Embed Size (px)
Citation preview

Complicacions infeccioses en el malalt neutropènic
Montserrat Rovira
Servei Hematologia, Hospital Clínic
Barcelona, 27 de gener 2011
VI Conferència d´experts de la SOCMIC

tracte gastro-
intestinal
accessos vasculars
Gram (-)
Gram (+)
Origen principal de les infeccions en el malalt neutropènic

mucosa
decreased cell renewal
epithelial thinning
mucositis
infection
bone marrow
Micro-organisms
myelosuppression
neutropeniathrombocytopenia
discomfortpaindry mouthburning sensationloss of tasteerythemaulceration
Conseqüencies de la quimioteràpia
Cytostatic chemotherapy
infectiousdisease

4
Clinical Infectious Diseases 2009: 49: 1 – 44.

5
Mucositis:

6
Mucositis:
diarrhea
vomiting
nausea
bowel cramps
pain

7
Risc infecciós durant neutropènia i mucositis
Days
0 10 20 30 40
Neutropenia
Mucositis
colonisation
invasion

8
bacteraemi
a
GR
AN
UL
OC
YT
ES
{lo
g(1
09/L
)}
0.1
1
0
1
2
3
Gra
de o
f m
uco
sit
is
Mucositis
Neutropènia
Mucositis i neutropènia després quimioteràpia
bacterièmia

9
Infeccions bacterianes

Febrile episodes in neutropenic patients – EORTC trials–
0
20
40
60
80
100
73-76 77-80 80-83 83-85 86-88 89-91 91-93 94-96
year of EORTC trial
Gram (-ve)
Gram (+ve)
year of EORTC study
withmicrobiological
diagnosis
33%
withoutmicrobiological
diagnosis
67%

Febrile episodes in neutropenic patients *
0
20
40
60
80
100
91-92 93-94 95-96 97-98 99-00 00-04 04-'08
3.3 3.8 2.0 1.9 1.8
Ratio G (+ve) / G (-ve)
Gram (- ve)
Gram (+ ve)
1.7
* Hospital Clínic. Barcelona 1991-2008
1.1

12
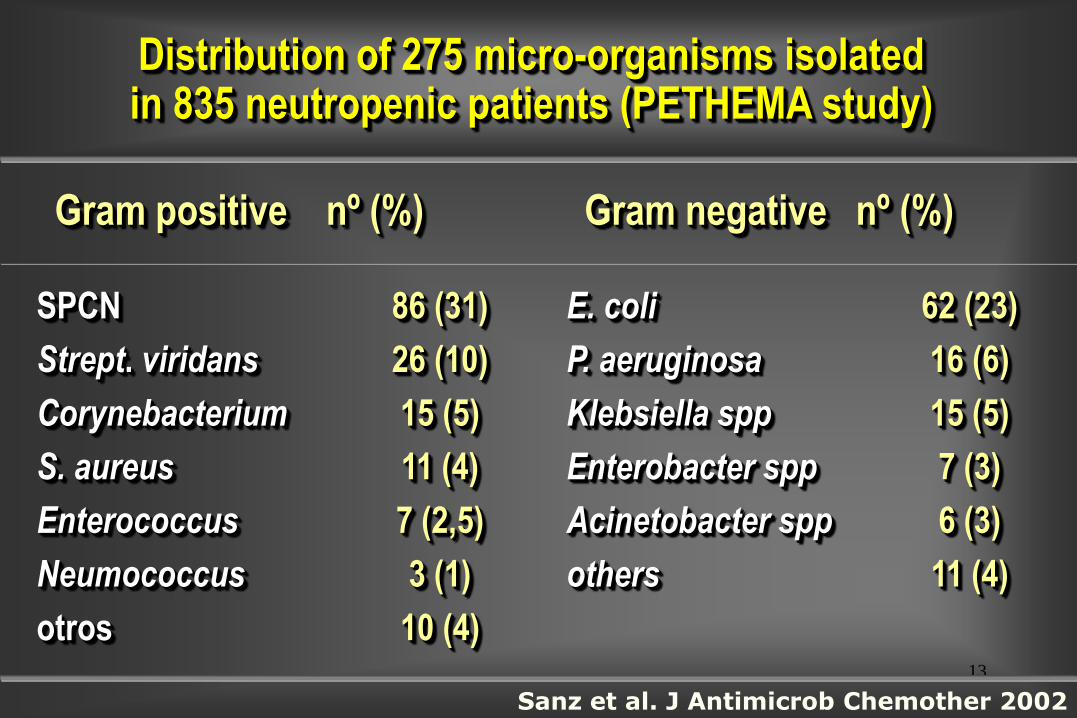
Distribution of 275 micro-organisms isolatedin 835 neutropenic patients (PETHEMA study)
Gram positive nº (%) Gram negative nº (%)
SPCN
Strept. viridans
Corynebacterium
S. aureus
Enterococcus
Neumococcus
otros
86 (31)
26 (10)
15 (5)
11 (4)
7 (2,5)
3 (1)
10 (4)
E. coli
P. aeruginosa
Klebsiella spp
Enterobacter spp
Acinetobacter spp
others
62 (23)
16 (6)
15 (5)
7 (3)
6 (3)
11 (4)
W/O microbiological diagnosis
67%
Sanz et al. J Antimicrob Chemother 2002
13
Distribution of 275 micro-organisms isolatedin 835 neutropenic patients (PETHEMA study)
Gram positive nº (%) Gram negative nº (%)
SPCN
Strept. viridans
Corynebacterium
S. aureus
Enterococcus
Neumococcus
otros
86 (31)
26 (10)
15 (5)
11 (4)
7 (2,5)
3 (1)
10 (4)
E. coli
P. aeruginosa
Klebsiella spp
Enterobacter spp
Acinetobacter spp
others
62 (23)
16 (6)
15 (5)
7 (3)
6 (3)
11 (4)
Sanz et al. J Antimicrob Chemother 2002
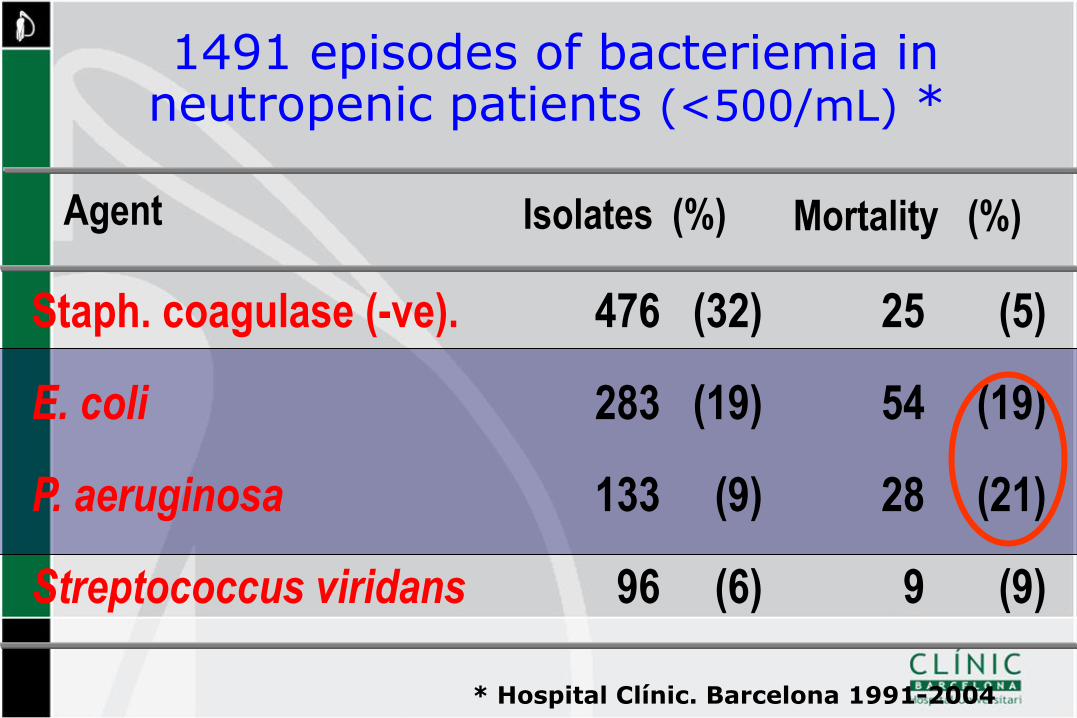
1491 episodes of bacteriemia inneutropenic patients (<500/mL) *
* Hospital Clínic. Barcelona 1991-2004
Agent Isolates (%)
Staph. coagulase (-ve).
E. coli
P. aeruginosa
Streptococcus viridans
476
283
133
96
(32)
(19)
(9)
(6)
Mortality (%)
(5)
(19)
(21)
(9)
25
54
28
9

Flora changes during severe disease evolution
Healthy
people
Severe
disease
Atb
>72 h
Long term
Atb - ICU
each
epithelium its
flora
flora
redistribution
flora
selection
multi-
resistant
flora
Haemophylus
S Aureus MS
Enterobacteria
Enterobact-R
non-ferm-GNB
S Aureus MR
Multi-R GNB
SPCN
Enterococcus
Candida
JM

16
Infeccions comuns durant neutropènia
39
40
41
Te
mp
era
ture
°C
Gra
nu
locyte
s (
log
10
1x 1
06/L
)
0.1
1
10
0 7 14 21 28 35 42 49 56 63
Days
bacteraemia skin lung

17
Infeccions comuns durant neutropènia
39
40
41
Te
mp
era
ture
°C
Gra
nu
locyte
s (
log
10
1x 1
06/L
)
0.1
1
10
0 7 14 21 28 35 42 49 56 63
Days
bacteraemia skin lung
• Bact gram(-):
E.coli, Klebsiella.,
pseudomona
• Staph. Aureus
•Aspergillus, mucor

18
Profilaxis

19
Profilaxis
39
40
41
Te
mp
era
ture
°C
Prophylaxis
Gra
nu
locyte
s (
log
10
1x 1
06/L
)
0.1
1
10
0 7 14 21 28 35 42 49 56 63
Days
quinolones
cotrimoxazole + colistin
nonabsorbable
none
Gram-negative
fluconazole
polyene
none
yeast
Posa/Itra/vori
amphotericin B
none
mould
Candins Candins

20
Bucaneve et al, NEJM 2005
Patients with acute Leukaemia
Probability of
Survival
free
of fever (%) Levo
Placebo
p<0.01
GID with levofloxacin

21
Imran et al. Eur J Clin Microbiol Infect Dis 2008; 27: 53–63
Meta-analysis randomized studies (2719 patients)
GID with quinolones

22
1st European Conference on Infections in Leukemia (ECIL)
ECIL1 Guidelines. EJC supplement 2007: 5(2)
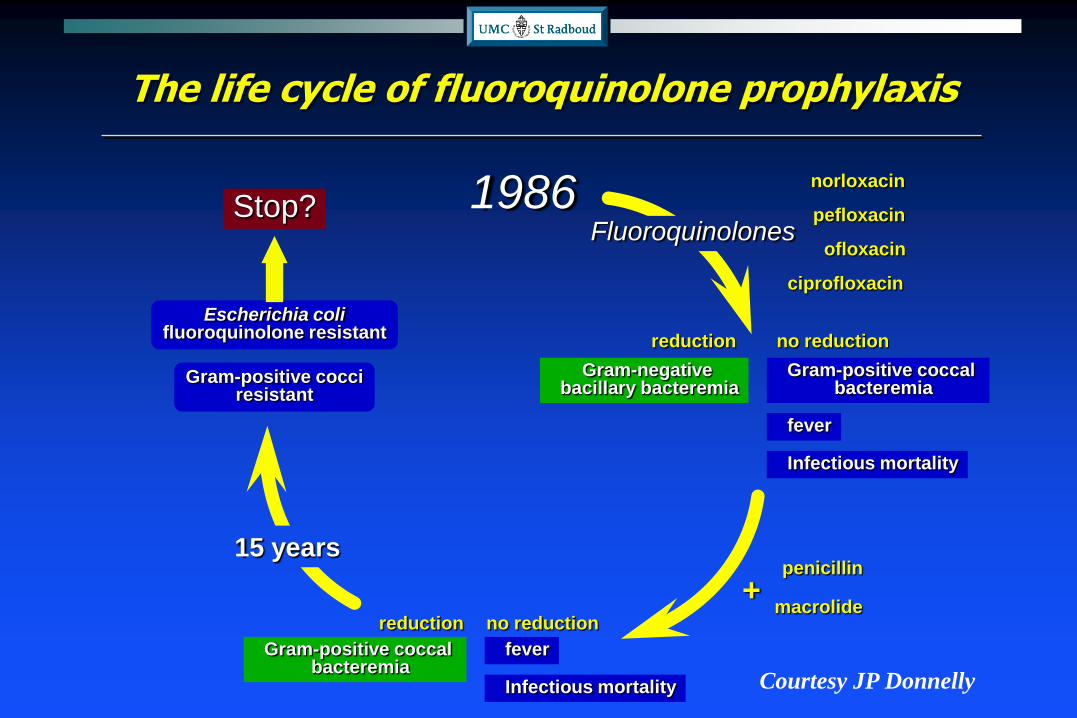
1986
The life cycle of fluoroquinolone prophylaxis
Gram-negative bacillary bacteremia
Gram-positive coccal bacteremia
fever
Infectious mortality
reduction no reduction
Gram-positive coccal bacteremia
fever
Infectious mortality
reduction no reduction
penicillin
macrolide+
Stop?
Escherichia colifluoroquinolone resistant
Gram-positive cocciresistant
Fluoroquinolones
ciprofloxacin
ofloxacin
norloxacin
pefloxacin
15 years
Courtesy JP Donnelly

Infeccions bacterianes
Tractament

25
A, B, C of treatment of febrile neutropenia
• It must be:
• Started immediately after onset of fever
• Based in an empirical approach
• Adapted to the flora usually observed in each
centre
• Adapted to the type of patient
• Adapted to the clinical situation
1
2
3

26
Distribution of 275 micro-organisms isolatedin 835 neutropenic patients (PETHEMA study)
Gram positive nº (%) Gram negative nº (%)
SPCN
Strept. viridans
Corynebacterium
S. aureus
Enterococcus
Neumococcus
otros
86 (31)
26 (10)
15 (5)
11 (4)
7 (2,5)
3 (1)
10 (4)
E. coli
P. aeruginosa
Klebsiella spp
Enterobacter spp
Acinetobacter spp
others
62 (23)
16 (6)
15 (5)
7 (3)
6 (3)
11 (4)
Sanz et al. J Antimicrob Chemother 2002
1

Flora changes during severe disease evolution
Healthy
people
Severe
disease
Atb
>72 h
Long term
Atb - ICU
each
epithelium its
flora
flora
redistribution
flora
selection
multi-
resistant
flora
Haemophylus
S Aureus MS
Enterobacteria
Enterobact-R
non-ferm-GNB
S Aureus MR
Multi-R GNB
SPCN
Enterococcus
Candida
JM
2

JM
Level of bacterial burden
pneumonia
meningitis
empiema
septic arthritis
endocarditis
osteomielitis
peritonitis, abscess
high > 107 UFC/mLlow < 105 UFC/mL
(urinary infection)
primary bacteraemia
catheter infection
B-lactamic B-lactamic + aminoglucoside
3 Adapted to clinical situation

29
• possible catheter infection
• severe mucositis
• colonization by MRSA
Summary: Initial empirical antibiotherapy in neutropenic patients with fever
antibioticclinical situation
- meropenem (AI)
- imipenem (AII)
- pipera.-tazo (AII)
- cefepime (AII)
• fever withoutclinical focality
- vancomycin
+AII
BIII
AII
JM

30
Initial empirical antibiotherapy in neutropenic patients with fever
antibioticclinical situation
- meropenem (AI)
- imipenem (AII)
- pipera.-tazo (AII)
- cefepime (AII)
• fever withoutclinical focality
• focality (tiphlytis, pneumonia,..)
• previous Atb treatment (>5-7d)
• colonization with resistant G(-ve)
• high incidence of ESBL
AII
BIII
BIII
+- aminoglucoside
JM
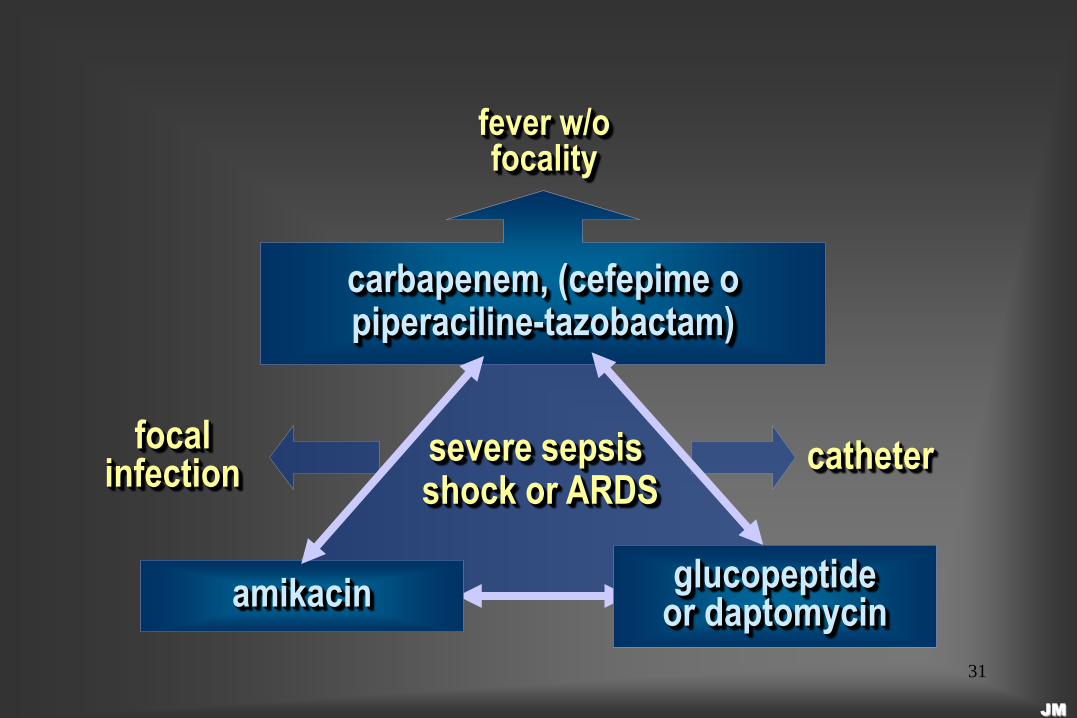
31
fever w/ofocality
severe sepsis shock or ARDS
amikacin
carbapenem, (cefepime opiperaciline-tazobactam)
glucopeptideor daptomycin
focalinfection catheter
JM
32
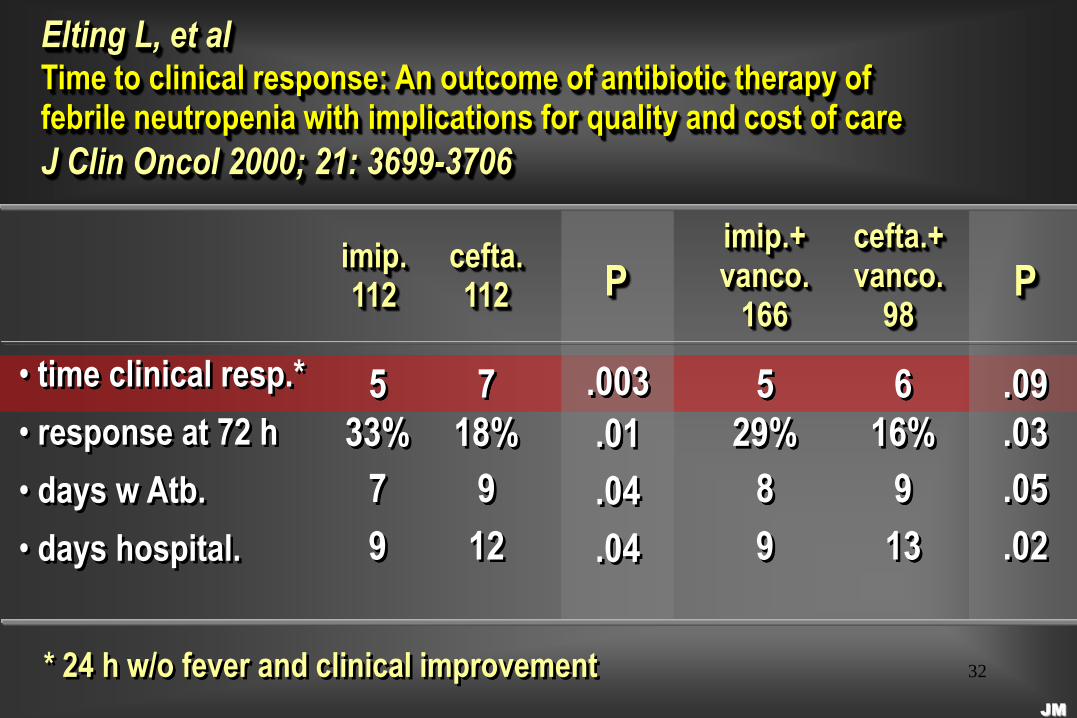
imip.112
Elting L, et alTime to clinical response: An outcome of antibiotic therapy offebrile neutropenia with implications for quality and cost of care
J Clin Oncol 2000; 21: 3699-3706
cefta.112
imip.+vanco.
166
cefta.+vanco.
98P P
• time clinical resp.*
• response at 72 h
• days w Atb.
• days hospital.
5
33%
7
9
.003
.01
.04
.04
7
18%
9
12
5
29%
8
9
6
16%
9
13
.09
.03
.05
.02
* 24 h w/o fever and clinical improvementJM

33
Infeccions fúngiques

34
Pre-emptiveantifungal
based on lab or imagine
tests
Therapeutic approaches to IFI in neutropenic patients
Prophylaxisantifungal to all patients (primary or secondary)
Empiricalantifungal due
to fever unresponsive to
antibact.
Treatmentantifungal based on proven IFI
Probability of IFI0% 100%
Anticipated
Early treatment
~ 80% unnecessary treat. (IFI incidence <20%)

35
0
5
10
15
20
25
30
Pizzo EORTC Pizzo EORTC
No therapy AmB-d
Empirical Ampho-d vs no therapyPizzo et al, Am J Med 1982 / EORTC, Am J Med 1989
4/16
1/18 4/64
3/16
1/18 4/64
0/68
Incidence IFI Mortality IFI
%
1/68

36
Empirical antifungal therapy
Double-blind clinical trialsAuthor,
year
Drugs
compared
Composite
Endpoint
Outcome
baseline
IFI
Break-
trough
IFI
Nephro-
toxicity
White
1998
ABCD
vs AmB-dNS NS NS Less
Walsh,
1999
Lipo-AmB
vs. AmB-dNS NS Less Less
Wingard,
2000
ABCD vs.
Lipo-AmBNS NS NS More
Walsh,
2002*
Vori vs.
Lipo-AmBNS NS Less NS
Walsh,
2004
Caspo vs.
Lipo-AmBNS Better NS Less
* open trial
38
ECIL recommendations
Empirical antifungal therapy in persistent febrile neutropenic patients
BII
Early therapy
Most patients do not have an IFIAdverse effects
Development of resistancesCosts
Better lab + imaging techniques

Neutropenia - bridging the gap with supportive care
Mucosal barrier injury
Antimicrobial agents
Other medication
Diagnosis
Blood products
Nutrition
Nursing
Courtesy JP Donnelly

40
Neutropènia /
Disf. Neutr.
Inmunodef.
Cel.lular
Inmunodef.
Humoral
Leucèmies agudes +++ / + + / - -
Mielodisplasies ++ / +++ + / - -
Linfoma – LLC-
Mieloma múltiple
+ / - ++ ++
Trasplant autòleg ++ / - ++ +
Trasplant
al.logènic
+++ / - +++ +++
No tots els pacients hematològics a risc
d´infeccions estàn neutropènics!!!!!

41
Impaired T-cell function: responsible agents
Bacteria
Listeria
Mycobacteria
Legionella
Nocardia
Brucella
Salmonella
Fungi
Pneumocystis j.
Cryptococcus
Histoplasma
Candida
Aspergillus
Blastomyces
Zygomicosis
Virus
Herpes
Respiratory virus
JC, EBV
Parasites
Toxoplasma
Giardia

42
• Capsulated bacteria
Streptococcus pneumoniae
Haemophilus influenzae
Neisseria meningitidis
• Parasites
Babesiosis
Impaired B-cell function: responsible agents

43
Agraïments:
• Dr E. Carreras
• Dr J. Mensa
• Dr JP. Donnelly
Moltes gràcies per la seva atenció!!!!