Embed Size (px)
Citation preview
Comparison of Pyrosequencing, Sanger Sequencing, and MeltingCurve Analysis for Detection of Low-Frequency Macrolide-ResistantMycoplasma pneumoniae Quasispecies in Respiratory Specimens
Kwok-Hung Chan,a Kelvin K. W. To,a,b,c,d Betsy W. K. Chan,a Clara P. Y. Li,a Susan S. Chiu,e Kwok-Yung Yuen,a,b,c,d Pak-Leung Hoa,b,c,d
Department of Microbiology,a State Key Laboratory for Emerging Infectious Diseases,b Research Centre of Infection and Immunology,c Carol Yu Centre for Infection,d andDepartment of Pediatrics and Adolescent Medicine,e The University of Hong Kong, Pokfulam, Hong Kong Special Administrative Region, China
Macrolide-resistant Mycoplasma pneumoniae (MRMP) is emerging worldwide and has been associated with treatment failure.In this study, we used pyrosequencing to detect low-frequency MRMP quasispecies in respiratory specimens, and we compared thefindings with those obtained by Sanger sequencing and SimpleProbe PCR coupled with a melting curve analysis (SimpleProbePCR). Sanger sequencing, SimpleProbe PCR, and pyrosequencing were successfully performed for 96.7% (88/91), 96.7% (88/91),and 93.4% (85/91) of the M. pneumoniae-positive specimens, respectively. The A-to-G transition at position 2063 was the onlymutation identified. Pyrosequencing identified A2063G MRMP quasispecies populations in 78.8% (67/88) of the specimens.Only 38.8% (26/67) of these specimens with the A2063G quasispecies detected by pyrosequencing were found to be A2063G qua-sispecies by Sanger sequencing or SimpleProbe PCR. The specimens that could be detected by SimpleProbe PCR and Sanger se-quencing had higher frequencies of MRMP quasispecies (51% to 100%) than those that could not be detected by those two meth-ods (1% to 44%). SimpleProbe PCR correctly categorized all specimens that were identified as wild type or mutant by Sangersequencing. The clinical characteristics of the patients were not significantly different when they were grouped by the presenceor absence of MRMP quasispecies, while patients with MRMP identified by Sanger sequencing more often required a switchfrom macrolides to an alternative M. pneumoniae-targeted therapy. The clinical significance of mutant quasispecies should beinvestigated further with larger patient populations and with specimens obtained before and after macrolide therapy.
Mycoplasma pneumoniae is a major cause of community-ac-quired pneumonia, especially for children and young adults
(1–3). Macrolides have been recommended for the treatment ofM. pneumoniae because of their low MIC and good safety profilefor children and pregnant women (4). However, macrolide-resis-tant M. pneumoniae (MRMP) has been increasingly prevalentworldwide, initially in Asia and now spreading to Europe andNorth America (5–11). School outbreaks due to MRMP have alsooccurred (12, 13). Treatment failures with macrolides due topneumonia caused by MRMP have been reported (14). These de-velopments highlight the need for a timely diagnosis of MRMP forthe clinical management of patients, infection control, and publichealth purposes.
MRMP has been attributed to point mutations in the 23SrRNA. High-level resistance is found for mutations at nucleotidepositions 2063 and 2064 where macrolide binds, while low-levelresistance is related to mutations at the nearby nucleotide posi-tions 2067 and 2617 (8). Macrolide resistance in M. pneumoniaehas traditionally been determined by broth dilution tests (15).However, M. pneumoniae culture is not usually available in mostclinical laboratories due to special requirements. Hence, molecu-lar methods have been used for the genotypic detection of muta-tions that confer resistance to macrolides. An important advan-tage of genotypic testing is that it can be performed directly on theclinical specimens. The techniques that have been applied for thedirect detection of MRMP include PCR followed by Sanger se-quencing (11, 14, 16), pyrosequencing (17, 18), high-resolutionmelting curve analysis (19–21), allele-specific PCR (22), and PCR-restriction fragment length polymorphism (23). In the context ofviral infections, natural occurrences of mixed drug-sensitive and-resistant subpopulations are well documented (24–28). The en-
richment of minor resistant subpopulations has further beendemonstrated to be associated with antiviral treatment failure (25,26). This has led to the term “quasispecies,” which has been usedwidely to describe sequence variants in heterogeneous virus pop-ulations (25, 26). Recent studies involving Sanger sequencing sug-gested that mycoplasma infections might also comprise mixedpopulations of drug-sensitive and drug-resistant molecular mu-tants (i.e., quasispecies at the 23S rRNA macrolide resistance mo-tif) (29). While Sanger sequencing can detect molecular mutantsthat are present in relatively high abundances, only pyrosequenc-ing can detect molecular mutants that are present at low frequen-cies (24).
In this study, we sought to determine the prevalence of MRMPin Hong Kong. We have used three different methods for the mo-lecular detection of macrolide-resistant mutants. Mutant quasi-species were detected and quantified by pyrosequencing. The re-sults from pyrosequencing were compared to those obtained fromSanger sequencing. We also developed a SimpleProbe real-timePCR coupled to melting curve analysis (SimpleProbe PCR) forrapid detection of the mutant genotype. Furthermore, we deter-
Received 25 March 2013 Returned for modification 22 April 2013Accepted 22 May 2013
Published ahead of print 29 May 2013
Address correspondence to Pak-Leung Ho, [email protected].
K.-H.C. and K.K.W.T. contributed equally to this article.
Copyright © 2013, American Society for Microbiology. All Rights Reserved.
doi:10.1128/JCM.00785-13
2592 jcm.asm.org Journal of Clinical Microbiology p. 2592–2598 August 2013 Volume 51 Number 8
on April 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
mined the subtype of M. pneumoniae and evaluated whether therewas any association between MRMP and M. pneumoniae subtype.
MATERIALS AND METHODSPatients. This study was conducted in a University of Hong Kong-affili-ated hospital with 1,650 beds. Patients were included if their respiratorytract specimens obtained between April 2010 and March 2012 were pos-itive for M. pneumoniae by PCR. Patients were excluded if there wereinsufficient archived specimens. Nasopharyngeal aspirate was collected inviral transport medium consisting of Earle’s balanced salt solution (Bio-Source International, Camarillo, CA), 4.4% bicarbonate, 5% bovine se-rum albumin, vancomycin (100 �g/ml), amikacin (30 �g/ml), and nys-tatin (40 U/ml), as described previously (30, 31). Sputum specimens werecollected with standard procedures (32). Requests for M. pneumoniaetesting were initiated by frontline clinicians when there was a clinicalsuspicion of M. pneumoniae infection. Clinical information was obtainedfrom the clinical management system. This study has been approved bythe institutional review board of the University of Hong Kong/HospitalAuthority Hong Kong West Cluster.
DNA extraction. Nucleic acid extraction was performed by using theNucliSENS easyMAG extraction system (bioMérieux, France), as de-scribed previously (33). Briefly, 250 �l of clinical specimens was added to2 ml of lysis buffer and incubated for 10 min at room temperature. Nucleicacid was finally eluted in 55 �l after automatic magnetic separation andstored at �80°C.
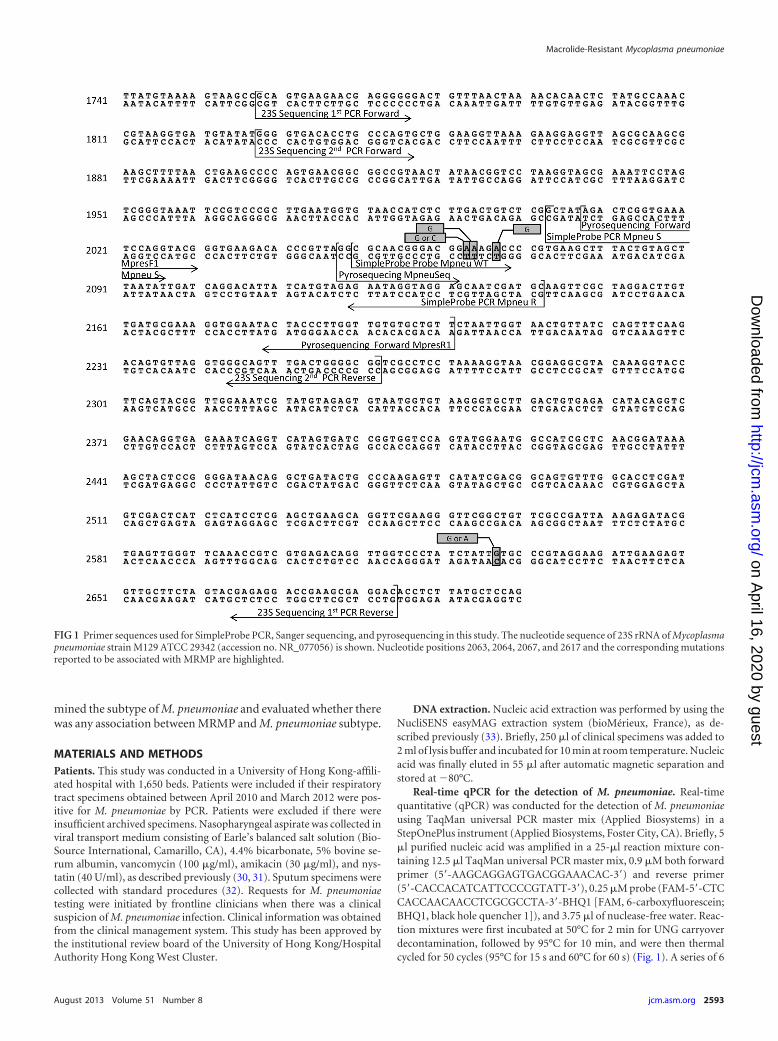
Real-time qPCR for the detection of M. pneumoniae. Real-timequantitative (qPCR) was conducted for the detection of M. pneumoniaeusing TaqMan universal PCR master mix (Applied Biosystems) in aStepOnePlus instrument (Applied Biosystems, Foster City, CA). Briefly, 5�l purified nucleic acid was amplified in a 25-�l reaction mixture con-taining 12.5 �l TaqMan universal PCR master mix, 0.9 �M both forwardprimer (5=-AAGCAGGAGTGACGGAAACAC-3=) and reverse primer(5=-CACCACATCATTCCCCGTATT-3=), 0.25 �M probe (FAM-5=-CTCCACCAACAACCTCGCGCCTA-3=-BHQ1 [FAM, 6-carboxyfluorescein;BHQ1, black hole quencher 1]), and 3.75 �l of nuclease-free water. Reac-tion mixtures were first incubated at 50°C for 2 min for UNG carryoverdecontamination, followed by 95°C for 10 min, and were then thermalcycled for 50 cycles (95°C for 15 s and 60°C for 60 s) (Fig. 1). A series of 6
FIG 1 Primer sequences used for SimpleProbe PCR, Sanger sequencing, and pyrosequencing in this study. The nucleotide sequence of 23S rRNA of Mycoplasmapneumoniae strain M129 ATCC 29342 (accession no. NR_077056) is shown. Nucleotide positions 2063, 2064, 2067, and 2617 and the corresponding mutationsreported to be associated with MRMP are highlighted.
Macrolide-Resistant Mycoplasma pneumoniae
August 2013 Volume 51 Number 8 jcm.asm.org 2593
on April 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

log10 dilutions equivalent to 1 � 101 to 1 � 106 copies per reaction mix-ture were prepared from a plasmid (pC-RII-TOPO vector; Invitrogen,CA) containing the corresponding target bacterial sequence to generatecalibration curves, and these were run in parallel with the test specimens.
Pyrosequencing. Pyrosequencing was performed using the PyroMarkPCR kit (Qiagen, Hilden, Germany) with forward primer MpresF1 (5=-AGACTCGGTGAAATCCAGGTACG-3=), the reverse biotinylated primerMpresR1 (5=-AACAGCACACAACCAAGGGTAGTA-biotin-3=), and thesequence primer MpresSeq (5=-AGGCGCAACGGGACG-3=). The PCRwas performed under the following conditions: 5 �l of nucleic acid ex-tract, 12.5 �l of PyroMark PCR master mix (2�), 2.5 �l of the primerF/primer R set (10�), and 5 �l of nuclease-free water. The total reactionmixture volume was 25 �l. The master mix was then transferred into athermal cycler GeneAmp PCR system 9700 (Applied Biosystems). Thecycling conditions were 10 min at 94°C followed by 45 cycles of 30 s at94°C, 30 s at 50°C, and 30 s at 72°C. The turnaround time was 87.5 min.The resulting biotinylated PCR products were immobilized to streptavi-din Sepharose high-performance beads (GE Healthcare) and then puri-fied using the PyroMark Q24 vacuum prep workstation. Finally, single-stranded DNA with a sequence primer was loaded into the PyroMark Q24instrument (Qiagen, Hilden, Germany). The data were then analyzed byPyroMark Q24 software.
PCR amplification and Sanger sequencing. Five microliters of thenucleic acid eluate was used for a first PCR amplification with 0.2 mMeach sense primer, 1758 (5=-GCAGTGAAGAACGAGGGG-3=, and anti-sense primer, 2684 (5=-GTCCTCGCTTCGGTCCTCTCG-3=), corre-sponding to the V domain of the 23S rRNA gene to amplify a 927-bpfragment, as described previously (15). Subsequently, 1 �l of the first PCRproduct was transferred to a second PCR tube for nested PCR using twoinner primers, 1719 (5=-TGGGGTGACACCTGCCCACT-3=) and 2154(5=-CCGCCCCAGTCAAACTGCCC-3=), which resulted in a 436-bpfragment. Amplification was performed for 45 cycles, consisting of a de-naturation step at 94°C for 30 s, an annealing step at 50°C for 30 s, and anextension step at 72°C for 30 s. The extension was continued at 72°C for 7min. The turnaround time was 98.75 min. The amplified DNA fragmentwas separated in a 2% agarose gel (Promega, Madison, WI). All positivePCR products from either the first or second nested PCRs were purifiedwith a QIAquick PCR purification kit (Qiagen, Hilden, Germany), ac-cording to the manufacturer’s protocol, and were sequenced in both di-rections with BigDye XTerminator version 1.1 (Applied Biosystems, CA)with corresponding specific primers and an ABI Prism 3100 genetic ana-lyzer (Applied Biosystems, NJ).
SimpleProbe real-time PCR coupled to melting curve analysis forMRMP detection. SimpleProbe real-time PCR coupled to melting curveanalysis (SimpleProbe PCR) was performed on the extracted nucleic acidfrom specimens to identify MRMP. The MRMP assay was done by usingthe LightCycler FastStart DNA master HybProbe kit (Roche Diagnostics,Germany) with the forward primer Mpneu S 5=-GCTATAGACTCGGTGAAATCCAGG-3=, reverse primer Mpneu R 5=-GCATCGATTGCTCCTACCTATTCT-3=, and probe Mpneu WT 5=-GCGCA XI ACGGGACGGAAAGAC–PH-3=, which were designed using LightCycler probe designsoftware 2.0. The PCR was performed using 5 �l nucleic acid, 2 �l Fast-Start DNA master 10�, 2 �l forward primer (1 �M), 2 �l reverse primer(5 �M), 2 �l probe (5 �M), 5.4 �l of nuclease-free water, and 1.6 �lMgCl2. The total reaction mixture volume was 20 �l. The master mix wasthen loaded in a LightCycler 2.0 instrument (Roche Diagnostics, Ger-many).
Cycling conditions were as follows: denaturation step of 10 min at95°C, amplification step of 45 cycles of 10 s at 95°C, 10 s at 55°C, and 15 sat 72°C, melting step of 20 s at 95°C, 20 s at 40°C, and a continuous raiseof temperature to 85°C at a 0.2°C ramp rate and a final cooling step of 30s at 40°C. Fluorescent signals were detected and analyzed with the Light-Cycler software 4.1 (Fig. 2). The turnaround time was 42 min.
Determination of detection limits of SimpleProbe PCR and pyrose-quencing. In order to determine the detection limits of SimpleProbe PCRand pyrosequencing for identification of mutations associated with mac-rolide resistance, two M. pneumoniae-positive patient specimens, onewild type (WT) and one mutant (with the transition A2063G), were di-luted with viral transport medium into batches of 104 copies/ml, 103 cop-ies/ml, 102 copies/ml, and 10 copies/ml. The viral transport medium isused routinely in our laboratory for the collection of nasopharyngeal as-pirate specimens (30, 31). These diluted specimens were then extracted byNucliSENS easyMAG and tested by SimpleProbe PCR and pyrosequencing.
Subtyping. For the subtyping of M. pneumoniae isolates, the MPN141(or P1) and MPN528a genes, using two sets of primers with modification,were examined as described previously (18). Briefly, the first set of primerswas forward primer 5=-TACGACTAGGAGATCATCAG-3= and reverseprimer 5=-TACGACTAGGAGATCATCCAG-3=,and the second set ofprimers was forward primer 5=-ATCTACCGATTCAACCAACTGCT andreverse primer GCTAACTGCGCTAGAGCAAAAT; these were used toamplify a 232-bp fragment of MPN141 and a 166-bp fragment ofMPN528a genes, respectively. The PCR amplification conditions of bothassays were the same: 5 min at 94°C, followed by 50 cycles of 10 s at 94°C,30 s at 55°C, and 30 s at 72°C. The PCR products were then followed bySanger sequencing as described earlier. For the MPN141 gene, a T is foundin subtype 1 strains and a C in subtype 2 strains at position 184991 in thegenomic sequence of M. pneumoniae strain M129. For the MPN528agene, an A in subtype 1 strains and a C in subtype 2 strains are found atposition 650584 of the M129 genome.
Statistical analysis. All statistical analysis was performed using PAWSStatistics version 18.0.0 for Windows. Chi-square and Mann-Whitney Utests were used to compare categorical and continuous variables, respec-tively. A P value of �0.05 was considered statistically significant.
RESULTSPrevalence of M. pneumoniae. During the study period, a total of653 respiratory specimens from 549 patients were investigated byreal-time PCR for the presence of M. pneumoniae. In spiking ex-periments, the limit of detection for the real-time qPCR was foundto be 440 DNA copies/ml of clinical specimen (10 DNA copies/reaction mixture). Overall, 17.5% (96/549) of the patients, includ-ing 15.3% (100/653) of the specimens, were positive for M. pneu-moniae. The M. pneumoniae-positive rate was highest amongchildren aged 2 to 11 years (30.1%), then in infants aged 0 to 1 year(18.1%) and teenagers aged 12 to 17 years (18.6%); it was lowest inadults aged 18 to 64 years (7.5%) and seniors aged �65 years(1.6%) (P � 0.001).
The specimens for five patients were not investigated furtherbecause of insufficient amounts of specimen (n � 2) or unavail-ability of the medical records (n � 3). Therefore, 91 M. pneu-moniae PCR-positive specimens (86 nasopharyngeal and five spu-tum specimens), originating from 91 patients, were analyzedfurther. The 91 patients had a median age of 6 years (range, 3months to 92 years). Eleven (12.1%) were adult patients aged �18years, and 41 (45.1%) were female patients.
Macrolides were prescribed for 78 (85.7%) patients, of whom15 patients were subsequently changed to tetracycline or fluoro-quinolone antibiotics.
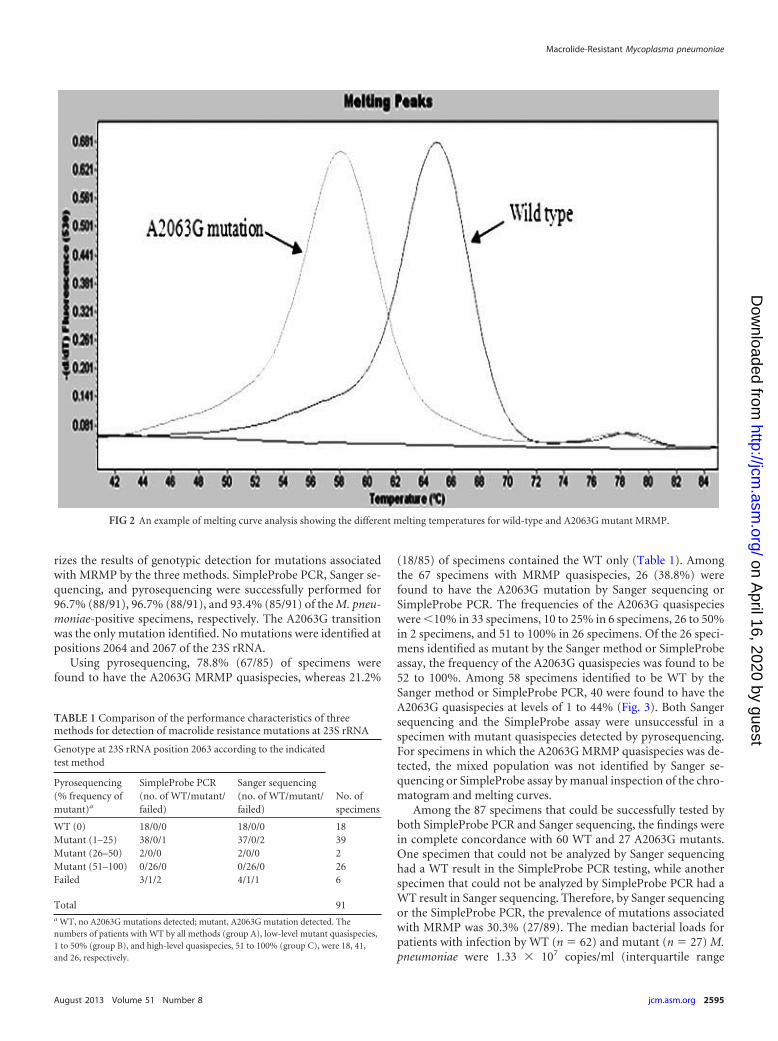
Evaluation of SimpleProbe PCR. SimpleProbe PCR showedthat amplicons from wild-type (WT) 23S rRNA exhibit a mean Tm
of 64.96°C (range, 64.01 to 65.25°C), whereas those from 23SrRNA with the mutation A2063G showed a mean Tm of 58.21°C(range, 57.73 to 58.56°C) (Fig. 2). The detection limits ofSimpleProbe PCR and pyrosequencing for both the WT and mu-tant were 103 copies/ml and 104 copies/ml, respectively.
Prevalence of macrolide-resistant genotype. Table 1 summa-
Chan et al.
2594 jcm.asm.org Journal of Clinical Microbiology
on April 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
rizes the results of genotypic detection for mutations associatedwith MRMP by the three methods. SimpleProbe PCR, Sanger se-quencing, and pyrosequencing were successfully performed for96.7% (88/91), 96.7% (88/91), and 93.4% (85/91) of the M. pneu-moniae-positive specimens, respectively. The A2063G transitionwas the only mutation identified. No mutations were identified atpositions 2064 and 2067 of the 23S rRNA.
Using pyrosequencing, 78.8% (67/85) of specimens werefound to have the A2063G MRMP quasispecies, whereas 21.2%
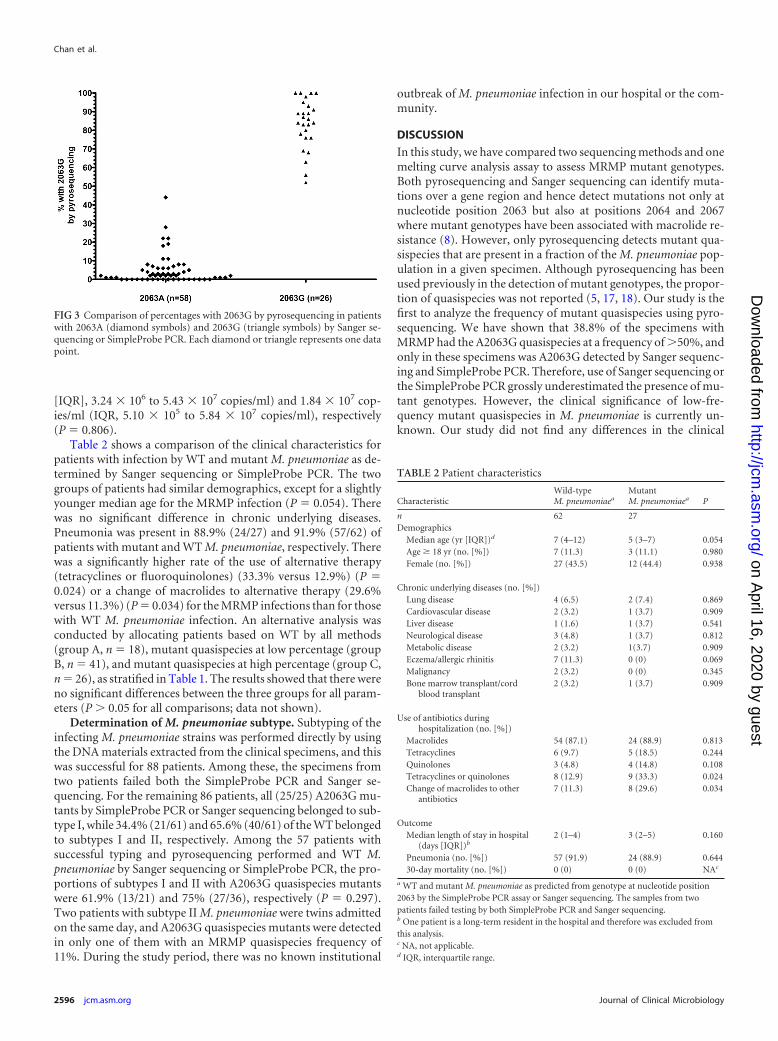
(18/85) of specimens contained the WT only (Table 1). Amongthe 67 specimens with MRMP quasispecies, 26 (38.8%) werefound to have the A2063G mutation by Sanger sequencing orSimpleProbe PCR. The frequencies of the A2063G quasispecieswere �10% in 33 specimens, 10 to 25% in 6 specimens, 26 to 50%in 2 specimens, and 51 to 100% in 26 specimens. Of the 26 speci-mens identified as mutant by the Sanger method or SimpleProbeassay, the frequency of the A2063G quasispecies was found to be52 to 100%. Among 58 specimens identified to be WT by theSanger method or SimpleProbe PCR, 40 were found to have theA2063G quasispecies at levels of 1 to 44% (Fig. 3). Both Sangersequencing and the SimpleProbe assay were unsuccessful in aspecimen with mutant quasispecies detected by pyrosequencing.For specimens in which the A2063G MRMP quasispecies was de-tected, the mixed population was not identified by Sanger se-quencing or SimpleProbe assay by manual inspection of the chro-matogram and melting curves.
Among the 87 specimens that could be successfully tested byboth SimpleProbe PCR and Sanger sequencing, the findings werein complete concordance with 60 WT and 27 A2063G mutants.One specimen that could not be analyzed by Sanger sequencinghad a WT result in the SimpleProbe PCR testing, while anotherspecimen that could not be analyzed by SimpleProbe PCR had aWT result in Sanger sequencing. Therefore, by Sanger sequencingor the SimpleProbe PCR, the prevalence of mutations associatedwith MRMP was 30.3% (27/89). The median bacterial loads forpatients with infection by WT (n � 62) and mutant (n � 27) M.pneumoniae were 1.33 � 107 copies/ml (interquartile range
FIG 2 An example of melting curve analysis showing the different melting temperatures for wild-type and A2063G mutant MRMP.
TABLE 1 Comparison of the performance characteristics of threemethods for detection of macrolide resistance mutations at 23S rRNA
Genotype at 23S rRNA position 2063 according to the indicatedtest method
No. ofspecimens
Pyrosequencing(% frequency ofmutant)a
SimpleProbe PCR(no. of WT/mutant/failed)
Sanger sequencing(no. of WT/mutant/failed)
WT (0) 18/0/0 18/0/0 18Mutant (1–25) 38/0/1 37/0/2 39Mutant (26–50) 2/0/0 2/0/0 2Mutant (51–100) 0/26/0 0/26/0 26Failed 3/1/2 4/1/1 6
Total 91a WT, no A2063G mutations detected; mutant, A2063G mutation detected. Thenumbers of patients with WT by all methods (group A), low-level mutant quasispecies,1 to 50% (group B), and high-level quasispecies, 51 to 100% (group C), were 18, 41,and 26, respectively.
Macrolide-Resistant Mycoplasma pneumoniae
August 2013 Volume 51 Number 8 jcm.asm.org 2595
on April 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from
[IQR], 3.24 � 106 to 5.43 � 107 copies/ml) and 1.84 � 107 cop-ies/ml (IQR, 5.10 � 105 to 5.84 � 107 copies/ml), respectively(P � 0.806).
Table 2 shows a comparison of the clinical characteristics forpatients with infection by WT and mutant M. pneumoniae as de-termined by Sanger sequencing or SimpleProbe PCR. The twogroups of patients had similar demographics, except for a slightlyyounger median age for the MRMP infection (P � 0.054). Therewas no significant difference in chronic underlying diseases.Pneumonia was present in 88.9% (24/27) and 91.9% (57/62) ofpatients with mutant and WT M. pneumoniae, respectively. Therewas a significantly higher rate of the use of alternative therapy(tetracyclines or fluoroquinolones) (33.3% versus 12.9%) (P �0.024) or a change of macrolides to alternative therapy (29.6%versus 11.3%) (P � 0.034) for the MRMP infections than for thosewith WT M. pneumoniae infection. An alternative analysis wasconducted by allocating patients based on WT by all methods(group A, n � 18), mutant quasispecies at low percentage (groupB, n � 41), and mutant quasispecies at high percentage (group C,n � 26), as stratified in Table 1. The results showed that there wereno significant differences between the three groups for all param-eters (P � 0.05 for all comparisons; data not shown).
Determination of M. pneumoniae subtype. Subtyping of theinfecting M. pneumoniae strains was performed directly by usingthe DNA materials extracted from the clinical specimens, and thiswas successful for 88 patients. Among these, the specimens fromtwo patients failed both the SimpleProbe PCR and Sanger se-quencing. For the remaining 86 patients, all (25/25) A2063G mu-tants by SimpleProbe PCR or Sanger sequencing belonged to sub-type I, while 34.4% (21/61) and 65.6% (40/61) of the WT belongedto subtypes I and II, respectively. Among the 57 patients withsuccessful typing and pyrosequencing performed and WT M.pneumoniae by Sanger sequencing or SimpleProbe PCR, the pro-portions of subtypes I and II with A2063G quasispecies mutantswere 61.9% (13/21) and 75% (27/36), respectively (P � 0.297).Two patients with subtype II M. pneumoniae were twins admittedon the same day, and A2063G quasispecies mutants were detectedin only one of them with an MRMP quasispecies frequency of11%. During the study period, there was no known institutional
outbreak of M. pneumoniae infection in our hospital or the com-munity.
DISCUSSION
In this study, we have compared two sequencing methods and onemelting curve analysis assay to assess MRMP mutant genotypes.Both pyrosequencing and Sanger sequencing can identify muta-tions over a gene region and hence detect mutations not only atnucleotide position 2063 but also at positions 2064 and 2067where mutant genotypes have been associated with macrolide re-sistance (8). However, only pyrosequencing detects mutant qua-sispecies that are present in a fraction of the M. pneumoniae pop-ulation in a given specimen. Although pyrosequencing has beenused previously in the detection of mutant genotypes, the propor-tion of quasispecies was not reported (5, 17, 18). Our study is thefirst to analyze the frequency of mutant quasispecies using pyro-sequencing. We have shown that 38.8% of the specimens withMRMP had the A2063G quasispecies at a frequency of �50%, andonly in these specimens was A2063G detected by Sanger sequenc-ing and SimpleProbe PCR. Therefore, use of Sanger sequencing orthe SimpleProbe PCR grossly underestimated the presence of mu-tant genotypes. However, the clinical significance of low-fre-quency mutant quasispecies in M. pneumoniae is currently un-known. Our study did not find any differences in the clinical
FIG 3 Comparison of percentages with 2063G by pyrosequencing in patientswith 2063A (diamond symbols) and 2063G (triangle symbols) by Sanger se-quencing or SimpleProbe PCR. Each diamond or triangle represents one datapoint.
TABLE 2 Patient characteristics
CharacteristicWild-typeM. pneumoniaea
MutantM. pneumoniaea P
n 62 27Demographics
Median age (yr [IQR])d 7 (4–12) 5 (3–7) 0.054Age � 18 yr (no. [%]) 7 (11.3) 3 (11.1) 0.980Female (no. [%]) 27 (43.5) 12 (44.4) 0.938
Chronic underlying diseases (no. [%])Lung disease 4 (6.5) 2 (7.4) 0.869Cardiovascular disease 2 (3.2) 1 (3.7) 0.909Liver disease 1 (1.6) 1 (3.7) 0.541Neurological disease 3 (4.8) 1 (3.7) 0.812Metabolic disease 2 (3.2) 1(3.7) 0.909Eczema/allergic rhinitis 7 (11.3) 0 (0) 0.069Malignancy 2 (3.2) 0 (0) 0.345Bone marrow transplant/cord
blood transplant2 (3.2) 1 (3.7) 0.909
Use of antibiotics duringhospitalization (no. [%])
Macrolides 54 (87.1) 24 (88.9) 0.813Tetracyclines 6 (9.7) 5 (18.5) 0.244Quinolones 3 (4.8) 4 (14.8) 0.108Tetracyclines or quinolones 8 (12.9) 9 (33.3) 0.024Change of macrolides to other
antibiotics7 (11.3) 8 (29.6) 0.034
OutcomeMedian length of stay in hospital
(days [IQR])b2 (1–4) 3 (2–5) 0.160
Pneumonia (no. [%]) 57 (91.9) 24 (88.9) 0.64430-day mortality (no. [%]) 0 (0) 0 (0) NAc
a WT and mutant M. pneumoniae as predicted from genotype at nucleotide position2063 by the SimpleProbe PCR assay or Sanger sequencing. The samples from twopatients failed testing by both SimpleProbe PCR and Sanger sequencing.b One patient is a long-term resident in the hospital and therefore was excluded fromthis analysis.c NA, not applicable.d IQR, interquartile range.
Chan et al.
2596 jcm.asm.org Journal of Clinical Microbiology
on April 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

characteristics between patients with low-frequency quasispeciesand those without quasispecies. Low-frequency antiviral-resistantmutant quasispecies have been shown to enrich during antiviraltherapy for influenza virus (34, 35), hepatitis B virus (36), hepati-tis C virus (37), and HIV infection (25). Recently, it has beenshown that MRMP can emerge during macrolide therapy (29, 38,39), and it remains to be determined whether mutant quasispecieswere already present in those cases before treatment.
Although sequencing techniques are powerful, they are usuallynot feasible for routine clinical practice because they are relativelytime-consuming and expensive. Therefore, we have developedand evaluated a rapid SimpleProbe PCR. Our findings showedthat the assay performance in terms of sensitivity and specificity issimilar to that of direct PCR followed by sequencing. Since themutant genotype A2063G is situated in an area of the 23S rRNAwith many high-binding secondary structures, we have designed aSimpleProbe probe that covered a short region, thereby improv-ing the chance of successful probe hybridization. As demonstratedby the melting curve analysis, the WT genotype could be readilydifferentiated from the mutant genotype. In addition, the limit ofdetection of SimpleProbe PCR was found to be one log lower thanthat for sequencing. The assay can be performed in conventionalreal-time thermocyclers that are now available in many clinicallaboratories. Sequencing facilities are not needed. The turnaroundtime (42 min) is short compared to that for PCR-Sanger sequenc-ing (1 to 2 days). All these make the Simple Probe assay an attrac-tive method for the rapid diagnosis of MRMP. Other groups havereported the use of high-resolution melting curve analysis to de-termine mutations associated with MRMP, but special equipmentis required for those (20).
In our study, patients with the A2063G mutation detected bySimpleProbe PCR or Sanger sequencing were more likely to re-quire a change from macrolides to fluoroquinolones or tetracy-clines for therapy, indicating that there was poor clinical responsefor macrolides. This is consistent with previous studies showingthe inferiority of macrolides in patients with this mutant genotype(8, 10). The detection of this mutant phenotype would be espe-cially important for patients who have more-severe clinical pre-sentations (14).
We did not find any statistically significant differences betweenthe rates of macrolide resistance in children and adults. This issimilar to the results reported from China (5) but in contrast toprevious studies from other countries, in which the adult popula-tion has a lower prevalence of MRMP than do children or adoles-cents (16, 40, 41). This may be related to the frequent travel be-tween Hong Kong and mainland China.
In a single outbreak, MRMP has been found to belong to asingle clonal group (12), but in the community, MRMP has ap-peared to be polyclonal using multilocus variable-number tan-dem-repeat analysis (42–45). In our study, all MRMP organismsbelonged to subtype I. This is similar to the situation reported inchildren from Shanghai, China, in which �80% of the resistantstrains belong to subtype I, while �15% belong to subtype II (46,47). Among patients with low frequencies of quasispecies, therewas no significant difference between subtypes I and II.
There are several limitations to our study. First, our sequencingdoes not cover mutations at position 2617. Previous studies haveshown that C2617A or C2617G mutations confer resistance tomacrolides, but the MIC due to mutation at the 2617 position isfar lower than that at position 2063 (15). Second, since M. pneu-
moniae culture was not performed, we were not able to determinethe MIC of the MRMP. Third, this is a retrospective study with arelatively small number of patients. A small difference betweenpatients with no mutant quasispecies and those with low-fre-quency mutant quasispecies could not be detected.
The prevalence of mutant genotypes far exceeded that whichcan be detected by conventional sequencing. Currently, there areinsufficient data on the clinical and public health significance oflow-frequency mutant quasispecies that can be detected only bypyrosequencing. Future studies would be necessary to understandthe changes in the frequency of mutant quasispecies in patientsrequiring macrolide therapy.
ACKNOWLEDGMENTS
This study is funded by research grants from the Queen Mary Hospitalcharitable trust training and research assistance scheme TRAS-11-04, theResearch Fund for the Control of Infectious Diseases, Health and FoodBureau, Hong Kong Special Administrative Region, and the National Sci-ence and Technology Major Project of China (grant no. 2012ZX10004-213-002).
REFERENCES1. Klapdor B, Ewig S, Pletz MW, Rohde G, Schütte H, Schaberg T, Welte
T, CAPNETZ Study Group. 2012. Community-acquired pneumonia inyounger patients is an entity on its own. Eur. Respir. J. 39:1156 –1161.
2. Stuckey-Schrock K, Hayes BL, George CM. 2012. Community-acquiredpneumonia in children. Am. Fam. Physician 86:661– 667.
3. Johansson N, Kalin M, Tiveljung-Lindell A, Giske CG, Hedlund J. 2010.Etiology of community-acquired pneumonia: increased microbiologicalyield with new diagnostic methods. Clin. Infect. Dis. 50:202–209.
4. Duffy LB, Crabb D, Searcey K, Kempf MC. 2000. Comparativepotency of gemifloxacin, new quinolones, macrolides, tetracycline andclindamycin against Mycoplasma spp. J. Antimicrob. Chemother.45(Suppl 1):29 –33.
5. Cao B, Zhao CJ, Yin YD, Zhao F, Song SF, Bai L, Zhang JZ, Liu YM,Zhang YY, Wang H, Wang C. 2010. High prevalence of macrolideresistance in Mycoplasma pneumoniae isolates from adult and adolescentpatients with respiratory tract infection in China. Clin. Infect. Dis. 51:189 –194.
6. Chironna M, Sallustio A, Esposito S, Perulli M, Chinellato I, Di Bari C,Quarto M, Cardinale F. 2011. Emergence of macrolide-resistant strainsduring an outbreak of Mycoplasma pneumoniae infections in children. J.Antimicrob. Chemother. 66:734 –737.
7. Yamada M, Buller R, Bledsoe S, Storch GA. 2012. Rising rates of mac-rolide-resistant Mycoplasma pneumoniae in the central United States. Pe-diatr. Infect. Dis. J. 31:409 – 410.
8. Morozumi M, Takahashi T, Ubukata K. 2010. Macrolide-resistant My-coplasma pneumoniae: characteristics of isolates and clinical aspects ofcommunity-acquired pneumonia. J. Infect. Chemother. 16:78 – 86.
9. Zhao F, Liu G, Wu J, Cao B, Tao X, He L, Meng F, Zhu L, Lv M, YinY, Zhang J. 2013. Surveillance of macrolide-resistant Mycoplasma pneu-moniae in Beijing, China, from 2008 to 2012. Antimicrob. Agents Che-mother. 57:1521–1523.
10. Principi N, Esposito S. 2013. Macrolide-resistant Mycoplasma pneu-moniae: its role in respiratory infection. J. Antimicrob. Chemother. 68:506 –511.
11. Lung DC, Chan YH, Kwong L, Que TL. 2011. Severe community-acquired pneumonia caused by macrolide-resistant Mycoplasma pneu-moniae in a 6-year-old boy. Hong Kong Med. J. 17:407– 409.
12. Wang Y, Qiu S, Yang G, Song L, Su W, Xu Y, Jia L, Wang L, Hao R,Zhang C, Liu J, Fu X, He J, Zhang J, Li Z, Song H. 2012. An outbreakof Mycoplasma pneumoniae caused by a macrolide-resistant isolate in anursery school in China. Antimicrob. Agents Chemother. 56:3748 –3752.
13. Suzuki Y, Itagaki T, Seto J, Kaneko A, Abiko C, Mizuta K, Matsuzaki Y.2012. Community outbreak of macrolide-resistant Mycoplasma pneu-moniae in Yamagata, Japan in 2009. Pediatr. Infect. Dis. J. 32:237–240.
14. To KKW, Chan KH, Fung YF, Yuen KY, Ho PL. 2010. Azithromycintreatment failure in macrolide-resistant Mycoplasma pneumoniae pneu-monia. Eur. Respir. J. 36:969 –971.
Macrolide-Resistant Mycoplasma pneumoniae
August 2013 Volume 51 Number 8 jcm.asm.org 2597
on April 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from

15. Lucier TS, Heitzman K, Liu SK, Hu PC. 1995. Transition mutations inthe 23S rRNA of erythromycin-resistant isolates of Mycoplasma pneu-moniae. Antimicrob. Agents Chemother. 39:2770 –2773.
16. Yoo SJ, Kim HB, Choi SH, Lee SO, Kim SH, Hong SB, Sung H, KimMN. 2012. Differences in the frequency of 23S rRNA gene mutations inMycoplasma pneumoniae between children and adults with community-acquired pneumonia: clinical impact of mutations conferring macrolideresistance. Antimicrob. Agents Chemother. 56:6393– 6396.
17. Spuesens EB, Meijer A, Bierschenk D, Hoogenboezem T, Donker GA,Hartwig NG, Koopmans MP, Vink C, van Rossum AM. 2012. Macrolideresistance determination and molecular typing of Mycoplasma pneu-moniae in respiratory specimens collected between 1997 and 2008 in theNetherlands. J. Clin. Microbiol. 50:1999 –2004.
18. Spuesens EB, Hoogenboezem T, Sluijter M, Hartwig NG, van RossumAM, Vink C. 2010. Macrolide resistance determination and moleculartyping of Mycoplasma pneumoniae by pyrosequencing. J. Microbiol.Methods 82:214 –222.
19. Wolff BJ, Thacker WL, Schwartz SB, Winchell JM. 2008. Detection ofmacrolide resistance in Mycoplasma pneumoniae by real-time PCR andhigh-resolution melt analysis. Antimicrob. Agents Chemother. 52:3542–3549.
20. Peuchant O, Ménard A, Renaudin H, Morozumi M, Ubukata K, BébéarCM, Pereyre S. 2009. Increased macrolide resistance of Mycoplasma pneu-moniae in France directly detected in clinical specimens by real-time PCRand melting curve analysis. J. Antimicrob. Chemother. 64:52–58.
21. Li X, Atkinson TP, Hagood J, Makris C, Duffy LB, Waites KB. 2009.Emerging macrolide resistance in Mycoplasma pneumoniae in children:detection and characterization of resistant isolates. Pediatr. Infect. Dis. J.28:693– 696.
22. Li SL, Sun HM, Zhao HQ, Cao L, Yuan Y, Feng YL, Xue GH. 2012. Asingle tube modified allele-specific-PCR for rapid detection of erythromy-cin-resistant Mycoplasma pneumoniae in Beijing. Chin. Med. J. (Engl.)125:2671–2676.
23. Matsuoka M, Narita M, Okazaki N, Ohya H, Yamazaki T, Ouchi K,Suzuki I, Andoh T, Kenri T, Sasaki Y, Horino A, Shintani M, ArakawaY, Sasaki T. 2004. Characterization and molecular analysis of macrolide-resistant Mycoplasma pneumoniae clinical isolates obtained in Japan. An-timicrob. Agents Chemother. 48:4624 – 4630.
24. Lindström A, Odeberg J, Albert J. 2004. Pyrosequencing for detection oflamivudine-resistant hepatitis B virus. J. Clin. Microbiol. 42:4788 – 4795.
25. Armenia D, Vandenbroucke I, Fabeni L, Van Marck H, Cento V,D’Arrigo R, Van Wesenbeeck L, Scopelliti F, Micheli V, Bruzzone B, LoCaputo S, Aerssens J, Rizzardini G, Tozzi V, Narciso P, Antinori A,Stuyver L, Perno CF, Ceccherini-Silberstein F. 2012. Study of genotypicand phenotypic HIV-1 dynamics of integrase mutations during raltegravirtreatment: a refined analysis by ultra-deep 454 pyrosequencing. J. Infect.Dis. 205:557–567.
26. Mello FC, Lago BV, Lewis-Ximenez LL, Fernandes CA, Gomes SA.2012. Detection of mixed populations of wild-type and YMDD hepatitis Bvariants by pyrosequencing in acutely and chronically infected patients.BMC Microbiol. 12:96. doi:10.1186/1471-2180-12-96.
27. Newman RM, Kuntzen T, Weiner B, Berical A, Charlebois P, KuikenC, Murphy DG, Simmonds P, Bennett P, Lennon NJ, Birren BW,Zody MC, Allen TM, Henn MR. 2013. Whole genome pyrosequenc-ing of rare hepatitis C virus genotypes enhances subtype classificationand identification of naturally occurring drug resistance variants. J.Infect. Dis. 208:17–31.
28. Arvia R, Corcioli F, Simi L, Orlando C, De Santis R, Facchini M,Donatelli I, Azzi A. 2012. Monitoring the susceptibility to oseltamivir ofinfluenza A(H1N1) 2009 virus by nested-PCR and pyrosequencing duringthe pandemic and in the season 2010 –2011. J. Virol. Methods 184:113–116.
29. Averbuch D, Hidalgo-Grass C, Moses AE, Engelhard D, Nir-Paz R.2011. Macrolide resistance in Mycoplasma pneumoniae, Israel, 2010.Emerg. Infect. Dis. 17:1079 –1082.
30. Hung IF, Cheng VC, Wu AK, Tang BS, Chan KH, Chu CM, Wong MM,Hui WT, Poon LL, Tse DM, Chan KS, Woo PC, Lau SK, Peiris JS, YuenKY. 2004. Viral loads in clinical specimens and SARS manifestations.Emerg. Infect. Dis. 10:1550 –1557.
31. To KK, Wong SC, Xu T, Poon RW, Mok KY, Chan JF, Cheng VC, Chan
KH, Hung IF, Yuen KY. 2013. Use of nasopharyngeal aspirate for diag-nosis of pneumocystis pneumonia. J. Clin. Microbiol. 51:1570 –1574.
32. Versalovic J, Funke G, Landry ML, Warnock DW. 2011. Manual ofclinical microbiology, 11th ed. ASM Press, Washington, DC.
33. Hung IF, To KK, Lee CK, Lee KL, Yan WW, Chan K, Chan WM, NgaiCW, Law KI, Chow FL, Liu R, Lai KY, Lau CC, Liu SH, Chan KH, LinCK, Yuen KY. 2013. Hyperimmune intravenous immunoglobulin treat-ment: a multicentre double-blind randomized controlled trial for patientswith severe A(H1N1)pdm09 infection. Chest doi:10.1378/chest.12-2907.
34. Nguyen HT, Trujillo AA, Sheu TG, Levine M, Mishin VP, Shaw M,Ades EW, Klimov AI, Fry AM, Gubareva LV. 2012. Analysis of influenzaviruses from patients clinically suspected of infection with an oseltamivirresistant virus during the 2009 pandemic in the United States. AntiviralRes. 93:381–386.
35. Chen N, Pinsky BA, Lee BP, Lin M, Schrijver I. 2011. Ultrasensitivedetection of drug-resistant pandemic 2009 (H1N1) influenza A virus byrare-variant-sensitive high-resolution melting-curve analysis. J. Clin. Mi-crobiol. 49:2602–2609.
36. Nishijima N, Marusawa H, Ueda Y, Takahashi K, Nasu A, Osaki Y,Kou T, Yazumi S, Fujiwara T, Tsuchiya S, Shimizu K, Uemoto S,Chiba T. 2012. Dynamics of hepatitis B virus quasispecies in associa-tion with nucleos(t)ide analogue treatment determined by ultra-deepsequencing. PLoS One 7:e35052. doi:10.1371/journal.pone.0035052.
37. Kuntzen T, Timm J, Berical A, Lennon N, Berlin AM, Young SK, Lee B,Heckerman D, Carlson J, Reyor LL, Kleyman M, McMahon CM, BirchC, Schulze Zur Wiesch J, Ledlie T, Koehrsen M, Kodira C, Roberts AD,Lauer GM, Rosen HR, Bihl F, Cerny A, Spengler U, Liu Z, Kim AY,Xing Y, Schneidewind A, Madey MA, Fleckenstein JF, Park VM, Gala-gan JE, Nusbaum C, Walker BD, Lake-Bakaar GV, Daar ES, JacobsonIM, Gomperts ED, Edlin BR, Donfield SM, Chung RT, Talal AH,Marion T, Birren BW, Henn MR, Allen TM. 2008. Naturally occurringdominant resistance mutations to hepatitis C virus protease and polymer-ase inhibitors in treatment-naive patients. Hepatology 48:1769 –1778.
38. Cardinale F, Chironna M, Dumke R, Binetti A, Daleno C, Sallustio A,Valzano A, Esposito S. 2011. Macrolide-resistant Mycoplasma pneu-moniae in paediatric pneumonia. Eur. Respir. J. 37:1522–1524.
39. Itagaki T, Suzuki Y, Seto J, Abiko C, Mizuta K, Matsuzaki Y. 2013. Twocases of macrolide resistance in Mycoplasma pneumoniae acquired duringthe treatment period. J. Antimicrob. Chemother. 68:724 –725.
40. Miyashita N, Kawai Y, Akaike H, Ouchi K, Hayashi T, Kurihara T,Okimoto N, Atypical Pathogen Study Group. 2012. Macrolide-resistantMycoplasma pneumoniae in adolescents with community-acquired pneu-monia. BMC Infect. Dis. 12:126. doi:10.1186/1471-2334-12-126.
41. Miyashita N, Oka M, Atypical Pathogen Study Group, Kawai Y, Yama-guchi T, Ouchi K. 2010. Macrolide-resistant Mycoplasma pneumoniae inadults with community-acquired pneumonia. Int. J. Antimicrob. Agents36:384 –385.
42. Liu Y, Ye X, Zhang H, Xu X, Wang M. 2012. Multiclonal origin ofmacrolide-resistant Mycoplasma pneumoniae isolates as determined bymultilocus variable-number tandem-repeat analysis. J. Clin. Microbiol.50:2793–2795.
43. Benitez AJ, Diaz MH, Wolff BJ, Pimentel G, Njenga MK, Estevez A,Winchell JM. 2012. Multilocus variable-number tandem-repeat analysisof Mycoplasma pneumoniae clinical isolates from 1962 to the present: aretrospective study. J. Clin. Microbiol. 50:3620 –3626.
44. Pereyre S, Charron A, Hidalgo-Grass C, Touati A, Moses AE, Nir-PazR, Bébéar C. 2012. The spread of Mycoplasma pneumoniae is polyclonal inboth an endemic setting in France and in an epidemic setting in Israel.PLoS One 7:e38585. doi:10.1371/journal.pone.0038585.
45. Pereyre S, Touati A, Petitjean-Lecherbonnier J, Charron A, Vabret A,Bébéar C. 2013. The increased incidence of Mycoplasma pneumoniae inFrance in 2011 was polyclonal, mainly involving M. pneumoniae type 1strains. Clin. Microbiol. Infect. 19:E212–E217. doi:10.1111/1469-0691.12107.
46. Liu Y, Ye X, Zhang H, Xu X, Li W, Zhu D, Wang M. 2010. Character-ization of macrolide resistance in Mycoplasma pneumoniae isolated fromchildren in Shanghai, China. Diagn. Microbiol. Infect. Dis. 67:355–358.
47. Liu Y, Ye X, Zhang H, Xu X, Li W, Zhu D, Wang M. 2009. Antimi-crobial susceptibility of Mycoplasma pneumoniae isolates and molecularanalysis of macrolide-resistant strains from Shanghai, China. Antimicrob.Agents Chemother. 53:2160 –2162.
Chan et al.
2598 jcm.asm.org Journal of Clinical Microbiology
on April 16, 2020 by guest
http://jcm.asm
.org/D
ownloaded from





























