Embed Size (px)
Citation preview

Diagnostic and Interventional Imaging (2014) 95, 1135—1144
CONTINUING EDUCATION PROGRAM: FOCUS. . .
Patient ‘‘candidate’’ for thrombolysis:MRI is essential
M. Tisserand, O. Naggara, L. Legrand, C. Mellerio,M. Edjlali, S. Lion, C. Rodriguez-Régent,R. Souillard-Scemama, C.-F. Jbanca, D. Trystram,J.-F. Méder, C. Oppenheim ∗
Centre de psychiatrie et neurosciences, Inserm S894, université Paris Descartes, SorbonneParis Cité, neuroimagerie, Sainte-Anne hospital, 1, rue Cabanis, 75014 Paris, France
KEYWORDSArterial ischemicstroke;Thrombolysis;Diffusion-weightedimaging;Penumbra;
Abstract Because of its excellent sensitivity and specificity to diagnose arterial ischemicstroke (AIS) in the acute phase, MRI answers the main questions to guide treatment in‘‘candidates’’ for thrombolysis. It lasts less than ten minutes, can confirm the diagnosis ofAIS and distinguish it from hematomas and other ‘‘stroke mimics’’. It can identify the ischemicpenumbra (perfusion-diffusion mismatch), determine the site of occlusion and provide progno-stic information to adapt treatment in some cases in which the indications are poorly defined.In light of the most recent scientific findings, MRI can guide the treatment turning it into the
Perfusion-weightedimaging
investigation of choice in ‘‘candidates’’ for thrombolysis.© 2014 Éditions francaises de radiologie. Published by Elsevier Masson SAS. All rights reserved.
Clinical studies showing the effectiveness of intravenous (IV) rt-PA (recombinant tissueplasminogen activator) in arterial ischemic stroke (AIS) have selected patients based onbrain CT. In this case the purpose of imaging was to exclude an intracranial hemorrhagiclesion. The NINDS [1] study, the princeps IV thrombolysis study, was published in 1995 andmany improvements have been made in imaging since then. Currently, more sophisticatedimaging is often preferred to select candidates for thrombolysis.
The French National Health Authority guidelines published in May 2009 [2] on the man-agement of AIS in the acute phase state: ‘‘patients suspected of having acute AIS musthave priority access (24/24 h 7/7 d) to cerebral imaging [. . .]. MRI is the best investigationto show early signs of ischemia and visualize intracranial hemorrhage. This should be
∗ Corresponding author.E-mail address: [email protected] (C. Oppenheim).
http://dx.doi.org/10.1016/j.diii.2014.07.0032211-5684/© 2014 Éditions francaises de radiologie. Published by Elsevier Masson SAS. All rights reserved.

1
pae[s
aiaaittiatoOa
o(
•••
•••••
P
T
Id
Fimasa
as•
•
•
umi
tmbolFfbiotusad
h
136
erformed as the first line examination. If MRI is availables a first line investigation it should be accessible in themergency settings and short protocols should be preferred. . .]. If urgent access to MRI is not available, a cerebral CThould be performed’’.
These guidelines stress the importance of accessibilitynd speed of MRI, which are the prerequisite conditions,n order to avoid delaying intravenous thrombolytic ther-py. Rapid MRI sequences (PROPELLER, Echo planar), whichre of slightly poorer quality compared to the images usedn other situations, can reduce the length of the investiga-ion consistent with the adage ‘‘time is brain’’ [3]. MRI canherefore be performed without delaying patient care. Thenvestigation protocol lasts between five and ten minutesnd covers the entire brain without radiation. Patient agita-ion may deteriorate image quality although the informationbtained is often sufficient for treatment decision (Fig. 1).nly 10—15% of patients therefore cannot access MRI (severegitation, unstable hemodynamics or contra-indication) [4].
Some information provided by MRI are essential whereasthers await validation, apart from some specific situations> 4.5 h, age over 80 years old, unknown time of onset, etc.).
The purposes of MRI are listed below:
Primary objectives:to exclude hematoma;to confirm the positive diagnosis of AIS;to exclude differential diagnoses.
Secondary objectives:to characterize the infarction;to date the infarction;to assess the ‘‘core’’ of the infarction (necrosis);to establish the site of occlusion and collaterality;to assess the penumbra.
rimary objectives
o exclude hematoma
n order to exclude intraparenchymal hematoma, the mainifferential diagnosis from AIS [5—8], MRI performs as well
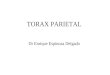
igure 1. Restless patient during MRI: the diffusion-weightedmage shows a hyperintensity in the superficial territory of the leftiddle cerebral artery (red arrows); MRA shows ipsilateral carotid
nd middle cerebral artery occlusion (blue arrow); the T2* imagehows no hemorrhagic lesion. This information is sufficient to decide
treatment intervention.
sE
C
MtaatFws‘n
E
BiTb
M. Tisserand et al.
s CT, including during the first few hours after the onset ofymptoms. The pattern of hematoma in the acute phase is:
diffusion-weighted imaging hyperintensity and reducedapparent diffusion coefficient. These can occasionallybe confused with those of an AIS although a hematomapresents a more heterogeneous pattern, with magneticsusceptibility effects and a brighter diffusion-weightedhyperintensity than an acute ischemic lesion. This het-erogeneous appearance is also seen on the T1-weightedimage (performed as the localizing sequence) with a T1-weighted hypointensity (whereas a hyperacute ischemiclesion is usually not seen on T1-weighted sequence) anda leaflike appearance in the periphery;pronounced FLAIR hyperintensitity (the FLAIR hyperinten-sity is unusual in ischemic lesions before 3 hours);peripheral T2*-weighted hypointensity consistent withthe presence of deoxyhemoglobin (Fig. 2).
Combined analysis of the different sequences, partic-larly diffusion-weighted and T2*-weighted images avoidissing the diagnosis of hematoma which is a contra-
ndication to thrombolytic therapy.Apart from symptomatic intraparenchymal hematoma,
he T2*-weighted image may show one or several chronicicrobleeds (Fig. 3). These are not seen on CT and maye single or multiple, lying deeply (hypertensive origin),r peripherally (in that case they are suggestive of amy-oid angiopathy [9]). In a meta-analysis of 570 patients,iehler et al. [10] found no additional risk of hemorrhagerom thrombolysis in patients with microbleeds (it shoulde noted that very few patients had multiple microbleedsn this meta-analysis [10]). The issue of the risk of hem-rrhagic transformation and/or cerebral hemorrhage afterhrombolysis in patients with numerous microbleeds is stillnanswered as this population was not represented in thetudy reported by Fiehler et al. A trend towards greater riskppeared in a more recent meta-analysis [11], although thisid not reach statistically significance.
T2*-weighted images can also assess the presence ofemorrhagic changes and is more sensitive than CT, clas-ifying hemorrhagic changes more severely according to theCASS classification [12] compared to CT [13] (Fig. 4).
onfirming the diagnosis of AIS
RI can confirm the positive diagnosis of acute AIS: hyperin-ensity on the diffusion-weighted images, distributed withinn arterial territory, with a homogeneous reduction of thepparent diffusion coefficient (Fig. 5). MRI is more sensitivehan CT particularly in the early phase of ischemia [14].alse negatives however can be seen with the diffusion-eighted images: posterior cerebral fossa lesions, small
trokes and recent lesions or transient symptoms [15]. An‘optimized’’ diffusion-weighted sequence can reduce theumber of false negatives [16] (Fig. 6).
xcluding the differential diagnoses
ased on the clinical presentation or even some imag-
ng appearances, a number of diseases may mimic AIS.hese differential diagnoses (‘‘stroke mimics’’) need toe excluded to avoid inappropriate thrombolysis. Other
Patient ‘‘candidate’’ for thrombolysis: MRI is essential 1137
Figure 2. MRI can distinguish AIS (acute ischemic stroke) from intraparenchymal hemorrhage. Case 1 is a left deep MCA (middle cerebralartery) AIS: homogenous hyperintensity on diffusion-weighted imaging with reduced ADC (apparent diffusion coefficient), hyperintensity onthe Fluid Attenuated Inversion Recovery (FLAIR) image without T2* hypointensity. Case 2 is a left deep hyperacute hematoma: heterogeneous
ointeance
S
T
Mtp
hyperintensity on diffusion-weighted imaging with a peripheral hypand hypointense on T2* (red arrows). This is confirmed by an unenh
diseases may, for example, cause a reduction in the appar-ent diffusion coefficient on MRI: a recent hematoma,other causes of cytotoxic edema (reversible posteriorencephalopathy, severe venous cerebral thrombosis, infec-tious encephalitis) [17,18] (Fig. 7), hypercellular lesions(lymphoma, medulloblastoma) [19,20] or hyperviscosity(pyogenic abscess) [21]. MRI can also correct the diag-
nosis in some ‘‘stroke mimics’’, which are more difficultto identify, using a combination of different sequences.These include for example, migraine aura or postictal edema[22,23].es4w
Figure 3. The T2* image is very sensitive to chronic microbleeds. Thrb: numerous deep bilateral microbleeds (> 10) are present, in a patient wlocated peripherally with superficial hemosiderosis: this appearance sug
nse collar and a reduced ADC, peripherally hyperintense on FLAIRd CT.
econdary objectives
o date the infarction
RI has been shown to be able to date an AIS of unknownime of onset (for example wake-up strokes) [24]. The tem-oral change in the diffusion-weighted image begins with an
arly diffusion-weighted hyperintensity after arterial occlu-ion. The ADC also decreases early, reaching a nadir around8 hours, returns to normal towards the end of the secondeek and then increases in the chronic phase [25]. The FLAIRee different patients: a: a single deep right microbleed is present.ith chronic hypertension. c: multiple bilateral microbleeds (> 100)
gests amyloid angiopathy.

1138 M. Tisserand et al.
Figure 4. Comparison of the T2* image with CT to assess hem-orrhagic transformation (at 24 h): a punctiform hypointensity ispresent on the T2* image in the left lenticulate nucleus (red arrow)whereas on unenhanced CT no hemorrhagic hyperdensity is seen.
Figure 5. Positive diagnosis of AIS: diffusion-weighted hyperin-tensity within an arterial territory (dotted red line) with reducedapparent diffusion coefficient (not shown) and no marked FluidAttenuated Inversion Recovery (FLAIR) hyperintensity with occlu-sion of the right middle cerebral artery on 3D TOF (Time-Of-Flight)at
isb•
Fvssi
Figure 7. MRI as a diagnostic tool in 3 patients suspected of hav-ing an AIS. The sequences used are: diffusion-weighted imagingwith ADC (apparent diffusion coefficient) map and Fluid Attenu-ated Inversion Recovery (FLAIR) from left to right. a: herpes virusencephalitis: left temporal diffusion-weighted hyperintensity pre-dominantly involving the cortex with focally cortico-subcorticalheterogeneously reduced ADC FLAIR hyperintensity with a swollenappearance of the left temporal lobe. On the right, meningealT1-weighted enhancement after gadolinium. b: glial tumor: leftparietal diffusion-weighted hyperintensity predominantly involvingthe cortex, with increased ADC, cortico-subcortical FLAIR hyperin-tensity with an unusual mass effect for an acute ischemic lesion.On the right the 3D TOF sequence does not show proximal arte-rial conclusion. c: cerebral venous thrombosis: left fronto-parietal
nd a ‘‘susceptibility vessel sign’’ on the T2* image representinghe intraluminal thrombus (red arrows).
mage is normal or subnormal in the initial hours and thenubsequently becomes positive (Fig. 8). Two situations cane distinguished based on the ‘‘diffusion/FLAIR’’ mismatch:
a diffusion-weighted hyperintensity with no FLAIR hyper-intensity, representing usually a subacute lesion (< 4.5 h)(Fig. 9);igure 6. Patient presenting with dizziness for 5 hours: the con-entional diffusion-weighted images show no clear hyperintensityuggestive of an ischemic lesion. An optimized diffusion-weightedequence shows multiple punctate cerebellar and brain stem hyper-ntensities confirming the suspected diagnosis.
diffusion-weighted hyperintensity predominantly involving the cor-tex with a heterogeneously increased ADC, FLAIR hyperintensity inthe underlying white matter. On the right the sagittal T1-weightedimages after gadolinium show a defect in the superior sagittal sinus(s
•
f
top). On T2* (bottom) susceptibility artefact in the superior sagittalinus and cortical veins consistent with thrombi.
a diffusion-weighted hyperintensity with a pronouncedFLAIR hyperintensity, representing an older ischemiclesion. In such case, the time from stroke onset is likelyto be > 4.5 hours, although AIS < 4.5 hours may show sub-tle signal changes on FLAIR. Its sensitivity and specificityto detect an AIS < 4.5 h are however not perfect (55%and 60% respectively on a 3T scanner [26]). The pres-ence of a ‘‘diffusion/FLAIR’’ mismatch is currently usedas an inclusion criterion into a clinical trial on intravenousthrombolysis for wake-up strokes, when by definition the
time of onset is unknown [27].The FLAIR sequence can therefore distinguish recentrom semi-recent or old ischemia [4] (Fig. 10) and assess the

Patient ‘‘candidate’’ for thrombolysis: MRI is essential 1139
Figure 8. Temporal change in ischemia on Fluid Attenuated Inversion Recovery (FLAIR) and diffusion-weighted images and apparentdiffusion coefficient (ADC) map; the pink curve shows the changes of ADC, the acute phase being characterized by an early diffusion-weighted hyperintensity after arterial occlusion. The ADC decreases early to a nadir around 48 hours returning to normal towards the endof the second week and is then increased in the chronic phase. The FLAbecomes positive.
cerebral parenchyma (lacunar stroke, leucoaraiosis, territo-rial ischemic strokes). These latter are occasionally betterseen on T2-weighted imaging for example an Echo planarview (b = 0 s/mm2) from the diffusion-weighted sequence.
To assess the ‘‘core’’ of the infarction
The ‘‘core’’ or ‘‘irreversible necrosis’’ is assessed as a pro-gnostic tool. The DEFUSE [28] and EPITHET [29] studiesdefined a ‘‘malignant profile’’ (defined by a diffusion-weighted lesion and/or perfusion volume over 100 mL).This profile is associated with poor functional prognosis at3 months and an increased risk of bleeding after reperfusion[30].
Figure 9. Fluid Attenuated Inversion Recovery (FLAIR)/diffusionmismatch: no FLAIR hyperintensity and diffusion-weighted hyperin-tensity in the right middle cerebral artery territory. This pattern issuggestive of an ischemic lesion before 4.5 h.
APmss(hcpmsuo
T
Tibceobsttti
cs‘i
IR image is normal or subnormal in the initial hours and thereafter
Another MRI approach to assess the ‘‘core’’ is the DWI-SPECTS score (diffusion-weighted imaging; Alberta Strokerogram Early CT score) (Fig. 11). This score can beore readily used in routine practice than volume mea-
urement as it provides a simple semi-quantitative visualcore alternative to volumetry [31]. Large ischemic strokelow DWI-ASPECTS score) represents an increased risk ofemorrhagic transformation after thrombolysis [32]. Thisonclusion, however, is disputed by Olivot et al. [33] in aopulation of patients receiving early intra-arterial treat-ent, as a high diffusion volume in this study was not always
ynonymous of poor outcome. This concept of a cut-off vol-me should therefore be adjusted by the time between thenset of symptoms and MRI.
o determine the site of occlusion
he 3D Time-of-Flight MR angiography (3D TOF) is a flowmage that visualizes the site of occlusion. However it shoulde borne in mind that failure to visualize an artery on 3D TOFan also represent severe slowing in an artery that is nev-rtheless patent. The occlusion site may have implicationsn the decision to treat for those cases that are reputed toe poorly responsive to intravenous therapy (basilar occlu-ion, T carotid occlusion combining occlusion of the end ofhe internal carotid artery and the proximal segments ofhe anterior and middle cerebral arteries for example) par-icularly in considering endovascular treatment [34]. Thesessues however remain to be solved.
MRA is not the only vascular sequence in the proto-
ol. A T2*-weighted sequence can be used to assess theite of occlusion through an artefact described as the‘susceptibility vessel sign’’ (SVS) [35—37] (Fig. 12). This signs extremely specific for occlusion of the internal carotid
1140 M. Tisserand et al.
Figure 10. Assessment of the brain parenchyma: Fluid Atten-uated Inversion Recovery (FLAIR) (a) and diffusion-weighted (b)images can distinguish a semi-recent ischemic lesion (FLAIR anddiffusion-weighted hyperintensity, red arrow) from an old ischemiclesion (FLAIR hyperintensity with no diffusion-weighted hyperin-ts
ar[[t
c
Figure 12. ‘‘Susceptibility Vessel Sign’’ or SVS: magnetic suscep-tr
(baTimm
T
The penumbra is the area of reversible ischemia [42]. It
FCav
ensity, blue arrow) in the same patient. FLAIR image (c) and (d)howing vascular leucopathy and old lacunar infarcts.
rtery or proximal segment (M1) of the MCA [35]. It iseported to be associated with cardio embolic thrombus38]. Its relationship with thrombus composition is debated39]. Extension of the thrombus can be scored semi quanti-
atively using the ‘‘clot burden score’’ [36].Vascular occlusion can also be indirectly assessed fromollaterality circulation from linear FLAIR hyperintensities
rln
igure 11. Volume assessment on diffusion-weighted images. a: DWI-AT score): in each region named by a letter or a letter combined with a
ffected region: in this case 7 regions are affected: M1, M2, M3, M5, M6,olume was 164 cm3.
ibility artefact on the T2* images in the proximal segment of theight middle cerebral artery due to a thrombus.
or FLAIR vascular hyperintensities, FVH) (Fig. 13) that cane seen in the subarachnoid spaces [40]. The FVH are seen inrterial occlusion and represent hemodynamic disturbances.heir prevalence and prognostic value however are debated
n the literature. According to Legrand et al., these abnor-alities represent a smaller volume of infarction and largerismatch volume [41].
o assess the penumbra
educes gradually with time from the arterial occlusioneaving in its place irreversible ischemia if the artery isot recanalized. This progressive decrease varies depending
SPECTS (diffusion-weighted imaging; Alberta Stroke Program Earlyfigure represents 1 point. One point is subtracted from 10 for each
L and I (DWI-ASPECTS = 3). b: volumetry: in this case the diffusion

Patient ‘‘candidate’’ for thrombolysis: MRI is essential 1141
Figure 13. Fluid Attenuated Inversion Recovery (FLAIR) vascularhyperintensities or FVH appearing as linear hyperintensities seen in
Figure 15. Cerebral blood flow (CBF) and Tmax maps illustratingthe homogeneous appearance of the Tmax within the white mat-ta
chpfnwber[c
tiobu[2fsap
ic
the subarachnoid spaces (red arrows) indicating slowing flow in themeningeal collateral vessels.
on the occlusion site, severity of the occlusion and pres-ence of collateral circulation. Penumbral tissue is thetarget for a possible revascularization intervention. Manymethods are available to assess the penumbra, the mostwidely used being the ‘‘perfusion-diffusion mismatch’’.Schematically, the diffusion-weighted sequence shows theirreversible ischemia or ‘‘core’’ (without considering thepotential reversibility of lesions on diffusion-weighted imag-ing [43]) and the perfusion-weighted sequence detects thehypoperfusion area. Lesions that are hypoperfused withoutdiffusion hyperintensity represent the penumbra (Fig. 14).The aim of this approach is to increase the thrombolysistime window, offering recanalization therapy beyond 4.5 hto patients with a penumbra in placebo-controlled random-
ized trials. Assessment of the penumbra volume can identifypatients who may benefit from treatment.Figure 14. Perfusion-diffusion mismatch: minimal punctiformdiffusion-weighted hyperintensity in the left superficial middlecerebral artery territory with larger abnormalities on the Tmaxmap. The 3D TOF image shows left proximal middle cerebral arteryocclusion.
C
MdtMitd
er and the gray matter (hypoperfusion in the left middle cerebralrtery territory with reduced CBF and increased Tmax).
Whilst this technique is attractive, there is, however, noonsensus on the best parameter to determine the severeypoperfusion area. The most widely used parameter atresent is the Tmax, which is the time to the peak of residualunction. This parameter presents the advantage of homoge-ous mapping (there is no difference in Tmax between thehite matter and gray matter as opposed to the cerebrallood flow and cerebral blood volume) (Fig. 15). This param-ter can be calculated even with short acquisitions andequires an arterial input function (AIF) for deconvolution44]. It correlates well with cerebral blood flow values cal-ulated using PET-CT (positron emission tomography) [45].
Moreover there is no consensus about the Tmax thresholdo use. Currently the threshold in the most recent stud-es is a Tmax > 6 s [46]. Discrepancies between studies existn the role of this mismatch in selecting candidates withoth positive results (mismatch useful to select patients tondergo revascularization) (DIAS [47], DEDAS [48], DEFUSE28], EPITHET [29], DEFUSE 2 [49]) and negative results (DIAS
[50], MR RESCUE [51]). New randomized trials are there-ore ongoing. The ECASS 4 study is a randomized phase 3tudy comparing IV thrombolysis to placebo between 4.5 hnd 9 h or in wake-up AIS. The main inclusion criterion is aerfusion-diffusion mismatch on imaging.
Other mismatch techniques are proposed to assess theschemic penumbra: diffusion/MR angiography and clini-al/diffusion [52].
onclusion
RI can be performed in the acute phase of an AIS withoutelaying patient management. It serves different purposes,o confirm the diagnosis of AIS and exclude a hematoma.RI provides better characterization of the infarction and
schemic penumbra and opens the possibility of extendinghe treatment time window (> 4h30) and adapting treatmentepending on individual patient findings.
TAKE-HOME MESSAGES
• MRI is the recommended investigation by the FrenchNational Health Authority (2009).
• It should be accessible and fast.

1142
• MRI meets the primary objectives:◦ excluding hematoma,
— MRI = CT to detect intraparenchymal hematoma;◦ confirming the positive diagnosis of ischemic
cerebrovascular accident,— diffuse hyperintensity in an arterial territory
with reduced apparent diffusion coefficient;◦ excluding differential diagnoses.
• MRI meets the secondary objectives (characterizingthe infarction):◦ dating the infarction with the FLAIR diffusion
mismatch,◦ assessing the ‘‘core’’ (necrosis) by DWI-ASPECTS
or volumetry (prognostic role),◦ assessing the site of occlusion/collaterality,◦ assessing the penumbra.
• MRI can guide treatment turning it into theinvestigation of choice in ‘‘candidates’’ for
C
Taa
Q
1
2
FtwFo
3
4
A
D
D
Tc
R
thrombolysis.
linical case
his 50-year-old right-handed female patient developedphasia of unknown time of onset. An MRI was performedt admission (Fig. 16).
uestions
) What is the diagnosis?A. Multiple hematomas.
B. Infarctions of different ages.C. Metastases.D. Abscess and pre-suppurative lesion.) Describe the appearances of the different lesions.
igure 16. MRI performed at admission (aphasia of unknownime of onset) from left to right and top to bottom. A diffusion-eighted sequence with ADC (apparent diffusion coefficient) map,luid Attenuated Inversion Recovery (FLAIR), T2* and MR 3D Time-f-Flight (TOF) angiography.
M. Tisserand et al.
) What does the left posterior insular T2* hypointensityrepresent?
) Should thrombolysis be performed in this patient?
nswers
A) Infarctions of different ages.B) The first left periventricular lesion displays a diffusion-
weighted hyperintensity with decreased ADC (apparentdiffusion coefficient) representing cytotoxic edemawithin an arterial territory. This is an acute ischemiclesion probably > 4.5 h because the FLAIR hyperintensityis already clearly visible. The second cortico-subcorticalright frontal lesion represents an older ischemia withmoderate diffusion-weighted hyperintensity with a highADC.
C) Distal thrombus appearing as a punctate T2* hypointen-sity.
) No: the time of onset is unknown and the most recentischemic lesion is already frankly hyperintense on FLAIRimages suggesting a lesion > 4.5 h. In addition there areno signs of proximal vascular occlusion.
isclosure of interest
he authors declare that they have no conflicts of interestoncerning this article.
eferences
[1] Tissue plasminogen activator for acute ischemic stroke. TheNational Institute of Neurological Disorders and Stroke rt-PAStroke Study Group. N Engl J Med 1995;333:1581—7.
[2] Recommandations de bonne pratique, accident vasculairecérébral : prise en charge précoce (alerte, phase pré-hospitalière, phase hospitalière initiale, indications de lathrombolyse). Haute Autorité de santé; 2009.
[3] Saver JL. Time is brain-quantified. Stroke 2006;37:263—6.[4] Hand PJ, Wardlaw JM, Rowat AM, Haisma JA, Lindley RI, Dennis
MS. Magnetic resonance brain imaging in patients with acutestroke: feasibility and patient related difficulties. J NeurolNeurosurg Psychiatry 2005;76:1525—7.
[5] Kidwell CS, Chalela JA, Saver JL, Starkman S, Hill MD, DemchukAM, et al. Comparison of MRI and CT for detection of acuteintracerebral hemorrhage. JAMA 2004;292:1823—30.
[6] Fiebach JB, Schellinger PD, Gass A, Kucinski T, Siebler M, Vill-ringer A, et al. Stroke magnetic resonance imaging is accuratein hyperacute intracerebral hemorrhage: a multicenter studyon the validity of stroke imaging. Stroke 2004;35:502—6.
[7] Oppenheim C, Touze E, Hernalsteen D, Peeters A, Lamy C,Mas JL, et al. Comparison of five MR sequences for thedetection of acute intracranial hemorrhage. Cerebrovasc Dis2005;20:388—94.
[8] Brazzelli M, Sandercock PA, Chappell FM, Celani MG, Righetti E,Arestis N, et al. Magnetic resonance imaging versus computedtomography for detection of acute vascular lesions in patientspresenting with stroke symptoms. Cochrane Database Syst Rev2009 [CD007424].
[9] Vernooij MW, van der Lugt A, Ikram MA, Wielopolski PA,Niessen WJ, Hofman A, et al. Prevalence and risk factors ofcerebral microbleeds: the Rotterdam Scan Study. Neurology2008;70:1208—14.

[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
Patient ‘‘candidate’’ for thrombolysis: MRI is essential
[10] Fiehler J, Albers GW, Boulanger JM, Derex L, Gass A,Hjort N, et al. Bleeding risk analysis in stroke imagingbefore thromboLysis (BRASIL): pooled analysis of T2*-weightedmagnetic resonance imaging data from 570 patients. Stroke2007;38:2738—44.
[11] Charidimou A, Kakar P, Fox Z, Werring DJ. Cerebral microbleedsand recurrent stroke risk: systematic review and meta-analysisof prospective ischemic stroke and transient ischemic attackcohorts. Stroke 2013;44:995—1001.
[12] Hacke W, Kaste M, Fieschi C, Toni D, Lesaffre E, von Kum-mer R, et al. Intravenous thrombolysis with recombinanttissue plasminogen activator for acute hemispheric stroke.The European Cooperative Acute Stroke Study (ECASS). JAMA1995;274:1017—25.
[13] Renou P, Sibon I, Tourdias T, Rouanet F, Rosso C, Galanaud D,et al. Reliability of the ECASS radiological classification of post-thrombolysis brain haemorrhage: a comparison of CT and threeMRI sequences. Cerebrovasc Dis 2010;29:597—604.
[14] Chalela JA, Kidwell CS, Nentwich LM, Luby M, Butman JA,Demchuk AM, et al. Magnetic resonance imaging and com-puted tomography in emergency assessment of patients withsuspected acute stroke: a prospective comparison. Lancet2007;369:293—8.
[15] Fustier A, Naggara O, Tisserand M, Touze E, Mellerio C, EdjlaliM, et al. Total mismatch in anterior circulation stroke patientsbefore thrombolysis. J Neuroradiol 2013;40:158—63.
[16] Bertrand A, Oppenheim C, Lamy C, Rodrigo S, Naggara O, MasJL, et al. Comparison of optimized and standard diffusion-weighted imaging at 1.5 T for the detection of acute lesions inpatients with transient ischemic attack. AJNR Am J Neuroradiol2008;29:363—5.
[17] Leach JL, Fortuna RB, Jones BV, Gaskill-Shipley MF. Imaging ofcerebral venous thrombosis: current techniques, spectrum offindings, and diagnostic pitfalls. Radiographics 2006;26 Suppl.1:S19—41 [discussion S42-13].
[18] Stevens CJ, Heran MK. The many faces of posterior reversibleencephalopathy syndrome. Br J Radiol 2012;85:1566—75.
[19] Toh CH, Castillo M, Wong AM, Wei KC, Wong HF, Ng SH, et al.Primary cerebral lymphoma and glioblastoma multiforme: dif-ferences in diffusion characteristics evaluated with diffusiontensor imaging. AJNR Am J Neuroradiol 2008;29:471—5.
[20] Yamashita Y, Kumabe T, Higano S, Watanabe M, TominagaT. Minimum apparent diffusion coefficient is significantlycorrelated with cellularity in medulloblastomas. Neurol Res2009;31:940—6.
[21] Rath TJ, Hughes M, Arabi M, Shah GV. Imaging of cerebri-tis, encephalitis, and brain abscess. Neuroimaging Clin N Am2012;22:585—607.
[22] Floery D, Vosko MR, Fellner FA, Fellner C, Ginthoer C, Gru-ber F, et al. Acute-onset migrainous aura mimicking acutestroke: MR perfusion imaging features. AJNR Am J Neuroradiol2012;33:1546—52.
[23] Danière F, Edjlali-Goujon M, Mellerio C, Turc G, Naggara O,Tselikas L, et al. MR screening of candidates for thrombolysis:how to identify stroke mimics? Journal of Neuroradiology. InPress.
[24] Petkova M, Rodrigo S, Lamy C, Oppenheim G, Touze E, MasJL, et al. MR imaging helps predict time from symptom onsetin patients with acute stroke: implications for patients withunknown onset time. Radiology 2010;257:782—92.
[25] Lansberg MG, Thijs VN, O’Brien MW, Ali JO, de Crespigny AJ,Tong DC, et al. Evolution of apparent diffusion coefficient,diffusion-weighted, and T2-weighted signal intensity of acutestroke. AJNR Am J Neuroradiol 2001;22:637—44.
[26] Emeriau S, Serre I, Toubas O, Pombourcq F, OppenheimC, Pierot L. Can diffusion-weighted imaging-fluid-attenuatedinversion recovery mismatch (positive diffusion-weightedimaging/negative fluid-attenuated inversion recovery) at
[
1143
3 Tesla identify patients with stroke at < 4.5 hours? Stroke2013;44:1647—51.
27] Thomalla G, Fiebach JB, Ostergaard L, Pedraza S, Thijs V,Nighoghossian N, et al. A multicenter, randomized, double-blind, placebo-controlled trial to test efficacy and safety ofmagnetic resonance imaging-based thrombolysis in wake-upstroke (WAKE-UP). Int J Stroke 2013.
28] Albers GW, Thijs VN, Wechsler L, Kemp S, Schlaug G, Skal-abrin E, et al. Magnetic resonance imaging profiles predictclinical response to early reperfusion: the diffusion and per-fusion imaging evaluation for understanding stroke evolution(DEFUSE) study. Ann Neurol 2006;60:508—17.
29] Davis SM, Donnan GA, Parsons MW, Levi C, Butcher KS, PeetersA, et al. Effects of alteplase beyond 3 h after stroke inthe Echoplanar Imaging Thrombolytic Evaluation Trial (EPI-THET): a placebo-controlled randomised trial. Lancet Neurol2008;7:299—309.
30] Mlynash M, Lansberg MG, De Silva DA, Lee J, Christensen S,Straka M, et al. Refining the definition of the malignant pro-file: insights from the DEFUSE-EPITHET pooled data set. Stroke2011;42:1270—5.
31] Barber PA, Hill MD, Eliasziw M, Demchuk AM, Pexman JH,Hudon ME, et al. Imaging of the brain in acute ischaemicstroke: comparison of computed tomography and magneticresonance diffusion-weighted imaging. J Neurol Neurosurg Psy-chiatry 2005;76:1528—33.
32] Singer OC, Kurre W, Humpich MC, Lorenz MW, Kastrup A,Liebeskind DS, et al. Risk assessment of symptomatic intracere-bral hemorrhage after thrombolysis using DWI-ASPECTS. Stroke2009;40:2743—8.
33] Olivot JM, Mosimann PJ, Labreuche J, Inoue M, Meseguer E,Desilles JP, et al. Impact of diffusion-weighted imaging lesionvolume on the success of endovascular reperfusion therapy.Stroke 2013;44:2205—11.
34] Saarinen JT, Sillanpaa N, Rusanen H, Hakomaki J, Huhtala H,Lahteela A, et al. The mid-M1 segment of the middle cerebralartery is a cutoff clot location for good outcome in intravenousthrombolysis. Eur J Neurol 2012;19:1121—7.
35] Rovira A, Orellana P, Alvarez-Sabin J, Arenillas JF, AymerichX, Grive E, et al. Hyperacute ischemic stroke: middle cere-bral artery susceptibility sign at echo-planar gradient-echo MRimaging. Radiology 2004;232:466—73.
36] Legrand L, Naggara O, Turc G, Mellerio C, Roca P, Calvet D, et al.Clot burden score on admission T2*-MRI predicts recanalizationin acute stroke. Stroke 2013;44:1878—84.
37] Naggara O, Raymond J, Domingo Ayllon M, Al-Shareef F, TouzeE, Chenoufi M, et al. T2* ‘‘susceptibility vessel sign’’ demon-strates clot location and length in acute ischemic stroke. PLoSONE 2013;8:e76727.
38] Cho KH, Kim JS, Kwon SU, Cho AH, Kang DW. Significance of sus-ceptibility vessel sign on T2*-weighted gradient echo imagingfor identification of stroke subtypes. Stroke 2005;36:2379—83.
39] Liebeskind DS, Sanossian N, Yong WH, Starkman S, Tsang MP,Moya AL, et al. CT and MRI early vessel signs reflect clot compo-sition in acute stroke. Stroke 2011;42:1237—43.
40] Lee KY, Latour LL, Luby M, Hsia AW, Merino JG, Warach S. Distalhyperintense vessels on FLAIR: an MRI marker for collateralcirculation in acute stroke? Neurology 2009;72:1134—9.
41] Legrand L, Tisserand M, Turc G, Naggara O, Edjlali M, MellerioC, et al. Do FLAIR vascular hyperintensities beyond the DWIlesion represent the ischemic penumbra? Stroke. In Press.
42] Astrup J, Siesjo BK, Symon L. Thresholds in cerebralischemia — The ischemic penumbra. Stroke 1981;12:723—5.
43] Labeyrie MA, Turc G, Hess A, Hervo P, Mas JL, Meder JF, et al.
Diffusion lesion reversal after thrombolysis: a MR correlate ofearly neurological improvement. Stroke 2012;43:2986—91.44] Calamante F, Christensen S, Desmond PM, Ostergaard L,Davis SM, Connelly A. The physiological significance of the

1
[
[
[
[
[
[
[
144
time-to-maximum (Tmax) parameter in perfusion MRI. Stroke2010;41:1169—74.
45] Zaro-Weber O, Moeller-Hartmann W, Heiss WD, Sobesky J.MRI perfusion maps in acute stroke validated with 15O-waterpositron emission tomography. Stroke 2010;41:443—9.
46] Olivot JM, Mlynash M, Thijs VN, Kemp S, Lansberg MG, Wech-sler L, et al. Optimal Tmax threshold for predicting penumbraltissue in acute stroke. Stroke 2009;40:469—75.
47] Hacke W, Albers G, Al-Rawi Y, Bogousslavsky J, DavalosA, Eliasziw M, et al. The Desmoteplase in Acute IschemicStroke Trial (DIAS): a phase II MRI-based 9-hour windowacute stroke thrombolysis trial with intravenous desmoteplase.Stroke 2005;36:66—73.
48] Furlan AJ, Eyding D, Albers GW, Al-Rawi Y, Lees KR, RowleyHA, et al. Dose escalation of desmoteplase for acute ischemicstroke (DEDAS): evidence of safety and efficacy 3 to 9 hoursafter stroke onset. Stroke 2006;37:1227—31.
[
M. Tisserand et al.
49] Lansberg MG, Straka M, Kemp S, Mlynash M, Wechsler LR, JovinTG, et al. MRI profile and response to endovascular reperfusionafter stroke (DEFUSE 2): a prospective cohort study. LancetNeurol 2012;11:860—7.
50] Hacke W, Furlan AJ, Al-Rawi Y, Davalos A, Fiebach JB,Gruber F, et al. Intravenous desmoteplase in patients withacute ischaemic stroke selected by MRI perfusion-diffusionweighted imaging or perfusion CT (DIAS-2): a prospective,randomised, double-blind, placebo-controlled study. LancetNeurol 2009;8:141—50.
51] Kidwell CS, Jahan R, Gornbein J, Alger JR, Nenov V, Ajani Z,et al. A trial of imaging selection and endovascular treatmentfor ischemic stroke. N Engl J Med 2013;368:914—23.
52] Mishra NK, Albers GW, Christensen S, Marks M, Hamilton S,Straka M, et al. Comparison of magnetic resonance imagingmismatch criteria to select patients for endovascular stroketherapy. Stroke 2014;45:1369—74.