Embed Size (px)
Citation preview
1 October 2017
CompanionA Publication of Indian Academy of Pediatrics, Kerala State Branch
Editor’s Page (3)
Message from President (4)
Message from President-Elect (5)
Secretary’s Message (6)
IAP Kerala Election Notification (7)
Ascertainment of Cause of death (8)
Child with behaviour problem (11)
Safe Media Use by Adolescents (15)
Beta Thalassemia (16)
Moments of Glory (19,21)
Refresh ur Radiology (20)
Pediatric Photo Quiz (21)
Journal Snippets (23)
Pediatric Malignancies (25)
Loop Diuretics (26)
Food Allergy (28)
Grand Rounds Case (30)
Acute Demyelination in a Child (33)
Failure to Thrive (36)
Pedi-Crossword (38)
Vol. 13 Issue 2 Kochi October 2017Pediatric
2 Pediatric Companion
3 October 2017
Editor’s Page
design & production : pixel studio, cochin @ 0484-2806301
Dear friends,
I am writing this message when health workers of this state are working day in and day out to eradicate two deadly diseases from our state, measles and rubella. Unlike previous years, we are facing a lot of resistance from anti vaccine hooligans. The work done by team IAP is commendable in this aspect and I am sure that final victory will be ours. The decision to introduce vaccination card at school entry is a mile stone in the history of health care achievements in Kerala. Other states will look at us with envy and respect and try to emulate us tomorrow.
IAP national election is nearing. Requesting all IAPians to cast your vote.
Good academic feast is waiting for us at sOUTh PEDICON Kollam and i wish the organizers a grand success.
“Blooming buds”, our President’s dream theme, was shown in thousands of schools and IAP meets as of now and the response was amazing. I take this opportunity to congratulate him who has shown the true spirit of leadership. Our secretary is doing a great work by coordinating thousands of activities all over the state, with his inherent cool and composed attitude and ever smiling face. hats off to you Dr Riaz!
Jai IAP,
Regards,
Dr. M. VijayakumarAddl. Professor, Dept. of PediatricsGovt. Medical College, CalicutMob : 94470 71637Email : [email protected]
President : Dr. M.N. VenkiteswaranVice President : Dr. V. Parmeswaransecretary : Dr. I. RiazTreasurer : Dr. Johny sebastianJoint secretary : Dr. D. Balachandar Imm. Past President : Prof Dr. Elizabeth K.E.President Elect : Dr. Mohammed Kunju
I A P S tAt e O f f I c e b e A r e r S 2 0 1 7Vice President Elect : Dr. M. NarayananEditor : Dr. M. VijayakumarWebsite Editor : Dr. shibu KizhaketharaNational EB Members : Dr. T. M. Ananda Kesavan Dr. K.K. Joshi, Dr. M.E. sugathanWomen’s Wing Co-ordinator : Dr. Prameela Jogi
P e D I At r I c c O M PA N I O N O f f I c e b e A r e r S 2 0 1 7
Dr. Ananda Kesavan T.M. Dr. Babu Francis C.A.Dr. sr. Betty JoseDr. Geeta GovindrajDr. Gireesh s.Dr. Jayakrishnan M.P.Dr. Jayakumar C.Dr. Jayakumar P.R.
Dr. JayasreeDr. Mohammed KunjuDr. Mohandas NairDr. Muhammed M.T.P.Dr. Narayanan M.Dr. Naushad K.Dr. Pisharody P.N.N.Dr. Remesh Kumar R.
Dr. T.V. RaviDr. santhosh M.K.Dr. silvan Mathews GeorgeDr. suresh Kumar E.K.Dr. Tonny MampillyDr. Venkiteswaran M.N.Dr. Zulfikar Ahmed
Advisory BoArd EditoriAl BoArdProf Dr MKC NairProf Dr TU sukumaranProf Dr Kurien ThomasDr shaji Thomas JohnDr Abraham K PaulDr s. s. KamathProf Dr PsN MenonProf Dr sushama BaiProf Dr Parvathy VKProf Dr Lalitha Kailas,Prof Dr Riyaz ADr. P.M.C. Nair
4 Pediatric Companion
M E S S A G E F R O M P R E S I D E N T
Dear Academicians,
I am immensely happy to note the brilliant activities of each Branch and Chapter presidents and secretaries for their committed community programmes. Let me express my sincere gratitude and appreciation to each and every one. No doubt our Companion Editor Dr. Vijayakumar gives encouragement for the researchers and academic inputs to the practicing pediatricians.
I also express my sincere gratitude to Dr. Riaz for the excellent support in implementing the projects.
The Government recognition to make IAP a major partner in planning programmes like IMR is a great achievement. Our vision to bring down IMR to a single digit became a reality. Every pediatrician can be proud of this great achievement. I should say the vision of IAP past Presidents and the team work of every member is well recognized. Under the Presidents action plan the programmes envisaged is almost complete with your great
support and enthusiasm. The programmes substance Abuse is well recognized by our Govt and various departments like Excise ,health and Education have given full support. My dream target of conducting 1000 programmes in the state would become a reality with your full support. TOT for Basic Life support, TOT for life skill education. TOT for antibiotic abuse, TOT for Learning Disability are almost reached the finishing stage. Training for Infant death audit with Govt and Unicef is also accomplished. The aim is to identify the cause of death and to find remedial measures thereby bringing down IMR to international standard.
The vision of IAP Kerala is to make Kerala as one of the model states in child health and to make our children intelligent, healthy and value educated New Gen
Jai hind, Jai IAP
Dr. M.N. Venkiteswaran President, IAP Kerala
PrEsidENts ACtioN PlAN1. Sbustance abuse Prevention Programme 1000 classes across the State with
projection of The Short Film - Blooming Buds
2. BLS for High Schhol & Higher secondary school students one training session by each branch [ 3 TOT for Doctors ]
3. Antibiotic abuse - 3 TOT
4. TIPPS Programme for Nurses - one programme for every branch.
5. Immunisation consensus.
6 . Infant death review
7. Life Skill Development One TOT
8 . Posoining Protocol
5 October 2017
M E S S A G E F R O M P R E S I D E N T 2 0 1 8
It is with great pleasure and immense satisfaction that I am jotting these lines. First of all I must thank all the IAP members of Kerala for electing me as Kerala state President of I AP for the year 2018. As Trivandrum District President for two terms I was able to do major pioneering work for the children of Kerala. Both the times we were able to get best branch awards at National level.
We in IAP are witnessing a flurry of activities and an unending enthusiasm. Each branch is doing its best regarding Presidential action plans and in disseminating Awareness about Child hood illnesses, social problems and immunisation realities. Dr. Anandakesavan, Dr. Pisharody, Dr. Parameswaran & Dr. Joshy must be congratulated for taking up the fight against anti vaccine lobby to their doorsteps, Dr. Venkiteswaran and Dr. Riyaz and team brought the IAP activities of 2017 into a higher level than previous years. Dr. Venkateswaran’s blooming buds documentary on drug abuse can be considered as a best professional work and it has been recognised by the government as well as the public and the media. The number of awards he got for the documentary tells the quality of the work and the yeoman service he has done to the society.
I place on record my congratulations to all the big contributors of IAP Kerala and child care at large. My special thanks to Dr. M.K.C. Nair, Dr. sachidanada Kamath,
D r . T . U . s u k u m a r a n , Dr. T.M. Anandakesavan, Dr. A.K. Ittoop, Dr. M.N. Venkiteshwaran, Dr. V. Parameswaran, Dr. D. Balachandar, Dr. Riaz I., Dr. Narayanan, Dr. Jayaraman, Dr. O. Jose, Dr. sugathan and all other IAP members for the love and affection showered upon me. We must specially appreciate our young turks like Dr. Thomas Varghese , Dr. Renjith from Calicut, Dr. Murari, Dr. sivaprsad, Dr. Abiram Dr. Indumathy, Dr. Anju Deepak etc.etc. I am excited by the unity and enthusiasm shown by our district office bearers and other members of IAP by flying to Delhi for the special general body meeting and fighting against the evils in the Central IAP.
As President of 2018 with my secretary Dr. Riyaz and other office bearers I wish that we will be able to match the work done by our previous stalwarts. My presidential action plans will be revealed during the south Pedicon. I request all the district branches and other subspecialty chapters to whole-heartedly support our 2018 teams activities.
seeking your blessings, suggestions and criticisms.
Yours in IAP,
Jai hind, Jai IAP
Dr. P.A.M. Kunju
6 Pediatric Companion
Respected teachers, seniors and dear friends,
I bring you warm wishes from the State IAP Office!
The IAP year 2017 is in its final lap and everyone
is busy preparing and sending the reports and getting
ready for the annual conference. Many branches this year had new sets of
office bearers and proved themselves as excellent leaders for tomorrow.
Dr. M.N. Venkiteshwaran, our dear President kept all of us in our toes
and successfully led us through the year and made us complete most of
the IAP action plan targets. The flagship program of the year, awareness
programme on the drug abuse prevention has penetrated into schools in
both urban and rural areas and was able to attract help as well as patronage
from government departments including Police, Anti Narcotic as well us
Education departments. IAP Kerala has now emerged as a major partner
in all activities the state plans for the health of children, be it the IMR
reduction or the MR Campaign. At this juncture we should thankfully
remember the excellent work done by our pioneering leaders like Dr MKC
Nair, Dr T U sukumaran and Dr sachidanandaKammath on making our
dear academy as strong as we are now.
As we are nearing the annual conference, this time south Pedicon, I
would like to place on record our sincere appreciation and gratitude to the
team Kollam for working hard all through the year to make the conference
a success. Let me stop by congratulating once again dear Dr.Vijayakumar
for making the journal better every time and astonishing all of us. I once
again thank my patrons, teachers and friends for being with me all through
the year.
Yours sincerely,
Dr. Riaz I.
S E C R E T A R Y ’ S M E S S A G E
7 October 2017
Nominations are invited for the following posts in IAP Kerala :
President & Vice President 2019
Last date for submitting Nominations. . . . . . . . . 4th Dec 2017
scrutiny. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7th Dec 2017
Last date for withdrawal of Nomination. . . . . .12th Dec 2017
sending ballot paper. . . . . . . . . . . . . . . . . . .16th-20th Dec 2017
Last date for receiving filled up ballot papers . . .8th Jan 2018
Counting of votes . . . . . . . . . . . . . . . . . . . . . . . . . . .9th Jan 2018
Deposit of Rs.5,000/- & Rs.2,500/- to be paid by the candidates applying for the post of President & Vice President respectively.
Nomination forms can be downloaded from IAP Kerala website : www.iapkerala.org
Completed Nomination forms to be sent to :
Dr. George F. Moolayil (Chief Election Commssioner),Emvee houseKizhthadiyoor P.O.Palai – 686574Kottayam Dist
by registered post, speed post or courier
Iap Kerala Election Notification

8 Pediatric Companion
ascertainment of Cause of death
Cause of death is defined as (a) the disease or injury that initiated the train of morbid events leading directly to death, or (b) the circumstances of the accident or violence that produced the fatal injury. In addition to the underlying cause of death, the report should contain the entire sequence of events leading to death as well as other conditions significantly contributing to death.
The underlying cause of death can be divided into three parts
Q The immediate cause of death is the final disease, injury, or complication directly causing death
Q The underlying cause of death is the disease or injury that initiated the chain of events that led directly and inevitably to death.
Q Other significant diseases, conditions or injuries that contributed to death but which did not result in the underlying cause of death given above.
A properly completed cause-of-death section provides an etiologic explanation of the order, type, and association of events resulting in death. The initial condition that starts the etiologic sequence is specific if it does not leave any doubt as to why it developed. For example, sepsis is not specific because a number of different conditions may have resulted in sepsis, whereas pneumococcal meningitis is specific. In certifying the cause of death, any disease, abnormality, injury, or poisoning, if believed to have adversely affected the decedent, should be reported. If the use of alcohol and/or other substance, a smoking history, a recent pregnancy, injury, or surgery was believed to have contributed to death, then this condition should be reported. The conditions present at the time of death may be completely unrelated, arising independently of each other;
they may be causally related to each other, that is, one condition may lead to another which in turn leads to a third condition; and so forth. Death may also result from the combined effect of two or more conditions.
The cause-of-death information should be the physician’s best medical OPINION. Causes of death on the death certificate represent a medical opinion that might vary among individual physicians. Report each disease, abnormality, injury, or poisoning that the physician believes adversely affected the decedent. A condition can be listed as ‘‘probable’’ if it has not been definitively diagnosed.
the ascertainment of cause of death The ascertainment of cause of death must be
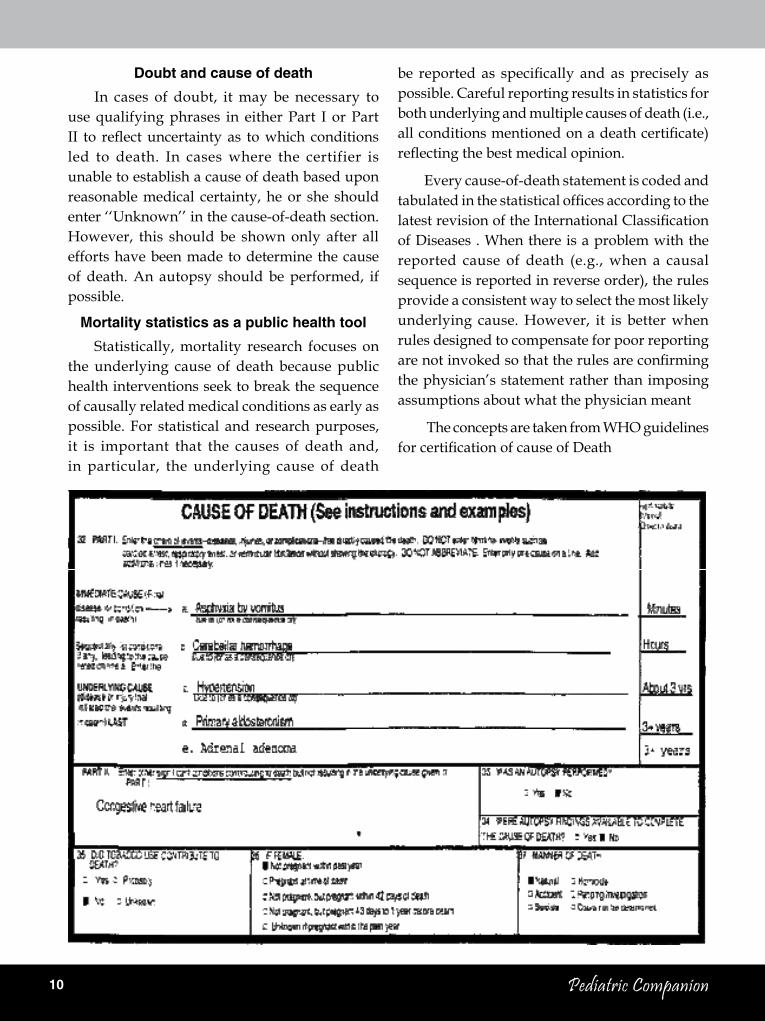
completed by the attending physician and should follows guidelines recommended by the World health Organization. The cause-of-death section consists of two parts (Figure 1). The first part is for reporting the sequence of events leading to death, proceeding backwards from the final disease or condition resulting in death. so each condition in Part I should cause the condition above it. A specific cause of death should be reported in the last entry in Part I so there is no ambiguity about the etiology of this cause. Other significant conditions that contributed to the death, but did not lead to the underlying cause, are reported in Part II.
The immediate cause of death is reported on line (a). This is the final disease, injury, or complication directly causing the death. An immediate cause of death must always be reported on line (a). It can be the sole entry in
dr. sankar v.H. (Addl. Professor) dr. santhosh Kumar A. (Prof. & HOD)
Dept. of Paediatrics, SAT Hospital Govt. Medical College, Trivandrum
9 October 2017
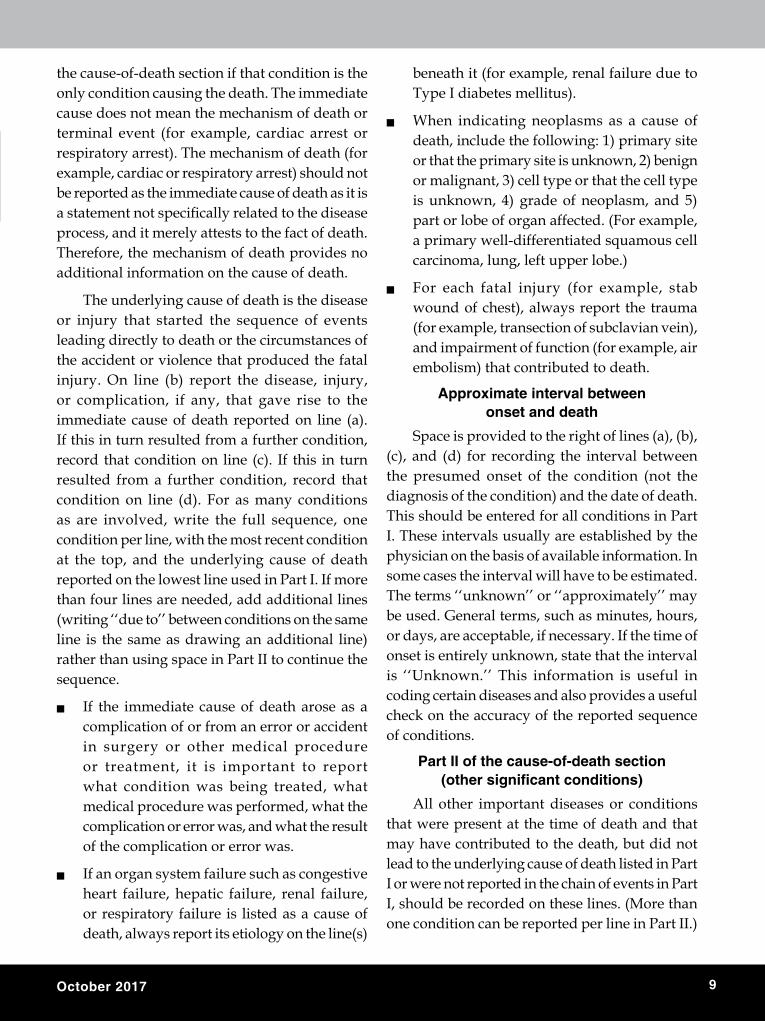
the cause-of-death section if that condition is the only condition causing the death. The immediate cause does not mean the mechanism of death or terminal event (for example, cardiac arrest or respiratory arrest). The mechanism of death (for example, cardiac or respiratory arrest) should not be reported as the immediate cause of death as it is a statement not specifically related to the disease process, and it merely attests to the fact of death. Therefore, the mechanism of death provides no additional information on the cause of death.
The underlying cause of death is the disease or injury that started the sequence of events leading directly to death or the circumstances of the accident or violence that produced the fatal injury. On line (b) report the disease, injury, or complication, if any, that gave rise to the immediate cause of death reported on line (a). If this in turn resulted from a further condition, record that condition on line (c). If this in turn resulted from a further condition, record that condition on line (d). For as many conditions as are involved, write the full sequence, one condition per line, with the most recent condition at the top, and the underlying cause of death reported on the lowest line used in Part I. If more than four lines are needed, add additional lines (writing ‘‘due to’’ between conditions on the same line is the same as drawing an additional line) rather than using space in Part II to continue the sequence.
Q If the immediate cause of death arose as a complication of or from an error or accident in surgery or other medical procedure or treatment, it is important to report what condition was being treated, what medical procedure was performed, what the complication or error was, and what the result of the complication or error was.
Q If an organ system failure such as congestive heart failure, hepatic failure, renal failure, or respiratory failure is listed as a cause of death, always report its etiology on the line(s)
beneath it (for example, renal failure due to Type I diabetes mellitus).
Q When indicating neoplasms as a cause of death, include the following: 1) primary site or that the primary site is unknown, 2) benign or malignant, 3) cell type or that the cell type is unknown, 4) grade of neoplasm, and 5) part or lobe of organ affected. (For example, a primary well-differentiated squamous cell carcinoma, lung, left upper lobe.)
Q For each fatal injury (for example, stab wound of chest), always report the trauma (for example, transection of subclavian vein), and impairment of function (for example, air embolism) that contributed to death.
Approximate interval between onset and death
space is provided to the right of lines (a), (b), (c), and (d) for recording the interval between the presumed onset of the condition (not the diagnosis of the condition) and the date of death. This should be entered for all conditions in Part I. These intervals usually are established by the physician on the basis of available information. In some cases the interval will have to be estimated. The terms ‘‘unknown’’ or ‘‘approximately’’ may be used. General terms, such as minutes, hours, or days, are acceptable, if necessary. If the time of onset is entirely unknown, state that the interval is ‘‘Unknown.’’ This information is useful in coding certain diseases and also provides a useful check on the accuracy of the reported sequence of conditions.
Part ii of the cause-of-death section (other significant conditions)
All other important diseases or conditions that were present at the time of death and that may have contributed to the death, but did not lead to the underlying cause of death listed in Part I or were not reported in the chain of events in Part I, should be recorded on these lines. (More than one condition can be reported per line in Part II.)
10 Pediatric Companion
doubt and cause of deathIn cases of doubt, it may be necessary to
use qualifying phrases in either Part I or Part II to reflect uncertainty as to which conditions led to death. In cases where the certifier is unable to establish a cause of death based upon reasonable medical certainty, he or she should enter ‘‘Unknown’’ in the cause-of-death section. however, this should be shown only after all efforts have been made to determine the cause of death. An autopsy should be performed, if possible.
Mortality statistics as a public health toolstatistically, mortality research focuses on
the underlying cause of death because public health interventions seek to break the sequence of causally related medical conditions as early as possible. For statistical and research purposes, it is important that the causes of death and, in particular, the underlying cause of death
be reported as specifically and as precisely as possible. Careful reporting results in statistics for both underlying and multiple causes of death (i.e., all conditions mentioned on a death certificate) reflecting the best medical opinion.
Every cause-of-death statement is coded and tabulated in the statistical offices according to the latest revision of the International Classification of Diseases . When there is a problem with the reported cause of death (e.g., when a causal sequence is reported in reverse order), the rules provide a consistent way to select the most likely underlying cause. however, it is better when rules designed to compensate for poor reporting are not invoked so that the rules are confirming the physician’s statement rather than imposing assumptions about what the physician meant
The concepts are taken from WhO guidelines for certification of cause of Death

11 October 2017
approach to a child with behaviour problem
When a child presents with abnormal behaviour or behaviour problem, the first step is to decide whether the behaviour is truly abnormal or problematic. Parent’s perception of abnormal behaviour may not always be true. The line separating “normal” and “abnormal” is very thin. Parenting skills and family factors greatly in-fluence the behaviour of the child. If the behaviour is causing problems in the family or at school, there is need for intervention. The next step is to decide whether the behaviour is appropriate to the age of the child. Behaviour which is normal in a 4 year old child may be abnormal in a10 year old child. ABC (A- what causes the behaviour; B-What is the behaviour; C- What are the consequences of the behaviour) will help to decide the nature of the behaviour problem and plan management.
There are two approaches to behaviour problems in a child. Dimensional ap-proach, where one concentrates on individual behaviours and categorical approach where one considers diagnostic categories. Delinquent behaviour, aggressive be-haviour, inattentive behaviour, hyperactive behaviour, impulsive behaviour etc are problem behaviours. Behaviour syndromes are categorised depending upon the confluence of behaviours. Thus, attention deficit hyperactivity disorder (ADhD), aut-ism spectrum disorder (ASD), oppositional defiant disorder, conduct disorder (CD) etc are behaviour disorders. Even though categorised based on the manifested be-haviour there are definite biological correlates to behaviour disorders and ADhD and AsD are neurodevelopmental disorders where the developing brain is affected.
so the next question is whether the behaviour fit into any known behaviour syndromes. We
will see the clinical characteristics of some of the common behaviour disorders.
Attention Deficit Hyperactivity Disorder (ADHD)
Attention Deficit hyperactivity Disorder (ADhD) is the most common child psychiatric disorder with a prevalence rate of 5-10% among school aged children. The three cardinal clinical features of ADhD are hyperactivity, im-pulsivity and inattention. There are three sub-types of ADhD - Predominantly hyperactive - impulsive type, predominantly inattentive type and the combined type. In majority of children all the three features are present. Children with hyperactivity present early during the preschool period itself whereas children with predominantly inattention present when attention problems affect academic functioning and hence usually during the primary school or secondary school age. As the age advances hyperactivity comes down and attention problems become more predominant.
There are no diagnostic tests for ADhD and the diagnosis is made based on clinical criteria. According to DsM 5, to make a diagnosis of ADhD, the symptoms should be present for more than six months duration and should be present in more than one setting. (eg. school and home). The symptoms must begin before the age of 12 years and should not be secondary to other medical or psychological disorders. The symptoms should cause impairment in social, academic or occupational functioning. Co-morbid psychiatric disorders like oppositional defiant
P. KrishnakumarAddl. Prof. of Paediatrics & Director
Institute of Mental Health and Neurosciences, Kozhikode

12 Pediatric Companion
disorder, conduct disorder, learning disorder, anxiety disorders and depression are common in children with ADhD. Tics disorder and seizure disorder may coexist.
Genetic factors, perinatal brain insult, environmental toxins, endocrine abnormalities and structural brain defects are implicated in the aetiology of ADhD. Thyroid hormone disorders and heavy metal poisoning like lead poisoning can lead to symptoms of ADhD and should be ruled out. Micronutrient deficiencies like iron deficiency, zinc deficiency may be associated with ADhD and should be treated. Food colouring agents and preservatives are reported to cause ADhD symptoms and should be looked for while treating children with ADhD.
Abnormalities in the level of various neurotransmitters like dopamine, nor-epinephrine and epinephrine in the CNs are associated with ADhD. Drugs effective for ADhD act through modifying the functioning of neural circuits involving these neurotransmitters.
The treatment of ADhD includes psycho-social interventions and pharmacotherapy. Pharmacotherapy should be combined with psychosocial interventions. Drugs used to control the symptoms of ADhD are usually divided into two groups - stimulant drugs and the non- stimulant drugs. stimulant drugs include methylphenidate, dextroamphitamine and their combinations. The non stimulants include atomoxetin, clonidine, and risperidone. For optimum results, pharmacotherapy should be combined with psychosocial interventions. Treatment of ADhD is not just prescribing drugs. Academic and school problems and problems in the family environment can precipitate and exacerbate the behaviour problems in a child with ADhD. These issues should be addressed along
with pharmacotherapy. Counselling regarding the importance of balanced diet, avoiding junk foods and food preservatives should be part of the treatment program. Correction of iron deficiency, zinc deficiency and other micronutrient deficiencies will go a long way in improving the behaviour and attention span. Advice regarding life style modification should be given. The importance of rest, play, TV time, and adequate sleep should be discussed with parents and children.
Autism Spectrum Disorder (ASD)
Autism spectrum Disorder (AsD) is characterised by impairment in reciprocal social communication, impairment in social interaction and restricted repetitive and stereotyped patterns of behaviour. The onset of the problem is during the early developmental period.
Impairment in social interaction is manifested as impairment in the use of non-verbal behaviours (such as eye to eye contact, facial expressions, body postures and gestures) and failure to develop age appropriate peer relationships, inability to share enjoyment, interest or achievements with others and lack of social or emotional reciprocity. Impairment in communication is manifested as delay or total lack of development of spoken language, impairment in the ability to initiate and sustain conversation, stereotyped or repetitive use of language. There could be stereotyped and repetitive motor mannerisms like body twisting, hand or finger flapping or twisting, inflexible adherence to routines or rituals. There may be associated features like abnormal fears and phobias, hyperactivity, eating and sleep problems, temper tantrums, aggressive behaviour, self injurious behaviour like wrist biting. seizures occur in about 25% of children. Though children with autism can have normal or

13 October 2017
above normal intelligence, majority of them have varying degrees of intellectual disability.
Asperger’s syndrome is a type of high functioning autism characterised by impairment in social interaction and repetitive, restricted and stereotyped behaviour with no delay in language development and no cognitive impairment.
The usual clinical presentation is in the toddler period with history of lan-guage delay. The parents may complain of odd behaviour. Motor milestones may be normal or delayed. It is important to look for hearing impairment in any child presenting with speech delay. Observe the child for any impairment in reciprocal social interaction. Most often behaviour observation for sufficient time will help to reach the diagnosis.
AsD may be the result of varying aetiologies causing insult to the developing brain. There is no laboratory diagnosis and no characteristic EEG or MRI findings. Since the aetiology varies, the clinical presentation also varies. It is in this context that the concept of autism spectrum disorder is relevant. The spectrum concept refers to children with mild autistic features at one end and with severe autistic features at the other end. Early detection and sensorimotor stimulation and initiation of remedial therapy will help a lot to overcome the disability. Parents should spend quality time with the child and promote reciprocal social interaction. Early initiation of preprimary schooling with special attention to the child will help in places where specialised therapy services are not available.
disruptive, impulse control and conduct disorders
Disruptive, impulse control and conduct disorders include behaviour disorders characterised by problems in the self control
of emotions and behaviour. These problems usually violates the rights of others and bring the individual into conflict with law or social norms or authority. The behaviour disorders in this group include oppositional defiant disorder,conduct disorder and intermittent explosive disorder. These disorders usually have onset during childhood or adolescence.
Oppositional Defiant Disorder (ODD)
ODD is characterised by irritable or angry mood, argumentative or defiant behaviour and vindictive nature. The problem is more common in boys and begin in the preadolescent age group. Child with ODD is most often angry or irritable. he often looses temper and is often touchy and easily annoyed. Arguments with authority figures or other children is common and refuses to comply with rules and regulations. he may blame others for his mistakes or misbehaviour. Vindictive nature may be present. The behaviour problem is usually present in one situation only. The usual clinical presentation is with history of behaviour problems at home while at school the child is well behaved. The problem is usually with adults or peers whom the child knows well. sibling rivalry may be present. ODD may be associated with ADhD. Anxiety disorders and depression may coexist. ODD may precede childhood onset type of conduct disorder or ODD may be milder type of conduct disorder.
Conduct Disorder (CD)
Conduct disorder is characterised by aggression to people and animals, destruction of property, deceitfulness or theft and serious violation of rules. Tendency towards aggression to people and animals result in behaviours like bullying or threatening others, initiating physical fights with others, using weapons to harm others,

14 Pediatric Companion
forced sexual activity and cruelty to animals. Tendency to destroy property is manifested as deliberate fire setting with the intention of causing damage and deliberate destroying property belonging to others. Deceitfulness or theft includes lying and stealing, cheating others like “con man”. Children with CD may present with history of behaviours like truancy (deliberately staying away from school and wandering outside), running away from home or staying away from home without parental consent. Various types of delinquent behaviour or substance abuse may be associated with CD.
There are three subtypes of conduct disorder, based on the age of onset of the symptoms- Childhood onset type, adolescent onset type and unspecified onset type. In the childhood onset type the onset of symptoms is before 10 years while in the adolescent onset type there are no conduct symptoms before the age of 10 years. The childhood onset conduct disorder usually present with problems in peer relation ship at school. There may be preceding features of ODD and associated ADhD. The problems can be mild moderate or severe. some children with CD have guilt or remorse over the behaviour, but others have no such prosocial feelings. There may be socialising type and non socialising type of children with CD. The prognosis is better in adolescent onset conduct disorder with most of them recovering before adulthood. The childhood onset type of CD is more serious and there is chance of developing antisocial personality or continuing problems into adult age. Treatment consists of behaviour intervention and counselling. Drugs may help to regulate mood or control behaviour.
Concept of Comorbidity
several disorders may coexist in a child. A
child with AsD may have features of ADhD like hyperactivity, impulsivity and inattention. A child with CD or ODD may have associated ADhD. Depressive disorders and anxiety disorders may be asso-ciated with many behaviour disorders. Scholastic backwardness and specific learning disorders may be the cause of many behaviour issues and may also occur secondary to behaviour disorders. One should look for co-morbid disorders and these should be considered while planning management strategies.
similarly physical problems like anaemia and micronutrient deficiency may con-tribute to behaviour problems in children. Behaviour problems are more in children with chronic physical illnesses like bronchial asthma and epilepsy. Dietary interven-tion and life style modification will be essential component of management of beha-viour disorders in children and adolescents.
recent behaviour change in a child
Onset of the behaviour disorder will help to reach a diagnosis. In neurodevelopmental disorders the symptoms will be present for long duration from early developmental period itself. Any child with acute behaviour change needs detailed evaluation to rule out organic causes. Neurodegenerative disorders may present initially with change in behaviour. Behaviour change may be the early feature of neurological disorders like ADEM or auto immune encephalopathies or ICsOL. Episodic abnormal behaviour may be manifestation of seizure disorder. Once organic causes are ruled out look for any stress full life events.Behaviour change may be manifestations of anxiety disorders depressive disorders or adjustment disorders.

15 October 2017
Safe Media Use by adolescentsThe media (e.g. Whatsapp and Google) are a
great blessing if used rightly, but a tremendous danger to the ignorant and the careless. We should teach adolescents – including our own children – how to use it wisely.
1. Limit media usagestrictly to 2 hours a day, and preferably 1 hour. This gives adolescents less time for mischief or getting into trouble, and more time to study. ‘Media’ includes the TV + computer (surfing, Facebook) + mobile (games, whatsapp, phoning).
2. Teach them the safety rulesa. Beware of strangers• Avoid chatting online with anyone you do
not know in the real world. That cute girl or smart guy you arechatting with online may actually be a nasty adult male.
• If you decide to meeta person you only know online, you should meet that person in a public placealong with a parent (or at least with a friend.)
b. Never respond to messages that hurt your feelings or make you feel uncomfortable. stop the communication, and tell a parent right away.
c. Never give out personal information• This includes your name, age, address,
phone number, personal interests, name of your school, or friends’ names.
• Never exchange photos with a stranger.• Never reveal passwords, not even to a
boyfriend, girlfriend, or best friend.
3.Explain issues to them, as theyare more likely toget into trouble from ignorance than irresponsibility.
• Surfing: is a common and safe activity, but a lot of online information is unreliable, and some websites arepornographicor violent.
• Ask them about cyberbullying: “it is very common, have youor any of your friendsever been bullied?... Never say something mean online that you wouldn’t say to someone in person. Never gossip or spread false rumoursusing whatsapp or chat or FB”.
• Inform them about sexting: A girl may sext as a way of flirting with her boyfriend. But he may feel boastful and show it to his best friend, and then it may go viral.
4. Monitor their online activity. a. Keep the home computer in a public area.
Up to high school, and probably until they go to College, do not give them personalsmartphones, tablets or laptops.
b. Parents should regularly check their young adolescents’ online history to see which sites they are visiting, but only afterinforming the children that they are doing it. Parents can share what they did online, and ask them daily which sites they visited, whom they chatted with, whether they made any post on Facebook or elsewhere.
c. Older adolescents need, and have a right to, much more privacy. But parents should demand to be kept informed of any new apps they’ve downloaded, or new sites they are visiting.
5. Visitthem onlineIf the adolescent is on Facebook or Twitter,
one of his parents too should be on it. One, so that they know what are the advantages and risks of Facebook and can guide them. Two, to monitor their posts. Make it a family policy that all family members on Facebook should ‘friend’ each other.
6. Consider using parental controls. Filtering software like NetNanny
• can restrict the time the adolescent spends on the computer.
• They can filter out websites that discuss drugs, alcohol, pornography or violence, or use filthy language.
• They caneven record his chats and copy his inbound and outbound emails. This horrible invasion of privacy is justifiable only when the parent has a genuine concern about drugs or bullying or stranger danger.
dr Newton luiz Dhanya Mission Hospital
Potta, Trichur

16 Pediatric Companion
atypical presentation of a case of Beta ThalassemiaBeta-thalassemia an autosomal recessive
disorder characterized by decrease in beta globin chains has been associated with osseous abnormalities which was first described by Cooley and Lee in 1927. historically fractures were cited as frequent problem in thalassemia patients prior to optimization of transfusion and chelation therapy (1). The pathogenesis of bony changes in thalassemia was attributed to the underlying massive ineffective erythropoiesis, erythroid expansion of medullary bone with thinning of cortical bone, as well as metabolic and endocrine dysfunction secondary to transfusional iron load(2).
Case reportA 4 year old apparently normal girl presented
with fracture of left forearm following a trivial fall. she was seen by the orthopedician who saw some abnormal bony changes along with the fracture and was hence referred to department of pediatrics. she also gives history of being treated with oral iron 2 months back as she was noted to be pale but was not further evaluated.
On examination child had pallor and jaundice. Abdominal examination showed firm liver palpable 5cm below the right costal margin and spleen was palpable 7cm below left costal margin.
On investigation: hb : 6.2gm/dl (MCV-71f/L;MCh-20pg/dl;MChC-29;RDW-50).LFT showed indirect hyperbilirubinemia (Total bilirubin-4.5mg/dl; direct bilirubin-1.6mg/dl) with mildly elevated transaminases (sGPT-61IU/L;sGOT-52IU/L).P eripheral smear showed anisopoikilocytosis with microcytes, target cells, tear drop cells and polychromatophilic cells. Reticulocyte count was 5.9% with corrected reticulocyte count of2.9%. serum ferritin was 462ng/ml. serum calcium was 8.4mg/dl, serum phosphorus was 2.3mg/dl and alkaline phosphatase was 236IU/L. her parents were
also investigated. Peripheral smear of father was also suggestive of thalassemia. high Performance Liquid chromatography of the child was suggestive of thalassemia major and that of father was thalassemia minor.
As the child was noted to have pallor 2 months back she was started only on oral iron therapy. No further evaluation was done at that time. There is no history of any blood transfusions and hence no use of any chelating agents in the past.
The child was first seen by an orthopedician for fracture of forarm. This child was referred to us for the abnormal bone shadow of the hand, for further evaluation(Fig 1-4). she was diagnosed to have thalassemia major and was given blood transfusion. she was also started on folic acid and calcium. Child is now kept under followup.
discussionFracture was documented in thalassemic
patients in the period of 1960s-1970s when transfusion and chelation therapies were not as widely used as of today(3). The management of these patients has improved dramatically with hyper transfusion therapy which in turn has reduced the ineffective erythropoietic process and prevented bone deformities. The overall fracture prevalence among all thalassemia syndromes was 12.1%.Fractures occurred more frequently in Thalassemia Major (16.6%) and Thalassemia Intermedia (12.2%) compared to E/Beta (7.4%) and alpha (2.3%).
The skeletal changes described in beta thalassemia are : fractures, premature epiphyseal closure, osteoartropathy and chelating agents side
Ananda Kesavan t.M. sithara surendran, Karthik Balasundaran
Dept. of Pediatrics Govt. Medical College Thrissur.

17 October 2017
effects. But usually these changes are reported in older children and in chidren on chelation therapy.
The first detailed study of beta thalassemia with bone deformities and fractures published in 1976 showed fractures in 25 of 75 (33%) patients (4). But later the studies in the 1980s reported a high fracture frequency, which ranged from 30 to 50% (5). Lower fracture rates, close to 15 to 19%, were reported in 1990s among transfusion-dependent beta-Thalassemia patients of Mediterranean and Middle Eastern origins (6).In beta thalassemia patients, the incidence of bone fractures range between 38 and 41% and occur as a consequence of falls in over 50% of cases. These fractures involves the upper limbs more frequently while spine, hips, and pelvis are affected in about 10% of cases (7).
Dines et al observed that fractures were common in patients above the age of 10 years, with no sex predilection(3). Basanagoudar et al observed that mean age at fracture occurrence was 9.2years(8).
According to Perisano et al the various mechanisms involved in the pathogenesis of bone modifications in beta thalassemia were as follows (1):
1. Impairments in osteoblast activity- Significant growth retardation, delayed bone age, reduced bone mineral density and low serum IGF-I levels was seen in children with thalassemia. Bone histomorphometry of these patients revealed increased osteoid thickness with delayed and defective osteoid maturation and mineralization(9).
2. Abnormal osteoclast activity- An association between increased circulating levels of proresorptive cytokines and altered bone turnover has been detected in thalassemic patients .Thalassemia patients showed no differences in plasma levels of osteoprotegerin (OPG) in the presence of higher circulating levels of RANKL, with consequent lower OPG/RANKL ratio and increased osteoclastic activity(10).
hence this provides the rationale for the use of bisphosphonates, potent inhibitors of osteoclast function for the management of thalassemia induced osteoporosis.
3. hormonal Factors- hormonal dysfunction like diabetes, thyroid/ parathyroid disorders and hypogonadism are believed to underlie the altered bone turnover observed in these patients. In female thalassemic patients, low estrogen and progesterone levels enhance osteoclast activity and reduce bone formation, while in males, low testosterone levels result in a decrease in its stimulatory effects on osteoblast proliferation and differentiation. In addition, insufficiency of the Gh-IGF-1 axis leads to impaired osteoblast proliferation and bone matrix formation, while increasing osteoclast activation (9).
4. Genetic Factors- Genetic factors have been shown to play a role in the pathogenesis of osteopenia in thalassemic patients. A G→T or TT polymerism in the regulatory region of COLIA1 at the recognition site
for transcription factor sp1 is associated with the presence of osteoporosis. Vitamin D receptor (VDR) polymorphisms at exon 2 (FokI) and intron 8 (BsmI) may be involved in determining the stature and bone mineral density at femoral neck and lumbar spine in thalassemic patients(10).
5. Iron Overload- This impairs osteoid maturation and inhibits local mineralization resulting in focal osteomalacia.
6. Chelation therapy- The iron chelating agent deferoxamine inhibits osteoblast and fibroblast proliferation, osteoblast precursor differentiation, DNA synthesis and collagen formation while it causes increased osteoblast apoptosis (8).
The various radiological features can be divided into those affecting the skeleton ( axial and appendicular) and those occurring extra-medullary.
I. Axial skeletal changes: skull and facial bones, show widening of the diploic space with

18 Pediatric Companion
thinning of the tables. sub periosteal reactions in the form of bony spicules may be seen radiographically and result in a classic “hair-on-end” appearance. Poor pneumatization of paranasal sinuses secondary to hypertrophy of osseous structures and a consequent prominence of the lateral margins of the malar eminences, together with anterior and medial displacement of developing teeth is also seen.
In vertebral bodies, only the primary bone trabeculae are preserved which gives a vertical striated appearance due to thickened vertical trabeculae. While in severely affected patients, biconcavity of the superior and inferior margins of the vertebral bodies or compression fractures may occur(11).
II. Appendicular skeleton: Phalanges show cortical thinning, osteopenia, and coarsening of the trabeculae with possible loss of normal tubulation, which frequently results in a squared or sausage-shaped configuration. The expanded bone marrow destroys the medullary trabeculae with subsequent trabecular coarsening resulting in the appearance of “cob-webbing” in the pelvis, medullary lucencies involving the metaphyseal and diaphyseal regions of humeri and femori(19). Ribs show variable spectrum of appearance from normal to osteopenia, localized lucencies, broadening (widening), thin cortices, cortical erosions and prominent vascular impression at inferior aspect of the lower ribs which has been described as, “rib within a rib” appearance(12).
III. Extra medullary hematopoiesis: It is manifested as soft tissue shadows within posterior and anterior mediastinum as well as para vertebral location(12).
hence fractures is frequent in patients with thalassemia but a case of asymptomatic thalassemia patient initially presenting with a fracture only is quite uncommon.
ConclusionBone changes seen in beta thalassemia
patients occur as a result of the hematological diseases’ complications, iron overload and also as
a consequence of the chelation therapy. Vertebral osteoporosis and long bone fractures are usually the major cause of morbidity in these patients. Timely identification and correction of nutritional and hormonal deficits must be ensured in these patients in order to reduce the incidence of osteoporosis and increase overall bone strength..
Thalassemia can present with a simple fracture .We have also observed that there has been a dearth of case reports of thalassemia presenting with pathological fractures alone at such an early age. hence all the cases of anemia must be extensively evaluated for its cause in order not to miss out hematological diseases.
reference1. Perisano.C. ,Marzett i .E. ,spinel l i .M.s. ,Cal l .C.
M.A.; Physiopathology of BoneModifications in β-Thalassemia;Anemia; Volume 2012, Article ID 320737, 5 pages.
2. Canale VC. Beta Thalassemia: a clinical review. Pediatr Ann. 1974; 3:6–30.
3. Dines DM, Canale VC, Arnold WD. Fractures in thalas-semia. J Bone Joint surg Am. 1976; 58(5):662–6.
4. V o g i a t z i a . M . G . , M a c k l i n b E . A . , F u n g E . B . , Vichinsky.E.;Prevalence of fractures among the Thal-assemia syndromes in North America; Bone. 2006 April ; 38(4): 571–575.
5. Exarchou E, Politou C, Vretou E, Pasparakis D, Madessis G, Caramerou A. Fractures and epiphyseal deformities in beta-thalassemia. Clin Orthop. 1984; 189:229–33.
6. Katz K, horev G, Goshen J, Tamary h. The pattern of bone disease in transfusion-dependent thalassemia major patients. Isr J Med sci. 1994; 30 (8):577–80.
7. haidar.R, K. M.Musallam, and A.T. Taher, “Bone disease and skeletal complications in patients with β thalassemia major,”Bone, vol. 48, no. 3, pp. 425–432, 2011.
8. Basanagoudar PL, Gill ss, Dhillon Ms, Marwaha RK. Fractures in transfusion dependent beta thalassemia—An Indian study. singapore Med J. 2001; 42(5):196–9.
9. Morabito.N., G. T. Russo, A. Gaudio et al., “The “lively”cytokines network in β-thalassemia major-related osteoporosis,”Bone, vol. 40, no. 6, pp. 1588–1594, 2007.
10. Ferrara, s. M. R. Matarese, M. Francese et al., “Effect of VDR polymorphisms on growth and bone mineral density in homozygous β thalassaemia,” British Journal of haematology, vol. 117, no. 2, pp. 436–440, 2002.
11. Orzincolo C, Castaldi GI, Bariani L, Franceschini F, Corcione s, scutellari P. Circumscribed lesions in the thalassaemic skull. skeletal Radiol 1998;17:344—7.
12. Lawson JP, Ablow RC, Pearson hA: The ribs in thalas-semia. II. The pathogenesis of the changes. Radiology 1981 sep; 140(3): 673-9.

19 October 2017 19 october 2017
M o m e n t s o f G l o r y
Dr. M.N. Venkiteswaran getting another honour by Priests of OCD Congregation on
the Doctors Day
Antibiotic Awareness Mid zone TOT at Cochin. Dr Kuttappan, DMO Ernakulum
inaugurates.
Drug abuse awareness progaramme - mid zone inauguration at N Parur
By the Stae President Dr MN Venkiteswaran
Our President Dr MN Venkiteswaran has been awarded as the Best Activist in the state. He received Gold
Trophy, Cash prize and Certificate from Houn’ble Chief Minister Sri Pinaryi Vijayan in presence of Health Minister Shylaja Teacher, Minister Kadannapilly
Ramakrishnan and Sremathy Teacher MP
Dr. M.N. Venkiteswaran getting another honour for the substance abuse programme organised by Deputy
Commissioner, Eranakulam. District Panchayath President, Asha Sanil adorning the Ponnada
The Short film ‘Blooming Buds’ is adjudged as the Best Short film. Dr. M.N. Venkiteswaran receiving the
Bharathan Smaraka award at Alleppey
20 Pediatric Companion20 Pediatric Companion
R E F R E S H U R R A D I O L O G Y dr.t.M. Ananda KesavanDept of Pediatrics
Govt. Medical College, Thrissur
(Answers on Page 27)
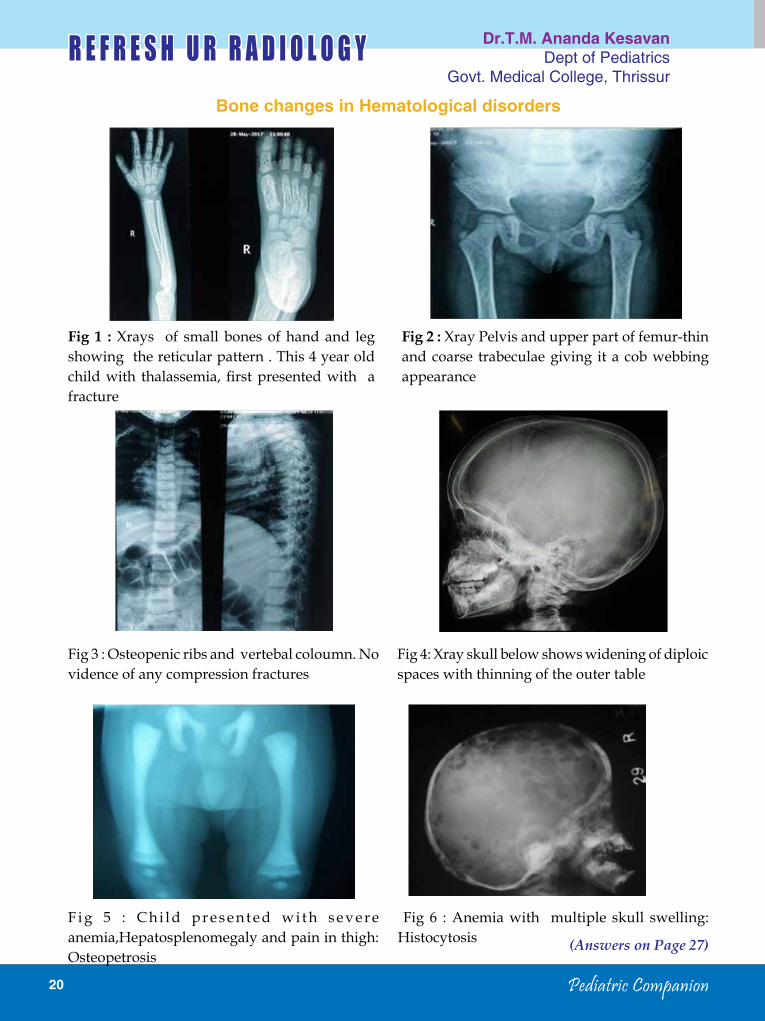
Bone changes in Hematological disorders
Fig 1 : Xrays of small bones of hand and leg showing the reticular pattern . This 4 year old child with thalassemia, first presented with a fracture
Fig 3 : Osteopenic ribs and vertebal coloumn. No vidence of any compression fractures
F i g 5 : C h i l d p r e s e n t e d w i t h s e v e r e anemia,hepatosplenomegaly and pain in thigh: Osteopetrosis
Fig 6 : Anemia with multiple skull swelling: histocytosis
Fig 4: Xray skull below shows widening of diploic spaces with thinning of the outer table
Fig 2 : Xray Pelvis and upper part of femur-thin and coarse trabeculae giving it a cob webbing appearance
21 October 2017
(Answers on Page 27)
21 october 2017
P E D I A T R I C P H O T O q U I z dr. sankar v.H. Addl. Professor, Geneticist
SAT, Trivandrum
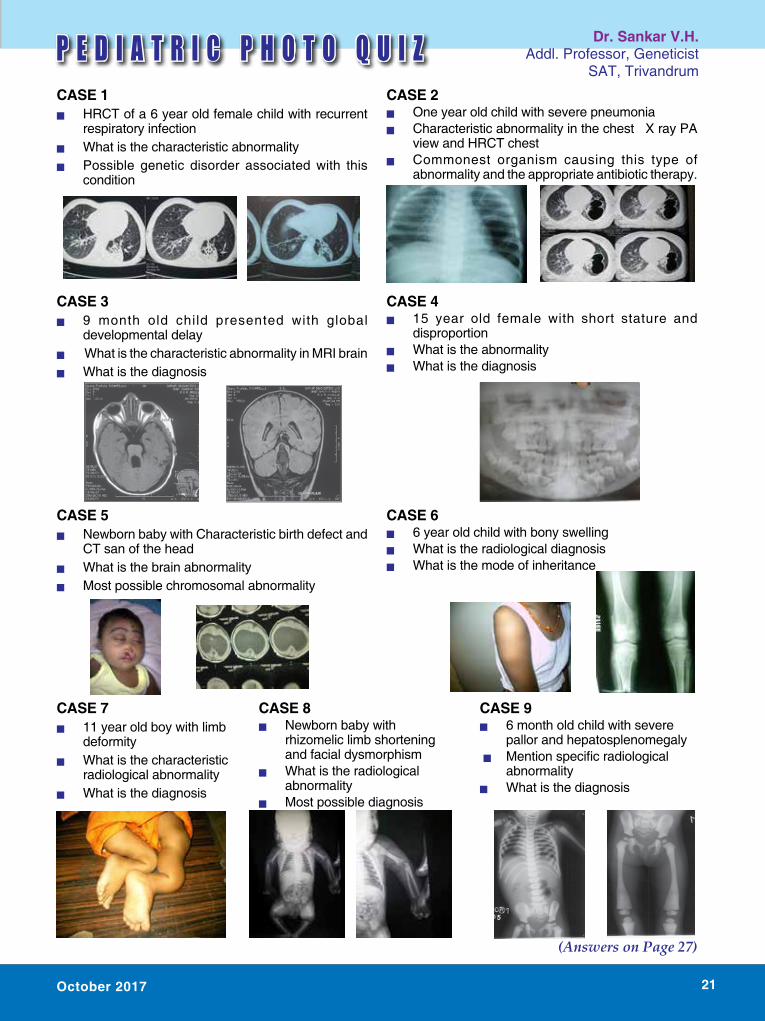
CAsE 1 Q HRCT of a 6 year old female child with recurrent
respiratory infection Q What is the characteristic abnormalityQ Possible genetic disorder associated with this
condition
CAsE 3 Q 9 month old child presented with global
developmental delayQ What is the characteristic abnormality in MRI brainQ What is the diagnosis
CAsE 5 Q Newborn baby with Characteristic birth defect and
CT san of the head Q What is the brain abnormalityQ Most possible chromosomal abnormality
CAsE 7 Q 11 year old boy with limb
deformityQ What is the characteristic
radiological abnormality Q What is the diagnosis
CAsE 2 Q One year old child with severe pneumonia Q Characteristic abnormality in the chest X ray PA
view and HRCT chestQ Commonest organism causing this type of
abnormality and the appropriate antibiotic therapy.
CAsE 4 Q 15 year old female with short stature and
disproportionQ What is the abnormalityQ What is the diagnosis
CAsE 6 Q 6 year old child with bony swelling Q What is the radiological diagnosisQ What is the mode of inheritance
CAsE 8 Q Newborn baby with
rhizomelic limb shortening and facial dysmorphism
Q What is the radiological abnormality
Q Most possible diagnosis
CAsE 9 Q 6 month old child with severe
pallor and hepatosplenomegaly Q Mentionspecificradiological
abnormalityQ What is the diagnosis
4
3
22 Pediatric Companion22 Pediatric Companion
IAP Cochin : Inauguration of Immunise Kochi programme
Dr. Nimmi E.J., Secretary, IAP Wayanad, leading the Awareness Rally
Installation of IAP Trichur Branch
Drug awareness class by the Prsident Dr. M.N. Venkiteswaran for NCC cadets at Aluva
Prof. Dr. Muhamed Kunhu receiving IMA Best Doctor Award from President IMA Kerala State
Dr. V.G. Pradeep Kumar
Dr. Ranjith P., Secretary, IAP Kozhikode with staff and students of Darul Huda Islamic
university during MR Vaccination program
Release of Ind Jl of Ped Neuro Dr. M.K.C. Nair, Vice Chancellor, KUHS inaugurating the NUTRICON - Trivandrum
Prof. Dr. Muhamed Kunhu receiving Best Doctor Award from Hon. Minister of Health and Family
Welfare
GAstroKid 2017, 5th Annual Conference of Pediatric Gastroenterology Chapter, IAP Kerala
on 27.8.2017 at Thiruvananthapuram.
BLS training class to NCC cadets by Dr Sivaprasad
M o m e n t s o f G l o r y
Inauguration of National Pediatric Neurology Conference at Lulu International Convention Centre, Thrissur by Hon
Education Minister Prof.C. Raveendranath

23 October 2017
was conducted in an outpatient hematology clinic at a Us tertiary care hospital.
Three mg/kg of elemental iron once daily as either ferrous sulfate drops or iron polysaccharide complex drops for 12 weeks.
What they found:From baseline to 12 weeks, mean hemoglobin increased from 7.9 to 11.9 g/dL (ferrous sulfate group) vs 7.7 to 11.1 g/dL (iron complex group). Median serum ferritin level increased from 3.0 to 15.6 ng/mL (ferrous sulfate) vs 2.0 to 7.5 ng/mL (iron complex) . Mean total iron-binding capacity decreased from 501 to 389μg/dL (ferrous sulfate) vs 506 to 417μg/dL (iron complex).
Conclusions:Among infants and children aged 9 to 48 months with nutritional iron-deficiency anemia, ferrous sulfate compared with iron polysaccharide complex resulted in a greater increase in hemoglobin concentration at 12 weeks. Once daily, low-dose ferrous sulfate should be considered for children with nutritional iron-deficiency anemia.
3. When to start fruit Juices in infants and children?: Current AAP Recommendations.
heyman MB, Abrams sA, sECTION ON GAsTROENTEROLOGY, hEPATOLOGY, AND NUTRITION, COMMITTEE ON NUTRITION, Pediatrics. 2017
Updated guidelines from the American Academy of Pediatrics (AAP) recommend avoiding fruit juice for infants younger than 12 months. Previous guidelines recommended
dr. Gireesh s.Associate Professor
Dept. of PediatricsGovt. Medical College, Kozhikode
1. How screen time is relatedto adiposity and insulin resistance in children?
Claire M Nightingale, Alicja R Rudnicka1, Angela s Donin, Naveed sattar, Derek G Cook, Peter h Whincup, Christopher G Owen. http://dx.doi.org/10.1136/archdischild-2016-312016.
What they did:A survey was conducted in 4495 children aged 9–10 years who had fasting cardiometabolic risk marker assessments, anthropometry measurements and reported daily screen time.
What they found: Compared with an hour or less screen time daily, those reporting screen time over 3 hours per day had higher ponderal index,skinfold thickness, fat mass index, leptin and insulin resistance.Associations with glucose, hbA1c, physical activity and cardiovascular risk markers were weak or absent. Associations with insulin resistance remained after adjustment for adiposity, socioeconomic markers and physical activity.
Conclusions: strong graded associations between screen time, adiposity and insulin resistance suggest that reducing screen time could facilitate early T2D prevention.
2. How effective is the low-dose ferrous sulfate compared to iron polysaccharide complex on raising hemoglobin concentration in young children with nutritional iron-deficiency anemia?
Powers JM, Buchanan GR, Adix L, Zhang s, Gao A, McCavit TL, JAMA. 2017;317(22):2297.
What they did:This was a double-blind randomized clinical trial of infants and children aged 9 to 48 months with nutritional IDA (assessed by history and laboratory criteria) that
J O U R N A L S N I P P E T S

24 Pediatric Companion
avoiding fruit juice for infants younger than 6 months and now suggest mashed or puréed whole fruit rather than fruit juice for infants age 6 to 12 months.
4. W h a t i s t h e r o l e o f s t e r o i d s (dexamethasone- DXM) in decreasing the time to recovery in patients with parapneumonic pleural effusion?
Alfredo Tagarro, PhD, MD, Enrique Otheo, MD, Fernando Baquero-Artigao, MD, María-Luisa Navarro, PhD et al. on behalf of the CORTEEC study Group
Journal of pediatrics June 2017 Volume 185, Pages 117–123.e6
What they did:This was a multicenter, randomized,doubleblind, parallel-group, placebo-controlled clinical trialof 60 children, ranging in age from 1 month to 14 years, with community-acquired pneumonia (CAP) and pleuraleffusion. Patients received either intravenous dexamethasone (0.25 mg/kg/dose) or placebo every 6 hours over a period of 48 hours, along with antibiotics. The primary endpoint was the time to recovery in hours, defined objectively.
What they found: Compared with placebo recipients, the patients receiving dexamethasone had a shorter time to recovery. The median time torecovery for patients receiving DXM was 68 hours (2.8 days) shorter than patients receiving placebo (109 hoursvs 177 hours; P = .037). The median time to recovery for patients with complicated effusion receiving DXM was 14 hours (0.5days) shorter than for patients with complicated effusion receiving placebo. There were no significantdifferences in complications or adverse events attributable to the study drugs, except for hyperglycemia.
Conclusion: In this trial, DXM seemed to be a safe and effective adjunctive therapy for parapneumonic pleuraleffusion.
5. Which drug to be used for closing preterm PDA? - Comparative study of the efficacy and safety of paracetamol, ibuprofen, and indomethacin in closure of patent ductus arteriosus in preterm neonates.
El-Mashad AER, El-Mahdy h, El Amrousy DE, Elgendy M.
Eur J Pediatr. 2017; 176( 2): 233– 240; doi: 10.1007/s00431-016-2830-7
What they did:300 preterm neonates with hemodynamically significant PDA (hs-PDA) were randomizedinto three groups. Group I (paracetamol group) received 15 mg/kg/6 h IV paracetamol infusion for 3 days. Group II(ibuprofen group) received 10 mg/kg IV ibuprofen infusionfollowed by 5 mg/kg/day for 2 days. Group III (indomethacingroup) received 0.2 mg/kg/12 h indomethacin IV infusion forthree doses. Laboratory investigations such as renal functiontest, liver function test, complete blood count, blood gases and echo were done before and 3 days aftertreatment.
What they found:There was no significant difference between all groups regarding efficacy of PDA closure (P = 0.868). There was a significant increase in serum creatinine levelsand serum blood urea nitrogen in the ibuprofen and indomethacin groups (P < 0.001). There was a significantreduction in platelet count and urine output in bothibuprofen and indomethacin groups (P < 0.001). There wasa significant increase in bilirubin levels in only the ibuprofen group (P = 0.003). No significant difference of haemoglobinlevel or liver enzymes in all groups (P > 0.05).
Conclusion : Paracetamol is as effective as indomethacin and ibuprofen in closure of PDA in preterm neonates andhas less side effects on renal function, platelet count,and GIT bleeding.

25 October 2017
dr. Purushothaman Prof & HOD, Pediatrics
Govt. Medical College, Trichur
Bit old stories in pediatric Malignancies Eighties
Outcome of pediatric malignancies improved a lot with the recent advances in this area Newer treatment modalities in the diagnosis prognostication treatment, both definitive and, supportive.
In eighties when we were PGs in calicut medical college we were able to get “event free survivals” in acute lymphatic leukemia and few of solid tumors like wilmstumor and neuroblastoma . Number of cases getting cure was very few . Many of the drugs for chemotherapy were either not available or too costly .In resource poor settings we were trying to overcome the shortage of these drugs by doing the chemotherapy in single session for same type of cases. Vials of drugs once opened and used during one session were stored for days and used in another session .
Most of the sessions two type of administration procedures also were done in same sitting ie Intrathecal administrat ion of drugs and Chemotherapy given through peripheral IV line were done in same sitting, for multiple patients. Most of these sessions were during the maintenance phase of Acute lymphatic leukemia (a patient getting intrathecal triple drugs and Intravenous vincristine)
Thinking back there are chances of grave mistakes likely to happen during these sessions. Most of us learn from mistakes , which happened in our life/ bit of imagination.
.Usual practice of conducting one of these session is like this .Calculated dosages of drugs prepared under sterile preparations and kept in tray. Usually all drugs meant for a patient is prepared for administration and kept in same trey Both his Lumbar puncture and intravenous administration of drugs finished before starting next patient . Lumbar puncture is done and the drugs introduced one by one intrathecally (iemethotrexate,hydrocortisone and cytosine arabinoside.) After finishing this injection vincristine is given Intravenously . One major mistake likely to happen here is injection of vincristine intrathecally . If vincristine is introduced into CsF whole spinal cord will get damaged irreversibly
so better do these two procedures separately . Never keep injection vincristine in same trey used for keeping prepared dose of intrathecal drugs.
2. Drugs used for one session better not to store for another session especially if it is for intrathecal
use. There is possibility of bacterial contamination and may lead to bacterial meningitis by dreaded organism entering directly to CsF.
Both the above scenarios are relevant now as most of us learned enough from similar mistakes .
Experience in NinetiesNot much was known about the atypical
presentation of acute leukemias in early nineties. A five year old boy was put on antituberculous drugs by pediatrician because child had contact with sputum positive pulmonary tuberculosis ,EsR was 120 but mantoux test was negative and X Ray was normal. he was referred to us as the fever did not subside and he started complaining of joint pains both hips and knee .he was pale ,few small cervical lymph nodes .Peripheral smear was normal , all the investigations for prolonged fever negative during his two weeks hospital stay . Working diagnosis of systemic onset juvenile rheumatoid arthritis was made and patient was put on steroids , he became afebrile, joint pain subsided he was sent home with a date to review. he came back after three months with severe pallor, generalised lymphadenopathy hepatosplenomegaly Peripheral smear full of blast, Lymphoblast. Bone marrow confirmed Acute lymphoblastic leukemia
he could not achieve remission with chemotherapy and succumbed during induction .
After that we were more aware of this type of presentation with joint involvement.
recently in 2014 A 7 year old girl presented with irregular fever
,hip pain of three weeks duration . On examination left supraclavicular lymph node were enlarged 2X2 cms. No hepatosplenomegaly . her peripheral smear was reported normal . UsG reported central caseous area and suggestive of tuberculosis .Mantoux test was negative . UsG abdomen showed an adrenal mass.
Urine vMA was normalLymph node biopsy and bone marrow showed
neuroblastoma .stage IV .Lesson learned .don’t depend too much on
VMA .It can be normal even with advance stage of neuroblastoma.

26 Pediatric Companion
Loop DiureticsLoop diuretics are the most potent of the
available diuretics (1). These agents work by blocking the Na+ -K+ -2Cl- transporter in the ascending loop of henle, inhibiting reabsorption of these ions. Because reabsorption of approximately 25% of the filtered sodium occurs in this tubular segment, use of loop diuretics results in significant diuresis (2). Potassium reabsorption in the ascending limb also is reduced, resulting in increased loss of potassium. With increased presentation of sodium to the distal tubule, secretion of potassium is enhanced thus contributing to the potassium loss. Because magnesium and calcium reabsorption in the thick ascending limb is dependent on the positive lumen voltage gradient set up by potassium recycling through renal outer medullary potassium channel, loop diuretics also inhibit their reabsorption. By disrupting the reabsorption of these ions, loop diuretics prevent the generation of a hypertonic renal medulla(2,3,4,5). Currently available loop diuretics include furosemide, bumetanide, and torsemide. Both furosemide and bumetanide have been studied in children. Unlike bumetanide, furosemide inhibits not only the Na+ -K+ -2Cl- pump but other ion channels as well. Thus, bumetanide seems to be a more specific inhibitor of the Na+ -K+ -2Cl- transporter. In vitro comparisons of furosemide and bumetanide have shown bumetanide to be 15 to 100 fold as potent as furosemide (6). The pharmacokinetics of furosemide and bumetanidehave been studied in children. In neonates, volume of distribution and half-life are significantly greater than in adults. In preterm infants the half-life of furosemide ranges from 24 to 46 hours, whereas in term neonates the half-life is generally less than 12 hours. As renal and hepatic functions mature, clearance increases and elimination halflife is shortened (4). In critically ill infants and children, the half-life of bumetanide is approximately two hours and one hour respectively (7,8). Furosemide is the most extensively used and studied diuretic in the pediatric population (5). Due to the continual
maturation of the kidney and the changes in fluid distribution in the pediatric population, it is especially important to monitor electrolytes during therapy. Following extended use of furosemide, hyponatremia, hypokalemia, and volume contraction may occur. Enhanced urinary calcium loss resulting from chronic furosemide use in neonates can cause nephrocalcinosis. Concurrent use of chlorothiazide has reportedly decreased hypercalciuria and dissolved some of the calculi (9). Furosemide is highly protein bound and may displace bilirubin from albumin, although a causal relationship between furosemide-induced bilirubin displacement and the development of kernicterus has not been shown (4). Premature infants appear to be at increased risk for development of furosemideinduced ototoxicity from the accumulation of furosemide due to its longer t1/2 in these babies. Beermann and associates found that high plasma levels of furosemide (above 50 mcg/ml) are associated with a higher incidence of auditory disturbances (10). Rupp calculated that injection of furosemide at a rate slower than 4 mg/min would not produce serum concentrations greater than 40 mcg/ml (11). This was substantiated by blood level measurements in patients with renal disease and no hearing loss was reported. Ototoxicity due to furosemide may be avoided by several methods. Continuous slow infusion of IV furosemide has been found to be a more effective method of drug administration to elicit a diuretic response in patients with ChF and avoids high peaks associated with ototoxicity. Divided oral doses are recommended as well as keeping blood levels < 50 mcg/ml to reduce the risk of ototoxicity (9). In both clinical trials and animal studies, bumetanide appears to be less ototoxic than furosemide (6). In patients
dr. Jeeson C. UnniEditor-in-chief, IAP Drug Formulary Associate Consultant in Paediatrics
Aster Medcity, Kochi
27 October 2017
.1) Honeycombingonbilaterallungfields
suggestive of Bronchiaectasis Cysticfibrosis
2) Pneumatocoeleinthelungfield Staphaylococcus aureus; antista-phylococcal antibiotics like cloxacillin
3. Molar tooth sign - Jouberts syndrome
4. Tooth - Cleidocranial dysplasia
5. Holoprosencephaly - Trisomy 13 (Patatu syndrome)
6. Multiple exostosis - Autosomal dominant
7. Popcorncalcification- Osteogenesis imperfecta
8. Punctuatecalcificationattheendofling bones (humerus) - Rhizomelic chondrodysplasia punctata (RCDP)
9. Dense bone – marble bone disease - osteopetrosis
PHoto QUiZ - ANsWErs (pAge 21)
receiving other ototoxic drugs, bumetanide may be a safer alternative (4). Bumetanide and furosemide have significant structural and pharmacodynamic similarities. Although direct comparison of the agents with respect to the incidence, prevalence, and clinical significance of adverse effects in children have not been done, bumetanide therapy appears to offer only marginal theoretic advantages when compared with furosemide (4). Bumetanide reaches the site of action by passive diffusion due to its high lipid solubility and therefore is much less dependent than furosemide on tubular secretion for reaching its site of action (5,12). When the dose response to bumetanide and furosemide are compared in terms of natriuresis and kaliuresis, the relative potency of bumetanide in promoting potassium excretion was significantly lower than its relative natriuretic response. The potential for decreased hypokalemia may be a potential advantage to bumetanide (5). At plasma concentrations above those achieved during routine therapeutic use, the binding of bumetanide to neonatal plasma proteins is approximately 97%. hence, saturation of albumin-binding sites is unlikely at therapeutic doses (4). In neonates, loop diuretics may be used with indomethacin to prevent NsAIDinduced nephrotoxicity during therapeutic closure of a patent ductusarteriosus (5,12,13). however, these agents stimulate renal synthesis of prostaglandin E and may interfere with closure of the PDA when given to premature infants. Adverse effects associated with loop diuretics include gastric irritation, diarrhea, weakness, fatigue, dizziness, muscle cramps, photosensitivity, anemia, leukopenia, thrombocytopenia, hyperglycemia, agranulocytosis, and various cutaneous eruptions (4,13).
references1. Bailie MD. Diuretic treatment agents. Adv. Pediatr 1993;
40:273-285.2. Baliga R, Lewy JE. Pathogenesis and treatment of
edema. PedClin North Am 1987;34(3);693-648.3. Rose BD. Diuretics.. Kidney International. 1991;39 (2):
336–52.4. Wells TG. The pharmacology and therapeutics of
diuretics in the pediatric patient. PedClin North Am
1990;37(2):463-504.5. Witte MK, stork JE, Blumer JL. Diuretic therapeutics in
the pediatric patient. Am J Card 1986;57:44a-53a.6. Rybak LP. Pathophysiology of furosemide ototoxicity.
J Otolaryngol 1982;11(2):127-133.7. sullivan JE, Yamashita Ts, Wells TG, et al. Pharma-
cokinetics and pharmacodynamics of bumetanide in critically ill children. ClinPharmacolTher 1995;57(2):180.
8. sullivan JE, Witte MK, Yamashita Ts, et al. Effects of age and disease on pharmacokinetics and pharmaco-dynamics of bumetanide in critically ill infants. Clin-PharmacolTher 1995;57(2):180.
9. Feig PU. Cellular mechanism of action of loop diuretics: Implications for drug effectiveness and adverse effects. Am J Cardiol 1986:57:14a-19a.
10. Beermann B, Dalen E, Lindstrom B. Elimination of furosemide in healthy subjects and in those with renal failure. ClinPharmacolTher 1977;22:70-8.
11. Rupp W. Pharmacokinetics and pharmacodynamics of lasix. scot Med J 1984;19(suppl):5-13.
12. Chemtob s, Kaplan Bs, sherbotie JR, et al. Pharmacol-ogy of diuretics in the newborn. PedClin North Am 1989;36(5):1231- 1250.
13. Olin BR ed. Diuretics. In:Drug Facts and Com-parisons. st . Louis: Facts and Comparisons, Inc.,1995:135a-138j.

28 Pediatric Companion
Food allergy - an Overview
Adverse reactions to foods can be true (immunologically mediated) food allergy or non-immunological adverse reactions to foods like food poisoning, food intolerance. A food allergy is an adverse health effect arising from a specific immune response that occurs reproducibly on exposure to a given food. Though food allergy has been noted in the urbanized western world for sometime, now a days it is becoming common all round the world. On the basis of recent studies, food allergy is estimated to affect more than 1% to 2% and less than 10% of the population.1 Although more than 170 foods have been identified as triggers of food allergy, those causing most of the significant allergic reactions include milk, egg, peanut, tree nuts, fish, shellfish, wheat, soy, and seeds.2,3
PathogenesisFood allergies are basically due to immune
responses to food proteins. It is predominantly caused by IgE-mediated and/or cell mediated mechanisms. On exposure to certain allergens, in susceptible individuals,food-specific IgE antibodies are formed that bind to receptors on mast cells, basophils, macrophages, and dendritic cells. When food allergens penetrate mucosal barriers and reach cell-bound IgE antibodies, mediators are released which produces symptoms of immediate hypersensitivity . These activated mast cells and macrophages may release several cytokines that attract and activate other cells, such as eosinophils and lymphocytes, leading to prolonged inflammation.
symptomsVariety of clinical signs and symptoms can
occur in food allergy. Reactions can occur in minutes to hours. IgE mediated food allergies can affect a variety of target organs: the skin, manifested as urticaria and/or angioedema4; the gastrointestinal tract, causing vomiting,
abdominal pain, and/or diarrhea; the respiratory tract, as wheezing and/or allergic rhinitis; and the cardiovascular system resulting in hypotension and/or cardiac arrythmias. An immediate, systemic IgE-mediated reaction is anaphylaxis and can develop into a potentially fatal allergic reaction.
Pollen-food allergy syndrome(oral allergy syndrome) is a form of localized IgE-mediated allergy, usually to raw fruits or vegetables, and confined to the lips, mouth, and throat.6 OAS most commonly affects patients who are allergic to specific pollens . Symptoms include pruritus and/or tingling of the lips, tongue, roof of the mouth, and throat with or without swelling. systemic clinical reactions are rare.
Food-dependent, exercise-induced anaphy-laxis should be considered when ingestion of causal food or foods and temporally related exercise result in symptoms of anaphylaxis. symptoms only occur with ingestion of the causal food or foods proximate to exercise and that ingestion of the food in the absence of exercise will not result in anaphylaxis.
With non-IgE mediated (or T-cell mediated) food allergies, patients can have reactions to food, such as atopic dermatitis flare-ups or severe vomiting and diarrhea progressing to shock on ingestion/exposure to the offending food.
diagnosis:A thorough history and physical examination
is the most important part in the assessment . The history is especially important in evaluating acute systemic, or anaphylactic, reactions.
dr. Krishna Mohan r. Consultant Pediatrician
Govt Health Services Kozhikode

29 October 2017
The following facts should be established:
• Food suspected of causing the reaction and the quantity ingested
• Interval between ingestion and the development of symptoms
• Types of symptoms
• Whether other inciting factors, such as exercise, are necessary
• Interval from the last reaction to the food.
A diet diary can be helpful in identifying a specific food as the causative agent.
Allergy skin prick tests and In Vitro laboratory tests are useful for demonstrating IgE sensitization.some fruits and vegetables may require prick-prick skin testing with fresh produce because labile proteins are destroyed during commercial preparation. A negative skin test result virtually excludes an IgE mediated form of food allergy5. Conversely, the majority of children with positive skin test responses to a food do not react when the food is ingested. so more definitive tests, such as quantitative IgE tests or food elimination and challenge, are often necessary to establish a diagnosis of food allergy.
In vitro serum IgE testing quantifies the amount of IgE to the food-specific protein via an enzymatic assay. Component-resolved diagnosis (CRD) identifies the patient’s sIgE reactivity to recombinant allergenic proteins rather than whole allergen. CRD is not routinely recommended for the diagnosis of food allergy, but CRD might be useful in certain clinical scenarios.7
The gold standard of food allergy testing is the double-blind, placebo controlled challenge. This should only be performed in a monitored setting where a severe reaction can be immediately treated. The patient is given increasing doses of the suspected food at intervals during constant observation. Once the top dose is reached the patient is observed for period of time, anywhere from 2.5 to 4 hours for allergic symptoms.
treatmentThe only proven therapy for food allergy
is strict elimination of the offending food. But complete elimination of common foods (milk, egg, soy, wheat, rice, chicken, fish, peanut, nuts) is very difficult because of their widespread use in a variety of processed foods. This requires extensive education and work on the part of the parents and any other caregiver, including babysitters, grandparents, etc, and includes reading all food labels as well as taking special care when ordering food in restaurants, notifying schools regarding snacks/ meals, etc. Parents of younger children with food allergies should be trained to identify early allergic symptoms and should have antihistamines and epinephrine available at all times.
Allergen specific therapies like oral, sublingual and epicutaneous immunotherapy and allergen non-specific therapies like Chinese herbal formula FAhF-2 and omalizumab are tried but more data on efficacy and safety are needed before these therapies become mainstream.
Natural course of food allergyKnowledge about the natural history of food
allergy is important in treatment to guide use of elimination diets and when it may be appropriate to consider re- introducing the diet to include a food that previously caused allergic symptoms. Most children “outgrow” milk and egg allergies, but 80-90% of children with peanut, nut, or seafood allergy retains their allergy for life.
Prevention of food allergy: Facts:• Exclusive breast feeding for 4-6 months is
beneficial.
• Introduction of complementary foods after the age of 4-6 months according to normal standard weaning practices and nutrition recommendations, for all children irrespective of atopic heredity. No need to avoid or delay8.
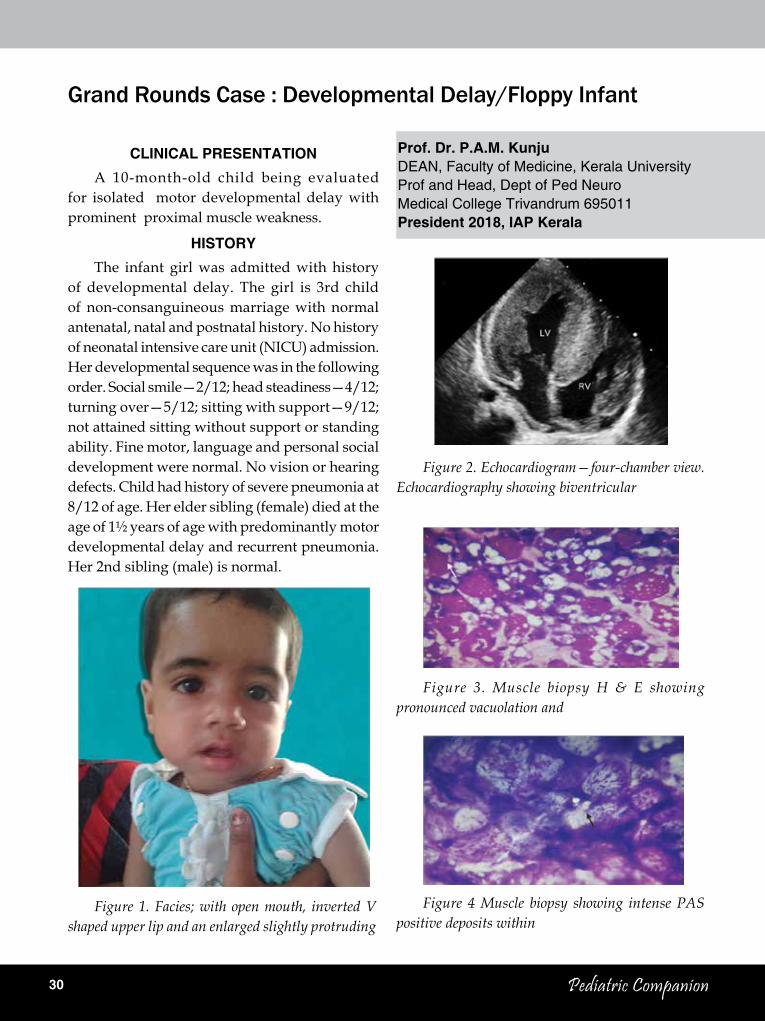
30 Pediatric Companion
Grand Rounds Case : Developmental Delay/Floppy Infant
CliNiCAl PrEsENtAtioNA 10-month-old child being evaluated
for isolated motor developmental delay with prominent proximal muscle weakness.
HistoryThe infant girl was admitted with history
of developmental delay. The girl is 3rd child of non-consanguineous marriage with normal antenatal, natal and postnatal history. No history of neonatal intensive care unit (NICU) admission. her developmental sequence was in the following order. social smile—2/12; head steadiness—4/12; turning over—5/12; sitting with support—9/12; not attained sitting without support or standing ability. Fine motor, language and personal social development were normal. No vision or hearing defects. Child had history of severe pneumonia at 8/12 of age. her elder sibling (female) died at the age of 1½ years of age with predominantly motor developmental delay and recurrent pneumonia. her 2nd sibling (male) is normal.
Prof. dr. P.A.M. KunjuDEAN, Faculty of Medicine, Kerala UniversityProf and Head, Dept of Ped NeuroMedical College Trivandrum 695011President 2018, iAP Kerala
Figure 1. Facies; with open mouth, inverted V shaped upper lip and an enlarged slightly protruding
Figure 2. Echocardiogram—four-chamber view. Echocardiography showing biventricular
Figure 3. Muscle biopsy H & E showing pronounced vacuolation and
Figure 4 Muscle biopsy showing intense PAS positive deposits within
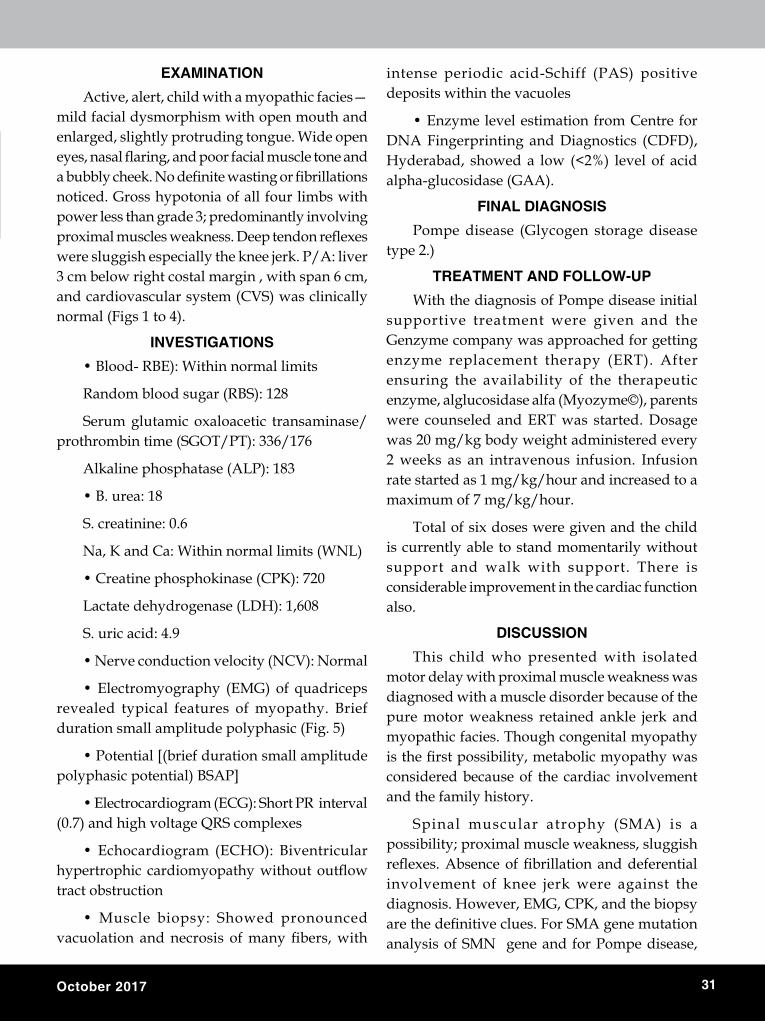
31 October 2017
EXAMiNAtioNActive, alert, child with a myopathic facies—
mild facial dysmorphism with open mouth and enlarged, slightly protruding tongue. Wide open eyes, nasal flaring, and poor facial muscle tone and a bubbly cheek. No definite wasting or fibrillations noticed. Gross hypotonia of all four limbs with power less than grade 3; predominantly involving proximal muscles weakness. Deep tendon reflexes were sluggish especially the knee jerk. P/A: liver 3 cm below right costal margin , with span 6 cm, and cardiovascular system (CVs) was clinically normal (Figs 1 to 4).
iNvEstiGAtioNs• Blood- RBE): Within normal limits
Random blood sugar (RBs): 128
serum glutamic oxaloacetic transaminase/prothrombin time (sGOT/PT): 336/176
Alkaline phosphatase (ALP): 183
• B. urea: 18
s. creatinine: 0.6
Na, K and Ca: Within normal limits (WNL)
• Creatine phosphokinase (CPK): 720
Lactate dehydrogenase (LDh): 1,608
s. uric acid: 4.9
• Nerve conduction velocity (NCV): Normal
• Electromyography (EMG) of quadriceps revealed typical features of myopathy. Brief duration small amplitude polyphasic (Fig. 5)
• Potential [(brief duration small amplitude polyphasic potential) BsAP]
• Electrocardiogram (ECG): Short PR interval (0.7) and high voltage QRs complexes
• Echocardiogram (ECHO): Biventricular hypertrophic cardiomyopathy without outflow tract obstruction
• Muscle biopsy: Showed pronounced vacuolation and necrosis of many fibers, with
intense periodic acid-schiff (PAs) positive deposits within the vacuoles
• Enzyme level estimation from Centre for DNA Fingerprinting and Diagnostics (CDFD), hyderabad, showed a low (<2%) level of acid alpha-glucosidase (GAA).
FiNAl diAGNosisPompe disease (Glycogen storage disease
type 2.)
trEAtMENt ANd FolloW-UPWith the diagnosis of Pompe disease initial
supportive treatment were given and the Genzyme company was approached for getting enzyme replacement therapy (ERT). After ensuring the availability of the therapeutic enzyme, alglucosidase alfa (Myozyme©), parents were counseled and ERT was started. Dosage was 20 mg/kg body weight administered every 2 weeks as an intravenous infusion. Infusion rate started as 1 mg/kg/hour and increased to a maximum of 7 mg/kg/hour.
Total of six doses were given and the child is currently able to stand momentarily without support and walk with support. There is considerable improvement in the cardiac function also.
disCUssioNThis child who presented with isolated
motor delay with proximal muscle weakness was diagnosed with a muscle disorder because of the pure motor weakness retained ankle jerk and myopathic facies. Though congenital myopathy is the first possibility, metabolic myopathy was considered because of the cardiac involvement and the family history.
spinal muscular atrophy (sMA) is a possibility; proximal muscle weakness, sluggish reflexes. Absence of fibrillation and deferential involvement of knee jerk were against the diagnosis. however, EMG, CPK, and the biopsy are the definitive clues. For SMA gene mutation analysis of sMN gene and for Pompe disease,
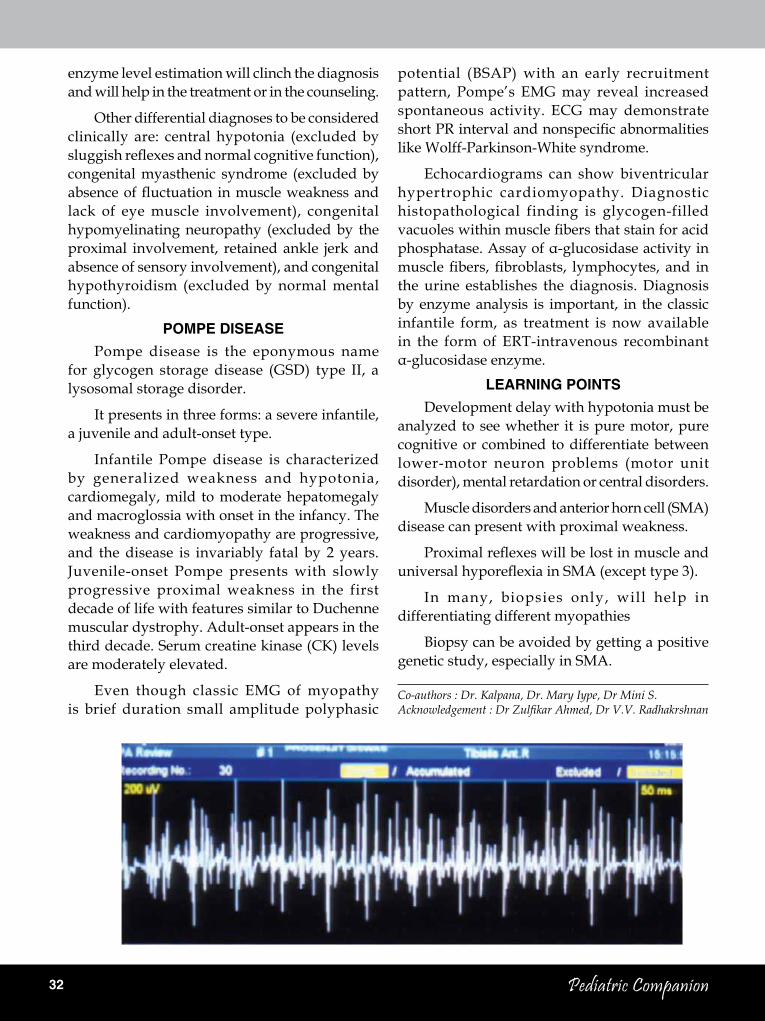
32 Pediatric Companion
enzyme level estimation will clinch the diagnosis and will help in the treatment or in the counseling.
Other differential diagnoses to be considered clinically are: central hypotonia (excluded by sluggish reflexes and normal cognitive function), congenital myasthenic syndrome (excluded by absence of fluctuation in muscle weakness and lack of eye muscle involvement), congenital hypomyelinating neuropathy (excluded by the proximal involvement, retained ankle jerk and absence of sensory involvement), and congenital hypothyroidism (excluded by normal mental function).
PoMPE disEAsEPompe disease is the eponymous name
for glycogen storage disease (GsD) type II, a lysosomal storage disorder.
It presents in three forms: a severe infantile, a juvenile and adult-onset type.
Infantile Pompe disease is characterized by generalized weakness and hypotonia, cardiomegaly, mild to moderate hepatomegaly and macroglossia with onset in the infancy. The weakness and cardiomyopathy are progressive, and the disease is invariably fatal by 2 years. Juvenile-onset Pompe presents with slowly progressive proximal weakness in the first decade of life with features similar to Duchenne muscular dystrophy. Adult-onset appears in the third decade. serum creatine kinase (CK) levels are moderately elevated.
Even though classic EMG of myopathy is brief duration small amplitude polyphasic
potential (BsAP) with an early recruitment pattern, Pompe’s EMG may reveal increased spontaneous activity. ECG may demonstrate short PR interval and nonspecific abnormalities like Wolff-Parkinson-White syndrome.
Echocardiograms can show biventricular hypertrophic cardiomyopathy. Diagnostic histopathological finding is glycogen-filled vacuoles within muscle fibers that stain for acid phosphatase. Assay of α-glucosidase activity in muscle fibers, fibroblasts, lymphocytes, and in the urine establishes the diagnosis. Diagnosis by enzyme analysis is important, in the classic infantile form, as treatment is now available in the form of ERT-intravenous recombinant α-glucosidase enzyme.
lEArNiNG PoiNtsDevelopment delay with hypotonia must be
analyzed to see whether it is pure motor, pure cognitive or combined to differentiate between lower-motor neuron problems (motor unit disorder), mental retardation or central disorders.
Muscle disorders and anterior horn cell (sMA) disease can present with proximal weakness.
Proximal reflexes will be lost in muscle and universal hyporeflexia in SMA (except type 3).
In many, biopsies only, will help in differentiating different myopathies
Biopsy can be avoided by getting a positive genetic study, especially in sMA.
co-authors : Dr. Kalpana, Dr. Mary Iype, Dr Mini S. Acknowledgement : Dr Zulfikar Ahmed, Dr V.V. Radhakrshnan

33 October 2017
a RaRE CaUSE OF aCUTE DEMYELINaTION IN a CHILD
iNtrodUCtioNNeurological manifestations of infectious
diseases are not rare in children. They can occur as primary CNs infection or complications of the disease. Meningitis and meningoencephalitis are frequently associated with infections .Other manifestations include cerebral hemorrhage, acute disseminated encephalomyelitis, acute cerebellar ataxia, cranial nerve palsy, hearing loss, myoclonus, myelitis, Guillain-Barre syndrome, brachial plexopathy, polyneuropathy etc We report the case of a seven year old girl who presented with acute onset of neurological symptoms suggestive of demyelination.
CAsE rEPortA seven year old girl was admitted to the
pediatric unit, Govt Medical College, Thrissur. she complained of giddiness, vomiting & head ache and diminished vision 3 days prior to admission. Mother had also noticed that the child had an unsteady gait since 2 days. she also had mild fever initially followed by high grade fever in the past two weeks. There was no history of rash, altered sensorium or convulsions. her development was normal for age with uneventful antenatal period and she had no significant medical illness in the past or convulsions. No significant medical illness in the past. On Clinical examination, she was alert,but had bilateral lateral rectus palsy, truncal ataxia and ataxic gait. she also had mild neck stiffness. Fundus examination showed papilledema. Blood counts showed a normocytic normochromic smear with neutrophilic leucocytosis.EsR 86mm/hr. CsF study showed TC-60(80% lymphocytes), sugar 85mg/dl,and protein 40g/dl. Mantoux test negative.MRI brain showed longitudinal demyelinating lesions from C6 extending to conus. A diagnosis of ADEM was considered. she was treated with Inj.Methylprednisolone . serological tests for hepatitis B,dengue, leptospirosis and mycoplasma as well as Widal test were negative. Weil Felix test was positive. IgM antibody assay for scrub typhus showed high titres. she was started on doxycycline and improved clinically.
A seven year old girl was admitted with giddiness and difficulty in walking since two days.she had a low grade fever in the past two weeks .No history of rash, altered sensorium or convulsions. No significant medical illness in the past. On Clinical examination, she was alert,but had bilateral lateral rectus palsy, truncal ataxia and ataxic gait. she also had mild neck stiffness. Fundus examination showed papilledema. Blood counts showed a normocytic normochromic smear with neutrophilic leucocytosis.EsR 86mm/hr. CsF study showed TC-60(80% lymphocytes), sugar 85mg/dl,and protein 40g/dl. Mantoux test negative.MRI brain showed longitudinal demyelinating lesions from C6 extending to conus. A diagnosis of ADEM was considered. she was treated with Inj.Methylprednisolone . serological tests for hepatitis B,dengue, leptospirosis and mycoplasma as well as Widal test were negative. Weil Felix test was positive. IgM antibody assay for scrub typhus showed high titres. she was started on doxycycline and improved clinically.
A seven year old girl was admitted with giddiness and difficulty in walking since two days. she had a low grade fever in the past two weeks. No history of rash, altered sensorium or convulsions. No significant medical illness in the past. On Clinical examination, she was alert, but had bilateral lateral rectus palsy, truncal ataxia and ataxic gait. she also had mild neck stiffness. Fundus examination showed papilledema. Blood counts showed a normocytic normochromic smear with neutrophilic leucocytosis.EsR 86mm/hr. CsF study showed TC-60(80% lymphocytes), sugar 85mg/dl,and protein 40g/dl. Mantoux test negative.MRI brain showed longitudinal demyelinating lesions from C6 extending to conus. A diagnosis of ADEM was considered. she was treated with Inj.Methylprednisolone . serological tests for hepatitis B,dengue,
dr. sheela t.A , dr. Nithya shyam dr. Babu K Joseph, dr. Nisha Narendran
Dept. of Pediatrics Govt. Medical College, Thrissur
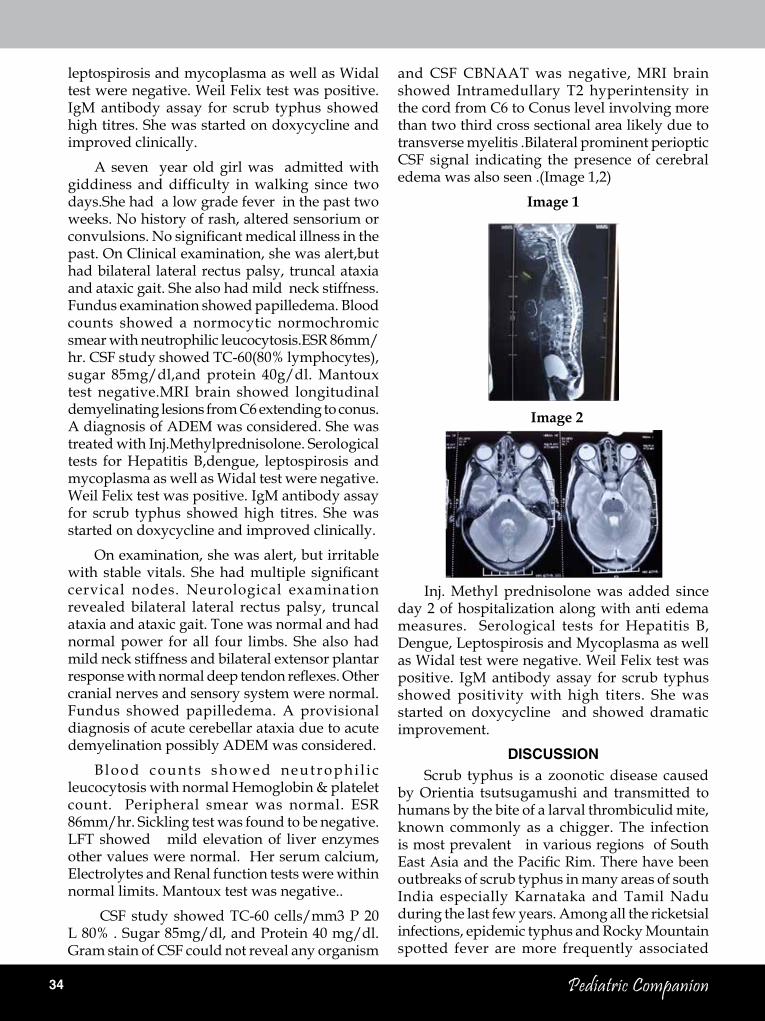
34 Pediatric Companion
leptospirosis and mycoplasma as well as Widal test were negative. Weil Felix test was positive. IgM antibody assay for scrub typhus showed high titres. she was started on doxycycline and improved clinically.
A seven year old girl was admitted with giddiness and difficulty in walking since two days.she had a low grade fever in the past two weeks. No history of rash, altered sensorium or convulsions. No significant medical illness in the past. On Clinical examination, she was alert,but had bilateral lateral rectus palsy, truncal ataxia and ataxic gait. she also had mild neck stiffness. Fundus examination showed papilledema. Blood counts showed a normocytic normochromic smear with neutrophilic leucocytosis.EsR 86mm/hr. CsF study showed TC-60(80% lymphocytes), sugar 85mg/dl,and protein 40g/dl. Mantoux test negative.MRI brain showed longitudinal demyelinating lesions from C6 extending to conus. A diagnosis of ADEM was considered. she was treated with Inj.Methylprednisolone. serological tests for hepatitis B,dengue, leptospirosis and mycoplasma as well as Widal test were negative. Weil Felix test was positive. IgM antibody assay for scrub typhus showed high titres. she was started on doxycycline and improved clinically.
On examination, she was alert, but irritable with stable vitals. She had multiple significant cervical nodes. Neurological examination revealed bilateral lateral rectus palsy, truncal ataxia and ataxic gait. Tone was normal and had normal power for all four limbs. she also had mild neck stiffness and bilateral extensor plantar response with normal deep tendon reflexes. Other cranial nerves and sensory system were normal. Fundus showed papilledema. A provisional diagnosis of acute cerebellar ataxia due to acute demyelination possibly ADEM was considered.
Blood counts showed neutrophi l ic leucocytosis with normal hemoglobin & platelet count. Peripheral smear was normal. EsR 86mm/hr. sickling test was found to be negative. LFT showed mild elevation of liver enzymes other values were normal. her serum calcium, Electrolytes and Renal function tests were within normal limits. Mantoux test was negative..
CsF study showed TC-60 cells/mm3 P 20 L 80% . sugar 85mg/dl, and Protein 40 mg/dl. Gram stain of CsF could not reveal any organism
and CsF CBNAAT was negative, MRI brain showed Intramedullary T2 hyperintensity in the cord from C6 to Conus level involving more than two third cross sectional area likely due to transverse myelitis .Bilateral prominent perioptic CsF signal indicating the presence of cerebral edema was also seen .(Image 1,2)
Image 1
Image 2
Inj. Methyl prednisolone was added since day 2 of hospitalization along with anti edema measures. serological tests for hepatitis B, Dengue, Leptospirosis and Mycoplasma as well as Widal test were negative. Weil Felix test was positive. IgM antibody assay for scrub typhus showed positivity with high titers. she was started on doxycycline and showed dramatic improvement.
disCUssioNscrub typhus is a zoonotic disease caused
by Orientia tsutsugamushi and transmitted to humans by the bite of a larval thrombiculid mite, known commonly as a chigger. The infection is most prevalent in various regions of south East Asia and the Pacific Rim. There have been outbreaks of scrub typhus in many areas of south India especially Karnataka and Tamil Nadu during the last few years. Among all the ricketsial infections, epidemic typhus and Rocky Mountain spotted fever are more frequently associated

35 October 2017
with neurological manifestations followed by scrub typhus. scrub typhus is presently a major public health problem because of the recent increase in case reports from various parts of Kerala. Though CNs involvement in scrub typhus reportedly ranges from aseptic meningitis to frank meningoencephalitis, an acute demyelinating disorder associated with illness is rare.(1)
The pathogen is an obligate intracellular Gram-negative bacterium. Infection involves multiple organs including the lung, heart, and CNs and is characterized by focal vasculitis or perivasculitis.(2) The organism attack endothelial cells by a mechanism of oxidative stress leading to inflammation of release of cytokines which damages the endothelium causing platelet aggregation, fluid leakage and focal microinfarction along with proliferation of polymorphs and monocytes causing local and systemic vasculitis. Myocarditis and encephalitis are the most life-threatening complications associated with the infection. Febrile illness due to scrub typhus presenting with acute cerebellar ataxia is rare.(3)
The main clinical features are high fever, rash, lymphadenopathy, and characteristic eschar formation, present in only 20-30 % and usually goes unnoticed in dark skinned people.(4)
The serological tests such as Micro immunofluorescence, latex agglutination, indirect hemagglutination, immunoperoxidase assay, and enzyme-linked immunosorbent assay (ELIsA) are used for identification , the “gold standard” test being Immunofluorescence assay (IFA). CT/MRI scans are often useful in diagnosing neurological involvements like hemorrhage, ADEM or cerebral edema.
Our patient did not have an eschar, rash .But she lived near a forest area where the chance of exposure to infected chiggers is high. Also, CsF findings showed lymphocytic pleocytosis and mildly elevated protein level. The combination of the cranial MRI and laboratory evidence for scrub typhus led to the conclusion of a demyelinating disease associated with scrub typhus.(5) encephalomyelitis: an update. Arch Neurol 2005;62:1673-
The diagnosis of ADEM is largely that of exclusion. It is made in the setting of a recent
infectious illness and neurological findings supported by MRI and CsF examination.The pathological mechanism is molecular mimicry by antigens simulating various natural neural antigens neither being recognized as foreign to be cleared nor as self to be immune tolerated. They are processed leading to T and B cell activation , enter CNs and recognize homologous myelin proteins and trigger inflammatory response against presumed foreign protein. This is followed by perivenular inflammatory response and subsequent damage to myelin. (6)
First-line treatment for demyelinating conditions is usually high dose glucocorticoids. Prognosis and response to glucocorticoids are generally good, as seen in our patient. Doxycycline is the drug of choice though drug resistance have been reported from some countries. In cases not responding to Doxycycline, Rifampicin and Chloramphenicol are other options. Early diagnosis and treatment with Doxycycline is necessary to prevent life threatening complications in children.
o conclude, acute demyelinating illness is rarely reported due to scrub typhus in the literature. however, serological assay for rickettsial infection is warranted in children with acute demyelination, especially when antimicrobial therapy needs to be initiated to avoid further complications.
rEFErENCEs1. saifudheen, K. et al. “First Case of scrub Typhus with
Meningoencephalitis from Kerala: An Emerging Infec-tious Threat.” Annals of Indian Academy of Neurology 15.2 (2012): 141–144
2. Mahajan sK, Rolain JM, Kanga A, Raoult D. scrub typhus involving central nervous system, India, 2004-2006. Emerg Infect Dis 2010;16:1641-3.
3. Ghosh A, sharma s, Choudhury J. Acute cerebellar ataxia in a 3-year-old Bengali girl: a novel presentation of scrub typhus in pediatric age group. Int J Contemp Pediatr 2017;4:652-4.
4. Viswanathan s, Muthu V, Iqbal N, Remalayam B, George T. scrub typhus meningitis in south India--a retrospective study. PLos One. 2013;8:e66595,
5. Menge T, hemmer B, Nessler s, et al. Acute dis-seminated encephalomyelitis: an update. Arch Neurol 2005;62:1673- 80.
6. TilMenge, Kieseier BC, Nassler s. Acute disseminated encephalomyelitis-An acute hit against the brain. Curr opin Neurol 2007; 20: 247-254

36 Pediatric Companion
C A S E R E P O R T
Failure to Thrive : a Rare Case Report
iNtrodUCtioN
Failure to thrive is a common health and social problem for paediatricians. Diencephalic syndrome is a rare condition associated with central nervous system tumors presenting as failure to thrive with proper caloric intake and no structural impairment. Diencephalic syndrome is a rare cause of failure to thrive in infants and young children. Despite the importance of this syndrome, little is known of its pathophysiology. This syndrome is characterized by profound emaciation, despite a normal or slightly diminished calorie intake. Linear growth is usually maintained.
CAsE rEPort
A 4-year-old girl was brought to our OPD for evaluation of recent loss of weight. she was the only girl child born out of non-consanguinous marriage to a 37-year-old father with neurofibromatosis and a 26-year-old mother with a speech defect and seizure disorder.her birth weight was 2.65 kg with adequate weight gain thereafter with developmental delay predominantly in the fine motor field (Development Quotient –35%) and gross motor and good linguistic skills. she developed recent onset left eye squint with restricted lateral movement over the past one year. The child does not have polyuria, exertional dyspnea, generalized edema or abdominal distension.
On examination child was hyperactive with cachexia, thin triangular face with stable vitals, with left eye esotropia of 300. There were multiple café au lait spots with neurofibromas. Her height was between 10thand 25thcentile and weight
was below 3rd centile. No signs of micronutrient deficiency. Cranial nerve examination revealed with sluggish left eye pupillary reflex and left lateral rectus palsy with bilateral cerebellar signs. Other system examination was normal.
Laboratory tests were performed to evaluate the nutritive status of the patient. Complete blood cell counts, fasting blood sugar levels, and serum total protein/albumin levels were obtained. Thyroid hormone levels were examined to evaluate thyroid function. All test were within normal limits.
Imaging studies were performed. There is isointense lobulated lesion in thalamus, hypothalamus, chiasm and suprasellar region with intense contrast enhancement(Fig 1) . The same lesion is hyperintense in T 2 image partially inverting on T 2 FLAIR sequence. Both optic nerves are thickened. There is a isointense in left orbital cone extending from the left optic nerve. This is consistent with a diagnosis of optic nerve glioma involving the chiasm extending to thalamus, hypothalamus and left optic nerve. There is hyperintensity of right midbrain on T2 and FLAIR with no contrast enhancement in T1 weighted image. There is an area of hyperintensity in right cerebellum. These lesions are consistent with hamartomas involving the left cerebellar hemisphere within the dentate nucleus and right
dr. Elizabeth Preethi thomas dr. Ananda Kesavan t.M.
dr. Anu Marie, dr. deepa Anirudhan dr. K.K. Purushothaman
Govt. Medical College,Thrissur
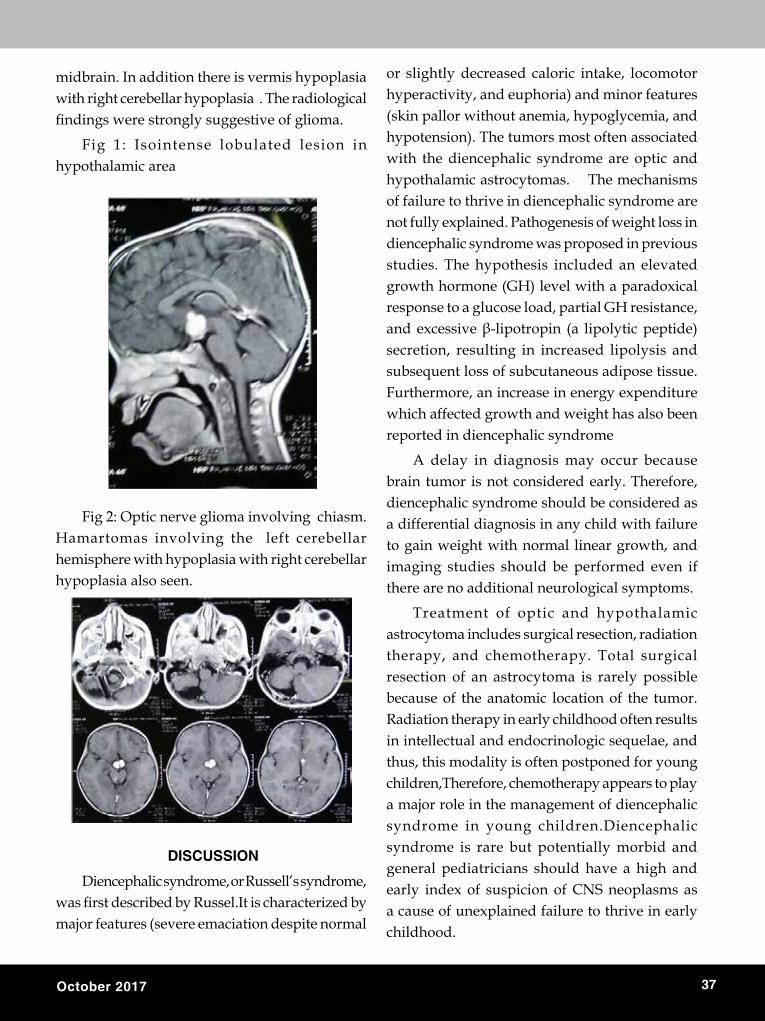
37 October 2017
midbrain. In addition there is vermis hypoplasia with right cerebellar hypoplasia . The radiological findings were strongly suggestive of glioma.
Fig 1: Isointense lobulated lesion in hypothalamic area
Fig 2: Optic nerve glioma involving chiasm. hamartomas involving the left cerebellar hemisphere with hypoplasia with right cerebellar hypoplasia also seen.
disCUssioN
Diencephalic syndrome, or Russell’s syndrome, was first described by Russel.It is characterized by major features (severe emaciation despite normal
or slightly decreased caloric intake, locomotor hyperactivity, and euphoria) and minor features (skin pallor without anemia, hypoglycemia, and hypotension). The tumors most often associated with the diencephalic syndrome are optic and hypothalamic astrocytomas. The mechanisms of failure to thrive in diencephalic syndrome are not fully explained. Pathogenesis of weight loss in diencephalic syndrome was proposed in previous studies. The hypothesis included an elevated growth hormone (Gh) level with a paradoxical response to a glucose load, partial Gh resistance, and excessive β-lipotropin (a lipolytic peptide) secretion, resulting in increased lipolysis and subsequent loss of subcutaneous adipose tissue. Furthermore, an increase in energy expenditure which affected growth and weight has also been reported in diencephalic syndrome
A delay in diagnosis may occur because brain tumor is not considered early. Therefore, diencephalic syndrome should be considered as a differential diagnosis in any child with failure to gain weight with normal linear growth, and imaging studies should be performed even if there are no additional neurological symptoms.
Treatment of optic and hypothalamic astrocytoma includes surgical resection, radiation therapy, and chemotherapy. Total surgical resection of an astrocytoma is rarely possible because of the anatomic location of the tumor. Radiation therapy in early childhood often results in intellectual and endocrinologic sequelae, and thus, this modality is often postponed for young children,Therefore, chemotherapy appears to play a major role in the management of diencephalic syndrome in young children.Diencephalic syndrome is rare but potentially morbid and general pediatricians should have a high and early index of suspicion of CNs neoplasms as a cause of unexplained failure to thrive in early childhood.
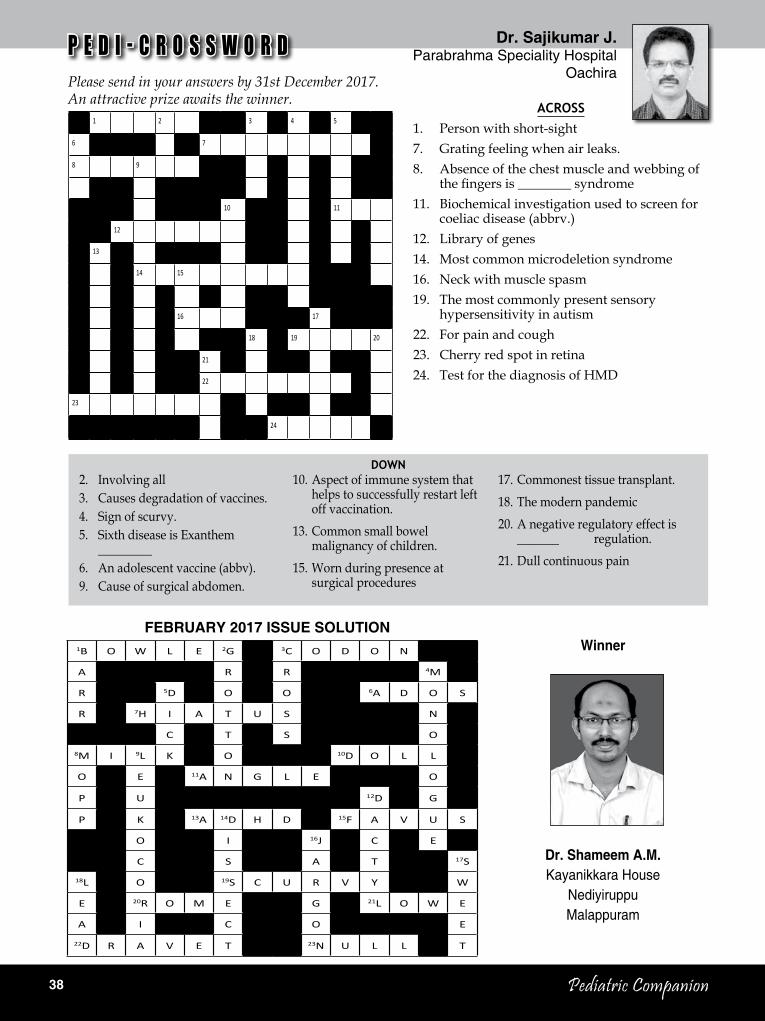
38 Pediatric Companion
dr. sajikumar J.Parabrahma Speciality Hospital
Oachira
2. Involving all3. Causes degradation of vaccines.4. sign of scurvy.5. sixth disease is Exanthem
_________6. An adolescent vaccine (abbv).9. Cause of surgical abdomen.
10. Aspect of immune system that helps to successfully restart left off vaccination.
13. Common small bowel malignancy of children.
15. Worn during presence at surgical procedures
Down
FEBrUAry 2017 issUE solUtioN
17. Commonest tissue transplant.18. The modern pandemic20. A negative regulatory effect is
_______ regulation.21. Dull continuous pain
P E D I - C R O S S W O R DPlease send in your answers by 31st December 2017. An attractive prize awaits the winner.
Across1. Person with short-sight7. Grating feeling when air leaks.8. Absence of the chest muscle and webbing of
the fingers is ________ syndrome11. Biochemical investigation used to screen for
coeliac disease (abbrv.)12. Library of genes14. Most common microdeletion syndrome 16. Neck with muscle spasm19. The most commonly present sensory
hypersensitivity in autism22. For pain and cough23. Cherry red spot in retina24. Test for the diagnosis of hMD
Winner
dr. shameem A.M.Kayanikkara House
NediyiruppuMalappuram
1B O W L E 2G 3C O D O N
A R R 4M
R 5D O O 6A D O S
R 7H I A T U S N
C T S O
8M I 9L K O 10D O L L
O E 11A N G L E O
P U 12D G
P K 13A 14D H D 15F A V U S
O I 16J C E
C S A T 17S
18L O 19S C U R V Y W
E 20R O M E G 21L O W E
A I C O E
22D R A V E T 23N U L L T
1 2 3 4 5
6 7
8 9
10 11
12
13
14 15
16 17
18 19 20
21
22
23
24
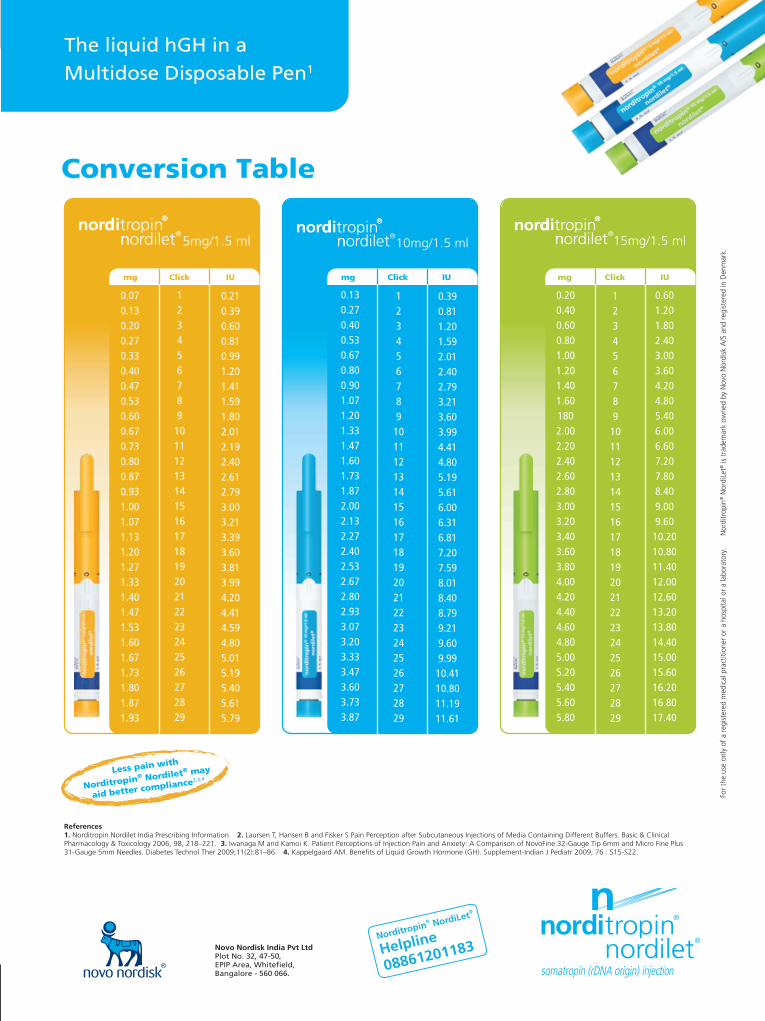
39 October 2017

40 Pediatric Companion
rNi regn. No. KErENG/2006/18758Pediatric Companion october 2017 rs.20.00
Owned, Printed, Published and Edited by Dr. M. Narayanan, ‘Sarovaram’ Mamangalam, Palarivattom P.O., Kochi 682 025, Kerala and printed at Geo Printshop, Kochi for G.K. Printers, Azad Road, Kaloor, Kochi-17, Published at Kochi. Design : Pixel Studio, Cochin-28