Embed Size (px)
Citation preview
234 Klimek et al., CAP and AP in pregnancy at neuroendocrinological risk
J. Perinat. Med.4(1976) 234
Comparative prognostic value of serum placental and tissue oxytocinase,alkaline phosphatase and its heat-stable fraction in pregnancy at neuro-endocrinological risk
Rudolf Klimek, Jerzy Stanek
Clinic of Endocrinology, Institute of Gynecology and Obstetrics, Medical Academy,Cracow/Poland
Although enzyme assays, especially those för oxy-tocinases (CAP), heat-stable alkaline phosphatase(HSAP) and histaminase, are now thought to bewell established diagnostic tools in so-called"placental insufficiency", opinions regarding theirusefulness for monitoring high-risk pregnancies arestill divided [11,17,23, 32]. Discrepant evaluationsare probably due to different profiles of pregnantwomen studied and to the fact that only singleenzyme assays and their correlations with resultsof hormonal studies are usually considered and areseldom compared with other enzymes. The purposeof this study was to compaie the prognostic valueof CAP and AP for endocrine monitoring ofpregnancy at neuroendocrinological risk, i.e. preg-nancy in women with neuroendocrinologicaldisturbances diagnosed prior to the pregnancyunder review [24]. We are not aware of any studieson the prognostic value of the aforementionedenzymes in cases of this sort.
Curriculum vitae
Prof. RUDOLF KLIMEK,M.D., was born in Cracow(Poland) in 1932. Degreewith distinction at theCracow Medical Academy.Assistant at the Biochemi-cal Department (Chairman:Prof. B. SKARZYNSKIylin 1954-1956. Since 1957resident in obstetrics andgynecology dt the I Clinicof Obstetrics and Gynecol-ogy in Cracow (Head: Prof.S. SCHWARZ/ AssistantProfessor (l 964) andProfessor of gynecology and o bstetrics(1972). Director of the Institute of Gynecology and Ob-stetrics in 1969-1972. Now Chairman of the Clinic ofEndocrinology of the Institute. He published on high-riskpregnancies, neuroendocrinology andclinicalbiochemistryand described a new entitf - the hypothalämic post-pregnancy syndrome. Member of the International Societyfor Biochemical Pharmacology, International Society ofEndocrinology, European Society for Clinicallnvestigation,American Association for the Advancement of Scienceand domestic societies.
l Case material and methods
The analysis concerns 364 pregnant women whosepregnancies were terminated by delivery and whohad been hospitalized at the Clinic of Endo-crinology of the Institute of Gynecology andObstetrics of the Medical Academy in Cracow inthe years 1971-1973. CAP was determined byTUPPY'S method modified by KLIMEK [19] at
pH = 7.9 (P-CAP) and pH = 6.0 (T.CAP) and APand HSAP by KING and KING'S method modifiedby HANSEN [14]. In these women, prior to thepresent pregnancy, ovarian disorders and/orsterility had been diagnosed äs the cause of failureto become pregnant, and the majority (189women) had been treated with hormones. Someof the women had been treated also during the
J. Perinat. Med. 4(1976)

Klimek et al., CAP and AP in pregnancy at neuroendocrinological risk 235
No.of estimotions35 40 38 41 49 51 66 69 85 108165174 88 29 17
l ι ι ι l l ι ι ι l l l l l T " ~ 1
percentile97.5
medion
percentile2.5
2930 32' 34 36' 38 40' 42 44'weeks of gestotion
Fig. 1. Percentile curves and fetal danger zone of P-CAP.
No.of estimations32 40 39 38 45 49 59 69 80 105160168 85 27 16
median
percentile2.5
'29 30 32' 34 36 3Θ 40 42 44weeks of gestation
No.of estimatJons38 30 32 48 87 158 2628 30 28 39 70 135 82 12ι—ι—ι—ι—ι—ι—\—ι—ι—ι—ι—\—ι—\—ι—i
percentile 97.5
median
percentile 2.5
30 32 34 36 38 40 42 44weeks of gestation
Fig. 3. Percentile curves and fetal danger zone of AP.
No.of estimations28 38 30 30 28 32 39 4870 871351568226 12
percentile 97.5 \
σ>§30
120
10
percentile 97.5median
percentile 25
1930 3Γ 34 3f) 38 40 42 44weeks of gestation
Fig. 2. Percentile curves and fetal danger zone of T-CAP. Fig. 4. Percentile curves and fetal danger zone of HSAP.
present pregnancy because of diabetes (9 women),cervical incompetence (10 women), gestosis (7women), threatened abortion (59 women), feto-maternal immunization (3 women), or toxoplas-mosis (25 women). Results of enzyme assays werecompared at the 95 per cent confidence level,based on 2.5, 50.0 and 97.5 percentiles [15] witha series of 200 healthy pregnant women whodelivered healthy children. Figs. 1—4 show thepercentile curves, smoothed out graphically, from
the calculated percentiles for each of the fourenzyme assays. Absolute values of each enzymeactivity and the curve profiles were evaluatedseparately.
l.Single values: Determinations were consideredabnormal if at least one of the values was belowthe 2.5 percentile (in the fetal danger zone). In364 pregnant women, P-CAP and T-CAP werecalculated, and in 346 AP and HSAP.
J. Perinat. Med. 4 (1976)
236 Klimek et al., CAP and AP in pregnancy at neuroendocrinological risk
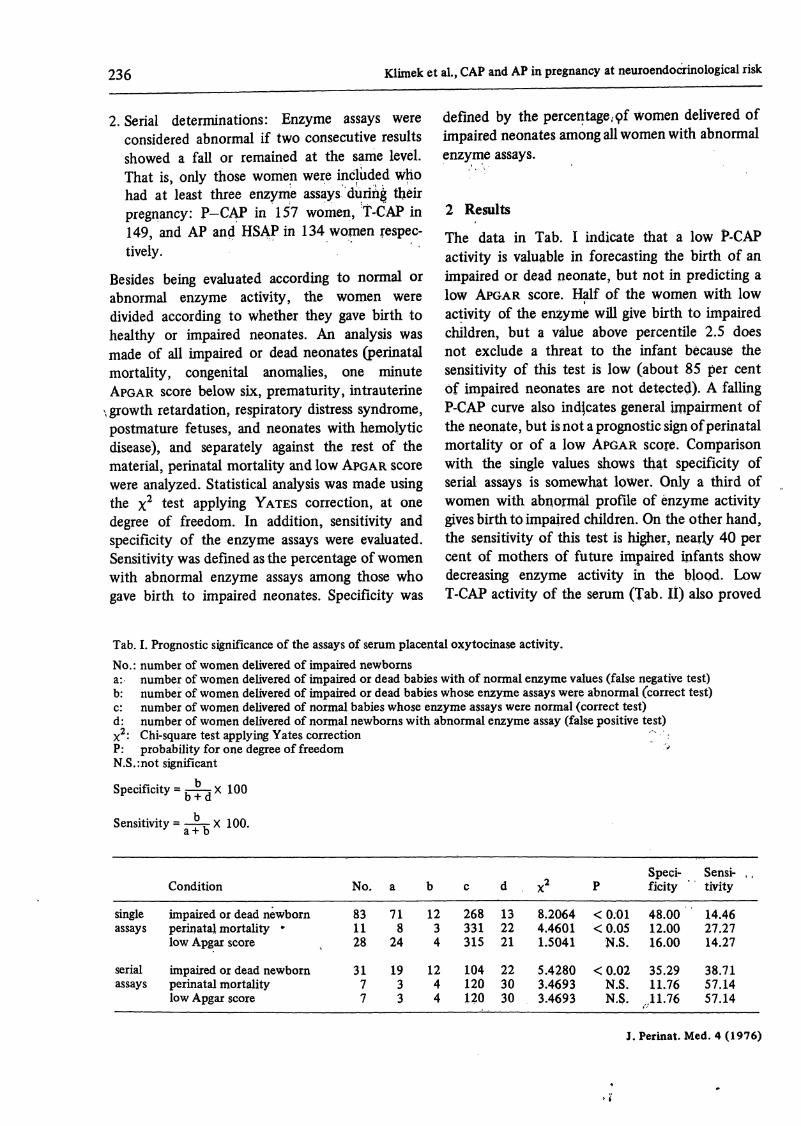
2. Serial determinations: Enzyme assays were defined by the percentage.pf women delivered ofconsidered abnormal if two consecutive results impaired neonates among all women with abnormalshowed a fall or remained at the same level. enzyme assays.That is, only those women were inclüded whohad at least three enzyme assays duririg theirpregnancy: P-CAP in 157 women, T-CAP in 2 Results149, and AP and HSAP in 134 women respec- The data in Tab j indicate that a low p„CAptivety· activity is valuable in forecasting the birth of an
Besides being evaluated according to normal or impaired or dead neonate, but not in predicting aabnormal enzyme activity, the women were low APGAR score. Half of the women with lowdivided according to whether they gave birth to activity of the enzyme will give birth to impairedhealthy or impaired neonates. An analysis was children, but a välue above percentile 2.5 doesmade of all impaired or dead neonates (perinatal not exclude a threat to the infant because themortality, congenital anomalies, one minute sensitivity of this test is low (about 85 per centAPGAR score below six, prematurity, intrauterine of impaired neonates are not detected). A falling
\growth retardation, respiratory distress syndrome, P-CAP curve also indjcates general impairment ofpostmature fetuses, and neonates with hemolytic the neonate, but is not a prognostic sign of perinataldisease), and separately against the rest of the mortality or of a low APGAR score. Comparisonmaterial, perinatal mortality and low APGAR score with the single values shows that specificity ofwere analyzed. Statistical analysis was made using serial assays is somewhat löWer. Only a third ofthe 2 test applying YATES correction, at one women with abnormal profile of enzyme activitydegree of freedom. In addition, sensitivity and gives birth to impaired children. On the otherhand,specificity of the enzyme assays were evaluated. the sensitivity of this test is higher, nearly 40 perSensitivity was definedasthe percentage of women cent of mothers of future impaired infants showwith abnormal enzyme assays among those who decreasing enzyme activity in the blood. Lowgave birth to impaired neonates. Specificity was T-CAP activity of the serum (Tab. ) also proved
Tab. I. Prognostic significance of the assays of serum placental oxytocinase activity.No.: number of women delivered of impaired newbornsa: number öf women delivered of impaired or dead babies with of normal enzyme values (false negative test)b: number of women delivered of impaired or dead babies whose enzyme assays were abnormal (correct test)c: number of women delivered of normal babies whose enzyme assays were normal (correct test)d: number of women delivered of normal newborns with abnormal enzyme assay (false positive test)
2: Chi-square test applying Yates correction :P: probability for one degree of freedom 'N.S.:not significant
Specificity = g-^j X 100
Sensitivity = -~- X 100.
singleassays
serialassays
Condition
impaired or dead newbornperinatal mortality *low Apgar score
impaired or dead newbornperinatal mortalitylow Apgar score
No.
831128
3177
a
718
24
1933
b
1234
1244
c
268331315
104120120
d
132221
223030
X2
8.20644.46011.5041
5.42803.46933.4693
P
< 0.01<0.05
N.S.
<0.02N.S.N.S.
Speci-ficity
48.0012.0016.00
35.2911.7611.76
Sensi- , ,tivity
14.4627.2714.27
38.7157.1457.14
J.Perinat.Med. 4(1976)

Klimek et al., GAP and AP in pregnancy at neuroendocrinological risk 237
Tab. II. Prognostic significance of the assays of tissue oxytocinase activity in the serum. Explanations see Tab. I.
singleassays
serialassays
Condition
impaired or dead newbornperinatal mortalitylow Apgar score
impaired or dead newbornperinatal mortalitylow Apgar score
No.
831128
3177
a
718
25
1831
b
1233
1346
c
268328311
819698
d
132525
374644
X2
8.20643.61100.0653
0.74080.89076.6752
P
< 0.01N.S.N.S.
N.S.N.S.
< 0.01
Speci-ficity
42.8610.7110.71
26.008.00
12.00
Sensi-tivity
14.4627.2710.71
41.9357.1585.71
Tab. III, Prognostic significance of the assays of serum alkaline phosphatase activity. Explanation see Tab. I.
singleassays
serialassays
Condition
impaired or dead newbornperinatal mortalitylow Apgar score
impaired or dead newbornperinatal mortalitylow Apgar score
No.
771127
3067
a
721024
2244
b
513
823
c
258320306
739191
d
111513
313736
x2
0.33420.00021.4265
0.01110.05130.1564
P
N.S.N.S.N.S.
N.S.N.S.N.S.
Speci-ficity
31.256.25
18.75
20.515.137.69
Sensi-tivity
6.499.09
11.11
26.6733.3342.86
Tab. IV. Prognostic significance of the assays of serum heat-stable alkaline phosphatase activity. Explanation see Tab. I.
singleassays
serialassays
Condition
impaired or dead newbornperinatal mortalitylow Apgar score
impaired or dead newbornperinatal mortalitylow Apgar score
No.
771127
3067
a
751126
2133
b
201
934
c
264328313
779595
d
576
273332
X2
0.00280.36470.0043
0.04240.70032.0118
P
N.S.N.S.N.S.
N.S.N.S.N.S.
Speci-ficity
28.570.00
14.29
25.008.33
11.11
Sensi-tivity
2.600.003.70
30.0050.0057.15
to be prognostic of birth of an impaired infant.Sensitivity of this test is similar to that of P-CAP.The differences in perinatal mortality and lowAPGAR score in this group are not significant.Falling T-CAP activity was related only to lowAPGAR score and allows no conclusions concerningimpairment of the neonate in general or perinatalmortality. Only one of every four women withfalling T-CAP activity gives birth to impairedinfants. 42 per cent of the mothers of impairedinfants, and 86 per cent of women who gave birthto infants with a low APGAR score, had an abnor-mal T-CAP profile during pregnancy.
Tabs. III and IV show that neither single nor serialassays of AP and HSAP have value in predictingneonatal impairment. Sensitivity to test was higherfor serial assays, and specificity for single ones,similarly to CAP, but lower äs a rule than those forboth P-CAP and T-CAP.
3 Comments
Until now, evaluation of the enzyme activitiesunder consideration varied. The opinion prevailedthat the phosphatases have no prognostic value forpredicting the state of the neonate [10,12, 25, 29,
J. Perinat. Med. 4(1976)

.238 Klimek et al, CAP and AP in pregnancy at neuroendocrinological risk
31]. Only a few authors emphasize that underpathologic conditions, mainly in gestoses andessential hypertension, a sudden rise or fall inHSAP concentration may be prognostically un-favorable [2,13, 26], and is an indication for strictmonitoring rather than for therapeutic decisions[3]. CAPis considered by most authors to be usefulin the diagnosis of threatened pregnancy [l, 4, 5,7, 8, 16, 18, 20, 21, 22, 28], although a few inves-tigators hold the opposite opinion [9]. A specialapplication of this enzyme assay is in the diagnosisof the hypothalamic post-pregnancy syndrome inpregnant women [23], and the combination ofCAP with AP and cytohormonal vaginal smearsmay be of value in the diagnosis of primary andsecondary placental insufficiency [30]. Thepurpose'cif this study was to compare the prognostic anddiagnostic significance of the aforementionedenzyme assays in pregnant women at neuroendo-crinological risk. We have not encountered ananalysis of this type in the literature and that iswhy we did not subdivide our material intoparticular kinds of high-risk pregnancy which onlyaccompanied the neuroendocrinological risk. Itwas previously found on our material that thearithmetic means of enzyme assays in differentmonths of pregnancy were inversely proportionalto the degree of risk to pregnancy [30], but thiswas not sufficient äs a prognostic measure of themagnitude of risk in the event of an abnormalassay result. In view of the above, two criteria ofabnormality have been proposed: low values andabnormal profile. Abnormally high values, postu-lated by some authors for CAP [27, 32] and AP[2, 13, 26], were not taken into account because
in our material of pregnancy at neuroendocrin-ological risk, increased fetal jeopardy was accom-panied by decreasing enzyme activities [30]. Theresults of the present analysis demonstrated prog-nostic value of oxytocinase assays in endocrino-logically risky pregnancy. Assays of P-CAP andT-CAP were of almost equal significance, not-withstanding reports of a greäter usefulness ofP-CAP [6]. On the other hand, this study confirmsthat phosphatase assays are of no value prognos-tically in neuroendocrinologically pathologic preg-nancy. HSAP was riot superior to AP, äs someauthors have claimed. In profile studies baseduponarithmetic means, AP was even more useful thanHSAP [30], probably owing to the greäter dis-persion of the values of the latter. We also foundthat assays of CAP are helpful in the prögriosis ofperinatal mortality and low APGAR score, i.e.conditions that are frequently encountered in"neuroendocrinological gestosis" [24], the termdenoting all neuroendocrinologic disturbance deve-loped during pregnancy, including placental insuf-ficiency, corpus luteum of pregnancy insufficiencyetc. However, about a half of futüre mothers ofimpaired neonates have values outside the ränge ofthese assays. This is understandable in view of thefact that these enzyme activities reflect placentalactivity but are not directly related to fetal metab-olism. In contemporary obstetric diagnostics, theyshould be supplemented by hormonal assays,especially estriol, examination pf amniotic fluid,ultrasonic examinations and others. If this is carriedout, unpleasant unexpected situations in thedelivery ward and neonatplotgical clinic will beavoided. x>
Summary
Serum enzyme determinations are now well-establisheddiagnostic tools in so-called "placental insufficiency".A good predictability of oxytocinases (P-CAP-placentaloxytocinase and T-CAP-tissue oxytocinase) and a doubtfulone of those of phosphatases (AP-alkaline phosphatase,HSAP-heat stable alkaline pho'sphatase) has been shown inhigh-risk pregnancies. The purpose of this study was todetermine the prognostic value of the above citedenzymes in the so-called "pregnaricy at neuroendo-crinological risk", i.e. pregnancy in women with a pre-pregnancy history of hormonal disorders. It was shownthat the outcome and results of such pregnancies arepoorer that those of normal pregnancies.
The series studied comprised 364 pregnant patients withpregnancy at neuroendocrinological risk that were beingmonitored by means of serum assays of the four enzymes.An attempt was made to assess each of these enzymeactivities both in single (at least one value below 2.5percentile calculated for healthy subjects) and serialdeterminations (two consecutive results decreasing orremaining at the same level). Normal and abnormalenzyme results were compared with normal and ab-normal conditions of the newborn. The resuits presentedshowed that P-CAP (Tab. I) and T-CAP (Tab. II) levelswere useful in prenatal diagnosis of fetal impaiiment ingeneral, in addition to perinatal mortality and low values
J. Perinat. Med. 4(1976)

Klimek et al., CAP and AP in pregnancy at neuroendocrinological risk 239
of the APGAR score. Neither the single nor serial assaysof AP (Tab. III) and HSAP (Tab. IV) were valuable inpredicting birth of an impaired neonate.Sensitivity of the test, i.e. percentage of women withabnormal enzyme assays among those patients who gavebirth to impaired neonates, and specificity of the test,i.e. the percentage of women delivered of impairedneonates among all women with abnormal enzyme assays,of the four enzymes were compared. Sensitivity and speci-ficity of P-CAP and T-CAP were higher than those for APand HSAP. Moreover, sensitivity for all four enzymes washigher in serial assays, and specificity was higher in singleassays.The results of the present analysis demonstrated theprognostic value of oxytocinase assays also in the preg-nancy at neuroendocrinological risk. Assays of P-CAP and
T-CAP were of equal significance, notwithstanding reportsof a greater usefulness of P-CAP. Assays of CAP werehelpful particularly in the conditions on which neuro-endocrinological gestosis exerts a direct influence, i.e. inlow Apgar score and perinatal mortality. On the otherhand, serum alkaline phosphatases proved useless inendocrine pathology of pregnancy and HSAP was notsuperior to AP.About one half of future mothers of impaired neonateshad enzyme results outside the ränge of the assays underconsideration. This could be explained by the fact thatthese enzymes activities reflect placental function andare not directly related to fetal metabolism. Because ofthat they should be supplemented by other diagnosticmethods being used in a clinic of high-risk pregnancy.
Keywords: APGAR score, high-risk pregnancy, perinatal mortality, placental insufficiency, pregnancy at neuroendo-crinological risk, serum alkaline phosphatase, serum heat-stable alkaline phosphatase, serum placental cystineaminopeptidase, serum tissue cystine aminopeptidase
Zusammenfassung
Vergleich des prognostischen Wertes der plazentaren undGewebs-Oxytocinase sowie der alkalischen Phosphataseund ihrer hitzestabilen Fraktion im Serum von Schwange-ren mit neuroendokrinologischem fetalem RisikoSerumenzymbestimmungen gehören heutzutage zum ein-geführten diagnostischen Instrumentarium bei der soge-nannten plazentaren Insuffizienz. Gute Voraussagekraftkonnte diesbezüglich bei Risikoschwangerschaften für dieOxytocinase (P-CAP plazentare Oxytocinase und T-CAPGewebsoxytocinase) und zweifelhafte Aussagekraft fürdie Phosphatasen (AP = alkalische Phosphatase, HSAP =hitzestabile alkalische Phosphatase) nachgewiesen werden.Ziel dieser Studie war es, den prognostischen Wert derangesprochenen Enzyme bei Schwangerschaften mit so-genanntem neuroendokrinologischem Risiko nachzu-weisen. Dabei handelt es sich um Schwangerschaften beiFrauen mit einer präpartalen Anamnese von Hormon^Störungen. Es konnte gezeigt werden, daß der fetale Aus-gang bei solchen Schwangerschaften ungünstiger ist als beinormalen Graviditäten.Die Serie bestand aus 364 schwangeren Frauen mit neuro-endokrinologischen Risiko schwanger Schäften, die durchdie Bestimmung der vier Enzyme überwacht wurden. Eswurde der Versuch unternommen, jede dieser Enzymak-tivitäten sowohl in Einfach- (mindestens ein Wert unter-halb der 2,5 ten Perzentile bezogen auf gesunde Indivi-duen), sowie in Serienbestimmungen (zwei aufeinander-folgende Meßresultate, die abfallen oder auf derselbenHöhe verbleiben) zu bestimmen. Normale und abnormeEnzymmeßresultate wurden mit unauffälligen sowie auf-fälligen Befunden beim Neugeborenen verglichen. Dievorgelegten Resultate zeigen, daß die P-CAP (Tab. I) undT-CAP (Tab. H) -Spiegel nützlich waren in der pränatalenDiagnostik einer generellen fetalen Beeinträchtigung un-abhängig von der perinatalen Mortalität und von tiefenAPGAR-Zahlen. Weder die Einzel- noch die Serienbe-stimmungen der alkalischen Phosphatase (Tab. III), sowie
der hitzestabilen alkalischen Phosphatase (Tab. IV) warenfür die Voraussage eines in seinem Zustand beeinträchtig-ten Neugeborenen brauchbar. Die Sensitivität und dieSpezifizität des Testes wurde für alle vier Enzyme mitein-ander verglichen, d.h., der Prozentsatz an Frauen mitnicht normalen Enzymwerten unter jenen Patientinnen,die ein geschädigtes Kind geboren hatten und der Prozent-satz an Frauen, die ein geschädigtes Neugeborenes hatteninnerhalb der Gruppe von Patientinnen, die alle abnormaleEnzymwerte aufwiesen. Die Sensitivität und Spezifitätder P-CAP und T-CAP war durchweg höher als jene derAP und HSAP. Darüberhinaus zeigte sich, daß die Sensi-tivität für alle vier Enzyme bei Serienbestimmungen höherwar, wo hingegen die Spezifität bei Einzelbestimmungenhöher lag. Die Ergebnisse der vorliegenden Analyse be-legen den prognostischen Wert der Oxytocinasebestim-mung auch bei Schwangerschaften mit neuroendokrino-logischem Risiko. Die Bestimmung der P-CAP und T-CAPwar von gleichwertiger Aussagekraft, was Berichten wider-spricht, die von größerer Brauchbarkeit der P-CAP be-richten. Die Bestimmung der P-CAP war besonders injenen Situationen hilfreich, bei welchen eine neuroendo-krinologische Gestose einen direkten Einfluß ausübte,d.h., bei tiefen Apgarzahlen und perinataler Mortalität.Andererseits zeigte sich die alkalische Serumphosphatasewenig geeignet beim Vorliegen von endokrinologischerSchwangerschaftspathologie und die HSAP war der APdiesbezüglich nicht überlegen. Ungefähr die Hälfte derwerdenden Mütter mit geschädigten Neonaten wiesenEnzymmeßwerte außerhalb der S treubreite für die jeweiligeEnzymbestimmung auf. Dies konnte durch die Tatsacheerklärt werden, daß diese Enzymaktivitäten die plazen-tare Funktion widerspiegeln und nicht direkt mit demfetalen Metabolismus zusammenhängen. Aus diesemGrunde sollten diese Bestimmungen durch andere dia-gnostische Methoden ergänzt werden, die in der Klinik,die Schwangerschaften betreut, zur Anwendung kommen.
Schlüsselwörter: APGAR-Score, alkalische Serumphosphatase, Fetus, Gewebs-Cystine Aminopeptidase, hitzestabileSerumphosphatase, perinatale Mortalität, Plazentainsuffizienz, plazentare Cystin-Aminopeptidase,Risikoschwangerschaft, Schwangerschaft mit neuroendokrinologischem Risiko.
J. Perinat. Med. 4 (1976)

240 Klimek et al., CAP and AP in pregnancy at neuroendocrinological risk
Resume
Valeur comparative de pronostic du serum-oxytocinaseplacentaire et tissulaire, de la phosphatase alcaline et de säfraction stable a la chaleur dans les grossesses avec risqueneuroendocrinologiqueLes evaluations d'enzymes du serum sont a present desmoyens eprouves pour le diagnostic de ladite «insuffisanceplacentaire». Une bonne prediction d'oxytocinases(P-CAP-oxytocinase placentaire et T-CAP-oxytocinase dutissu) et une douteuse de celles de phosphatases (AP-phosphatase alcaline, HSAP-phosphatase alcaline stable ala chaleur) ont ete prouvees pour les grossesses avec undegre eleve de risque. Cette etude a pour but d'illustrer lavaleur de pronostic des enzymes cites ci-dessus dans ladite«grossesse a risque neuroendocrinologique», c.a.d. cellede femmes ayant eu des troubles hormonaux avant ledebut de leur grossesse. On a vu que Tissue et les resultatsde telles grossesses sont moins bons que ceux des grossessesnormales.Les series examinees ont porte sur 364 femmes enceintesa grossesse avec risque neuroendocrinologique qui ont etecontrölees au moyen de serotests des quatre enzymes. Ona essaye d'evaluer chacune de ces enzyme-activites a lafois en determinations simples (au moins une valeur au-dessous de 2,5 pour cent calculee pour les sujets sains) etserielles (deux resultats consecutifs en baisse ou restantau meme niveau). Puis on a compare les enzyme-resultatsnormaux et anormaux aux conditions normales etanormales des nouveaux-nes.Les resultats presentes ont montre que les niveaux P-CAP(Tab. I) et T-CAP (Tab. II) sont utiles pour le diagnosticprenatal de troubles foetaux d.une fa$on generale, outrela mortalite perinatale et les valeurs basses du scoreAPGAR. Ni les essais simples, ni ceux en serie de AP(Tab. III) et HSAP (Tab. IV) n'ont ete valables pour faire
•
prevoir la naissance d'un nouveau-ne en mauvaisecondition.On a compare la sensitive du test des quatre enzymes,c.a.d. le pourcentage des femmes aux enzyme-testsanormaux parmi les parturientes ayant donne naissance ades nouveauxnes en mauvais etat de sant6, et la specificitedu test, c.a.d. le pourcentage des femmes ayant accouchedes nouveaux-nes non sains parmi toutes les femmes auxenzyme-tests anormaux. La sensitivite et la specificite deP-CAP et de T-CAP ont ete plus eleves que celles de APet de HSAP. De plus, la sensitivite pour les quatre enzymesa ete plus elevee dans les essais en serie, et la specificiteplus elevee dans les essais simples.Les resultats de Fanalyse presente ont d6montre la valeurde pronostic des essais d'oxytocinase aussi dans la grossesseavec risque neuroendocrinologique. Les essais de P-CAPet de T-CAP ont ete d'egale signification, malgre lesrapports d'une plus grande utilite de P-CAP. Les tests deCAP ont ete particulierement utiles pour illustrer lessonditions dans lesquelles la gestose neuroendocrinologiqueexerce une influence directe, c.a.d. dans ün score Apgarbas et la mortalite perinataie. D'autre part, les serum-phosphatases alcalines se sont revelees inutiles dans lapathoiogie endocrinienne de grossesse et HSAP n'a pasete superieure a AP. A peu pres la moitie des füturesmeres de nouveaux-nes non sains ont eu des enzyme-rosultats en dehors de la zone des essais consideeres, cequi a pu s'expliquer du fait que ces enzyme-activitesrefletent lafonctiöri placentaire et ne sont pas directementreliees au metabolisme foetal. A cause de cela ilconviendrait de les completer par d'autres methodes dediagnostic utilisees dans un hopital oü sont soigneesbeaucoup de grossesses avec un degre eleve de risque.
Mots-cles: Score APGAR, foetus, grossesse avec risque neuroendocrinologique, grossesse avec un degre eleve de risque,insuffisance placentaire, mortalite perinatale, serum-aminopeptidase cystine placentaire, serum-aminopeptidasecystine tissulaire, serum-phosphatase alcaline, serum-phosphatase alcaline stable a la chaleur.
Bibliography
[1] BABUNA, C., E. VENEN: Enzymatic determinationof placental function. Amer. J. Obstet. Gynec. 95(1966) 925
[2J BADER, P., U. BAERTSCHI, P. J. KELLER,J. SCHMID: Die hitzestabile alkalische Phosphatase(HSAP) bei Spätgestose und Hypertonie. Zbl. Gynäk.2(1971)459
[31 BAERTSCHI, u., P. BADER, J. SCHMID, P. J.KELLER: Die hitzestabile alkalische Phosphatase inder normalen und patologischen Schwangerschaft.Arch. Gynäk. 212 (1972) 217
[4] BLUNT, A.: The value of plasma oxytocinase in theassessment of fetal placental function. Aust. N. Z.Obstet. Gynaec. 11 (1971) 37
[5 ] CARTER, E. R., L. V. GOODMAN, R. M. DE HAAN,J. T. SO BOT A: Serum oxytocinase levels. A labora-tory and clinical appraisal. Amer. J. Obstet. Gynec.119 (1974) 76
[6] CHRISTENSEN, A.: Hormone and enzyme assays inpregnancy. I. Studies on the placental and the tissuecystine-aminopeptidase activity in peripheral plasmafrom non-pregnant and pregnant women and inplasma from the umbilical cord. Acta Endocr 76(1974) 189
[7] CHRISTENSEN, A.: Hormone and enzyme assays inpregnancy. HI. The placental cystine-aminopeptidaseand the urinary öestrogens in pregnancies complic'atedwith essential hypertension, mild qr severe pre-eclampsia. Acta Endocr. 76 (1974) 353
[8] CHRISTENSEN, A., D. FR0YSHOW, P. FYLLING:Hormone and enzyme assays in pregnancy. IV. Thehuman chorionic somatomammotrophin, placentalcystine äminopeptidase, progesterone and theurinary oestrogens in pregnancies complicated withessential hypertension, mild or severe pre-eclampsia.Acta Endocr. 77 (1974) 344 ,·.·
J. Perinat. Med. 4(1976)

Klimek et al, CAP and AP in pregnancy at neuroendocrinological risk 241
[9JCURZEN, P., R. VARMA: A comparison of serumcystine aminopeptidase and urinary estrogen excretionäs placental function tests. Amer. J. Obstet. Gynec.115(1973)929
[10JCURZEN, P., R. VARMA:, A comparison of serumheat stable alkaline phosphatase and urinary estrogenexcretion in the mother äs placental function tests. J.Obstet. Gynaec. Brit. Cwlth 78 (1971) 686
[11JDICZFALUSY, E.: Endocrine functions of thehuman fetus and placenta. Amer. J. Obstet. Gynec.119(1974)419
112] DUMONT, M., R. MALLEIN, Y. PAGE, J. LANSAC:The alkaline phosphatase thermostable at 65°C andplacenta function. Rev. Franc. Gynec. 66 (1971) 187
[13JELDER, M. G.: Serum heat-stable alkaline phos-phatase levels in normal and abnormal pregnancy.Amer. J. Obstet. Gynec. 113 (1972) 833
[14] HANSEN, P. W.: A simplification of King and King'smethod for determination of serum phosphatase.Scand. J. Clin. Lab. Invest. 18 (1966) 353
[15JHERRERA, L.: The precision of percentiles inestablishing normal limits in medicine. J. Lab. Clin.Med. 52 (1958) 34
[16JHURRY, D. J., J. E. TOVEY, D. A. ROBINSON,C. L. BEYNON, K. COOPER: Cystine aminopeptidasein normal and complicated pregnancies. J. Obstet.Gynaec. Brit. Cwlth 79 (1972) 788
[17JHYTTEN, F. E., T. LIND: Diagnostische Indizes inder Schwangerschaft. Ciba-Geigy Ltd., Basle 1974
[18] KLEINER, H.: Serum L-leucyl^S-naphthylamidehydrolase (LNAse) activity in normal human preg-nancy and in pregnancy associated with foetaldysmaturity. Exe. Med. Int. Congr. Ser. 183 (1968)363
[19] KLIMEK, R., M. PlETRZYCKA: BiochemischeMethode zur Bestimmung der Oxytocinase und ihreklinische Bewertung. Clin. Chim. Acta 6 (1961) 326
[20] KLIMEK, R., A. BIENIASZ: Studies on therelationbetween serum oxytocinase and course of labor.Amer. J. Obstet. Gynec. 104 (1969) 959
[21] KLIMEK, R.,K. DREWNIAK, A. BIENIASZ: Furtherstudies on the oxytocin-oxytocinase System. Amer.J. Obstet. Gynec. 105 (1969) 427
[22] KLIMEK, R., E. MALOLEPSZY: Evaluation of arapid enzymatic test for determining placentalfunction. Clin. Chim. Acta 24 (1969) 349
[23] KLIMEK, R., M. PAWLIKOWSKI: Neuroendo-krynologiakliniczna. Panstwowy Zaklad WydawnictwLekarskich, Warszawa 1973
[24] KLIMEK, R., J. STANEK: Ciaza o wysokim ryzykuw ujeciu neuroendokrynologicznym. Gin. Pol. 47(1976) 89
[25] LIESER, H., . w. TIETZE, G. H. RATHGEN:Untersuchungen zur Bedeutung der hitzestabilenalkalischen Phosphatase im Schwangerenserum zurErkennung fetaler Risikozustände. Geburtsh. Frauen-heük. 33(1973) 395
[26] MERRETT, J. D., R. J. HUNTER: Serum heat stablealkaline phosphatase levels in normal and abnormalpregnancies. J. Obstet. Gynaec. Brit. Cwlth. 80 (1973)957
[27] POCH, G., L. ABADMARTINEZ, E. HOLZER,W. HOHLWEG: Vergleich der Oxytocinaseaktivitätdes Serums mit der Ausscheidung von Choriongonado-tropin und Östriol während der zweiten Schwanger-schaftshälfte. Arch. Gynäk. 208 (1970) 416
[28] RYDEN, G.: Cystine aminopeptidase activity in preg-nancy. Acta Obstet. Gynec. Scand. 53 (1974) 341
[29] SHANE, J. M., K. SUZUKI: Placental alkaline phos-phatase: a review and reevaluation of its applicabilityin monitoring fetoplacental function. Obstet. Gynec.Surv. 29 (1974) 97
[30] STANEK, J.: Enzymatyczno-cytohormonalnemonitorowanie endokrynologicznie zagrozonej ciazy.FoliaMed. Cracov. 17 (1975) 365
[31] TATRA, G., H. CAUCIG, A. SEIDL: Hitzestabilealkalische Phosphatase bei normaler und pathologi-scher Schwangerschaft. Geburtsch. Frauenheilk. 32(1972)336
[32] WEIN GOLD, A. B.: Approaches to the fetus-ante-partum and extrauterine. In: ABRAMSON, H.:Symposium on the functional physiopathology ofthe fetus and neonate. Mosby, Saint Louis 1971
Received May 27, 1975. Accepted June 14, 1976.
Prof. Dr. R. KlimekClinic of EndocrinologyInstitute of Gynecology and Obstetrics23, Kopernika St.,31-501 Cracow/Poland
J. Perinat. Med. 4(1976)





























