Embed Size (px)
Citation preview

einstein. 2009; 7(4 Pt 1):529-31
Learning By images
Congenital mesoblastic nephromaNefroma mesoblástico congênito
Fábio de Vilhena Diniz1, Ronaldo Hueb Baroni2, Yoshino Tamaki Sameshina3, Rodrigo Gobbo Garcia4, Danielle Azevedo Chacon5, Amilcar Martins Giron6, Marcelo Buarque de Gusmão Funari7
Study carried out at Hospital Israelita Albert Einstein – HIAE, São Paulo (SP), Brazil.1 MD of Hospital Israelita Albert Einstein – HIAE, São Paulo (SP), Brazil.2 PhD; Radiologist of Hospital Israelita Albert Einstein – HIAE, São Paulo (SP), Brazil.3 MD of Hospital Israelita Albert Einstein – HIAE, São Paulo (SP), Brazil.4 MD of Hospital Israelita Albert Einstein – HIAE, São Paulo (SP), Brazil.5 MD of Hospital Israelita Albert Einstein – HIAE, São Paulo (SP), Brazil.6 MD of Hospital Israelita Albert Einstein – HIAE, São Paulo (SP), Brazil.7 Radiologist; Head of the Imaging Department at Hospital Israelita Albert Einstein – HIAE, São Paulo (SP), Brazil.
Corresponding author: Ronaldo Hueb Baroni – Alameda Jaú 731 – apto. 172 – Cerqueira César – CEP 01420-001 – São Paulo (SP), Brasil – Tel.: 11 3251-1006 – e-mail: [email protected]
Received on: May 4, 2009 – Accepted on: Oct 13, 2009
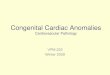
Figure 1. Right kidney – longitudinal ultrasound. A heterogeneous renal mass on the right, poorly outlined, occupying the middle and lower thirds, measuring about 3.8 x 3.4 cm, with thick perirenal fluid collection compatible with subcapsular hematoma
Figure 2. Right kidney Doppler image – slight increase in vascular formation inside the renal mass
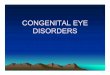
Figure 3. A-D: Abdominal CT Scan (corticomedullary and excretory phases) – enlarged right kidney due to a solid mass involving the kidney middle and lower thirds, with no signs of capsular rupture and causing compression and partial obliteration of the inferior calyx in this kidney, determining extrinsic impression with anterior shifting of the pelvis and proximal ureter
a B C D

einstein. 2009; 7(4 Pt 1):529-31
530 Diniz FV, Baroni RH, Sameshina YT, Garcia RG, Chacon DA, Giron AM, Funari MBG
A preterm male newborn (gestational age 34 weeks and 6 days), whose mother had gestational diabetes and used insulin during pregnancy, showed polyhydramnios in the obstetric (fetal) ultrasound study and a renal mass on the right side. His birth weight was 2,980 g – adequate for gestational age, Apgar score of 6 in the first minute and 8 in the fifth minute. He suffered acute distress respiratory syndrome, initially handled with nasal CPAP and later on submitted to orotracheal
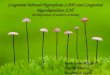
Figure 4. Macroscopy – specimen of right-side kidney in formalin, weighing 30 g and measuring 5.0 x 3.0 x 2.8 cm, comprising kidney and perirenal fat tissue, previously sectioned.
intubation treated with one dose of surfactant. He was extubated in his second day of life and was kept in supplemental oxygen until the third day. He also had neonatal jaundice and was treated with phototherapy for five days. The physical examination revealed a palpable abdominal mass in his right flank, systemic arterial hypertension associated with microscopic hematuria and proteinuria, without renal function impairment. Assessment by abdominal ultrasound showed a poorly outlined heterogeneous right kidney mass, occupying the middle and inferior thirds, measuring 3.8 x 3.4 cm in its largest axes, associated with thick perirenal fluid collection compatible with subcapsular hematoma (Figure 1). The study with colored Doppler showed a mild vascularization inside the mass (Figure 2).
A multislice CT scan of the entire abdomen with endovenous administration of non-ionic iodine contrast and multiplanar reconstruction complemented the study and showed a solid mass involving the inferior pole and the middle third of the right kidney, with no signs of capsular rupture. It caused compression with partial obliteration of the inferior calyx of the kidney and also an intrinsic impression with anterior shifting of the pelvis and proximal ureter (Figure 3 A-D).
After right side radical nephrectomy, the anatomopathological study confirmed the diagnosis of congenital mesoblastic nephroma (Figures 4, 5A and B). The patient developed no complications after the procedure and was discharged from hospital after five days.
A renal mass in children may result from numerous causes, including infection, infarction, lymphatic malformation, trauma and benign and malignant neoplasms, such as Wilms’ tumor and renal teratoma. It is important to stress the predominance of mesoblastic nephroma at this age group and the importance of understanding its characteristics in imaging exams to make a differential diagnosis. Thus, it is possible to make a correct early diagnosis, decide about management and avoid complications.
Congenital mesoblastic nephroma, also known as fetal renal hamartoma or mesenchymal hamartoma, is the most common solid tumor in neonates, corresponding to approximately 3% of all renal neoplasias in children, and is generally benign. It is usually diagnosed in the first three months of life (90% in the first year), and there is a greater incidence among males(1). Although most of the time patients have a palpable abdominal mass, 14% of the cases present polyhydramnios, gastrointestinal malformations, neuroblastoma and genitourinary anomalies, and such alterations can be identified by a prior fetal ultrasound examination. Other less common symptoms include hypercalcemia associated with arterial hypertension, congestive heart failure, and hematuria.
Figure 5. A and B: A. Microscopy – classic pattern mesoblastic nephroma, with spindle-cell intersection (arrow), mild atypia (arrowhead) and rare mitotic cells. (Hematoxylin-eosin, 200X). B. Light microscopy – on the periphery, tumor extensively infiltrating the renal parenchyma, permeating tubules and glomeruli (arrows). (Hematoxylin-eosin, 40X).
a
B

einstein. 2009; 7(4 Pt 1):529-31
Congenital mesoblastic nephroma 531
Polyuria and anemia may also be present(2-3). Although rarely necessary, urography reveals a large, non-functional intrarenal mass which shifts and distorts the adjacent parenchyma and the collecting system. Usually, there is no hydronephrosis associated. The ultrasound often shows a well outlined unilateral, homogeneous and hypoechogenic mass. The presence of hyperechogenic and hypoechogenic concentric rings helps in the diagnosis. A more complex pattern caused by hemorrhage or necrosis can be observed. Color Doppler usually shows hypervascularization and shifting of adjacent vessels. The CT scan demonstrates an intrarenal mass with unspecific attenuation pattern, which can be homogeneous or heterogeneous(4). The characteristics of the lesions on magnetic resonance imaging are not well established yet.
From the pathology standpoint, we know the classic, cellular and mixed subtypes. The classic variant is seen in the macroscopic exam as a large and firm mass, with infiltrating borders and appearance similar to that of uterine leiomyoma. The cellular variant is softer, with cystic areas and irregular contours.
In the classic variant microscopy, enlarged cells (myofibroblasts) are seen infiltrating the surrounding renal parenchyma, impairing the growth of tubules and glomeruli. It is characterized by low cellularity, predominance of matrix and no atypia. Conversely, the cellular variant has a high cellularity, high nucleus/cytoplasm ratio, with mitoses, nuclear atypia and areas of necrosis, thus having a more aggressive behavior(4).
Complete tumor excision spares patients from subsequent complementary treatment. Nonetheless, an insufficient surgical margin requires a new intervention in order to remove the residual disease. Chemotherapy is occasionally used in cases of residual microscopic disease or in cases of tumor rupture, as well as in rare recurrences or metastases.
The treatment advocated is immediate tumor resection by radical nephrectomy(5-7). Most cases have favorable outcomes.
reFerenCes 1. Stiller CA, Parkin DM. International variations in the incidence of childhood
renal tumours. Br J Cancer. 1990;62(6):1026-30.
2. Lustemberg A, Gutirrez C, Caggiani M, Scivoli F. Nefroma mesoblástico congénito: variante multiquística. Arch Pediatr Urug. 2005;76(2): 140-4.
3. Gormley TS, Skoog S, Jones R, Maybee D. Cellular congenital mesoblastic nephroma: what are the options. J Urol. 1989;142(2 Pt 2):479-83.
4. Wootton SL, Rowen SJ, Griscom NT. Pediatric case of the day. Congenital mesoblastic nephroma. Radiographics.1991;11(4):719-21.
5. Varsa EW, McConnell TS, Dressler LG, Duncam M. Atypical congenital mesoblastic nephroma. Report of a case with karyotypic and flow cytometric analysis. Arch Pathol Lab Med. 1989;113(9):1078-80.
6. Howell CG, Othersen HB, Kiviat NE, Norkool P, Beckwith JB, DAngio GJ. Therapy and outcome in 51 children with mesoblastic nephroma: a report of the National Wilms’ Tumor Study. J Ped Surg. 1982;17(6):826-31.
7. Truong LD, Williams R, Ngo T, Cawood C, Chevez-Barrios P, Awalt HL, et al. Adult mesoblastic nephroma: expansion of the morphologic spectrum and review of literature. Am J Surg Pathol. 1998;22(7):827-39.