Embed Size (px)
Citation preview
Company: Aeon Astron Europe B.V.Date: Apr-15-2013
Management of Glaucoma Surgery: Indian Perspective
OverviewBackground
Glaucoma overviewAre we ready to meet challenge
Surgery Forward – A “Cutting” edge solution?Trabeculectomy and its limitationsNew surgical trend and collagen implantScientific merits
Moving forward
Glaucoma Overview
Glaucoma is the second leading cause of blindness in India(Vijaya et al., 2006)
India est. to host 20% world glaucoma ppl by 2020 (Quigley & Broman, 2006)
Estimated approx. 12 million affected in 2010, and est. to reach 16 million in 2020 (Vijaya et al., 2006)
Are We Ready to Meet Challenge?
Many public & private hospital offer high quality care by well trained residents, BUT
More than 90% glaucoma remain undiagnosed contrary to 50-60% in developed countries (Ramakrishnan & Mona, 2011)
In 2001, est.12,000 ophthalmologists (i.e., 1/100,000 pt) with few glaucoma specialist (George etal., 2010)
Most ophthalmologists (70%) locate in urban cater only 23% ppl (Anderson & Douglas, 2003)
Medicine side lead to decreased QoL, poor compliance, along with life-long cost burden
Surgery Forward – The “Cutting” Edge Solution?
Suggested glaucoma surgery to overcome socio-economic burden with controlled IOP outcome (Ramakrishnan & Mona, 2011)
Ideal surgery isEasily performed by all surgeonsRequiring simple instrumentationMinimal complicationsReplicable technique with short
learning curveEconomic with long term success
outcome
Trabeculectomy – Golden Standard Option
Trabeculectomy remains the “gold standard” surgical option for reduction of IOP after failed maximal tolerated medication
However, episcleral fibrosis and subconjunctival scarring are the major causes of surgical failure
Limitation of MMC
MMC and 5-FU are the most commonly used adjunctive for the inhibition of fibroblast proliferation to prevent scarringChemo toxic and teratogenicBlebs is thinner with more irregular epithelium, breaks
in basement membrane, fewer goblet cells, and atrophic and avascular stroma
Blebitis or endophthalmitis commonly associated with thin, avascular, leaking blebs
Comprises > 90% atelocollagen and< 10% glycosaminoglycans
Highly porous structure with pore sizes ranges between 10~300µm
Good pliable strength to maintain the surgical space
Biocompatible and biodegradable
Ready for use
What is ologen® Collagen Matrix
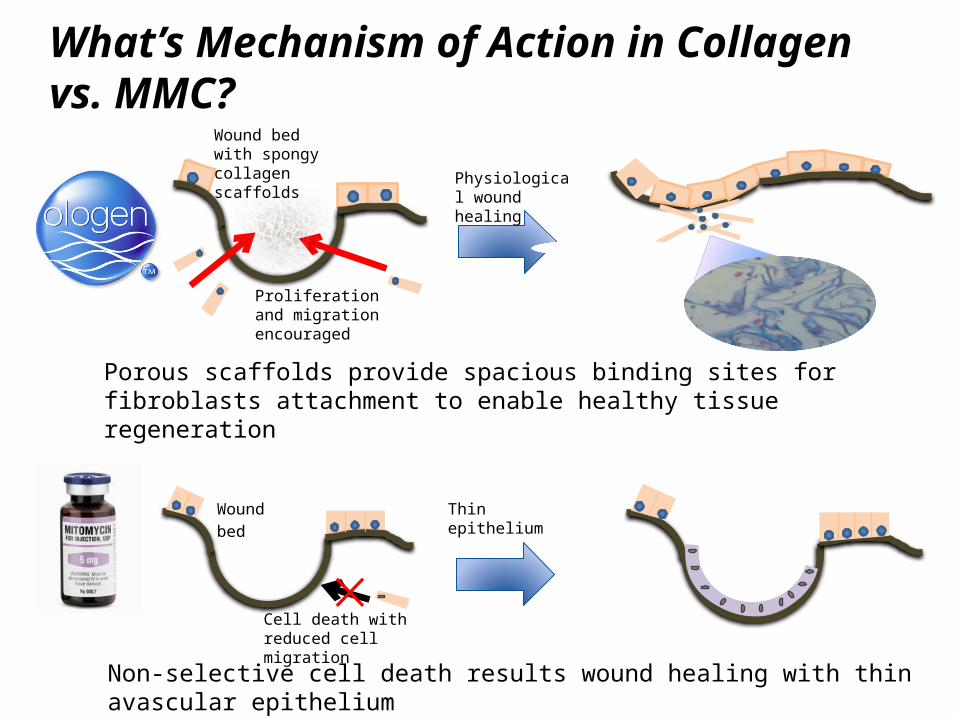
What’s Mechanism of Action in Collagen vs. MMC?
Thin epithelium
Non-selective cell death results wound healing with thin avascular epithelium
Wound
bed
Cell death with reduced cell migration
Wound bed with spongy collagen scaffolds
Proliferation and migration encouraged
Porous scaffolds provide spacious binding sites for fibroblasts attachment to enable healthy tissue regeneration
Physiological wound healing
10
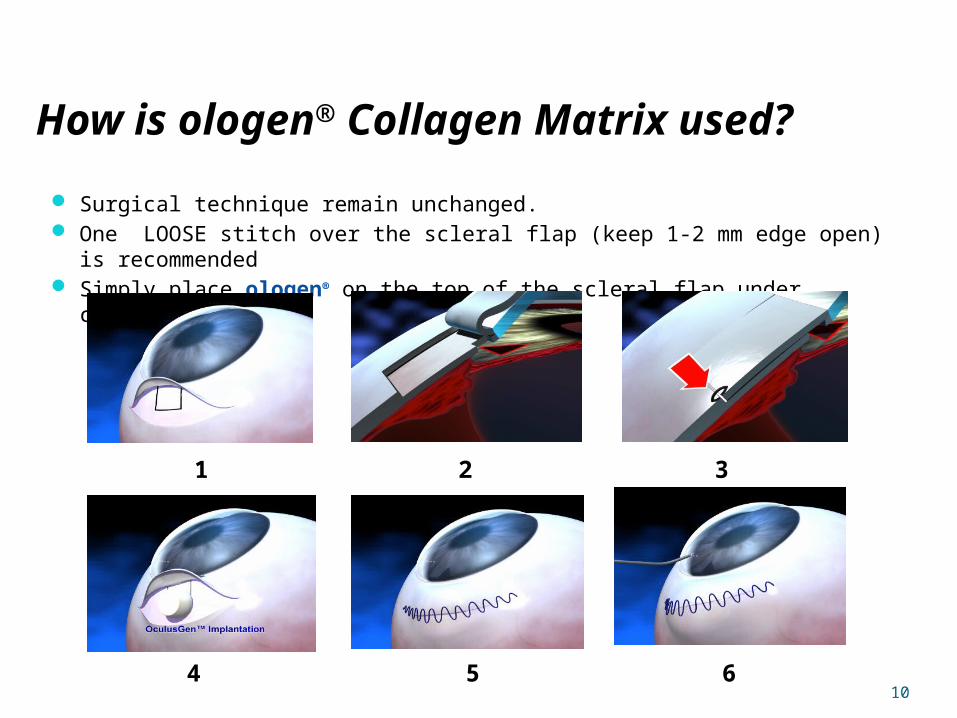
Surgical technique remain unchanged. One LOOSE stitch over the scleral flap (keep 1-2 mm edge open) is recommended Simply place ologen® on the top of the scleral flap under conjunctiva
1 2 3
4 5 6
How is ologen® Collagen Matrix used?
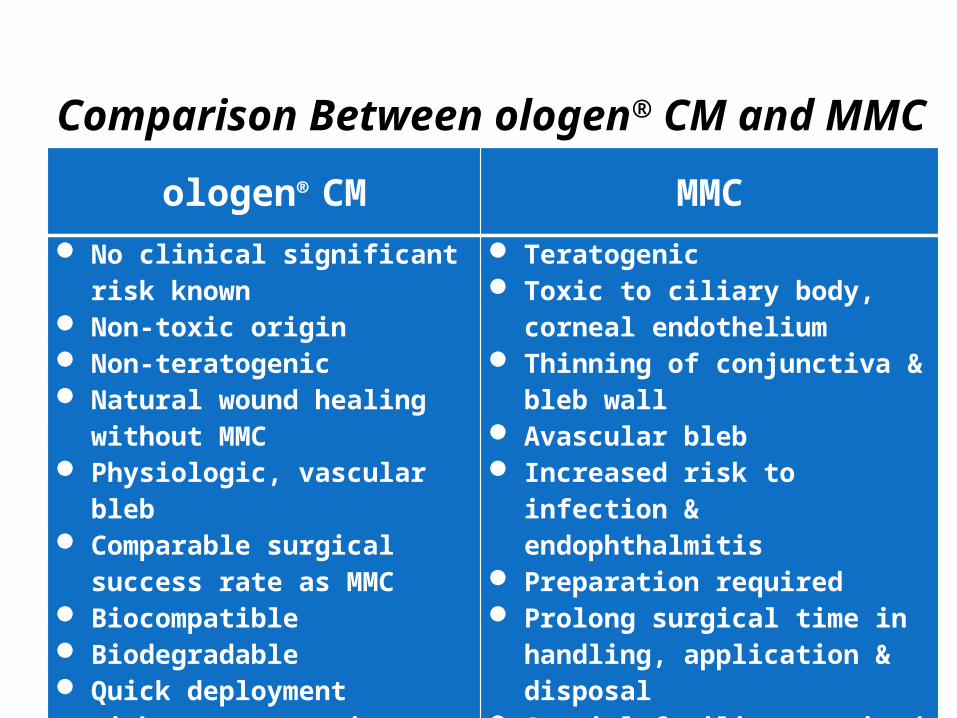
Comparison Between ologen® CM and MMC
ologen® CM MMC
No clinical significant risk known
Non-toxic origin Non-teratogenic Natural wound healing
without MMC Physiologic, vascular bleb Comparable surgical success
rate as MMC Biocompatible Biodegradable Quick deployment without
preparation Save operation time
Teratogenic Toxic to ciliary body, corneal
endothelium Thinning of conjunctiva & bleb
wall Avascular bleb Increased risk to infection &
endophthalmitis Preparation required Prolong surgical time in
handling, application & disposal
Special facility required for handling (Hume hood)
Accreditations & Merits
CE marked, FDA 510k cleared, Canada approved
Over 150 scientific publications in academic conferences & journals
Discussed in 2 textbooksDiagnosis & management of
GlaucomaBasic concepts of glaucoma
Other ongoing studies
Research – 2-year Randomized Controlled Study
Prospective randomized controlled trial Postop. visit at 24±4 hours, 7±1 days, 2 weeks, and 1, 2, 3, 6,
12, 18 and 24 months Outcomes:
IOP target ≤ 21, ≤ 17, ≤ 15 mm Hg (complete or qualified success) Moorfields bleb grading system; SD-OCT (Topcon 3DOCT-1000) Number of glaucoma medications Postoperative adjunctive procedures Complications
Published in Eye Sep-16-2011
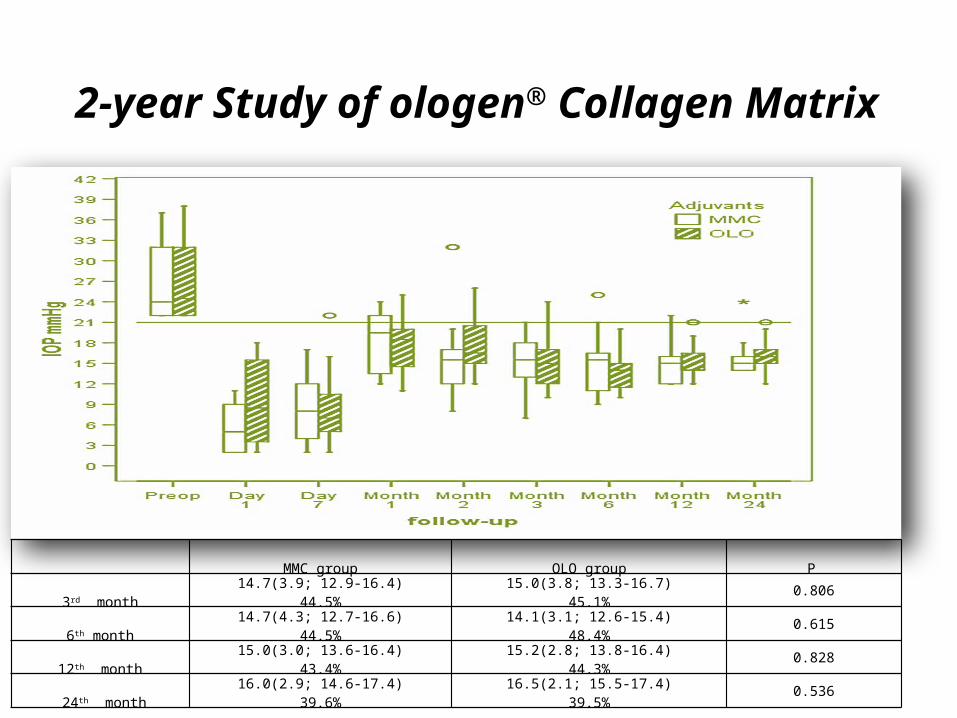
2-year Study of ologen® Collagen Matrix
MMC group OLO group P
3rd month14.7(3.9; 12.9-16.4)
44.5%15.0(3.8; 13.3-16.7)
45.1% 0.806
6th month14.7(4.3; 12.7-16.6)
44.5%14.1(3.1; 12.6-15.4)
48.4% 0.615
12th month15.0(3.0; 13.6-16.4)
43.4%15.2(2.8; 13.8-16.4)
44.3% 0.828
24th month16.0(2.9; 14.6-17.4)
39.6%16.5(2.1; 15.5-17.4)
39.5% 0.536
15
Looking Forwards
Promote glaucoma awarenessImproved early diagnose rateSave patients before vision lossCollect clinical data to study socio-economic burdenWelcome opportunity to allies Vision Foundation
across Taiwan, Japan to initiate glaucoma care program