Embed Size (px)
DESCRIPTION
dengeu shock syndrome
Citation preview

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
The ne w engl and
journal of medicineestablished in 1812 september 1 , 2005 vol. 353 no. 9
Perbandingan 3 Jenis Larutan Infus Untuk Resusitasi Pada Sindrom Syok Dengue
Bridget A. Wills, M.R.C.P., Nguyen M. Dung, M.D., Ha T. Loan, M.D., Dong T.H. Tam, M.D., Tran T.N. Thuy, M.D., Le T.T. Minh, M.D., Tran V. Diet, M.D., Nguyen T. Hao, M.D., Nguyen V. Chau, M.D., Kasia Stepniewska,
Ph.D., Nicholas J. White, F.R.C.P., and Jeremy J. Farrar, F.R.C.P.
Abstrak
LatarbelakangSindrom Syok Dengue Ditandai dengan kebocoran plasma berat serta gangguan hemostasis, kematian terjadi pada 1 sampai 5 persen kasus. Walaupun resusitasi cairan merupakan terapi pilihan utama namun WHO lebih menganjurkan terapi empiris disbanding terapi berdasarkan evidence based.
MetodeJurnal ini memilih metode double blind dengan membandingkan 3 jenis cairan resusitasi yang diberikan pada anak dari Negara Vietnam dengan sindrom syok dengue. Kami memilih 383 anak dengan sindrom syok dari tingkatan sedang hingga berat untuk mendapat cairan resusitasi Ringer Laktat, 6 persen dextran 70 (koloid) atau 6 persen hydroxyethyl starch (koloid) dan 129 anak dengan syok berat untuk menerima 1 koloid. Penilaian dilakukan setelah pasien mendapatkan cairan koloid.
HasilHanya 1 orang yang meninggal (angka mortalitas <0.2 persen). Hasil awal yang dinilai adalah dari relative risk pada pasien yang mendapat ringer laktat yaitu 1.08 (95 percent con- fidence interval, 0.78 to 1.47; P = 0.65). Pada anak yang mendapat cairan dekstran relative risk nya adalah 1.13 (95 per- cent confidence interval, 0.74 to 1.74; P = 0.59) dan pada anak yang mendapat HES relative risknya adalah 0.88 (95 percent confi- dence interval, 0.66 to 1.17; P=0.38). Biarpun terapi dengan menggunakan Ringer laktat menghasilkan peningkatan hematokrit yang tidak signifikan dan memiliki waktu pemulihan yang lebih lama dibandingkan cairan lain namun ringer laktat memiliki efek samping yang minimal dibandingkan dengan 2 cairan lain. Efek samping dapat berupa pendarahan, kelainan koagulasi darah dan kelebihan cairann..
Kesimpulan
Resusitasi awal dengan menggunakan ringer laktat dipergunakan pada anak dengan sindrom syok dengue dengan tingkatan sedang hingga berat. Dextran 70 dan 6 persen hydroxyethyl starch memiliki efek terapi yang sama namun hydroxyethyl starch memiliki efek samping minimal sehingga menjadi terapi cairan terpilih.
From the Oxford University Clinical Re- search Unit, Hospital for Tropical Dis- eases, Ho Chi Minh City, Vietnam, and the Centre for Clinical Vaccinology and Tropi- cal Medicine, Oxford University, Oxford, United Kingdom (B.A.W., K.S., N.J.W., J.J.F.); and the Hospital for Tropical Dis- eases, Ho Chi Minh City, Vietnam (N.M.D., H.T.L., D.T.H.T., T.T.N.T., L.T.T.M., T.V.D., N.T.H., N.V.C.). Address reprint requests to Dr. Wills at Oxford University Clinical Research Unit, Hospital for Tropical Dis- eases, 190 Ben Ham Tu, Quan 5, Ho Chi Minh City, Vietnam, or at bridgetw@hcm. vnn.vn.
N Engl J Med 2005;353:877-89.Copyright © 2005 Massachusetts Medical Society.
n engl j med 353;9 www.nejm.org september 1, 2005 877

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
Dengue shock syndrome adalah manifestasi paling serius dari demam berdarah dengue, yang telah menyebar semakin luas melalui Asia dan Amerika Selatan. Kejadian pertama kali muncul sejak yang pertama muncul-terorganisir di Bangkok, Thailand, di 1950s.1 dicirikan oleh kebocoran vascular sistemik dan kegagalan hemostasis dan dapat mengembangkan setelah infeksi dengan salah satu dari empat serotypes.2 virus dengue , 3 antara 250.000 dan 500.000 kasus demam berdarah dengue, terutama pada anak-anak, yang dilaporkan untuk organisasi kesehatan dunia (WHO) per tahun, dengan angka kematian dari 1 sampai 5 persen antara pasien dengan shock.1,4 pathophysio – patofisiologi yang mendasari kebocoran-usia pembuluh darah dan koagulopati yang kurang dipahami, dan tidak ada pengobatan khusus juga tersedia. Hanya dua percobaan acak dan buta yang telah menyelidiki efek kristaloid yang berbeda dan rejimen cairan koloid pada hasil dari dengue shock syndrome. Yang pertama, studi di mana
50 anak menerima salah satu dari empat cairan (6 persen dextran 70, 3 persen gelatin, Ringer laktat, atau 0,9 persen garam) selama dua jam untuk inisiasi esensial resusitasi, menunjukkan bahwa ada perbaikan secara signifikan lebih besar dalam indeks jantung, matocrit dia-, dan tekanan darah pada akhir infus cairan studi di kalangan anak-anak yang memiliki menerima solusi koloid dibandingkan mereka yang telah menerima solution. 12 kristaloid Semua anak-anak pulih, tetapi perbedaan efek berkelanjutan antara empat cairan tidak diperiksa.
Hal ini diikuti oleh sebuah studi satu tahun dari 230 anak-anak dengan sindrom syok dengue yang menerima pengobatan dengan cairan yang sama. Penelitian difokuskan pada berkelanjutan serta effects.13 perawatan segeraHasil penelitian menunjukkan tidak ada keuntungan yang jelas antara cairan dalam hal waktu untuk pulih dari esensial episode inisiasi shock, waktu untuk mencapai stabilitas mobil-akhir diovascular, atau persyaratan untuk penyelamatan koloid. Faktor yang paling signifikan menentukan respon klinis adalah tekanan nadi (yaitu, perbedaan antara langkah-tekanan sistolik dan diastolik) pada presentasi dengan kejutan. Dengue adalah un biasa dalam bahwa kebocoran lambat terjadi selama beberapa hari, memungkinkan mekanisme kompensasi untuk beroperasi. Sebelum pengembangan terbuka selang col- kardiovaskular, tekanan diastolik naik untuk memenuhi tekanan folat sistemik, dan tekanan nadi menyempit; sehingga tekanan nadi merupakan penanda keparahan kebocoran cular vas-. Menurut pedoman WHO, sebuah rawat-pasien dengan demam berdarah dengue dianggap memiliki dengue shock syndrome setelah tekanan nadi menyempit ke 20 mm Hg atau kurang. Analisis post hoc dari studi satu tahun menunjukkan bahwa pengobatan dini dengan solusi koloid mempercepat pemulihan pada anak-anak dengan tekanan nadi dari 10 mm Hg atau kurang pada presentasi (yaitu, kelompok dengan
penyelamatan pengobatan koloid yang diperlukan, dan kami menguji hipotesis bahwa tidak ada perbedaan dalam persyaratan untuk pengobatan dengan penyelamatan loid col setelah resusitasi awal dengan tate Ringer lac-, 6 persen dekstran 70, atau 6 persen etil hidroksi pati (masing-masing pada 25 ml per kilogram berat badan) antara anak-anak Vietnam dengan dengue shock syndrom

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
Metode
Desain penelitianSidang adalah pusat-tunggal, acak, perbandingan buta ganda dari solusi kristaloid isotonik (Ringer laktat) dan dua solusi koloid isotonik (6 persen dextran pati 70 [dekstran] dan 6 persen droxyethyl hidrokarbon 200 / 0.5 [pati]) untuk resusitasi darurat dari anak-anak dengan dengue shock syndrome. Anak-anak dikelompokkan berdasarkan tekanan nadi saat masuk, penanda kerusakan dari pembuluh darah yang bocor.13 anak-anak dalam kelompok dengan shock berat menerima kristaloid karena kekhawatiran tentang potensi pengembangan criti- kal kelebihan cairan tanpa akses dukungan pernafasan respi- canggih. Penelitian ini berlangsung di unit perawatan intensif anak di Rumah Sakit untuk Tropical Disease memudahkan di Kota Ho Chi Minh, Vietnam. Etika dan ilmu komite rumah sakit menyetujui protokol. Populasi penelitian Anak 2-15 tahun menyajikan langsung ke rumah sakit dengan klinis dengue shock syndrome yang memenuhi syarat untuk pendaftaran yang disediakan orang tua atau wali memberikan persetujuan tertulis. Pedoman WHO yang digunakan untuk diagnosis dengue shock syndrome.6 Pada awal penelitian kami mencatat atas memperlihatkan data yang ographic, sejarah, dan temuan pemeriksaan, dan kami memperoleh sampel plasma sitrat untuk skrining modulasi dan serum sampel coag- untuk diagnosis demam berdarah . Pasien yang terdaftar dalam salah satu dari dua kelompok sesuai dengan tekanan nadi di misi ad-. Anak-anak dengan syok keparahan sedang (tekanan nadi,> 10 dan ≤20 mm Hg) merupakan kelompok 1 dan secara acak ditugaskan untuk menerima Ringer laktat, dekstran, atau pati. Kelompok 2 con- sisted dari mereka dengan shock berat (tekanan nadi,≤10 mm Hg); anak-anak ini secara acak ditugasi untuk menerima baik dekstran atau pati. Setiap anak menerima 15 ml per kilogram berat badan dari cairan yang dialokasikan selama satu jam, diikuti oleh 10 ml per kilogram selama jam kedua.

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
Alokasi pengobatan ditentukan terlebih dahulu dengan penggunaan sistem acak yang dihasilkan komputer. Untuk memastikan Botol 500 ml cairan studi, disegel di dalam wadah khusus disiapkan karton dan diidentifikasi hanya oleh sejumlah peneliti , yang dipasok ke bangsal untuk setiap pasien. Paket perawatan untuk setidaknya lima pasien berikutnya disimpan di bangsal setiap saat. Kedua program diawasi oleh staf riset independen tidak terlibat dalam perawatan klinis. Sebuah amplop tertutup yang berisi identitas cairan studi melekat file studi untuk setiap anak dalam keadaan darurat.Setelah infus cairan, anak-anak menerima resusitasi dengan Ringer laktat yang melibatkan pengurangan pada interval waktu tertentu untuk tingkat pemeliharaan setelah delapan jam. Nadi, tekanan darah, dan perfusi perifer dipantau setidaknya per jam sampai mereka stabil selama minimal 24 jam, dan kemudian setiap 4 jam sampai debit. Kapiler hematokrit diukur pada awal,
2 dan 6 jam setelah awal penelitian, dan kemudian kira-kira setiap 12 jam atau dalam hal kerusakan kardiovaskular. Tambahan sampel plasma sitrat untuk skrining koagulasi diperoleh dari studi hari 2 dan 4, bersama-sama dengan sampel rum se- kedua untuk pengujian serologi untuk dengue infeksi tion di debit. Scan ultrasound dari dada dan perut dilakukan pada studi hari 3 oleh salah satu dari dua pengamat terlatih dengan penggunaan protokol terwujud standar-untuk mengukur kedalaman setiap efusi pleura dan menilai keparahan ascites.
Pasien yang statusnya kardiovaskular tidak mengalami pernbaikan setelah pemberian cairan studi (yaitu, mereka yang memiliki mempersempit atau tidak ada respon dalam tekanan nadi, bersama-sama dengan Bertahan atau worsen- ing mematikan perifer, hematokrit meningkat, atau keduanya) menerima infus 5 sampai 10 ml per kilogram penyelamatan koloid (biasanya dekstran) pada kebijaksanaan dokter. Demikian pula, jika setelah respon yang menguntungkan awal, tekanan nadi kemudian nar- mendayung lagi untuk 20 mm Hg atau kurang dengan vasokonstriksi perifer, hematokrit meningkat, atau keduanya, Rescue isyarat koloid dapat diberikan. Itu tidak mungkin untuk memperbaiki kriteria mutlak untuk penggunaan penyelamatan koloid, tapi kelompok inti yang sama dari dokter bertanggung jawab atas perawatan pasien selama penelitian, dan kebijakan umum unit perawatan intensif anak untuk intervensi setelah resusitasi awal adalah konservatif

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
Pasien menerima inotropik, transfusi darah, diuretik, dan terapi lain pada kebijaksanaan dokter yang merawat.
prosedur laboratoriumDiagnosis infeksi dengue dibuat dengan menggunakan Dengue Duo IgM capture dan menangkap IgG enzyme-linked immunosorbent assay kit (PanBio) pada sampel serum dipasangkan. Skrining koagulasi dilakukan dengan menggunakan kit yang diperoleh dari Diagnostica Stago; tes termasuk orang-orang untuk waktu trombin pro, diaktifkan waktu parsial tromboplastin-, dan tingkat fibrinogen dan uji semikuantitatif untuk produk fibrin-degradasi. Hanya hasil sampel dipisahkan dalam waktu 12 jam mendatang venipunc- dan tanpa hemolisis terlihat atau bekuan tion formasi yang dimasukkan dalam analisis.Ukuran hasil
Ukuran Hasil utama adalah kebutuhan untuk intervensi tambahan dengan penyelamatan koloid setiap saat setelah infus cairan. Ukuran hasil sekunder berikut adalah perawatan : waktu yang dibutuhkan untuk mencapai stabilitas kardiovaskular awal (didefinisikan sebagai waktu di jam dari awal penelitian sampai tekanan nadi mencapai dan dijaga pada ≥25 mm Hg dengan sistolik tekanan yakin ≥80 mm Hg selama minimal dua jam), waktu yang dibutuhkan untuk mencapai stabilitas kardiovaskular berkelanjutan (didefinisikan sebagai waktu di jam dari awal penelitian untuk mencapai dan mempertahankan ini indeks kardiovaskular tanpa batas tanpa intervensi lebih lanjut), volume penyelamatan koloid dan jumlah cairan parenteral diperlukan, pola perubahan dalam crit hemato-, dan jumlah hari di rumah sakit. Seorang pengamat gle sin- tidak terlibat dalam manajemen klinis dihitung setiap saat pemulihan dan volume cairan. Selain itu, empat efek samping yang mungkin berikut dari berbagai cairan diselidiki: perdarahan klinis; bukti laboratorium koagulopati; keparahan kebocoran pembuluh darah yang dinilai secara klinis, dengan ultrasonografi, dan dengan persyaratan untuk terapi uretic di-; dan kejadian alergi tipe reaksi.analisaUkuran sampel 360 pasien (120 dalam setiap kelompok cairan) dihitung untuk studi utama untuk memberikan persen listrik 80 untuk mendeteksi penurunan 50 persen dalam persyaratan untuk penyelamatan koloid pada tingkat signifikansi 5 persen, mengambil sebagai dasar temuan
dari studi sebelumnya, di mana sekitar 30 per- persen dari anak-anak dengan sindrom syok dengue kembali quired penyelamatan colloid.13 perekrutan Sejajar dengan penelitian yang membandingkan penggunaan dua koloid pada anak dengan shock berat diharapkan pada rasio kira-imately tiga pasien dengan syok cukup parah ke satu pasien dengan shock berat.Sebuah statistik yang tidak terlibat dalam disain atau pelaksanaan penelitian yang dilakukan semua ses analisi dengan penggunaan Stata (versi 8.0) atau StatsDi- rect software statistik. Sebuah analisis sementara direncanakan dilakukan sekitar setengah jalan melalui penelitian, dan hasilnya ditinjau oleh komite monitoring data dan keamanan. Af- ter serangkaian reaksi yang merugikan, analisis kedua, dengan fokus pada keamanan, dilakukan setelah 440 anak-anak telah direkrut; panitia-rekomendasi diperbaiki bahwa persidangan terus. Semua analisa dilakukan secara intention-to-treat. Karakteristik pasien dan efek pengobatan berbagai cairan dibandingkan dengan penggunaan chi-kuadrat atau uji Fisher untuk bles variasi yang kategori dan uji Mann-Whitney atau Kruskal-Wallis untuk variabel kontinyu. Waktu pemulihan kardiovaskular dibandingkan dengan penggunaan tes log-rank, dan probabilitas diperkirakan pemulihan disajikan sebagai kurva Kaplan-Meier. Dekstran dibandingkan dengan pati di kategori tekanan nadi; perbandingan dilakukan dengan menggunakan uji Mantel-Haenszel untuk hasil kategoris, dengan regresi logistik bersyarat digunakan untuk menguji hubungan fluida dengan keluar-terus menerus datang. Perbandingan angka kejadian antara kelompok cairan pengobatan ious var- disajikan sebagai risiko tive, berfokus pada perbandingan antara kristaloid dan salah satu dari kelompok koloid, atau tween dekstran dan kelompok pati. Kami menggunakan metode Koopman untuk rasio binomial untuk menentukan interval keyakinan persen

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
Hasil
fluid resuscitation for dengue shock syndrome
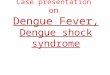
641 Eligible for enrollment during trial period
512 Enrolled 129 Not enrolled; all recovered5 Refused consent
91 Because of logistic problems with supply of study fluids in Vietnam
33 Because of temporary suspension of study pending safety analysis
Group 1 383 Underwent randomization Group 2 129 Underwent randomization
126 Assigned to dextran 129 Assigned to starch 128 Assigned toRinger’s lactate 67 Assigned to dextran 62 Assigned to starch
126 Analyzed2 With error of
enrollment or randomization
2 With negativeor indeterminate serologic tests
4 With study fluid not within 10% of protocol
2 With allocation unblinded
129 Analyzed3 With error of
enrollment or randomization
3 With negativeor indeterminate serologic tests
5 With study fluid not within 10% of protocol
1 With allocation unblinded
128 Analyzed5 With error of
enrollment or randomization
2 With negativeor indeterminate serologic tests
3 With study fluid not within 10% of protocol
0 With allocation unblinded
67 Analyzed1 With error of
enrollment or randomization
0 With negativeor indeterminate serologic tests
3 With study fluid not within 10% of protocol
3 With allocation unblinded
62 Analyzed3 With error of
enrollment or randomization
0 With negativeor indeterminate serologic tests
2 With study fluid not within 10% of protocol
0 With allocation unblinded
Figure 1. Profile of the Trial
Alokasi pemerintah adalah unblinded di enam pasien (lima menerima dextran, dan satu pati menerima) setelah alergi tipe reaksi parah terhadap cairan studi, untuk mengizinkan keputusan yang harus dibuat tentang yang koloid digunakan untuk terapi penyelamatan berikutnya. Semua karakteristik awal yang serupa di antara kelompok-kelompok id-pengobatan flu- untuk 383 anak-anak dengan mod- syok erately berat (kelompok 1) dan untuk 129 anak-anak dengan shock berat (kelompok 2) (Tabel 1). Satu anak (penerima pati) meninggal karena syok mendalam dan perdarahan gastrointestinal..
881

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
Table 1. Baseline Characteristics of the Patients.*
Characteristic Group 1 Group 2
Dextran Starch Ringer’s Lactate Dextran Starch(N=126) (N=129) (N=128) (N=67) (N=62)
Age — yr
Median 10 10 10 9 9
90% range 6 – 14 4.5 – 14 5 – 14 4 – 13 5 – 14
Male sex — no. (%) 57 (45) 70 (54) 66 (52) 29 (43) 33 (53)
Day of illness at shock — no. (%)
≤4 38 (30) 45 (35) 42 (33) 25 (37) 24 (39)
5–6 60 (48) 48 (37) 54 (42) 25 (37) 22 (35)
≥7 28 (22) 36 (28) 32 (25) 17 (25) 16 (26)
Fluid treatment before study entry — no. (%)
None 64 (51) 65 (50) 53 (41) 45 (67) 43 (69)
Maintenance only 62 (49) 61 (47) 72 (56) 21 (31) 18 (29)
More than maintenance 0 3 (2) 3 (2) 1 (1) 1 (2)
Weight — kg
Median 25 25 25 24 22
90% range 15 – 43 14 – 40 15 – 42 14 – 40 14 – 41
Temperature — °C
Median 37.0 37.0 37.0 37.0 37.0
90% range 37.0 – 38.1 37.0 – 38.4 37.0 – 38.7 37.0 – 38.0 37.0 – 38.4
Pulse rate — beats/min†
Median 110 110 120 120 120
90% range 80 – 140 80 – 130 90 – 140 80 – 140 83 – 142
Systolic blood pressure — mm Hg‡
Median 90 90 90 90 90
90% range 75 – 110 80 – 110 72 – 113 80 – 106 70 – 110
Diastolic blood pressure — mm Hg§
Median 75 75 75 80 80
90% range 57 – 90 60 – 90 55 – 95 66 – 94 59 – 100
Respiratory rate — breaths/min
Median 24 24 24 26 28
90% range 20–29 20–31 20–32 20–32 20–32
Bleeding manifestations — no. (%)
None 25 (20) 25 (19) 18 (14) 9 (13) 12 (19)
Skin only 79 (63) 78 (60) 87 (68) 43 (64) 40 (65)
Mucosal 17 (13) 26 (20) 21 (16) 12 (18) 8 (13)
Missing data 5 (4) 0 2 (2) 3 (4) 2 (3)
Liver size — cm
Median 2.0 2.0 2.0 2.0 2.0
90% range 0 – 4.0 0 – 3.6 0.3 – 4.0 0 – 3.0 0 – 3.0
Hematocrit — %
Median 48 47 48 51 51
90% range 42–54 41–55 42–54 45–56 43–58
882 n engl j med 353;9 www.nejm.org september 1, 2005

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
fluid resuscitation for dengue shock syndrome
Table 1. (Continued.)
Characteristic Group 1 Group 2
Dextran Starch Ringer’s Lactate Dextran Starch(N=126) (N=129) (N=128) (N=67) (N=62)
Platelet count — per mm3
Median 48,000 56,000 50,000 48,000 53,000
90% range 16,000 – 150,000 18,000 – 152,000 19,000 – 141,000 15,000 – 143,000 14,000 – 159,000Prothrombin time — sec¶¿
Median 12.8 13.0 13.1 13.7 14.1
90% range 11.8 – 16.2 11.8 – 21.7 11.9 – 19.2 11.9 – 18.6 11.7 – 22.4
Activated partial-thromboplastin time — sec¶**
Median 39.4 42.1 41.4 43.9 51.9
90% range 31.7 – 54.1 32.6 – 74.6 32.0 – 70.8 31.4 – 69.6 33.2 – 76.2
Fibrinogen — g/liter¶¿
Median 2.2 2.1 2.0 2.3 1.9
90% range 1.5 – 3.3 0.8 – 3.7 1.1 – 3.0 0.9 – 3.7 1.1 – 2.4
Fibrin-degradation products — no. (%)¶¿
Negative 29 (63) 22 (61) 30 (68) 18 (82) 11 (52)
Weakly positive 9 (20) 8 (22) 10 (23) 4 (18) 7 (33)
Strongly positive 8 (17) 6 (17) 4 (9) 0 3 (14)
Study fluid volume received — ml/kg
Median 25.0 25.0 25.0 25.0 25.0
90% range 24.0 – 25.8 22.8 –2 5.6 23.8 – 25.7 22.8 – 25.5 23.8 – 25.5
* Patients in group 1 had a pulse pressure greater than 10 mm Hg and less than or equal to 20 mm Hg. Patients in group 2 had a pulse pres- sure of 10 mm Hg or less. Percentages may not sum to 100 because of rounding.
† Data are for those patients with recordable values for cardiovascular characteristics at admission. In group 1, data are for 119 patients receiving dextran, 117 receiving starch, and 119 receiving Ringer’s lactate. In group 2, data are for 39 patients receiving dextran and 34 receiving starch.
‡ Data are for those patients with recordable values for cardiovascular characteristics at admission. In group 1, data are for 125 patients receiv- ing dextran and 127 receiving Ringer’s lactate. In group 2, data are for 47 patients receiving dextran and 39 receiving starch.
§ Data are for those patients with recordable values for cardiovascular characteristics at admission. In group 1, data are for 125 patients receiv- ing dextran and 127 receiving Ringer’s lactate. In group 2, data are for 43 patients receiving dextran and 36 receiving starch.
¶ Data are for samples separated within 12 hours, with no hemolysis or visible clot formation.¿ In group 1, data are for 46 patients receiving dextran, 36 receiving starch, and 44 receiving Ringer’s lactate. In group 2, data are for 22
patients receiving dextran and 21 receiving starch.** In group 1, data are for 45 patients receiving dextran, 35 receiving starch, and 44 receiving Ringer’s lactate. In group 2, data are for 22
patients receiving dextran and 20 receiving starch.
antara anak-anak yang menerima dekstran dibandingkan dengan pati dalam analisis gabungan. Anak-anak dalam kelompok 1 yang menerima Ringer laktat untuk resusitasi primer membutuhkan waktu lebih lama untuk mencapai stabilitas kardiovaskular awal dari pasien yang menerima salah satu dari koloid (Gbr. 2A), tetapi tingkat mise compro- selama periode ini umumnya tidak cukup untuk menjamin intervensi dengan penyelamatan koloid, dan waktu untuk stabilitas kardiovaskular akhir tidak berbeda- ent antara kelompok cairan-pengobatan (Gambar. 2B).Tidak ada anak dalam kelompok 1 yang telah menerima pati untuk resusitasi utama penyelamatan diperlukan koloid untuk kembali penutup dari episode ini. Secara keseluruhan, secara signifikan lebih sedikit penerima pati daripada dekstran diperlukan Rescue isyarat koloid pada tahap awal ini pada kedua kelompok keparahan; risiko relatif dari kebutuhan untuk penyelamatan koloid untuk episode awal shock adalah 0,34 (95 persen interval kepercayaan, 0,07-1,71; P = 0,03) antara penerima pati dibandingkan dengan penerima dekstran dalam analisis gabungan. Ada keuntungan kecil yang sesuai pada waktu awal pemulihan kardiovaskular di Ent alamat penerima pati dibandingkan dengan penerima dekstran dalam kelompok 2 (median, satu jam vs dua jam; P = 0,03 dengan uji log-rank). Namun, angka-angka yang terlibat kecil dan efeknya
n engl j med 353;9 www.nejm.org september 1, 2005 883

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
Table 2. Primary and Secondary Outcome Measures.*
Outcome Dextran Starch Ringer’s Lactate P Value†
Any rescue colloid — no. (%)Group 1 31 (25) 43 (33) 40 (31) 0.28Group 2 28 (42) 23 (37) — 0.59Groups combined 59 (31) 66 (35) — 0.38
Rescue colloid for initial resuscitation — no. (%)Group 1 5 (4) 0 4 (3) 0.05Group 2 6 (9) 3 (5) — 0.49Groups combined 11 (6) 3 (2) — 0.03
Rescue colloid required subsequently — no. (%)Group 1 29 (23) 43 (33) 38 (30) 0.18Group 2 26 (39) 22 (35) — 0.70Groups combined 55 (28) 65 (34) — 0.22
Total volume of rescue colloid — ml/kgGroup 1 0.11
Median 0 0 090% range 0–17 0–26 0–29
Group 2 0.76Median 0 0 —90% range 0 – 25 0 – 33 —
Groups combined 0.16Median 0 0 —90% range 0–22 0–28 —
Total fluid volume — ml/kgGroup 1 0.76
Median 100 100 10090% range 66 – 142 70 – 163 65 – 157
Group 2 0.70Median 104 106 —90% range 63 – 178 66 – 202 —
Groups combined 0.17Median 100 100 —90% range 64 – 152 70 – 166 —
Percentage reduction in hematocrit at 2 hr‡Group 1 <0.001
Median 25 22 990% range 10–35 7–31 1–19
Group 2 <0.001Median 28 25 —90% range 21 – 37 16 – 34 —
Groups combined <0.001Median 26 22 —90% range 10–36 10–32 —
Days in hospitalAll groups 0.81
Median 4 4 490% range 4–7 4–7 4–7
* In group 1, data are for 126 patients receiving dextran, 129 receiving starch, and 128 receiving Ringer’s lactate. In group 2, data are for 67 pa- tients receiving dextran and 62 receiving starch. In the groups combined, data are for 193 patients receiving dextran and 191 receiving starch. A dash denotes not applicable.
† The chi-square or Fisher’s exact test was used for categorical variables, and the Mann–Whitney or Kruskal–Wallis test for continuous variables. Comparisons between the children receiving dextran and starch across the two severity groups were carried out with the use of the Mantel– Haenszel test for categorical outcomes, with conditional logistic regression used to test fluid association with continuous outcomes. P values are for three-way comparisons in group 1 and for two-way comparisons in group 2 and the combined group analyses. For the combined analy- ses, tests for heterogeneity were not significant in each instance.
‡ In group 1, data are for 121 patients receiving dextran, 123 receiving starch, and 126 receiving Ringer’s lactate. In group 2, data are for 62 pa- tients receiving dextran and 60 receiving starch.
884 n engl j med 353;9 www.nejm.org september 1, 2005

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
fluid resuscitation for dengue shock syndrome
volume penyelamatan koloid atau total cairan
parenteral diberikan, dalam waktu pemulihan akhir, atau jumlah hari di rumah sakit.Perbedaan ditandai dicatat antara cairan dalam efek mereka pada hematokrit kapiler. Dua jam setelah awal penelitian, penurunan median di hematokrit dari awal adalah 9 persen (90 kisaran persen, 1-19 persen) untuk anak-anak dalam kelompok 1 yang menerima Ringer laktat dibandingkan dengan 25 per- persen (kisaran 90 persen,10 untuk 35 persen) bagi mereka
kemungkinan komplikasi pengobatan cairanTidak ada perbedaan yang signifikan Menurut Fluid Resusitasi Diterima.Dari 383 pasien dalam kelompok 1, 126 menerima dekstran, 129 pati, dan laktat 128 Ringer.curred dalam waktu enam jam dari mulai penelitiancairan. Kultur bakteri dan tes untuk endotoksin con-tamination negatif, tapi penyelidikan yang sedang berlangsung menunjukkan kontaminasi batch tertentu dengan pirogen nonendotoxin (Dr. S. Poole, Nasional In- stitute Biologi Standar dan Pengendalian, bujur don: komunikasi pribadi). Ruam urtikaria tanpa demam dikembangkan pada satu pasien dalam kelompok pati pada akhir infus. Semua pasien re- ditanggapi untuk pengobatan simtomatik saja.Tidak ada perbedaan antara kelompok perlakuan fluid- dalam pengembangan manifestasi baru bleed- ing, kelebihan cairan klinis, ukuran objektif dari keparahan keseluruhan kebocoran pembuluh darah, atau penggunaan furosemide (Tabel 3). Serial coag- tes modulasi-screening mengungkapkan coagulop- ringan Pada awal penelitian di semua kelompok pasien, seperti guna yang diharapkan, yang memburuk sedikit pada studi hari 2 tapi ditingkatkan lagi oleh studi hari 4 (Tabel 4). Satu-satunya perbedaan yang signifikan adalah antara nilai absolut untuk waktu parsial tromboplastin-pada anak-anak dalam kelompok 2 yang menerima dekstran atau pati pada hari 2. Namun, semua variabel koagulasi yang sedikit lebih buruk sebelum masuk penelitian pada anak-anak dalam kelompok 2 yang menerima pati, dan hari 2 re- Hasil pengujian sebenarnya mewakili peningkatan dari hari 1. Semua perbandingan lain menunjukkan tidak ada perbedaan antara kelompok cairan-pengobatan, termasuk parisons com- perubahan persentase setiap variasi yang ble pada hari yang berbeda (data tidak ditunjukkan).
n engl j med 353;9 www.nejm.org september 1, 2005 885

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
Table 3. Possible Adverse Effects of Fluid Treatment.*
Adverse Effect Group 1 Group 2
Dextran Starch Ringer’s Lactate Dextran Starch(N=126) (N=129) (N=128) (N=67) (N=62)
New bleeding after study entry — no. (%)
None 103 (82) 106 (82) 108 (84) 58 (87) 52 (84)
Minor skin bleeding 16 (13) 17 (13) 12 (9) 5 (7) 5 (8)
Mucosal or major soft-tissue bleeding 6 (5) 5 (4) 5 (4) 2 (3) 4 (6)
Any bleeding requiring transfusion 1 (<1) 1 (<1) 3 (2) 2 (3) 1 (2)
Clinical fluid overload — no. (%) 44 (35) 39 (30) 39 (30) 27 (40) 24 (39)
Depth of right pleural effusion — cm†
Median 4.4 4.6 4.3 4.8 4.9
90% range 0 – 7.2 0 – 7.7 0 – 7 2 – 6.8 2.1 – 8.5
Volume of ascites — no. (%)†
None 7 (9) 5 (6) 3 (4) 0 0
Mild 21 (27) 20 (24) 27 (35) 12 (29) 10 (28)
Moderate 46 (59) 54 (66) 43 (56) 27 (66) 23 (64)
Severe 4 (5) 3 (4) 4 (5) 2 (5) 3 (8)
Diuretic therapy — no. (%)
None 91 (72) 93 (72) 103 (80) 44 (66) 42 (68)
≤2 mg/kg furosemide, total dose 30 (24) 31 (24) 18 (14) 19 (28) 18 (29)
>2 mg/kg furosemide, total dose 5 (4) 5 (4) 7 (5) 4 (6) 2 (3)
Severe allergic-type reactions after infusion — no (%)‡ 9 (7) 1 (<1) 0 6 (9) 0
* Percentages may not sum to 100 because of rounding.† Data are for children for whom an ultrasound scan was performed 48 to 72 hours after study entry (i.e., in group 1, 78 patients receiving dex-
tran, 82 receiving starch, and 77 receiving Ringer’s lactate; and in group 2, 41 receiving dextran and 36 receiving starch). To assess the severity of leakage, the depth of fluid (in centimeters) in the right hemithorax posterior to the liver was measured with the patient lying flat and the probe placed at the costal margin in the mid-clavicular line.
‡ P<0.001 for group 1 and P = 0.03 for group 2 by Fisher’s exact test. All other statistical comparisons were not significant.
discussion tensive care units, has advanced considerably the general debate about crystalloids versus colloids.Meskipun penggantian volume diterima sebagai andalan pengobatan untuk anak-anak dengan sindrom syok dengue, dua penelitian sebelumnya yang pun semakin vestigated khasiat cairan yang berbeda di uation sit ini tidak memadai didukung sehubungan dengan hasil klinis yang relevan untuk memungkinkan perbandingan yang pasti antara manajemen dengan kristaloid dan koloid solusi. Penelitian ini, dengan persyaratan untuk penyelamatan koloid sebagai indikator hasil, pem- lishes bahwa termurah dan paling aman pilihan, laktat Cincin er ini, sama efektifnya dengan salah satu koloid untuk resusitasi awal anak-anak dengan moderat kejutan ly parah. Publikasi terbaru dari garis Setan vs Albumin Fluid Evaluasi (SAFE) Temuan studi, 15 menunjukkan bahwa albumin dan normal garis sa- sama-sama efektif untuk resusitasi cairan pada besar, populasi heterogen pasien di dalam-
Our trial, focusing on a single disease entity for which fluid resuscitation is the essential and usual- ly sole intervention required, indicates that even in patients with vascular leak, isotonic crystalloid so- lutions are as effective as colloid solutions for the majority of patients.
More patients with severe shock at presentation required rescue colloid than did patients with mod- erately severe shock, but only minor differences in efficacy were detected between the colloids in either severity group. Although minor benefits were seen among the recipients of starch during the initial re- suscitation, the relatively large molecular size of starch as compared with dextran did not result in prolonged intravascular persistence or a more sus- tained volume-expanding effect. We found no ev- idence of adverse effects of either colloid on the
886 n engl j med 353;9 www.nejm.org september 1, 2005

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
fluid resuscitation for dengue shock syndrome
Table 4. Results of Serial Coagulation-Screening Tests According to Day of Shock.*
Variable Day 1
Ringer’s
Day 2
Ringer’s
Day 4
Ringer’sDextran Starch Lactate Dextran Starch Lactate Dextran Starch Lactate
Group 1
No. of patients 46 36 44 90 96 95 97 90 89
Prothrombin time — sec
Median 12.8 13.0 13.1 13.3 13.1 13.1 12.2 12.2 12.1
90% range 11.8–16.2 11.8–21.7 11.9–19.2 11.9–19.4 11.9–18.5 11.9–18.5 11.1–14.7 11.0–15.1 11.2–14.5
Activated partial-thromboplastin time — sec
Median 39.4 42.1 41.4 43.8 42.8 42.2 35.4 35.0 34.8
90% range 31.7–54.1 32.6–74.6 32.0–70.8 32.0–60.4 32.1–59.3 32.5–59.2 30.1–44.8 29.8–46.4 30.1–47.4
Fibrinogen — g/liter
Median 2.2 2.1 2.0 1.6 1.5 1.7 2.1 2.3 2.3
90% range 1.5–3.3 0.8–3.7 1.1–3.0 0.8–3.1 0.7–2.7 0.7–2.9 1.1–3.3 1.5–3.2 1.1–3.4
Fibrin-degradation products —no. (%)
Negative 29 (63) 22 (61) 30 (68) 67 (74) 74 (77) 75 (79) 62 (64) 56 (62) 55 (62)
Weakly positive 9 (20) 8 (22) 10 (23) 13 (14) 17 (18) 17 (18) 18 (19) 24 (27) 20 (22)
Strongly positive 8 (17) 6 (17) 4 (9) 10 (11) 5 (5) 3 (3) 17 (18) 10 (11) 14 (16)
Group 2
No. of patients 22 21 — 48 44 — 52 48 —
Prothrombin time — sec
Median 13.7 14.1 — 13.8 14.4 — 12.6 12.7 —
90% range 11.9–18.6 11.6–22.4 — 11.2–21.8 11.8–21.8 — 11.2–16.1 10.9–19.0 —
Activated partial-thromboplastin time — sec
Median 43.9 51.9 — 42.2† 48.5† — 35.5 36.8 —
90% range 31.4–69.6 33.2–76.2 — 32.1–62.3 34.3–63.1 — 30.7–51.1 31.7–53.8 —
Fibrinogen — g/liter
Median 2.3 1.9 — 1.4 1.5 — 2.3 2.3 —
90% range 0.9–3.7 1.1–2.5 — 0.9–3.3 0.7–3.0 — 1.5–3.9 1.4–3.9 —
Fibrin-degradation products —no. (%)
Negative 18 (82) 11 (52) — 36 (73) 36 (82) — 26 (50) 22 (46) —
Weakly positive 4 (18) 7 (33) — 10 (20) 6 (14) — 16 (31) 14 (29) —
Strongly positive 0 3 (14) — 3 (6) 2 (5) — 10 (19) 12 (25) —
* The day of study entry is day 1. Data are for samples separated within 12 hours, with no hemolysis or visible clot formation. Dashes denote not applicable. Percentages may not sum to 100 because of rounding.
† In group 2 on day 2, the activated partial-thromboplastin time was significantly prolonged in the children who received starch as compared with those who received dextran (P<0.001 by the Kruskal–Wallis test). All other comparisons for the absolute values and for the percentage changes in the variables at each time point showed no differences among the fluids.
intrinsic coagulopathy or clinical bleeding mani- festations or on the severity of fluid overload.
The serial hematocrit measurements reflect a combination of the effects of fluid treatment and ongoing vascular leak. The hematocrit data indicate that the two colloids exert a dramatic immediate ef-
fect that is followed by a rebound increase in vascu- lar leak a few hours later.
Current theories of microvascular ultrafiltration support the basic Starling principle of a balanced equilibrium between opposing oncotic and hydro- static pressures but postulate that the glycocalyx,
n engl j med 353;9 www.nejm.org september 1, 2005 887

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
rather than the endothelial cells themselves, is the major regulator of fluid flow.16,17 There is good ev- idence that plasma proteins, particularly albumin, adsorb to positive residues in the glycocalyx layer and restrict ultrafiltration.18-20
Albumin is probably washed out of this layer during dengue infections but may be replaced temporarily by the synthetic col- loids, which are known to permeate the glycocalyx at different rates, depending on molecular size.21 In this way, colloids may briefly alter the selective per- meability of the endothelial barrier, reducing out- ward flux and permitting the low hydrostatic pres- sure of the capillaries to rise until the colloid molecules themselves are washed out and the net Starling forces again favor leakage but from a higher baseline hydrostatic pressure. In contrast, crystal- loid solutions equilibrate rapidly throughout the in- travascular and interstitial fluid spaces and appear to have no effect on the function of the endothelial barrier. The effects of colloids are transient, how- ever, and despite the early rebound in the hemat- ocrit seen in the children receiving colloids, we found no difference between the different fluids in the overall severity of fluid overload when it was assessed 48 to 72 hours after the study infusion.
During the study, an excess of febrile responses occurred in the recipients of dextran. Dextrans are produced by a process involving bacterial degrada- tion, and despite purification, residual pyrogens may be sufficient to induce febrile responses. In the present study, febrile responses were associated with particular batches of fluids. The overall fre- quency and importance of this adverse effect in the management of dengue remain to be determined.
In addition to its relevance to dengue, major strengths of this large, randomized trial in the general debate about crystalloids versus colloids are the uniform nature of the underlying disease pro- cess and the fact that fluid resuscitation is the single most important therapeutic intervention. Subgroup analysis of the SAFE trial suggested a treatment effect favoring albumin in patients with severe sep- sis of mixed underlying causes,15
many of whom are likely to have had an associated vascular-leak syndrome. In our study, however, there was no clear benefit to the use of a colloid in children with moderately severe shock due to vascular-leak syn- drome. Although the pathophysiological mecha- nism underlying the vascular leak associated with severe sepsis may well be different from that asso- ciated with the dengue virus, this group of chil- dren showed considerable cardiovascular compro-
mise, and yet most did well with Ringer’s lactate alone.
Unlike the SAFE trial, the present trial did not examine mortality as an outcome; our primary out- come was an intervention based on the treating clinician’s subjective assessment of need. However, our study took place in a single ward staffed by the same core group of doctors throughout and study treatment was concealed and blinded so that dif- ferences in the threshold for intervention are likely to have been distributed evenly across the groups of children receiving the various fluids. Although there is no proven relationship to mortality, colloid rescue is an integral part of the WHO management guidelines for resuscitation of dengue shock syn- drome, and a substantial requirement for rescue colloid is considered by physicians in endemic ar- eas to be a poor prognostic marker.
It is likely that the excellent overall outcome (one death among 641 children with dengue shock syndrome treated during the trial period) reflects meticulous overall medical and nursing care as much as the specific treatments used. Hourly ob- servations, immediate access to ward-based hema- tocrit measurements, and a conservative interven- tion policy ensure that patients receive volumes of intravenous fluid that are titrated carefully to re- quirements, thus providing sufficient fluid to main- tain vital functions during the period of systemic leakage without overfilling the intravascular space. Respiratory compromise secondary to fluid over- load is a major contributor to mortality in settings with poor resources, few personnel, and limited equipment. In general, in the Southeast Asian re- gion, mortality rates of 1 to 5 percent persist, and efforts to improve management must continue. For ethical reasons, we did not address the issue of the use of crystalloids for patients with profound or re- current shock, two situations in which colloid so- lutions are thought to be beneficial, despite a lack of good supporting evidence. Further studies are needed that focus on these high-risk groups. The uniformly good outcome in children with shock of moderate severity who received the crystalloid in this study may help to provide reassurance for future studies. In addition, work to better define the patho- physiological mechanisms underlying the vascular- leak process will be useful to inform future studies.
In conclusion, most children with dengue shock syndrome respond well to judicious treatment with isotonic crystalloid solutions. Early intervention with colloid solutions is not indicated. The fluid

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
888 n engl j med 353;9 www.nejm.org september 1, 2005

The New England Journal of MedicineDownloaded from nejm.org on October 19, 2015. For personal use only. No other uses without permission.
Copyright © 2005 Massachusetts Medical Society. All rights reserved.
fluid resuscitation for dengue shock syndrome
regimen of Ringer’s lactate at 25 ml per kilogram over a period of two hours is now supported by strong prospective evidence and should be recom- mended for children with moderately severe shock. For those with severe shock, the situation is less clear-cut, and clinicians must continue to rely on personal experience, familiarity with particular products, local availability, and cost. Minor advan- tages in initial recovery were shown with starch, and significantly more adverse reactions were as- sociated with dextran, so if the use of a colloid is considered necessary, starch may be the preferred option.
Supported by the Wellcome Trust. Dr. Wills is a Wellcome Trust Career Development Fellow, Dr. Farrar is a Wellcome Trust Senior Fellow, and Professor White is a Wellcome Trust Principal Fellow.
We are indebted to the directors of the Hospital for Tropical Dis- eases for their encouragement, to the medical and nursing staff of the pediatric intensive care unit for their care of the patients, to the staff of the Oxford University Clinical Research Unit for laboratory and clerical support, to B. Braun Medical Industries in Vietnam for donating all the parenteral fluids and providing the containers for blinding, to Dr. Stephen Poole (principal scientist, National Insti- tute for Biological Standards and Control, London) for investigat- ing possible contamination of dextran fluid batches, and to the data and safety monitoring committee (Dr. Rose McGready at the Shoklo Malaria Research Unit, Mae Sot, Thailand, and Dr. Delia Bethell at the Mahidol University–Oxford Tropical Medicine Re- search Progamme, Bangkok, Thailand, in addition to Professor White and Dr. Stepniewska).
references
1. Halstead SB. Epidemiology of dengue Crystalloids vs. colloids in fluid resuscita- 15. The SAFE Study Investigators. A com-and dengue haemorrhagic fever. In: Gubler tion: a systematic review. Crit Care Med parison of albumin and saline for fluid re-DJ, Kuno G, eds. Dengue and dengue haem- 1999;27:200-10. suscitation in the intensive care unit. N
Englorrhagic fever. Wallingford, England: CAB 9. Alderson P, Schierhout G, Roberts I, J Med 2004;350:2247-56.International, 1997:23-44. Bunn F. Colloids versus crystalloids for 16. Starling EH. On the absorption of fluids2. Cohen SN, Halstead SB. Shock associ- fluid resuscitation in critically ill patients. from the connective tissue spaces. J Physiolated with dengue infection. I. Clinical and Cochrane Database Syst Rev 2000;2: 1896;19:312-26.physiologic manifestations of dengue hem- CD000567. 17. Michel CC, Curry FE. Microvascular per-orrhagic fever in Thailand, 1964. J Pediatr 10. Haupt MT, Kaufman BS, Carlson RW. meability. Physiol Rev 1999;79:703-61.1966;68:448-56. Fluid resuscitation in patients with increased 18. Haraldsson B, Rippe B. Orosomucoid3. Rigau-Perez JG, Clark GG, Gubler DJ, vascular permeability. Crit Care Clin 1992;8: as one of the serum components contribut-Reiter P, Sanders EJ, Vorndam AV. Dengue 341-53. ing to normal capillary permselectivity in ratand dengue haemorrhagic fever. Lancet 11. Griffel MI, Kaufman BS. Pharmacology skeletal muscle. Acta Physiol Scand 1987;1998;352:971-7. of colloids and crystalloids. Crit Care Clin 129:127-35.4. Monath TP. Dengue: the risk to devel- 1992;8:235-53. 19. Schneeberger EE, Lynch RD, Neary BA.oped and developing countries. Proc Natl 12. Dung NM, Day NP, Tam DT, et al.
FluidInteraction of native and chemically modi-
Acad Sci U S A 1994;91:2395-400. replacement in dengue shock syndrome: fied albumin with pulmonary microvascular5. Technical guides for diagnosis, treat- a randomized, double-blind comparison of endothelium. Am J Physiol 1990;258:L89-ment, surveillance, prevention and control four intravenous-fluid regimens. Clin Infect L98.of dengue haemorrhagic fever. Geneva: Dis 1999;29:787-94. 20. Huxley VH, Curry FE. Differential ac-World Health Organization, 1975. 13. Ngo NT, Cao XT, Kneen R, et al. Acute tions of albumin and plasma on capillary6. Dengue haemorrhagic fever: diagnosis, management of dengue shock syndrome: solute permeability. Am J Physiol 1991;260:treatment, prevention and control. 2nd ed. a randomized double-blind comparison of H1645-H1654.Geneva: World Health Organization, 1997. 4 intravenous fluid regimens in the first 21. Vink H, Duling BR. Capillary endothe-7. Schierhout G, Roberts I. Fluid resuscita- hour. Clin Infect Dis 2001;32:204-13. lial surface layer selectively reduces plasmation with colloid or crystalloid solutions in 14. Wills BA, Oragui EE, Dung NM, et al. solute distribution volume. Am J Physiolcritically ill patients: a systematic review of Size and charge characteristics of the protein Heart Circ Physiol 2000;278:H285-H289.randomised trials. BMJ 1998;316:961-4. leak in dengue shock syndrome. J Infect Dis Copyright © 2005 Massachusetts Medical Society.
8. Choi PT, Yip G, Quinonez LG, Cook DJ. 2004;190:810-8.
n engl j med 353;9 www.nejm.org september 1, 2005 889