Embed Size (px)
Citation preview

Compliance with protocols in transferringemergency patients to a tertiary care centre
$
Erol Armagana, Murat Gultekin Ala, Zulfi Engindeniza, Rifat Tokyayb,*
aDepartment of Emergency Medicine, Uludag University Medical School, 16059 Bursa, TurkeybDepartment of Surgery, Uludag University Medical School, 16059 Bursa, Turkey
Accepted 14 October 2003
Introduction
Inter-hospital patient transfers are necessary in thehealth care system to provide better care for
patients. Treating a patient in a health care facilityinappropriately staffed or ill equipped for the careof that patient’s need might have serious conse-quences.3 As all medical facilities do not have thesame sophisticated diagnostic, medical and surgicalcapabilities, physicians or administrators in a hos-pital may request the transfer of a patient toanother hospital. In some countries, as in ours,patients themselves may ask for their transferbecause their insurance company may not reim-
Injury, Int. J. Care Injured (2004) 35, 857—863
KEYWORDS
Patient transfer; Patient
transport; Inter-hospital
transfers; Emergency
medical services
Summary Study objectives: We evaluated compliance with standard patient transferprotocols in a pre- and post-interventional study among patients transferred from otherhospitals to our tertiary care university hospital. Methods: In the first phase, transferinformation was recorded on the arrival in 174 consecutive patients transferred to ouremergency department (ED) over a 2-month period in 1999. Emergency caregiversthroughout the province then received education about proper transfer procedures.This training was provided through monthly citywide co-ordination and co-operationmeetings among the physicians of the emergency medical services (EMS) and theemergency departments of the hospitals in the city and the nearby counties. Fifteenmonths after the beginning of these educational efforts, the second observational phasewas implemented. Over a period of 2 months in early 2001, information was recordedfrom 180 consecutive patients transferred to our ED. Presence of patient medicalrecords, laboratory results, and X-rays; clearly delineated reason for transfer; priornotification of transfer; and appropriate care during transport from the initial facilitywere the parameters compared in the pre- and post-intervention periods. Results:Patients in phase-II were found to have had moreappropriate care in some respects, suchas presence of cervical collar and proper airway management, during transport from theinitial facility than patients in phase-I ðP < 0:05Þ. However, other parameters were notsignificantly different between the two phases. Conclusion: We have concluded that ourmonthly meetings and conferences have made a positive impact on compliance withsome of the standard transfer protocols. We must however, continue our efforts toincrease compliance with other aspects of standard patient transfer guidelines.� 2004 Published by Elsevier Ltd.
$The abstract of this study was presented at the FirstMediterranean Emergency Medicine Congress at Stresa, Italy,2—5 September 2001.
*Corresponding author. Tel.: þ90-224-442-8097;fax: þ90-224-442-8097.
E-mail address: [email protected] (R. Tokyay).
0020–1383/$ — see front matter � 2004 Published by Elsevier Ltd.doi:10.1016/j.injury.2003.09.038
burse medical expenses incurred in that particularhealth care facility.3,11,16,23
Although patient transfer is often done to providebetter care for the patient, it also carries somemedical risks for the patient and medico-legal risksfor the transferring physician. Complications andiatrogenic problems can occur, especially duringthe transport of critically ill patients, seriouslyincreasing their morbidity and mortality(M&M).8,15,25 Therefore, it is essential to establishcertain policies and protocols for patient transfers.In that regard, the most important issue is thedefinition of the patient being ‘‘fit for transfer’’.Measures and precautions to be followed to ensuresafe patient transport also need to be agreed.1,6
Turkey is a developing country with a populationof 67 million. Its gross national product (GNP) percapita is around US$ 2500 and it spends only 3.5% ofits GNP on health care.
Our 800-bed, university hospital serves a popu-lation of 11 million, 1 million urban and 10 millionrural. Bursa, the fifth largest city and an importantindustrial region, is placed in the west and rela-tively more developed part of Turkey. In themetropolitan area there are eight state-owned,one military and three private hospitals. Four ofthese state-owned hospitals are general hospitals(two for the public two for working men and theirfamilies) that may be categorised as level II (400—600 beds) and level III trauma centres (150—250beds) and the other four are speciality hospitals,children’s, oncology, gynaecology and obstetrics,respiratory disease. In the rural area, there are 12level III—IV hospitals (50—150 beds). In Turkey
there are hospitals with more facilities and lessbeds but usually the facilities a hospital hasincrease with the number of beds. The Americansystem of categorisation (level I—IV) was used togive the reader a rough idea about that hospital’snumber of beds, departments, personnel, facil-ities, resources, and capabilities.
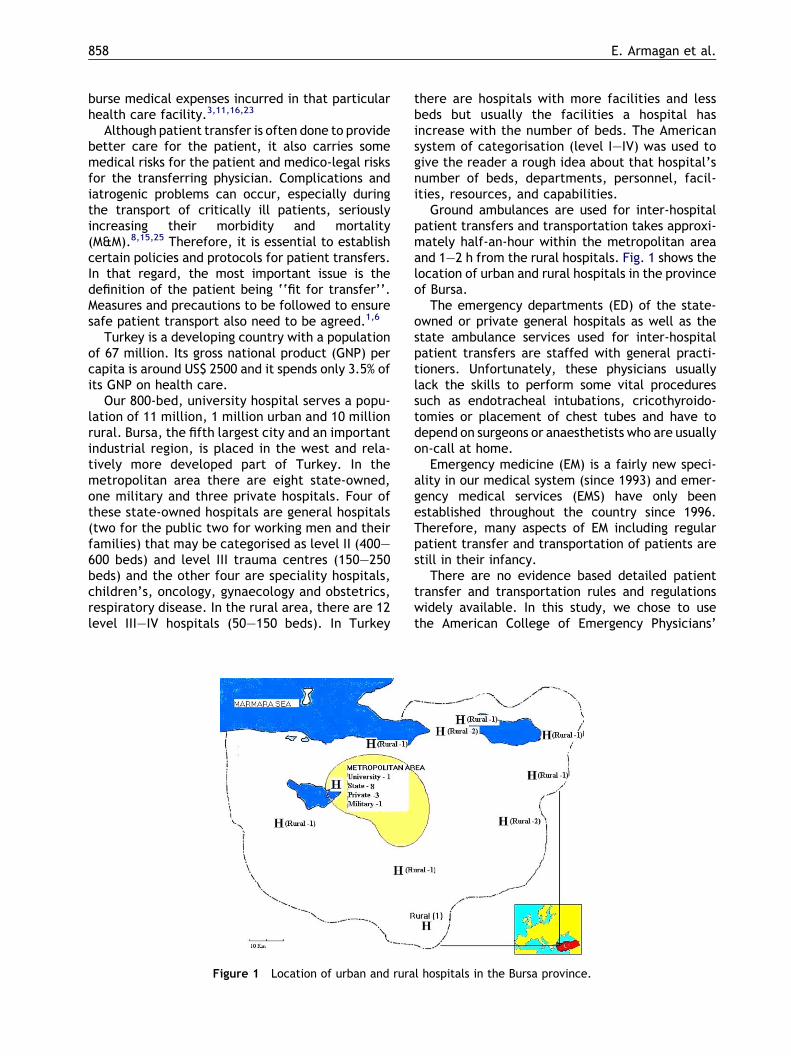
Ground ambulances are used for inter-hospitalpatient transfers and transportation takes approxi-mately half-an-hour within the metropolitan areaand 1—2 h from the rural hospitals. Fig. 1 shows thelocation of urban and rural hospitals in the provinceof Bursa.
The emergency departments (ED) of the state-owned or private general hospitals as well as thestate ambulance services used for inter-hospitalpatient transfers are staffed with general practi-tioners. Unfortunately, these physicians usuallylack the skills to perform some vital proceduressuch as endotracheal intubations, cricothyroido-tomies or placement of chest tubes and have todepend on surgeons or anaesthetists who are usuallyon-call at home.
Emergency medicine (EM) is a fairly new speci-ality in our medical system (since 1993) and emer-gency medical services (EMS) have only beenestablished throughout the country since 1996.Therefore, many aspects of EM including regularpatient transfer and transportation of patients arestill in their infancy.
There are no evidence based detailed patienttransfer and transportation rules and regulationswidely available. In this study, we chose to usethe American College of Emergency Physicians’
Figure 1 Location of urban and rural hospitals in the Bursa province.
858 E. Armagan et al.
(ACEP) guide lines as a reference and investigatedthe compliance with these guidelines in patientswho were transferred to our university hospitalfrom other hospitals in the city or nearby towns.
The aim of this study was two-fold. Firstly, todetermine the present problems in inter-hospitalpatient transfers in our area, secondly to find out ifthere was an increase in compliance following theintroduction of patient transfer rules to and educa-tion of the emergency caregivers in the province.
Methods
Prospective data were collected from patientstransferred to our 800-bed, tertiary care universityhospital. The following data were collected:
� reason for transfer;� presence of any risks for transfer;
� lack of airway support;� no intravenous line (IV);� no cervical collar;
� presence of prior inter-hospital, physician to phy-sician communication;
� adequacy of the medical records;� availability of diagnostic tests/X-rays performed
in the transferring hospital.
These data were collected with a detailed formcompleted by emergency residents. Adequacies ofmedical records sent with patient and of interven-tions before and during transport were evaluated bythe authors’ committee daily. In phase-I a writtennote of the problem, treatment given, and thepatient’s status at the time of transfer was consid-ered as an adequate medical record. In the secondphase, a standardised transfer sheet had to be filledin to consider medical records as adequate. Thissheet included the patient’s name, initial diagnosis,history of illness or injury, condition at admission,vital signs, treatment rendered, fluids given,laboratory and X-ray findings, and the name ofthe referring physician and hospital.
Adequacy of airway management was assessedaccording to the indications stated in the AmericanCollege of Surgeon’s Advanced Trauma Life Supportfor Doctors (ATLS) student course manual.2 If apatient had a decreased level of consciousness thatcould have caused airway obstruction, but did nothave an oropharyngeal airway to prevent this onarrival, then airway management was considered asinadequate. If a patient needed either airway pro-tection or assisted ventilation but did not have adefinitive airway (endotracheal tube or surgical air-way) on arrival that patient’s airway managementwas also considered inadequate.
Criteria for determining the need for airwayprotection were:
� unconscious patient;� severe maxillofacial trauma;� aspiration risk due to bleeding and vomiting;� obstruction risk due to laryngo-tracheal injury.
Criteria for determining the need for assistedventilation were the presence of:
� tachypnoea (>35 breaths/min);� hypoxia (pO2 <70 mmHg);� hypercarbia (pCO2 >50 mmHg);� cyanosis.
in spite of oxygen supplementation by mask.Prior stabilisation of transferred trauma patients
requires some further actions to comply with the‘‘transfer rules’’:
� Cervical spine must be immobilised.� A nasogastric (NG) tube must be placed to avoid
aspiration.� A urinary catheter must be inserted to monitor
urine output.
To assess compliance with these we chose tomeasure the rates of cervical collor placement,bladder catheterisation and nasogastric tube place-ment in the transferred trauma patients.
The study was conducted in two phases: in phase-I we collected data on 174 transfers between 1 Mayand 30 June 1999.
Then, our emergency department organisedmonthly regional EMS meetings. Initially, atten-dance for these meetings was on a voluntary basisbut after the second meeting all the physiciansworking in the ambulances and the emergencydepartments of the state hospitals in our regionwere officially invited by the chief of the city healthdepartment. In the first three meetings, our EM staffemphasised the following fundamental rules of theACEPs guidelines for patient transfer:
1. A proper medical record including X-rays anddiagnostic test results should be sent with thepatient.
2. The receiving hospital must be informed beforethe transfer and there should be discussionbetween physicians at both hospitals.
3. Medical evaluation and proper stabilisationshould be performed before the transfer andappropriate care should be available on route.
Results of the first phase were also presented anddiscussed in these three initial meetings. Officers inthe department of health and managers of the cityand county state hospitals were also informed aboutthese results. After the first 3 monthly meetings an
Compliance with protocols in transferring emergency patients to a tertiary care centre 859
morbidity and mortality type format was adaptedfor the next 12 months. Patients thought to haveincreased morbidity or mortality due to inadequateprior stabilisation or inappropriate handling duringtransport were presented by the involved hospitalor the ambulance service and the mistakes made,lessons learned, and measures which should havebeen taken were discussed.
Fifteen months after the conclusion of the firstphase the second phase was started. In this phase,180 transferred patients in a period of 2 monthsfrom 1 February to 31 March 2001 were evaluated.The rates of compliance were determined for eachphase separately and then compared with eachother by using w2-test.
Results
A total number of 354 patients, ages ranging from 6to 90 years, were included in the study. The mostfrequent diagnoses of these patients were trauma(31.07%), cerebrovascular diseases (21.75%) andcoronary artery diseases (13.55%).
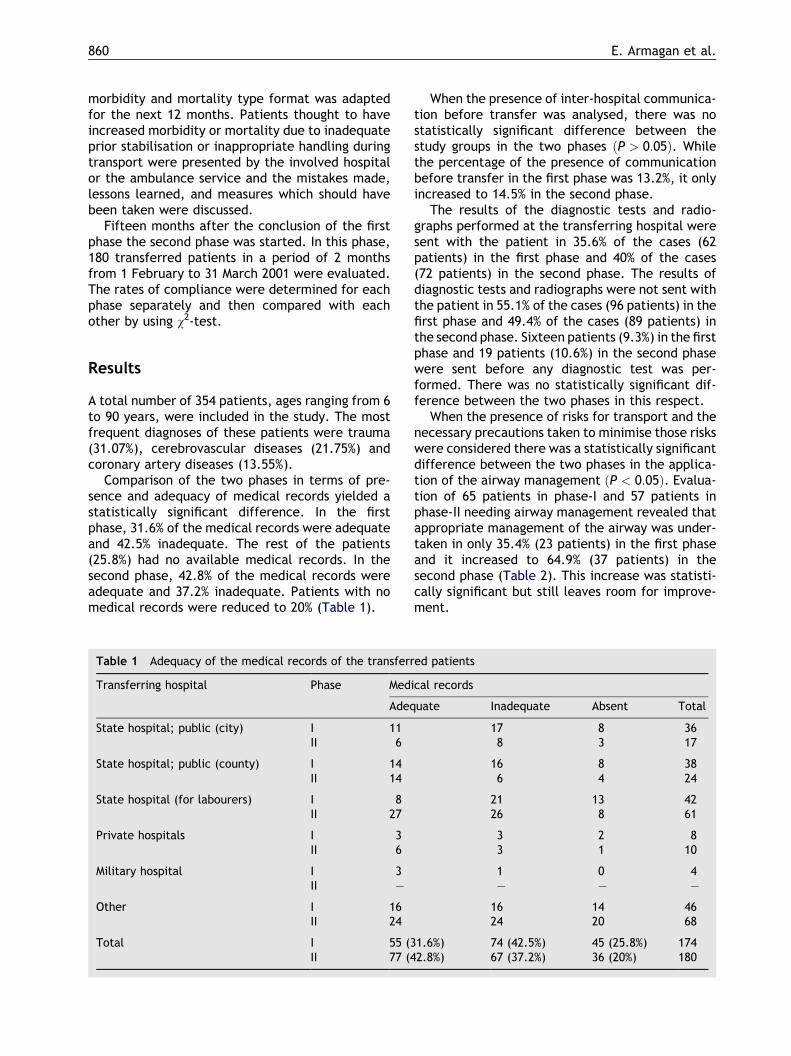
Comparison of the two phases in terms of pre-sence and adequacy of medical records yielded astatistically significant difference. In the firstphase, 31.6% of the medical records were adequateand 42.5% inadequate. The rest of the patients(25.8%) had no available medical records. In thesecond phase, 42.8% of the medical records wereadequate and 37.2% inadequate. Patients with nomedical records were reduced to 20% (Table 1).
When the presence of inter-hospital communica-tion before transfer was analysed, there was nostatistically significant difference between thestudy groups in the two phases ðP > 0:05Þ. Whilethe percentage of the presence of communicationbefore transfer in the first phase was 13.2%, it onlyincreased to 14.5% in the second phase.
The results of the diagnostic tests and radio-graphs performed at the transferring hospital weresent with the patient in 35.6% of the cases (62patients) in the first phase and 40% of the cases(72 patients) in the second phase. The results ofdiagnostic tests and radiographs were not sent withthe patient in 55.1% of the cases (96 patients) in thefirst phase and 49.4% of the cases (89 patients) inthe second phase. Sixteen patients (9.3%) in the firstphase and 19 patients (10.6%) in the second phasewere sent before any diagnostic test was per-formed. There was no statistically significant dif-ference between the two phases in this respect.
When the presence of risks for transport and thenecessary precautions taken to minimise those riskswere considered there was a statistically significantdifference between the two phases in the applica-tion of the airway management ðP < 0:05Þ. Evalua-tion of 65 patients in phase-I and 57 patients inphase-II needing airway management revealed thatappropriate management of the airway was under-taken in only 35.4% (23 patients) in the first phaseand it increased to 64.9% (37 patients) in thesecond phase (Table 2). This increase was statisti-cally significant but still leaves room for improve-ment.
Table 1 Adequacy of the medical records of the transferred patients
Transferring hospital Phase Medical records
Adequate Inadequate Absent Total
State hospital; public (city) I 11 17 8 36II 6 8 3 17
State hospital; public (county) I 14 16 8 38II 14 6 4 24
State hospital (for labourers) I 8 21 13 42II 27 26 8 61
Private hospitals I 3 3 2 8II 6 3 1 10
Military hospital I 3 1 0 4II — — — —
Other I 16 16 14 46II 24 24 20 68
Total I 55 (31.6%) 74 (42.5%) 45 (25.8%) 174II 77 (42.8%) 67 (37.2%) 36 (20%) 180
860 E. Armagan et al.
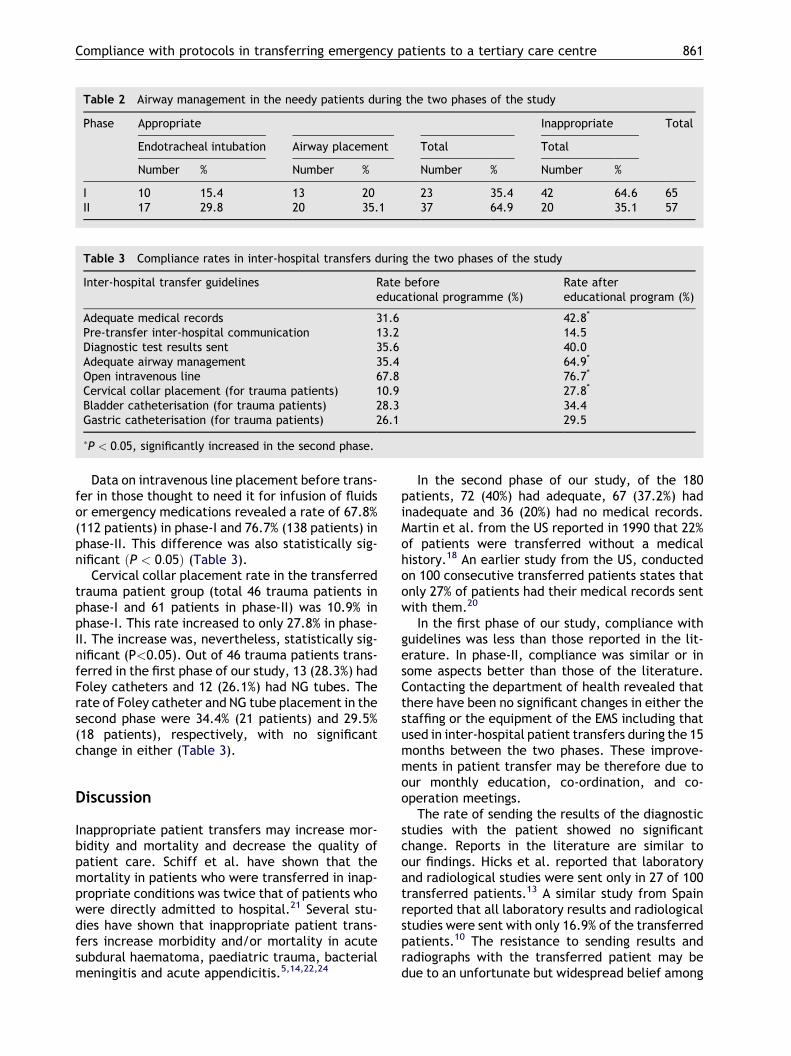
Data on intravenous line placement before trans-fer in those thought to need it for infusion of fluidsor emergency medications revealed a rate of 67.8%(112 patients) in phase-I and 76.7% (138 patients) inphase-II. This difference was also statistically sig-nificant ðP < 0:05Þ (Table 3).
Cervical collar placement rate in the transferredtrauma patient group (total 46 trauma patients inphase-I and 61 patients in phase-II) was 10.9% inphase-I. This rate increased to only 27.8% in phase-II. The increase was, nevertheless, statistically sig-nificant (P<0.05). Out of 46 trauma patients trans-ferred in the first phase of our study, 13 (28.3%) hadFoley catheters and 12 (26.1%) had NG tubes. Therate of Foley catheter and NG tube placement in thesecond phase were 34.4% (21 patients) and 29.5%(18 patients), respectively, with no significantchange in either (Table 3).
Discussion
Inappropriate patient transfers may increase mor-bidity and mortality and decrease the quality ofpatient care. Schiff et al. have shown that themortality in patients who were transferred in inap-propriate conditions was twice that of patients whowere directly admitted to hospital.21 Several stu-dies have shown that inappropriate patient trans-fers increase morbidity and/or mortality in acutesubdural haematoma, paediatric trauma, bacterialmeningitis and acute appendicitis.5,14,22,24
In the second phase of our study, of the 180patients, 72 (40%) had adequate, 67 (37.2%) hadinadequate and 36 (20%) had no medical records.Martin et al. from the US reported in 1990 that 22%of patients were transferred without a medicalhistory.18 An earlier study from the US, conductedon 100 consecutive transferred patients states thatonly 27% of patients had their medical records sentwith them.20
In the first phase of our study, compliance withguidelines was less than those reported in the lit-erature. In phase-II, compliance was similar or insome aspects better than those of the literature.Contacting the department of health revealed thatthere have been no significant changes in either thestaffing or the equipment of the EMS including thatused in inter-hospital patient transfers during the 15months between the two phases. These improve-ments in patient transfer may be therefore due toour monthly education, co-ordination, and co-operation meetings.
The rate of sending the results of the diagnosticstudies with the patient showed no significantchange. Reports in the literature are similar toour findings. Hicks et al. reported that laboratoryand radiological studies were sent only in 27 of 100transferred patients.13 A similar study from Spainreported that all laboratory results and radiologicalstudies were sent with only 16.9% of the transferredpatients.10 The resistance to sending results andradiographs with the transferred patient may bedue to an unfortunate but widespread belief among
Table 2 Airway management in the needy patients during the two phases of the study
Phase Appropriate Inappropriate Total
Endotracheal intubation Airway placement Total Total
Number % Number % Number % Number %
I 10 15.4 13 20 23 35.4 42 64.6 65II 17 29.8 20 35.1 37 64.9 20 35.1 57
Table 3 Compliance rates in inter-hospital transfers during the two phases of the study
Inter-hospital transfer guidelines Rate beforeeducational programme (%)
Rate aftereducational program (%)
Adequate medical records 31.6 42.8*
Pre-transfer inter-hospital communication 13.2 14.5Diagnostic test results sent 35.6 40.0Adequate airway management 35.4 64.9*
Open intravenous line 67.8 76.7*
Cervical collar placement (for trauma patients) 10.9 27.8*
Bladder catheterisation (for trauma patients) 28.3 34.4Gastric catheterisation (for trauma patients) 26.1 29.5
�P < 0:05, significantly increased in the second phase.
Compliance with protocols in transferring emergency patients to a tertiary care centre 861
physicians and hospital administrators in our coun-try that these must be kept in the first hospital incase of legal action. Sending copies would be anoption but we think that no one would really botherunless it was made obligatory in the official transferguidelines set by the state or the regional healthauthorities. We think that continuation of ourmonthly meetings and the invitation of a forensicmedicine specialist to these meetings may make adifference.
Another parameter that was not improved sta-tistically between the two phases of our study wasthe presence of inter-hospital communicationbefore transfer. In the second phase we found thatonly 14.5% of the transfers were done after notify-ing the receiving hospital. A study conducted byKellerman and Hackman from the United Statesreported this ratio as 45%.16 Bullard et al. reportedthis as 10.6% in Taiwan.4 It is thought that lack ofcompliance with this rule may be due to severalfactors.
Firstly, since there are no set rules in this regard,it may be difficult for the transferring physician tofind the right person to accept that patient.
Secondly, it is common for the transferring phy-sician to be told that there are no available ICUbeds. He may be sceptical about the sincerity of thisanswer and therefore chooses not to ask at all.
Thirdly, he may feel too busy to call the receivinghospital. We believe that if appropriate protocolsare used this should cease. Therefore, we are plan-ning to itemise the most frequently neglected trans-fer and referral rules and regulations observed inthis study and distribute these to the referringhospitals.
Perhaps, the most important of ACEPs rules oftransportation is the one about stabilisation beforetransfer. According to ACEP guidelines and theAmerican statute, Emergency Medical Treatmentand Active Labour Act (EMTALA) a patient cannotbe transferred unless he is appropriately stabilised.1
Airway management is accepted as a priority instabilisation of all patients. In the second phaseof our study, we found that of 57 patients needingadvanced airway management, appropriate airwaystabilisation was performed in 37 patients (64.9%).As shown in Table 2, airway management andrespiratory support was inadequate in 20 patients(35.1%). Dunn reported that 6% of the transferredcranial injury patients were hypoxic due to airwayproblems during transport.9 Henning from Australiareported that majority of the transferred paediatricpatients had serious hypoxaemia and hypoventila-tion.12 Bullard et al. reported that in their study 55%of the patients who needed endotracheal intubationprior to transfer had been transferred without intu-
bation.4 Martin et al. reported that 28% of hypoxia intrauma patients was due to inadequate oxygensupply during transport.18 In the second phase ofour study, 19 of the 32 trauma patients (59.3%) hadappropriate airway management before transfer.We believe that, although statistically significant,this rate is still unacceptably low.
Placement of a proper intravenous line andadministering fluids is the second most importantmeasure in the haemodynamic stabilisation of thetrauma patients after haemorrhage control.19 Ourfindings indicate that intravenous line placement inthe transferred patients improved significantly inthe second phase of the study from 67.8 to 76.7%.Reports in the literature are similar. Bullard et al.found that 20.7% of the transferred patients did nothave an intravenous line and 63.2% had inadequateintravenous access.4 Martin et al. reported inade-quate intravenous line rate as 29%.18 Another simi-lar study reported this rate as 8%.20 Our secondphase findings, in this respect, are generally con-sistent with the literature. Deane et al. reportedthat inadequate fluid resuscitation is one of themost important defects encountered in haemody-namic stabilisation.7 Dunn found serious hypoten-sion in 15% of the transferred patients.9 Lambertand Willet from UK reported that 4 of 21 patients(19%) had hypovolaemic shock due to inadequatefluid resuscitation during transport.17
Out of 61 trauma patients transferred in thesecond phase of our study, 17 (27.8%) had a cervicalcollar, 21 (34.4%) had a Foley catheter and 18(29.5%) had an NG tube. Comparison of these find-ings with the literature suggests that our compli-ance to trauma patient transfer rules is deficient.Martin et al. reported that 68% of trauma patientshad adequate cervical stabilisation.16 Olson et al.found that 92% of transferred trauma patients hadcervical collar, 89% had NG tube and 96% had urinarycatheter.20 Mayer, in his review of literature, foundthat appropriate stabilisation before transfer wasnot performed in 24—70% of the trauma patients.25
There are literature reports implying that mortalityrate may increase up to 40% in trauma patients inwhom appropriate stabilisation is not performed.11
Literature findings suggest that our compliancewith inter-hospital patient transfer rules is poorerthan most of the Anglo-American literature butcomparable with Taiwan or the United States beforethe 1980s.
In conclusion, there is a widespread deficiency incompliance with the guidelines for patient transferin our region. Inappropriate patient transfers causeimportant problems in modern health care systems.One of our aims at initiating the monthly conjointmeetings in our city among the EMS and emergency
862 E. Armagan et al.

department physicians was to establish betterpatient transfer conditions. We believe that wehave, at least partially, achieved this goal. How-ever, the benefit gained is hardly enough to justifythe effort. To improve other aspects of patienttransfers and thus improve quality of patient carewe are planning to continue these meetings withadditional efforts to increase participation andestablish and refine inter-hospital protocols forpatient transfers.
On the other hand, we believe that, these volun-tary and dedicated efforts are not enough toimprove compliance. Throughout the country, med-ical malpractice law and laws similar to the Amer-ican statue, EMTELA, ensuring the care of theemergency patients, must be enforced; officialpatient transfer protocols must be prepared bythe local health authorities or medical boards andcompliance with these protocols are strictly super-vised; quality of education in medical schools mustbe improved; the quality and quantity of primaryand secondary health care centres throughout thecountry must be increased; and public awarenessmust be raised in this and similar issues.
Acknowledgements
We thank Ilker Ercan for helping with the statisticalanalysis of the data.
Contributions. The study was conceived by RTand designed by EA and MGA. Data collection wasundertaken by MGA. Data analysis was undertakenby EA. ZE drafted the manuscript. All authors con-tributed to revision. RT takes the responsibility forthe paper as a whole.
References
1. American College of Emergency Physicians: appropriateinterhospital patient transfer. Ann Emerg Med 1993;22:761—7.
2. American College of Surgeons Committee on Trauma:Advanced Trauma Life Support for Doctors. Student CourseManual, 6th ed.; 1997. p. 65.
3. Breitsch LM. Economic patient dumping. Whose life is itanyway? J Leg Med 1989;10:433—78.
4. Bullard MJ, Liaw SJ, Chen JC, Hu PM. Compliance with thelaw and appropriate medical standards during interhospitaltransfers. J Formos Med Assoc 1998;97:770—6.
5. Condon RE. Appendicitis. In: Sabiston D, editor. Textbook ofsurgery. Philadelphia: WB Saunders Co.; 1981. p. 1048—64.
6. Crippen D. Critical care transportation medicine: newconcepts in pretransport stabilization of critically illpatient. Am J Emerg Med 1990;8:551—4.
7. Deane SA, Gaudry PL, Woods WP, Read CM, McNeil RJ.Interhospital transfer in the management of acute trauma.Aust N Z J Surg 1990;60:441—6.
8. Domeier RM, Hill JD, Simpson RD. The development andevaluation of a paramedic-staffed mobile intensive careunit for interfacility patient transport. Prehosp Dis Med1996;11:37—43.
9. Dunn LT. Secondary insults during the interhospital transferof head injured patients: an audit of transfers in Merseyregion. Injury 1997;38:427—31.
10. Etxebarria MJ, Serrano S, Ruiz Ribo D, Cia MT, Olaz F, LopezJ. Prospective application of risk scores in the interhospitaltransport of patients. Eur J Emerg Med 1998;5:13—7.
11. Friedman E. Problems plaguing hospitals: uninsured patienttransfers, tight funds, mismanagement and misperception.JAMA 1987;257:1850—7.
12. Hennig R. Emergency transport of critically ill children:stabilization before departure. Med J Aust 1992;157:66—7.
13. Hicks T, Danzi DF, Thomas DM, Flint LM. Resuscitation andtransfer of trauma patients: a prospective study. Ann EmergMed 1982;11:296—9.
14. Holmes MJ, Reyes HM. A critical review of urban pediatrictrauma. J Trauma 1984;24:253—5.
15. Kanter RK, Tompkins JM. Adverse events during interhospi-tal transport: physiologic deterioration associated withpretransport severity of illness. Pediatrics 1989;84:43—8.
16. Kellerman AL, Hackman BS. Emergency department patientdumping: an analysis of interhospital transfer to theregional center at Memphis, Tennessee. Am J Public Health1988;78:1287—92.
17. Lambert SM, Willet K. Transfer of Multiply injured patientsfor neurosurgical opinion: a study of the adequacy ofassessment and resuscitation. Injury 1993;24:333—6.
18. Martin GD, Cogbill TH, Landercasper J, Strutt PJ. Prospec-tive analysis of rural interhospital transfer of injuredpatients to a referral trauma center. J Trauma 1990;30:1014—9.
19. Martin RR, Bickell WH, Pepe PE, Burch JM, Mattox KL.Prospective evaluation of preoperative fluid resuscitation inhypotensive patients with penetrating truncal injury. JTrauma 1992;33:354—61.
20. Olson CM, Jastremski MS, Vilogi JP, Medden CM, Beney KM.Stabilization of patients prior to interhospital transport. AmJ Emerg Med 1987;5:33—9.
21. Schiff RL, Ansell DA, Schlosser JE, Idris AH, Morrison A,Whitman S. Transfers to a public hospital: a prospectivestudy of 467 patients. N Engl J Med 1986;314:552—7.
22. Stone JL, Lowe RJ, Jonasson O, Baker RJ, Barrett J,Oldershaw JB, et al. Acute subdural hematoma: directadmission to trauma center yields improved results. JTrauma 1986;26:445—50.
23. Strobos J. Tightening the screw: statutory and legal super-vision of interhospital patient transfers. Ann Emerg Med1991;20:302—10.
24. Weistein L. Bacterial meningitis. Med Clin North Am 1985;69:219—29.
25. Wuerz R, Meador S. Adverse events during interfacilitytransfer by ground advanced life support services. PrehospDis Med 1994;9:50—3.
Compliance with protocols in transferring emergency patients to a tertiary care centre 863





























