prior to discharge
► Implement comprehensive discharge planning that includes patient/caregiver Provide Patient Friendly Post Hospital Care Plan
► Call patients 48-72 hour post discharge
► Provide timely handover communication to next level of care ( nursing homes, MD, home health)
► Provide patient with follow-up phone number prior to discharge to call if has questions
In summary
39
► GHA HEN and Alliant | GMCF, the Georgia QIO, are partnering to maximize efforts to reduce readmissions in Georgia
► Community partnerships are essential to lowering readmissions
Now what?
40
► Find out when and where your local community readmissions coalition or cross-setting group meets and participate!
► Reach out to your referral hospitals and nursing homes to see what they are doing to improve care coordination and lower readmissions.
► Contact the QIO for on-site technical assistance and for resource support
Thank you
41
Community Healthcare Connection schedule – www.gmcf.org
INTERACT II – http://interact2.net
Mary Perloe – [email protected]
This material was prepared by Alliant | GMCF, the Medicare Quality Improvement Organization for Georgia, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. Publication No. 10SOW-GA-ICPC-12-44





























