Embed Size (px)
Citation preview

Arch Gynecol Obstet
DOI 10.1007/s00404-006-0288-yORIGINAL ARTICLE
Comparison of Nicolaides’ risk evaluation for down’s syndrome with a novel software: an analysis of 1,463 cases
Peter Schmidt · Ismini Staboulidou · Philipp Soergel · Max Wüstemann · Peter Hillemanns · Alexander Scharf
Received: 12 September 2006 / Accepted: 6 November 2006© Springer-Verlag 2007
AbstractObjective The individual risk assessment of fetalDown’s syndrome based on measurement of nuchaltranslucency (NT) according to Nicolaides, optionallycomplemented by the determination of PAPP-A andfree beta HCG has progressively supplanted othersearch strategies for fetal aneuploidies. It could beshown that this diagnostic strategy equally detectsother numeric aneuploidies at a comparable rate. Apositive test result is also predictive for the presence ofa fetal malformation. In this Weld, several computerprograms are available for clinical use. The objective ofour study was to re-evaluate the Wrst consecutive 1463NT-risk calculations determined by Nicolaides’method and to compare the risk calculation to the JOYsoftware (NT-risk calculation module, JOY PatientDatabase) introduced in 2002.Material and methods At the Department of Obstet-rics and Gynecology, Hannover Medical School, 1463consecutive complete data sets comprising Wrst trimes-ter screening performed between May 2, 2000 and June26, 2003 and corresponding fetal outcome were analysed
using risk assessment based on the Nicolaides method(PIA Fetal Database NT-Module) and compared withthe risk evaluation as determined by the JOY software(JOY Patient Database NT module). A risk exceeding1:300 was considered to indicate the need for furtherinvasive testing. In a Wrst step, only cytogeneticallydetectable chromosomal aberrations were analysed.Then, a second evaluation including fetal malforma-tions was performed.Results Among the 1463 cases, 1445 (98.77%) fetusesrevealed to be cytogenetically healthy. Both softwaresshowed identical detection rates at the genetic andsomatic level:13 cases of Down-Syndrome (0.89%), 2cases of trisomy 18 (0.14%), one case of triploidy, oneTurner-Syndrome, one Klinefelter-Syndrome (0.07%each) were detected. A positive test result was found in15 cases ending in a spontaneous abortion, intrauterinedeath or peripartum death (1.03%) and in 22 cases offetal malformation (1.50%). At the level of geneticdetection the test positive rate dropped from 92 (PIA)to 71 (JOY) (-22.8%). At the level of combinedadverse outcome the test positive rate was reducedfrom 100 (PIA) to 76 (JOY) (-22.0%), thus yielding ina marked improvement of the characteristic test per-formance parameters.Conclusion The novel, recently developed JOY soft-ware package allowed reliable evaluation of the risk foraneuploidy with increased speciWcity whereas sensitivitywas unchanged. Our data suggest an improvement ofthe screening for aneuploidy when using this novel soft-ware: With an identical detection rate, the number ofunnecessary invasive measures may be reduced.
Keywords Nuchal translucency · Risk · Aneuploidy · Software · Down syndrome
P. Schmidt · I. Staboulidou · P. Soergel · M. Wüstemann · P. HillemannsDepartment of Obstetrics and Gynecology, Division of General Gynecology and Perinatal Medicine, Medical University of Hannover, Hannover, Germany
P. Schmidt (&)Werner-Schrader-Str. 61, 38302 Wolfenbüttel, Germanye-mail: [email protected]
A. ScharfUniversity of Heidelberg, Heidelberg, Germany
123

Arch Gynecol Obstet
Introduction
In 1998 Nicolaides and coworkers presented theirmulticenter study on Wrst-trimester aneuploidyscreening [1], which is based on maternal age andfetal nuchal translucency (NT) [2, 3]. This methodfound broad acceptance as well in Europe as inmany other countries worldwide [4]. For the Wrsttime risk assessment could be obtained by fetalultrasound [5–7]. Individualized risk-adaptation wasextended to the so-called ‘combined testing’ andincludes the maternal age, gestational age, NTnormalized to fetal crown-rump length (CRL), andbiochemical parameters [pregnancy-associatedplasma protein A (PAPP-A) and free (f) �-HCG][8].
In April 2001 this method was implemented as aroutine procedure in our hospital (Department ofObstetrics and Gynecology, Hannover MedicalSchool, Hannover, Germany) and hence has beenperformed successfully in more than 3,600 patients.Even if considered a routine procedure, it cannot beneglected that the consequence of possibly invasivediagnostic measures refers to important clinical, ethi-cal, and psychological considerations [9]. Since, early2003, a novel software for individual aneuploidy risk-calculation based on published data (NT-risk calcula-tion module, JOY patient database, PET-Software,Wolfenbüttel, Germany) is available. This methodapplies an algorithm similar to Nicolaides’ principle ofsequential screening with determination of test-spe-ciWc probability-factors using Palomaki’s likelihoodmethod [10, 11]. The background risk was calculatedbased on the tables published by Snijders in 1999 [12].Normal distribution curves for NT were derived fromdata by Nicolaides et al. [13]. The NT-likelihood ratiowas calculated on the base of the 1998 British multi-center study data [1]. Likelihood ratios for the bio-chemical parameters were calculated from the datapublished by Wald and Hackshaw [14]. Therefore,JOY was established on the basis of previously pub-lished and well-evaluated studies with large patientnumbers. In an introductory retrospective study, itsclinical applicability could be demonstrated [15]. Atthe Department of Obstetrics and Gynecology, Han-nover Medical School, all Wrst trimester tests were cal-culated prospectively with both PIA and JOY,starting in February 2003. The aim of this study was tore-evaluate the results of the initial study in a dis-tinctly larger number of cases examined at the level ofdetection of genetic as well as somatic fetal disordersafter the use of both softwares in an additionalprospective setting.
Materials and methods
Examinations of 1,480 singleton pregnancies at theMedical Highschool of Hannover had been evaluatedbetween May 2, 2000, and June 26, 2003. Ultrasoundmeasurements had been performed between 11 + 0and 13 + 6 weeks of gestation according to the stan-dards of the Fetal Medicine Foundation (FMF). Allexaminers were trained and certiWed by the FMF(London, UK). The following parameters were usedfor calculation: maternal age at time of measurement,gestational age, CRL, NT, PAPP-A, and f�-HCG asmultiple of medians (MoM). Since, April 2001, the bio-chemical parameters were determined systematically.Only in cases with serious increased NT and a consecu-tive high-suspicious adjusted risk biochemical parame-ters had not been valuation at all times. Some womenwith increased NT, especially above 99th percentile,opted for direct invasive testing rather than await theresults of the combined test. Determinations were per-formed in a single laboratory (Pruggmayer, Peine, Ger-many) certiWed by the FMF. Risk calculation wascomputed using both the original Nicolaides software(PIA Fetal Database, GE-Viewpoint, Wesseling, Ger-many) and the novel JOY software (PET Software,Wolfenbuettel, Germany). Both softwares computerisks for trisomy 21 in an identical way on the base of acommon background risk [12], which is multiplied bylikelihood ratios according to the NT measurementvalue [1] and—if available—by likelihood ratiosaccording to free �-Hcg and Papp-A [11, 14].
The following results were determined:
(1) Background risk for Down’s syndrome based onmaternal age and gestational age.
(2) Adjusted risk
(a) +NT-measurement (n = 209), or—if available—(b) +NT-measurement + biochemical parameters
(PAPP-A and f�-HCG) (n = 1,270).
In a Wrst step, these results were analyzed regarding therespective test performance parameters (sensitivity,speciWcity, positive predictive value (PPV), negativepredictive value (NPV), and frequency of invasive test-ing) on the level of detecting genetic disorders bymeans of a fourfold table analysis. In a second step, theaforementioned analysis was applied to the overall testperformance on the level of detecting genetic disordersor somatic malformations or intrauterine/perinataldeath. Statistical signiWcance testing was performed byMcNemar-test by WinStat (R. Fitch-software, Staufen,Germany).
123

Arch Gynecol Obstet
Results
Out of 1,480 cases, one case of Turner syndrome at10 + 2 gestational weeks (out of validated time frame),and 16 data sets lacking information on genetic outcomedue to either spontaneous abortion or termination ofpregnancy in the face of the seriousness of a diagnosedsomatic disorder were found. Thus, with respect to ageneral outcome 1,479 cases (99.93%) and with respectto known genetic outcome 1,463 cases could be ana-lyzed (98.85%). Of the latter 1,463 cases, 1,445 showedto have a normal karyotype (either prenatal genetic test-ing or normal postpartum clinical appearance). In 18cases (1.23%), an abnormal karyotype was found(Table 1). In 27 cases, an ultrasonographically detect-able fetal malformation was found (Table 2). six of thesecases (2£ hygoma, 2£ fetal hydrops, 1£ thanatophoricdysplasia, 1£ hygroma colli) were not genetically ana-lyzed. Twenty-one of these cases underwent a geneticalanalysis. A normal result was found in 19 cases. Amongthe three cases of hygroma and hydrops each, one caseof trisomy 21 was found.
The age of the observed pregnant women rangedfrom 16 to 43 years (mean: 31.3 years, median: 32 years).In the Weld of cytogenetical suspicioucities the meanage was slightly increased (mean: 33.7 years, median35 years, and range 23–43 years). Out of 1,479 preg-nancies with known general outcome 38 cases showedsomatic malformations with or without intrauterine
death. Thereof the genetic result of 16 fetuses had notbeen retrieved. Of the remaining 22 cases a trisomy 21had been detected in three fetuses. All other pregnan-cies were cytogenetically healthy.
Measurement values of the NT ranges from 0.5 to5.5 mm (median: 1.5 mm, mean 1.57 mm) in healthyfetuses. Cases with trisomy 21 had a median NT of4.6 mm (mean 4.67, range 1.5–8.7 mm). The NT wasfound to be between 1.5 and 4.1 mm (median 2.8 mm,mean 2.8 mm) in pregnancies with trisomy 18. Othergenetical anomalities showed a NT value of 5.83 mmby mean [1.5–12.2 mm (45 £ 0), median 3.8 mm].Cases with malformations and/or intrauterine deathhad a NT value between 0.8 and 12.5 mm (median1.9 mm, mean 3.17 mm).
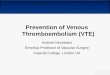
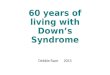
On the level of detecting genetic disorders as well asat level of overall detection, both softwares showedidentical or nearly identical results regarding sensitivityand NPV (Tables 3, 4, Figs. 1, 2). In comparison toPIA, the usage of JOY increased speciWcity from 94.5to 96.1% (P < 0.00001) (genetic detection) and from94.7 to 96.2% (P < 0.00001) (overall detection). Simul-taneously, the PPV in JOY was found to be 4.2%(genetic detection) and 6.8% (overall detection)increased as compared to PIA.
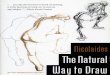
At the level of genetic detection, with the applica-tion of JOY, the test positive rate dropped from 92(PIA) to 70 (JOY), hence reducing the number ofunnecessary invasive procedures from 79 (PIA) to 57(JOY). This equals a reduction of 23.9% regarding testpositive rate and a reduction of 27.9% regarding falsepositive rate (Table 3, Fig. 3).
At the level of overall detection, with the applica-tion of JOY, the test positive rate dropped from 100(PIA) to 78 (JOY) (P < 0.00001), hence reducing thenumber of unnecessary invasive procedures from 76(PIA) to 54 (JOY) (P < 0.00001). This equals a reduc-tion of 22.0% regarding test positive rate and a reduc-tion of 29.0% regarding false positive rate (Table 4).
Table 1 Genetic disorders in this study. PIA and JOY softwareprovided identical detection
Type of genetic disorder
n (%) NT > 95 percentile (n)
Positive test results (PIA/JOY)
Trisomy 21 13 (0.89) 10 10/10Trisomy 18 2 (0.14) 1 1/1Triploidy 1 (0.07) 1 1/1Turner-Syndrome 1 (0.07) 1 1/1Triplo-X-Syndrome 1 (0.07) 0 0/0
Table 2 Overview of the malformations that were found in this study. PIA and JOY software provided identical detection
Type of malformation n (%) NT > 95 percentile (n)
Positive test results (PIA/JOY)
Cardiac malformations (VSD, TGA, PS, HLHS) 8 (0.54) 2 2/2Hygroma colli 3 (0.20) 3 3/3CNS malformations (anencephaly, microcephaly,
Dandy–Walker anomaly)3 (0.20) 0 0/0
Defects of outer surface (exomphalos, hypospadia, fetal facial clefts)
3 (0.20) 1 1/1
Skeletal anomalies (polydaytyly, club foot, thanatophoric dysplasia)
3 (0.20) 1 1/1
Hydrops fetalis 3 (0.20) 3 3/3Renal anomalies (hydronephrosis, renal hypoplasia) 2 (0.14) 0 0/0Cystic neck teratoma 1 (0.07) 0 0/0Severe combined malformation syndome 1 (0.07) 0 0/0
123

Arch Gynecol Obstet
Discussion
The presented Wndings corroborate the results of theinitial study of our working group in this Weld [15].
Regarding genetic test performance rates, both soft-wares detected the same number of true positive casesin identical individuals (n = 13). Hence, both softwaresshow identical values for sensitivity and NPV. Due tothe reduced count of false positives in JOY, the rate oftrue negatives is found to be increased (1,387 vs. 1,366),thus yielding a higher speciWcity and markedly increasedPPV (31% improvement). With both PIA and JOY, 5cases of aneuploidy (three cases of trisomy 21, one caseof trisomy 18, one case of Triple-X-Syndrome) were notdetected regarding risk assessment for trisomy 21 alone.The case of trisomy 18 had a normal NT measurement(1.5 mm), PAPP-A was at 0.39 MoM, free �HCG wasfound to be 0.12 MoM. This resulted in an adjusted riskassessment of 1: 306 with PIA and 1: 314 in JOY. Con-trary to the mere risk assessment regarding trisomy 21,an invasive test was carried out because of the clinician’sappraisal of the conspicuous biochemistry. The otherfour cases occurred in the initial phase of this study,when biochemistry was not yet routinely measured.Therefore, risk assessment in these four cases was basedon NT measurement solely. These results correspond topublished data, which document a signiWcant increase ofsensitivity when Wrst trimester biochemistry is included
Table 3 Test performance parameters for PIA and JOY soft-ware regarding genetic disorders only
PIA JOY
Sensitivity (%) 72.22 72.22SpeciWcity (%) 94.53 96.06Positive predictive value (%) 14.13 18.57Negative predictive value (%) 99.64 99.64Test positive rate (n) 92 70Test positive rate (%) 100.00 76.09Number of unnecessary interventions (n) 79 57Number of unnecessary interventions (%) 100.00 72.15
Table 4 Test performance parameters for PIA and JOY soft-ware regarding genetic disorders as well as somatic malforma-tions
PIA JOY
Sensitivity (%) 44.44 44.44SpeciWcity (%) 94.67 96.21Positive predictive value (%) 24.00 30.77Negative predictive value (%) 97.83 97.86Test positive rate (n) 100 78Test positive rate (%) 100.00 78.00Number of unnecessary interventions (n) 76 54Number of unnecessary interventions (%) 100.00 71.05
Fig. 1 Comparison of test performance parameters “Sensitivity”and “SpeciWcity”
Fig. 2 Comparison of test performance parameters “PPV” and“NPV”
123

Arch Gynecol Obstet
[1, 16] and strongly support a combined (NT plus bio-chemistry) policy of Wrst trimester screening (FTS) [17].
Regarding overall test performance rates, both soft-wares detected the same number of true positive casesin identical individuals (n = 24). Hence, both softwaresshow identical values for sensitivity and nearly identi-cal values for NPV (diVerence not signiWcant, P =0.32). Due to the reduced count of false positives inJOY, the rate of true negatives is found to be increased(1,372 vs. 1,350), thus yielding a higher speciWcity andon this level markedly increased PPV (28% improve-ment).
In addition to the aforementioned Wve cases of over-seen genetical disorders (out of a total of 18), 9 of 14cases with intrauterine demise or spontaneous abortionwere not correctly predicted (sensitivity 35%). At thelevel of structural fetal malformations (total number:27), six of eight cardiac defects were not detected (sen-sitivity: 25%). All three CNS-malformations were notdetected by both software programs. Of the remaining16 malformations, six cases (one cystic neck teratoma,one thanatophoric dysplasia, two cases of fetalhydrops, two cases of fetal hygroma) were detectedwith both search strategies (sensitivity: 37.5%). Thelow-detection rate of cardiac defects in this studyappears to be in contrast to published data, where amaximum 56% sensitivity has been reported with a 5%false positive rate [18, 19].
The low-detection rates of FTS regarding fetal mal-formations and intrauterine demise/abortion deWnitelycontributes to the markedly lower sensitivity of 44% ofcombined NT measurement when used as a general,unspeciWc search strategy for fetal pathologies. In thisrespect, FTS seems not to be suitable for this purposeas opposed to its performance on the genetical level.However, FTS shows to have a relatively high PPV inthis Weld (24% in PIA, 30% in JOY). This is mainlycaused by the fact that the incidence of abortionsbeyond the Wrst trimester as well as the prevalence ofmajor fetal malformations ranges around 3% each [20,21] and is thus tenfold higher as the prevalence ofDown-Syndrome being the most frequent numericalchromosomal aberration. FTS therefore seems to be asuitable tool in screening for fetal pathologies.
In single case comparisons it could be documentedthat the diVerences of the generated adjusted risks inboth programs are mainly caused by diVerences in theirrespective biochemical parts. While the NT calculationin PIA and JOY are based on the same published data[1], the computing of the biochemical likelihood ratiosin the PIA software utilizes the data analysis of Spen-cer et al. [16]. In contrast, JOY utilizes the data pub-lished by Wald and Hackshaw [14] for this purpose.Obviously, the latter data seem to reXect biologicalinterdependencies in this respect in a more accuratemanner. This can also be documented in the reducedfrequency of invasive follow-up tests. In the study athand, with the application of JOY, a reduction of the(in retrospect) unnecessary puncture rate of 27.8%(genetical test) and 29.0% (overall test) could beachieved.
As a summary, JOY software yields a markedlyreduced count of false positive results with an identicaldetection rate of fetal distinctive features, hence con-tributing signiWcantly to an increased selectivity ofFTS.
References
1. Snijders RJ, Noble P, Sebire N, Souka A, Nicolaides KH(1998) UK multicentre project on assessment of risk of tri-somy 21 by maternal age and fetal nuchal-translucency thick-ness at 10-14 weeks of gestation. Fetal Medicine FoundationFirst Trimester Screening Group. Lancet 352:343–346
2. Pandya PP, Snijders RJ, Johnson SP, De Lourdes Brizot M,Nicolaides KH (1995) Screening for fetal trisomies by mater-nal age and fetal nuchal translucency thickness at 10 to14 weeks of gestation. Br J Obstet Gynaecol 102:957–962
3. Schuchter K, Wald N, Hackshaw AK, Hafner E, Liebhart E(1998) The distribution of nuchal translucency at 10-13 weeksof pregnancy. Prenat Diagn 18:281–286
Fig. 3 Test positive rate (Genetic detection)
123

Arch Gynecol Obstet
4. Krampl E, Wertaschnigg D, Husslein P (2002) First-trimesterscreening for Down’s syndrome. Geburtshilfe Frauenheilkd62:843–848
5. Nicolaides KH, Azar G, Byrne D, Mansur C, Marks K (1992)Fetal nuchal translucency: ultrasound screening for chromo-somal defects in Wrst trimester of pregnancy. BMJ 304:867–869
6. Snijders RJ, Holzgreve W, Cuckle H, Nicolaides KH (1994)Maternal age-speciWc risks for trisomies at 9-14 weeks’ gesta-tion. Prenat Diagn 14:543–552
7. Braithwaite JM, Morris RW, Economides DL (1996) Nuchaltranslucency measurements: frequency distribution andchanges with gestation in a general population. Br J ObstetGynaecol 103:1201–1204
8. Wald N, Stone R, Cuckle HS, Grudzinskas JG, Barkai G,Brambati B, Teisner B, Fuhrmann W (1992) First trimesterconcentrations of pregnancy associated plasma protein A andplacental protein 14 in Down’s syndrome. BMJ 305:28
9. Kowalcek I, MühlhoV A, Bieniakiewizc I, Gembruch U(2001) Non-invasive and invasive prenatal diagnosis and psy-chological challenges for the pregnant patient. GeburtshilfeFrauenheilkd 61:593–598
10. Snijders RJM, Nicolaides KH (1996) Assessment of risks. In:Snijders RJM, Nicolaides KH (eds) Ultrasound markers forfetal chromosomal defects. Parthenon Publishing, Carnforth,UK, pp 109–113
11. Palomaki GE, Haddow JE (1987) Maternal serum alpha-fetoprotein, age, and Down syndrome risk. Am J ObstetGynecol 156:460–463
12. Snijders RJ, Sundberg K, Holzgreve W, Henry G, NicolaidesKH (1999) Maternal age- and gestation-speciWc risk for tri-somy 21. Ultrasound Obstet Gynecol 13:167–170
13. Nicolaides KH, Sebire N, Snijders RJM (1999) Nuchal trans-lucency and chromosomal anomalies. In: Nicolaides KH,
Sebire N, Snijders RJM (eds) The 11-14-week scan: the diag-nosis of fetal abnormalities. Parthenon Publishing, Carnforth,UK, pp 3–72
14. Wald NJ, Hackshaw AK (1997) Combining ultrasound andbiochemistry in Wrst-trimester screening for Down’s syn-drome. Prenat Diagn 17:821–829
15. Scharf A, Schmidt P, Seppelt M, Maul H, Wuestemann M,Sohn C (2003) Vergleich der Risikokalkulation für Trisomie21 nach Nicolaides mit einer neu entwickelten Software: Ret-rospektive Analyse an 744 Fällen, Geburtsh Frauenheilk63:148–152
16. Spencer K, Souter V, Tul N, Snijders R, Nicolaides KH(1999) Screening program for trisomy 21at 10/14 weeks usingfetal nuchal translucency, maternal serum free �-human cho-rionic gonadotropin an prgnancy-associated plasma protein-A. Ultrasound Obstet Gynecol 13:231–237
17. Scharf A, Bock N, Maul H, Sohn C (2006) Analyse desNackentransparenz (NT-)Screeningkonzepts an der Frauen-klinik der MHH: Eine prospektive Follow-up-Studie. Z Ge-burtshilfe Neonatol 210(3):99–106
18. Souka A, Heath V (1999) Increased nuchal translucency withnormal karyotype. In: Nicolaides KH, Sebire N, SnijdersRJM (eds) The 11-14-week scan: the diagnosis of fetal abnor-malities. Parthenon Publishing, Carnforth, UK, pp 73–97
19. Hyett J, Perdu M, Sharland G, Snijders R, Nicolaides KH(1999) Using fetal nuchal translucency to screen for majorcongenital cardiac defects at 10-14 weeks of gestation: popu-lation based cohort study. BMJ 318(7176):81–85
20. Harlap S; Shiono PH (1980) Alcohol, smoking, and incidenceof spontaneous abortions in the Wrst and second trimester.Lancet 2(8187):173–176
21. Chitty LS, Hunt GH, Moore J, Lobb MO (1991) EVectivenessof routine ultrasonography in detecting fetal structuralabnormalities in a low risk population. BMJ 303:1165–1169
123