Embed Size (px)
DESCRIPTION
a
Citation preview

Case report and review of the literature
CONSERVATIVE MANAGEMENT OF MAJOR BLUNT RENAL TRAUMA IN A CHILD: IS IT A SAFE THERAPEUTIC MODALITY? CASE REPORT AND REVIEW OF THE LITERATURE
Zlatan Zvizdić*1, Emir Milišić1, Carmen Dedić1, Amra Džananović2 Lejla Milišić2.
1Clinic of Pediatric Surgery, Clinical Center University of Sarajevo, Bolnička 25, 71000 Sarajevo, Bosnia and Herzegovina
2Clinic of Radiology, Clinical Center University of Sarajevo, Bolnička 25, 71000 Sarajevo, Bosnia and Herzegovina
* Corresponding author
ABSTRACT
Renal parenchymal injuries can lead to significant morbidity and mortality, but there is still no consensus about the optimal treatment of the high-grade renal injuries. Hundreds of papers about the modalities of treatment of renal injuries have been published in medical literature, but there remains a regional and individual differences in the treatment of children and adults with high-grade kidney injury, which impedes the establishment of a unified algorithmic treatment. The aim of this study was to contribute to the knowledge that nonoperative management strategy can be safely chosen in children with severe blunt renal injuries who were hemodynamically stable, as the preliminary step or as the definitive treatment.
Key words: Blunt renal trauma, nonoperative management, children
INTRODUCTION
Kidney injuries occur in approximately 10% of all blunt abdominal trauma cases [1]. Blunt trauma is the most common type of the injury of the kidney and represent 82%-95% of all renal trauma [2]. CT scan has proved to be an effective means of staging renal trauma [3]. Based on severity, renal injuries were divided in five grades using the classification of the organic injuries survey committee from the American Association of Surgery in Trauma (AAST) [4]. (Table 1)
Table 1. Organ Injury Scale for kidneyAAST Classification
Grade Findings
I Parenchymal contusions and isolated subcapsular hematomasII Superficial cortical lacerations less than 1 cm in depth and nonexpanding
perirenal hematomasIII Lacerations greater than 1 cm in depth without extension into the collecting
system or evidence of urinary extravasationIV Deep lacerations that involve the collecting system, traumatic thrombosis of a
segmental renal arterial branch, and injuries to the main renal artery not associated with renal devascularization
V Shattering of the kidney into multiple fragments and devascularizing injuries to the renal pedicle, avulsion of the renal artery, as well as in situ thrombosis of an intact renal artery

Informations from ref. 4.
Blunt renal trauma may be classified as minor or major [4]. More than three quarters of cases of renal trauma (75-85%) are classified as minor and majority of them is treated conservatively. High-grade renal injuries comprise the remaining 15% of cases with grade V injuries representing only 5% of blunt renal injuries [4]. The reported incidence of high-grade renal injuries is 1%-2% of all traumas [5]. The conservative management of grade III to IV renal injuries in the setting of blunt trauma has been well established, the treatment of grade V injury remains a subject of debate. In the past, grade V injuries treated surgically, while recent papers suggest that this grade can be treated conservatively in hemodynamically stable patients. We report a case of a grade III renal injury with a large perinephritic hematoma in a 7-year boy managed successfully with conservative measures.
CASE REPORT
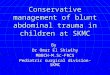
A 7 year-old boy who sustained blunt abdominal trauma following fall on the stair, presented to emergency room of University Clinical Center Sarajevo with complaints of lower left abdominal pain and left back pain since the time of injury. No history of hematuria. The physical examination revealed marked tenderness present in the left lower abdomen and the left lumbar region. The patient was hemodynamically stable (systolic blood pressure > 90 mm Hg, puls 96 per minute). Serum haemoglobin was 110 g/L. Urine analysis showed microscopic haematuria (40-50 RBCs). At admission ultrasonograpy of abdomen showed features suggestive of left renal injury. Computerized Tomography (CT) of the abdomen and pelvis with intravenous contrast demonstrated deep parenchymal laceration 2.1 cm in depth with active bleeding and a large perinephritic hematoma (Figure 1.).
Figure 1. Initial sagittal CT scan showing deep parenchymal laceration 2,1 cm in depth (white arrow) with a large perinephritic hematoma (black arrows).
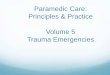
Three dimensional reconstruction of contrast CT showed left kidney laceration without contrast extravasation (Figure 2.).

Figure 2. Three dimensional reconstruction of contrast sagittal CT showing left kidney laceration without contrast extravasation
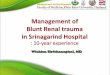
Base on the American Association for the Surgery of Trauma organ injury scale [4], the renal injury was compatible with a grade III injury. The opposite kidney was normal. Becase of the patient's hemodynamic stability, the boy was admitted to the pediatric surgery ward and treated conservatively with controlled fluid resuscitation, bed rest, frequent serum haemoglobin monitoring, IV antibiotics and analgesics. On day 3 repeated abdominal and pelvis CT scan showed no previously reported active bleeding with the persistence of laceration of the left kidney and perinephritic hematoma.
Figure 3. Sagittal computerized tomography after 72 h showing no evidence of the left perinephritic expanding hematoma (black arrows) and no evidence of active bleeding.
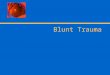
On the day 5 the the tenderness of the left lower abdomen and the left lumbar region decreased significantly. Urine analysis showed no evidence of microscopic hematuria. Abdominal ultrasonography on day 7 showed substantial resolution of the mass with residual reduced perinephritic hematoma. CT scan done on day 11 showed near complete resolving of renal laceration and perinephritic hematoma.

Figure 4. Sagittal computerized tomography on the day 11 showing a significant regresion of perinephritic hematoma (white arrows) with advanced healing of parenchymal laceration
All the time, vitals, hemoglobin level and serum electrolytes were normal. Patient was discharged on day 12 with oral antibiotics for 7 days. On follow up at 1, 3 and 6 month child was normotensive and ultrasonography findings were normal.
DISCUSSION
Due to differences in anatomy and physiology, as well as the higher incidence of pre-existing renal disease, children are more prone to renal injury than adults. Children's kidney is placed lower in the abdomen, more mobile, less protected by the lower ribs and the muscles of the abdomen and flank and perirenal fat is less developed. Also, the kidney of a child is proportionately larger than the adult kidney. Preservation of the kidney either by conservative treatment or operative reconstruction is an essential part of management of blunt renal injury. The decrease of surgical interventions in the recent years reflected better understanding of the natural history of blunt renal trauma [6]. The current indications for surgical exploration in children with blunt renal trauma and major renal lacerations (grades III-V) include a changing abdominal examination suggestive of a major intra-abdominal injury, persistent life-threatening bleeding with hemodynamic instability, expanding or pulsatile retroperitoneal hematoma, inability to stop persistent or delayed hemorrhage via selective vascular embolization and accompanying extraabdominal or intraabdominal lesions [7]. On the other hand, recent publications showed successful conservative treatment of high-grade renal injuries associated with high grade intraabdominal solid organs injuries [8]. However, a significant number of high grade renal injuries in children will heal with no intervention [1,9]. In fact, pilot study by Santucci et al [9] evaluated 2 047 blunt renal traumas and concluded that more than 75% high grade renal blunt trauma needed surgical interventions. The rate of surgical management of high grade renal injury due to blunt traumas had gradually decreased to 35% in 2010 [5]. The decrease of surgical interventions reflected better understanding of the natural history of blunt renal trauma. The safety of nonoperative treatment of major renal injuries in children has been confirmed by several studies [10,11,12]. Fitzerald et al. instituted a conservative management protocol for blunt renal trauma in pediatric patients and suggested that nearly 80% of pediatric patients with high-grade blunt renal trauma were able to be management expectantly [13]. They used conservative approach in cases that were hemodynamically stable or had a favorable response with up to 2 units of blood transfused and no operative renal lesion on imaging [13]. Although hematuria is a common sign of renal trauma, being present in 80–94% of cases [14], the decision for renal imaging in diagnosing

and grading the renal injuries should not be based on urine analysis solely. Numerous studies have shown that there was no absolute correlation between the presence, absence or degree of hematuria and the severity of the renal injury [14,15,16]. The patient’s clinical status, history, and injury mechanism should also be considered. In our case, microscopic hematuria (<50 red blood cells per high-powered field) is no correlated with the severity of renal injury. Therefore, we believe that the ideal diagnostic methodology in the cases of blunt abdominal trauma would be performing abdominal/pelvic CT and urinalysis on all children who presented with blunt abdominal trauma. In fact, abdominal/pelvic CT scanning is the most accurate screening test for high-grade renal injuries in children since the rate of diagnosis of blunt renal trauma by computed tomographic is 100% [17]. Other diagnostic methods have the lower diagnostic rate, so that the ultrasonography has the diagnosis rate of 91% and intravenous pyelography (IVP) of 82% [17].
CONCLUSION
Based on our experience with this case and the cases presented in recent medical literature, we think that conservative management of III-IV grade renal hemodynamically stable injuries is appropriate in the management of renal trauma. We believe that conservative treatment reduces the number of emergency operations and the numbers of unnecessary nephrectomies as well as the rate of early and late postoperative complications. Certainly, each case must be individually analyzed and a decision on the type of treatment should be made on the basis of the mechanism of injury, radiological findings and the patient's hemodynamic stability.
REFERENCES
1. Santucci R, Wessells H, Bartsch G, Descotes J, Heyns CF, McAninch JW et al: Evaluation and management of renal injuries: Consensus statement of the renal trauma subcommittee BJU Int 2004; 93:937-954.
2. Wessells H, Suh D, Porter JR, Rivara F, MacKenzie EJ, Jurkovich GJ, Nathens AB. Renal injury and operative management in the United States: results of a population based study. J Trauma 2003; 54: 423-430.
3. Alonso RC, Nacenta SB, Martinez PD, Guerrero AS, Fuentes CG. Kidney in danger: CT findings of blunt and penetrating renal trauma . Radiographics 2009;29(7):2033-2053.
4. Moore EE, Shackford SR, Pachter HL, McAninch JW, Browner BD, Champion HR, et al. Organ injury scaling: spleen, liver and kidney. J Trauma 1989; 29:1664-1666.
5. Dugi DD 3rd, Morey AF, Gupta A, Nuss GR, Sheu GL, Pruitt JH. American Association for the Surgery of Trauma grade 4 renal injury substratification into grades 4a (low risk) and 4b (high risk). J Urol 2010;183(2):592-597.
6. Saidi A, Bocqueray F, Descotes JL, Cadi P, Terrier N, Boillot B, Rembeaud JJ. Blunt kidnez trauma: A ten-year experience. Progrol 2004; 14: 1125-1131.
7. Bozeman C, Carver B, Zabari G, Caldito G, Venable D. Selective operative management of major blunt renal trauma. J Trauma 2004; 57: 305-309.
8. Stahlschmidt CM, Stahlschmidt FL, Von Bahten LC, Nicoluzzi JE, Costa T. Conservative management of a grade V renal trauma associated with a grade III

hepatic lesion: is it possible? Ulus Travma Acil Cerrahi Derg. 2006 Oct;12(4):311-314.
9. Santucci RA,McAninch JW. Diagnosis and management of renal trauma: past, present and future. J Am Coll Surg 2000;191(4):443-451.
10. Russell RS, Gomelsky A, McMahon DR, Andrews D, Nasrallah PF. Management of grade IV renal injury in children. J Urol 2001; 166: 1049–1050.
11. Nance ML , Lutz N, Carr MC, Canning DA, Stafford PW. Blunt renal injuries in children can be managed nonoperatively: outcome in a consecutive series of patients. J Trauma 2004; 57(3):474-478.
12. Eassa W , El-Ghar MA, Jednak R, El-Sherbiny M. Nonoperative management of grade 5 renal injury in children: does it have a place? Eur Urol. 2010;57(1):154-161.
13. Fitzerald CL, Tran P, Burnell J, Broghmmer JA, Santucci R. Instituting a conservative management protocol for pediatric blunt renal trauma: Evaluation of a prospectively maintained patient registry. J Urol 2011; 185: 1058-1064.
14. Thorp AW, Young TP, Brown L. Test Characteristics of Urinalysis to Predict Urologic Injury in Children. West J Emerg Med. 2011;12(2):168-172.
15. Carlin BI, Resnick MI. Indications and techniques for urologic evaluation of the trauma patient with suspected urologic injury. Semin Urol 1995; 13: 9–24.
16. Brandes SB, McAninch JW. Urban free falls and patterns of renal injury: a 20-year experience with 396 cases. J Trauma 1999; 47: 643–650.
17. He B, Lin T, Wei G, He D, Li X. Management of blunt renal trauma : An experience in 84 children . Int Urol Nephrol 2011 Apr 24. [Epub ahead of print]
Address:Zlatan Zvizdić, Pediatric Surgeon MD. MScClinic of Pediatric SurgeryClinical Center University of SarajevoBolnička 25, 71000 SarajevoBosnia and HerzegovinaPhone: ++387 33 297 [email protected]















![MDCTof blunt renal trauma: imaging findings and ... · withother visceral injuries, with the majorityof isolatedrenal injuries represented by low-grade lesions [8–10]. Although](https://img.pdfslide.net/doc/110x75/5ea60cc29e786b3aa956feb3/mdctof-blunt-renal-trauma-imaging-findings-and-withother-visceral-injuries.jpg)