Embed Size (px)
Citation preview

1083
results cannot be explained by changed reportingrequirements. Some deviation from the model was observedin the central and northern regions after April, 1986, but thiswas most striking in the south which was, despite localvariations in fallout, the most severely contaminated of theregions. Further investigations are essential to confirm orrefute an association between early infant mortality andradioactive fallout after Chernobyl. These may include amore complex regression model, that takes account of otherfactors such as birthweight (which tends to fall with
increased maternal radiation exposure) and congenitalmalformations. Other epidemiological indices in other
age-groups need close examination, particularly incidencerates of cancer and immunodeficiency. If an association isconfirmed, it could indicate that either the levels ofradioactive fallout after Chernobyl were higher than known(or admitted), or the level of radiation exposure commonlyconsidered to be "safe" requires reassessment.
We thank Dr E. Sternglass, whose works have motivated this study; Mr J.Gould for financial support; Dr M. Vicker and Dr K. Batjer for valuablediscussions; and Dr I. Schmitz-Feuerhake for encouragement.
Correspondence should be addressed to J. S.
REFERENCES
1. Stewart AM, Webb J, Hewitt D. A survey of childhood malignancies. Br Med J 1958;i: 1495-508.
2. Sternglass EJ. Secret fallout. New York: McGraw-Hill, 1981.3. Gould JM. US mortality and the Three Mile Island nuclear accident. New York:
Public Data Access, 1989.4. Bertell R, Jacobson N, Stogre M. Environmental influence on survival of low birth
weight infants in Wisconsin 1963-1975. Int Perspectives Public Health 1984; 1: 12.5. Sternglass EJ. Cancer: relation of prenatal radiation to the development of the disease
in childhood. Science 1963; 140: 1102.6. Kneale GW, Stewart AM. Childhood cancers in the UK and their relation to
background radiation. In: Jones RR, Southwood R, eds. Radiation and health.New York: John Wiley, 1987.
7. Thieme Ch, Lack N. Zur Gefahrdung von Schwangeren nach Tschernobyl. DFrauenarzt 1987; 6: 15.
8. Bericht zum Beschluß des Bayrischen Landtags, Drucksache 11/3653 betreffendeventuelle Erhöhung der Fehlgeburten, Fälle von Sauglingssterblichkeit,Mißbildung und geistigen Retardationen. Munich: Bavarian State Ministry of theInterior, 1987.
9. Auswirkungen des Reaktorunfalles in Tschernobyl auf die BundesrepublikDeutschland. Veröffentlichungen der Strahlenschutzkommission, Band 7. Bonn:Federal Ministry of Environment, Nature Protection, and Reactor Safety, 1987.
10. Winter M, Völkle H, Narrog J, Meyer P, Kirchoff K. Die Radioaktivitat in der BRDund in der Schweiz nach dem Reaktorunfall in Tschemobyl. Bonn: Fachverbandfur Strahlenschutz, 1986.
11. Schmidt M, Ziggel H. Frühe Säuglingssterblichkeit in der BRD vor und nachTschemobyl. Reiber der Universität Bremen (in press).
Therapeutics
CONTINUOUS INFUSION OF OCTREOTIDE INACROMEGALY
ROBERT A. JAMESMICHAEL C. WHITENIELS MOLLER
SUDIP CHATTERJEEKEITH HALL
PAT KENDALL-TAYLOR
Royal Victoria Infirmary, Newcastle upon Tyne
Summary 15 patients with acromegaly were treatedwith continuous subcutaneous infusion of
octreotide in increasing dose from 200 to 1600 µg per 24 h by200 µg increments each week. Patients were studied duringthe initial 7 h of infusion, weekly at each dose level, then after1 and 2 months at maximum dosage. 13 patients respondedwell, as judged by growth hormone (GH) suppression andreturn of insulin-like growth factor 1 to normal, although 1patient withdrew due to adverse effects; 2 patients showedno significant reduction in GH. In the 12 responders GHlevel fell within the first 3 h of infusion at a mean plasmaoctreotide level of 0·76 (SE 0·26) µg/l, corresponding to25 µg of infused drug. Optimum suppression of GHoccurred at a dosage of 600 µg per 24 h, a plasma drug levelof 3·5 (0·5) µg/l. A definite reduction in tumour size was seenon computerised tomographic scan in 2 patients. All
responders noted subjective improvement in acromegalicsymptoms. Adverse effects comprised gastrointestinaldisturbances, which were transient and mild in 14 patientsbut severe in 1; biliary sludging occurred in 1 patient. Nosignificant deterioration in carbohydrate tolerance was seenin the responders.
INTRODUCTION
THE treatment of choice in acromegaly is removal of theadenoma. However, complete removal is not alwayspossible and additional irradiation may be required. Despitethis treatment some patients have residual disease, whichoften responds poorly to dopamine agonists.2,3 Octreotide, asomatostatin analogue, is an alternative therapy.4Intermittent subcutaneous injection of octreotide inhibits
excessive growth hormone (GH) secretion .3-1--12 Most
patients improved clinically during the first few weeks oftreatment with a reduction in both GH and insulin-like
growth factor 1 (IGF-1). Increases in the dose of theintermittent injections, in some cases up to 1000 (ig per day,gave a better and longer lasting suppression of GH.1O,11 Theshort half-life of octreotide (113 min9) results in escape fromGH inhibition 6-8 h after a subcutaneous injection,4 whichmay account for the failure of IGF- to decrease to normal.Administration of octreotide by continuous subcutaneousinfusion would be expected to overcome this disadvantage.Tumour shrinkage during treatment with intermittent
injections of octreotide has been reported10-12 but hasgenerally been modest and occurred in less than half of allpatients with somatotropinomas.4 We have administeredoctreotide by continuous subcutaneous infusion to
investigate whether GH would be suppressed, whetherIGF-1 would return to normal, and whether tumourshrinkage would be improved.
PATIENTS AND METHODS
Patients.-15 patients with active acromegaly were recruited(table 1). 10 had undergone one or more unsuccessful operations ontheir pituitary glands. 7 had received non-curative radiotherapymore than 2 years before entry to the trial. 6 had received both
surgery and radiotherapy, yet still had active disease as assessed by24 h mean GH profile of 5 mU/1 or higher and/or failure of GH tofall to 2 mUll or less during a 75 g oral glucose load. 2 patients,previously treated with bromocriptine with little benefit, had thismedication withdrawn at least 2 months before study. 11 patientshad hypopituitarism (10 as a result of previous treatment, 1 becauseof tumour size) and were maintained on one or more hormonereplacement therapies. All patients gave informed consent to thestudy protocol, which had the approval of the local ethicalcommittee.
Initial clinical and biochemical studies.-Before the start of
therapy, blood pressure and ring size were recorded and the patientswere photographed. Biochemical evaluation included a 24 h GHprofile, with samples being withdrawn every 2 h from an indwellingcannula, and a midday IGF-1 measurement. Other relevanthormones were assayed. Dynamic tests included the glucose andGH response to a 75 g oral glucose load and the GH response to a200 (ig intravenous injection of thyrotropin releasing hormone.Drug administration.--0ctreotide was administered by
continuous subcutaneous injection with a variable dose, battery

1084
TABLE I-DETAILS OF PATIENTS
*Radiotherapy=45 cGy. TSA=trans-sphenoidal adenomectomy; T4=L-thyroxine.
driven, MS-26 syringe pump (Graseby, Watford, UK). Patientswere taught how to insert a 15 mm 27 G needle, which they resitedevery 1-3 days, into the abdominal wall. The cannula wasconnected to the pump via a 600 mm giving set (Travenol Labs,USA). The initial dose was 200 ug per 24 h for the first 40 h. Iftolerated the dose was increased to 400 ug per 24 h for 1 week.Thereafter the dose was increased by a further 200 g per 24 h atweekly visits until the maximum dose of 1600 ug per 24 h wasattained by the sixth week. Patients were subsequently maintainedat this dose for the remaining 8 weeks of the trial.
Assessment of clinical response.-To monitor the initial response totreatment patients were evaluated hourly for the first 7 h bymeasurements of GH and drug level; thereafter measurements weremade each week during the incremental dose phase. Patientsattended for 8 h during the day when 2 hourly samples were takenfor GH assay. Plasma drug levels were measured at 0800 and 1200and samples were taken for IGF-1 assays at 1200. Patients’
subjective feelings of improvement and any adverse reactions wererecorded. At the end of the 14 weeks of treatment patients attendedfor a detailed assessment similar to the initial evaluation, withadditional samples for plasma drug levels taken 2 hourly for 24 h.
Safety.-At baseline and each visit, additional samples wereobtained for full blood count, coagulation studies, measurement ofglycosylated haemoglobin, fasting lipids, and serum electrolytes,and liver function. Routine ward urinalysis was recorded. Biliaryultrasound was done at the beginning and end of the trial.
Radiological assessment.-Detailed and standardised pre and posttreatment scans were done of the pituitary fossa with an IGE 9800high-resolution computerised tomographic (CT) scanner. Wherepossible the pituitary was scanned in the direct coronal plane afteradministration of contrast medium; slices were 1-5 mm thick.
Biochemical assays-Hormones were measured in duplicate inspecific radioimmunoassays. Serum GH was measured againstWHO international reference preparation 66/217 as standard. Theintra-assay and interassay coefficients of variation were 34% and8-4%, respectively. IGF-1 was measured with a kit (Incstar Corp,Stillwater, Minnesota). The interassay coefficient of variation was9-2% at all concentrations measured. The intra-assay coefficient is13-08%, according to the manufacturer. Octreotide levels weremeasured in plasma without extraction in a radioimmunoassay kitsupplied by Sandoz (Basle, Switzerland); the intra-assay coefficientof variation was 64%. Blood samples were taken into lithium/heparin tubes, the plasma separated immediately at 4°C, andsamples were stored at - 30°C before batch analysis.
RESULTS
Serum GH and IGF-l Levels
12 patients had a good response as judged by a decrease inmean GH levels from 32 9 (SE 9-3) to 4-3 (0-9) mU/1 during
the 24 h measurement period (p<001 compared withpretreatment values, paired t test) (figs 1 and 2). In additionIGF-1 levels fell to normal (reference ranges, nmol/1:female, 12-48; male, 9-46) (fig 2). 1 initially responsivepatient had to be withdrawn after only 10 days of treatmentbecause of persistent nausea and vomiting. 2 patients (no 11and 12) failed to respond (fig 2).
In the responders mean GH level fell during the initial 3 hinfusion from 32-9 (9-3) to 51 (1-9 mU/1) (p<0-01), which
corresponded to a total infused dose of 25 ug and a meanplasma drug level of 0-76 (0-26) µg/1 (fig 3). In the 2non-responders GH levels were not significantly differentfrom baseline after 3 h (79-5 [8’23] vs 73 and 14-8 [0.94] vs 16mU/1 for patients 11 and 12, respectively). Mean GH leveldecreased progressively with incremental doses ofoctreotide (fig 4). The optimum reduction in mean GH, to2-3 (0-4) mU/1, was obtained with 600 g per 24 h, corres-ponding to a mean plasma octreotide level of 3-5 (0-5) µg/1.
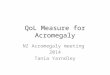
Fig 1-GH levels over 24 h before treatment and at end of 8 weeks’treatment with octreotide, 1600 µg per 24 h by continuoussubcutaneous infusion.
Fig 2--Changes in mean GH and IGF-1 achieved on subcutaneousoctreotide infusion (1600 jig per 24 h) for patients completing thetrial (n = 14).
Solid line=GH, dashed line=IGF-1, *=non-responder. Arrows= =increases or decreases.

1085
mvm ki iuul 0)
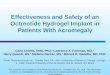
Fig 3-Reduction in GH ([]) with corresponding increase in plasmaoctreotide (0) over first 7 h of continuous octreotide infusion, 200µg per 24 h (n = 12).
Mean GH concentration did not fall further after the dosewas increased beyond this level. Similarly mean serumIGF-1 levels decreased progressively with dose, the mostdramatic reduction being in the range up to 400 µg per 24 h.
Fig 4-Mean GH of 2 hourly samples, IGF-1, and plasma octreotidelevels at each dose up to 1600 Ng per 24 h, and after 1 and 2 months’treatment at that dosage (n = 12).
TABLE II-GH AND GLUCOSE RESPONSES TO 75 g ORAL GLUCOSEBEFORE AND AFTER TREATMENT
Mean (SE, n= 12). Pretreatment versus post-treatment, *p < 0-05 and tp < 0-01.
The best reduction of IGF-1 was obtained with a dose of800 Ilg per 24 h. A normal IGF-1 concentration was
maintained, but no further reduction was achieved when thedosage was increased beyond this level (fig 4).The plasma octreotide levels rose linearly as the dose was
increased, reaching a plateau during the 8 weeks ofmaximum dose (mean 12-3 [1-2] fJ.g/1) (fig 4). There wasconsiderable variation between patients in the plasma druglevel required to produce the best GH suppression, rangingfrom 0-9 to 6-3 ug/1 (infused dose 200-800 µg per 24 h; mean3,5 [0°5] ug/1 during administration of 600 µg per 24 h). Theplasma drug levels achieved at maximum dosage were muchhigher than those required to produce and maintain atherapeutic reduction in mean GH and IGF-1 levels.
Dynamic Endocrine Tests
A standard 75 g oral glucose load during treatment withoctreotide led to suppression of mean GH concentration to2-5 (0-7) mU/1 at 90 min. In contrast to the paradoxical riseof mean GH to 30-2 (7-1 ) mU/1 during the pretreatment test,carbohydrate tolerance did not change significantly (tablen). The paradoxical and exaggerated GH response tointravenous thyrotropin releasing hormone was suppressedfrom a mean of 92-6 (21-8) to 13-1 (3-9) mU/1 at 20 min byoctreotide infusion.
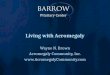
Fig 5--CT in 2 patients before and after 14 weeks of octreotideinfusion.
Left - before and right = after treatment; top = patient 14,bottom = patient 15.

1086
Clinical EffectsAll responders reported increased vitality, improved skin
texture and decreased skin thickness with less sweating, anda general softening of facial features during treatment withoctreotide. Ring size was reduced, indicating a decrease insoft-tissue mass, in 11 out of 12 patients. Patients were fullycompliant and treatment up to a maximum dose of 1600 gper 24 h was well tolerated. The continuous infusion pumpproved to be an acceptable mode of delivery. Abdominalcramps, flatulence, and loose motions were experienced byalmost all patients. However, these side-effects were usuallytransient and did not require withdrawal or reduction intherapy except in 1 patient. This patient (no 13) was knownto have hypopituitarism and, although treatment evoked anendocrine response, persistent nausea and vomitingnecessitated withdrawal. 1 unresponsive patient (no 11) hadtenderness and erythema at injection sites during the finalmonth of treatment. Subsequent tests have detectedantibodies to octreotide in this patient’s serum.13
Radiological FindingsIn 2 responders who had not previously undergone
pituitary surgery or received radiotherapy, definite tumourshrinkage was documented after the 14 weeks’ infusion (fig5). The remaining patients did not demonstrate any tumourshrinkage but many of these had previously undergonepituitary surgery, radiotherapy, or both, hence makinginterpretation of CT difficult.
SafetyFull blood counts, coagulation studies, measurements of
glycosylated haemoglobin, fasting lipids, and serum
electrolytes, and liver function tests showed no detrimentaleffects arising from continuous subcutaneous infusion ofhigh-dose octreotide. Asymptomatic biliary sludging,which was not present before therapy with octreotide, wasfound in 1 patient (no 5) after the 14 weeks of treatment.
DISCUSSION
We have confirmed the efficacy of octreotide in
acromegaly. By continuous infusion GH level was moreconsistently suppressed than had previously been attainedby intermittent injection .2,5 7,10 Adequate GH suppressionwith intermittent administration may require four injectionsdaily and an unacceptably high dose.10-12 Preliminarystudies suggested that more effective control of GH may beobtained by continuous subcutaneous infusion.14,15 GHlevels were controlled by this regimen through the night,which is important because GH most frequently peaks afterthe onset of sleep in both normal and acromegalic subjects.Whether total abolition of GH peaks is desirable or evendetrimental is not known. The prolonged suppression ofGH was also reflected in the maintenance of a normal IGF-1 1concentration in all the responders who completed the trial,which is achieved in only half the patients with intermittentinjection.8,16 Plasma drug levels were correlated with
response and there was a linear rise in octreotideconcentration with increase in dose. A plateau was reachedduring the period of maximum infusion of 1600 ug per 24 h.
Despite the exceptionally high drug levels achieved nounexpected or dose-related side-effects occurred. Mildgastrointestinal side-effects, experienced by most patients,were transient and did not worsen with increasing dose. 1
patient, who had hypopituitarism, withdrew because ofsevere gastrointestinal disturbance. For patients on
hydrocortisone replacement therapy our current practice isto increase their steroid dosage for 2-3 days during the initialinfusion. Biliary sludging in 1 patient after 14 weeks ofoctreotide, although asymptomatic, gives cause for concern.This side-effect, which has been noted previously duringintermittent injection with octreotide,4 is predicted by theoccurrence of gall stones in the few reported cases of patientswith somatostatinomasP Whether this problem will limitthe therapeutic usefulness of somatostatin analogues has yetto be established.
Octreotide had a negligible effect on carbohydratetolerance, even when used at high dose. Acromegalicpatients are predisposed to impaired glucose tolerance dueto the antagonistic effects of GH on the actions of insulin.Improvement in carbohydrate tolerance might therefore beexpected, but this is offset by the attenuation of the insulinresponse to carbohydrate loading evoked by octreotide.Hence the overall effect on glucose tolerance is unchanged.The most appropriate method to evaluate therapy for
acromegaly is controversial. Suppression of the mean 24 hGH below 5 ng/ml (10 mU/1), suppression of GH with oralglucose loading to less than 2 ng/ml (4 mU/1), reversal of theparadoxical GH response to thyrotropin releasing hormone,and a return of IGF-1 to normal have all been used.18 By anyof these criteria the 12 responders we saw must be regardedas having a good result, although the pattern of GH releaseduring frequent sampling indicates that restoration to
normal pulsatile secretion cannot be claimed. In view of therelation of IGF-1 to integrated GH secretion, and its longerhalf-life (3-6 h), IGF-1 is now thought to reflect accuratelyoverall GH activity.16 The return to normal of IGF-1 in allour responders therefore indicates a good response. IGF-1measurement is also a convenient means of assessingtreatment, obviating the need for repeated sampling andassay of GH.
2 patients failed to respond, despite increases in the doseup to 1600 pg per 24 h and attainment of plasma drug levelssimilar to those of responders. Occasional lack of
responsiveness to octreotide may be explained by a
deficiency of somatostatin receptors at the cell surface. 19 Thedemonstration of a significant decline in GH levels withinthe first 3 h of treatment is important since the occasionalnon-responder can be identified early. In such patientsoctreotide can be discontinued and alternative therapyplanned.
Reduction in tumour size was demonstrated in 2 of the 4
patients who had not previously undergone ablative
pituitary treatment, but no change was seen when suchtreatment had previously been given, even though tumourmass was still demonstrable on CT. Tumour shrinkage,though often slight, has been reported in up to half thepatients treated intermittently with octreotide.4,10-12 It wastherefore disappointing that, despite maintaining highplasma drug levels for 2 months with almost continuousinhibition of GH production, the effects on tumour sizewere not more striking. Tumour shrinkage may be due to areduction in intracellular stores of GH with decreased cellmass, as a result of lysosomal breakdown induced bylong-term suppression of GH secretion by somatostatinanalogues19 Reduced vascularisation has also been
suggested.14 On stopping therapy GH rapidly returns topretreatment levels, along with a reversal of any previouslyseen tumour shrinkage.19 However, a direct or indirectanti-proliferative role for somatostatin analogues cannot beruled out.2o
In view of the high cost of octreotide careful consideration

1087
should be given to patient selection. Octreotide is likely to bemost useful in patients who have active, symptomaticacromegaly, who are either unresponsive to or unsuitable forablative pituitary therapy, and who are not adequatelycontrolled by bromocriptine. Octreotide would also beindicated to suppress GH production in patients who areawaiting the beneficial effects of pituitary radiotherapy.Continuous subcutaneous infusion may be more cost
effective than intermittent injection. We envisage use of thecontinuous regimen in patients whose GH is not adequatelycontrolled by multiple daily injections or in whom
unacceptably large bolus doses are required to attain
suppressive levels of octreotide. Continuous infusion of600 pg per 24 h is the best dosage for most acromegalicpatients.We thank Mrs A. Potts for secretarial help; Dr P. G. Rose for biliary
ultrasonography; Sister Harris and staff of the Programmed InvestigationUnit, Royal Victoria Infirmary; Dr J. Dewar and Dr D. Cook, SupraregionalAssay Laboratory, Royal Victoria Infirmary, for assay of GH and IGF-1; DrAtholl Johnston, Chemical Pathology Unit, St Bartholomew’s Hospital,London, for assay of plasma octreotide levels; and Mrs E. R. Baister and DrM. J. Dunne, Sandoz Pharmaceuticals, for provision of octreotide.
Correspondence should be addressed to P. K.-T., Endocrine Unit, RoyalVictoria Infirmary, Newcastle upon Tyne NEl 4LP.
REFERENCES
1. Teasdale G. Surgical treatment of pituitary adenoma. In: Scanlon M, ed. Clinics inendocrinology and metabolism. Vol 12, neuroendocrinology. London: Saunders,1983: 789-823.
2 Lamberts SWJ, Zweens M, Verschoor L, Del Pozo E. A comparison among thegrowth hormone-lowering effects in acromegaly of the somatostatin analogue SMS201-995, bromocriptine and the combination of both drugs. J Clin EndocrinolMetab 1986; 63: 16.
3. Chiodini PG, Cozzi R, Dallabonzana D, et al. Medical treatment of acromegaly withSMS 201-995, a somatostatin analogue: a comparison with bromocriptine. J ClinEndocrinol Metab 1987; 64: 447-53.
4. Lamberts SWJ. The role of somatostatin in the regulation of anterior pituitaryhormones and the use of its analogues in the treatment of human pituitary tumours.Endocrinol Rev 1988; 9: 417-36.
5 Barnard LB, Grantham WG, Lamberlon P, O’Dorisio TM, Jackson IMD.Treatment of resistant acromegaly with a long-acting somatostatin analogue (SMS201-995). Ann Intern Med 1986; 105: 856-61.
6. Sandler LM, Burrin JM, Williams G, Joplin GF, Carr DH, Bloom SR. Effectivelong-term treatment of acromegaly with a long-acting somatostatin analogue (SMS201-995). Clin Endocrinol 1987; 26: 85-96.
7. Comi RJ, Gorden P. The response of serum growth hormone levels to the long actingsomatostatin analogue SMS 201-995 in acromegaly. J Clin Endocrinol Metab 1987;64: 37-42.
8. Lamberts SWJ, Uitterlinden P, del Pozo E. SMS 201-995 induces a continuousdecline in circulating growth hormone and somatomedin-C levels during therapyof acromegalic patients for over two years. J Clin Endocrinol Metab 1987; 65:703-10.
9. Del Pozo E, Nevfeld M, Schluter K, et al. Endocrine profile of a long actingsomatostatin derivative SMS 201-995: study in normal volunteers followingsubcutaneous administration. Acta Endocrinol 1986; 111: 433-39.
10 Tolis G, Yotis A, Del Pozo E. Therapeutic efficacy of a somatostatin analogue (SMS201-995) in active acromegaly. J Neurosurg 1986; 65: 37-40.
11 Ch’ng LJC, Sandler LM, Kraenzlin ME, Burrin JM, Joplin GF, Bloom SR. Longacting treatment of acromegaly with a long acting analogue of somatostatin. BrMed J 1985; 290: 284-85.
12. Barkan AL, Kelch RP, Hopwood NJ, Beitins IZ. Treatment of acromegaly with thelong-acting somatostatin analogue SMS 201-995. J Clin Endocrinol Metab 1988;66: 16-23.
13 Kendall-Taylor P, Chatterjee S, White MC, et al. Octreotide. Lancet 1989; ii: 859-60.14. Christensen SE, Weeke J, Orskov H, et al. Continuous subcutaneous pump infusion of
somatostatin analogue SMS 201-995 versus subcutaneous injection schedule inacromegalic patients. Clin Endocrinol 1987; 27: 297-306.
15. Timsit J, Chanson P, Larger E, et al. The effect of subcutaneous infusion versussubcutaneous injections of a somatostatin analogue (SMS 201-995) on the diumalGH profile in acromegaly. Acta Endocrinol 1987; 116: 108-12.
16. Lamberts SWJ, Uitterlinden P, Schuijff PC, Klijn JGM. Therapy of acromegaly withsandostatin: the predictive value of an acute test, the value of serum somatomedin Cmeasurements in dose adjustment and the definition of a biochemical "cure". ClinEndocrinol 1988;; 29: 411-20.
17. Krejs GJ, Orci L, Conlon JM, et al. Somatostatinoma syndrome: biochemical,morphological and clinical features. N Engl J Med 1979; 301: 285-92.
18 Quabbe H-J. Acromegaly: an overview. In: Lamberts SWJ, Tilders FJH, eds. Trendsin diagnosis and treatment of pituitary adenomas. Proceedings of the 3rd EuropeanWorkshop on Pituitary Adenomas, Amsterdam, Sept 1983.
19. Reubi JC, Heitz PV, Landolt AM. Visualization of somatostatin receptors andcorrelation with immunoreactive growth hormone and prolactin in humanpituitary adenomas: evidence for different tumour subclasses. J Clin EndocrinolMetab 1987; 65: 65-73.
20. Lamberts SWJ, Koper JW, Reubi JC. Potential role of somatostatin analogues in thetreatment of cancer. Eur J Clin Invest 1987; 17: 281-87.
Computers in Medicine
TELECOMMUNICATION DISCUSSIONGROUPS FOR HEALTH SERVICES AND
MEDICAL RESEARCH
DONALD F. PARSONS
Wadsworth Center for Laboratories and Research, New York StateDepartment of Health, Albany, New York, USA
Summary International university and researchinstitute telecommunication links provide
free or low-cost access to several computer networks
(commercial and non-commercial). Previously used byscience researchers, such networks are now used in clinicaland social medicine. University affiliation, a personalcomputer, and a modem and software are needed. A
host-computer, at a local computing centre, operates serversoftware that automatically distributes information to
subscribers. The server stores all messages in a monthlylogbook that can be edited to produce an electronic
magazine. The magazine can also be accessed by non-subscribers. The software gives convenient, fast, single-keyprocessing of messages and files and also allows on-lineconferences. Discussion groups on several medical
specialties and data bases for AIDS and othercommunicable diseases are already operating.
INTRODUCTION
EASY access to up-to-date information and to the adviceof specialists is a high priority for many clinicians andresearchers. A telecommunication system that allowedcontact between a consultant and general practitioner couldprove valuable and cost-effective. Specialist advice andsecond opinions need no longer be restricted geographically.International contacts can be made at small or no cost.
Confidentiality is ensured by computer security procedures.Data bases of disease statistics could be accessed directly,which would be a useful addition to computer searches of
published reports. Such telecommunication is alreadyprovided by the university networks, such as JANET in theUK and BITNET in the USA and Mexico, which has beenoperating since 1981. BITNET extends into Canada
(NETWORTH), Europe (EARN),’ Japan (AsiaNet), andSouth America. Whilst BITNET was initially supported byIBM, all the research networks are now self-supporting andmostly no-cost. The networks have few restrictions onmembership or topics or on type of host mainframe
computer. The main users were basic scientists who wereoften working on joint international projects and who neededto write collaborative papers. Now the networks are beingused for a wider range of disciplines, including medicine.The services provided by networks such as JANET and
BITNET are more powerful than those of bulletin boards,which lack many of the important automatic mail and filehandling abilities of the university networks. Function keysare assigned to complex mail handling procedures; afterinstallation, an office worker can receive, send, anddistribute messages with minimum computer expertise.
ADVANTAGES AND DISADVANTAGES OF NETWORKING
The main advantage of this type of networking is that Ican ask specific questions of an audience of several hundredsubscribers, and sometimes even larger audiences by