Embed Size (px)
Citation preview

• Introduction • ACMG-AMP Classification System • Other Classification Systems • Evaluation of inter-laboratory concordance (Amendola et al. 2016)
Please download ACMG Standards and Guidelines (page 8-10)
https://www.acmg.net/docs/Standards_Guidelines_for_the_Interpretation_of_Sequence_Variants.pdf search: “acmg standards and guidelines”
OVERVIEW

Gattaca (1997)
INTRODUCTION

In the not-too-distant future… …we will not perform NIPT anymore …we will do WGS in four seconds
INTRODUCTION

Lessons learned: Why not NIPT ? They do a three seconds WGS
INTRODUCTION

In the not-too-distant distant future… …we will not perform NIPT anymore …we will do WGS in four seconds …INCLUDING interpretation / classification Did you notice the molecularbiologist ?
INTRODUCTION

Starting Point:
Assessing pathogenicity is not an easy task (it never was, but
NGS does not make it better…)
Conflicting systems among labs / reseachers cause confusion
(best case) or wrong clinical recommendations (worst case)
Need to standardize Variant Classification
VARIANT CLASSIFICATION

VARIANT CLASSIFICATION BRCA2 NM_000059.1: c.8488-1G>A

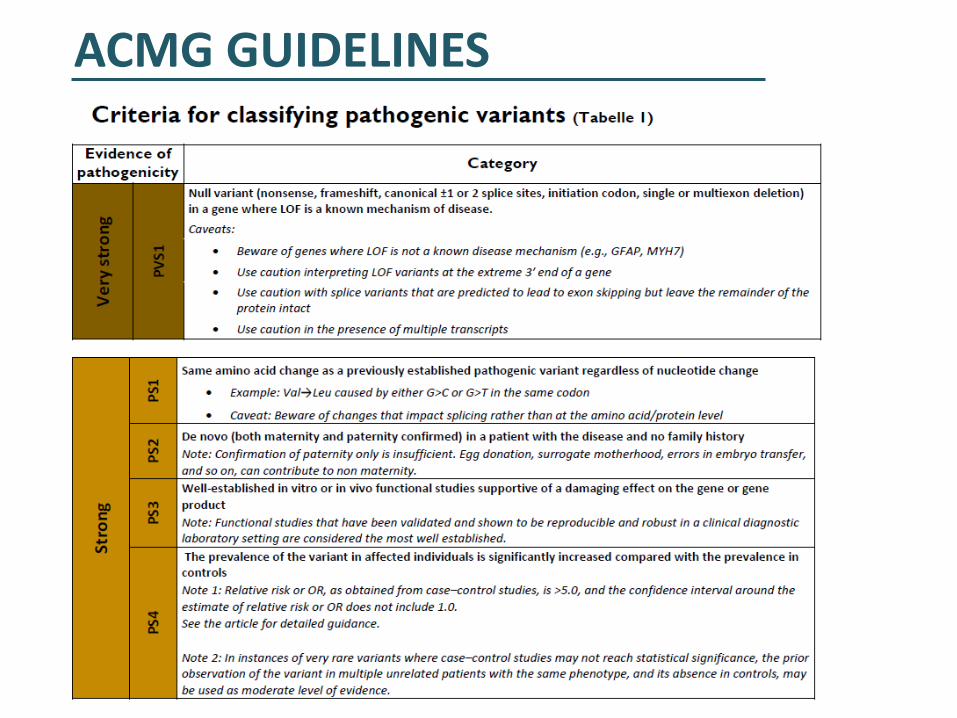
Qualitative evaluation of different data types (28 defined criteria with assigned code)
Each code is assigned a weight (stand-alone, very strong, strong, moderate, or supporting) and direction (benign or pathogenic)
Variants then can be assigned in one of 5 classes (IARC 5-tier system)
If not enough lines of evidence are invoked to classify a variant as P, LP, LB, or B, or there are valid but contradictory lines of evidence, a variant is interpreted as a VUS
ACMG GUIDELINES

ACMG GUIDELINES

ACMG GUIDELINES

General Considerations: • for variants in all Mendelian genes (single gene, gene panel, exome, genome or transcriptome)
• not for somatic, Px, multigenic/complex disorders
• cave: candiate genes („genes of uncertain significance“; „GUS“; Oct.2016: OMIM 3648 genes)
• the terms „mutation“ and „polymorphism“ should not be used
• instead use „variant“ (pathogenic (5); likely pathogenic (4); uncertain significance (3); likely benign (2); benign (1))
• variants should be reported using the HGVS nomenclature (http://www.hgvs.org/mutnomen)
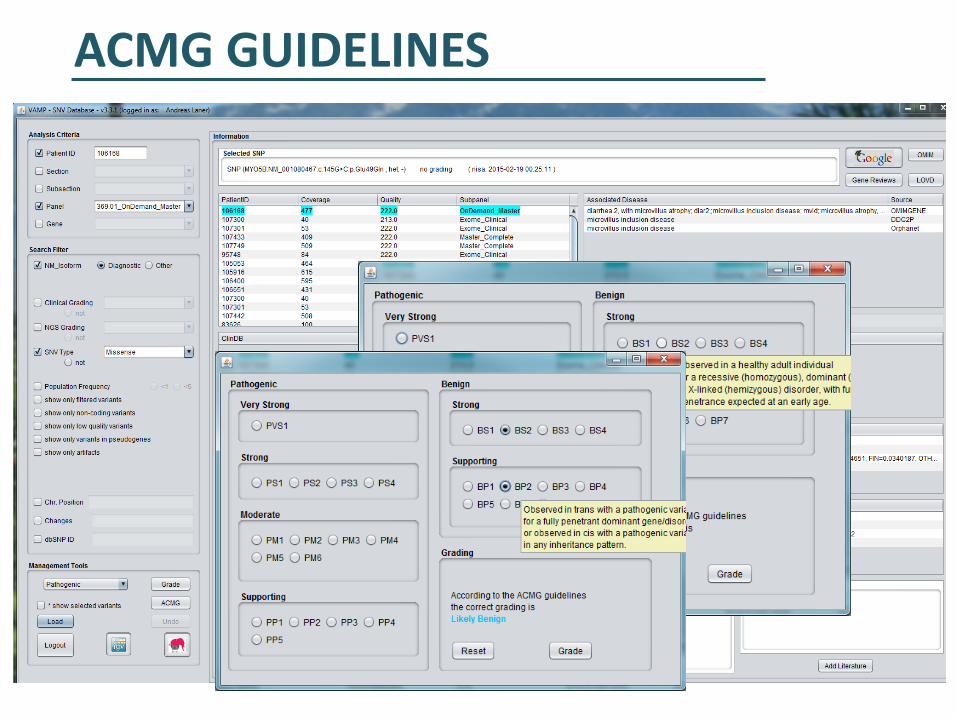
• to provide flexibility: some criteria listed as one weight can be moved to another weight using professional
judgment, depending on the evidence collected (multiple observations of a variant in trans with path. variant – PM3 to PS)
„Pathogencity should be determined by the entire body of evidence in aggregate, including all cases studied, arriving at a single conclusion“
ACMG GUIDELINES

0.90-0.99
0.001-0.10
0.11-0.89
ACMG GUIDELINES
ACMG GUIDELINES

ACMG GUIDELINES

ACMG GUIDELINES

ACMG GUIDELINES

ACMG GUIDELINES

ACMG GUIDELINES

ACMG GUIDELINES
BP2+BS4+BS3
BS1
BP4
BS1+BS3+BS4+BP2+BP4 = class 1

ACMG GUIDELINES
BP2+BS4+BS3
BS1
BP4
PP5??
BS1+BS3+BS4+BP2+BP4 = class 1
ACMG GUIDELINES
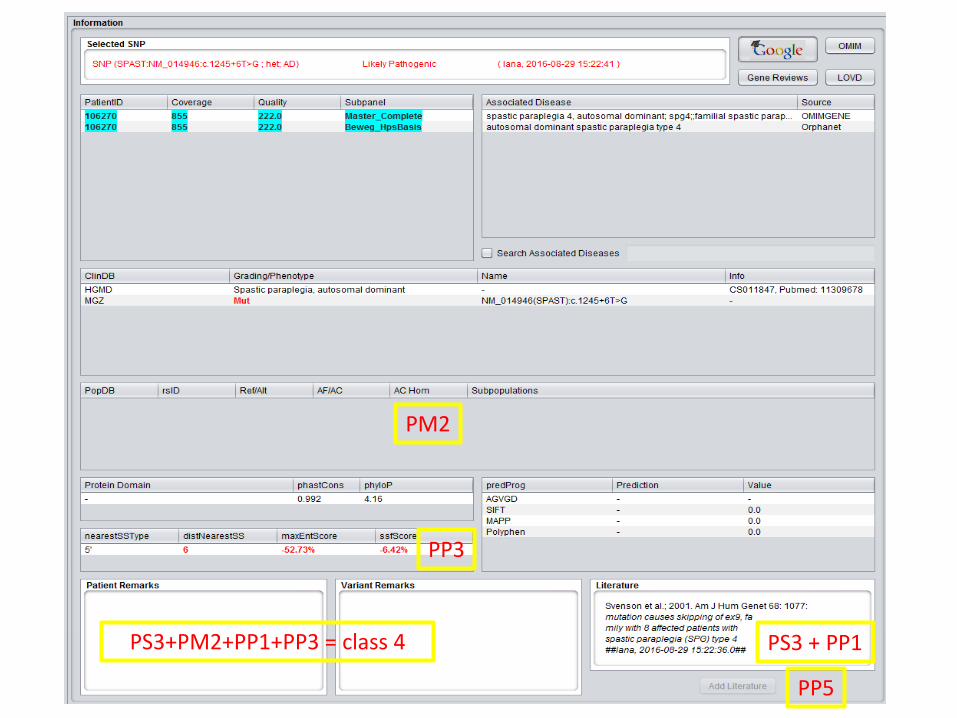
PM2
PS3 + PP1
PP3
PP5
PS3+PM2+PP1+PP3 = class 4

ACMG GUIDELINES
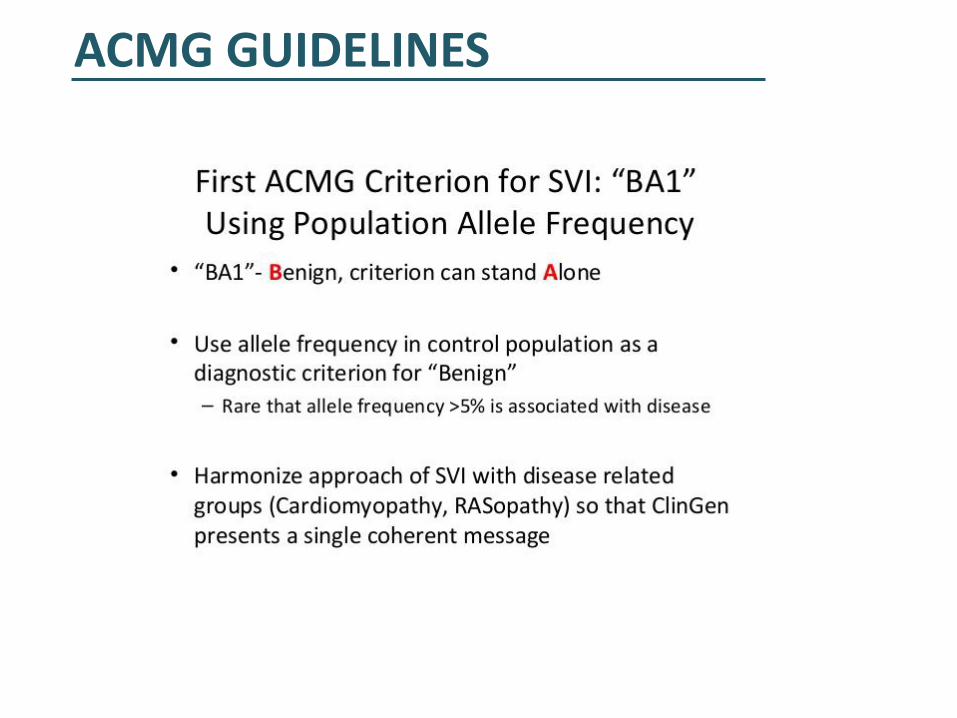
What are the requirements? • Detailed population frequency data • Thorough literature search (time consuming, often not consistent) • Clinical databases / LSDB´s • Link genes to associated phenotypes and MOI (latter is sometimes not trivial) • Bioinformatic prediction integrated (protein, splice sites)
He who makes no mistakes, makes nothing …. you won´t get the best possible classification for your variant (=VUS)

InSiGHT classification rules (4 MMR genes) • VIC (J.P. Plazzer) • monthly conference calls, ~10 variants classified per session • InSiGHT-LOVD DB
ENIGMA classification rules (BRCA1/BRCA2)
OTHER GUIDELINES

INSIGHT HNPCC CLASSIFICATION

ENIGMA BRCA CLASSIFICATION

• 9 CSER-labs classifying 99 variants (9 all, 90 by 3 labs, 2 labs contrib. ACMG)
• Using the lab´s own method and the ACMG-AMP Guidelines
• Agreement within labs was high: 79% concordance
• BUT: only 34% concordance for either classification system across labs
• After consensus discussion and detailed review: 71% concordance
EVALUATION OF INTER-LABORATORY CONCORDANCE

EVALUATION OF INTER-LABORATORY CONCORDANCE
SGP7 BTD
No phenotype when homozygous (found homo in ExAC) Pathogenic only when in combination with pathogenic variant

EVALUATION OF INTER-LABORATORY CONCORDANCE
Reasons for Discrepancy • VUS criteria: conflicting pathogenic and benign lines of evidence
Some labs allowed one line of conflicting benign evidence of only a supporting level
(e.g., predictions) to override otherwise strong evidence of pathogenicity. Expert
judgment: disregarding limited conflicting evidence
• 2 discordant variants needed one labs internal data (not accessible to the other)
• Interpreting same variant for different associated conditions (different disease
frequencies…)
• Tabulation errors: codes did not support classification (use a classification tool)

EVALUATION OF INTER-LABORATORY CONCORDANCE
Reasons for Discrepancy • VUS criteria: conflicting pathogenic and benign lines of evidence
Some labs allowed one line of conflicting benign evidence of only a supporting level
(e.g., predictions) to override otherwise strong evidence of pathogenicity. Expert
judgment: disregarding limited conflicting evidence
• 2 discordant variants needed one labs internal data (not accessible to the other)
• Interpreting same variant for different associated conditions (different disease
frequencies…)
• Tabulation errors: codes did not support classification (use a classification tool)
ACMG GUIDELINES

EVALUATION OF INTER-LABORATORY CONCORDANCE

ACMG GUIDELINES
ACMG GUIDELINES

TAKE HOME MESSAGE ….
Like every new technology / method the ACMG-AMP classification rules need training and time
Eventually we will get used to it …..






























