-
7/31/2019 Comprehensive Examination of Cadiovascular System
1/19
-
7/31/2019 Comprehensive Examination of Cadiovascular System
2/19
Introduction
at the start
Wash your hands, introduce yourself, obtain consent.
Patient position:
Always make sure the patient is comfortable. Sit the
patient up at 45o. Obtain adequate exposure - thepatient should
be exposed up to the waist. For femalepatients, bras should ideally
be removed, or else it can bevery difficult to palpate or
auscultate at the apex.
-
7/31/2019 Comprehensive Examination of Cadiovascular System
3/19
From the end of the bed:
- Look at the patient: oxygen masks / signs ofrespiratory
distress / pain / cyanosis / lines / scars (eg.pacemaker), etc.
- Look around the bed: medication (eg. GTN sprays) /fluids /
walking aids / cigarette packets, etc.
-
7/31/2019 Comprehensive Examination of Cadiovascular System
4/19
Peripheral signs
Hands:
- Tremor: Can be caused by thyrotoxicosis - can cause Atrial
Fibrillationand congestive heart failure (CHG).
- Clubbing: Causes - congenital (cyanotic) heart disease,
sub-acuteinfective endocarditis.
- Tar staining: Smokers. - Nail bed capillary pulsation:
'Quinke's sign' of Aortic Regurgitation. - Splinter haemorrhage:
Endocarditis, acute glomerulonephritis. - Osler nodes: Small and
painful red-brown subcutaneous papules on
the pulps of the fingers or toes (infective endocarditis). -
Jane way lesions: Small and non-tender
erythematous/haemorrhagic
macules on the palms/soles of feet(infective endocarditis). -
Arachnodactyly: Long slender hand and fingers - Marfan's syndrome.
- Xanthomata: Yellowish macular deposits found on the tendons
with
hypercholesterolaemia. - Koilonychia: Spoon-shaped nails caused
by iron deficiency anaemia
(which can cause heart failure).
-
7/31/2019 Comprehensive Examination of Cadiovascular System
5/19
Pulse
General tips
- Note the following: rate / rhythm / character /symmetry
(between left & right side).
- Always palpate: Radial and carotid pulses.- Consider
palpating: Other relevant pulses (brachial, abdominalaorta,
femoral, popliteal, posterior tibial and dorsalispedis). The
brachial pulse should certainly be used ifasked to measure the
Blood Pressure. It may also be
worth routinely palpating for radio-femoral delay (asign of
coarctation of the aorta).
-
7/31/2019 Comprehensive Examination of Cadiovascular System
6/19
What to do:
. 1. Palpate the radial pulses of both arms at the same time.
Initiallycount the rate (ideally you should do this for 30seconds).
Also be feelingfor radio-radial differences/delay (a feature of
aortic dissection).
2. Note the following features of the pulse:
Rate: Tachycardia (>100bpm) can be caused by anxiety, pain,
congestivecardiac failure, pulmonary emboli, hyperthyroidism,
anaemia,fever/sepsis, medications (eg. beta-agonists such as
Salbutamol), etc.Bradycardia (
-
7/31/2019 Comprehensive Examination of Cadiovascular System
7/19
Pulse count. Character: A collapsing pulse (also known as a
'water-hammer' pulse)
is jerky, with a full expansion phase followed by a sudden
collapse uponraising the arm to above heart level (seen mainly with
AorticRegurgitation, however other cause scan include a Patent
Ductus
Arteriosus, thyrotoxicosis, A-V fistulae, pregnancy, Paget's
disease andanaemia). An anecdotic (slow rising) pulse is seen in
Aortic Stenosis.Pulses alternant (regular rate, alternating
amplitude that varies frombeat-to-beat) is seen in Left Ventricular
Failure. Pulses bisferiens (2strong systolic peaks separated by a
mid-systolic 'dip') is seen in aortic
valve disease and hypertrophic cardiomyopathy. A diacrotic pulse
(twosystolic and diastolic peaks) is seen in septic, hypovolaemic
and
cardiogenic shock. Pulsus paradoxus is seen in severe asthma,
cardiactamponade and massive Pulmonary Emboli. The pulse pressure
normalfalls with inspiration, however when this is
exaggerated(>10mmHgdifference) then this is deemed pulsus
paradoxus.
-
7/31/2019 Comprehensive Examination of Cadiovascular System
8/19
Pulse count. 3. Mention to the examiner at this point, that you
would ideally like to measure the
Blood Pressure. If they want to you to do this, then they will
hand you asphygmomanometer. If they wish you to carry on with your
examination, they willusually tell you what the blood pressure is.
Don't ignore what they say - it could give
you a clue as to the diagnosis! A narrow pulse pressure (pulse
pressure=systolic-
diastolic)is a feature of aortic stenosis. A widened pulse
pressure is a feature ofaortic regurgitation.
4. If you wish to feel for radio-femoral delay (seen in
coarctation of the aorta), thendo so at this stage. Remember to
explain to the patient what you are doing before
you just reach for their groin!
5. Palpate the carotid pulse before you examine the face, or
else you may forget later.Never palpate both sides at once -
inducing a spot of syncope in your older patientsis not something
you ideally want to do in an exam. Note the same features of
thispulse. Some of the signs may be easier to determine in this
pulse, as compared tothe radial pulse.
-
7/31/2019 Comprehensive Examination of Cadiovascular System
9/19
Face General features:
- Anxious / apprehensive looking faces: pain, anxiety,
respiratory distress (could be a sign of aMyocardial Infarction or
angina-related chest pain, Pulmonary Embolus, Pulmonary oedema /
heartfailure, and various cardiac arrhythmias, including AF,
supraventricular tachycardia and ventriculartachycardia.
- Colour: Many conditions can lead to a change in the normal
colour of the skin, particularlynoticeable at the face. These
include: Malar flush: Red areas on the upper cheeks - seen in
MitralStenosis and similar to the butterfly rash of Systemic Lupus
Erythematosus. Polycythemia: causes adark reddish appearance to the
skin. It is important, as it can be a cause of thrombotic events,
infarctsandhypertension. Haemochromatosis: also known as 'bronze
diabetes' due to the deposition of iron(can lead to
cardiomyopathy). Addison's disease: dark buccal pigmentation (can
be a cause ofhypotension). Carcinoid syndrome: Release of 5-HT
leads to flushing and hypotension.
- Shape: Classical 'moon-face' of Cushing's disease (a cause of
hypertension).
- Skin texture: Coarse & dry 'toad face' of hypothyroidism
(can cause bradycardia).
- Central cyanosis: A bluish tongue suggests either a right to
left intra-cardiac shunts or lung disease.
- Head shape: Paget's disease: features a large head (can lead
to high-output failure). Marfan'ssyndrome (long narrow face -
associated with aortic regurgitation). Williams syndrome (small
elf-like
forehead, turned up nose, low set ears - associated with Aortic
Stenosis). Noonan's syndrome (widelyset eyes, web neck - associated
with Pulmonary Stenosis.
-
7/31/2019 Comprehensive Examination of Cadiovascular System
10/19
Eyes: - Roth spots: Retinal haemorrhages (white/pale centres),
usually seen on
fundoscopy. Caused by microemboli (bacterial endocarditis).
Roth's spots may
be observed in leukaemia, sub-acute bacterial endocarditis,
ischemic eventsassociated with elevated venous pressure and
systemic vascular conditions withcapillary fragility.
- Xanthelasma: Yellowish macules on the eyelids (similar to
tendonxanthomata) seen in hypercholesterolaemia.
- Eyelid (periorbital) oedema: Seen in hypothyroidism, nephrotic
syndrome,
etc. - Exophthalmos: Along with other signs such as eyelid
retraction, is a feature of
(hyper)thyroid eye disease (which causes AF and can lead to a
high-outputheart failure).
- Corneal arcus senilis: A grey-ish ring around the outer
cornea. Whilst
relatively common in the elderly, in young people it can
indicateshypercholesterolaemia.
- Blue sclera: Seen in Marfan's and Ehlers-Danlos syndromes (is
associatedwith Aortic Regurgitation, as well as Mitral Valve
Prolapse, and Atrial SeptalDefects.) Lens subluxation is another
feature of Marfan's.
- Argyll Robertson Pupil: The 'prostitute's pupil' -
accommodates, but does not
react (to light). Seen in neurosyphilis (which can cause Aortic
Regurgitation).
-
7/31/2019 Comprehensive Examination of Cadiovascular System
11/19
JVP/CAROTID WAVEFRONT
How to perform:
- Get the patient to turn their head away from you and hold it
still. You should then look 'along' the skin(i.e.. with your line
of sight almost in line with the neck surface). Look for the
internal jugular (the lessobvious waveform) rather than the
external (easily seen, superficial).The JVP can be differentiated
fromthe carotid pulse by a number of features (see below). A quick
test is to confirm if it can be occluded bypressure - the carotid
pulse cannot be, whilst the JVP is occluded by this manoeuvre.
- Remember that the JVP will be affected by the patient's
position. It is usually described as theequivalent of a column of
fluid - i.e.. how far the 'column' of the JVP rises above the
manubriosternalangle.- To 'accentuate' the JVP, you can gently
press down on the abdomen (hepato-jugular reflux - raises
intra-abdominal pressure and enhances venous return). Make sure the
patient has no abdominal pain beforeyou do this.
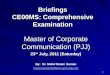
Waveform:
- A-wave: Atrial contraction (systole).- C: Tricuspid valve
closure. Start of ventricular systole. Coincides with palpable
carotid pulse and first
heart sound.
- - X-descent: Ventricular systole.- - V: End of ventricular
systole and start of atrial filling (with closed tricuspid valve).-
- Y-descent: Tricuspid valve opens.
-
7/31/2019 Comprehensive Examination of Cadiovascular System
12/19
JVP COUNT.
JVP vs Carotid waveform:
FEATURES JVP CAROTID PULSE
WAVES 3 1
ABDOMINALPRESSURE RAISED NO EFFECT
FINGER PRESSUREObliterates waveform NO EFFECT
RESPIRATIONDecreases on inspiration(Kussmaul's sign is a
paradoxicalrise in JVP)
NO EFFECT
POSITIONDEPENDANT?
Yes - lower with sitting up moreNO EFFECT
-
7/31/2019 Comprehensive Examination of Cadiovascular System
13/19
I i
-
7/31/2019 Comprehensive Examination of Cadiovascular System
14/19
Inspection
Look for:
As before, look carefully, ensuring you do not missany scars
(eg. median sternotomy / smaller
thoracic scars from valve repairs). Also, lookfor anysigns of a
pacemaker. These are normally found inthe 'upper-outer' quadrant of
the pectoral area.These are usually small and thin box
likestructures
just deep to the skin. Also look for abnormalities ofthe chest
wall (eg. pectus excavatum in Marfan's).
-
7/31/2019 Comprehensive Examination of Cadiovascular System
15/19
Palpation
Feel for:
- Apex beat: This is defined as the most inferior and lateral
site at which thepulse can be palpated. It is located at the 5th
left intercostal space, in the mid-clavicular line, and is the
'most forceful' palpable pulsationof the heart. Lateraldeviation
suggests left ventricular enlargement. If you cannot feel it then
tryagain (dextrocardia is a classic exam trick and it can be very
embarrassing tosay you felt the apex when it was actually way over
the other side...). Animpalpable apex can be caused by 'DOPES':
Death, Obesity, Pericarditis,Emphysema/COPD, Situs inversus. Normal
apex beats are brief outwardimpulse. There are many confusing
wordsused to describe abnormal apex beats- do not try and
understand or remember these. Just remember: 'tapping' inMitral
Stenosis and 'hyperdynamic' in Aortic Stenosis.
- Parasternal heave: Use the lateral edge of your palm. Palpate
either side of thesternal border. Palpable upwards movements are
suggestive of RightVentricular Hypertrophy, although they can also
be felt in patients with thinchest walls.
- Thrills: Palpable murmurs. Again, using the lateral edge/palm
of your hands,
feel at the upper chest (just below the clavicles).
-
7/31/2019 Comprehensive Examination of Cadiovascular System
16/19
Auscultation
Listen for:
- Listen at the 4 main areas: Aortic (2nd right intercostal
space),Tricuspid (lower left sternal edge), Pulmonary (2nd left
intercostalspace) and Mitral (apex beat). Always start at the apex.
A good way toremember the order, is the mnemonic 'At The Post
Mortem' (Aortic,
Tricuspid, Pulmonary, Mitral), going diagnonally up-and-down
thechest. Always palpate a 'central' pulse (the carotid, or
alternatively thesubclavian - can be easier to palpate and is found
just above the medialborder of the clavicle), at the same time.
This will help you to time anymurmurs.
- Heart sounds: 1st sound = mitral and tricuspid closure, 2nd
sound =aortic and pulmonary closure. Listen at the apex for extra
heart sounds:
3rd sound = immediately after the 2nd sound - like 'ken-tucky'
(normalin young patients, suggests over-rapid ventricular filling
with a failureof the ventricle to relax, eg. in heart failure,
thyrotoxicosis), 4th sound= immediately before the 1st sound - like
'tenne-ssee' (alwaysabnormal, cause by a stiff ventricle, found in
left ventricularhypertrophy, hypertrophic cardiomyopathy, acute
infarction, etc.)
-
7/31/2019 Comprehensive Examination of Cadiovascular System
17/19
AUSCULTATION COUNT.- Murmurs:At the apex, use the bell and then
the diaphragm. The bell
will be useful for low frequency diastolic murmurs. Get the
patient to lean
on their left side (left lateral position) whilst auscultating
at the apex.This will accentuate the mid-diastolic murmur of mitral
stenosis.Remember to listen in the axilla for radiation of mitral
murmurs.- Listen at the carotids, for both, bruits and radiation of
aortic areamurmurs. Tell the patient to hold their breath so breath
sounds do not
impede what you can hear. Ejection systolic murmurs heard at the
aorticarea but that do not radiate to the carotids may be cause by
aortic(calcific) sclerosis rather than stenosis.- Get the patient
to lean forwards, whilst holding your stethoscope at thelower left
sternal edge. Get the patient to take a deep breath in, breath
allthe way out, then hold it there. Listen during held expiration
for the earlydiastolic murmur of aortic regurgitation.
- See the 'murmurs' notes for more information on cardiac
murmurs.
- Finally, listen at the lung bases (posteriorly) for signs of
pulmonary
oedema (left sided heart failure).
-
7/31/2019 Comprehensive Examination of Cadiovascular System
18/19
To complete your examinationAlso examine:
- Feel the pre-tibial area for pedal pitting oedema (sign of
right heart failure).- Palpate the peripheral pulses for
abnormalities (eg. aneurysms). Start fromthe abdominal aorta, then
palpate bilaterally at the femorals, popliteal,posterior tibial and
dorsalis pedis). You can usually skip this step inexaminations
unless specifically asked - saying to the examiner that'tocomplete
my examination, I would like to palpate the peripheral pulses'
isusually enough.
- Also mention that you would like to palpate the abdomen for
signs of rightheart failure ('smooth' hepatomegaly and hepatic
pulsatility).
Finally:
- Ask for the following investigations to complete your
examination:Temperature (raised in endocarditis), Urine Dipstick
(blood in hypertension
or endocarditis, glucose in diabetes), Blood Pressure (if not
already done so),Chest X-ray(approximate heart size, rib notching
in coarctation of the aorta),and a cardiac echo scan (especially if
a murmur was heard or there was anyevidence of heart failure).
-
7/31/2019 Comprehensive Examination of Cadiovascular System
19/19
Presenting your findings
Example presentation:
On examination, Mrs Jones appeared mildly short of breath at
rest.She was on 5L of Oxygen through nasal prongs. She had tar
stainingon her hands, and there was a packet of cigarettes by the
side of thebed, suggesting that Mrs Jones is a smoker. Her pulse
was slowrising, and her blood pressure was 96/70, demonstrating a
narrowpulse pressure. There were no other peripheral stigmata
ofcardiovascular disease. On palpation, her apex beat was present
andhyperdynamic in character. On auscultation, both heart
soundswere present, however the second heart sound was quiet. There
wasan ejection-systolic murmur that was loudest at the 2nd
right
intercostal space, and that radiated to the carotids. There were
nosigns of heart failure. In summary, these findings are
consistentwith a diagnosis of aortic stenosis.