Embed Size (px)
Citation preview

Congenital Larynx Lesions &
Stridor Evaluation
Dr. Vishal Sharma

Epidemiology
• 80 – 85 % children < 3 yrs with stridor have
congenital etiology for stridor
• 60 % of these anomalies are in larynx
• 20-25 % are anomalies of trachea + bronchi
• 45% patients have more than 1 anomalies

Supraglottis: Laryngomalacia, Supraglottic web,
Saccular cyst, Congenital
laryngocoele, Supraglottic cleft
Glottis: Vocal cord paralysis, Glottic web,
Glottic stenosis, Cri-du-chat syndrome
Subglottis: Subglottic stenosis, Subglottic web,
Subglottic hemangioma
Etiology

Common congenital lesions
• Laryngomalacia (60%)
• Congenital vocal cord paralysis (20%)
• Congenital subglottic stenosis (15%)
• Subglottic hemangioma (1.5%)

Supra-glottic
abnormalities

• Most common congenital laryngeal anomaly
Etiology:
• Exact cause is not known
1. Mal-development of cartilaginous structures
2. Gastro-esophageal reflux disease
3. Immaturity of neuromuscular control
Laryngomalacia

Clinical presentation• Symptoms begin few weeks after birth, progress
over 9-12 months & resolve by 2 years
• Inspiratory stridor: 1. increased by: supine
position, feeding, resp. infection & exertion (crying).
2. relieved by: neck extension & prone position.
• Phonation & cry are normal. Feeding difficulties,
failure to thrive, dyspnoea & cyanosis are rare.

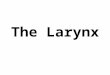
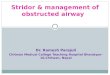
Flexible laryngoscopy
• Elongation + longitudinal folding of epiglottis (omega
shaped, ), falls postero-inferiorly on inspiration
• Redundant bulky arytenoids prolapse anteriorly &
medially on inspiration. Shortening + medial collapse
of aryepiglottic folds. Expiration results in expulsion
of these structures with free flow of air
• Rigid bronchoscopy GA: exclude other anomaly

Omega-shaped epiglottis

Flexible laryngoscopy

Inspiration vs. Expiration

Treatment
1. 99% cases: reassurance, sleep in prone
position
2. Treatment of gastro-esophageal reflux disease
3. Surgical management (for 1% cases):
a. Emergency Tracheostomy: kept till 2 yrs age
b. Epiglottoplasty: cautery or laser assisted

Epiglottoplasty for laryngomalacia

Problem: tubular epiglottis

Rx: trimming of epiglottis

Problem: medial collapse of corniculate cartilages

Rx: removing cartilage + redundant mucosa

Problem: posterior displacement of epiglottis

Rx: epiglottopexy

Epiglottopexy

Problem: short ary-epiglottic folds

Rx: division of ary-epiglottic folds

Pre-op vs. Post-op

Problem: medial collapse of ary-epiglottic fold

Rx: removing wedge of ary-epiglottic folds

Congenital laryngocoeleAir filled dilatation of ventricular sinus of Morgagni
C/F: 1. Hoarseness or respiratory distress
2. Neck swelling es on Valsalva maneuver
Investigation: 1. Plain X-ray soft tissue neck
2. Flexible laryngoscopy
Treatment: 1. Endoscopic marsupialization
2. External excision by thyrotomy

Swelling es with Valsalva

Types of laryngocoele
• Internal (20%): contained entirely within endolarynx
with bulge in false vocal fold & aryepiglottic fold
• External (30%): only neck swelling without visible
endolaryngeal swelling
• Combined (50%): Also extends into anterior triangle of
neck through foramen for superior laryngeal nerve &
vessels in thyrohyoid membrane. Dumbbell shaped.

Types of laryngocoele
Internal External Combined

X-ray neck A.P. view

Flexible laryngoscopy

CT scan: mixed laryngocoele

Endoscopic marsupialization

External approach

Congenital saccular cyst
• Due to obstruction of orifice of saccule in
laryngeal ventricle
• 40% congenital cysts found within hours of birth
• 95% of infants have symptoms within 6 months
• C/F: Inspiratory stridor improves on extension of
head, cyanosis, feeding problem & failure to thrive

Anterior saccular cystSmaller in size, project into laryngeal lumen in
anterior ventricular region

Lateral saccular cystLarger, present as bulge in false vocal fold or
ary-epiglottic fold, extend into neck

Treatment
1. Emergency tracheostomy for acute stridor
2. Endoscopic de-roofing or marsupialization:
cold knife Laser-assisted
3. Endoscopic incision & drainage
4. Total excision:
endoscopic laryngofissure approach

Glottic abnormalities

Congenital vocal cord palsy

Etiology1. Idiopathic: most common
2. C.N.S. Lesions: Arnold-Chiari malformation,
cerebral palsy, hydrocephalus, myelo-
meningocele, spina bifida, hypoxia
3. Birth trauma: a. cervical spine
b. recurrent laryngeal nerve
4. Mediastinum lesions: a. tumors
b. vascular malformation

Clinical FeaturesUnilateral paralysis: 4 times common
Hoarse, breathy cry aggravated by agitation
Feeding difficulty Aspiration
Bilateral paralysis:
Biphasic stridor (worsens on agitation) + near-
normal phonation: abductor paralysis
Lung aspiration + aphonia: adductor paralysis

Diagnosis:
1. Flexible laryngoscopy shows vocal fold palsy
2. Rigid bronchoscopy GA: other anomaly
Treatment:
Bilateral paralysis:
1. Vocal cord lateralization 2. Cordotomy
3. Cordectomy 4.Subtotal arytenoidectomy
5. Tracheostomy
Unilateral paralysis: Observation

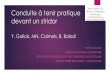
Fibre-optic laryngoscopy
paralyzed vocal fold foreshortened, lateralized & flaccid

B/L abductor palsy
Inspiration Expiration

Vocal cord lateralization (laterofixation / cordopexy)

Cordectomy

Cordectomy + lateralization

Posterior cordotomy

Arytenoidectomy

Cordotomy + arytenoidectomy

Glottic web
Treatment:
Endoscopic division
with knife / laser &
insertion of
McNaught laryngeal
keel

Glottic stenosis
Treatment:
Endoscopic division
with knife / laser &
insertion of
McNaught laryngeal
keel

McNaught Keel

Cri-du-chat syndrome• Cri – du – chat means cry of the cat
• Partial depletion of short arm of chromosome 5
• High pitched mewing stridor
• Diamond shaped glottic space, narrow vocal
cords, curved & elongated supraglottis
• Treatment: 1. Supportive care
2. Genetic counseling

Sub-glottic abnormalities

Congenital subglottic stenosis• Definition: diameter of subglottic lumen < 4 mm in
term infant & < 3 mm in pre-term infant
• Etiology: Incomplete recanalization of laryngo-
tracheal tube during 3rd month of
gestation
• Types: 1. Membranous: more common & mild form
2. Cartilaginous: less common & severe form
• Clinical presentation: Symptoms appear in first
few months of life. Biphasic stridor. Cry is normal.

Flexible laryngoscopy

Radiology

TreatmentMost cases resolve spontaneously by 4 years.
Tracheostomy for significant stridor. Tube
removed by 4 years when subglottic space widens.
Laser ablation for membranous stenosis < 5 mm.
Crico-tracheal resection & Laryngo-tracheo-plasty
in patients who could not be decannulated.

Tracheostomy

Laryngo-tracheoplasty

Subglottic hemangioma• Capillary hamartomas
• Symptoms appear by age 2-12 months
• Biphasic stridor, barking cough & hoarse cry
• 50% have cutaneous hemangiomas of head & neck
• Flexible laryngoscopy: unilateral or bilateral lesion
• Located postero-laterally in subglottis submucosa,
pink-blue in color, sessile & easily compressible

Flexible laryngoscopy

Management
Observation: for small lesions without stridor
Tracheostomy: for significant airway obstruction.
Tube kept till 5 years.
Specific treatment:
1. Laser ablation 2. Cryosurgery
3. Sclerosing agent: intra-lesional injection
4. Open surgical excision

Subglottic web
Treatment:
Endoscopic
division with knife
/ laser & insertion
of McNaught
laryngeal keel

Evaluation of Stridor

Stridor vs. Stertor
• Stertor is noisy respiration due to turbulent air
flow through partially narrowed air passage above
larynx
• Stridor is noisy respiration due to turbulent air
flow through partially narrowed air passage at or
below level of larynx

Etiology for stertor
Nasal: choanal atresia, ethmoid polyps
Mandible: Pierre Robin syndrome
Tongue: macroglossia, lingual thyroid
Pharynx: adeno-tonsillar hypertrophy, retro-
pharyngeal abscess, neoplasm
Miscellaneous: Ludwig’s angina, Maxillo-facial #

Etiology for stridor

Congenital Acquired
Laryngomalacia 1. Inflammatory:
Vocal cord palsy Acute epiglottitis, croup,
Subglottic stenosis laryngeal edema, T.B.
Subglottic hemangioma 2. Trauma: accidental,
Laryngeal web & atresia iatrogenic, heat, chemical
Laryngeal cyst 3. Neoplasm
Vascular compression on 4. Foreign body
trachea 5. B/L vocal cord palsy

Causes of B/L vocal cord palsy
• Thyroid surgery
• Ca thyroid
• Cancer cervical esophagus
• Cervical lymphadenopathy

History Taking1. Congenital or acquired after birth
2. Present only during sleep stertor
3. Related to feeding aspiration due to laryngeal
paralysis, esophageal
obstruction
4. Foreign body, blunt injury, endoscopy, intubation
5. Sudden onset foreign body, injury, infection
6. Long standing + progressive Laryngomalacia,
laryngeal stenosis,
neoplasm

1. Respiratory timing of stridor:
Inspiratory supraglottis or pharynx
Biphasic glottis, subglottis or cervical trachea
Expiratory lower trachea, bronchi or alveoli
2. Signs of airway resistance: nasal flaring, intercostal /
subcostal / supraclavicular recession, cyanosis
Physical Examination

Physical Examination
3. Associated fever: inflammatory cause
4. Stridor disappears in prone position:
laryngomalacia, macroglossia, micrognathia,
vascular compression of trachea
5. Resting respiratory rate: look for tachypnoea
6. Resting heart rate: look for tachycardia

Investigations1. Arterial blood gas analysis: for hypoxia
2. X-Ray soft tissue neck: for epiglottitis, stenosis
3. X-Ray chest: for mediastinal lesion
4. Flexible laryngoscopy & bronchoscopy
5. Direct laryngoscopy & rigid bronchoscopy
6. C.T. scan of neck & chest
7. M.R.I. of neck & chest
8. Barium swallow & esophagoscopy

Thank You