Embed Size (px)
Citation preview

Consensus-Derived Practice Standards Plan for ComplicatedKaposiform Hemangioendothelioma
Beth A. Drolet, MD1, Cameron C. Trenor, III, MD2, Leonardo R. Brand~ao, MD3, Yvonne E. Chiu, MD1,
Robert H. Chun, MD4, Roshni Dasgupta, MD5, Maria C. Garzon, MD6, Adrienne M. Hammill, MD, PhD7,
Craig M. Johnson, DO8, Brook Tlougan, MD6, Francine Blei, MD9, Mich�ele David, MD10, Ravindhra Elluru, MD, PhD11,
Ilona J. Frieden, MD12, Sheila F. Friedlander, MD13, Ionela Iacobas, MD14, John N. Jensen, MD15, David M. King, MD16,
Margaret T. Lee, MD17, Stephen Nelson, MD18, Manish Patel, DO19, Elena Pope, MD20, Julie Powell, MD21,
Marcia Seefeldt, RN22, Dawn H. Siegel, MD1, Michael Kelly, MD, PhD23, and Denise M. Adams, MD7
From the 1Departments of Pediatrics and Dermatology, Medical College ofWisconsin, Milwaukee, WI; 2Division of Hematology/Oncology, Boston Children’sHospital, Harvard Medical School, Boston, MA; 3Departments ofHematology/Oncology, The Hospital for Sick Children, University of Toronto,Toronto, Canada; 4Departments of Otolaryngology, Medical College of Wisconsin,Milwaukee, WI; 5Department of Surgery, Cincinnati Children’s Hospital MedicalCenter, Cincinnati, OH; 6Department of Dermatology and Pediatrics, ColumbiaUniversity, New York, NY; 7Department of Hematology-Oncology, CincinnatiChildren’s Hospital Medical Center, Cincinnati, OH; 8Department of Radiology,University of Central Florida, Orlando, FL; 9Department of Pediatrics, VascularBirthmark Institute of St. Luke’s Roosevelt Hospital, New York, NY; 10Department ofHematology-Oncology, CHU Sainte-Justine Research Center, Universite deMontreal, Montreal, Canada; 11Department of Otolaryngology, Cincinnati Children’sHospital Medical Center, Cincinnati, OH; 12Departments of Dermatology andPediatrics, University of California San Francisco, San Francisco, CA; 13Departmentof Dermatology, University of California San Diego, San Diego, CA; 14Department ofHematology-Oncology, St. Peter’s University Hospital, New Brunswick, NJ;15Departments of Plastic Surgery, and 16Orthopedic Surgery, Medical College ofWisconsin, Milwaukee, WI; 17Division of Pediatric Hematology/Oncology/Stem CellTransplantation, Columbia University, New York, NY; 18Departments of Pediatricsand Hematology, Children’s Hospital and Clinics of Minnesota, Minneapolis, MN;19Department of Radiology, Cincinnati Children’s Hospital Medical Center,
20
Kaposiform hemangioendothelioma (KHE) is a rare,potentially life-threatening vascular tumor often as-sociated with a coagulopathy known as Kasabach–
Merritt phenomenon (KMP).1 Optimal therapy for KHE isnot known, and despite well-published classification systems,physicians still confuse this entity with other vascular anom-alies. In the interest of standardizing clinical practice acrossspecialties and institutions and to establish a basis for the de-sign of comparative effectiveness studies in vascular tumors,we have developed a consensus-derived standard of practicefor the treatment of KHE with and without associated KMP.
Vascular anomalies encompass a heterogeneous groupof tu-mors and malformations characterized by the presence of ab-normal vascular structures. Vascular anomalies most oftenoccur in the skin and soft tissue; however, they canoccurwithinany organ and present with a wide range of symptoms andcomplications, depending on the type and location of thelesion(s). As a result of the heterogeneity of clinical presenta-tions, patients have traditionally been referred to both adultand pediatric specialists in dermatology, hematology/oncol-ogy, interventional radiology, surgery, plastic surgery, ophthal-mology, and/or otolaryngology to address a particular clinicalproblem. This type of “problem-driven” care has resulted inpatients being seen by multiple specialists without a cohesiveunderstanding of the natural history or mechanism of disease.
The formation of interdisciplinary vascular anomaliescenters has advanced our ability to diagnose and classify theseconditions; however, standardized treatment protocols andassessment of response criteria do not currently exist. Clini-cians rely on case reports, limited retrospective series, and ex-pert opinion when selecting therapeutic interventions forcomplicated patients. This knowledge gap underscores theimportance of gaining consensus in the treatment of theserare, often life-threatening anomalies. Consensus will limitpractice variability and will allow comparison of data acrossinstitutions and subspecialties and facilitate the developmentof evidence-based practice standards.
KHE Kaposiform hemangioendothelioma
KMP Kasabach–Merritt phenomenon
MRI Magnetic resonance imaging
TA Tufted angioma
In October 2011, the National Institute of Arthritis andMusculoskeletal and Skin and Diseases and the Office RareDisease Research supported a meeting of expert cliniciansand scientists to focus on 2 vascular anomalies associatedwith high morbidity and mortality, KHE and multifocal lym-phangioendotheliomatosis with thrombocytopenia. Thispaper will focus on KHE and summarize the clinical, epide-miologic, and radiological features of KHE. An in-depth lit-erature review and national survey of the therapeuticinterventions for KHE was also completed. With this reviewas the evidence base, a multidisciplinary, multi-institutionalexpert panel developed a standardized, consensus-derivedstandard of practice for the treatment of KHE. As moreinformation is available, it is expected that this standard ofpractice will be updated.
Clinical Features
In 1940, Kasabach and Merritt described an infant witha “capillary hemangioma” with extensive purpura and pro-found thrombocytopenia.1 Following this original report, it
Cincinnati, OH; Department of Dermatology, University of Toronto, Toronto,Canada; 21Department of Dermatology (Pediatrics), CHU Sainte-Justine, UniversitedeMontreal,Montreal, Canada; 22Department of Dermatology, Children’s Hospital ofWisconsin; and 23Department of Hematology-Oncology, Medical College ofWisconsin, Milwaukee, WI
Funded by the National Institutes of Health (1R13AR061943-01). I.F. is a consultantfor Pierre Fabre Dermatology. The other authors declare no conflicts of interest.
0022-3476/$ - see front matter. Copyright ª 2013 Mosby Inc.
All rights reserved. http://dx.doi.org/10.1016/j.jpeds.2013.03.080
285

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 163, No. 1
was erroneously assumed that this type of coagulopathycould complicate common infantile hemangiomas. It wasnot until 1993 that KHE was first distinguished from true in-fantile hemangioma, and retrospective review of the originalreport by Kasabach revealed that the infant originally de-scribed did not have a hemangioma but rather had KHE.2-4
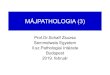
Classically, KHE most often presents as a solitary, firm tu-mor located in the skin or soft tissue. They are large (>5 cm),red-purple tumors or plaques (Figure). They are indurated,often with an inconsistent, pebbly texture and ill-definedmargins. Ecchymosis can be seen with or withouttelangiectasia. The lesions can have hypertrichosis and,rarely, excessive sweating can occur over the lesion. KHElesions may have episodic engorgement, purpura, and pain,often triggered by local trauma, infection, or replacementof blood products. The tumors may spontaneously decreasein size with time; however, complete regression isuncommon. Residual cutaneous lesions are variable andmay resemble port-wine stains with dermal papules, havetelangiectasias with swelling (lymphedema), or have a firmfibrotic texture.5
KHEtypicallyoccurson the lateral neck (Figure), axilla, groin,extremities, and trunk (Table I, case 2). Numerous case reportshave identified KHE in non-cutaneous locations, includingbone, mediastinum, and retroperitoneum. Furthermore, directextension from retroperitoneal and mediastinal lesions havebeen reported in the pancreas, mesentery, pericardium,thymus, and lymph nodes. The tumors are usually solitary;however, multifocal disease, particularly within bone, has beenreported.6-10 Metastatic disease has not been reported. There isno significant sex or ethnicity bias, and there are no reports offamilial cases, underlying genetic mutations, or clonality.9
Tufted angioma (TA) was first described in the late 1980sin the dermatopathology literature.11,12 It is now generallyaccepted that TA and KHE are synonymous vascular tumorswith similar presenting symptoms and potential for KMP.
Figure. Newbornwith large firm, infiltrative tumor, and severethrombocytopenia/KMP
286
Transformation from TA to KHE has been reported13
and histologic features of KHE are more common in “active”lesions with KMP compared with features of TA in residuallesions.5,14 In this paper, we will use “KHE” as an all-encompassing term.The age of presentation with KHE varies, with some cases
diagnosed in utero. Patients diagnosed prenatally or in theneonatal period appear to have increased disease severity.Complications include fetal hydrops, pleural and pericardialeffusion, and multiorgan failure. Adult-onset KHE has alsobeen reported. Lesions are usually focal without KMP.Adult-onset KHE has also been reported with variable clinicalpresentations, though lesions are usually focal withoutKMP.15-25 Although the diagnosis of KHE may be suspectedclinically, it must be confirmed by characteristic imagingand/or histopathologic diagnosis.KMP is a rare clinical-laboratory entity associated exclu-
sively with KHE. Its laboratory hallmark consists of pro-found thrombocytopenia and hypofibrinogenemia withelevated markers of coagulation activation such as D-dimersor fibrin degradation products. The thrombocytopenia isusually severe, with platelet counts <50 � 109/mL. Studiesof the pathophysiology of KMP revealed intralesional plate-let trapping within vascular channels with approximately50% fewer platelets from intralesional blood samples whencompared with systemic samples.26 Platelet trapping wasalso demonstrated by tracing transfused radiolabeled plate-lets trapped within the vascular tumors,27 and by immuno-histochemistry (positive CD-61 marker within tumor).28
Moreover, trapping of radiolabeled fibrinogen infused intopatients with KMP also suggests additional local fibrinogenconsumption secondary to a similar mechanism.29 KMP as-sociated with KHE should be distinguished from the throm-bocytopenia or coagulopathy observed within large, complexvascular malformations (blue rubber bleb syndrome, venousmalformations, and congenital non-progressive hemangi-omas).30 There may be overlap in the laboratory abnormal-ities seen in these two clinical scenarios; however, asa general rule, the thrombocytopenia is more severe inKMP, and coagulopathy (prothrombin time/activated par-tial prothrombin time, low fibrinogen, high D-dimer) ismore prominent in venous malformations. In massive or in-fected lesions, the severity of hematologic perturbation blursthese distinctions.A major referral center recently reported the largest cohort
of KHE patients to date,9 describing 107 cases from 30 statesand 15 countries. In this cohort, 93% presented in infancyand 60% as neonates. Males were slightly more commonthan females (1.3:1). Common presenting symptoms in-cluded an expanding cutaneous lesion, musculoskeletalpain, and/or thrombocytopenia. In this cohort, 11% of pa-tients lacked cutaneous features, and these patients presentedwith respiratory distress, abdominal distension, hypotonia,heart failure, or hematochezia. KMP developed in 71%,and the greatest risk factors for KMP in this cohort weredepth of infiltration into muscle or fascia and mediastinalor retroperitoneal involvement. Cutaneous lesions with
Drolet et al

Table I. Summary of cases for consensus voting
Case 1 Infant with an enlarging, unresectable KHE affecting thelower extremity with severe thrombocytopenia exhibitingKMP (KHE+KMP).
Consensus Recommendation: For cases of KHEassociated with KMP, first-line therapy with intravenousvincristine 0.05 mg/kg once weekly AND oralprednisolone 2 mg/kg/d OR intravenousmethylprednisolone 1.6 mg/kg/d is recommended.
Case 2 Infant with an enlarging, unresectable TA located on thetrunk without KMP (KHE/TA, no KMP)
Consensus Recommendation: For cases of KHE thatrequire intervention because of growth or symptoms butdo not have KMP, oral prednisolone 2 mg/kg/d is therecommended first-line therapy.
July 2013 WORKSHOP/SYMPOSIUM SUMMARY
maximal dimension >5-8 cm are also correlated withKMP risk.31 This cohort may over-represent severe cases ofKHE and associated KMP because of tertiary referral bias.
Diagnostic Imaging
Characteristic imaging features may aid in the diagnosis ofKHE, as well as determining extent of involvement and re-sponse to treatment. Magnetic resonance imaging (MRI)with and without gadolinium is the imaging modality ofchoice. A fairly homogeneous increased T2 signal as well asdecreased T1 signal are seen.31 Additional characteristicMRI findings include varying degrees of dermal and subcuta-neous thickening, infiltrative and ill-defined margins oftenextending into adjacent muscles, surrounding edema-likepattern, and ectatic high-flow vessels. The skin thickeningand edema-like pattern, often described as “stranding,” arebest seen on T2 fat-saturated sequences and most likely rep-resent a combination of ectatic adjacent lymphatic channelsand tumor.4
Gadolinium-enhanced images typically demonstratesubstantial enhancement.32 One of the findings in treatmentresponse is both decreased size and involution of the tumoras well as decreased enhancement. Conventional MRIsequences occasionally demonstrate variably sized flow voidssurrounding the tumor depending on size. MagneticResonance angiography may better define arterial supplyand venous drainage of the tumor.
Computed tomography, ultrasound, and radiographs areof limited usefulness in the evaluation of KHE. Computedtomography findings are nonspecific and include soft tissueattenuation, irregular and infiltrative margins, homogenousenhancement, and skin thickening when the lesion issubcutaneous. Bone involvement and intralesional calcifica-tions are rare.31 Ultrasound is limited in determining thefull extent of involvement (except in superficial lesions) aswell as determining the presence of multifocal disease. Ultra-sound characteristically demonstrates a solid tumor with het-erogeneous hyperechoic echotexture and irregular margins.Color Doppler imaging may demonstrate intralesional
Consensus-Derived Practice Standards Plan for Complicated Ka
vessels with high resistance arterial Doppler waveforms andhypervascularity of the tumor; however, flow is variableand may be dependent on tumor size, location, and degreeof platelet trapping.
Surgical Treatment of KHE
Although complete surgical resection has been touted as thegold standard for cure of KHE, total resection is often nota viable option given the high risk of morbidity and mortal-ity.33,34 Most KHE are infiltrative in nature and often in-vade large neurovascular structures, muscle, and fascia.Moreover, as tumors may occur in a discontinuous fashion,clear surgical margins are nearly impossible to achieve.Partial resections have been reported to improve symptoms,but residual lesions often recur locally.16 Severe coagulop-athy may preclude surgery, and manipulation of the tumormay further complicate KMP with worsening of coagulop-athy increasing the risk of hemorrhage, both locally andsystemically.Although surgical excision is often not a primary treat-
ment option, it may be a secondary consideration for tumorsthat have failed medical management or for imminently life-threatening tumors when the time to response to medicaltherapy is considered too long.35 In any case, careful perio-perative planning is essential to reduce the morbidity of sur-gical excision, especially when the lesion is associated withKMP. Compression of KHE lesions that are located on theextremities can decrease flow, and can be a useful tempo-rizing method while other inventions are initiated.
Imaging-Guided Therapy for KHE
Angiography and embolization have historically been usedin the diagnosis and treatment of KHE.36 The effects ofthese procedures have proven to be temporary and are cur-rently used primarily as an adjunct to surgery to minimizebleeding during a planned resection. Angiography demon-strates hypertrophied and tortuous feeding arteries with sig-nificant and diffuse vascular blush. KHE does not typicallydemonstrate intralesional aneurysm formation or arteriove-nous shunting.37,38 The success of embolization has beendifficult to determine, given the relatively few cases in theliterature. In this expert group’s experience, arterial emboli-zation will often produce initial rises in platelet levels anda decrease in the size and redness of the mass; however,the results tend to be temporary. In severe or life-threatening situations, arterial embolization may servea temporizing role, providing additional time for medicaltherapy to be effective.
Radiation Therapy
In the past, radiation therapy was widely used for the treat-ment of proliferative benign lesions, including infantile hem-angiomas and KHEs.39,40 In the face of current treatmentoptions, the long-term risk-benefit ratio of this therapeutic
posiform Hemangioendothelioma 287

Table II. Initial diagnostic work-up
Laboratory studiesCBC w/platelet countCoagulation studies (PT, PTT, fibrinogen, d-Dimer levels)
Imaging studiesMRI with and without contrast
Tissue biopsy
CBC, complete blood count; PT, prothrombin time; PTT, partial prothrombin time.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 163, No. 1
option is not acceptable, especially because pharmacologicinterventions have been successful.
Review of Pharmacologic Treatment of KHE
There have been no prospective studies regarding the treat-ment of KHE or standardized outcome measures to docu-ment responses, or systematically obtained long-termfollow-up data. The medical literature regarding pharmaco-logic treatment consists primarily of small case series and sin-gle case reports. Furthermore, some of these may not becompletely reliable, as many did not perform or fully reportpathologic findings, and most predate the report of KHE asa distinct clinical entity established in 1993.2
The pharmacologic treatment of KHE, although not alwayscurative, aims to decrease tumor size and correct coagulop-athy. Corticosteroids, although widely considered first-linetherapy, have never been investigated in a prospective man-ner. Most published cases report partial response, and corti-costeroids are infrequently effective as a solitary agent.Vincristine has also been widely used, mostly in combinationwith corticosteroids. In one retrospective case series, vincris-tine was effective in the majority of patients.41 First-linetherapy with vincristine is often delayed secondary to theneed for central access necessitating the initiation of cortico-steroids first. Interferon-a has been used with some reportedsuccess, but has been associated with a risk of spastic diplegiain infants less than 8months of age.42 Antiplatelet agents suchas ticlopidine and clopidogrel have been used in combinationwith other therapies, with mixed results.43 Aspirin has alsobeen used as an antiplatelet agent, with some success in con-trolling pain related to the coagulopathy, but not necessarilyeffectively preventing platelet consumption.44
Antifibrinolytic agents such as aminocaproic acid and tra-nexamic acid are frequently used as adjunctive therapies in aneffort to decrease transfusion requirements, with mixed re-sults.45 In particular refractory cases, in which patients donot respond or cannot be tapered off of corticosteroids, otherchemotherapies have historically been added. These are mostcommonly cyclophosphamide alone or with agents such asvincristine and actinomycin-D.46,47
Recently, there have been reports of additional agents be-ing used in the treatment of KHE. Propranolol, which is nowbeing widely used in the treatment of infantile hemangioma,was reported as being used successfully in one case of KHE48;however, a recent case series found little to no benefit.49 Useof sirolimus was recently described in 2 case reports of refrac-tory KHE, with excellent results.50,51 These patients both hadrapid improvement in hematopoietic parameters. One ofthese patients, who is now several years post-treatmentwith no recurrence of coagulopathy, has full function ofher affected limb and an excellent cosmetic result (per per-sonal communication). Sirolimus, a mammalian target of ra-pamycin inhibitor, is currently being tested in a prospectiveclinical trial for diagnoses that include, but are notlimited to, complicated KHE tumors (ClinicalTrials.gov;NCT00975819).
288
Methods
Prior to the consensus meeting, a survey was conducted to as-sess the initial management of KHE. It was developed by aninterdisciplinary team of with the goal of collecting datafrom 27 vascular anomalies centers in the US and Canada.Two representative cases (Table I) were presented: first, aninfant with an unresectable KHE exhibiting KMP, andsecond, an infant with an unresectable KHE without KMP.The response rate for the survey was 88%, and 80% of the
vascular anomalies groups indicated that they had cared for 5or more patients with these tumors at their institutionswithin the last ten years, totaling over 150 patients. The ma-jority of sites (92%) reported that they do not have a writtenstandard of practice for the management of tumors associ-ated with KMP.Experts were polled about the indications for the use of
platelet transfusions for the management of children withthrombocytopenia associated with KMP. Eighty percent re-ported that they transfuse if the patient is actively bleeding,whereas 60% reported that they would do so if surgical inter-vention is planned. A smaller group (24%) noted that plateletcounts <10 � 109/L would be an additional indication forplatelet transfusion, and 8% indicated that they would usethe fibrinogen level (<100 mg/dL) as a determinant. Addi-tional information was obtained about the use of other bloodproducts, which can be found in our complete article.52
Case 1 (KHE+KMP)There was excellent (80%) agreement among centers on ini-tial work-up (Table II). Sixty-four percent of centers did notthink that a tissue biopsy was necessary to confirm diagnosis.The most common initial therapy for KHE with KMPreported by respondents was a combination of systemiccorticosteroids and vincristine (12/24 centers; 50%),followed by systemic steroids alone (7/24 centers; 29%),and vincristine alone (2/24; 8%); cyclophosphamide,sirolimus, and steroids plus propranolol were the initialtreatments of choice for 1 center each. Vincristine andsirolimus were the most common second-line treatments.The most common corticosteroid dose was the equivalentof 2 to 3 mg/kg/d of oral prednisone, and the majority ofsites stated that the decision to proceed with oral vsintravenous corticosteroids would depend upon the patientand clinical situation, such as intravenous line access andseverity of the illness. Parameters for tapering therapyincluded improvement or normalization of platelet count
Drolet et al

July 2013 WORKSHOP/SYMPOSIUM SUMMARY
(22/24; 92%), reduction in the size of the mass (19/24; 79%),resolution of functional impairment (15/24; 63%), andnormalization of D-dimer (14/24; 58%).
Case 2 (KHE/TA, no KMP)The most common initial treatment for the patient in thisclinical scenario was systemic corticosteroids (8/24; 33%)and steroids plus vincristine (1/24; 4%) (total of 9/24;38%). This was followed by clinical monitoring with periodicreassessment (8/24; 33%), vincristine (2/24; 8%), proprano-lol (2/24; 8%), aspirin (1/24; 4%), and sirolimus (1/24; 4%).The most common second-line therapy was vincristine.
Consensus Methodology
A meeting was held at the Medical College of Wisconsin inMilwaukee, Wisconsin on October 6, 2011. The goal of thismeeting was to gather a multidisciplinary team of expertsto share existing knowledge about KHE and developconsensus-derived treatment protocols for first-line treat-ment of KHE. Forty-three participants representing 9 pediat-ric subspecialties attended, of whom 16 had sufficientexperience in the treatment of these rare tumors to partici-pate in the voting process. The survey described above wasdistributed to a broader group of experts from 24 institutionsprior to the meeting, and the same 2 case scenarios were usedas the basis for the consensus protocol.
Given the efficacy of medical therapy and challenges of re-section due to infiltrative disease or hematologic instability,most patients are initially treated with pharmacologic thera-pies. The group agreed that surgical resection should be con-sidered for patients with KHE that can be safely andcompletely excised. Nominal group technique was used to de-vise treatment protocols recommended as first-line pharma-cologic treatment for unresectable KHE with and withoutKMP (Table I). Treatment approaches from the surveyresults were each written on large sheets of flip-chart paper.Time was provided for individuals to list additionaltreatment protocols, and these were solicited from theaudience without discussion. Combination therapy anddosage variations were considered distinct treatmentapproaches and written individually on the sheets. Eachvoting participant received 5 colored stickers, which he/shewas allowed to distribute in any fashion, including multiplestickers for 1 treatment option. General discussion of theresults followed, and those treatment protocols that receivedfewer than 20 votes (<75% of the 80 total) were eliminated.Steps 4 and 5 were repeated until consensus was obtained.
Results
Case 1 (KHE+KMP)After 1 round of voting, 1 treatment protocol was clearly themajority preference, as it was the only one to receive 20 ormore votes. After eliminating the other treatment approachesthat received fewer than 20 votes, this consensus treatmentprotocol was selected as the unanimous decision of the ex-
Consensus-Derived Practice Standards Plan for Complicated Ka
perts. For cases of KHE associated with KMP, first-line ther-apy with intravenous vincristine 0.05 mg/kg once weeklyAND oral prednisolone 2 mg/kg/d OR intravenous methyl-prednisolone 1.6 mg/kg/d is recommended. Patients with se-vere KMP should be treated aggressively with a combinationregimen; monotherapy is not recommended; however, theauthors recognize that vincristine may not be immediatelyavailable because of lack of central venous access or otherfactors. In those situations, corticosteroid therapy shouldbe started immediately so that therapy is not delayed by anunavailability of vincristine.The authors consider oral prednisolone and intravenous
methylprednisolone to be equivalent in the treatment of thesepatients, and choice of the agent would be based on individ-ual factors such as intravenous access and ability to adminis-ter oral medications. The duration of therapy should be basedon each individual patient and his or her treatment response.The goal is to wean the corticosteroid after 3 to 4 weeks ifthere has been good clinical response and stabilization ofthe patient’s hematologic status. As mentioned earlier, it israre to see complete clearance of this tumor, even with pro-longed pharmacologic therapy. Residual tumor or fibrosis iscommon, especially in more aggressive lesions, and is nota reason to continue therapy if high risk symptoms have re-solved and the tumor is stable on serial imaging. The in-tended length of vincristine therapy is typically 20-24 weeksin duration, but should be patient-specific and driven by res-olution of high risk symptoms, tumor response, and accept-able therapy related toxicity. Currently, data regardingtreatment and outcomes are not evidence-based but repre-sent consensus-based recommendations. Sirolimus is a prom-ising agent for KHE, with prospective studies underway toevaluate safety and efficacy in patients with KHE.The expert group also agreed upon a number of recom-
mendations regarding the management of KMP. Althoughprophylactic platelet transfusions are often indicated in in-fants and children with thrombocytopenia, this recommen-dation applies to thrombocytopenia as a result of reducedproduction and cannot be extrapolated to patients withKMP.53 Platelet transfusions have been shown to be of min-imal benefit and tend to have a very short half-life in thisclinical scenario.54 Furthermore, platelets are known to beretained within KHE, often resulting in increased pain andenlargement of the tumor.28,54 Local platelet activationmay also lead to the release of proangiogenic factors, possiblypromoting tumor proliferation. Platelet transfusion is onlyindicated for active bleeding and/or immediately prior tosurgery.Heparin is not indicated because of bleeding risk and min-
imal effect on platelets. There are inconsistent resultsreported from use of antiplatelet and anti-fibrinolytic ther-apy. Conversely, if there is acquired hypofibrinogenemia(<100 mg/dL), the administration of frozen plasma or cryo-precipitate is recommended, especially in the presence ofbleeding. Cryoprecipitate should be given when the requiredvolume of plasma is relatively contraindicated and targetedfibrinogen replacement in a smaller volume is preferred.
posiform Hemangioendothelioma 289

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 163, No. 1
Case 2 (KHE/TA, no KMP)After 1 round of voting, 1 treatment protocol received themajority votes as it was the only one to receive 20 or morevotes. After eliminating the other treatment approachesthat received fewer than 20 votes, this consensus treatmentprotocol was selected as the unanimous decision of the ex-perts. For cases of KHE that require intervention becauseof growth or symptoms but do not have KMP, oral prednis-olone 2 mg/kg/d is the recommended first-line therapy.Treatment with aspirin at an antiplatelet dose of 2 to 5 mg/kg/d could be considered as adjunctive therapy.
Again, the duration of therapy should be individualized,and the prednisolone should be weaned as soon as medicallyfeasible.
Discussion
The rationale for arriving at a consensus-derived treatmentplan was to provide a uniform approach for the care of thischallenging disorder, utilizing expertise from diverse medicaldisciplines from various vascular anomalies centers. By pool-ing the collective experience of a multispecialty expert panelwe were able to decrease variability among providers and in-stitutions and agree upon a number of recommendations.These recommendations were guided by a survey of 24 vascu-lar anomalies centers, and a review of existing evidence, sup-plemented by expert opinion and clinical experience. Wehave developed a consensus-derived first-line therapy forcomplicated KHE and KHE associated with KMP. We antic-ipate that these practice standards will be modified as moredata are made available. This consensus-derived treatmentplan will serve as a standard for future comparative effective-ness studies and enable prospective data collection at multi-ple institutions, with the ultimate goal of developingevidence-based guidelines of care. We hope that this collab-orative project will serve as a model for other rare vascularanomalies and enable our field to move forward toward theidentification of evidence-based guidelines, therebyminimiz-ing morbidity and mortality and improving the long-termoutcomes of these patients. n
Submitted for publication Nov 9, 2012; last revision received Jan 22, 2013;
accepted Mar 29, 2013.
Reprint requests: Beth A. Drolet, MD, Departments of Pediatrics and
Dermatology, Medical College of Wisconsin, 8701 Watertown Plank Road,
TBRC, 2nd floor, Suite C2010,Milwaukee,WI 53226. E-mail: [email protected]
References
1. Kasabach HH, Merritt KK. Capillary hemangioma with extensive pu-
pura. Am J Dis Child 1940;59:1063-70.
2. Zukerberg LR, Nickoloff BJ, Weiss SW. Kaposiform hemangioendothe-
lioma of infancy and childhood. An aggressive neoplasm associated with
Kasabach–Merritt syndrome and lymphangiomatosis. Am J Surg Pathol
1993;17:321-8.
3. Enjorlas O, Wassef M, Mazoyer E, Frieden IJ, Rieu PN, Drouet L, et al.
Infants with Kasabach–Merritt syndrome do not have “true” hemangi-
omas. J Pediatr 1997;130:631-40.
290
4. Sarkar M, Mulliken JB, Kozakewich HP, Robertson RL, Burrows PE.
Thrombocytopenic coagulopathy (Kasabach–Merritt phenomenon) is
associated with Kaposiform hemangioendothelioma and not with com-
mon infantile hemangioma. Plast Reconstr Surg 1997;100:1377-86.
5. Enjorlas O, Mulliken JB, Wassef M, Frieden IJ, Rieu PN, Burrows PE,
et al. Residual lesions after Kassabach–Merritt phenomenon in 41 pa-
tients. J Am Acad Dermatol 2000;42(2 Pt 1):225-35.
6. Gianotti R, Gelmetti C, Alessi E. Congenital cutaneous multifocal kapo-
siform hemangioendothelioma. Am J Dermatopathol 1999;21:557-61.
7. Chen YJ, Wang CK, Tien YC, Hsieh TJ. MRI of multifocal kaposiform
hemangioendothelioma without Kasabach–Merritt phenomenon. Brit
J Radiol 2009;82:e51-4.
8. Veening MA, Verbeke JI, Witbreuk MM, Kaspers GJ. Kaposiform (spin-
dle cell) hemangioendothelioma in a child with an unusual presentation.
J Pediatr Hematol Oncol 2010;32:240-2.
9. Croteau SE, Liang MG, Kozakewich HP, Alomari AI, Fishman SJ,
Mulliken JB, et al. Kaposiform hemangioendothelioma: atypical features
and risks of Kassabach–Merritt phenomenon in 107 referrals. J Pediatr
2013;162:142-7.
10. Deraedt K, Vander Pooten V, Van Geet C, Renard M, De Wever I,
Sciot R. Multifocal kaposiform hemangioendothelioma. Virchows
Arch 2006;448:843-6.
11. Alessi E, Bertani E, Sala F. Acquired tufted angioma. Am J Dermatopa-
thol 1986;8:426-9.
12. Jones EW, Orkin M. Tufted angioma (angioblastoma). A benign pro-
gressive angioma, not to be confused with Kaposi’s sarcoma or low-
grade angiosarcoma. J Am Acad Dermatol 1989;20(2 Pt 1):214-25.
13. Chu CY, Hsiao CH, Chiu HC. Transformation between Kaposiform he-
mangioendothelioma and tufted angioma. Dermatology 2003;206:
334-7.
14. Lyons LL, North PE,Mac-Moune Lai F, Stoler MH, Folpe AL,Weiss SW.
Kaposiform hemangioendothelioma: a study of 33 cases emphasizing its
pathologic, immunophenotypic, and biologic uniqueness from juvenile
hemangioma. Am J Surg Pathol 2004;28:559-68.
15. Yu L, Yang SJ. Kaposiform hemangioendothelioma of the spleen in an
adult: an initial case report. Pathol Oncol Res 2011;17:69-72.
16. Kim MG, Choi YS, Park SJ, Chong SM. Kaposiform hemangioendo-
thelioma of the breast in an adult female. Clin Breast Cancer 2011;
11:135-7.
17. White JB, Pullman J, Wenig B, Smith RV. Kaposiform hemangioendo-
thelioma of the tongue in an adult. Arch Otolaryngol Head Neck Surg
2009;135:824-6.
18. Karnes JC, Lee BT, Phung T, Alomari AI, Mulliken JB, Greene AK.
Adult-onset kaposiform hemangioendothelioma in a posttraumatic
site. Ann Plast Surg 2009;62:456-8.
19. Zamecnik M, Koys F, Mikleova Z, Michal M. Additional case of kaposi-
form hemangioendothelioma in an adult. Cesk Patol 2001;37:128-9.
20. Hardisson D, Prim MP, DeDiego JI, Patron M, Escribano A, Rabanal I.
Kaposiform hemangioendothelioma of the external auditory canal in an
adult. Head Neck 2002;24:614-7.
21. Mac-Moune Lai F, To KF, Choi PC, Leung PC, Kumta SM, Yuen PP,
et al. Kaposiform hemangioendothelioma: five patients with cutaneous
lesion and long follow-up. Mod Pathol 2001;14:1087-92.
22. Zamencnik M, Mikleova Z, Michal M. Kaposiform hemangioendothe-
lioma in adult. Report of a case with amianthoid-like fibrosis and angiec-
tases. Cesk Patol 2000;36:163-7.
23. Senturk N, Yyldiz L, Aydin F, Eroglu L, Canturk T, Turlani AY. Kaposi-
form hemangioendothelioma in an adult with an unusual presentation. J
Eur Acad Dermatol Venereol 2006;20:630-2.
24. Mentzel T, Mazzoleni G, Dei Tos AP, Fletcher CD. Kaposiform heman-
gioendothelioma in adults. Clinicopathologic and immunohistochemi-
cal analysis of three cases. Am J Clin Pathol 1997;108:450-5.
25. Cho SH, Na KS. Hemangioendothelioma on the conjunctiva of the up-
per eyelid. Clin Experiment Ophthalmol 2006;34:794-6.
26. Gilon E, Ramot B, Sheba C. Multiple hemangiomata associated with
thrombocytopenia: remarks on the pathogenesis of the thrombocytope-
nia in this syndrome. Blood 1959;14:74-9.
Drolet et al

July 2013 WORKSHOP/SYMPOSIUM SUMMARY
27. Shulkin BL, Argenta LC, Cho KJ, Castle VP. Kasabach–Merritt syn-
drome: treatment with ε-amniocaproic acid and assessment by indium
111 platelet scintigraphy. J Pediatr 1990;117:746-9.
28. Seo SK, Suh JC, Na GY, Kim IS, Sohn KR. Kasabach–Merritt syndrome:
identification of platelet trapping in a tufted angioma by immunohisto-
chemistry technique using monoclonal antibody to CD61. Pediatr Der-
matol 1999;16:392-4.
29. Straub PW, Kessler S, Schreiber A, Frick PG. Chronic intravascular co-
agulation in Kasabach–Merritt syndrome. Preferential accumulation of
fibrinogen 131 in a giant hemangioma. Arch InternMed 1972;129:475-8.
30. Dompmartin A, Acher A, Thibon P, Tourbach S, Hermans C, Deneys V,
et al. Association of localized intravascular coagulopathy with venous
malformations. Arch Dermatol 2008;144:873-7.
31. Gruman A, Liang MG, Mulliken JB, Fishman SJ, Burrows PE,
Kozakewich HP, et al. Kaposiform hemangioendothelioma without Ka-
sabach–Merritt phenomenon. J Am Acad Dermatol 2005;52:616-22.
32. Rodriguez V, Lee A, Witman PM, Anderson PA. Kasabach–Merritt phe-
nomenon: case series and retrospective review of the Mayo Clinic expe-
rience. J Pediatr Hematol Oncol 2009;31:522-6.
33. Drolet BA, Scott LA, Esterly NB, Gosain AK. Early surgical intervention
in a patient with Kasabach–Merritt phenomenon. J Pediatr 2001;138:
756-8.
34. George M, Signhal V, Sharma V, Nopper AJ. Successful surgical excision
of a complex vascular lesion in an infant with Kasabach–Merritt syn-
drome. Pediatr Dermatol 2002;19:340-4.
35. Jiang RS, Hu R. Successful treatment of Kasabach–Merritt syndrome
arising from kaposiform hemangioendothelioma by systemic corticoste-
roid therapy and surgery. Int J Clin Oncol 2012;17:512-6.
36. Yesudian PD, Klafkowski J, Parslew R, Gould D, Lloyd D, Pizer B. Tufted
angioma-associated Kasabach–Merritt syndrome treated with emboliza-
tion and vincristine. Plast Reconstr Surg 2007;119:1392-3.
37. Enomoto Y, Yoshimura S, Egashira Y, Iwama T. Transarterial emboliza-
tion for cervical hemangioma associated with Kassabach–Merritt syn-
drome. Neurol Med Chir (Tokyo) 2011;51:375-8.
38. Wolfe SQ, Farhat H, Elhammady MS, Moftakhar R, Aziz-Sultan MA.
Transarterial embolization of scalp hemangioma presenting with Kasa-
bach–Merritt syndrome. J Neurosurg Pediatr 2009;4:453-7.
39. Saito M, Gunji Y, Kashii Y, Odaka J, Yamachui T, Kanai N, et al. Refrac-
tory kaposiform hemangioendothelioma that expressed vascular endo-
thelial growth factor receptor (VEGFR)-2 and VEGFR-3: a case report.
J Pediatr Hematol Oncol 2009;31:194-7.
40. Vin-Christian K, McCalmont TH, Frieden IJ. Kaposiform hemangioen-
dothelioma. An aggressive, locally invasive vascular tumor that can
mimic hemangioma of infancy. Arch Dermatol 1997;133:1573-8.
41. Haisley-Royster C, Enjorlas O, Frieden IJ, Garzon M, Lee M, Oranje A,
et al. Kasabach–Merritt phenomenon: a retrospective study of treatment
with vincristine. J Pediatr Hematol Oncol 2001;24:459-62.
Consensus-Derived Practice Standards Plan for Complicated Ka
42. Barlow CF, Priebe CJ, Mulliken JB, Barnes PD, MacDonald D,
Folkman J, et al. Spastic diplegia as a complication of interferon Alfa-
2a treatment of hemangiomas of infancy. J Pediatr 1998;132(3 Pt 1):
527-30.
43. Fernandez-Pineda I, Lopez-Gutierrez JC, Chocarro G, Bernabeu-
Wittel J, Ramirez-Villar GL. Long-term outcome of vincristine-aspi-
rin-ticlopidine (VAT) therapy for vascular tumors associated with
kasabach-merritt phenomenon. Pediatr Blood Cancer 2013 [Epub
ahead of print].
44. Fernandez-Pineda I, Lopez-Gutierrez JC, Ramirez G, Marquez C. Vin-
cristine-ticlopidine-aspirin: an effective therapy in children with Kasa-
bach–Merritt phenomenon associated with vascular tumors. Pediatr
Hematol Oncol 2010;27:641-5.
45. Hanna BD, Berenstein M. Tranexamic acid in the treatment of Kasa-
bach–Merritt syndrome in infants. Am J Pediatr Hematol Oncol 1989;
11:191-5.
46. Blei F, Karp N, Rofsky N, Rosen R, Greco MA. Successful multimodal
therapy for kaposiform hemangioendothelioma complicated by Kasa-
bach–Merritt phenomenon: case report and review of the literature. Pe-
diatr Hematol Oncol 1998;15:295-305.
47. Hauer J, Graubner U, Konstantopoulous N, Schmidt S, Pfluger T,
Schmid I. Effective treatment of kaposiform hemangioendotheliomas as-
sociated with Kasabach–Merritt phenomenon using four-drug regimen.
Pediatr Blood Cancer 2007;49:852-4.
48. Hermans DL, van Beynum IM, van der Vijver RJ, Kool LJ, de Blaauw I,
van der Vleuten CJ. Kaposiform hemangioendothelioma with Kasa-
bach–Merritt syndrome: a new indication for propranolol treatment. J
Pediatr Hematol Oncol 2011;33:e171-3.
49. Chiu YE, Drolet BA, Blei F, CarcaoM, Fangusaro J, Kelly ME, et al. Vari-
able response to propranolol treatment of kaposiform hemangioendo-
thelioma, tufted angioma, and Kasabach–Merritt phenomenon.
Pediatr Blood Cancer 2012;59:934-8.
50. Blatt J, Stavas J, Moats-Staats B, Woosley J, Morrell DS. Treatment of
childhood kaposiform hemangioendothelioma with sirolimus. Pediatr
Blood Cancer 2010;55:1396-8.
51. Hammill AM, Wentzel M, Gupta A, Nelson S, Lucky A, Elluru R, et al.
Sirolimus for the treatment of complicated vascular anomalies in chil-
dren. Pediatr Blood Cancer 2011;57:1018-24.
52. Tlougan BE, Drolet BA, Frieden IJ, Adams DM, Lee MT, Kelly ME, et al.
Medical management of tumors associated with Kasabach–Merritt Phe-
nomenon. Presented at 38th Annual Meeting of the Society of Pediatric
Dermatology; 2012 July 12-14; Monterey, CA.
53. Gibson BE, Todd A, Roberts A, Pamphilon D, Rodeck C, Bolton-
Maggs P, et al. Transfusion guidelines for neonates and older children.
Br J Haematol 2004;124:433-53.
54. Phillips WG, Marsden JR. Kasabach–Merritt syndrome exacerbated by
platelet transfusion. J R Soc Med 1993;86:231-2.
posiform Hemangioendothelioma 291