Embed Size (px)
Citation preview
Multi‐Agency Protocol Safeguarding Children and Young People Living with Parental Substance Misuse. March 2012
1
2
Contents Contents 2
Foreword 3
1. Introduction 4
2. Aims of the Protocol 6
3. Principles 7
4. Identifying the needs of children and unborn babies where their parents or
carers misuse substances 8
5. Working with partner agencies to assess families needs 12
6. Identifying children in need of protection and/or who are at risk of significant
harm 14
7. What to do if you’re worried that a child is at risk of significant harm 16
8. Multi-agency information sharing 19
9. Resolving professional differences 20
Appendix 1: Assessment tool 21
Appendix 2: The impact of parental drug/alcohol use on children 24
Appendix 3: Confidentiality and information sharing in Bromley Drug and Alcohol
Services 26
Appendix 4: Referral Pathways between Children's Social Care and Adult
Substance Misuse Services 28
Appendix 5: Sources 33
Appendix 6: Who to contact in Bromley 34
Foreword This multi-agency protocol has been developed to encourage all agencies in Bromley to meet the challenge of delivering their responsibilities to safeguard and promote the well-being of children and young people who are living with parents or carers who misuse drugs or alcohol. Bromley Safeguarding Children Board (BSCB) endorses the London Child Protection Procedures which sets out guidance of how to safeguard such children and young people. A working group to review and update the protocol also drew on the guidance from the revised statutory guidance Working Together to Safeguarding Children (WT2010) and the National Treatment Agency to set out the key factors in this area of work for Bromley. Our vision is for every child in Bromley to be safe from harm or to know that if they are harmed, those they turn to for support know what to do to protect them. Research informs us that children and young people at increased risk of abuse or neglect are often living with parents who have a combination of problems - the trio of substance misuse, domestic violence and parental mental ill health (WT 2010 para 9.19). Working Together to Safeguard Children states that; “It is hard to know with any degree of certainty how many children are living with parents who are problem drug users as such behaviour is against the law and characterised by denial and secrecy…..To understand how problem drug use can affect parent’s capacity to meet the developmental needs of their children is far from simple and it is important not to generalise or make assumptions about the impact on children of parental drug misuse” (WT 2010 paras 9.38- 9.39). The day to day actions of professionals working in partnership can support the well being of a child or young person living in these circumstances. These might include taking account of : poor housing, nutrition and mental health Emotional attachment and development Supportive family members Regular checks on the child or young person
The BSCB challenges the partnership to consider how it implements the protocol within its agency, fostering partnership working at every level. I hope this protocol will be used by all professionals who work with children and young people living with parental substance misuse. Jenny Dibsdall Chair, Bromley Safeguarding Children Board
3
4
1. Introduction 1.1. This protocol should be used whenever there are concerns about the well-
being or safety of children whose parents or carers have substance misuse problems, specifically where these difficulties are impacting, or are likely to impact, on their ability to meet the needs of their children. It also applies to pregnant women who have substance misuse problems, where their partners are known to have substance misuse problems or where someone with substance misuse problems is living in a household where children are present. This protocol should be read in conjunction with local guidance on service provision and child protection thresholds which are included in ‘The Child’s Journey in Bromley’.
1.2. In this protocol the term substance misuse refers to alcohol, prescribed and
illegal drugs, over the counter medicines and solvents. We also are describing problematic use and its associated dependence.
1.3. Substance Misuse itself is not sufficient reason for considering a child to be at
risk of significant harm or to start child protection procedures. However, the misuse of drugs and alcohol by parents is an important factor to consider when assessing a parent’s skills to care for their child and the risks to the child.
1.4. Research tells us that one in three adults have used drugs at least once,
although the ‘problem drug users’ (using opiates such as heroin and cocaine) make up less than 1% of the population in England. The General Lifestyle survey (2008) suggests that 7% of men and 4% of women regularly drink at higher-risk levels (that’s 6 units a day for a woman and 8 for a man). Another 20% of men and 14% of women engage in what is called binge drinking.
1.5. As the intensity and range of usage varies from individual to individual, this
protocol advocates a careful individual analysis of the individual’s use and how that impacts on their pregnancy and/or parenting of children.
1.6. Parental or carer drug or alcohol use can reduce the capacity for effective
parenting. In particular the children of parents or carers who are dependent on drugs or alcohol are more likely to develop behaviour problems, experience low educational attainment, and be vulnerable to developing substance misuse problems themselves. Some children’s health or development may be impaired to the extent that they are suffering or likely to suffer significant harm. (National Treatment Agency 2011 http://www.nta.nhs.uk/families.aspx).
1.7. Parental substance misuse is recognised as being one of the significant
factors in child deaths or serious injury, often in association with mental health or domestic violence (Brandon et al 2008). It can have an impact on parents’ ability to look after their children through lack of awareness of the child’s needs, lack of emotional control, neglect of the child’s physical needs and poor attachment (Cleaver et al, 1999).
1.8. Becoming a parent can be the trigger for a drug user to seek treatment and
stop using drugs or drinking excessively. Many behaviours linked to drug or alcohol use can reduce a person's ability to parent effectively. The impact can take a variety of forms affecting people in different ways and can depend on
the individual’s current mental state, tolerance of the drug or alcohol, expectations, and personality. It can affect concentration, induce sleep, reduce co-ordination, or to lose inhibitions which might diminish their self control.
1.9. Substance misuse is one of a trio of frequent factors in the family
background that is evident in the vast majority of serious case reviews where a child has died or suffered significant harm. The other factors are parental mental ill health and domestic violence.
1.10. The Advisory Council on the Misuse of Drugs defines substance misuse as a
condition which may cause an individual to experience social, psychological, physical or legal problems related to intoxication and / or regular excessive consumption, and / or dependence, as a consequence of their use of drugs or other chemical substances.
1.11. For the children involved, having a parent in treatment can be a protective
factor. This protocol encourages them to seek help, support and treatment to address their substance misuse problem to reduce the harm it causes to the individual, family and society.
5
2. Aims of the Protocol 2.1. The aim of this protocol is to improve understanding of the impact of an adult's
substance misuse problems on children's lives and to ensure that children living in families where there is substance misuse are appropriately safeguarded through:
• ensuring that there is early intervention by universal and specialist
services to improve the identification of children in need;
• ensuring the provision of co-ordinated services to families in which there are dependent children of parents, carers or pregnant women with substance misuse problems
• ensuring good co-operation and collaborative decision-making between services on whether child protection issues are present such as in assessment processes.
6
3. Principles 3.1. All professionals who come into contact with children, their parents or carers
in their work have a statutory duty to safeguard and promote the welfare of the child (Children Act 2004). This applies to volunteers as well as staff working in statutory or non-statutory agencies as well as community organisations. The following principles underpin work to safeguard children living with parental substance misuse.
• The child’s welfare and safety is paramount whether you work
predominantly with adults, parents, children or families.
• Where parents, carers or pregnant women have substance misuse issues, consideration must be given to the needs of the child and their development.
• Risks to children are significantly reduced through effective information sharing and multi-agency working. Agencies have a duty to share information where there are concerns for the welfare or safety of a child. The absence of consent from parents or carers to liaise with appropriate agencies should not be a barrier to prevent liaison with the appropriate agencies. For further information on consent and confidentiality see Section 8 and Appendix 3.
• Assessments and interventions should be based on observable evidence, and objective judgements. It is important to be aware of the particular stereotypes and assumptions that exist about people who use various substances. It is essential that these stereotypes and assumptions do not influence the assessment.
• Improved outcomes for children can be achieved through building effective relationships with the children, parents and through partnership working with other agencies so that possible consequences are fully understood.
• Substance misuse by parents and pregnant women should not be seen in isolation, but needs to be placed in a wider context which includes the impact on the individual and the family.
• Parents and pregnant women who misuse substances should be supported to acquire necessary skills to put their child’s welfare first.
• The wishes of children of parents who misuse substances must be taken into account in any decisions made on their behalf and on behalf of their family.
• Assumptions that parents or others in the home are misusing or have stopped misusing substances should not be based on whether they are engaged with services.
• Consideration should be given to the role of the child/young person as a young carer.
7
4. Identifying the needs of children and unborn babies where their parents or carers misuse substances
4.1. Identifying the needs of children where their parents or carers misuse
substances is a role for everyone working with children and families including health, education, voluntary organisations and adult focused agencies (including substance misuse agencies and adult mental health services).
4.2. Adult focussed agencies should include the needs of the child and impact of
parental/carer substance misuse within their assessments of adults. Children living in these households may be in need of assessment for services provided by a range of agencies from universal and early intervention to specialist services.
4.3. When assessing the situation it is important to explore the substance misuse
from the child’s point of view and the impact it has on his/her life and development.
4.4. The table overleaf can be used by professionals alongside the Bromley
Safeguarding Continuum of Need and Intervention triangle in ‘The Child’s Journey in Bromley’ to help identify the types of services and intervention that are needed.
Identifying substance misuse in pregnancy 4.5. Some pregnant women who misuse substances do not come for antenatal
care until late in pregnancy or when they are in labour. Some may feel that it is better not to reveal their substance misuse to antenatal care staff as they fear the attitudes of staff and the possible involvement of statutory services, and some women may not know that they are pregnant, or may not be clear about the duration of the pregnancy.
4.6. Agencies in the community can play a key role in supporting these women in
a range of ways. This includes identifying substance misuse / pregnancy at an early stage, referring on to appropriate help and support, identifying risks, and providing support and advice around pregnancy and/or substance misuse.
4.7 Where appropriate, substance misuse agencies and other agencies should
offer and carry out a pregnancy test with the consent of the woman. If the woman is pregnant she should be encouraged to inform her GP as soon as possible and refer herself/or be referred to Maternity Services.
8
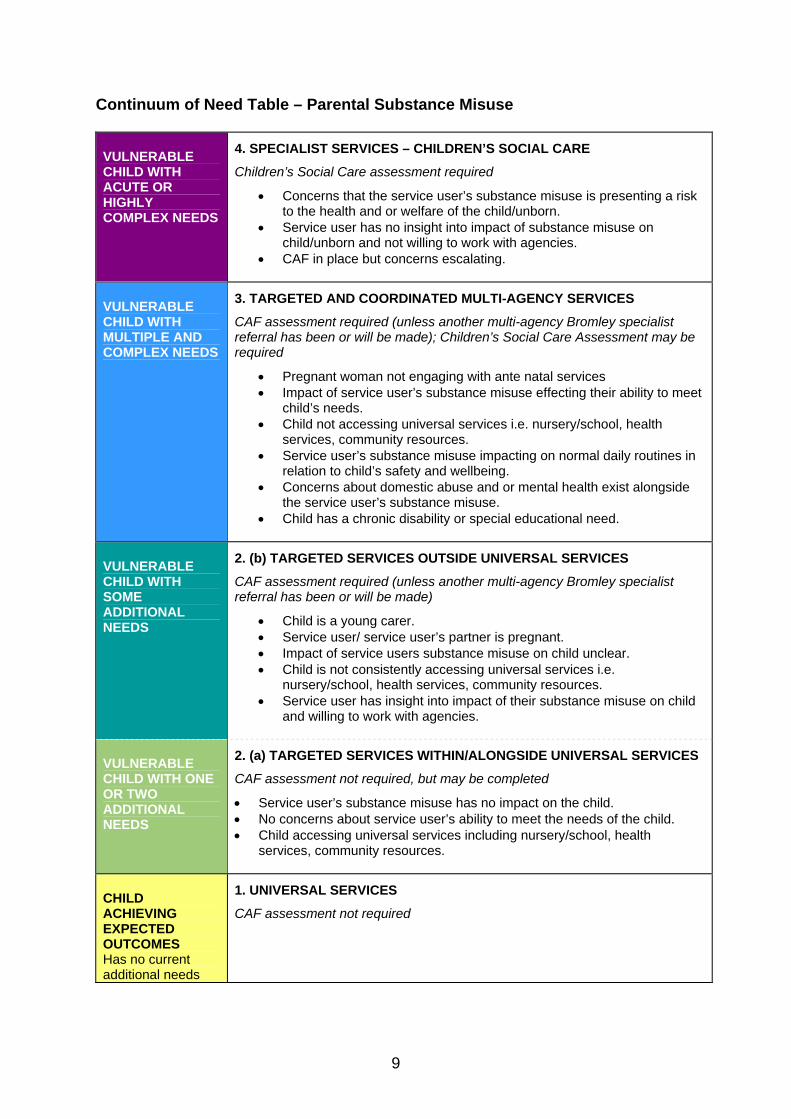
Continuum of Need Table – Parental Substance Misuse
VULNERABLE CHILD WITH ACUTE OR HIGHLY COMPLEX NEEDS
4. SPECIALIST SERVICES – CHILDREN’S SOCIAL CARE
Children’s Social Care assessment required
• Concerns that the service user’s substance misuse is presenting a risk to the health and or welfare of the child/unborn.
• Service user has no insight into impact of substance misuse on child/unborn and not willing to work with agencies.
• CAF in place but concerns escalating.
VULNERABLE CHILD WITH MULTIPLE AND COMPLEX NEEDS
3. TARGETED AND COORDINATED MULTI-AGENCY SERVICES
CAF assessment required (unless another multi-agency Bromley specialist referral has been or will be made); Children’s Social Care Assessment may be required
• Pregnant woman not engaging with ante natal services • Impact of service user’s substance misuse effecting their ability to meet
child’s needs. • Child not accessing universal services i.e. nursery/school, health
services, community resources. • Service user’s substance misuse impacting on normal daily routines in
relation to child’s safety and wellbeing. • Concerns about domestic abuse and or mental health exist alongside
the service user’s substance misuse. • Child has a chronic disability or special educational need.
VULNERABLE CHILD WITH SOME ADDITIONAL NEEDS
2. (b) TARGETED SERVICES OUTSIDE UNIVERSAL SERVICES
CAF assessment required (unless another multi-agency Bromley specialist referral has been or will be made)
• Child is a young carer. • Service user/ service user’s partner is pregnant. • Impact of service users substance misuse on child unclear. • Child is not consistently accessing universal services i.e.
nursery/school, health services, community resources. • Service user has insight into impact of their substance misuse on child
and willing to work with agencies.
VULNERABLE CHILD WITH ONE OR TWO ADDITIONAL NEEDS
2. (a) TARGETED SERVICES WITHIN/ALONGSIDE UNIVERSAL SERVICES
CAF assessment not required, but may be completed
• Service user’s substance misuse has no impact on the child. • No concerns about service user’s ability to meet the needs of the child. • Child accessing universal services including nursery/school, health
services, community resources.
CHILD ACHIEVING EXPECTED OUTCOMES Has no current additional needs
1. UNIVERSAL SERVICES
CAF assessment not required
9
Antenatal assessment and care 4.8 When an agency identifies a pregnant woman/partner of a pregnant woman
experiencing substance misuse problems a Common Assessment Framework (CAF) should be considered and if they are not already involved, a referral made to adult substance misuse services. This should include gathering relevant information from the GP and Substance Misuse Services, in addition to any other agencies involvement, to ensure that the full background is obtained about any existing or previous diagnosis, or treatment for mental illness. This is especially important where service awareness of earlier births may need to be clarified, for example, in the case of older or overseas children. The Assessment tool in Appendix 1 can be used as a useful tool.
4.9 On no account should any agency inform a pregnant woman to stop misusing
substances without first referring the matter to the woman’s obstetrician and key worker or discussing with the key worker in substance misuse services. The immediate withdrawal of such drugs or alcohol could result in premature birth or miscarriage.
4.10 All pregnant women should be asked about their use of prescribed and non-
prescribed drugs, both legal and illegal, as part of routine enquiries about general health during pregnancy. Time should be allowed for the exploration of the patient's and the professional's concerns about the risks for both the mother and the child. This needs to be done sensitively so that the woman is not deterred from seeking help, even if she continues to use. However practitioners should ensure that the woman and her partner are aware of the impact of the following behaviours: • The use of tobacco, street drugs, alcohol and some over the counter
drugs, including the adverse effects of some medicines • Chaotic drug/alcohol use; e.g. polydrug use, erratic dosage precipitating
withdrawals or intoxication • Injecting and sharing of injecting paraphernalia • Unprotected sexual activity
4.11 If the woman's partner misuses substances, they should be encouraged to
access treatment as this increases the chances that the patient will be able to control her substance misuse during pregnancy. Agencies working with men who misuse substances should consider the impact on unborn children of the service users partner and make appropriate referrals to ensure support and assessment.
4.12 Cases of ante natal substance misuse should be referred to the maternity
cause for concern meetings via the woman’s midwife. These meetings plan intervention and monitor progress throughout pregnancy and are often undertaken along side CAF and other assessment processes such as Child in Need and Section 47 child protection enquiries.
4.13 Substance misuse workers, maternity staff and other practitioners working
with pregnant women, their partners, children and their families should consider the following as a part of the ongoing assessment process:
10
• Which substances are being used • Current amounts of substance use • Patterns of use • Route of administration (injecting or smoking) • Other risk behaviour related to the substance use • Whether the woman is receiving substitute medication which means that
they are stable • Stage of pregnancy • The woman’s support networks • The needs of unborn child • Whether the women has other children; their living situation; and their
main carer / guardian 4.14 It is recognised that assessment is an on-going process and practitioners
must ensure that the other key professionals involved with the woman are aware of the following in line with confidentiality agreements: • Changes in amounts, patterns, or routes of administration
(injecting/smoking) of drug/alcohol use • Changes in accommodation • Changes in relationships / support networks
4.15 A multi-agency meeting may be called at any point, by any professional,
during the course of the pregnancy to coordinate the care plan. Risk factors: Co-morbidity 4.5 The coexistence of mental health issues and substance misuse is generally
referred to as 'comorbidity' or 'dual diagnosis' and people with mental health issues and substance misuse problems have particular needs that must also be met with a co-ordinated approach from substance misuse agencies and mental health services.
4.6 Since both mental health issues and substance misuse problems carry a
powerful social stigma, difficulties may arise for parents with co-morbidity in accessing either the mental health or substance misuse agencies. In some instances Children’s Social Care Referral and Assessment Teams may be the initial agency to identify these issues. The allocated Social Worker should therefore consider referring these parents to the Stabilisation and Assessment service within the substance misuse service in order to be assessed. This assessment will include a risk assessment and aim to maximise the support that the parents receive.
4.7 Where parents have both mental health issues and substance misuse
problems, a referral should be made to either the mental health service or substance misuse service, depending on the priority issues and the services will work together.
4.8 Parents with substance misuse and mental health issues are not necessarily
unable to successfully parent their children. However, for many such parents there is a clear need for support and access to joined up services.
11
5 Working with partner agencies to assess families needs
5.1 Professionals should familiarise themselves with the local threshold criteria for
referral to services based on children’s needs which are set out in ‘The Child’s Journey in Bromley’.
Using the Common Assessment Framework (CAF)
5.2 The Common Assessment Framework (CAF) can be carried out at anytime
that you have concerns about the child’s welfare and need greater clarity. The use of the CAF process enables the needs of the children to be identified at an early stage and can be used when:
• you are worried about how well a child is progressing in terms of
health, welfare, behaviour, learning;
• parents have raised concerns with you;
• needs are unclear and it would help to have them clearly identified;
• needs go beyond the service your agency provides. 5.3 The CAF Team can be contacted at any point for further information and to
discuss if it is appropriate to do a CAF. Agencies can also contact the CAF Team to identify whether a CAF has already been initiated. Where a CAF already exists for a child, then your agency can update the CAF with the new information you hold about the family and contribute to the multi-agency support for the child. Contact details for the CAF Team are in Appendix 6.
5.4 Where there are a number of professionals involved with a child, a Team
around the Child (TAC) approach can help practitioners to come together and assess those needs and decide with the child/ family a course of action to provide the services needed. Where consent is not given by parents or carers to undertake a CAF, this must be discussed with the child protection lead in your agency to decide whether there is sufficient evidence to support a referral to Children’s Social Care.
Referral to Adult Substance Misuse Services 5.5 Services for children and young people work with the family as a whole, with
the child’s needs as the focus. These services should consider parental substance misuse when making an assessment of the child’s needs. Agencies should incorporate the themes from the assessment tool in Appendix 1 into existing assessment procedures to help ensure that children receive an appropriate assessment.
5.6 Referral to adult substance misuse services should always be made if there is
concern about an individual’s substance misuse which indicates a risk to the service user themselves or to others, particularly children. The substance misuse service can also be contacted for consultation before a formal referral
12
5.7 If there is an immediate danger to the service user or others, including a child,
the Police must be contacted via 999. Staff must ensure that their decision and agreed course of action is fully and accurately documented, signed and dated. Contact with the GP and Substance Misuse Services is essential to ensure that the full background is obtained regarding any information about previous or current treatment or referrals.
5.8 Triggers that may indicate that a referral should be made to Substance
Misuse Services for parents include:
• Previous or current history of significant substance misuse.
• Current intravenous drug use.
• Excessive drug/alcohol use.
• History of binge drug or alcohol use.
• Drug paraphernalia left lying around or clearly visible in the household.
• Past or recent history of overdose (depending on the nature and intention of the overdose it may be appropriate to refer to mental health services e.g. for overdoses of prescription drugs).
• Factors such as domestic violence, sex working and homelessness which may be connected with a substance misuse problem.
• A child’s or other’s expression of concern regarding change in parent’s and/or carer’s behaviour or attitude.
• Co-morbidity with mental health problems. Joint working 5.9 Joint visits between key agencies working with families should be made to
fully assess the needs of the family and to plan joint working arrangements.
13
6 Identifying children in need of protection and/or who are at risk of significant harm
Signs and symptoms in pregnancy
6.1 Maternal substance misuse while pregnant may place the unborn child in
danger. In problem drug use, factors include the composition of the drug, the gestation of pregnancy as well as how the drug is administered and the duration of the substance misuse. Risks include: low birth weight, premature delivery, perinatal mortality and cot death.
6.2 The effect of alcohol on the developing foetus is related to the amount and
pattern of alcohol consumption and the stage of pregnancy. Drinking in the first three months of pregnancy is linked with increased miscarriage rates. Drinking alcohol can lead to Foetal Alcohol Syndrome, whose features include: deficiencies in height and weight, distinctive pattern of facial features and physical characteristics and central nervous system dysfunction.
Signs and symptoms in new born babies and children
6.3 Babies experiencing withdrawal symptoms may become sleepy and
unresponsive, have a high-pitched crying and difficulties feeding, all of which can affect attachment between mother and child.
6.4 The London Child Protection Procedures set out the risks that may arise for
children:
• Substance misuse affecting their parent/s’ practical caring skills: perceptions, attention to basic physical needs and supervision which may place the child in danger (e.g. getting out of the home unsupervised);
• Substance misuse may also affect control of emotion, judgement and quality of attachment to, or separation from, the child;
• Parents experiencing mental states or behaviour that put children at risk of injury, psychological distress (e.g. absence of consistent emotional and physical availability), inappropriate sexual and / or aggressive behaviour, or neglect (e.g. no stability and routine, lack of medical treatment or irregular school attendance);
• Children are particularly vulnerable when parents are withdrawing from drugs;
• The risk is also greater where there is evidence of mental ill health, domestic violence and when both parents are misusing substances;
• There being reduced money available to the household to meet basic needs (e.g. inadequate food, heat and clothing, problems with paying rent [that may lead to household instability and mobility of the family from one temporary home to another]);
14
• Exposing children to unsuitable friends, customers or dealers;
• Normalising substance use and offending behaviour, including children being introduced to using substances themselves;
• Unsafe storage of injecting equipment, drugs and alcohol (e.g. methadone stored in a fridge or in an infant feeding bottle). Where a child has been exposed to contaminated needles and syringes (see also LCPP section 5.4 Blood-borne viruses);
• Children having caring responsibilities inappropriate to their years placed upon them (see LCPP section 5.47 Young carers);
• Parents becoming involved in criminal activities, and children at possible risk of separation (e.g. parents receiving custodial sentences);
• Children experiencing loss and bereavement associated with parental ill health and death, parents attending inpatient hospital treatment and rehab programmes;
• Children being socially isolated (e.g. impact on friendships), and at risk of increased social exclusion (e.g. living in a drug using community);
• Children may be in danger if they are a passenger in a car whilst a drug / alcohol misusing carer is driving.
6.5 Children whose parent/s are misusing substances may suffer impaired growth and development or problems in terms of behaviour and / or mental / physical health, including alcohol / substance misuse and self-harming behaviour.
Signs and symptoms in older children
6.6 For the older child research indicates that children’s educational attainment
may suffer as children’s thoughts become occupied by their parent’s problems. Some believe they are to blame for their parents’ problem, the relationship between the parent and child may deteriorate and the child feels less important in their parent’s life. Such children may feel they need to grow up more quickly, take care of themselves, school work is neglected, and attendance at school may be erratic and there maybe difficulties forming friendships. For others school, clubs and friendships may offer respite. In adolescence there is also the possibility that a few young people mirror their parents coping strategies and experiment with drugs and alcohol themselves.
6.7 Further information about the impact of parental substance misuse on children
and unborn babies is available in Appendix 2.
15
7 What to do if you’re worried that a child is at risk of significant harm
Referrals to Children’s Social Care
7.1 A referral to Children’s Social Care must always be made if a parent, carer or
pregnant woman is considered to have significant substance misuse problems as indicated by the triggers given below. A referral must always be discussed with a manager or child protection lead officer. If there is an immediate danger to the service user or others, including a child, the Police must be contacted. Staff must ensure that their decision and agreed course of action is fully and accurately documented, signed and dated, and that a written referral follows any telephone conversation or referral.
7.2 Details on when and how to make a referral to Children’s Social Care are
included in The Child’s Journey (July 2011). If you are unsure about whether it is appropriate to make a referral, discuss this with the children’s social care referral and assessment team first (see Appendix 6 for contact details).
7.3 Triggers that may alert for a referral to children’s social care for child
protection are given below. This is not an exhaustive list and is provided to assist professional decision-making:
• Step up from Common Assessment Framework (CAF)/ Team around
the Child (TAC) – where a CAF/TAC have been in place and the concerns escalate.
• Concerns that parents/carers substance misuse is presenting a risk to the health / and or welfare of the child.
• Pregnant women who are substance misusing, and where there are concerns about the impact on an unborn child, or a woman’s ability to meet the child’s needs once born.
• Concerns about domestic violence which exist along side substance misuse issues.
• Concerns about parental/carer mental health which exist alongside substance misuse.
• Where a family member or partner is a person identified as presenting a risk to children.
• When a pregnant woman or her partner has been identified with substance misuse, a pre-birth assessment must be undertaken in accordance with the London Child Protection Procedures (2010) Section 6.8.
• Children who have been the subject of previous child protection investigations, child protection registration, local authority care, or alternative care arrangements.
16
Assessment
7.4 When referrals are made to Children’s Social Care, the Referral & Assessment Team will decide whether it meets the threshold and consider whether an initial assessment and a core assessment are needed.
7.5 Where the referral meets the threshold, child protection procedures must be
initiated and the assessment conducted in line with the Framework for Assessment of Children in Need and their Families. As in all child protection work, all inquiries, investigations and assessments should be undertaken in partnership with parents whenever possible; this includes open discussion of concerns and expectations and clear information about plans.
7.6 As part of the assessment the Social Worker will need to consult and liaise
with any professional, including Drug/Alcohol Workers involved with the service user. This will include the various treatment and support options available. There will also be close liaison between the Social Worker and the Drug/Alcohol Worker and other involved agencies/professionals and ensure that they are aware of the actions that are being taken in individual cases.
Pre-birth assessments
7.7 A pre-birth initial assessment should be undertaken on all pre-birth referrals
and a professionals strategy meeting held where any one of the following applies:
• A sibling in the household is subject of a child protection plan.
• A sibling has previously been removed from the household either temporarily or by court order.
• The degree of parental substance misuse is likely to significantly impact on the baby’s safety or development.
• In addition to substance misuse, the degree of parental mental illness/impairment is likely to significantly further impact on the baby’s safety or development.
• There is a high risk of relapse of significant mental illness either in the ante- or post natal period.
• There is significant domestic violence reported within the household.
• There are concerns about parental ability to self-care and/or to care for the child e.g. unsupported young or learning disabled mother.
• Any other concern exists that the baby may be at risk of significant harm: o including a parent previously suspected of fabricating or
inducing illness in a child. o There is an individual living in the household with a substance
misuse problem.
17
7.8 If it is decided that a pre-birth inter-agency meeting is not needed this decision must be endorsed by a manager and the reason for such a decision must be clearly recorded on agency records.
7.9 A professional / planning meeting for the expectant mother may be called at
any time to update and coordinate the multi-agency care plan. The meeting should be an opportunity to discuss the mother's and baby's needs for the last part of the pregnancy and after the birth. The meeting should look at the needs of the woman, the father and baby; and identify any likely problems, and the services that parent(s) need to care for the new baby. It is important to note that the birth of the baby may create further problems, particularly if there is an unstable relationship or financial or housing difficulties.
7.10 If a pre birth conference is considered necessary this should be convened by
the 30th week of the pregnancy. The GP, health visitor, staff from the maternity and neonatal services and substance misuse services as well as relevant professionals from other specialist services such as mental health care coordinator should be invited. London Child Protection Procedures (2010) must be followed
On going review and assessment
7.11 Assessment and identification of parents, carers or children’s need for
services is not a static process. The assessment should also inform future work and build in evaluation of the progress and effectiveness of any intervention. Agencies should always take into account the changing needs of adults and children.
7.12 Where more than one agency continues to be involved in a joint assessment
or provision of services for parents or carers with substance misuse problems, and their children, regular review dates must be set to jointly review the situation and to ensure that inter-agency work continues to be co-ordinated. Each agency should document their own actions and responsibilities clearly and also the roles and responsibilities of other agencies.
7.13 There should always be the flexibility for cases to be reviewed at any time, or
jointly reassessed speedily before planned review dates, if new concerns or support needs are identified.
7.14 Any strategy meetings /discussions, child protection conferences and core
group meetings must include professionals from any substance misuse service involved with the family.
18
8 Multi-agency information sharing 8.1 Successful multi-agency working depends on effective information sharing. 8.2 It is essential for all services to accurately record the names, dates of birth,
involvement of other agencies and areas of concern for all children in families known to them. If parents, carers or pregnant women decline to provide basic information about themselves or their families this must be recorded and, if necessary, advice sought.
8.3 Any areas of identified concern or support need to be discussed with the
parents, carers or pregnant woman. The need for involvement of another service should be explained, while taking account of the parents’, carers’ or pregnant woman’s right to confidentiality.
8.4 Personal information held by professionals and agencies is subject to a legal
duty of confidence and should not normally be disclosed without the consent of the young person or parent/ carer. Unless it is assessed that a child is suffering, or is likely to suffer, from significant harm the consent of parents or carers should normally be obtained before making a referral to any other service.
8.5 If parents or carers do not share a professional’s concerns, the requirement to
pass information to other agencies must where appropriate be made clear to them and their views recorded. If there is any uncertainty about sharing information, advice must be sought from your line manager or your agency’s designated child protection lead officer/ adviser.
8.6 When information about a service user or patient is received from another
agency it must be treated with respect and with a high level of regard for confidentiality. It must be shared only on a need-to-know basis.
8.7 Confidentiality is an important principle of service delivery particularly in the
case of substance misuse. Bromley’s substance misuse services request consent to share information with relevant agencies on a need to know basis. Further information about confidentiality and information sharing in Bromley’s substance misuse services can be found in Appendix 3.
8.8 When children are in the care of a service user, it is essential to acknowledge
that there are certain limits to confidentiality - important information must be shared with other agencies where children may be at risk. As stated in the Children Act 1989, the child's welfare is paramount and this should be made clear to service users when they first access a service (HMSO 1989).
19
9 Resolving professional differences 9.1 Research and case enquiries have shown that difference of opinion between
agencies can lead to conflict resulting in less favourable outcomes for the child.
9.2 If there is a difference of opinion the professionals concerned should try to
resolve the issue through discussion within one working week. If the differences cannot be resolved then the Bromley Safeguarding Children Board (BSCB) Escalating Concerns: a Multi Agency Arbitration Process for resolving professional differences (2010) should be implemented. This involves the professionals involved taking the issue to the line manager/ commissioner or named/ designated safeguarding lead adviser within a prescribed timeframe leading ultimately to the Director of Children’s Service London Borough of Bromley.
9.3 Records of discussions and any decisions must be maintained by all agencies
involved and recorded on the forms provided.
20
Appendix 1: Assessment tool Assessment tool for assessing problem drug / alcohol use and impact on parenting This assessment framework has been adapted and expanded from guidelines produced by the Standing Conference on Drug Abuse (SCODA 1997). It is important to note that this is a multi‐agency risk assessment; it is not expected that one agency would be able to gather all of the information alone from the family. Close liaison with the range of services involved with the family is required to complete this risk assessment. Children in the family – provision of good basic care • How many children are in this family? • What are their names and ages (wherever possible include dates of birth)?
For each child: • Where and with whom they live? • Who else cares for them? And whether the carers misuse drugs/alcohol? • Is there adequate food, clothing and warmth for the child? Is height and weight normal
for the child’s age and stage of development? • Is the child’s health and development consistent with their age and stage of
development? Has the child received necessary immunisations? Is the child registered with a GP and a dentist? Do the parents seek health care for the child(ren) appropriately?
• Does he or she attend nursery or school regularly? If not, why not? Is he or she achieving appropriate academic attainment?
• Does the child present any behavioural problems, or emotional problems? • Does the parent manage the child’s distress or challenging behaviour appropriately? • Are children engaged in age‐appropriate activities? • Are there any indications that any of the children are taking on a parenting role within
the family (e.g. caring for other children, excessive household responsibilities etc.)? • Is the care for the child consistent and reliable? Are the child’s emotional needs being
adequately met? • Is there a risk of repeated separation for example because of periods of imprisonment
(eg. short custodial sentences or fine default) • How does the child relate to unfamiliar adults? • Are there non‐drug using adults in the family readily accessible to the child who can
provide appropriate care and support when necessary? Describing parental drug use (identify sources of information, including conflicting reports) • Is the drug use by the parent • experimental? • recreational? • chaotic? • dependent?* • Does the user move between these types of drug use at different times? • Does the parent misuse alcohol? • Does the parent use alcohol concurrently with other drugs?
21
• How reliable is current information about the parent’s drug use? • Is there a drug free parent, supportive partner or relative? • Is the quality of parenting or childcare different when a parent is using drugs and when
not using? • Does the parent have any mental health problems alongside drug use? If so, how are
mental health problems affected by the parent’s drug use? Are mental health problems directly related to drug use?
*Experimental use ‐ The use of drugs/alcohol as a means of ‘finding out’ about their effects. People may experiment with different drugs or with the same drug in different situations. Most people who have used illegal drugs will have only used experimentally and as a one‐off experience. Recreational use ‐ The regular use of drugs/alcohol (whether occasional or often) without the development of associated problems. The extent to which people can use drugs/alcohol recreationally will vary. Problematic use ‐ The use of drugs/alcohol which causes, or is linked with other problems present in the user’s life. Problems caused by drug/alcohol use can be far reaching and may include detrimental effects on health (mental and physical), relationships, family, employment, finances, accommodation, legal aspects and the community as a whole. Dependant use ‐ The use of drugs/alcohol because of a physical or psychological dependence. This is generally associated with problematic use but this is not always the case (e.g. a user who uses prescribed methadone may be dependant but does not necessarily experience problematic use). Chaotic use ‐ The use of drugs/alcohol which follows no pattern and causes multiple problems in the user’s life. Chaotic users are likely to use a range of different drugs (including alcohol). Accommodation and the home environment • Is the family’s living accommodation suitable for children? Is it adequately equipped and
furnished? Are there appropriate sleeping arrangements for each child, for example does each child have a bed or cot, with sufficient bedding?
• Are rent and bills paid? Does the family have any arrears or significant debts? • How long have the family lived in their current home / current area? Does the family
move frequently? If so, why? Are there problems with neighbours, landlords or dealers? • Do other drug users share or use the accommodation? If so, are relationships with them
harmonious, or is there conflict? • Is the family living in a drug using community? • If parents are using drugs, do children witness the taking of the drugs, or other
drugs/alcohol? • Could other aspects of drug use constitute a risk to children (e.g. conflict with or
between dealers, exposure to criminal activities related to drug use)? Procurement of drugs • Where are the children when their parents are procuring drugs or getting supervised
methadone? Are they left alone? Are they taken to unsuitable places where they might be at risk, such as street meeting places, flats, needle exchanges, adult clinics?
• How much do the parents spend on drugs (per day? per week?) How is the money obtained?
• Is this causing financial problems? • Do the parents sell drugs in the family home?
22
• Are the parents allowing their premises to be used by other drug users? Health risks • Where in the household do parents store drugs? • Do the children know where the drugs are kept? • What precautions do parents take to prevent their children getting hold of their drugs? Are these adequate? • What do parents know about the risks of children ingesting methadone and other
harmful drugs? • Are they in touch with local agencies that can advise on such issues such as needle
exchanges, substitute prescribing programmes, detoxification and rehabilitation facilities? If they are in touch with agencies, how regular is the contact?
If parent(s) inject: • Where do they keep injecting equipment? In the family home? Are works kept securely? • Do they share injecting equipment? • Do they use a needle exchange scheme? • How do they dispose of syringes? • What do they know about the health risks of injecting or using drugs? Family and social supports • Do the parents primarily associate with other problem drug users, non‐drug users or
both? • Are relatives aware of parent(s) drug use? Are they supportive of the parent(s)/ the
child? • Will parents accept help from relatives, friends or professional agencies? • Is social isolation a problem for the family? • How does the community perceive the family? Do neighbours know about the parents
drug use? Are neighbours supportive or hostile? Parents’ perception of the situation • Do the parents see their drug use as harmful to themselves or to their children? • Is there evidence that the parents place their own needs and procurement of drugs
before the care and welfare of their children? • Do the parents know what responsibilities and powers agencies have to support and
protect children at risk? • The ability of a parent to care adequately for their children may at any given time vary
depending on the amount of drug use, treatment undertaken, withdrawal from drugs and other circumstances.
Some parents who use drugs have poor parenting skills for reasons other than their problem drug use. If parents stop using drugs suddenly, withdrawal can increase stress and anxiety and decrease the ability of parents to care for children. Nor should it be assumed that if the problem drug use is controlled, the parents will immediately be capable of looking after children safely or satisfactorily. Any change in the parents’ drug/alcohol use will warrant re‐assessment of the impact of the change on other family members, and in particular dependent children.
23
Appendix 2: The impact of parental drug/alcohol use on children Pregnancy The following factors are linked to dependent / chaotic drug/alcohol use and may impact on the health and wellbeing of the foetus: • Poor nutrition and vitamin deficiencies • Anaemia • Infections
a) Bacterial (Abscesses, Septicaemia, Bacterial Endocarditis) b) Blood borne viruses (HIV, Hep A, B & C) c) Sexually transmitted diseases
• Chest infections – recurrent, acute and chronic • Non or poor attendance at Antenatal Clinic • Delayed confirmation of pregnancy • Possible intermittent withdrawal or overdose from drug/alcohol use
Drug/alcohol use may impact on the fetus in the following ways: • Intra‐uterine growth retardation • Preterm delivery • Increased rates of low birth weight and perinatal mortality • Death in utero The effects of individual drugs Cocaine • Intra‐uterine growth retardation, premature delivery, low birth weight, death in utero • Higher rates of early miscarriage • Higher rates of third trimester placental abruption • Higher rates of stillbirth and neonatal death (Chasnoff et al) • Higher rates of Sudden Infant Death Syndrome (Kandall et al) Opiates • No reports of increase in foetal abnormalities • Intra‐uterine growth retardation, premature delivery, low birth weight, death in utero • Abruption of the placenta with consequent stillbirth or neonatal death Barbiturates • Withdrawal effects may occur in infants • Studies have shown a small increase in fetal abnormalities possibly related to folate deficiencies Benzodiazepines • Some evidence of increase in oral cleft deficits • If the mother is taking these drugs at the time of delivery the baby may be hypnotic,
hypothermic and have respiratory difficulties • Also theoretical risk of increased neonatal jaundice due to enzyme reduction
24
Neonatal period Drug/alcohol use during pregnancy can impact on the child in the following ways • Abstinence syndrome (24‐72 hours after delivery but can be delayed if the mother has
been using Methadone and Benzodiazepines) • Foetal distress • Foetal Alcohol Syndrome
Childhood Children of drug/alcohol misusing parents are at greater risk of the following hazards: • Sustained or intermittent poverty • Physical; emotional; sexual abuse • Neglect, inadequate supervision and inappropriate parenting practices • Toxic substances and drug using paraphernalia (needles/syringes etc) in the home and
therefore possible exposure to blood borne virus infection or poisoning • Exposure to criminal or other inappropriate adult behaviour • Domestic abuse is observed • Inadequate accommodation and frequent changes in residence and carers • Social isolation The above may be in addition to, and interact with mental health problems and parental underattainment. Possible adverse consequences of parental drug/alcohol misuse • Emotional, cognitive and behavioural problems • School refusal / truanting • Increased prevalence of learning problems and poor educational achievement • Inadequate healthcare: • Higher rates of chronic illness • Respiratory infections • Hearing loss • Nutritional and growth problems • Accidents (Kurtz & Stanley 1995) • Incomplete immunisation • Poor socialisation • Early drug/alcohol use / misuse • Early offending behaviour Protective factors
1. The risk of a child developing behavioural or other problems will not be determined by one single risk factor (parental drug/alcohol use) but by the interaction between risk and protective factors over time (Dawe et al 2000)
2. Protective factors include strong family support; support from a non‐using adult such as teacher or other professional; parental controlled drug dosage and maintenance of family routines (Barnard and McKegany 2004).
25
Appendix 3: Confidentiality and information sharing in Bromley Drug and Alcohol Services
1. Background
The vision for drug and alcohol services in Bromley is based on the key principle that all service users receive the right treatment at the right time with the most appropriate services involved in their journey to achieve recovery and that commissioned services are delivered both efficiently and effectively through robust monitoring whilst delivering value for money. Overall within Bromley, the storage, access and sharing of information is underpinned by three values: • Confidentiality- Information is only shared amongst those who need to
know
• Integrity-Information is only changed by those authorised and qualified to do so
• Availability- Information is available to those who need it when they need it
Sharing information sensitively and appropriately is therefore essential to good management of services with due consideration to client confidentiality.
2. General consent and access to services
Service users will be asked to establish proof of residency and links with the borough in order to access treatment. General consent will be requested to share information with relevant agencies on a need to know basis. This means that the information to be shared is to prevent or minimise any harm to the service user or where the use of the information can be justified to prepare for future commissioning activities, to help protect the health of the public generally and to assist in health research for the benefit of everyone. If it is agreed for a service user to access any form of residential intervention, then emergency contact information will be required. Generally, information disclosed by a service user should not be shared without their consent; however there are exceptions to this.
26
3. Limits of confidentiality
Bromley services cannot operate a policy of absolute confidentiality. The exceptions to maintaining confidentiality are:
• Where there is a real and validated concern that a service user is
putting themselves or a third party (including employees and volunteers) at substantial risk.
• When the third party being put at substantial risk is a child e.g.
suspected child abuse, then this will always be viewed as sufficient reason to breach confidentiality in which case Child Protection Procedures should be applied
• When instructed by the Courts to do so (only under the Prevention of
Terrorism Act 1989, Drug Trafficking Offences Act 1994, Mental Health Act 1983 & 2007 or during investigations of the Serious Fraud Squad where services are legally obliged to disclose information).
• When the service user falls seriously ill on the premises and is in need
of urgent medical attention or to share emergency contact information. Details of name and address and where appropriate next of kin will be given to the ambulance crew or medical personnel or relevant professional.
4. Responsible and responsive management of information
Disclosure of information without the informed consent of the service user will only ever be made after careful, thorough consideration and assessment of risk and is only appropriate in the most exceptional of circumstances and expedited where required. Agencies are to be transparent and open with service users from the outset as to how their information will be used, including who information may be shared with and why. If there are agencies which the service user does not wish their information to be passed to the service user has the opportunity to express this at any point within their treatment. The exceptions to this have been referred to earlier in this document.
27
Appendix 4: DRAFT Pathways to Substance Misuse Services Procedure – Children’s Social Care and Adult Substance Misuse Services
Issue No: 1 Issue Date: March 2012
1. Introduction The aim of this procedure is to ensure there is joint working between Bromley Children’s Social Care and Bromley adult substance misuse services. This procedure sets out the process for staff in Bromley Children’s Social Care to make a referral to Adult substance misuse services and for arranging drug testing etc. It also sets out the process for staff in Bromley Adult Substance Misuse services to make a referral to children’s social care. Substance misuse itself is not sufficient reason for considering a child to be at risk of significant harm or to start child protection procedures. However, the misuse of drugs and alcohol by parents is an important factor to consider when assessing a parent’s skills to care for their child and the risks to the child. For further information about the impact of parental substance misuse on children and young people refer to the Bromley Safeguarding Children Board (BSCB) Multi-agency protocol Safeguarding Children and Young people living with parental substance misuse. 2. Procedures for Children’s Social Care Staff A referral to adult substance misuse services should always be made if there is concern about an individual’s substance misuse which indicates a risk to the service user or to others, particularly children. The Bromley adult substance misuse service can be contacted for advice about making a referral. Triggers that may indicate a referral are:
• Previous or current history of significant substance misuse • Current intravenous drug use • Excessive drug/ alcohol use • History of binge drug or alcohol use • Drug paraphernalia left lying around or clearly visible in the household • Past or recent history of overdose (depending on the nature and intention of the
overdose it may be appropriate to refer to mental health services e.g. for overdoses of prescription drugs).
• Factors such as domestic violence, sex working, and homelessness which may be connected with a substance misuse problem
• A child’s or other’s expression of concern regarding change in parent’s and/ or carer’s behaviour or attitude
Referrals should be made to: Bromley Drug and Alcohol Service (BDAS) 35 London Road, Bromley BR1 1DG Phone: 0208 289 1999
28
Bromley Drug and Alcohol Service is commissioned by NHS Bromley on behalf of the London Borough of Bromley. When referrals are made to the Adult Substance Misuse Service, an appointment will be made for a triage assessment to be carried out within 48 hours. Wherever possible a joint visit between Children’s Social Care and adult substance misuse services should be carried out to fully assess the needs of the family. In certain circumstances, drug screening can be done. This should be discussed with a manager. Drug screening on its own doesn’t provide a complete picture of someone’s drug or alcohol use and should be part of a whole assessment and exploration with the service user. 3. Procedures for Adult Substance Misuse Staff Where service users are parents or have childcare responsibilities, a risk assessment should consider if the children are at risk. Where service users have children, or regular access to children, Adult substance misuse services should make initial checks to identify if the child is known or open to Children’s Social Care. Initial checks can be made through the Multi Agency Support Hub (MASH) tel: 020 8461 7309 or 0208 461 7014. Where cases are known/ open to Children’s Social Care, the allocated social worker or team should be contacted. The Child’s Journey in Bromley (2011) will help to decide whether or not the child or young person has additional needs and whether a referral should be made to Children’s Social Care. Triggers that may alert for a referral to Children’s Social Care are:
• Concerns that parents/carers substance misuse is presenting a risk to the health / and or welfare of the child.
• Pregnant women who are substance misusing, and where there are concerns about the impact on an unborn child, or a woman’s ability to meet the child’s needs once born.
• Concerns about domestic violence which exist along side substance misuse issues
• Concerns about parental/carer mental health which exist alongside substance misuse
• Where a family member or partner is a person identified as presenting a risk to children.
The Multi Agency Support Hub (MASH) can be contacted to provide advice on whether a referral to Children’s Social Care is appropriate. Where a child does not meet the threshold criteria for Children’s Social Care but they may require additional support, consideration should be given to initiating a Common Assessment Framework (CAF). The CAF is a standard approach to conducting an assessment of the needs of a child and deciding how they should be met. Further information is available from the Bromley CAF Team (Tel: 020 8461 7174). Referrals for Children’s Social Care should be made to the Referral & Assessment Team: Referral & Assessment Team Phone: 020 8461 7373 / 7379 / 7404 / 7309
29
London Borough of Bromley E-mail: [email protected] Old Town Hall Tweedy Road Bromley BR1 3FE Fax: 01689 897 475 Emergency Duty Team (at weekends and outside normal working hours) Phone: 020 8464 4848 All referrals should be sent in writing using the referral form. The exception is in the case of urgent child protection, where the referral will be taken over the phone and followed up in writing by the next working day. Permission to make a referral should be sought except in cases where the child or young person is at immediate risk. When referrals are made to Children’s Social Care, the Referral & Assessment Team will decide whether it meets the threshold for children’s social care and consider whether an initial assessment and a core assessment are needed. Wherever possible a joint visit between children and adult substance misuse services should be carried out to fully assess the needs of the family. Throughout the assessment process and where it is decided to convene an Initial Child Protection Conference, those agencies who have worked with the parents in relation to their drug use must be asked to contribute to the assessment, be invited to participate in the Strategy discussion and attend all relevant meetings including child protection conferences and core group meetings. The adult substance misuse service will make engagement reports available five working days prior to core group meetings and child protection conferences. Care Programme meetings regarding drug or alcohol abusing parents must include consideration of any needs or risk factors for the children concerned. Children’s Social Care must be given the opportunity and should contribute to such discussions.
30
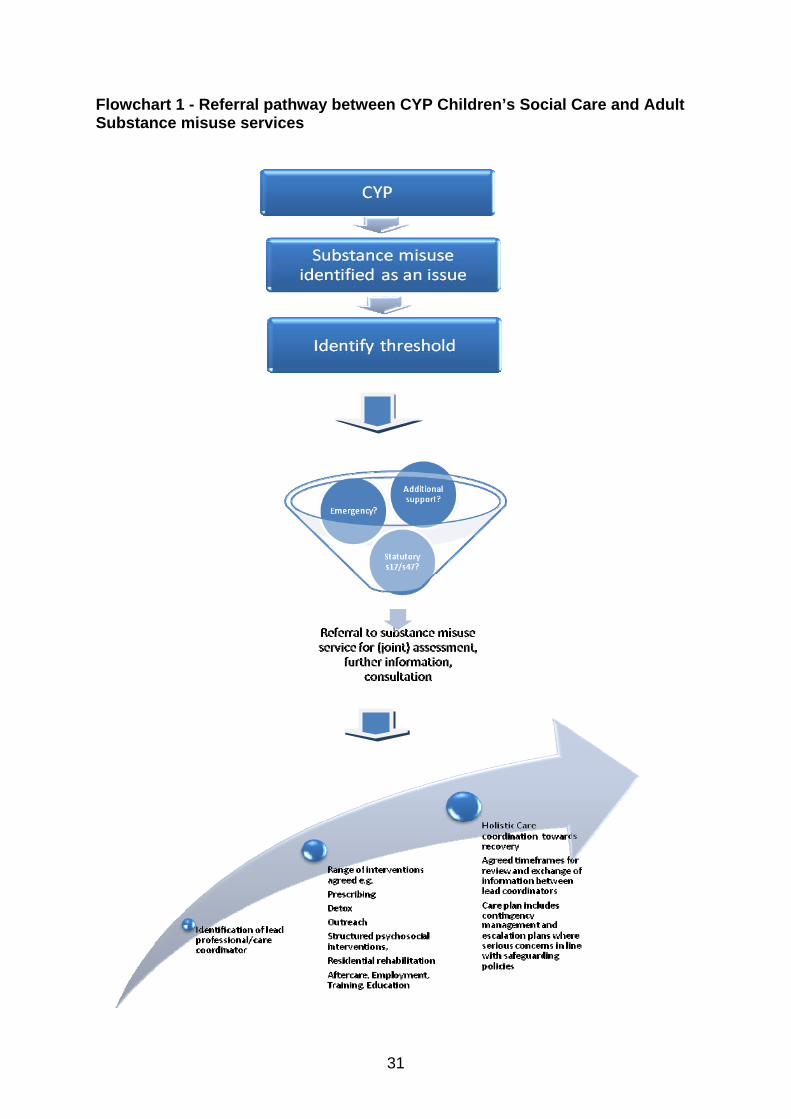
Flowchart 1 - Referral pathway between CYP Children’s Social Care and Adult Substance misuse services
31
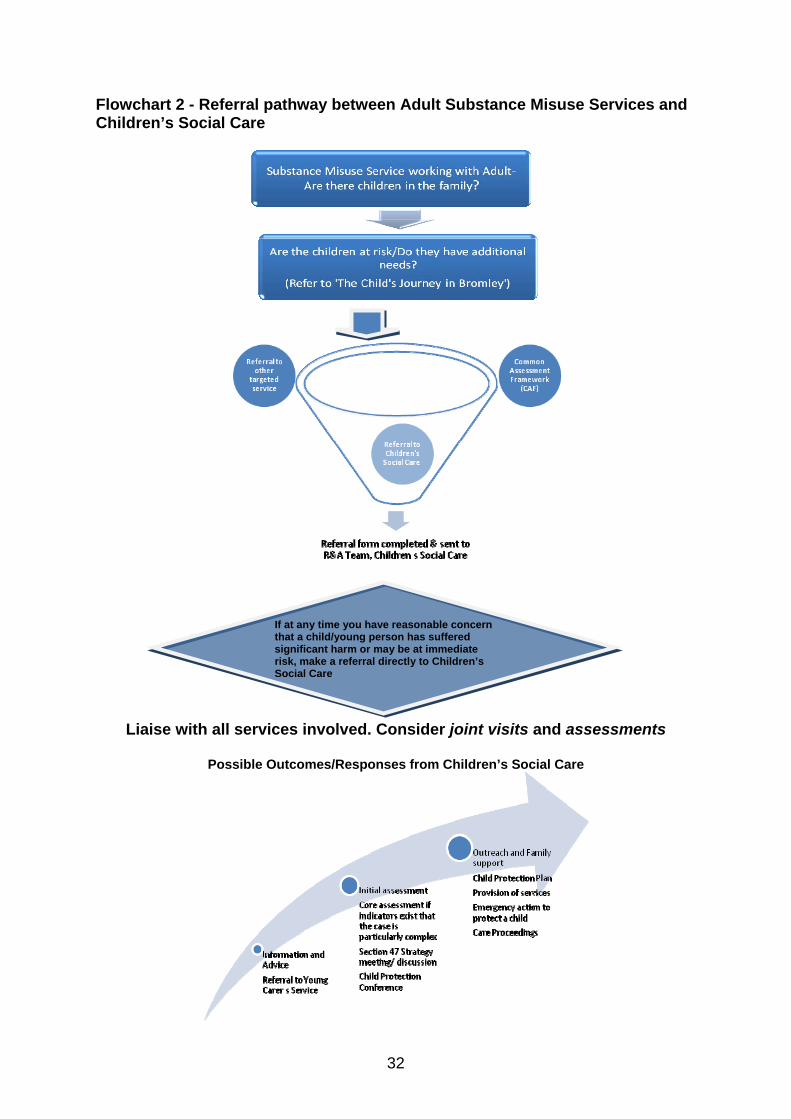
Flowchart 2 - Referral pathway between Adult Substance Misuse Services and Children’s Social Care
Liaise with all services involved. Consider joint visits and assessments
If at any time you have reasonable concern that a child/young person has suffered significant harm or may be at immediate risk, make a referral directly to Children’s Social Care
Possible Outcomes/Responses from Children’s Social Care
32
Appendix 5: Sources This Protocol is informed by: Analysing child deaths and serious injury through abuse and neglect: what can we learn? Brandon et al., 2008 Children Act 1989 Children Act 2004 Children’s Needs – Parental Capacity: The impact of parental mental illness, problem alcohol and drug use, and domestic violence on children’s development, Cleaver et al, 1999 Common Assessment Framework, CWDC, 2009 Drug Misuse in Pregnancy, Drugscope Escalating Concerns: a Multi Agency Arbitration Process for resolving professional differences, 2010, Bromley Safeguarding Children Board (BSCB) Framework for the Assessment of Children in Need and their Families, DH, 2000
Joint Guidance on Development on Local Protocols between Drug and Alcohol Treatment Services and Local Safeguarding and Family Services, National Treatment Agency, 2009 London Child Protection Procedures, LSCB, 2010 Mental Health Act 1983
National Service Framework for Children and Young People and Maternity Services, DH, 2004 What to do if you’re worried a child is being abused, DH, 2006
Working together to safeguard children: a guide to inter-agency working to safeguard and promote the welfare of children, HM Government, 2010 www.nta.nhs.uk/families , National Treatment Agency, 2011
33
Appendix 6: Who to contact in Bromley If you are concerned about a child you must always do something. If you’re not sure – seek advice If you think a child is in immediate danger contact the police by dialling 999. If you want to report a crime against a child, contact your local police station. Children’s Social Care To make a referral to the Referral and Assessment Team or discuss a potential referral contact: Referral & Assessment Team London Borough of Bromley Old Town Hall Tweedy Road Bromley BR1 3FE Telephone 0208 461 7373/7379/7404 Fax 01689 897475 E‐mail: [email protected] Emergency Duty Team (Out of Hours) 5pm – 9am weekdays, weekends and bank holidays 020 8464 4848 Common Assessment Framework (CAF) Team Common Assessment Framework Team Bromley Central Library, 3rd Floor High Street Bromley BR1 1EX Tel: 020 8461 7174 Adult Substance Misuse Bromley Community Drug and Alcohol Service 35 London Road, Bromley BR1 1DG Disabled access is available Service manager: Jonathan Williams 0208 289 1999 Bromley Community Drug and Alcohol Service is commissioned by NHS Bromley on behalf of LBB. The service offers a range treatment options including, substitute prescribing,
34
outreach, psychosocial interventions, one to one and group interventions. The service works holistically and in partnership to address the many issues related to substance misuse such as poor physical health, offending housing, education, training and employment. Assessment, as well as advice and information and consultation with professionals is also provided. KCA Shared Care Service 19A Widmore Rd Bromley Kent BR1 1RL Service manager: Swital Patel Contact 0208 460 9952 Shared Care provides ongoing support for people who are stable on substitute medication
such as methadone or subutex and is supported by Shared Care workers and GPs within
the borough. Service users are provided with a range of support packages which include
one to one sessions at least once per month and have access to counselling and groups
where appropriate. Service users will usually have been engaged within the community
drug and alcohol service initially before being referred to Shared Care.
Young Person’s Substance Misuse
BYPASS 19A Widmore Road Bromley Kent BR1 1RL Service manager: Tina Ganja Contact 0208 460 9952 BYPASS is funded by London Borough of Bromley Drug Action Team to work with young people, their parents and professionals. They offer advice, support and information to people who live, work or access services in Bromley. They work 1‐2‐1 or in small groups with young people who have issues/difficulties around alcohol or drugs, by offering advice, information and a range of treatment interventions on site or through satellites and assertive outreach across the borough. Professionals can refer and young people can refer themselves. Health Designated Nurse for Safeguarding Designated Doctor for Child Protection 01689 880 655 020 8466 9988
35
Hospital Bromley Healthcare Safeguarding team Princess Royal University Hospital Phoenix CRC Farnborough Mason’s Hill 01689 863 000 020 8466 9988 Mental Health Oxleas NHS Foundation Trust Liaison & Intake Team Telephone: 020 8466 2500 Stepping Stones 38 Masons Hill Bromley, BR2 9JG Child and Adolescent Mental Health Services (CAMHS) 2 Newman Road Bromley BR1 1RJ 020 8315 4430 Police Child Abuse Investigation Team 020 7230 3700 Education Education Welfare Office Safeguarding Lead for Education Civic Centre, 1st Floor Rm B40 Stockwell Close St. Blaise Building Bromley Stockwell Close BR1 3UH Bromley BR1 3UH 020 8313 4150 020 8461 7669
36