Embed Size (px)
Citation preview
Controversies in Anticoagulation and Thromboembolism Amir Jaffer, MD Scott Kaatz, DO
This pre-course is conducted by members of the Anticoagulation/Thromboembolism Interest Group. We hope that the interactive format will spur audience discussion. We are fortunate to have many leaders and world experts in this field involved to help us improve the care of our patients. Summary: • Orthopedists disagree on how long hip arthroplasty patients should receive
postoperative Venous Thromboembolism (VTE) prophylaxis. • Intensivists differ on which patients with pulmonary embolism should be treated with
thrombolysis. • Hospitalists are sometimes uncertain of the optimal duration of warfarin therapy for
patients with idiopathic DVT. • Hematologists debate on which patients need a hypercoagulable work-up in patients
with venous thromboembolic disease. • Cardiologists vacillate regarding which patients with atrial fibrillation should be
anticoagulated. Out of this chaos of multiple specialties managing different aspects of thromboembolic disease comes the critical role of general internists both inside the hospital and in their practices to orchestrate the care of their patients. Five brief cases representing these controversies will be presented during this precourse. Each case will be followed by a query of the audience by the facilitator for their opinions and feedback regarding their position. Each case will then be followed by two presentations with each speaker presenting their position. The speakers are all members of the Anticoagulation and Thromboembolism Interest Group and the facilitators are senior members who will facilitate the discussion. This pre-course is designed to be very lively and highly interactive. Learning Objectives: 1. Be aware of the strength of evidence supporting new guidelines for the duration of
venous thromboembolism in patients undergoing hip replacement surgery. 2. Understand the limitations of the evidence for thrombolysis in patients with sub-
massive pulmonary embolism. 3. Become familiar with the considerable evidence to guide the duration of warfarin
therapy for patients with idiopathic venous thromboembolism. 4. Learn about the pitfalls in conducting a hypercoagulable work-up 5. Appreciate the tools available to internists to risk stratify patients with atrial
fibrillation to help them make an informed decision regarding anticoagulation.
Duration Topic Presenters
5 minutes Introduction/rules of engagement Scott Kaatz 2 minutes How long should prophylaxis be
used in patients undergoing hip replacement surgery? Query the audience.
Scott Kaatz
10 minutes 10 days Peter Kaboli 10 minutes 28 days Rich White 10 minutes Audience questions Scott Kaatz 2 minutes Should thrombolysis be used in
patients with sub massive PE? Query the audience.
Amir Jaffer
10 minutes Yes Tracy Minichiello 10 minutes No Pungi Dorasamy 10 minutes Audience questions Amir Jaffer 2 minutes How long should a patient with
idiopathic DVT be treated with warfarin? Query the audience.
Scott Kaatz
10 minutes 6 months Andrew Dunn 10 minutes Indefinitely Rebecca Beyth 10 minutes Audience questions Scott Kaatz 30 minutes Break 2 minutes Should a patient with idiopathic DVT
undergo a hypercoagulable work up? Query the audience.
Amir Jaffer
10 minutes Yes Matt Eisen 10 minutes No Doug Einstadter 10 minutes Audience questions Amir Jaffer 2 minutes A 64-year-old female patient with
atrial fibrillation and hypertension, would you anticoagulate? Query the audience.
Scott Kaatz
10 minutes Yes Steven Cohn 10 minutes No Brian Gage 10 minutes Audience questions Scott Kaatz 5 minutes Closing remarks Amir Jaffer
References How long should prophylaxis be used in patients undergoing hip replacement surgery? 1. White RH, Romano PS, Zhou H, Rodrigo J, Bargar W. Incidence and time course
of thromboembolic outcomes following total hip or knee arthroplasty. Arch Intern Med 1998; 158:1525-31.
2. Heit JA, Elliott CG, Trowbridge AA, Morrey BF, Gent M, Hirsh J. Ardeparin
sodium for extended out-of-hospital prophylaxis against venous thromboembolism after total hip or knee replacement. A randomized, double-blind, placebo-controlled trial. Annals of Internal Medicine 2000; 132:853-61.
3. Comp PC, Spiro TE, Friedman RJ, et al. Prolonged enoxaparin therapy to prevent
venous thromboembolism after primary hip or knee replacement. Enoxaparin Clinical Trial Group. Patient Care Management 2001; 83-A:336-45.
4. Eikelboom JW, Quinlan DJ, Douketis JD. Extended-duration prophylaxis against
venous thromboembolism after total hip or knee replacement: a meta-analysis of the randomised trials. Lancet 2001; 358:9-15.
5. Warkentin TE, Roberts RS, Hirsh J, Kelton JG. An improved definition of
immune heparin-induced thrombocytopenia in postoperative orthopedic patients. Archives of Internal Medicine 2003; 163:2518-24.
6. Bergqvist D, Benoni G, Bjorgell O, et al. Low-molecular-weight heparin
(enoxaparin) as prophylaxis against venous thromboembolism after total hip replacement. New England Journal of Medicine 1996; 335:696-700.
7. Silbersack Y, Taute BM, Hein W, Podhaisky H. Prevention of deep-vein
thrombosis after total hip and knee replacement. Low-molecular-weight heparin in combination with intermittent pneumatic compression. Journal of Bone & Joint Surgery - British Volume 2004; 86:809-12.
8. Best AJ, Williams S, Crozier A, Bhatt R, Gregg PJ, Hui AC. Graded compression
stockings in elective orthopaedic surgery. An assessment of the in vivo performance of commercially available stockings in patients having hip and knee arthroplasty. Journal of Bone & Joint Surgery - British Volume 2000; 82:116-8.
9. Anonymous. Prevention of pulmonary embolism and deep vein thrombosis with
low dose aspirin: Pulmonary Embolism Prevention (PEP) trial. Lancet 2000; 355:1295-302.
1
White RH, Romano PS, Zhou H, Rodrigo J, Bargar W. Incidence and time course of thromboembolic outcomes following total hip or knee arthroplasty. Arch Intern Med. 1998 Jul 27;158(14):1525-31. White RH, Gettner S, Newman JM, Trauner KB, Romano PS. Predictors of rehospitalization for symptomatic venous thromboembolism after total hip arthroplasty. N Engl J Med. 2000 Dec 14;343(24):1758-64. White RH, Zhou H, Romano PS. Incidence of symptomatic venous thromboembolism after different elective or urgent surgical procedures. Thromb Haemost. 2003 Sep;90(3):446-55. White RH, Henderson MC. Risk factors for venous thromboembolism after total hip and knee replacement surgery. Curr Opin Pulm Med. 2002 Sep;8(5):365-71. Should thrombolysis be used in patients with sub massive PE? Wan S, Quinlan DJ, Agnelli G, Eikelboom JW. Thrombolysis compared with heparin for the initial treatment of pulmonary embolism, A meta-analysis of Randomized Controlled Trials. Arch Intern Med. 2002 Dec 9-23;162(22):2537-41 PMID: 12456225 Kanter DS, Mikkola KM, Patel SR, Parker JA, Goldhaber SZ. Thrombolytic therapy for pulmonary embolism. Frequency of intracranial hemorrhage and associated risk factors. CHEST 1997;111:1241-1245. Goldhaber SZ. Thrombolysis in submassive pulmonary embolism. J Thromb Haemost. 2004 Aug;2(8):1473-4 PMID: 15304059 Meneveau N, Ming LP, Seronde MF, Mersin N, Schiele F, Caulfield F, Bernard Y, Bassand JP. In-hospital and long-term outcome after sub-massive and massive pulmonary embolism submitted to thrombolytic therapy.Eur Heart J. 2003 Aug;24(15):1447-54 PMID: 12909074 Konstantinides S. Thrombolysis in submassive pulmonary embolism? Yes. J Thromb Haemost. 2003 Jun;1(6):1127-9. PMID: 12871305 Agnelli G, Becattini C, Kirschstein T. Thrombolysis vs heparin in the treatment of pulmonary embolism: a clinical outcome-based meta-analysis.Arch Intern Med. 2002 Dec 9-23;162(22):2537-41. PMID: 12456225
2

Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W; Management Strategies and Prognosis of Pulmonary Embolism-3 Trial Investigators. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N Engl J Med. 2002 Oct 10;347(15):1143-50. PMID: 12374874 Goldhaber SZ. Thrombolysis for pulmonary embolism.N Engl J Med. 2002 Oct 10;347(15):1131-2. PMID: 12374871 Kasper W, Konstantinides S, Geibel A, Olschewski M, Heinrich F, Grosser KD, Rauber K, Iversen S, Redecker M, Kienast J.Management strategies and determinants of outcome in acute major pulmonary embolism: results of a multicenter registry. J AM Coll Cardiol. 1997;3-:1165-1171 PMID: 9350909 Goldhaber SZ, Visani L, De Rosa M.Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER) Lancet. 1999 Apr 24;353(9162):1386-9. PMID: 10227218 Kreit JW. The impact of right ventricular dysfunction on the prognosis and therapy of normotensive patients with pulmonary embolism.Chest. 2004 Apr;125(4):1539-45. PMID: 15078772 The urokinase pulmonary embolism trial. A national cooperatieve study. Circulaiton 1973;47:108-111 Goldhaber SZ, Haire WD, Feldstein ML, Miller M, Toltzis R, Smith JL, Taveira da Silva AM, Come PC, Lee RT, Parker JA, et al. Alteplase versus heparin in acute pulmonary embolism: randomised trial assessing right-ventricular function and pulmonary perfusion. Lancet. 1993 Feb 27;341(8844):507-11. PMID: 8094768 Konstantinides S, Tiede N, Geibel A, Olschewski M, Just H, Kasper W. Comparison of alteplase versus heparin for resolution of major pulmonary embolism.Am J Cardiol. 1998 Oct 15;82(8):966-70. PMID: 9794353 Konstantinides S, Geibel A, Olschewski M, Heinrich F, Grosser K, Rauber K, Iversen S, Redecker M, Kienast J, Just H, Kasper W. Association between thrombolytic treatment and the prognosis of hemodynamically stable patients with major pulmonary embolism: results of a multicenter registry.Circulation. 1997 Aug 5;96(3):882-8. PMID: 9264496
3

Meneveau N, Ming LP, Seronde MF, Mersin N, Schiele F, Caulfield F, Bernard Y, Bassand JP. In-hospital and long-term outcome after sub-massive and massive pulmonary embolism submitted to thrombolytic therapy.Eur Heart J. 2003 Aug;24(15):1447-54. PMID: 12909074 Kucher N, Goldhaber SZ. Cardiac biomarkers for risk stratification of patients with acute pulmonary embolism. Circulation. 2003 Nov 4;108(18):2191-4. PMID: 14597581 La Vecchia L, Ottani F, Favero L, Spadaro GL, Rubboli A, Boanno C, Mezzena G, Fontanelli A, Jaffe AS. Increased cardiac troponin I on admission predicts in-hospital mortality in acute pulmonary embolism. Heart. 2004 Jun;90(6):633-7. PMID: 15145864 Blackmon JR, Sautter RD, Wagner HN et al. Urokinase Pulmonary Embolism Trial: Phase 1 results. JAMA 1970; 214: 2163-72 Dalla-Volta S, Palla A, Santolicandro A, et al. PAIMS 2: Alteplase combined with heparin versus heparin in the treatment of acute pulmonary embolism. Plasminogen activator Italian multicentre study 2. J Am Coll Cardiol 1992; 20:520 Levine M, Hirsh J, Weitz J, et al. A randomized trial of a single bolus dosage regimen of recombinant tissue plasminogen activator in patients with acute pulmonary embolism. Chest 1990; 98:1473 PIOPED Investigators. Tissue plasminogen activator for the treatment of acute pulmonary embolism. A collaborative study by the PIOPED Investigators. Chest 1990; 98: 1473-9 Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W. Heparin plus Alteplase compared with Heparin alone in patients with submassive pulmonary embolism. N Engl J Med 2002;347: 1143-1150 Goldhaber SZ, Kessler CM, Heit JA, et al. Recombinant tissue-type plasminogen activator versus a novel dosing regimen of urokinase in acute pulmonary embolism: a randomized controlled multicentre trial. J Am Coll Cardiol 1992; 20:24 Dalen JE The uncertain role of thrombolytic therapy in the treatment of pulmonary embolism [editorial]. Arch Intern Med. 2002;162:2521-2523 Goldhaber SZ, Haire WD, Feldstein ML et al. Alteplase versus heparin in acute pulmonary embolism: randomised trial assessing RV function and pulmonary perfusion. Lancet 1993;341: 507-11 Ribeiro A, Lindmarker P, et al. Echocardiography Doppler in pulmonary embolism: right ventricular dysfunction as a predictor of mortality rate. Am Heart J 1997; 134: 479-87
4

Grifoni S, Olivotto I, Cecchini P, et al. Short-term clinical outcome of patients with aacute pulmonary embolism, normal blood pressure, and echocardiographic right ventricular dysfunction. Circulation 2000; 101: 2817 Vieillard-Baron A, Page B, Augarde R et al. Acute cor pulmonale in massive pulmonary embolism: incidence echocardiographic pattern, clinical implications and recovery rate. Intensive Care Med 2001; 27: 1481-6 Hamel E , Pacouret G, Vincentelli D, et al. Thrombolysis or heparin therapy in massive pulmonary embolism with right ventricular dilation: results from a 128-patient monocenter registry. Chest 2001; 120: 120-5 Turpie AGG, Levine MN, Hirsh J, et al. Tissue plasminogen-activator versus heparin in deep venous thrombosis. Chest 1990; 97:172S Tapson VF, Witty LA. Massive pulmonary embolism: Diagnostic and therapeutic strategies. Clin Chest Med 1995; 16: 329-340 Konstantinides S, Geibel A, Olschewski M, et al. Association between thrombolytic treatment and prognosis of hemodynamically stable patients with major pulmonary embolism: results of a multicentre registry. Circulation 1997; 96:882-8 Goldhaber SZ, Visani L, De Rosa M. Acute Pulmonary Embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER) Lancet 1999; 353:1386-1389 Should a patient with idiopathic DVT undergo a hypercoagulable work up? Auerbach AD. Cost-effectiveness of testing for hypercoagulability and effects on treatment strategies in patients with deep vein thrombosis. Am J Med 2004; 116(12): 816-28 [PMID: 15178497] Baglin T, Luddington R, Brown K, Baglin C. Incidence of recurrent venous thromboembolism in relation to clinical and thrombophilic risk factors: prospective cohort study. Lancet. 2003 Aug 16;362(9383):523-6. [PMID: 12932383] Bauer KA, Rosendaal FR, Heit JA. Hypercoagulability: too many tests, too much conflicting data. Hematology (Am Soc Hematol Educ Program). 2002;:353-68. [PMID: 12446432] Bauer KA. The Thrombophilias: Well-Defined Risk Factors with Uncertain Therapeutic Implications. Ann Intern Med 2001;135:367-373 [PMID: 11529700] Crowther MA. Congenital Thrombophilic States Associated with Venous Thrombosis: A Qualitative Overview and Proposed Classification System. Ann Intern Med 2003;138:128-134 [PMID: 12529095]
5
Deitcher SR. Hypercoagulable state testing and malignancy screening following venous thromboembolic events. Vasc Med 2003; 8(1): 33-46 [PMID: 12866610] Feero WG. Genetic thrombophilia. Prim Care 2004; 31(3): 685-709, xi [PMID: 15331254] Greaves M, Baglin T. Laboratory testing for heritable thrombophilia: impact on clinical management of thrombotic disease annotation. Br J Haematol. 2000 Jun;109(4):699-703. [PMID: 10929018] Haemostasis and Thrombosis Task Force, British Committee for Standards in Haematology. Investigation and management of heritable thrombophilia. Br J Haematol. 2001 Sep;114(3):512-28. [PMID: 11552975] Lindmarker P, Schulman S, Sten-Linder M, Wiman B, Egberg N, Johnsson H. The risk of recurrent venous thromboembolism in carriers and non-carriers of the G1691A allele in the coagulation factor V gene and the G20210A allele in the prothrombin gene. DURAC Trial Study Group. Duration of Anticoagulation. Thromb Haemost. 1999 May;81(5):684-9. [PMID: 10365737] Murin S, Marelich GP, Arroliga AC, Matthay RA. Hereditary thrombophilia and venous thromboembolism. Am J Respir Crit Care Med. 1998 Nov;158(5 Pt 1):1369-73. [PMID: 9817680] Perry SL. Clinical and laboratory evaluation of thrombophilia. Clin Chest Med 2003; 24(1): 153-70 [PMID: 12685062] Ridker PM, Goldhaber SZ, Danielson E, Rosenberg Y, Eby CS, Deitcher SR, Cushman M, Moll S, Kessler CM, Elliott CG, Paulson R, Wong T, Bauer KA, Schwartz BA, Miletich JP, Bounameaux H, Glynn RJ; PREVENT Investigators. Long-term, low-intensity warfarin therapy for the prevention of recurrent venous thromboembolism. N Engl J Med. 2003 Apr 10;348(15):1425-34. Epub 2003 Feb 24. [PMID: 12601075] A 64-year-old female patient with atrial fibrillation and hypertension, would you anticoagulate? Gage BF, van Walraven C, Pearce L, et al. Selecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin. Circulation. 2004;110(16):2287-92. Snow V, Weiss KB, LeFevre M, et al. Management of newly detected atrial fibrillation: a clinical practice guideline from the American Academy of Family Physicians and the American College of Physicians. Ann Intern Med. 2003;139(12):1009-17.
6
Hylek EM, Go AS, Chang Y, et al. Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation. N Engl J Med. 2003;349(11):1019-26. Fuster V, Ryden LE, Asinger RW, et al. ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: executive summary. A Report of the American College of Cardiology/ American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines and Policy Conferences (Committee to Develop Guidelines for the Management of Patients With Atrial Fibrillation): developed in Collaboration With the North American Society of Pacing and Electrophysiology. J Am Coll Cardiol. 2001;38(4):1231-66. Levine MN, Raskob G, Landefeld S, Kearon C. Hemorrhagic complications of anticoagulant treatment. Chest. 2001;119(1 Suppl):108S-121S. Hart RG, Halperin JL. Atrial fibrillation and thromboembolism: a decade of progress in stroke prevention. Ann Intern Med. 1999;131(9):688-95. Hart RG, Benavente O, McBride R, Pearce LA. Antithrombotic therapy to prevent stroke in patients with atrial fibrillation: a meta-analysis. Ann Intern Med. 1999;131(7):492-501. Ezekowitz MD, Levine JA. Preventing stroke in patients with atrial fibrillation. Jama. 1999;281(19):1830-5. Monette J, Gurwitz JH, Rochon PA, Avorn J. Physician attitudes concerning warfarin for stroke prevention in atrial fibrillation: results of a survey of long-term care practitioners. J Am Geriatr Soc. 1997;45(9):1060-5. Man-Son-Hing M, Laupacis A, O'Connor A, et al. Warfarin for atrial fibrillation. The patient's perspective. Arch Intern Med. 1996;156(16):1841-8. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford M. Validation of Clinical Classification Schemes for Predicting Stroke: Results from the National Registry of Atrial Fibrillation. JAMA. 2001;285:2864-2870. Gage BF, van Walraven C, Pearce L, et al. Selecting patients with atrial fibrillation for anticoagulation: stroke risk stratification in patients taking aspirin. Circulation. Oct 19 2004;110:2287-2292. Go AS, Hylek EM, Chang Y, ...Singer D. Anticoagulation therapy for stroke prevention in atrial fibrillation: how well do randomized trials translate into clinical practice? JAMA. Nov 26 2003;290:2685-2692. Caro JJ, Flegel KM, Orejuela ME, Kelley HE, Speckman JL, Migliaccio-Walle K. Anticoagulant prophylaxis against stroke in atrial fibrillation: effectiveness in actual practice. Cmaj. 1999;161:493-497. Birman-Deych E, Nilasena DS, Radford MJ, Gage BF. Real-World
7

Effectiveness of Warfarin Therapy for Stroke Prevention in Medicare Beneficiaries of All Races. Poster session 3; poster #23.
8
1
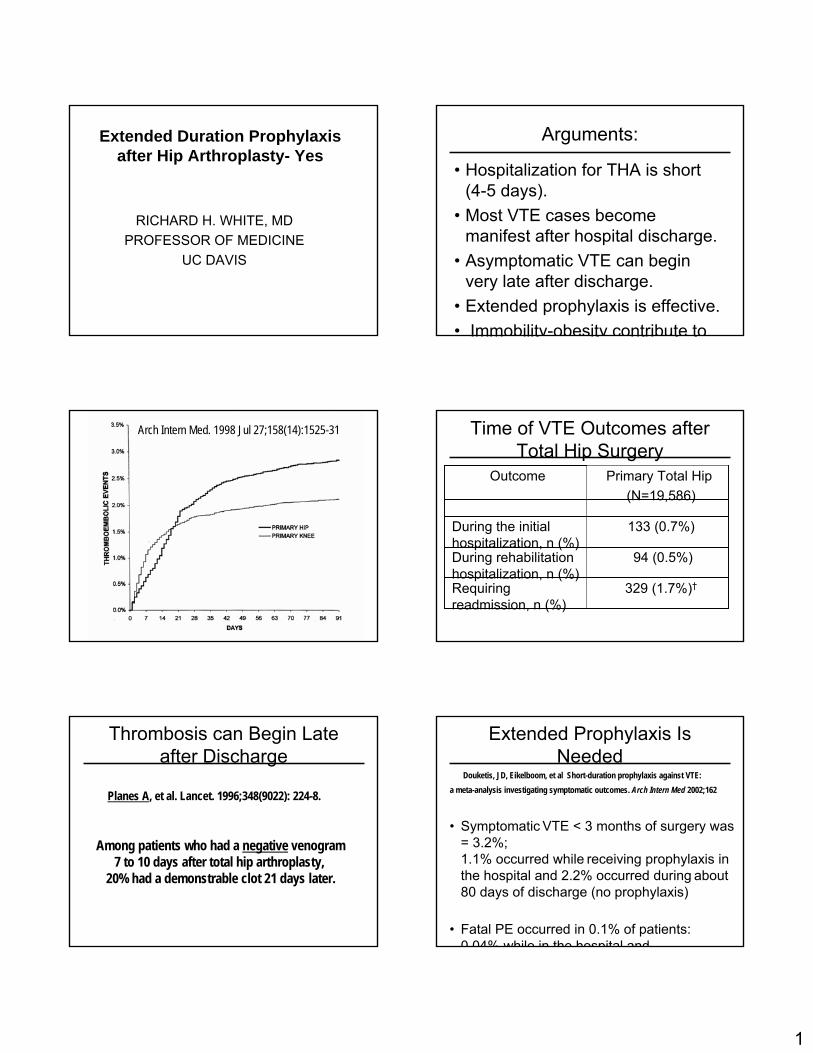
Extended Duration Prophylaxis after Hip Arthroplasty- Yes
RICHARD H. WHITE, MDPROFESSOR OF MEDICINE
UC DAVIS
Arguments:
• Hospitalization for THA is short (4-5 days).
• Most VTE cases become manifest after hospital discharge.
• Asymptomatic VTE can begin very late after discharge.
• Extended prophylaxis is effective.• Immobility-obesity contribute to
Arch Intern Med. 1998 Jul 27;158(14):1525-31 Time of VTE Outcomes after Total Hip Surgery
Primary Total Hip(N=19,586)
Outcome
133 (0.7%)During the initial hospitalization, n (%)
94 (0.5%)During rehabilitation hospitalization, n (%)
329 (1.7%)†Requiring readmission, n (%)
Thrombosis can Begin Late after Discharge
Among patients who had a negative venogram 7 to 10 days after total hip arthroplasty,
20% had a demonstrable clot 21 days later.
Planes A, et al. Lancet. 1996;348(9022): 224-8.
Extended Prophylaxis Is Needed
• Symptomatic VTE < 3 months of surgery was = 3.2%; 1.1% occurred while receiving prophylaxis in the hospital and 2.2% occurred during about 80 days of discharge (no prophylaxis)
• Fatal PE occurred in 0.1% of patients:0 04% while in the hospital and
Douketis, JD, Eikelboom, et al Short-duration prophylaxis against VTE: a meta-analysis investigating symptomatic outcomes. Arch Intern Med 2002;162
2
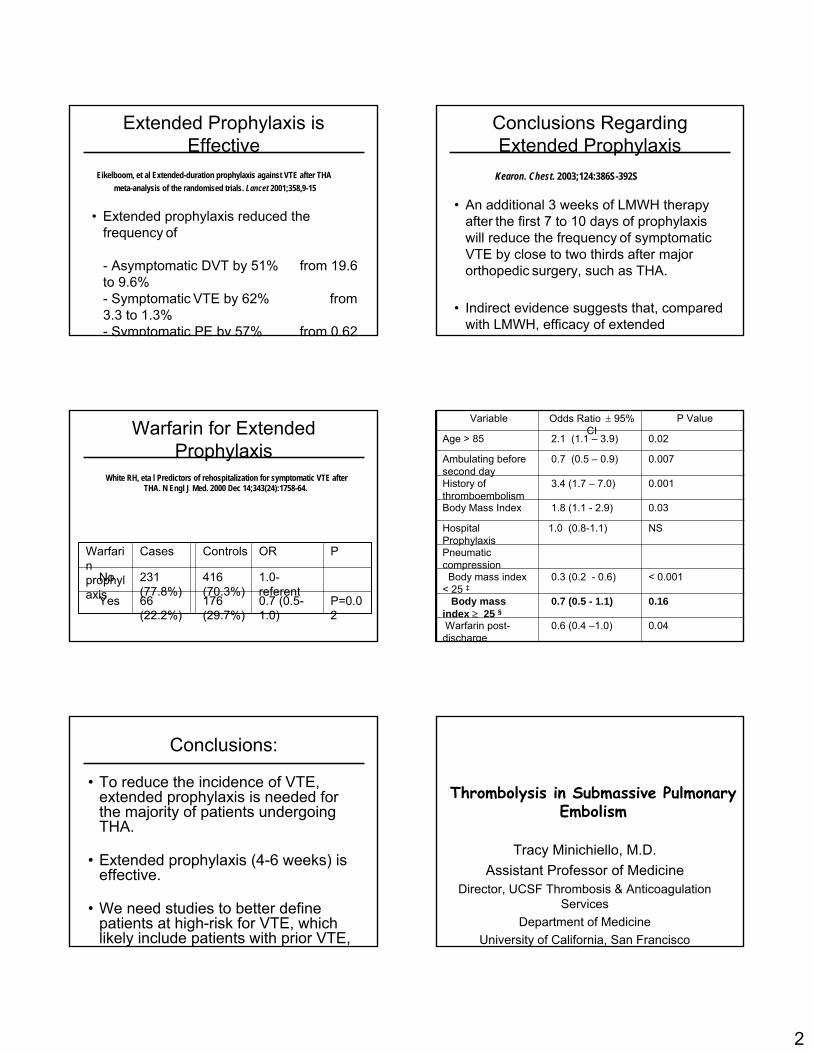
Extended Prophylaxis is Effective
• Extended prophylaxis reduced the frequency of
- Asymptomatic DVT by 51% from 19.6 to 9.6% - Symptomatic VTE by 62% from 3.3 to 1.3%- Symptomatic PE by 57% from 0.62
Eikelboom, et al Extended-duration prophylaxis against VTE after THAmeta-analysis of the randomised trials. Lancet 2001;358,9-15
Conclusions Regarding Extended Prophylaxis
• An additional 3 weeks of LMWH therapy after the first 7 to 10 days of prophylaxis will reduce the frequency of symptomatic VTE by close to two thirds after major orthopedic surgery, such as THA.
• Indirect evidence suggests that, compared with LMWH, efficacy of extended
h l i ft hi l t i
Kearon. Chest. 2003;124:386S-392S
Warfarin for Extended Prophylaxis
P=0.02
0.7 (0.5-1.0)
176 (29.7%)
66 (22.2%)
Yes
1.0-referent
416 (70.3%)
231 (77.8%)
No
PORControlsCasesWarfarin prophylaxis
White RH, eta l Predictors of rehospitalization for symptomatic VTE afterTHA. N Engl J Med. 2000 Dec 14;343(24):1758-64.
0.040.6 (0.4 –1.0)Warfarin post-discharge
0.160.7 (0.5 - 1.1)Body mass index ≥ 25 §
< 0.0010.3 (0.2 - 0.6) Body mass index < 25 ‡
Pneumatic compression
NS1.0 (0.8-1.1)Hospital Prophylaxis
0.031.8 (1.1 - 2.9)Body Mass Index
0.0013.4 (1.7 – 7.0)History of thromboembolism
0.0070.7 (0.5 – 0.9)Ambulating before second day
0.022.1 (1.1 – 3.9)Age > 85
P ValueOdds Ratio ± 95% CI
Variable
Conclusions:
• To reduce the incidence of VTE, extended prophylaxis is needed for the majority of patients undergoing THA.
• Extended prophylaxis (4-6 weeks) is effective.
• We need studies to better define patients at high-risk for VTE, which likely include patients with prior VTE, i bilit b it d d d
Tracy Minichiello, M.D.Assistant Professor of Medicine
Director, UCSF Thrombosis & Anticoagulation Services
Department of MedicineUniversity of California, San Francisco
Thrombolysis in Submassive Pulmonary Embolism
3
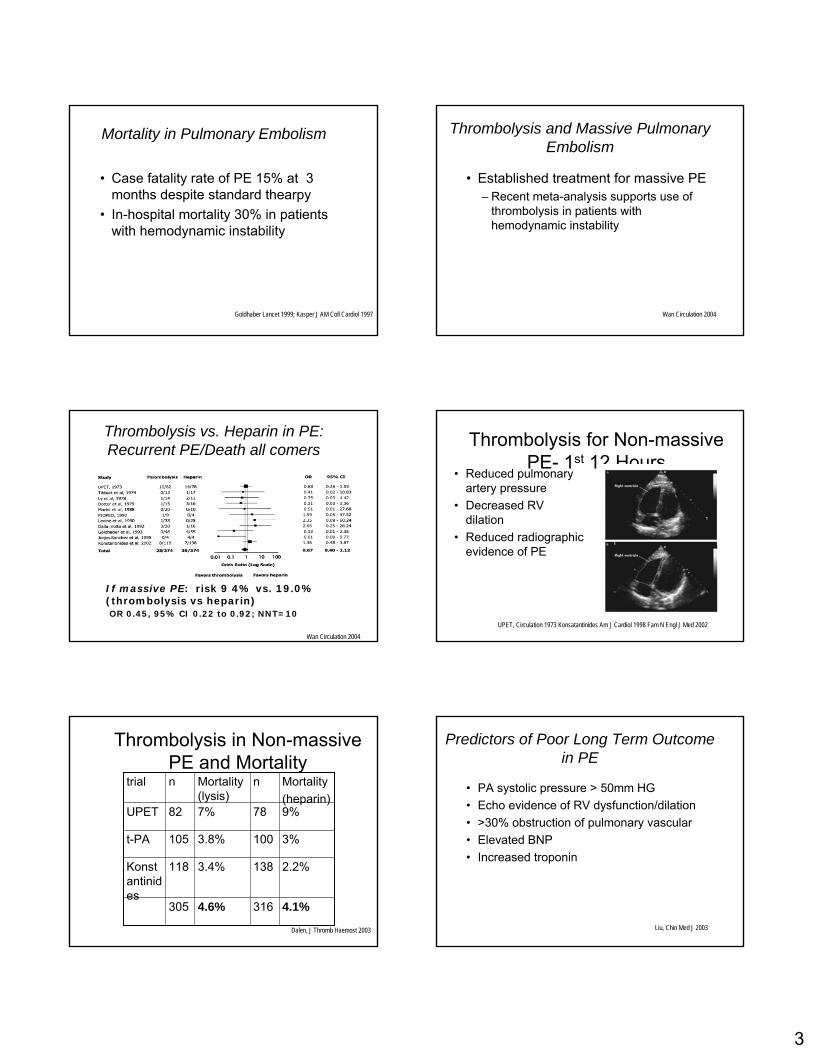
Mortality in Pulmonary Embolism
• Case fatality rate of PE 15% at 3 months despite standard thearpy
• In-hospital mortality 30% in patients with hemodynamic instability
Goldhaber Lancet 1999; Kasper J AM Coll Cardiol 1997
Thrombolysis and Massive Pulmonary Embolism
• Established treatment for massive PE – Recent meta-analysis supports use of
thrombolysis in patients with hemodynamic instability
Wan Circulation 2004
Thrombolysis vs. Heparin in PE: Recurrent PE/Death all comers
Wan Circulation 2004
If massive PE: risk 9 4% vs. 19.0% (thrombolysis vs heparin)OR 0.45, 95% CI 0.22 to 0.92; NNT=10
Thrombolysis for Non-massive PE- 1st 12 Hours
• Reduced pulmonary artery pressure
• Decreased RV dilation
• Reduced radiographic evidence of PE
UPET, Circulation 1973 Konsatantinides Am J Cardiol 1998 Fam N Engl J Med 2002
Thrombolysis in Non-massive PE and Mortality
4.1%3164.6%305
2.2%1383.4%118Konstantinides
3%1003.8%105t-PA
9%787%82UPET
Mortality(heparin)
nMortality (lysis)
ntrial
Dalen, J Thromb Haemost 2003
Predictors of Poor Long Term Outcome in PE
• PA systolic pressure > 50mm HG• Echo evidence of RV dysfunction/dilation• >30% obstruction of pulmonary vascular • Elevated BNP• Increased troponin
Liu, Chin Med J 2003
4
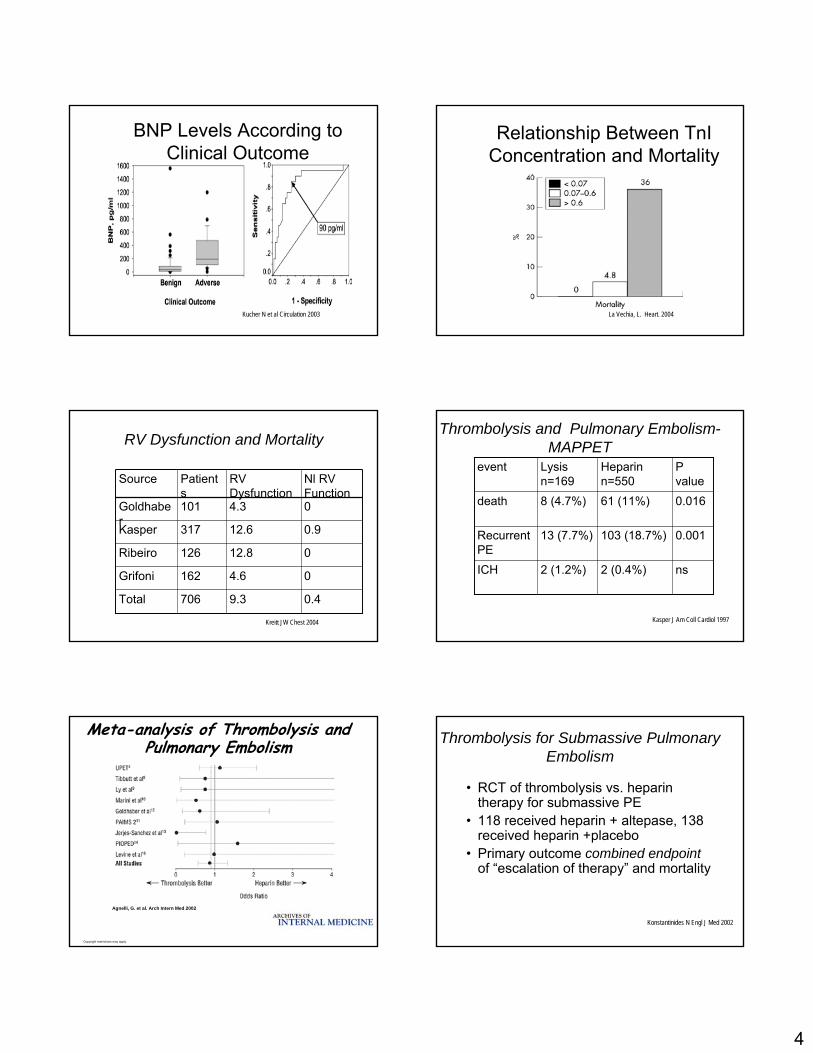
BNP Levels According to Clinical Outcome
Kucher N et al Circulation 2003
Relationship Between TnIConcentration and Mortality
La Vechia, L. Heart. 2004
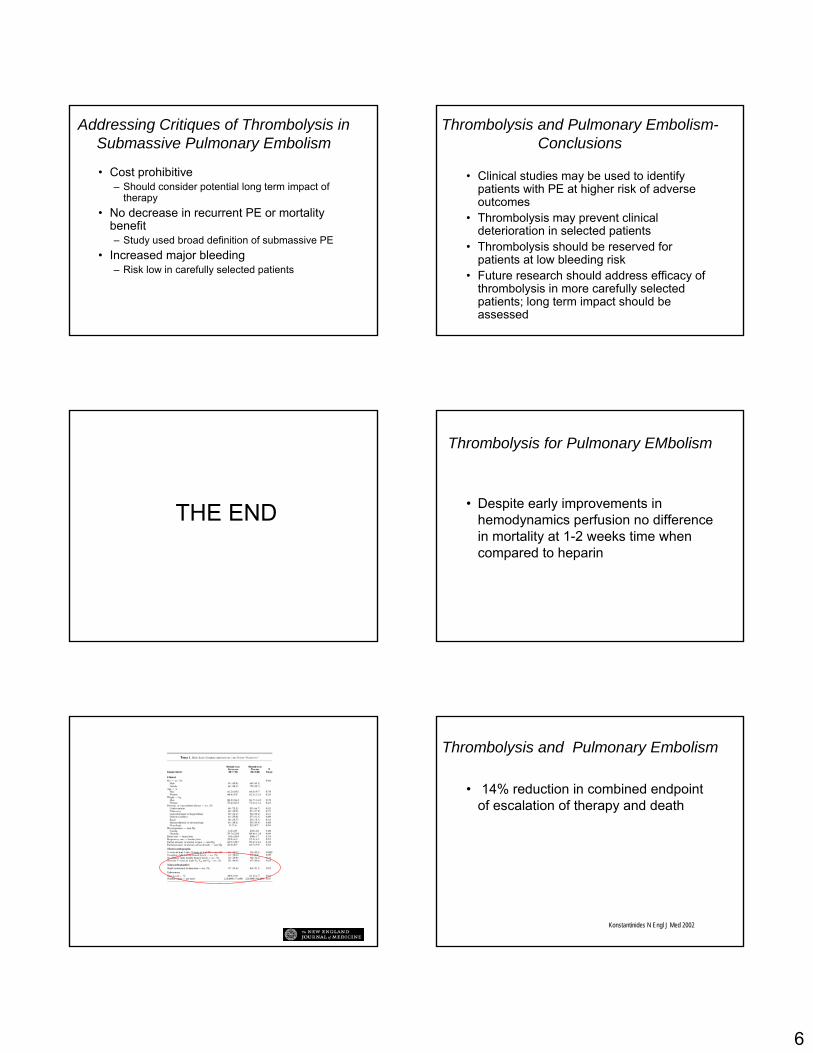
RV Dysfunction and Mortality
0.49.3706Total
04.6162Grifoni
012.8126Ribeiro
0.912.6317Kasper
04.3101Goldhaber
Nl RV Function
RV Dysfunction
Patients
Source
Kreitt JW Chest 2004
Thrombolysis and Pulmonary Embolism-MAPPET
Kasper J Am Coll Cardiol 1997
ns2 (0.4%)2 (1.2%)ICH
0.001103 (18.7%)13 (7.7%)Recurrent PE
0.01661 (11%)8 (4.7%)death
P value
Heparin n=550
Lysisn=169
event
Copyright restrictions may apply.
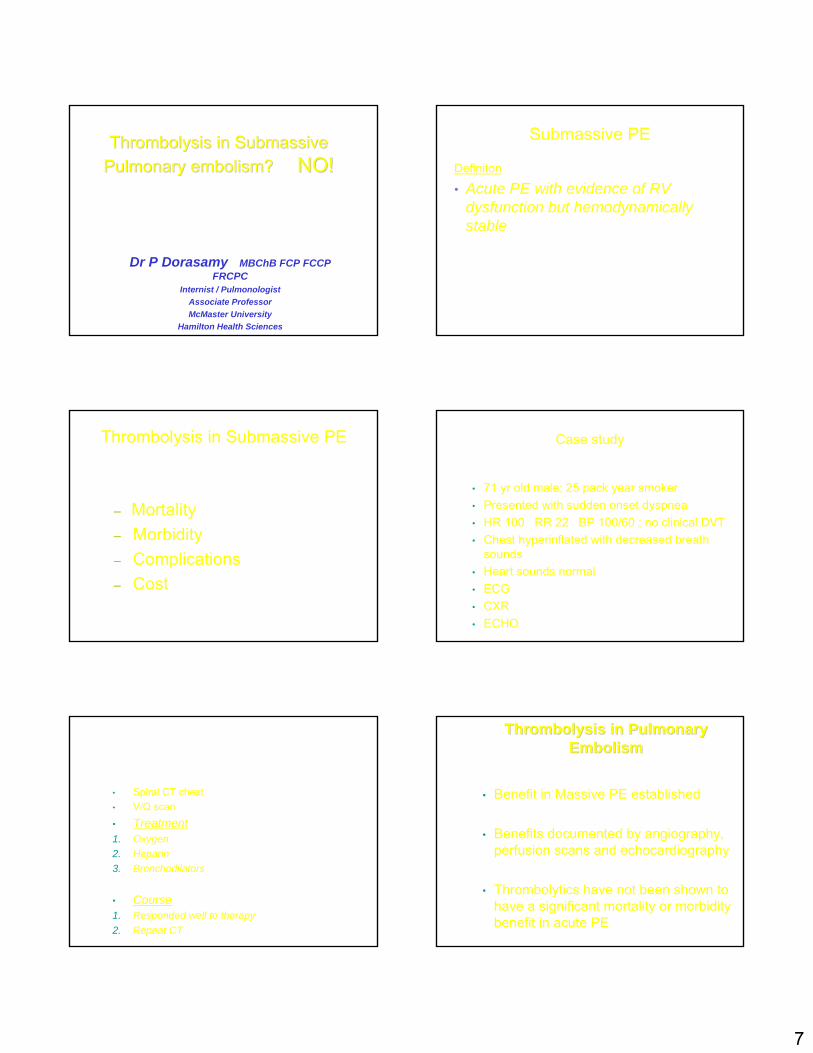
Agnelli, G. et al. Arch Intern Med 2002
Meta-analysis of Thrombolysis and Pulmonary Embolism Thrombolysis for Submassive Pulmonary
Embolism
• RCT of thrombolysis vs. heparin therapy for submassive PE
• 118 received heparin + altepase, 138 received heparin +placebo
• Primary outcome combined endpointof “escalation of therapy” and mortality
Konstantinides N Engl J Med 2002

5
Thrombolysis for Submassive Pulmonary Embolism
• Acute PE without hemodynamiccompromise plus– RV dysfunction on ECHO– Pulmonary hypertension on ECHO
or right heart cath– New RV strain on ECG
Konstantinides N Engl J Med 2002
Defining Submassive Pulmonary Embolism
• PE without evidence of hemodynamicinstability, plus – Echocardiographic evidence of RV dysfunction– Subclinical impending right heart failure– Clinical evidence of pulmonary hypertension or
right ventricular dysfunction
Thrombolysis for Submassive Pulmonary Embolism
• Exclusion– major surgery/ biopsy(7days) – major trauma (10 days)– CVA/TIA or CNS trauma (6 months).– GI bleed (3 months)– uncontrolled hypertension– a known bleeding disorder– known diabetic retinopathy
Konstantinides N Engl J Med 2002
Event Free Survival
Konstantinides, S. et al. N Engl J Med 2002
In-hospital Clinical Events
Konstantinides, S. et al. N Engl J Med 2002
Thrombolysis and Pulmonary Embolism-Bleeding risk
Kanter CHEST 1997
0.7-4.11.96/312total
0.3-3.31.34/312Nonfatal
0.08-2.30.62/312Fatal
95% CI%NoICH
6
Addressing Critiques of Thrombolysis in Submassive Pulmonary Embolism
• Cost prohibitive– Should consider potential long term impact of
therapy• No decrease in recurrent PE or mortality
benefit– Study used broad definition of submassive PE
• Increased major bleeding– Risk low in carefully selected patients
Thrombolysis and Pulmonary Embolism-Conclusions
• Clinical studies may be used to identify patients with PE at higher risk of adverse outcomes
• Thrombolysis may prevent clinical deterioration in selected patients
• Thrombolysis should be reserved for patients at low bleeding risk
• Future research should address efficacy of thrombolysis in more carefully selected patients; long term impact should be assessed
THE END
Thrombolysis for Pulmonary EMbolism
• Despite early improvements in hemodynamics perfusion no difference in mortality at 1-2 weeks time when compared to heparin
Base-Line Characteristics of the Study Patients
Konstantinides, S. et al. N Engl J Med 2002
Thrombolysis and Pulmonary Embolism
• 14% reduction in combined endpoint of escalation of therapy and death
Konstantinides N Engl J Med 2002
7
ThrombolysisThrombolysis in in SubmassiveSubmassivePulmonary embolism? Pulmonary embolism? NO!NO!
Dr P Dorasamy MBChB FCP FCCP FRCPC
Internist / PulmonologistAssociate ProfessorMcMaster University
Hamilton Health SciencesO t i C d
Submassive PE
Definiton
• Acute PE with evidence of RV dysfunction but hemodynamicallystable
Thrombolysis in Submassive PE
– Mortality– Morbidity– Complications– Cost
Case study
• 71 yr old male; 25 pack year smoker• Presented with sudden onset dyspnea• HR 100 RR 22 BP 100/60 ; no clinical DVT• Chest hyperinflated with decreased breath
sounds• Heart sounds normal• ECG• CXR• ECHO
• Spiral CT chest• V/Q scan• Treatment1. Oxygen2. Heparin3. Bronchodilators
• Course1. Responded well to therapy2. Repeat CT
ThrombolysisThrombolysis in Pulmonary in Pulmonary EmbolismEmbolism
• Benefit in Massive PE established
• Benefits documented by angiography, perfusion scans and echocardiography
• Thrombolytics have not been shown to have a significant mortality or morbidity benefit in acute PE
8
Disadvantages of Thrombolytics
• Increased major bleeding complications
• Increased cost
Randomized trials of Heparin vs Thrombolytic therapy in hemodynamically stable PE patients
4.1%3164.6%305TOTAL
2.2%1383.4%118rt - PAKonstantinides [6]
3%1003.8%105rt - PArt – PA trials [2-5]
9%787%82UrokinaseUPET [1]
MortalityNo. heparinMortalityNo. treatedLytic agentReport
1. Blackmon et al JAMA 1970; 214: 2163-722. Dalla-Volta et al J Am Coll Cardiol 19923. Goldhaber et al Lancet 19934. Levine et al Chest 19905. PIOPED Investigators - Chest 1990
6. Konstantinides et al NEJM 2002
ThrombolysisThrombolysis in Pulmonary in Pulmonary EmbolismEmbolism
• Recurrent PE is the principal cause of death in hemodynamically stable PE patients
• Thrombolysis will decrease mortality only if it decreased the rate of recurrent PE
ThrombolysisThrombolysis in Pulmonary in Pulmonary EmbolismEmbolism
• In studies where recurrent PE has been documented by follow-up lung scans or pulmonary angiograms, there has been no difference between patients treated with thrombolytics or heparin (JAMA 1970; J Am Coll Cardiol 1992; Chest 1990; NEJM 2002)
• Patients with hemodynamically stable PE, mortality with heparin therapy is < 5% (Dalen Arch Int Med 2002)
• Thrombolytics are not appropriate in these patients
Mortality in PE• Patients with submassive PE have a higher
mortality ( approx. 50% of all PE patients have RV dysfunction) (Goldhaber Lancet 1993)
• Mortality in patients with RV dysfunction was 4% vs 0.9% in those without RV dysfunction (RVD)
1. Am Heart J 1997 (Ribeiro et al)2. Circulation 2000 ( Grifoni et al)3. Intensive Care Med 2001 ( Vieillard-Baron et al)
• In 719 PE patients who were hemodynamically stable, mortality in those with RVD was 10% vs 4.1% in those without RVD (Konstantinides et al Circulation 1997)
Mortality in PE
• Hamel et al Chest 2001 reported from a French registry of 153 patients with massive PE treated consecutively with either Heparin or a thrombolytic; non-randomised; matched for right ventricular dysfunction, age, lung scans and the presence of cardiac or respiratory disease
• Mortality in 64 pts. treated with thrombolysiswas 6% vs 0% in those treated with heparin
• No difference in rate of recurrence of PE
9
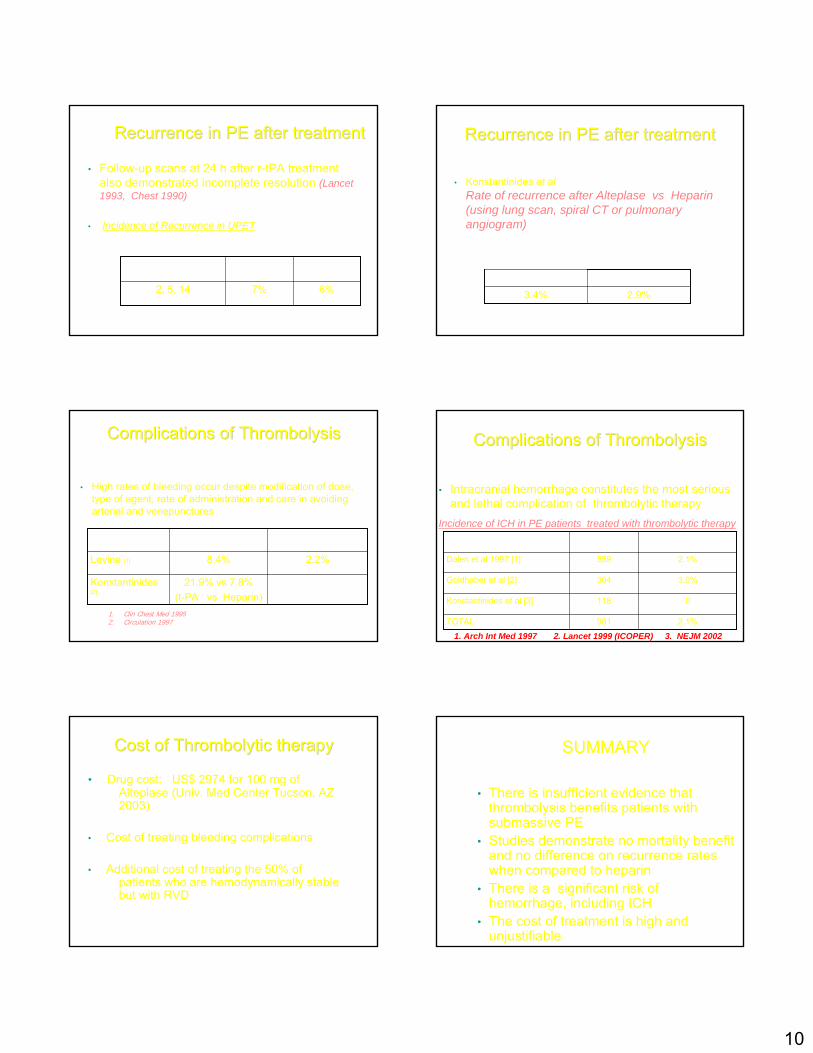
Mortality in PEMortality in PE
• Mortality in 118 pts. randomised to receive alteplase + heparin (3.4%) vs 138 pts. on heparin alone (2.2%)
• Primary end-point was in-hospital death or “clinical deterioration requiring an escalation of treatment”
Mortality in PEMortality in PE
Mortality in PEMortality in PE
• Escalation of treatment occurred in 24.6% of patients in the heparin group vs 10.2% in the alteplasegroup ( P = 0.004)
• Secondary thrombolysis occurred in 23% in the heparin group vs 7.6% in the alteplase group ( P = 0.001)
• Primary indication for secondary thrombolysis was “worsening of clinical symptoms, particularly dyspnea”.
• Mortality in 118 pts. randomised to receive alteplase+ heparin (3.4%) vs 138 pts. on heparin alone (2.2%)
• 106/138 pts. in heparin group avoided complications and excessive cost of thrombolytic treatment
ThrombolysisThrombolysis in PE patients with in PE patients with shockshock
• No randomized clinical trials comparing heparin to thrombolytic therapy in patients with massive PE complicated by shock
• Because of high mortality (30%) in PE patients with shock, thrombolysis is considered
• Shock present in 10% of patients diagnosed with PE
Impact of Impact of ThrombolysisThrombolysis on on morbidity in PEmorbidity in PE
• In patients who survive acute PE, morbidity may be due to unresolved pulmonary embolic obstruction, or to recurrent PE
• Thrombolytic therapy increases the early resolution rate of pulmonary embolic obstruction as assessed by repeat lung scans or pulmonary angiograms 24 h after therapy. BUT the degree of resolution 24 h after thrombolytic therapy is incomplete
Morbidity in PEMorbidity in PE
• The Urokinase PE trial (UPET)(JAMA 1970)
Percent resolution by lung scan after therapy
77.2%78.8%1 year
56.2%55.4%2 weeks
8.3%24.1%24 h
HeparinUrokinaseTime since treatment
10
Recurrence in PE after treatmentRecurrence in PE after treatment
• Follow-up scans at 24 h after r-tPA treatment also demonstrated incomplete resolution (Lancet 1993, Chest 1990)
• Incidence of Recurrence in UPET
6%7%2, 5, 14
HeparinUrokinaseDays after treatment
Recurrence in PE after treatmentRecurrence in PE after treatment
• Konstantinides et alRate of recurrence after Alteplase vs Heparin (using lung scan, spiral CT or pulmonary angiogram)
2.9%3.4%
HeparinAlteplase
Complications of Complications of ThrombolysisThrombolysis
• High rates of bleeding occur despite modification of dose, type of agent, rate of administration and care in avoiding arterial and venepunctures
21.9% vs 7.8%(t-PA vs Heparin)
Konstantinides[2]
2.2%8.4%Levine [1]
Fatal hemorrhageMajor bleeding
1. Clin Chest Med 19952. Circulation 1997
Complications of Complications of ThrombolysisThrombolysis
• Intracranial hemorrhage constitutes the most serious and lethal complication of thrombolytic therapy
Incidence of ICH in PE patients treated with thrombolytic therapy
2.1%981TOTAL
0118Konstantinides et al [3]
3.0%304Goldhaber et al [2]
2.1%559Dalen et al 1997 [1]
Incidence of ICHPatients (n)Report
1. Arch Int Med 1997 2. Lancet 1999 (ICOPER) 3. NEJM 2002
Cost of Cost of ThrombolyticThrombolytic therapytherapy
• Drug cost: US$ 2974 for 100 mg ofAlteplase (Univ. Med Center Tucson, AZ 2003)
• Cost of treating bleeding complications
• Additional cost of treating the 50% ofpatients who are hemodynamically stable but with RVD
SUMMARY
• There is insufficient evidence that thrombolysis benefits patients with submassive PE
• Studies demonstrate no mortality benefit and no difference on recurrence rates when compared to heparin
• There is a significant risk of hemorrhage, including ICH
• The cost of treatment is high and unjustifiable
11
Duration of Anticoagulation for Treatment of Acute VTE
Andrew Dunn, MD, FACPDirector, General Medicine Anticoagulation Service
Mount Sinai Medical CenterNew York, NY
SGIM PRECOURSEMay 11, 2005
A 48 year-old female presents with 4 days of right leg pain and swelling. An ultrasound confirms the presence of a right LE DVT.
Treatment with outpatient LMWH and warfarin is begun. LMWH is discontinued when the INR is therapeutic on day #6.
The patient does not have h/o VTE, had no recent surgery or trauma, and is not on OCP or HRT. There is no family history of VTE. A thrombophilia work-up is negative.
How long will you treat the patient with warfarin?
48 year-old female with idiopathic right LE DVT
• 6 months
• 12 months
• Lifelong
• 3 months
• Even longer
• Indefinitely
• 2 years
Expert opinion?
48 year-old with first idiopathic DVT
Buller HR. Chest. 2004;126:401S-428S.
“For patients with a first episode of idiopathic DVT, we recommend treatment with a VKA for at least 6 to 12 months.”
“We suggest that patients with first-episode idiopathic DVT be considered for indefinite anticoagulant therapy.”
What Is Worse?
+
Extended OAC for First VTE3 months vs 24 months
Kearon C. NEJM. 1999;340:901-7.
All patients received 3 months of standard treatment
Randomized to:Additional 24 months OAC (INR goal 2-3) or placebo
Study terminated early (mean f/u 10 months)
12
Standard Extended
Recurrent VTE
Fatal PE
Major Bleeding
1 (1)
0 (0) 3 (4)
1 (1) 0 (0)
17 (27) P<.001
P=.09
P=NS
Kearon C. NEJM. 1999;340:901-7.
Extended OAC for First VTE
n=79 n=83
Extended OAC for First DVT3 months vs 1 year
Agnelli G. NEJM. 2001;345:165-9.
…and lets look 1 year (or more) later
Agnelli G. NEJM. 2001;345:165-9.
3 months 1 year
Recurrent VTE
Recurrent VTE(months 3-12)
Major Bleeding
21 (16)
2 (1.5) 4 (3)
11 (8) 4 (3)
21 (16)
P=NS
P=NS
P=NS
Average f/u 38 months
Extended OAC for First DVT3 months vs 1 year
Extended OAC Duration Treatment of PE
Agnelli G. Ann Intern Med. 2003;139:19-25.
3 months OAC for acute PE vs
6 months (transient risk factor) or 12 months (idiopathic)
Followed for average of 3 years.
Italian study, 19 hospitals.
N = 326
3 months Extended
Recurrent VTETotal group, n (%)
15/165 (9.1)18/369 (11.2) P=NS
PE Treatment3 months vs Extended Duration
Agnelli G. Ann Intern Med. 2003;139:19-25.
Recurrent VTEIdiopathic
11/90 (12.2)11/91 (12.1) P=NS
All but 1 recurrence occurred after OAC discontinued
Long-term Low-Intensity Warfarin for Prevention of Recurrent VTE
PREVENT
Ridker PM. NEJM. 2003:348:1425-34.
Low-intensity Warfarin (INR 1.5-2.0) indefinitely vs Placebo
All received standard treatment (mean 6.5 months)N=508
Average follow-up 2.1 years.
Trial terminated early
13
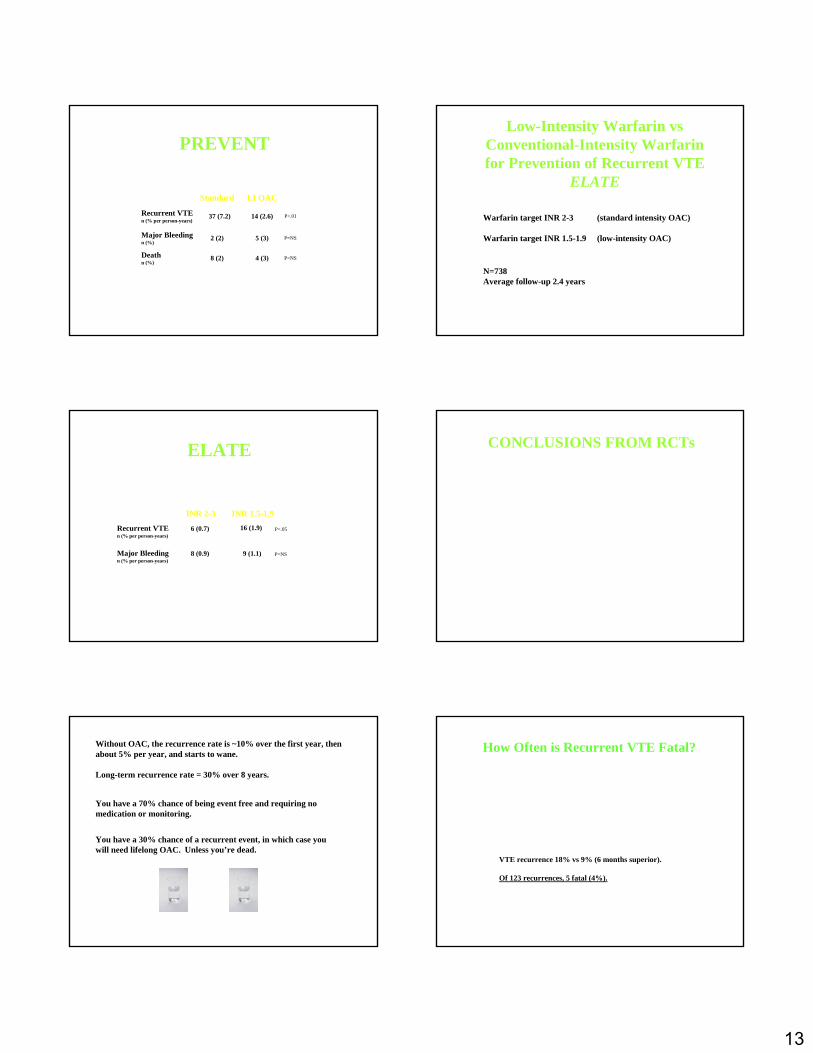
Ridker PM. NEJM. 2003:348:1425-34.
PREVENT
Standard LI OAC
Recurrent VTEn (% per person-years)
Major Bleedingn (%)
14 (2.6)
2 (2) 5 (3)
37 (7.2)
P=NS
P<.01
Deathn (%)
8 (2) 4 (3) P=NS
Low-Intensity Warfarin vs Conventional-Intensity Warfarin for Prevention of Recurrent VTE
ELATE
Kearon C. NEJM. 2003:349:631-9.
Warfarin target INR 2-3 (standard intensity OAC)
Warfarin target INR 1.5-1.9 (low-intensity OAC)
N=738Average follow-up 2.4 years
INR 2-3 INR 1.5-1.9
Recurrent VTEn (% per person-years)
Major Bleedingn (% per person-years)
16 (1.9)
8 (0.9) 9 (1.1)
6 (0.7)
P=NS
P<.05
ELATE
Kearon C. NEJM. 2003:349:631-9.
CONCLUSIONS FROM RCTs
• Warfarin works when you are on it
• When you stop warfarin, there is a “catch-up” phenomenon
• If you are treating long-term or indefinite, you are treating lifelong
• If you are going to stop eventually, 6 months reasonable choice
• Major bleeding doesn’t happen in large RCTs
Without OAC, the recurrence rate is ~10% over the first year, then about 5% per year, and starts to wane.
Long-term recurrence rate = 30% over 8 years.
You have a 70% chance of being event free and requiring no medication or monitoring.
You have a 30% chance of a recurrent event, in which case you will need lifelong OAC.
Prandoni P. Annals Intern Med. 1996;125:1-7.
Unless you’re dead.
How Often is Recurrent VTE Fatal?
Schulman S. NEJM. 1995;332:1661-5.
Duration of Anticoagulation Trial Study Group (DURAC)
6 weeks vs 6 months. F/U for 2 years.N = 498.
VTE recurrence 18% vs 9% (6 months superior).
Of 123 recurrences, 5 fatal (4%).
14
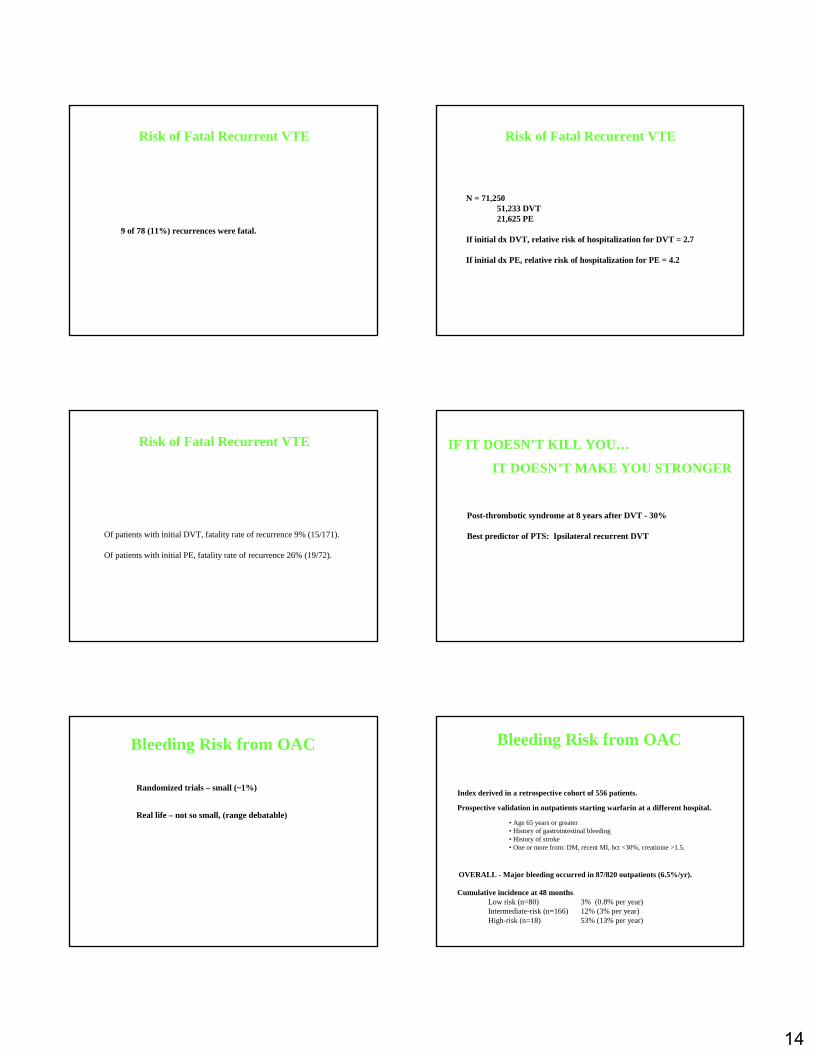
Risk of Fatal Recurrent VTE
Long-term follow-up study355 patients with first DVT
Prandoni P. Annals Intern Med. 1996;125:1-7.
9 of 78 (11%) recurrences were fatal.
Analysis of California Discharge Database - VTE diagnoses
Risk of Fatal Recurrent VTE
Murin S. Thromb Haem. 2002;88:407-14
N = 71,25051,233 DVT21,625 PE
If initial dx DVT, relative risk of hospitalization for DVT = 2.7
If initial dx PE, relative risk of hospitalization for PE = 4.2
Review of 25 studies of treatment of DVT or PE
Risk of Fatal Recurrent VTE
Douketis JD. JAMA. 1998;279:458-62
Of patients with initial DVT, fatality rate of recurrence 9% (15/171).
Of patients with initial PE, fatality rate of recurrence 26% (19/72).
IF IT DOESN’T KILL YOU…
IT DOESN’T MAKE YOU STRONGER
Prandoni P. Annals Intern Med. 1996;125:1-7.
Post-thrombotic syndrome at 8 years after DVT - 30%
Best predictor of PTS: Ipsilateral recurrent DVT
Bleeding Risk from OAC
Randomized trials – small (~1%)
Real life – not so small, (range debatable)
Outpatient Bleeding Risk Index (OBRI)
Beyth RJ. Am J Med. 1998;91-99.
Index derived in a retrospective cohort of 556 patients.
Prospective validation in outpatients starting warfarin at a different hospital.
OVERALL - Major bleeding occurred in 87/820 outpatients (6.5%/yr).
• Age 65 years or greater• History of gastrointestinal bleeding• History of stroke• One or more from: DM, recent MI, hct <30%, creatinine >1.5.
Bleeding Risk from OAC
Cumulative incidence at 48 monthsLow risk (n=80) 3% (0.8% per year)Intermediate-risk (n=166) 12% (3% per year)High-risk (n=18) 53% (13% per year)
15
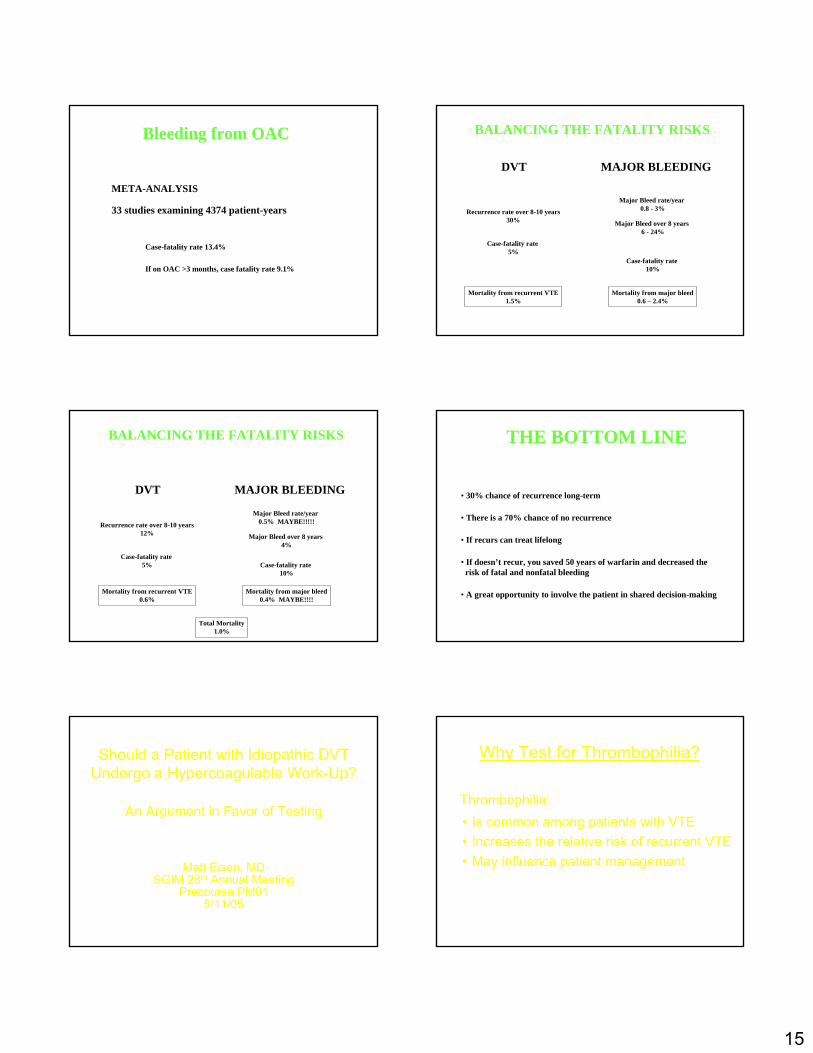
How often is it fatal?
Linkins L. Ann Intern Med. 2003;139:893-901.
META-ANALYSIS
Bleeding from OAC
33 studies examining 4374 patient-years
Case-fatality rate 13.4%
If on OAC >3 months, case fatality rate 9.1%
BALANCING THE FATALITY RISKS
DVT MAJOR BLEEDING
Recurrence rate over 8-10 years30%
Case-fatality rate 5%
Mortality from recurrent VTE1.5%
Major Bleed rate/year 0.8 - 3%
Case-fatality rate 10%
Mortality from major bleed0.6 – 2.4%
Major Bleed over 8 years 6 - 24%
without warfarin with warfarin
BALANCING THE FATALITY RISKS
DVT MAJOR BLEEDING
Recurrence rate over 8-10 years12%
Case-fatality rate 5%
Mortality from recurrent VTE0.6%
Major Bleed rate/year 0.5% MAYBE!!!!!
Case-fatality rate 10%
Mortality from major bleed0.4% MAYBE!!!!
Major Bleed over 8 years 4%
If on low-dose warfarin
Total Mortality1.0%
THE BOTTOM LINE48 year-old female first idiopathic DVT
• 30% chance of recurrence long-term
• If recurs can treat lifelong
• If doesn’t recur, you saved 50 years of warfarin and decreased the risk of fatal and nonfatal bleeding
• A great opportunity to involve the patient in shared decision-making
• There is a 70% chance of no recurrence
Should a Patient with Idiopathic DVT Undergo a Hypercoagulable Work-Up?
An Argument in Favor of Testing
Matt Eisen, MDSGIM 28th Annual Meeting
Precourse PM015/11/05
Why Test for Thrombophilia?
Thrombophilia:• Is common among patients with VTE• Increases the relative risk of recurrent VTE• May influence patient management
16
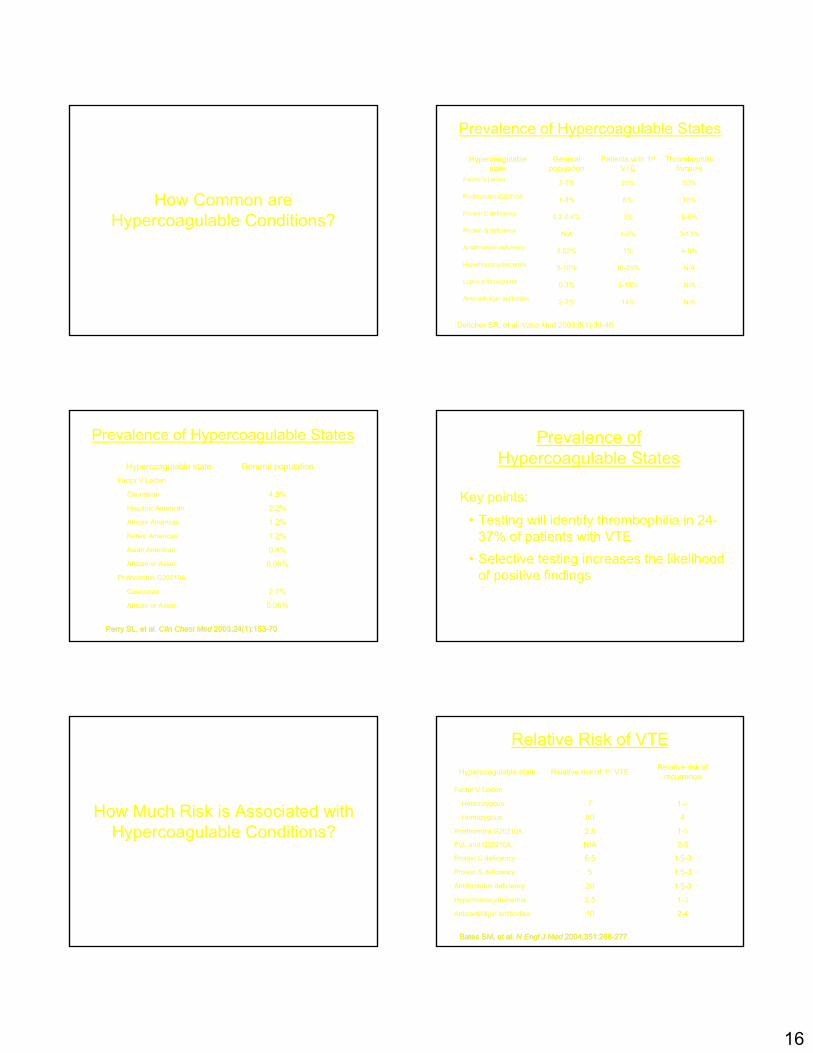
How Common are Hypercoagulable Conditions?
Prevalence of Hypercoagulable States
N/A14%2-7%Anticardiolipin antibodies
N/A5-15%0-3%Lupus anticoagulant
N/A10-25%5-10%Hyperhomocysteinemia
4-8%1%0.02%Antithrombin deficiency
3-13%1-2%N/AProtein S deficiency
6-8%3%0.2-0.4%Protein C deficiency
18%6%1-3%Prothrombin G20210A
50%20%3-7%Factor V Leiden
Thrombophilicfamilies
Patients with 1st
VTEGeneral
populationHypercoagulable
state
Deitcher SR, et al. Vasc Med 2003;8(1):33-46
Increasing Prevalence
Prevalence of Hypercoagulable States
0.06%African or Asian
2.7%Caucasian
Prothrombin G20210A
0.05%African or Asian
0.4%Asian American
1.2%Native American
1.2%African American
2.2%Hispanic American
4.8%Caucasian
Factor V Leiden
General populationHypercoagulable state
Perry SL, et al. Perry SL, et al. ClinClin Chest MedChest Med 2003;24(1):1532003;24(1):153--7070
Prevalence ofHypercoagulable States
Key points:
• Testing will identify thrombophilia in 24-37% of patients with VTE
• Selective testing increases the likelihood of positive findings
How Much Risk is Associated with Hypercoagulable Conditions?
Relative Risk of VTE
2-410Anticardiolipin antibodies
1-32.5Hyperhomocysteinemia
1.5-320Antithrombin deficiency
1.5-35Protein S deficiency
1.5-36.5Protein C deficiency
2-5N/AFVL and G20210A
1-52.8Prothrombin G20210A
480Homozygous
1-47Heterozygous
Factor V Leiden
Relative risk of recurrenceRelative risk of 1st VTEHypercoagulable state
Bates SM, et al. Bates SM, et al. N N EnglEngl J MedJ Med 2004;351:2682004;351:268--277277
17
How Might the Presence of Thrombophilia Affect Patient
Management?
Duration of Therapy
Consider extended anticoagulation in patients with 1st idiopathic VTE and:• Homozygous factor V leiden or prothrombin
gene mutation• Combined heterozygous defects• Protein C or S deficiency• Antithrombin deficiency• Antiphospholipid antibodies
Intensity/Monitoring of Therapy
In patients with antiphospholipid antibody syndrome:• Consider higher target INR• Consider monitoring by chromogenic
factor X assay
Other Therapies
In patients with hyperhomocysteinemia:
• Consider giving folate / B6 / B12 and monitoring for improvement in serum homocysteine
Screening Family Members
Finding of thrombophilia has implications for:
• Decision to use OCPs• Decision to use HRT• Management of pregnancy
Feero WG. Prim Care 2004;31(3):685-709,xi
18
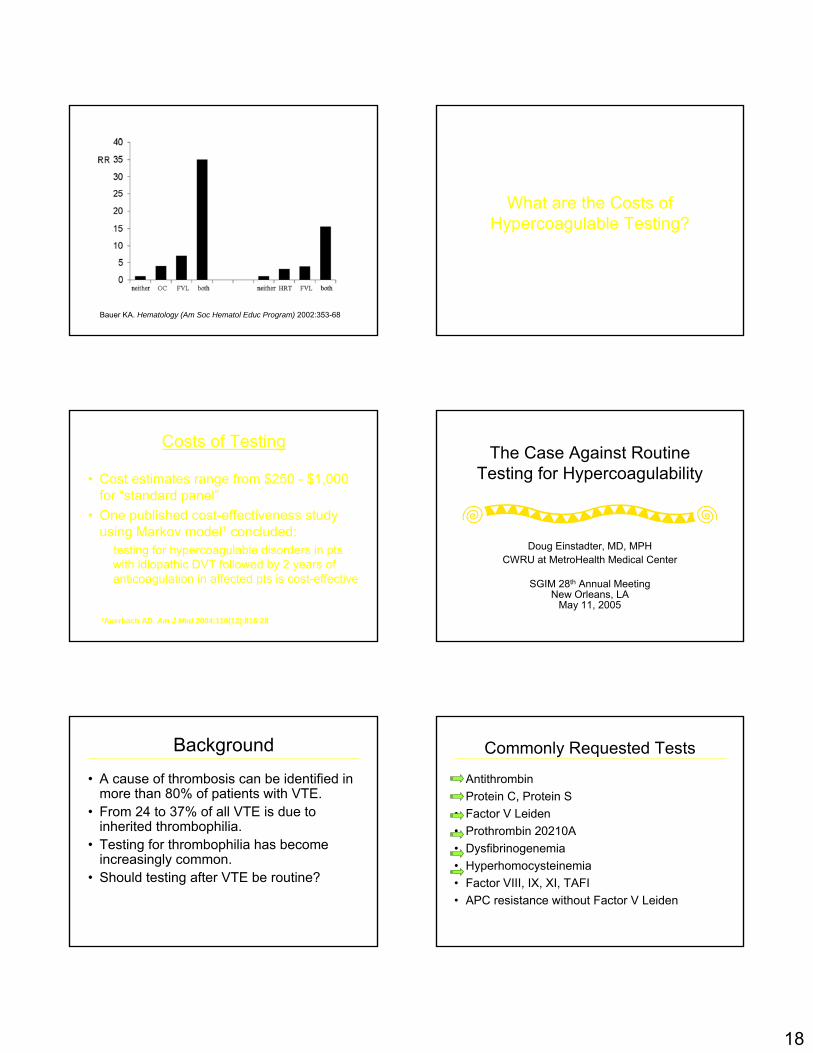
Bauer KA. Hematology (Am Soc Hematol Educ Program) 2002:353-68
What are the Costs of Hypercoagulable Testing?
Costs of Testing
• Cost estimates range from $250 - $1,000 for “standard panel”
• One published cost-effectiveness study using Markov model¹ concluded:
testing for hypercoagulable disorders in pts with idiopathic DVT followed by 2 years of anticoagulation in affected pts is cost-effective
¹Auerbach AD. Am J Med 2004;116(12):816-28
The Case Against Routine Testing for Hypercoagulability
Doug Einstadter, MD, MPHCWRU at MetroHealth Medical Center
SGIM 28th Annual Meeting New Orleans, LA
May 11, 2005
Background
• A cause of thrombosis can be identified in more than 80% of patients with VTE.
• From 24 to 37% of all VTE is due to inherited thrombophilia.
• Testing for thrombophilia has become increasingly common.
• Should testing after VTE be routine?
Commonly Requested Tests
• Antithrombin• Protein C, Protein S• Factor V Leiden• Prothrombin 20210A• Dysfibrinogenemia• Hyperhomocysteinemia• Factor VIII, IX, XI, TAFI• APC resistance without Factor V Leiden
19
Potential Reasons to Test
• To determine optimal duration of therapy• To determine optimal intensity of therapy• To identify and recommend prophylaxis for
asymptomatic family members during:– High risk situations– Pregnancy, oral contraceptive use, HRT
• “Need to know” (intellectual curiosity)
Assumptions Underlying a Decision to Test
1. Presence of identified thrombophilia predicts greater risk of recurrence.
2. More intense treatment for those with thrombophilia leads to better outcomes.
3. Family members of patients with VTE and thrombophilia are at increased risk.
4. Prophylactic treatment of family members leads to improved outcomes.
Does the Literature Support the Assumptions for Testing?
Is Risk of RecurrentVTE Increased?
• The overall risk of recurrent VTE in patients with and without thrombophilia is similar
Lancet 2003; 362: 523Lancet 2003; 362: 523--2626
HR 1.50 [95% CI 0.82–2.77]; p=0.187
Risk of Recurrent VTE with and without Identified Thrombophilia
Is Risk of RecurrentVTE Increased?
• The overall risk in patients with and without thrombophilia is similar
• Risk for patients with and without heterozygous Factor V Leiden or G20210A is similar; risk in patients with homozygous Factor V Leiden probably is increased
20
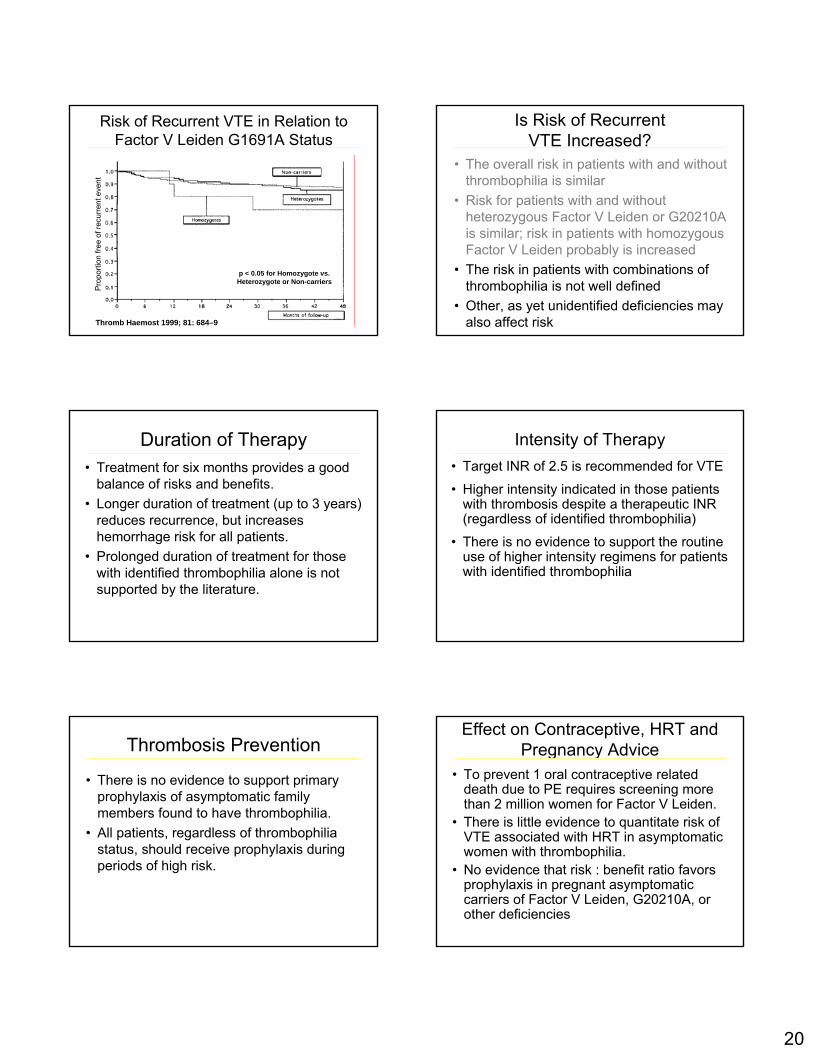
Thromb Haemost 1999; 81: 684–9
Risk of Recurrent VTE in Relation to Factor V Leiden G1691A Status
Pro
porti
on fr
ee o
f rec
urre
nt e
vent
p < 0.05 for Homozygote vs. Heterozygote or Non-carriers
Is Risk of RecurrentVTE Increased?
• The overall risk in patients with and without thrombophilia is similar
• Risk for patients with and without heterozygous Factor V Leiden or G20210A is similar; risk in patients with homozygous Factor V Leiden probably is increased
• The risk in patients with combinations of thrombophilia is not well defined
• Other, as yet unidentified deficiencies may also affect risk
Duration of Therapy• Treatment for six months provides a good
balance of risks and benefits. • Longer duration of treatment (up to 3 years)
reduces recurrence, but increases hemorrhage risk for all patients.
• Prolonged duration of treatment for those with identified thrombophilia alone is not supported by the literature.
Intensity of Therapy• Target INR of 2.5 is recommended for VTE
• Higher intensity indicated in those patients with thrombosis despite a therapeutic INR (regardless of identified thrombophilia)
• There is no evidence to support the routine use of higher intensity regimens for patients with identified thrombophilia
Thrombosis Prevention
• There is no evidence to support primary prophylaxis of asymptomatic family members found to have thrombophilia.
• All patients, regardless of thrombophilia status, should receive prophylaxis during periods of high risk.
Effect on Contraceptive, HRT and Pregnancy Advice
• To prevent 1 oral contraceptive related death due to PE requires screening more than 2 million women for Factor V Leiden.
• There is little evidence to quantitate risk of VTE associated with HRT in asymptomatic women with thrombophilia.
• No evidence that risk : benefit ratio favors prophylaxis in pregnant asymptomatic carriers of Factor V Leiden, G20210A, or other deficiencies
21
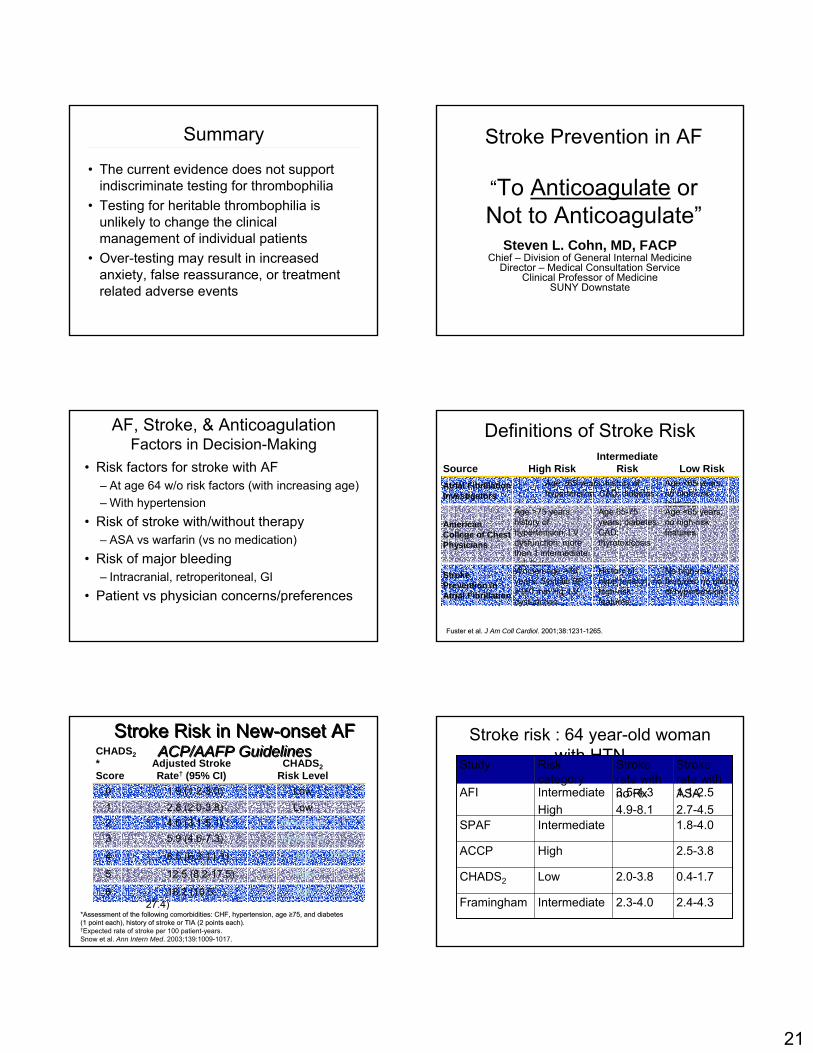
Summary
• The current evidence does not support indiscriminate testing for thrombophilia
• Testing for heritable thrombophilia is unlikely to change the clinical management of individual patients
• Over-testing may result in increased anxiety, false reassurance, or treatment related adverse events
Stroke Prevention in AF
“To Anticoagulate or Not to Anticoagulate”
Steven L. Cohn, MD, FACPChief – Division of General Internal Medicine
Director – Medical Consultation ServiceClinical Professor of Medicine
SUNY Downstate
AF, Stroke, & AnticoagulationFactors in Decision-Making
• Risk factors for stroke with AF– At age 64 w/o risk factors (with increasing age)– With hypertension
• Risk of stroke with/without therapy– ASA vs warfarin (vs no medication)
• Risk of major bleeding– Intracranial, retroperitoneal, GI
• Patient vs physician concerns/preferences
Definitions of Stroke Risk
No high-risk features; no history of hypertension
History of hypertension; no high-risk features
Women age >75 years; Systolic BP >160 mm Hg; LV dysfunction
Stroke Prevention in Atrial Fibrillation
Age <65 years; no high-risk features
Age 65-75 years; diabetes; CAD; thyrotoxicosis
Age >75 years; history of hypertension; LV dysfunction; more than 1 intermediate risk factor
American College of Chest Physicians
Age <65 years; no high-risk features
Age ≥65 years; history of hypertension; CAD; diabetes
Atrial Fibrillation Investigators
Low RiskIntermediate
RiskHigh RiskSource
Fuster et al. Fuster et al. J Am Coll CardiolJ Am Coll Cardiol. 2001;38:1231. 2001;38:1231--1265.1265.
Stroke Risk in New-onset AFACP/AAFP Guidelines
Stroke Risk in New-onset AFACP/AAFP Guidelines
Moderate5.9 (4.6-7.3)3
High8.5 (6.3-11.1)4
High12.5 (8.2-17.5)5
High18.2 (10.5-27.4)
6
Low1.9 (1.2-3.0)0
Moderate4.0 (3.1-5.1)2Low2.8 (2.0-3.8)1
CHADS2Risk Level
Adjusted Stroke Rate† (95% CI)
CHADS2*Score
*Assessment of the following comorbidities: CHF, *Assessment of the following comorbidities: CHF, hypertensionhypertension, age , age ≥≥75, and diabetes 75, and diabetes (1 point each), history of stroke or TIA (2 points each). (1 point each), history of stroke or TIA (2 points each). †Expected rate of stroke per 100 patient-years.Snow et al. Ann Intern Med. 2003;139:1009-1017.
Warfarin
Stroke risk : 64 year-old woman with HTN
2.4-4.3
0.4-1.7
2.5-3.8
1.8-4.0
1.1-2.52.7-4.5
Stroke rate with ASA
2.3-4.0
2.0-3.8
3.5-4.34.9-8.1
Stroke rate with no Rx
IntermediateFramingham
LowCHADS2
HighACCP
IntermediateSPAF
IntermediateHigh
AFI
Risk category
Study
22
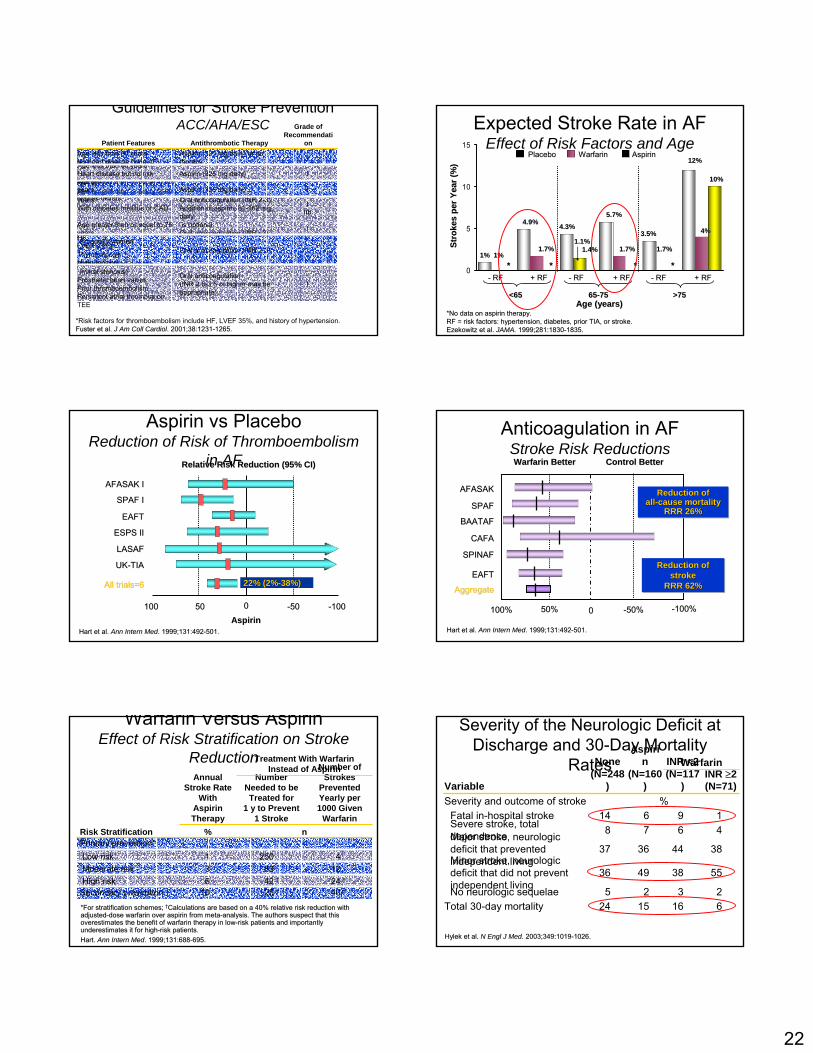
Guidelines for Stroke PreventionACC/AHA/ESC
*Risk factors for thromboembolism include HF, LVEF 35%, and history of hypertension.Fuster et al. Fuster et al. J Am Coll CardiolJ Am Coll Cardiol. 2001;38:1231. 2001;38:1231--1265.1265.
IOral anticoagulation(INR 2.5-3.5 or higher may be appropriate)
Rheumatic heart disease(mitral stenosis)
Prosthetic heart valvesPrior thromboembolismPersistent atrial thrombus on TEE
IOral anticoagulation (INR 2-3)
HFLVEF ≤35%.ThyrotoxicosisHypertension
IIIb
I
Oral anticoagulation (INR 2-3)Addition of aspirin, 81-162 mg dailyis optional
Oral anticoagulation (INR ≈2)
Age greater than or equal to 60 yearsWith diabetes mellitus or CAD
Age greater than or equal to 75 years,especially women
IAspirin (325 mg daily)Age greater than or equal to 60 yearsNo risk factors*
IAspirin (325 mg daily)Age less than 60 yearsHeart disease but no risk factors*
IAspirin (325 mg daily) or no therapy
Age less than 60 yearsNo heart disease (lone AF)
Grade of Recommendati
onAntithrombotic TherapyPatient Features
Expected Stroke Rate in AFEffect of Risk Factors and Age
*No data on aspirin therapy.*No data on aspirin therapy.RF = risk factors: RF = risk factors: hypertensionhypertension, diabetes, prior TIA, or stroke., diabetes, prior TIA, or stroke.Ezekowitz et al. Ezekowitz et al. JAMA.JAMA. 1999;281:18301999;281:1830--1835.1835.
0
5
10
15
-- RFRF -- RFRF -- RFRF+ RF+ RF + RF+ RF + RF+ RF
Age (years)Age (years)
Stro
kes
per Y
ear (
%)
Stro
kes
per Y
ear (
%)
WarfarinWarfarinPlaceboPlacebo AspirinAspirin
>75>756565--7575<65<65
10%10%
4%4%
12%12%
**
1.7%1.7%
3.5%3.5%
1.7%1.7%
**
5.7%5.7%
1.4%1.4%1.1%1.1%
4.3%4.3%
1.7%1.7%
**
4.9%4.9%
1%1% 1%1%**
Aspirin vs PlaceboReduction of Risk of Thromboembolism
in AFAFASAK IAFASAK I
SPAF ISPAF I
EAFTEAFT
ESPS IIESPS II
LASAFLASAF
UKUK--TIATIA
All trials=6All trials=6
Relative Risk Reduction (95% CI)Relative Risk Reduction (95% CI)
100100 5050 00 --5050 --100100AspirinAspirin
Hart et al. Hart et al. Ann Intern MedAnn Intern Med. 1999;131:492. 1999;131:492--501.501.
22% (2%22% (2%--38%) 38%)
Anticoagulation in AFStroke Risk Reductions
Hart et al. Hart et al. Ann Intern MedAnn Intern Med. 1999;131:492. 1999;131:492--501.501.
Warfarin BetterWarfarin Better Control BetterControl Better
AFASAKAFASAK
SPAFSPAF
BAATAFBAATAF
CAFACAFA
SPINAFSPINAF
EAFTEAFT
100%100% 50%50% 00 --50%50% --100%100%
AggregateAggregate
Reduction of stroke
RRR 62%
Reduction of Reduction of strokestroke
RRR 62% RRR 62%
Reduction ofall-cause mortality
RRR 26%
Reduction ofReduction ofallall--cause mortality cause mortality
RRR 26%RRR 26%
Warfarin Versus AspirinEffect of Risk Stratification on Stroke
Reduction
*For stratification schemes; *For stratification schemes; ††Calculations are based on a 40% relative risk reduction with Calculations are based on a 40% relative risk reduction with adjustedadjusted--dose warfarin over aspirin from metadose warfarin over aspirin from meta--analysis. The authors suspect that this analysis. The authors suspect that this overestimates the benefit of warfarin therapy in lowoverestimates the benefit of warfarin therapy in low--risk patients and importantly risk patients and importantly underestimates it for highunderestimates it for high--risk patients.risk patients.Hart. Hart. Ann Intern MedAnn Intern Med. 1999;131:688. 1999;131:688--695.695.
40 †25 †10Secondary prevention24 †42 †6High risk12833Moderate risk42501Low risk
Primary prevention*n%Risk Stratification
Number of Strokes
Prevented Yearly per 1000 Given
Warfarin
Number Needed to be Treated for
1 y to Prevent 1 Stroke
Treatment With Warfarin Instead of Aspirin
Annual Stroke Rate
With Aspirin Therapy
Severity of the Neurologic Deficit at Discharge and 30-Day Mortality
Rates
Hylek et al. Hylek et al. N Engl J MedN Engl J Med. 2003;349:1019. 2003;349:1019--1026.1026.
6161524Total 30-day mortality2325No neurologic sequelae
55384936Minor stroke, neurologic deficit that did not prevent independent living
38443637Major stroke, neurologic deficit that prevented independent living
4678Severe stroke, total dependence
19614Fatal in-hospital stroke%Severity and outcome of stroke
INR ≥2(N=71)
INR <2(N=117
)
Aspirin
(N=160)
None(N=248
)Variable
Warfarin
23
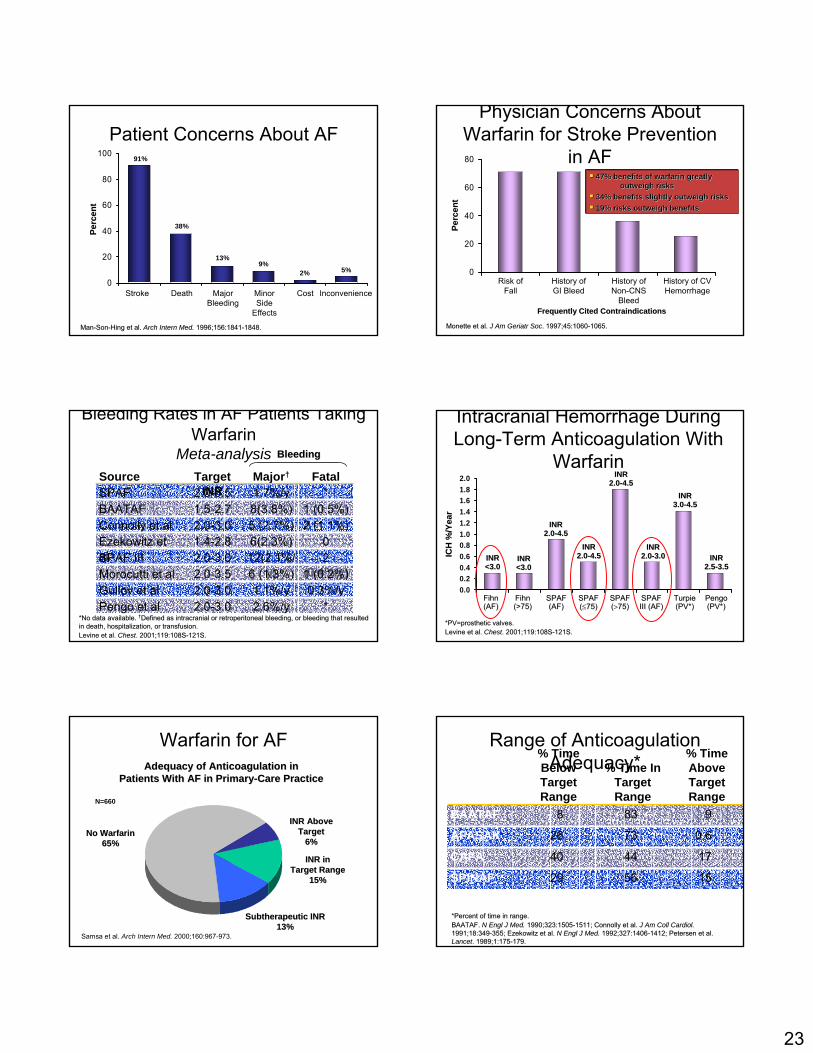
Patient Concerns About AF
0
20
40
60
80
100
Stroke Death Major Bleeding
InconvenienceMinor Side
Effects
Cost
ManMan--SonSon--Hing et al. Hing et al. Arch Intern Med.Arch Intern Med. 1996;156:18411996;156:1841--1848.1848.
Perc
ent
Perc
ent
91%
38%
13%9%
2% 5%
Physician Concerns About Warfarin for Stroke Prevention
in AF
0
20
40
60
80
Risk of Fall
History of GI Bleed
History of Non-CNS
Bleed
History of CV Hemorrhage
Monette et al. Monette et al. J Am Geriatr SocJ Am Geriatr Soc. 1997;45:1060. 1997;45:1060--1065.1065.
47% benefits of warfarin greatly 47% benefits of warfarin greatly outweigh risksoutweigh risks
34% benefits slightly outweigh risks34% benefits slightly outweigh risks19% risks outweigh benefits19% risks outweigh benefits
Frequently Cited ContraindicationsFrequently Cited Contraindications
Perc
ent
Perc
ent
Bleeding Rates in AF Patients Taking Warfarin
Meta-analysis
2 (0.4%/y)
12(2.1%/y)
2.0-3.0SPAF III
*2.6%/y2.0-3.0Pengo et al0.3%/y1.1%/y2.0-3.0Gullov et al
1 (0.2%)6 (1.3%)2.0-3.5Morocutti et al
06(2.3%)1.4-2.8Ezekowitz et al
2 (1.1%)5 (2.7%)2.0-3.0Connolly et al1 (0.5%)8(3.8%)1.5-2.7BAATAF
*1.7%/y2.0-3.5SPAFFatalMajor†Target
INRSource
*No data available. *No data available. ††Defined as intracranial or retroperitoneal bleeding, or bleedingDefined as intracranial or retroperitoneal bleeding, or bleeding that resulted that resulted in death, hospitalization, or transfusion.in death, hospitalization, or transfusion.Levine et al. Levine et al. ChestChest. 2001;119:108S. 2001;119:108S--121S.121S.
BleedingBleeding
0.00.20.40.60.81.01.21.41.61.82.0
Intracranial Hemorrhage During Long-Term Anticoagulation With
Warfarin
*PV=prosthetic valves.*PV=prosthetic valves.Levine et al. Levine et al. ChestChest. 2001;119:108S. 2001;119:108S--121S.121S.
ICH
%/Y
ear
ICH
%/Y
ear
Fihn Fihn (AF)(AF)
INRINR<3.0<3.0
INRINR<3.0<3.0
Fihn Fihn (>75)(>75)
Turpie Turpie (PV*)(PV*)
SPAF SPAF ((≤≤75)75)
SPAF SPAF (AF)(AF)
PengoPengo(PV*)(PV*)
SPAF SPAF ((>>75)75)
SPAF SPAF III (AF)III (AF)
INRINR2.02.0--4.54.5
INRINR2.02.0--3.03.0 INRINR
2.52.5--3.53.5
INRINR3.03.0--4.54.5
INRINR2.02.0--4.54.5
INRINR2.02.0--4.54.5
Warfarin for AF
Samsa et al. Arch Intern Med. 2000;160:967-973.
INR Above INR Above TargetTarget
6%6%
Subtherapeutic INR Subtherapeutic INR 13%13%
INR inINR inTarget RangeTarget Range
15%15%
No WarfarinNo Warfarin65%65%
Adequacy of Anticoagulation inAdequacy of Anticoagulation inPatients With AF in PrimaryPatients With AF in Primary--Care PracticeCare Practice
N=660
174440CAFA
155629SPINAF
0.67326AFASAK
9838BAATAF
% Time Above Target Range
% Time In Target Range
% Time Below Target Range
Range of Anticoagulation Adequacy*
*Percent of time in range.*Percent of time in range.BAATAF. BAATAF. N Engl J Med.N Engl J Med. 1990;323:15051990;323:1505--1511; Connolly et al. 1511; Connolly et al. J Am Coll Cardiol.J Am Coll Cardiol.1991;18:3491991;18:349--355; Ezekowitz et al. 355; Ezekowitz et al. N Engl J Med.N Engl J Med. 1992;327:14061992;327:1406--1412; Petersen et al. 1412; Petersen et al. LancetLancet. 1989;1:175. 1989;1:175--179.179.
24
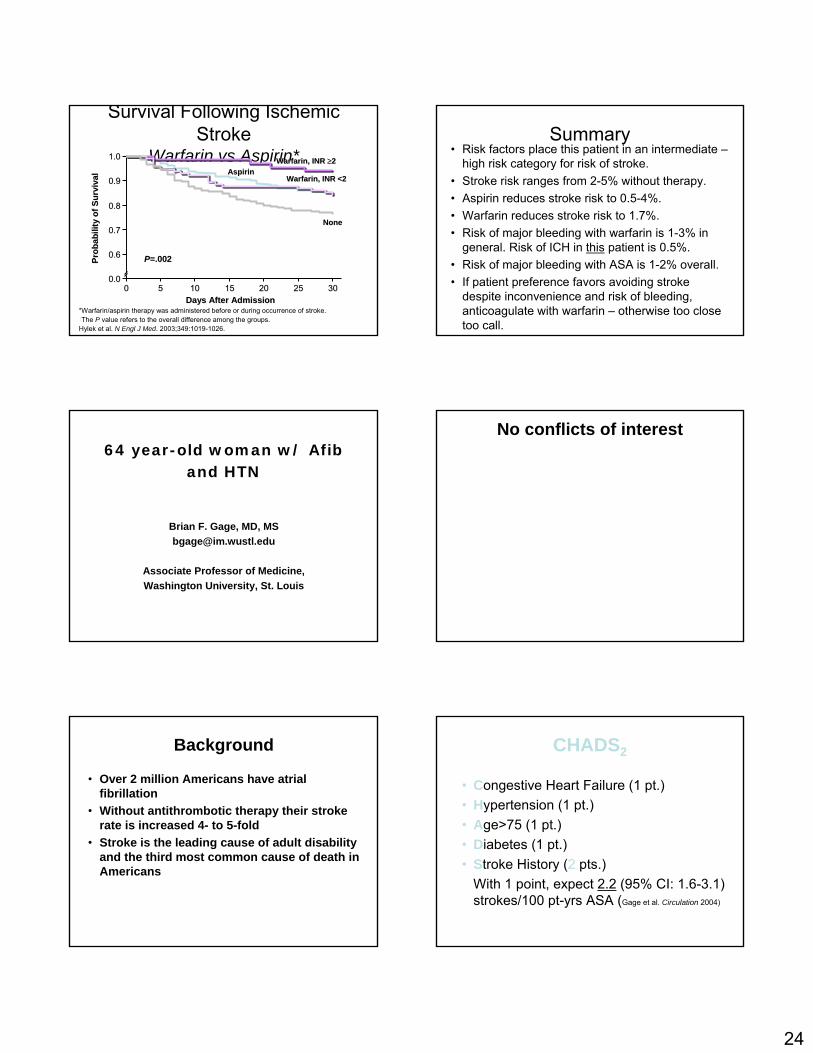
Survival Following Ischemic Stroke
Warfarin vs Aspirin*
Prob
abili
ty o
f Sur
viva
lPr
obab
ility
of S
urvi
val
1.01.0
0.90.9
0.80.8
0.70.7
0.60.6
0.00.000 55 1010 1515 2020 2525 3030
Days After AdmissionDays After Admission
PP=.002=.002††
Warfarin, INR Warfarin, INR ≥≥22AspirinAspirin
Warfarin, INR Warfarin, INR <2<2
NoneNone
*Warfarin/aspirin therapy was administered before or during occurrence of stroke.††The P value refers to the overall difference among the groups.Hylek et al. N Engl J Med. 2003;349:1019-1026.
Summary• Risk factors place this patient in an intermediate –
high risk category for risk of stroke.• Stroke risk ranges from 2-5% without therapy.• Aspirin reduces stroke risk to 0.5-4%.• Warfarin reduces stroke risk to 1.7%.• Risk of major bleeding with warfarin is 1-3% in
general. Risk of ICH in this patient is 0.5%. • Risk of major bleeding with ASA is 1-2% overall.• If patient preference favors avoiding stroke
despite inconvenience and risk of bleeding, anticoagulate with warfarin – otherwise too close too call.
64 year-old woman w/ Afib and HTN
Brian F. Gage, MD, [email protected]
Associate Professor of Medicine,Washington University, St. Louis
No conflicts of interest
Background
• Over 2 million Americans have atrial fibrillation
• Without antithrombotic therapy their stroke rate is increased 4- to 5-fold
• Stroke is the leading cause of adult disability and the third most common cause of death in Americans
CHADS2
• Congestive Heart Failure (1 pt.)• Hypertension (1 pt.)• Age>75 (1 pt.)• Diabetes (1 pt.)• Stroke History (2 pts.)
With 1 point, expect 2.2 (95% CI: 1.6-3.1) strokes/100 pt-yrs ASA (Gage et al. Circulation 2004)
25
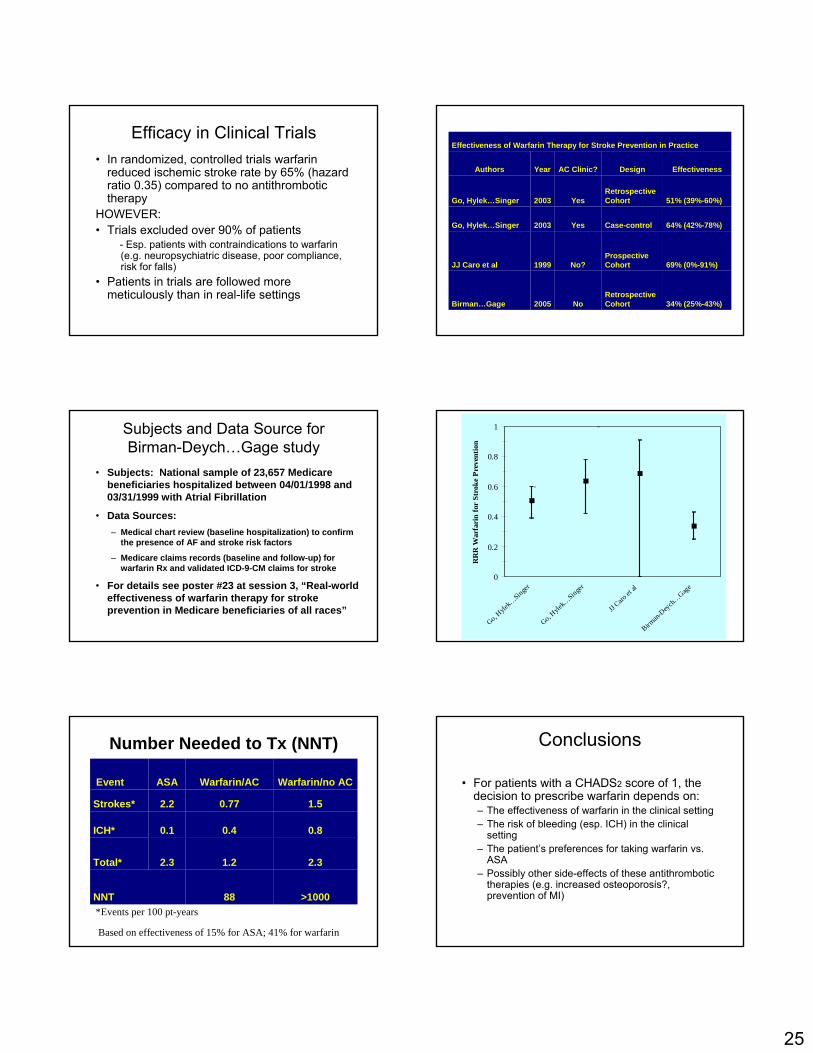
Efficacy in Clinical Trials• In randomized, controlled trials warfarin
reduced ischemic stroke rate by 65% (hazard ratio 0.35) compared to no antithrombotic therapy
HOWEVER: • Trials excluded over 90% of patients
- Esp. patients with contraindications to warfarin (e.g. neuropsychiatric disease, poor compliance, risk for falls)
• Patients in trials are followed more meticulously than in real-life settings
34% (25%-43%)Retrospective CohortNo2005Birman…Gage
69% (0%-91%)Prospective CohortNo?1999JJ Caro et al
64% (42%-78%)Case-controlYes2003Go, Hylek…Singer
51% (39%-60%)Retrospective CohortYes2003Go, Hylek…Singer
EffectivenessDesignAC Clinic?YearAuthors
Effectiveness of Warfarin Therapy for Stroke Prevention in Practice
Subjects and Data Source for Birman-Deych…Gage study
• Subjects: National sample of 23,657 Medicare beneficiaries hospitalized between 04/01/1998 and 03/31/1999 with Atrial Fibrillation
• Data Sources:– Medical chart review (baseline hospitalization) to confirm
the presence of AF and stroke risk factors
– Medicare claims records (baseline and follow-up) for warfarin Rx and validated ICD-9-CM claims for stroke
• For details see poster #23 at session 3, “Real-world effectiveness of warfarin therapy for stroke prevention in Medicare beneficiaries of all races”
0
0.2
0.4
0.6
0.8
1
Go, Hyle
k…Singer
Go, Hyle
k…Singer
JJ Caro
et al
Birman-
Deych…Gage
RR
R W
arfa
rin
for
Stro
ke P
reve
ntio
n
>100088NNT
2.31.22.3Total*
0.80.40.1ICH*
1.50.772.2Strokes*
Warfarin/no ACWarfarin/ACASAEvent
*Events per 100 pt-years
Number Needed to Tx (NNT)
Based on effectiveness of 15% for ASA; 41% for warfarin
Conclusions
• For patients with a CHADS2 score of 1, the decision to prescribe warfarin depends on:– The effectiveness of warfarin in the clinical setting– The risk of bleeding (esp. ICH) in the clinical
setting– The patient’s preferences for taking warfarin vs.
ASA– Possibly other side-effects of these antithrombotic
therapies (e.g. increased osteoporosis?, prevention of MI)
Arguments Against the Prolonged Out-of-Hospital Prophylaxis for ALL Patients with Total Hip Arthroplasty (THA)
One size does not fit all: There is a range of potential risk from relatively low to very high post-discharge
o Unfortunately there is no well-validated method to predict reliably who will have a VTE event There are ~300,000 THA procedures performed annually in the US, so What is the rate of Symptomatic VTE after hospitalization for THA without extended prophylaxis?
• White et al, Arch Int Med 1998: 2-3% at 30-90 days1 • Heit et al, Ann Int Med June 2000: 2.2% at 120 days2 • Comp et al, JBJS 2001: 3.8% at 120 days3 • Eikelboom et al, Lancet July 2001 Meta-analysis4
o Symptomatic VTE rate from 9 studies 3.3% in controls (58/1,744) o 1.3% in treatment groups (12/1,954)
ARR = 2.0% NNT = 50 (PE NNT = 250) O.R. 0.38 (.24-.61)
What is the rate of HIT and Major Bleeding?
• Warkentin et al Arch Int Med 20035 (<50% fall in plt count from post-operative peak) 0.6% with LMWH in orthopedic patients
• Major Bleeding rate (transfusion, wound hematoma requiring surgery, etc) 0.2-1.4% (best guess is ~0.5%)
• Combined HIT and Major Bleeding Rate of ~1.0% Balancing reductions in symptomatic events with adverse events, the overall ARR with out of hospital LMWH prophylaxis will be ~1.0%. Patient Compliance Issues In one of the first studies to suggest out-of-hospital LMWH prophylaxis was effective in THA6, injections were administered by a study nurse, ensuring compliance. In a follow-up LMWH trial2, patients self-administered and were included if they received at least 50% of their injections, which is more reflective of actual clinical practice. My Approach: All patients get prophylaxis of surgeon’s choice at the time of THA, preferably multi-modal
• LMWH for most patients without contraindication and who agree to out-of-hospital injections if needed (considering both cost and convenience)
• Warfarin for patients who would prefer out of hospital prophylaxis with pills and blood tests, if out of hospital prophylaxis warranted.
• Pneumatic devices intra-op and post-op until ambulatory7 • TED hose, if they fit properly, during hospitalization and 4 weeks after discharge8 • ASA in hospital and at discharge for 4 weeks if no warfarin or LMWH, since ASA has been
shown to reduce the rate of fatal PE.9 • Prolonged out of hospital prophylaxis only for those who are at the highest risk based upon risk
factors. Unfortunately, there is no validated way to predict who is at this highest risk because the number of out of hospital VTE events is very small and would take an extremely large study, or a very well-done administrative data study.
• More studies are needed to determine cost-effectiveness and clinical effectiveness
Peter Kaboli, MD, MS [email protected] Iowa City VAMC and University of Iowa
References: 1. White RH, Romano PS, Zhou H, Rodrigo J, Bargar W. Incidence and time course of
thromboembolic outcomes following total hip or knee arthroplasty. Arch Intern Med 1998; 158:1525-31.
2. Heit JA, Elliott CG, Trowbridge AA, Morrey BF, Gent M, Hirsh J. Ardeparin sodium for extended out-of-hospital prophylaxis against venous thromboembolism after total hip or knee replacement. A randomized, double-blind, placebo-controlled trial. Annals of Internal Medicine 2000; 132:853-61.
3. Comp PC, Spiro TE, Friedman RJ, et al. Prolonged enoxaparin therapy to prevent venous thromboembolism after primary hip or knee replacement. Enoxaparin Clinical Trial Group. Patient Care Management 2001; 83-A:336-45.
4. Eikelboom JW, Quinlan DJ, Douketis JD. Extended-duration prophylaxis against venous thromboembolism after total hip or knee replacement: a meta-analysis of the randomised trials. Lancet 2001; 358:9-15.
5. Warkentin TE, Roberts RS, Hirsh J, Kelton JG. An improved definition of immune heparin-induced thrombocytopenia in postoperative orthopedic patients. Archives of Internal Medicine 2003; 163:2518-24.
6. Bergqvist D, Benoni G, Bjorgell O, et al. Low-molecular-weight heparin (enoxaparin) as prophylaxis against venous thromboembolism after total hip replacement. New England Journal of Medicine 1996; 335:696-700.
7. Silbersack Y, Taute BM, Hein W, Podhaisky H. Prevention of deep-vein thrombosis after total hip and knee replacement. Low-molecular-weight heparin in combination with intermittent pneumatic compression. Journal of Bone & Joint Surgery - British Volume 2004; 86:809-12.
8. Best AJ, Williams S, Crozier A, Bhatt R, Gregg PJ, Hui AC. Graded compression stockings in elective orthopaedic surgery. An assessment of the in vivo performance of commercially available stockings in patients having hip and knee arthroplasty. Journal of Bone & Joint Surgery - British Volume 2000; 82:116-8.
9. Anonymous. Prevention of pulmonary embolism and deep vein thrombosis with low dose aspirin: Pulmonary Embolism Prevention (PEP) trial. Lancet 2000; 355:1295-302.
Peter Kaboli, MD, MS [email protected] Iowa City VAMC and University of Iowa

Richard H. White, MD UC Davis Q: How long should prophylaxis be used in patients undergoing hip replacement surgery or other high risk surgical procedures?-
The case for extended prophylaxis. ____________________________________________________________________________ Before one can make a rational decision, you have to ask: What is the incidence and timing of thromboembolic events after surgery? REF 1 White RH, Romano PS, Zhou H, Rodrigo J, Bargar W. Incidence and time course of thromboembolic outcomes following total hip or knee arthroplasty. Arch Intern Med. 1998 Jul 27;158(14):1525-31.
Outcome
Primary Total Hip (N=19,586)
Thromboembolic event by time of diagnosis:
During the initial hospitalization, n (%) 133 (0.7%)
During rehabilitation hospitalization, n (%) 94 (0.5%)
Requiring readmission, n (%) 329 (1.7%)†
P<0.01 Over 50% of all VTE events in the first 90 days occurred after discharge!
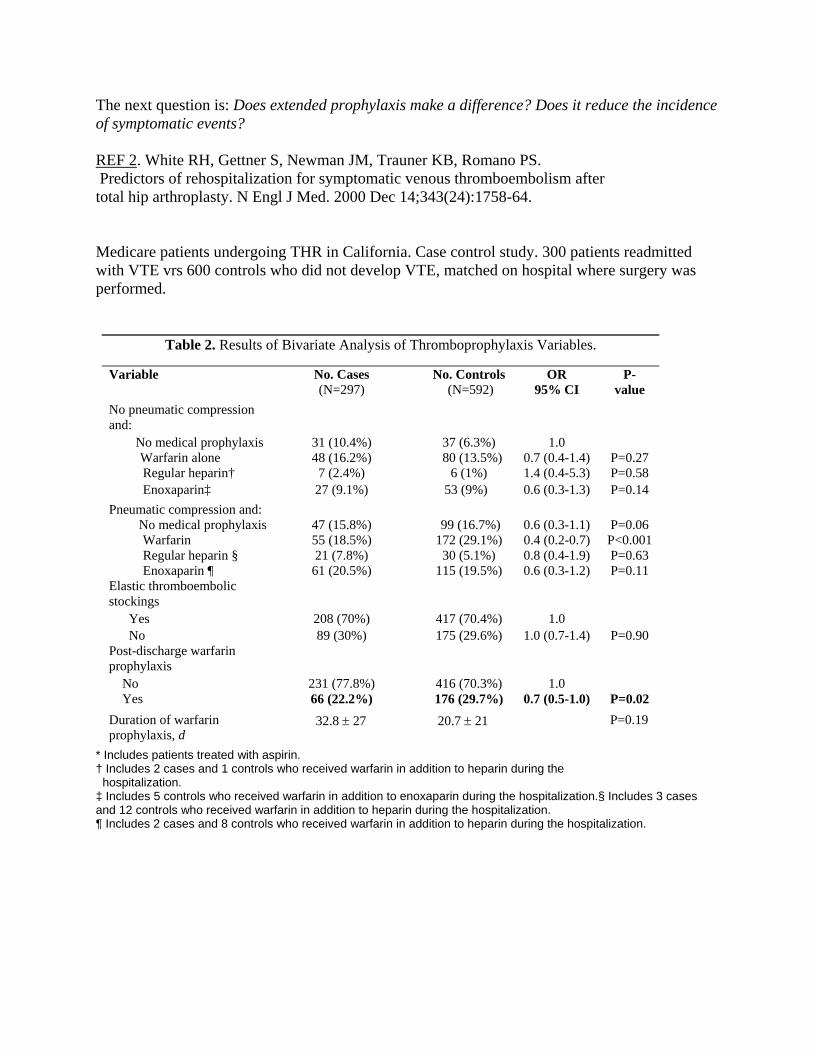
The next question is: Does extended prophylaxis make a difference? Does it reduce the incidence
EF 2
of symptomatic events? R . White RH, Gettner S, Newman JM, Trauner KB, Romano PS.
sm after
edicare patients undergoing THR in California. Case control study. 300 patients readmitted
Table 2. Results of Bivariate Analysis of Thromboprophylaxis Variables.
Predictors of rehospitalization for symptomatic venous thromboembolitotal hip arthroplasty. N Engl J Med. 2000 Dec 14;343(24):1758-64. Mwith VTE vrs 600 controls who did not develop VTE, matched on hospital where surgery was performed.
Variable No95
P- v
. Cases No. Controls OR (N=297) (N=592) % CI alue
No pneumatic compression
o medical prophylaxis 31 (10.4%) 37 (6.3%) 1.0 0.7 ( .4) P= 27
† 5
Pneum ion and: 47 (1 8%) 99 (1 .7%) 0.6 (0 -1.1) P= 06
parin §
Elasti lic
208 (70%) 417 (70.4%) 1.0 1.0 ( .4) P= 90
charge warfarin
231 (77.8%) 416 (70.3%) 1.0 0.7 ( .0) P=0.02
rfarin
* treated with aspirin. eceived warfarin in addition to heparin during the
tion.§ Includes 3 cases
and: N
Warfarin alone 48 (16.2%) 80 (13.5%) 0.4-1 0.Regular heparin 7 (2.4%) 6 (1%) 1.4 (0.4-5.3) P=0.58 Enoxaparin‡ 27 (9.1%) 3 (9%) 0.6 (0.3-1.3) P=0.14 atic compress
No medical prophylaxis 5. 6 .3 0.Warfarin 55 (18.5%) 172 (29.1%) 0.4 (0.2-0.7) P<0.001 Regular he 21 (7.8%) 30 (5.1%)
10.8 (0.4-1.9) P=0.63
Enoxaparin ¶ 61 (20.5%) 15 (19.5%) 0.6 (0.3-1.2) P=0.11 c thromboembo
stockings Yes
No 89 (30%) 175 (29.6%) 0.7-1 0.Post-disprophylaxis No
Yes 66 (22.2%) 176 (29.7%) 0.5-1Duration of waprophylaxis, d
Includes patients
32.8 ± 27 20.7 ± 21 P=0.19
† Includes 2 cases and 1 controls who r hospitalization.
ols who received warfarin in addition to enoxaparin during the hospitaliza‡ Includes 5 contrand 12 controls who received warfarin in addition to heparin during the hospitalization. ¶ Includes 2 cases and 8 controls who received warfarin in addition to heparin during the hospitalization.
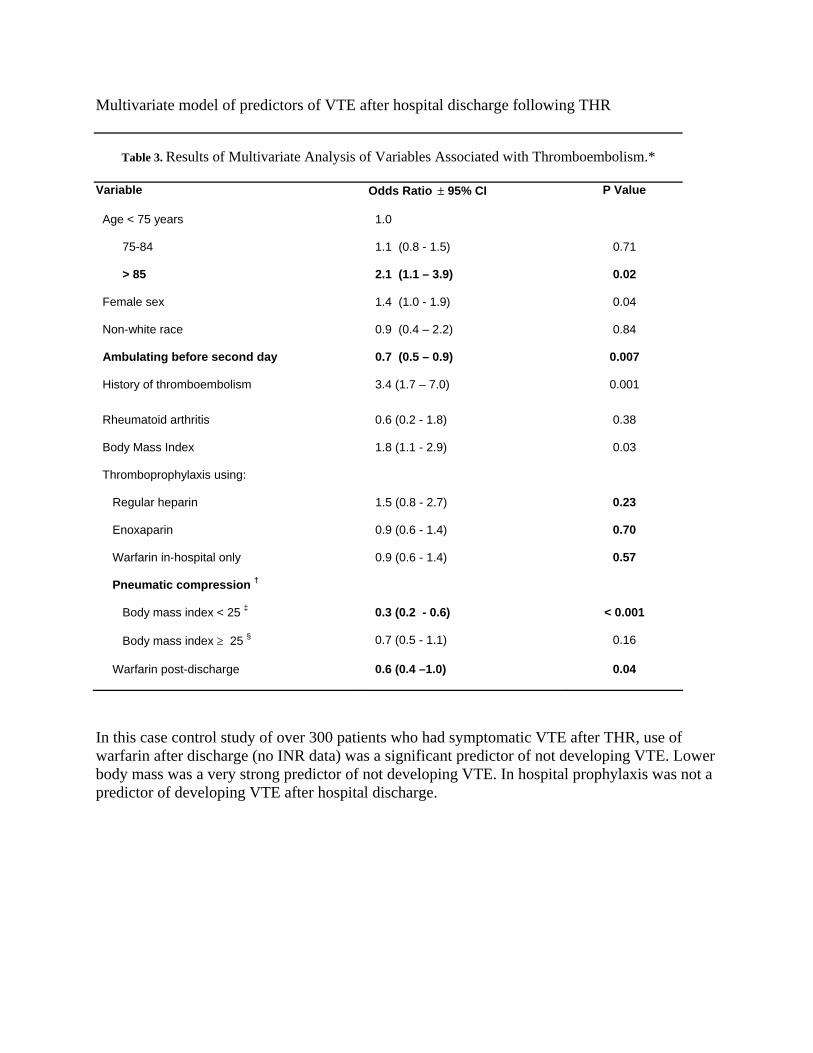
Multivariate model of predictors of VTE after hospital discharge following THR
Table 3. Results of Multivariate Analysis of Variables Associated with Thromboembolism.*
Variable Odds Ratio ± 95% CI P Value
Age < 75 years 1.0
75-84 1.1 (0.8 - 1.5) 0.71
> 85 2.1 (1.1 – 3.9) 0.02
Female sex 1.4 (1.0 - 1.9) 0.04
Non-white race 0.9 (0.4 – 2.2) 0.84
Ambulating before second day 0.7 (0.5 – 0.9) 0.007
History of thromboembolism 3.4 (1.7 – 7.0) 0.001
Rheumatoid arthritis 0.6 (0.2 - 1.8) 0.38
Body Mass Index 1.8 (1.1 - 2.9) 0.03
Thromboprophylaxis using:
Regular heparin 1.5 (0.8 - 2.7) 0.23
Enoxaparin 0.9 (0.6 - 1.4) 0.70
Warfarin in-hospital only 0.9 (0.6 - 1.4) 0.57
Pneumatic compression †
Body mass index < 25 ‡ 0.3 (0.2 - 0.6) < 0.001
Body mass index ≥ 25 § 0.7 (0.5 - 1.1) 0.16
Warfarin post-discharge 0.6 (0.4 –1.0) 0.04
In this case control study of over 300 patients who had symptomatic VTE after THR, use of warfarin after discharge (no INR data) was a significant predictor of not developing VTE. Lower body mass was a very strong predictor of not developing VTE. In hospital prophylaxis was not a predictor of developing VTE after hospital discharge.
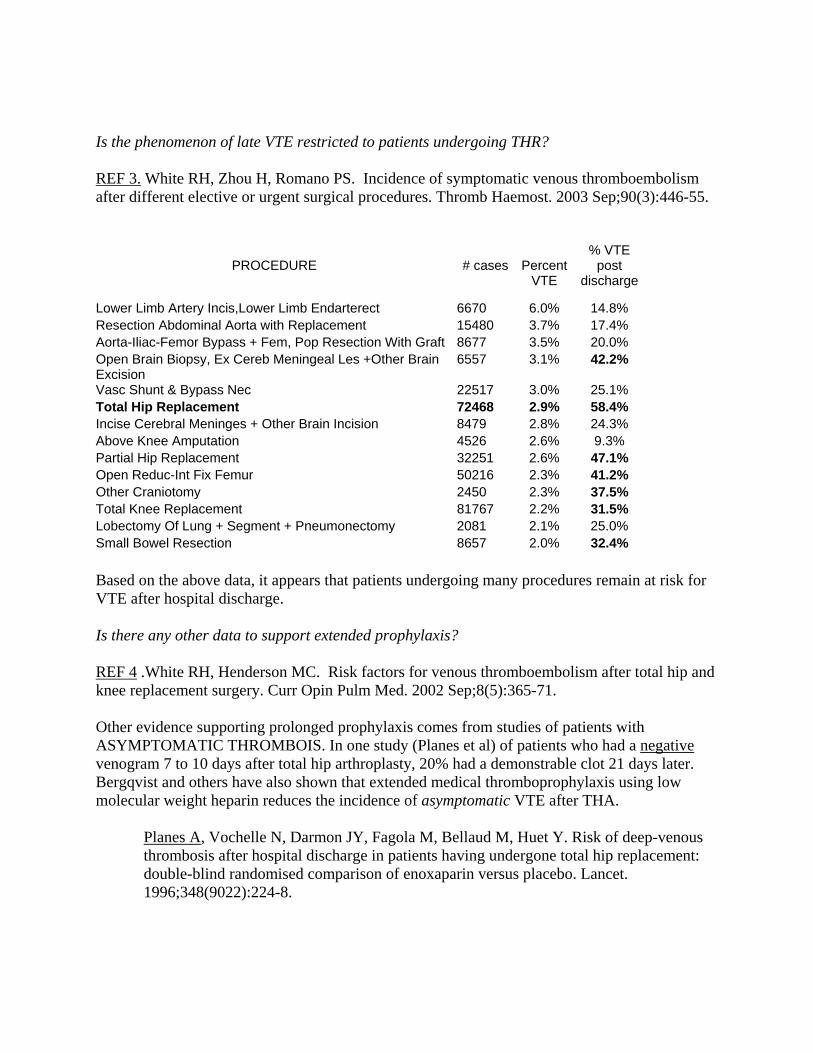
Is the phenomenon of late VTE restricted to patients undergoing THR? REF 3. White RH, Zhou H, Romano PS. Incidence of symptomatic venous thromboembolism after different elective or urgent surgical procedures. Thromb Haemost. 2003 Sep;90(3):446-55.
PROCEDURE
# cases
Percent
VTE
% VTE post
discharge
Lower Limb Artery Incis,Lower Limb Endarterect 6670 6.0% 14.8% Resection Abdominal Aorta with Replacement 15480 3.7% 17.4% Aorta-Iliac-Femor Bypass + Fem, Pop Resection With Graft 8677 3.5% 20.0% Open Brain Biopsy, Ex Cereb Meningeal Les +Other Brain Excision
6557 3.1% 42.2%
Vasc Shunt & Bypass Nec 22517 3.0% 25.1% Total Hip Replacement 72468 2.9% 58.4% Incise Cerebral Meninges + Other Brain Incision 8479 2.8% 24.3% Above Knee Amputation 4526 2.6% 9.3% Partial Hip Replacement 32251 2.6% 47.1% Open Reduc-Int Fix Femur 50216 2.3% 41.2% Other Craniotomy 2450 2.3% 37.5% Total Knee Replacement 81767 2.2% 31.5% Lobectomy Of Lung + Segment + Pneumonectomy 2081 2.1% 25.0% Small Bowel Resection 8657 2.0% 32.4% Based on the above data, it appears that patients undergoing many procedures remain at risk for VTE after hospital discharge. Is there any other data to support extended prophylaxis? REF 4 .White RH, Henderson MC. Risk factors for venous thromboembolism after total hip and knee replacement surgery. Curr Opin Pulm Med. 2002 Sep;8(5):365-71. Other evidence supporting prolonged prophylaxis comes from studies of patients with ASYMPTOMATIC THROMBOIS. In one study (Planes et al) of patients who had a negative venogram 7 to 10 days after total hip arthroplasty, 20% had a demonstrable clot 21 days later. Bergqvist and others have also shown that extended medical thromboprophylaxis using low molecular weight heparin reduces the incidence of asymptomatic VTE after THA.
Planes A, Vochelle N, Darmon JY, Fagola M, Bellaud M, Huet Y. Risk of deep-venous thrombosis after hospital discharge in patients having undergone total hip replacement: double-blind randomised comparison of enoxaparin versus placebo. Lancet. 1996;348(9022):224-8.
Bergqvist D, Benoni G, Bjorgell O, et al. Low-molecular-weight heparin (enoxaparin) as prophylaxis against venous thromboembolism after total hip replacement [see comments]. N Engl J Med. 1996;335(10):696-700.
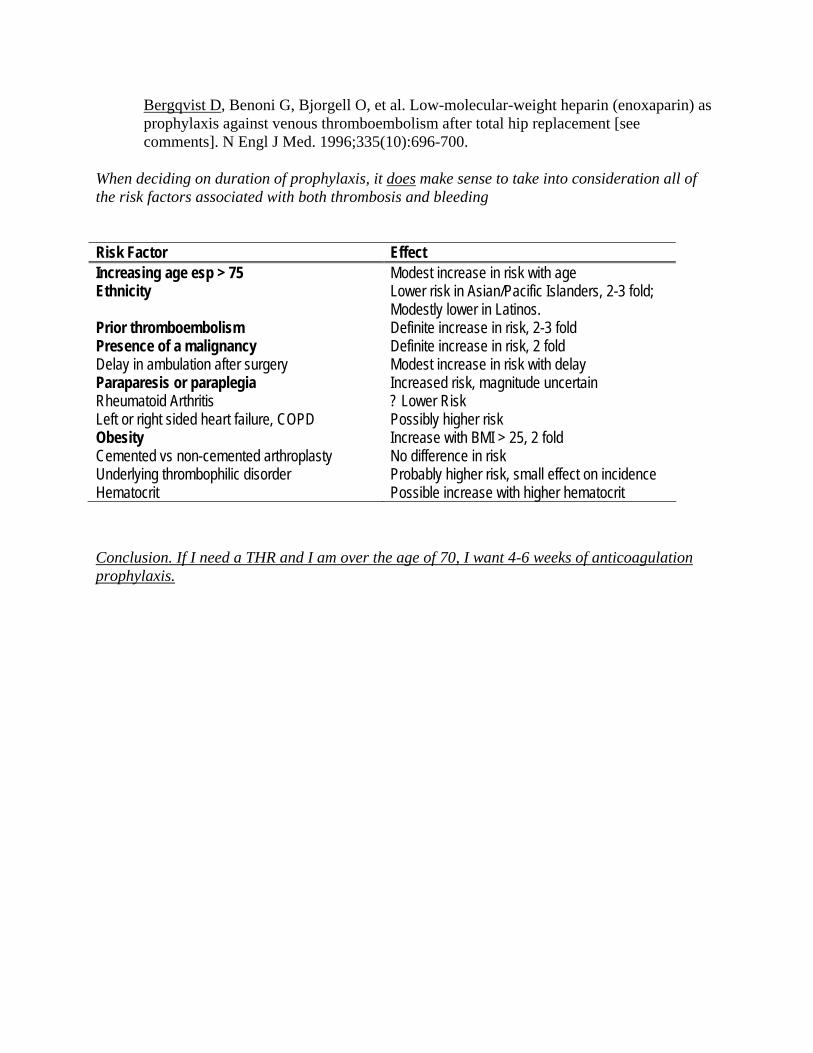
When deciding on duration of prophylaxis, it does make sense to take into consideration all of the risk factors associated with both thrombosis and bleeding Risk Factor Effect Increasing age esp > 75 Modest increase in risk with age Ethnicity Lower risk in Asian/Pacific Islanders, 2-3 fold;
Modestly lower in Latinos. Prior thromboembolism Definite increase in risk, 2-3 fold Presence of a malignancy Definite increase in risk, 2 fold Delay in ambulation after surgery Modest increase in risk with delay Paraparesis or paraplegia Increased risk, magnitude uncertain Rheumatoid Arthritis ? Lower Risk Left or right sided heart failure, COPD Possibly higher risk Obesity Increase with BMI > 25, 2 fold Cemented vs non-cemented arthroplasty No difference in risk Underlying thrombophilic disorder Probably higher risk, small effect on incidence Hematocrit Possible increase with higher hematocrit Conclusion. If I need a THR and I am over the age of 70, I want 4-6 weeks of anticoagulation prophylaxis.
Extended Duration Prophylaxis Extended Duration Prophylaxis after Hip Arthroplastyafter Hip Arthroplasty-- YesYes
RICHARD H. WHITE, MDRICHARD H. WHITE, MDPROFESSOR OF MEDICINEPROFESSOR OF MEDICINEUC DAVISUC DAVIS

Arguments:Arguments:Hospitalization for THA is short (4Hospitalization for THA is short (4--5 days).5 days).Most VTE cases become manifest after hospital Most VTE cases become manifest after hospital discharge.discharge.Asymptomatic VTE can begin very late after Asymptomatic VTE can begin very late after discharge. discharge. Extended prophylaxis is effective.Extended prophylaxis is effective.ImmobilityImmobility--obesity contribute to VTE riskobesity contribute to VTE risk
a reason extended is needed.a reason extended is needed.
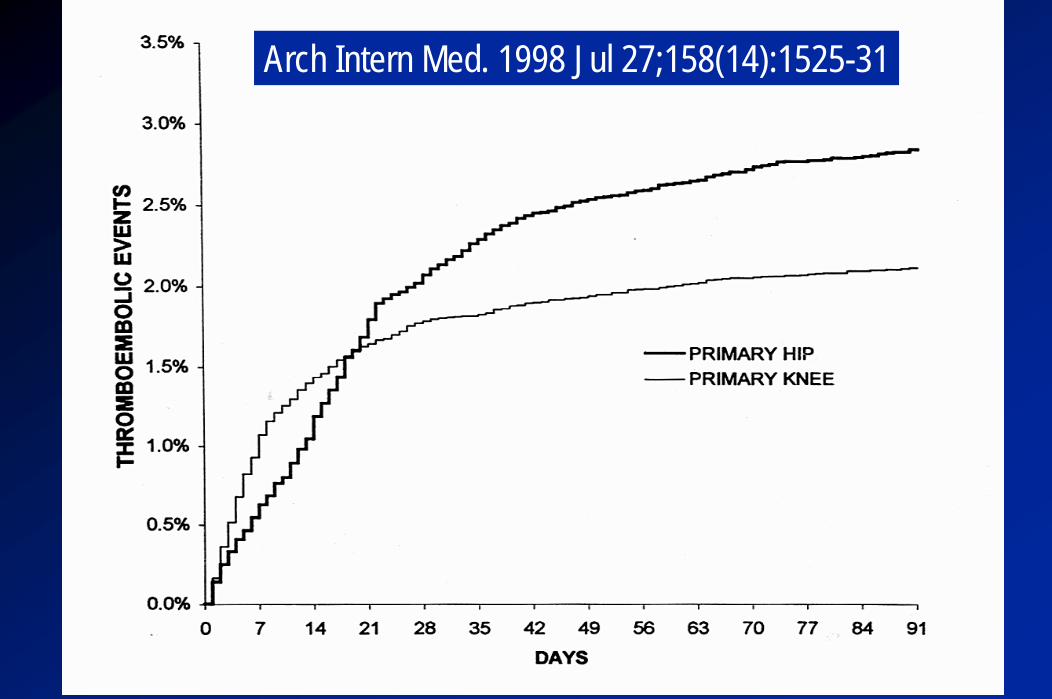
Arch Intern Med. 1998 Jul 27;158(14):1525-31
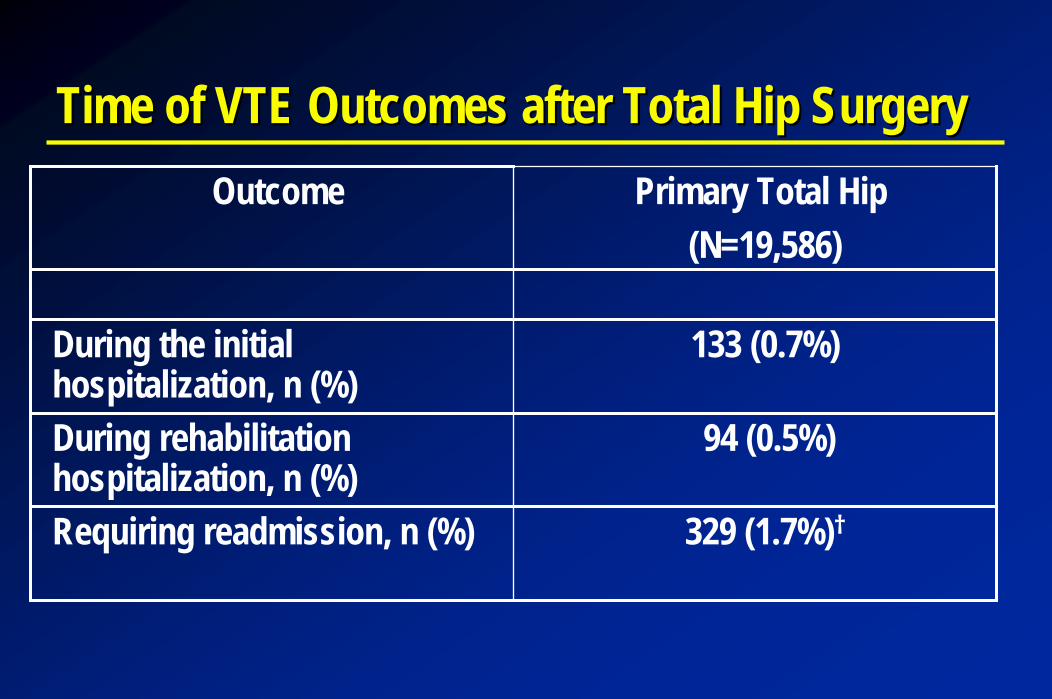
Time of VTE Outcomes after Total Hip SurgeryTime of VTE Outcomes after Total Hip SurgeryOutcome Primary Total Hip
(N=19,586)
During the initial hospitalization, n (%)
133 (0.7%)
During rehabilitation hospitalization, n (%)
94 (0.5%)
Requiring readmission, n (%) 329 (1.7%)†
Thrombosis can Begin Late after DischargeThrombosis can Begin Late after Discharge
Planes A, et al. Lancet. 1996;348(9022): 224-8.
Among patients who had a negative venogram 7 to 10 days after total hip arthroplasty,
20% had a demonstrable clot 21 days later.
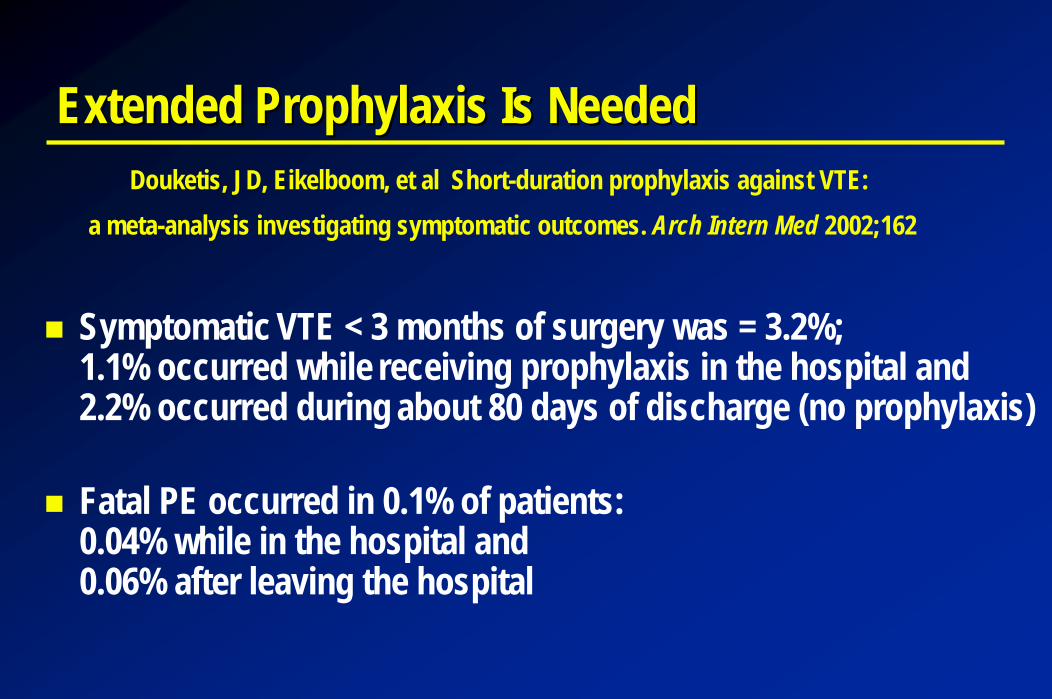
Extended Prophylaxis Is NeededExtended Prophylaxis Is NeededDouketis, JD, Eikelboom, et al Short-duration prophylaxis against VTE:
a meta-analysis investigating symptomatic outcomes. Arch Intern Med 2002;162
Symptomatic VTE < 3 months of surgery was = 3.2%; 1.1% occurred while receiving prophylaxis in the hospital and 2.2% occurred during about 80 days of discharge (no prophylaxis)
Fatal PE occurred in 0.1% of patients:0.04% while in the hospital and 0.06% after leaving the hospital
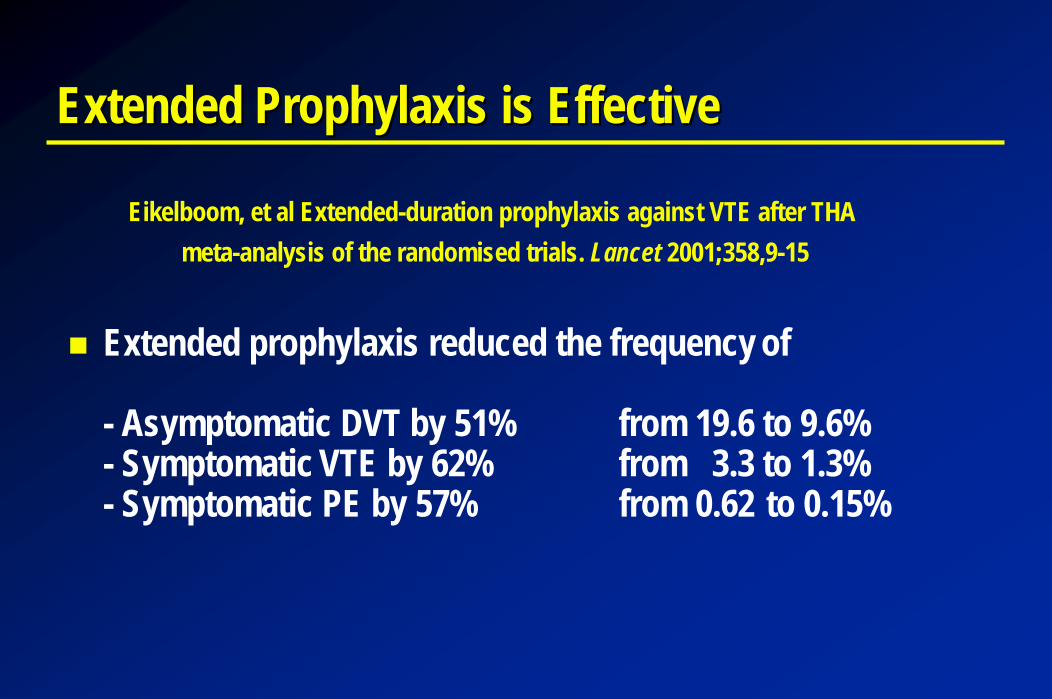
Extended Prophylaxis is EffectiveExtended Prophylaxis is Effective
Eikelboom, et al Extended-duration prophylaxis against VTE after THAmeta-analysis of the randomised trials. Lancet 2001;358,9-15
Extended prophylaxis reduced the frequency of
- Asymptomatic DVT by 51% from 19.6 to 9.6% - Symptomatic VTE by 62% from 3.3 to 1.3%- Symptomatic PE by 57% from 0.62 to 0.15%
Conclusions Regarding Extended ProphylaxisConclusions Regarding Extended Prophylaxis
Kearon. Chest. 2003;124:386S-392S
An additional 3 weeks of LMWH therapy after the first 7 to 10 days of prophylaxis will reduce the frequency of symptomatic VTE by close to two thirds after major orthopedic surgery, such as THA.
Indirect evidence suggests that, compared with LMWH, efficacy of extended prophylaxis after hip replacement is greater with fondaparinux, similar with warfarin, and less with aspirin.
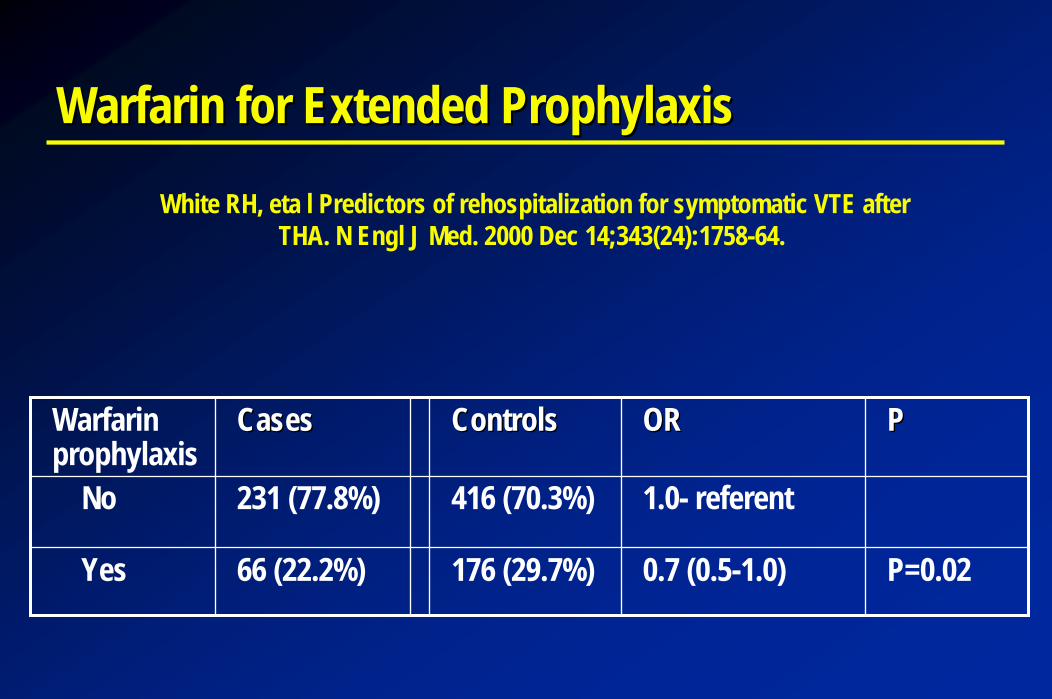
Warfarin for Extended ProphylaxisWarfarin for Extended Prophylaxis
White RH, eta l Predictors of rehospitalization for symptomatic VTE afterTHA. N Engl J Med. 2000 Dec 14;343(24):1758-64.
Warfarin prophylaxis
CasesCases ControlsControls OROR PP
No 231 (77.8%) 416 (70.3%) 1.0- referent
Yes 66 (22.2%) 176 (29.7%) 0.7 (0.5-1.0) P=0.02
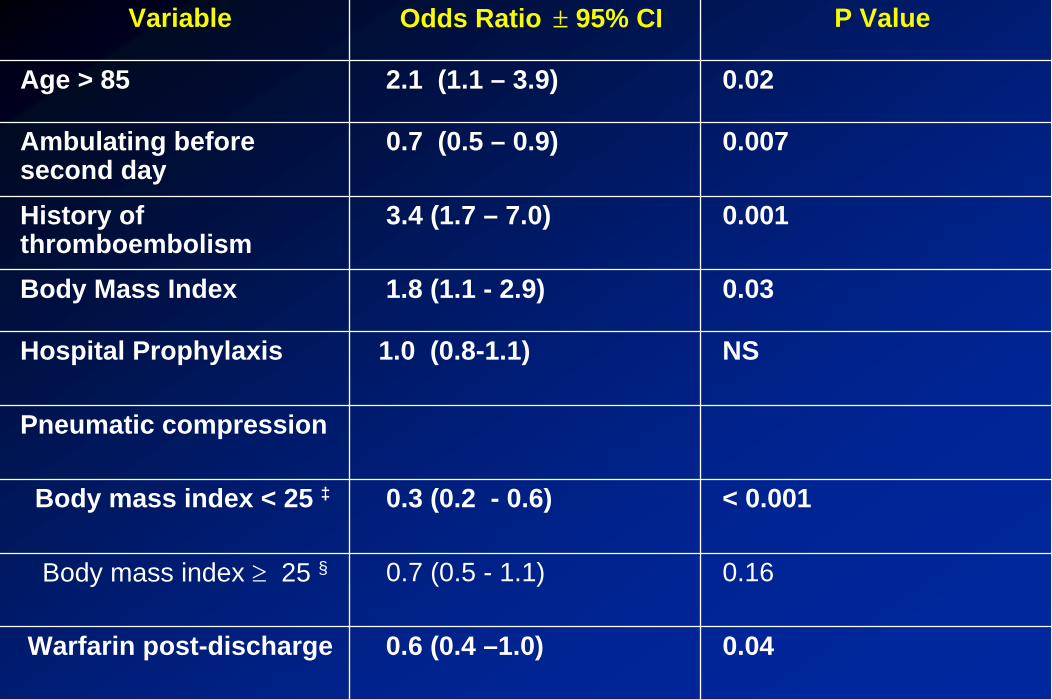
Variable Odds Ratio ± 95% CI P Value
Age > 85 2.1 (1.1 – 3.9) 0.02
Ambulating before second day
0.7 (0.5 – 0.9) 0.007
History of thromboembolism
3.4 (1.7 – 7.0) 0.001
Body Mass Index 1.8 (1.1 - 2.9) 0.03
Hospital Prophylaxis 1.0 (0.8-1.1) NS
Pneumatic compression
Body mass index < 25 ‡ 0.3 (0.2 - 0.6) < 0.001
Body mass index ≥ 25 § 0.7 (0.5 - 1.1) 0.16
Warfarin post-discharge 0.6 (0.4 –1.0) 0.04
Conclusions:Conclusions:
To reduce the incidence of VTE, extended To reduce the incidence of VTE, extended prophylaxis is needed for the majority of patients prophylaxis is needed for the majority of patients undergoing THA.undergoing THA.
Extended prophylaxis (4Extended prophylaxis (4--6 weeks) is effective.6 weeks) is effective.
We need studies to better define patients at highWe need studies to better define patients at high--risk risk for VTE, which likely include patients with prior VTE, for VTE, which likely include patients with prior VTE, immobilityimmobility--obesity and advanced age.obesity and advanced age.

Thrombolysis in Submassive Pulmonary Embolism
Tracy Minichiello, M.D.Assistant Professor of Medicine
Director, UCSF Thrombosis & Anticoagulation ServicesDepartment of Medicine
University of California, San Francisco
Mortality in Pulmonary Embolism
Case fatality rate of PE 15% at 3 months despite standard thearpyIn-hospital mortality 30% in patients with hemodynamic instability
Goldhaber Lancet 1999; Kasper J AM Coll Cardiol 1997
Thrombolysis and Massive Pulmonary Embolism
Established treatment for massive PE Recent meta-analysis supports use of thrombolysis in patients with hemodynamic instability
Wan Circulation 2004
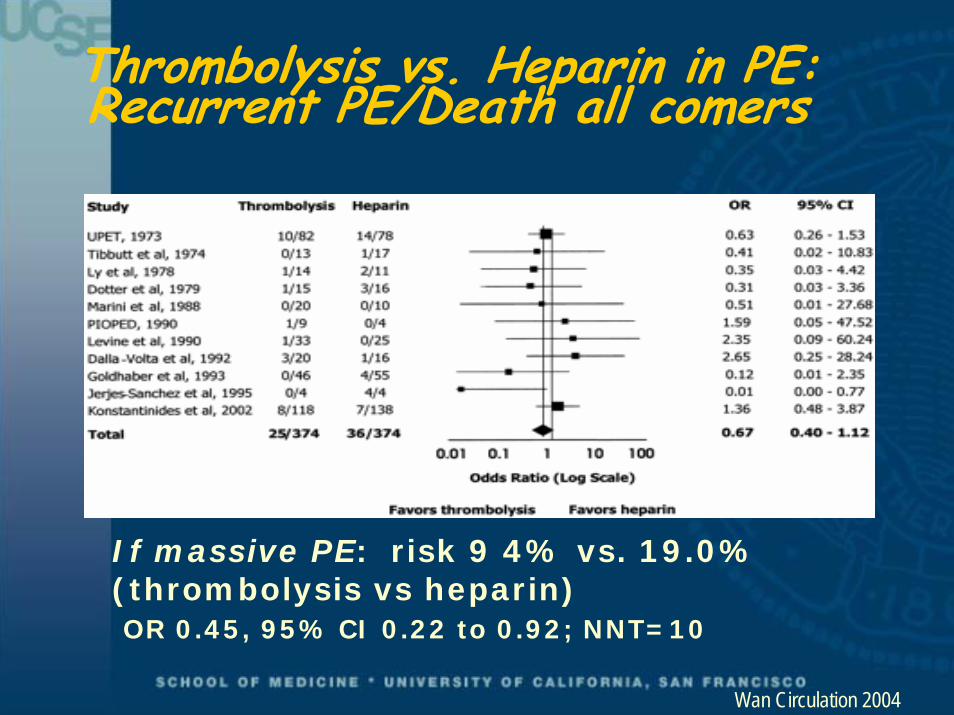
Thrombolysis vs. Heparin in PE: Recurrent PE/Death all comers
If massive PE: risk 9 4% vs. 19.0% (thrombolysis vs heparin)OR 0.45, 95% CI 0.22 to 0.92; NNT=10
Wan Circulation 2004
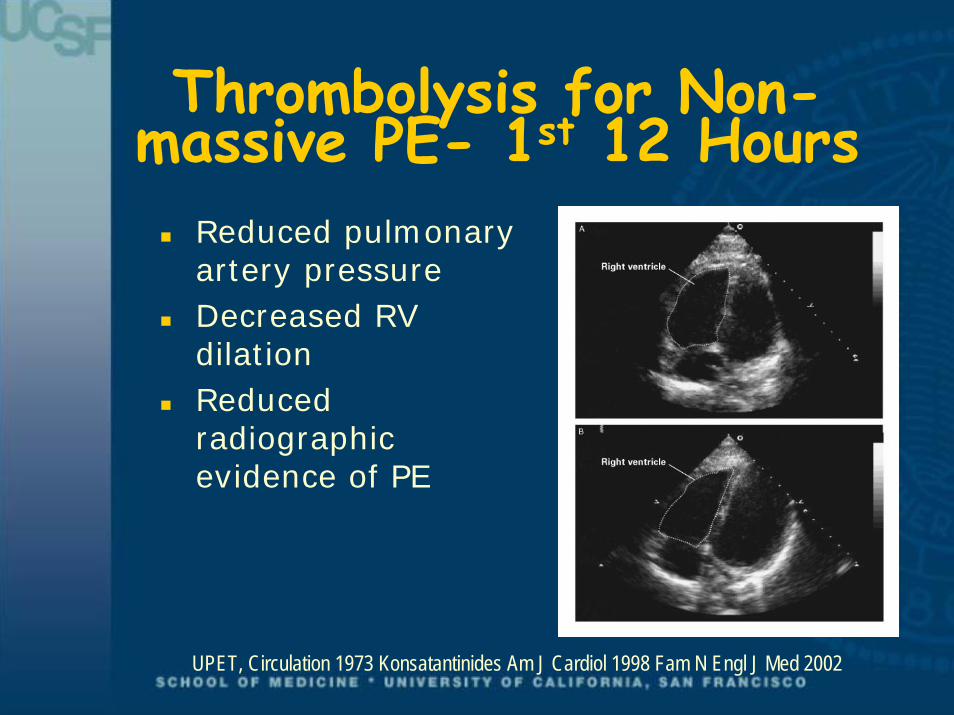
Thrombolysis for Non-massive PE- 1st 12 Hours
Reduced pulmonary artery pressureDecreased RV dilationReduced radiographic evidence of PE
UPET, Circulation 1973 Konsatantinides Am J Cardiol 1998 Fam N Engl J Med 2002
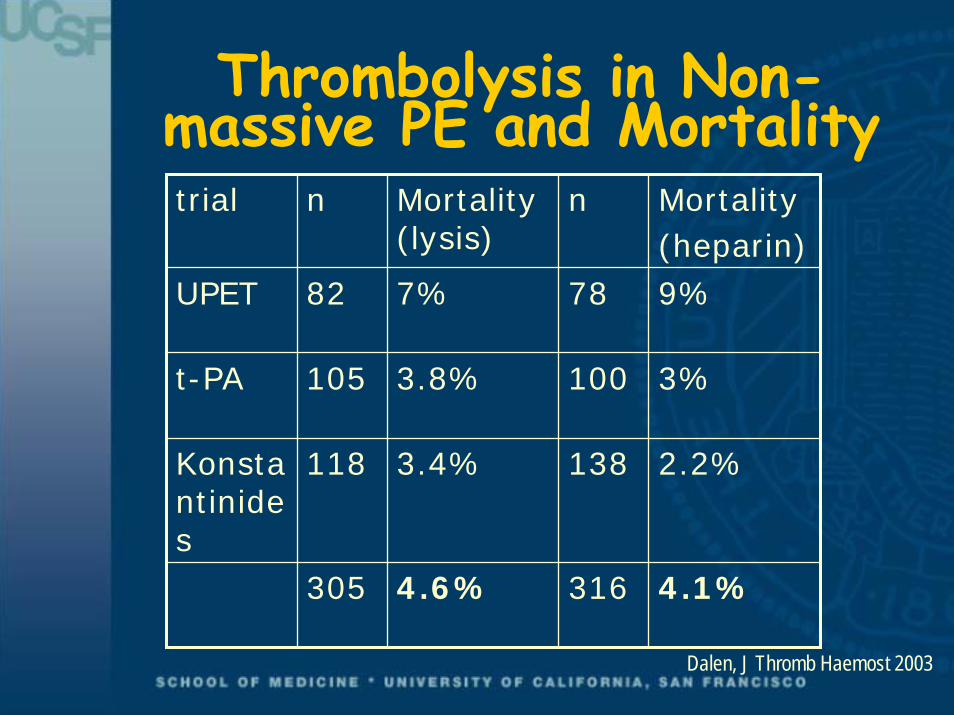
Thrombolysis in Non-massive PE and Mortalitytrial n Mortality
(lysis)n Mortality
(heparin)UPET 82 7% 78 9%
t-PA 105 3.8% 100 3%
Konstantinides
118 3.4% 138 2.2%
305 4.6% 316 4.1%
Dalen, J Thromb Haemost 2003
Predictors of Poor Long Term Outcome in PE
PA systolic pressure > 50mm HGEcho evidence of RV dysfunction/dilation>30% obstruction of pulmonary vascular Elevated BNPIncreased troponin
Liu, Chin Med J 2003

BNP Levels According to Clinical Outcome
Kucher N et al Circulation 2003
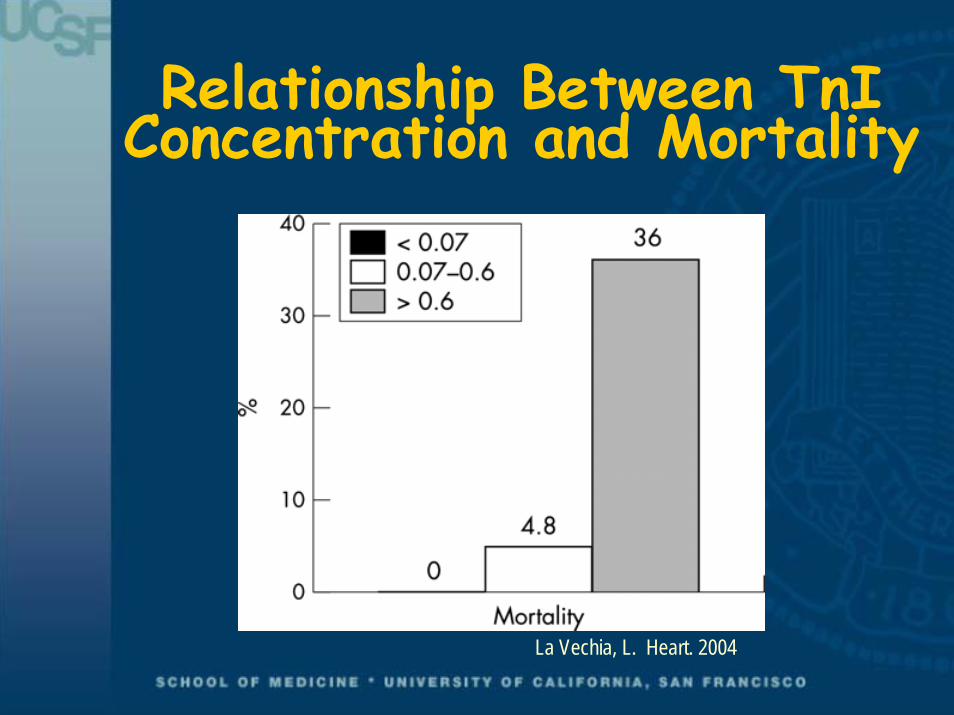
Relationship Between TnIConcentration and Mortality
La Vechia, L. Heart. 2004
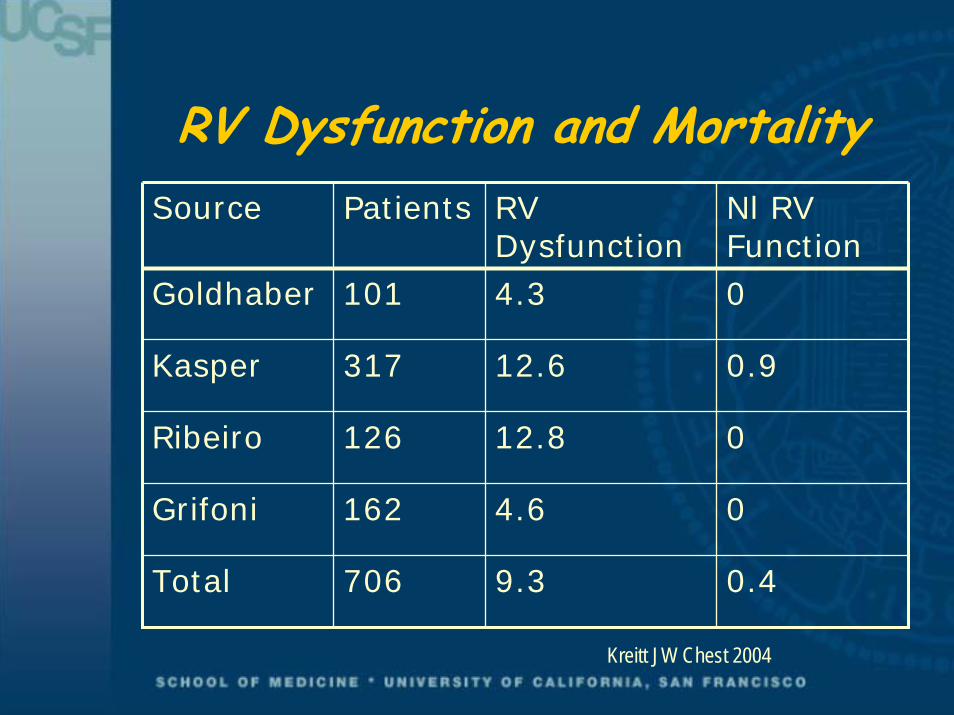
RV Dysfunction and MortalitySource Patients RV
DysfunctionNl RV Function
Goldhaber 101 4.3 0
Kasper 317 12.6 0.9
Ribeiro 126 12.8 0
Grifoni 162 4.6 0
Total 706 9.3 0.4
Kreitt JW Chest 2004
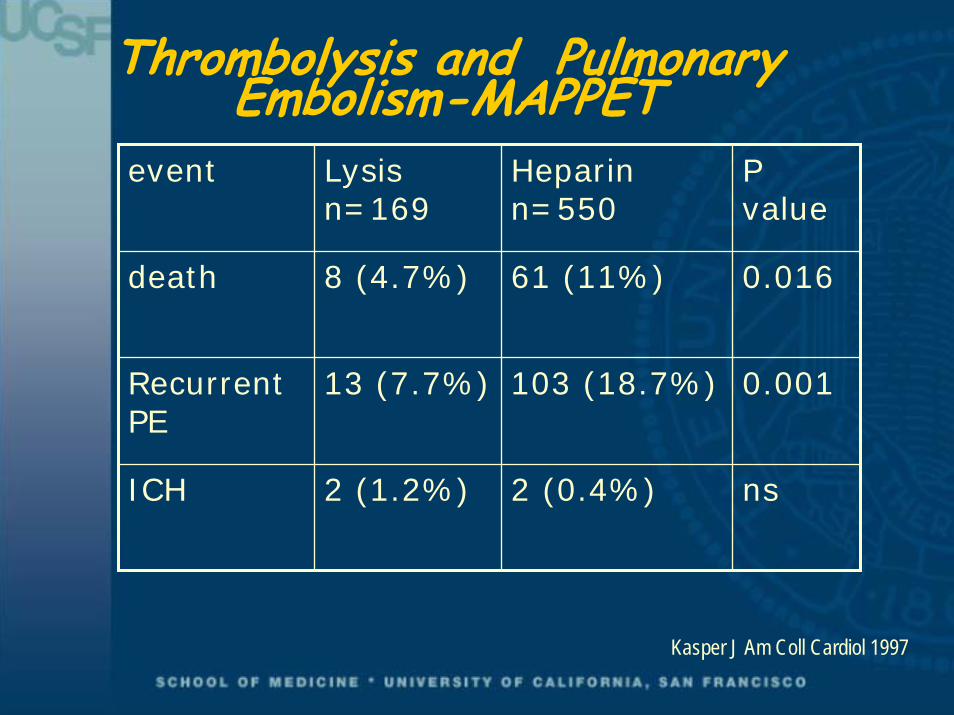
Thrombolysis and Pulmonary Embolism-MAPPET
event Lysisn=169
Heparin n=550
P value
death 8 (4.7%) 61 (11%) 0.016
Recurrent PE
13 (7.7%) 103 (18.7%) 0.001
ICH 2 (1.2%) 2 (0.4%) ns
Kasper J Am Coll Cardiol 1997
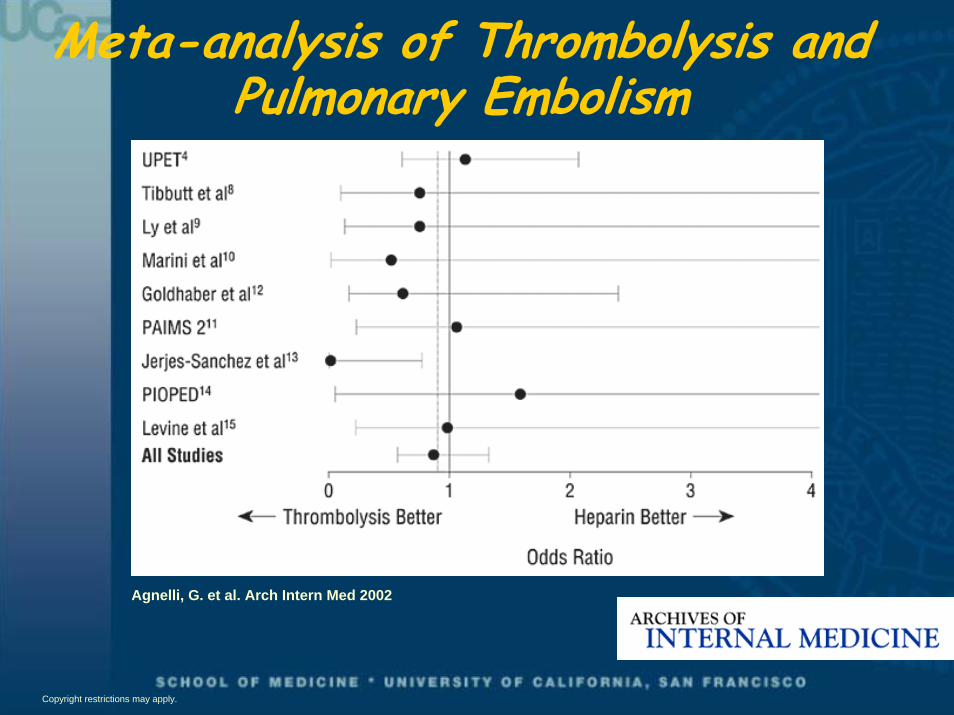
Meta-analysis of Thrombolysis and Pulmonary Embolism
Agnelli, G. et al. Arch Intern Med 2002
Copyright restrictions may apply.
Thrombolysis for SubmassivePulmonary Embolism
RCT of thrombolysis vs. heparin therapy for submassive PE118 received heparin + altepase, 138 received heparin +placeboPrimary outcome combined endpointof “escalation of therapy” and mortality
Konstantinides N Engl J Med 2002
Thrombolysis for SubmassivePulmonary Embolism
Acute PE without hemodynamiccompromise plus
RV dysfunction on ECHOPulmonary hypertension on ECHO or right heart cathNew RV strain on ECG
Konstantinides N Engl J Med 2002
Defining Submassive Pulmonary Embolism
PE without evidence of hemodynamicinstability, plus
Echocardiographic evidence of RV dysfunctionSubclinical impending right heart failureClinical evidence of pulmonary hypertension or right ventricular dysfunction

Thrombolysis for SubmassivePulmonary Embolism
Exclusionmajor surgery/ biopsy(7days) major trauma (10 days)CVA/TIA or CNS trauma (6 months).GI bleed (3 months)uncontrolled hypertensiona known bleeding disorderknown diabetic retinopathy
Konstantinides N Engl J Med 2002
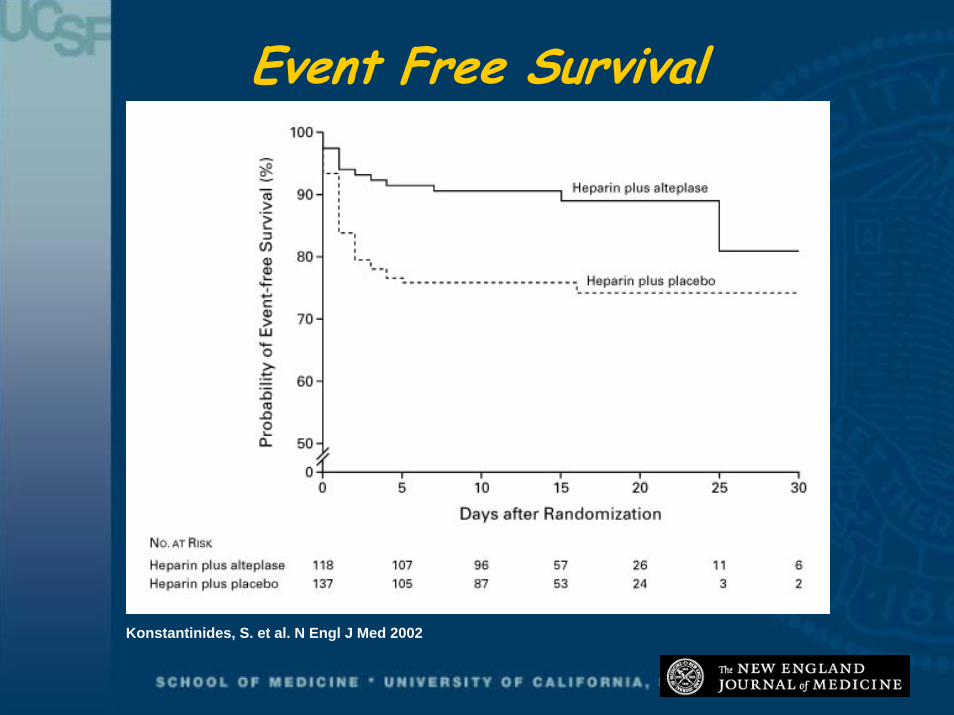
Event Free Survival
Konstantinides, S. et al. N Engl J Med 2002
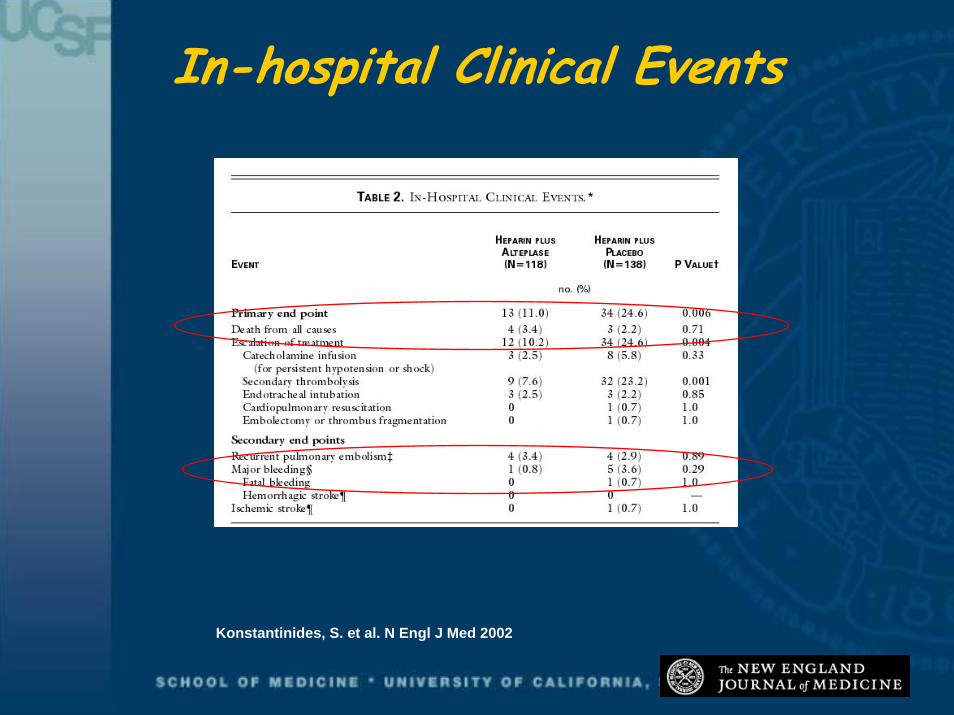
In-hospital Clinical Events
Konstantinides, S. et al. N Engl J Med 2002
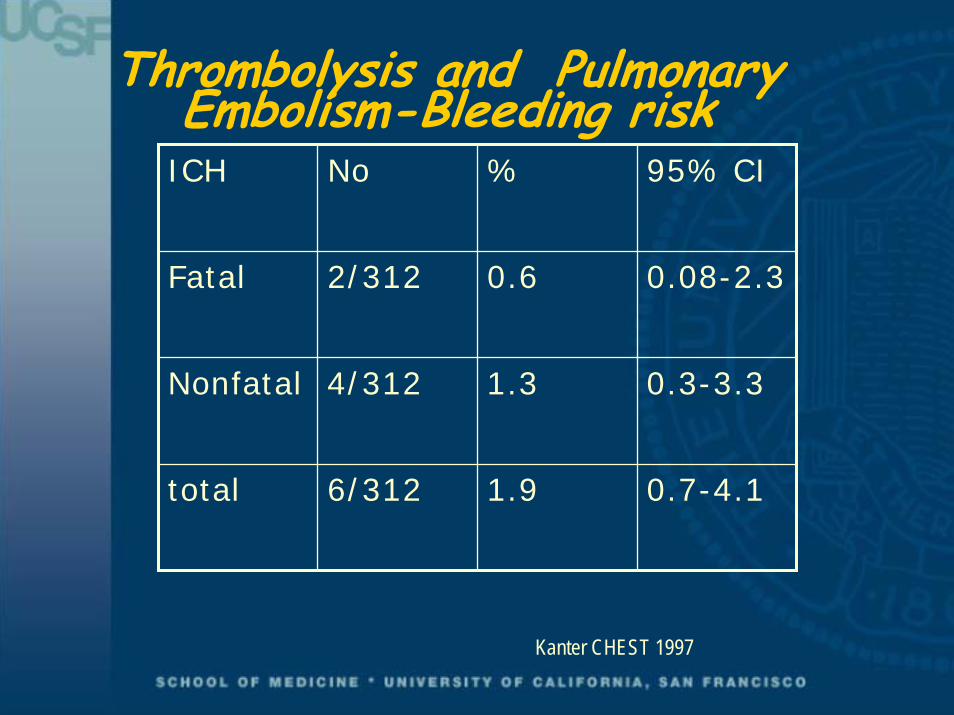
Thrombolysis and Pulmonary Embolism-Bleeding risk
ICH No % 95% CI
Fatal 2/312 0.6 0.08-2.3
Nonfatal 4/312 1.3 0.3-3.3
total 6/312 1.9 0.7-4.1
Kanter CHEST 1997
Addressing Critiques of Thrombolysisin Submassive Pulmonary Embolism
Cost prohibitiveShould consider potential long term impact of therapy
No decrease in recurrent PE or mortality benefit
Study used broad definition of submassive PEIncreased major bleeding
Risk low in carefully selected patients
Thrombolysis and Pulmonary Embolism-Conclusions
Clinical studies may be used to identify patients with PE at higher risk of adverse outcomesThrombolysis may prevent clinical deterioration in selected patientsThrombolysis should be reserved for patients at low bleeding riskFuture research should address efficacy of thrombolysis in more carefully selected patients; long term impact should be assessed
THE END
Thrombolysis for Pulmonary EMbolism
Despite early improvements in hemodynamics perfusion no difference in mortality at 1-2 weeks time when compared to heparin
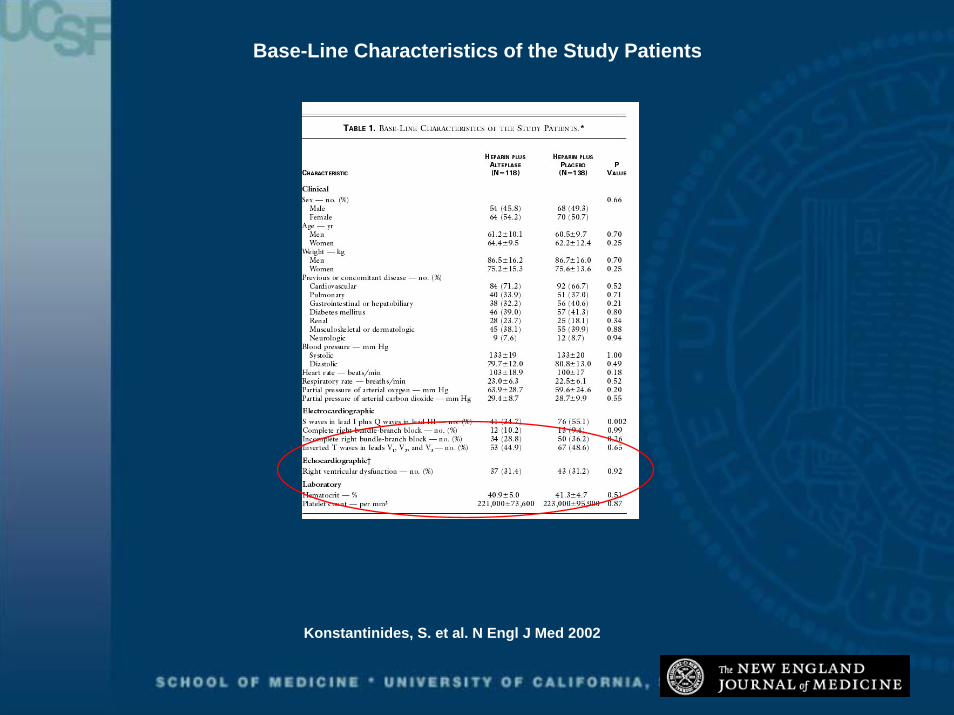
Base-Line Characteristics of the Study Patients
Konstantinides, S. et al. N Engl J Med 2002
Thrombolysis and Pulmonary Embolism
14% reduction in combined endpoint of escalation of therapy and death
Konstantinides N Engl J Med 2002

ThrombolysisThrombolysis in in SubmassiveSubmassivePulmonary embolism? Pulmonary embolism? NO!NO!
Dr P Dorasamy MBChB FCP FCCP FRCPC
Internist / PulmonologistAssociate ProfessorMcMaster University
Hamilton Health SciencesO t i C d

Submassive PEDefiniton
Acute PE with evidence of RV dysfunction but hemodynamicallystable
Thrombolysis in Submassive PE
MortalityMorbidityComplicationsCost
Case study
71 yr old male; 25 pack year smokerPresented with sudden onset dyspneaHR 100 RR 22 BP 100/60 ; no clinical DVTChest hyperinflated with decreased breath soundsHeart sounds normalECGCXRECHO
Spiral CT chestV/Q scanTreatment
1. Oxygen2. Heparin3. Bronchodilators
Course1. Responded well to therapy2. Repeat CT

ThrombolysisThrombolysis in Pulmonary in Pulmonary EmbolismEmbolism
Benefit in Massive PE established
Benefits documented by angiography, perfusion scans and echocardiography
Thrombolytics have not been shown to have a significant mortality or morbidity benefit in acute PE
Disadvantages of Thrombolytics
Increased major bleeding complications
Increased cost
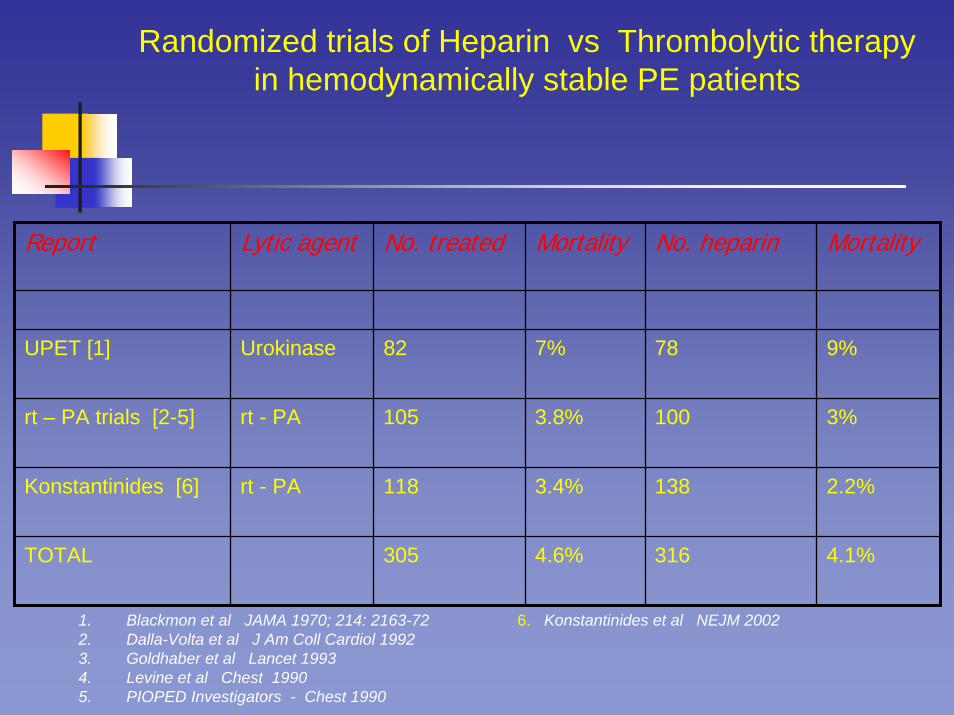
Randomized trials of Heparin vs Thrombolytic therapy in hemodynamically stable PE patients
Report Lytic agent No. treated Mortality No. heparin Mortality
UPET [1] Urokinase 82 7% 78 9%
rt – PA trials [2-5] rt - PA 105 3.8% 100 3%
Konstantinides [6] rt - PA 118 3.4% 138 2.2%
TOTAL 305 4.6% 316 4.1%
6. Konstantinides et al NEJM 20021. Blackmon et al JAMA 1970; 214: 2163-722. Dalla-Volta et al J Am Coll Cardiol 19923. Goldhaber et al Lancet 19934. Levine et al Chest 19905. PIOPED Investigators - Chest 1990
ThrombolysisThrombolysis in Pulmonary in Pulmonary EmbolismEmbolism
Recurrent PE is the principal cause of death in hemodynamically stable PE patients
Thrombolysis will decrease mortality only if it decreased the rate of recurrent PE
ThrombolysisThrombolysis in Pulmonary in Pulmonary EmbolismEmbolism
In studies where recurrent PE has been documented by follow-up lung scans or pulmonary angiograms, there has been no difference between patients treated with thrombolytics or heparin (JAMA 1970; J Am Coll Cardiol 1992; Chest 1990; NEJM 2002)
Patients with hemodynamically stable PE, mortality with heparin therapy is < 5% (Dalen Arch Int Med 2002)
Thrombolytics are not appropriate in these patients

Mortality in PEPatients with submassive PE have a higher mortality ( approx. 50% of all PE patients have RV dysfunction) (Goldhaber Lancet 1993)
Mortality in patients with RV dysfunction was 4% vs 0.9% in those without RV dysfunction (RVD)
1. Am Heart J 1997 (Ribeiro et al)2. Circulation 2000 ( Grifoni et al)3. Intensive Care Med 2001 ( Vieillard-Baron et al)
In 719 PE patients who were hemodynamically stable, mortality in those with RVD was 10% vs 4.1% in those without RVD (Konstantinides et al Circulation 1997)
Mortality in PEHamel et al Chest 2001 reported from a French registry of 153 patients with massive PE treated consecutively with either Heparin or a thrombolytic; non-randomised; matched for right ventricular dysfunction, age, lung scans and the presence of cardiac or respiratory diseaseMortality in 64 pts. treated with thrombolysiswas 6% vs 0% in those treated with heparinNo difference in rate of recurrence of PE
Mortality in PEMortality in PE
Mortality in 118 pts. randomised to receive alteplase + heparin (3.4%) vs 138 pts. on heparin alone (2.2%)Primary end-point was in-hospital death or “clinical deterioration requiring an escalation of treatment”

Mortality in PEMortality in PE
Mortality in PEMortality in PEEscalation of treatment occurred in 24.6% of patients in the heparin group vs 10.2% in the alteplasegroup ( P = 0.004)Secondary thrombolysis occurred in 23% in the heparin group vs 7.6% in the alteplase group ( P = 0.001)Primary indication for secondary thrombolysis was “worsening of clinical symptoms, particularly dyspnea”.Mortality in 118 pts. randomised to receive alteplase+ heparin (3.4%) vs 138 pts. on heparin alone (2.2%)106/138 pts. in heparin group avoided complications and excessive cost of thrombolytic treatment
ThrombolysisThrombolysis in PE patients with in PE patients with shockshock
No randomized clinical trials comparing heparin to thrombolytic therapy in patients with massive PE complicated by shock
Because of high mortality (30%) in PE patients with shock, thrombolysis is considered
Shock present in 10% of patients diagnosed with PE
Impact of Impact of ThrombolysisThrombolysis on on morbidity in PEmorbidity in PE
In patients who survive acute PE, morbidity may be due to unresolved pulmonary embolic obstruction, or to recurrent PE
Thrombolytic therapy increases the early resolution rate of pulmonary embolic obstruction as assessed by repeat lung scans or pulmonary angiograms 24 h after therapy. BUT the degree of resolution 24 h after thrombolytic therapy is incomplete

Morbidity in PEMorbidity in PEThe Urokinase PE trial (UPET)(JAMA 1970)
Percent resolution by lung scan after therapy
Time since treatment Urokinase Heparin
24 h 24.1% 8.3%
2 weeks 55.4% 56.2%
1 year 78.8% 77.2%
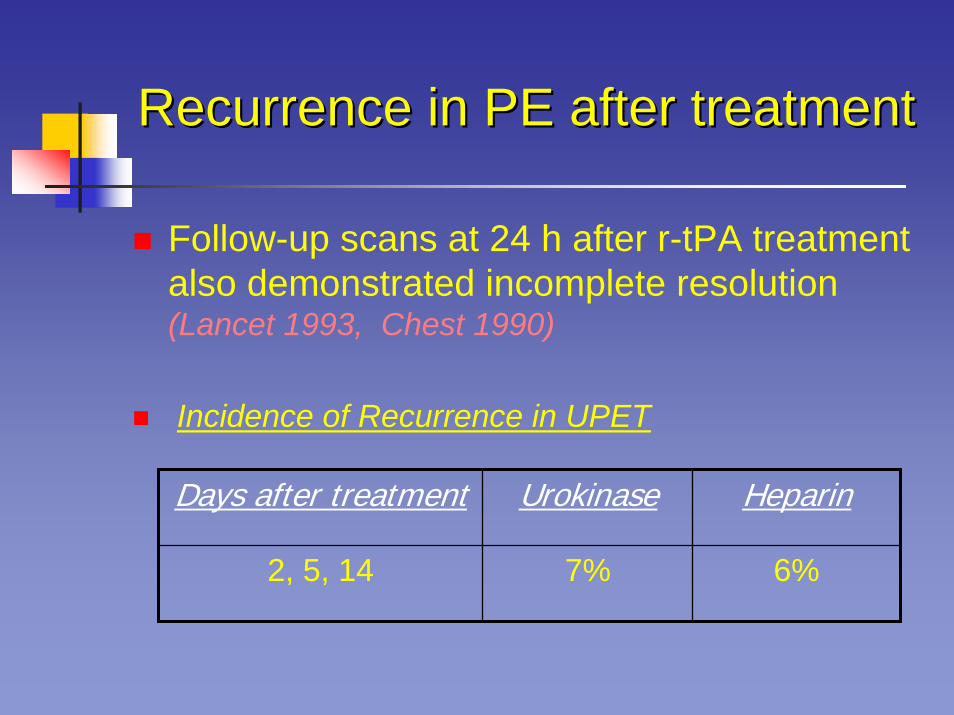
Recurrence in PE after treatmentRecurrence in PE after treatment
Follow-up scans at 24 h after r-tPA treatment also demonstrated incomplete resolution (Lancet 1993, Chest 1990)
Incidence of Recurrence in UPET
Days after treatment Urokinase Heparin
2, 5, 14 7% 6%
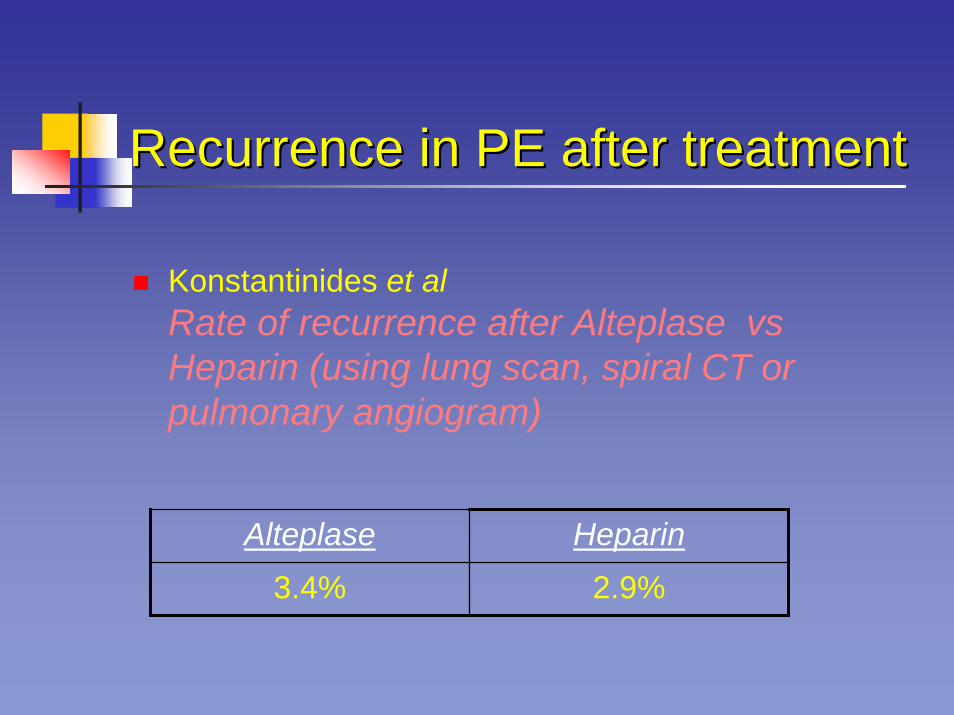
Recurrence in PE after treatmentRecurrence in PE after treatment
Konstantinides et alRate of recurrence after Alteplase vsHeparin (using lung scan, spiral CT or pulmonary angiogram)
Alteplase Heparin
3.4% 2.9%
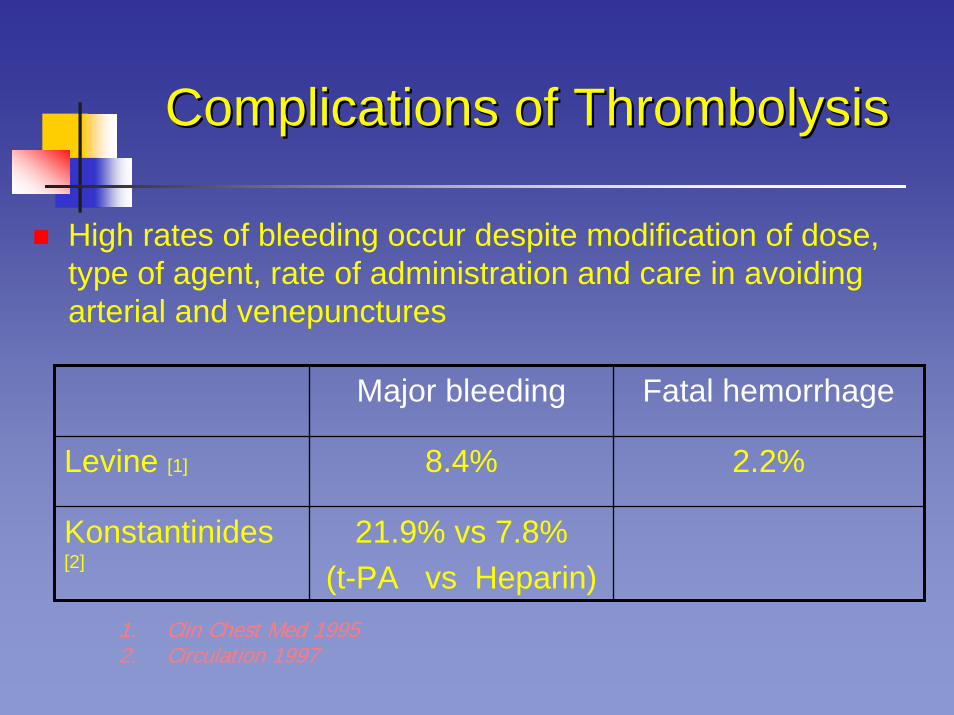
Complications of Complications of ThrombolysisThrombolysis
High rates of bleeding occur despite modification of dose, type of agent, rate of administration and care in avoiding arterial and venepunctures
Major bleeding Fatal hemorrhage
Levine [1] 8.4% 2.2%
Konstantinides[2]
21.9% vs 7.8%(t-PA vs Heparin)
1. Clin Chest Med 19952. Circulation 1997

Complications of Complications of ThrombolysisThrombolysis
Intracranial hemorrhage constitutes the most serious and lethal complication of thrombolytic therapy
Incidence of ICH in PE patients treated with thrombolytic therapyReport Patients (n) Incidence of ICH
Dalen et al 1997 [1] 559 2.1%
Goldhaber et al [2] 304 3.0%
Konstantinides et al [3] 118 0
TOTAL 981 2.1%
1. Arch Int Med 1997 2. Lancet 1999 (ICOPER) 3. NEJM 2002
Cost of Cost of ThrombolyticThrombolytic therapytherapyDrug cost: US$ 2974 for 100 mg of
Alteplase (Univ. Med Center Tucson, AZ 2003)
Cost of treating bleeding complications
Additional cost of treating the 50% ofpatients who are hemodynamically stable but with RVD
SUMMARY
There is insufficient evidence that thrombolysis benefits patients with submassive PEStudies demonstrate no mortality benefit and no difference on recurrence rates when compared to heparinThere is a significant risk of hemorrhage, including ICHThe cost of treatment is high and unjustifiable


Duration of Anticoagulation for Treatment of Acute VTE
SGIM PRECOURSEMay 11, 2005
Andrew Dunn, MD, FACPDirector, General Medicine Anticoagulation Service
Mount Sinai Medical CenterNew York, NY
A 48 year-old female presents with 4 days of right leg pain and swelling. An ultrasound confirms the presence of a right LE DVT.
The patient does not have h/o VTE, had no recent surgery or trauma, and is not on OCP or HRT. There is no family history of VTE. A thrombophilia work-up is negative.
Treatment with outpatient LMWH and warfarin is begun. LMWH is discontinued when the INR is therapeutic on day #6.
48 year-old female with idiopathic right LE DVT
How long will you treat the patient with warfarin?
• 3 months
• 6 months
• 12 months
• 2 years
• Indefinitely
• Lifelong
• Even longer
48 year-old with first idiopathic DVT
Expert opinion?
“For patients with a first episode of idiopathic DVT, we recommend treatment with a VKA for at least 6 to 12 months.”
“We suggest that patients with first-episode idiopathic DVT be considered for indefinite anticoagulant therapy.”
Buller HR. Chest. 2004;126:401S-428S.
What Is Worse?
+
Extended OAC for First VTE3 months vs 24 months
All patients received 3 months of standard treatment
Randomized to:Additional 24 months OAC (INR goal 2-3) or placebo
Study terminated early (mean f/u 10 months)
Kearon C. NEJM. 1999;340:901-7.
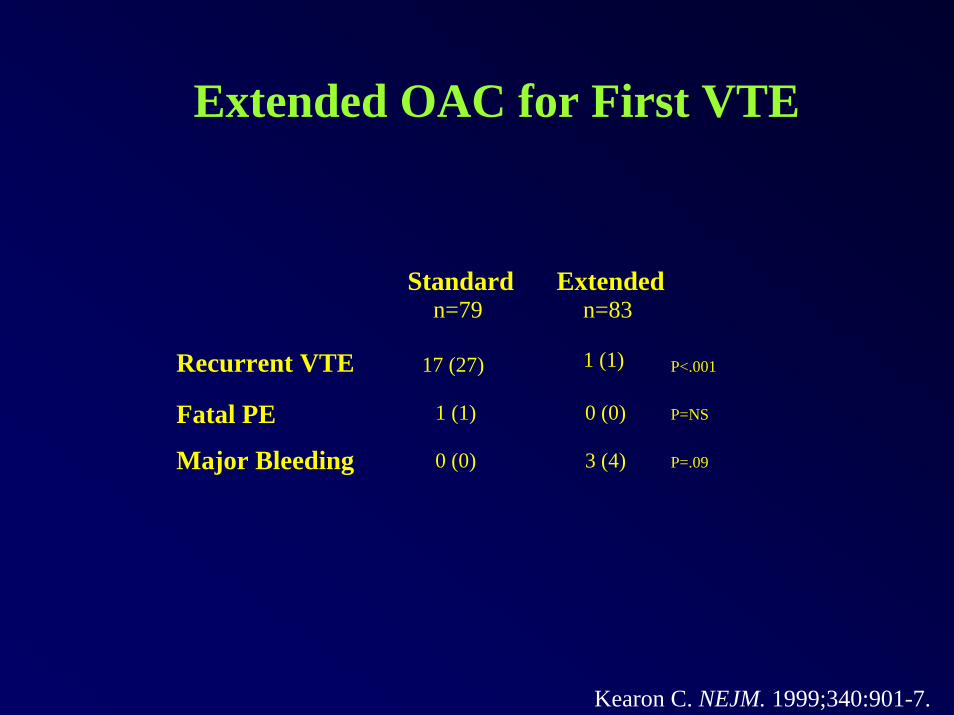
Extended OAC for First VTE
Standardn=79
Extendedn=83
Recurrent VTE 1 (1)17 (27) P<.001
Fatal PE 1 (1) 0 (0) P=NS
Major Bleeding 0 (0) 3 (4) P=.09
Kearon C. NEJM. 1999;340:901-7.
Extended OAC for First DVT3 months vs 1 year
…and lets look 1 year (or more) later
Agnelli G. NEJM. 2001;345:165-9.
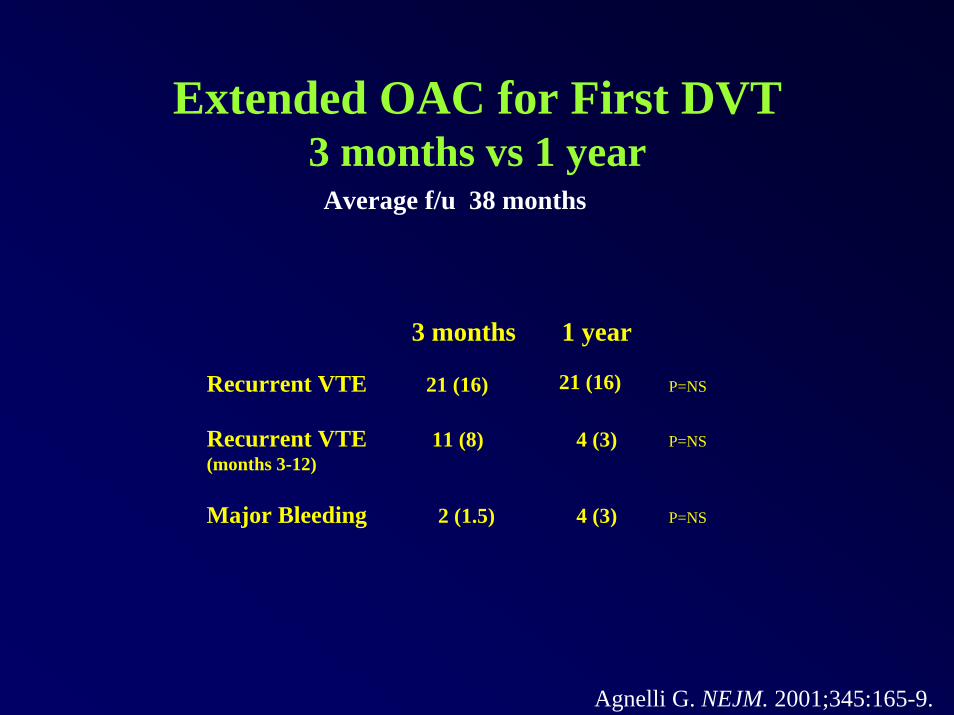
Extended OAC for First DVT3 months vs 1 year
Average f/u 38 months
3 months 1 year
Recurrent VTE 21 (16)21 (16) P=NS
Recurrent VTE(months 3-12)
11 (8) 4 (3) P=NS
Major Bleeding 2 (1.5) 4 (3) P=NS
Agnelli G. NEJM. 2001;345:165-9.
Extended OAC Duration Treatment of PE
3 months OAC for acute PE vs
6 months (transient risk factor) or 12 months (idiopathic)
Followed for average of 3 years.
Italian study, 19 hospitals.
N = 326
Agnelli G. Ann Intern Med. 2003;139:19-25.
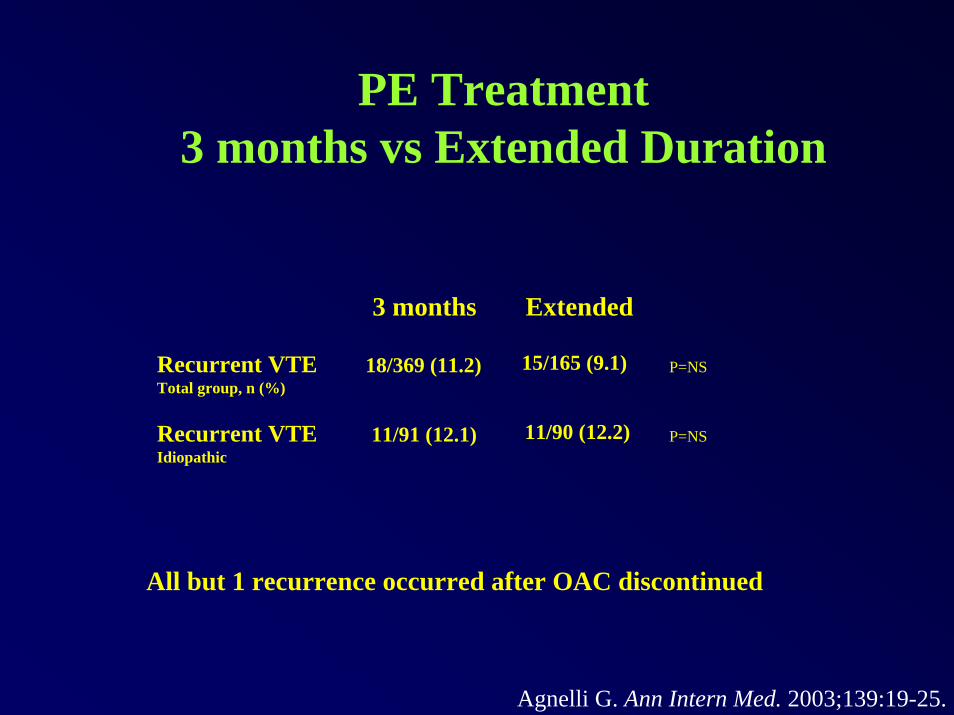
PE Treatment3 months vs Extended Duration
3 months Extended
Recurrent VTETotal group, n (%)
15/165 (9.1)18/369 (11.2) P=NS
Recurrent VTEIdiopathic
11/90 (12.2)11/91 (12.1) P=NS
All but 1 recurrence occurred after OAC discontinued
Agnelli G. Ann Intern Med. 2003;139:19-25.
Long-term Low-Intensity Warfarin for Prevention of Recurrent VTE
PREVENT
All received standard treatment (mean 6.5 months)N=508
Low-intensity Warfarin (INR 1.5-2.0) indefinitely vs Placebo
Average follow-up 2.1 years.
Trial terminated early
Ridker PM. NEJM. 2003:348:1425-34.
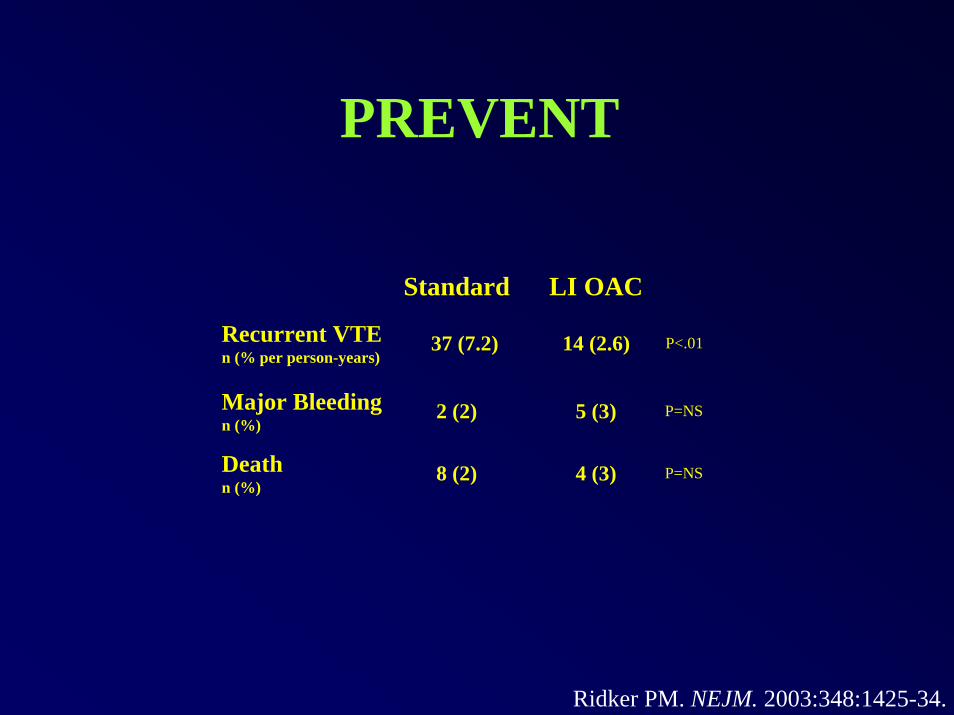
PREVENT
Standard LI OAC
Recurrent VTEn (% per person-years)
37 (7.2) 14 (2.6) P<.01
Major Bleedingn (%)
2 (2) 5 (3) P=NS
Deathn (%)
8 (2) 4 (3) P=NS
Ridker PM. NEJM. 2003:348:1425-34.
Low-Intensity Warfarin vs Conventional-Intensity Warfarin for Prevention of Recurrent VTE
ELATE
Warfarin target INR 2-3 (standard intensity OAC)
Warfarin target INR 1.5-1.9 (low-intensity OAC)
N=738Average follow-up 2.4 years
Kearon C. NEJM. 2003:349:631-9.
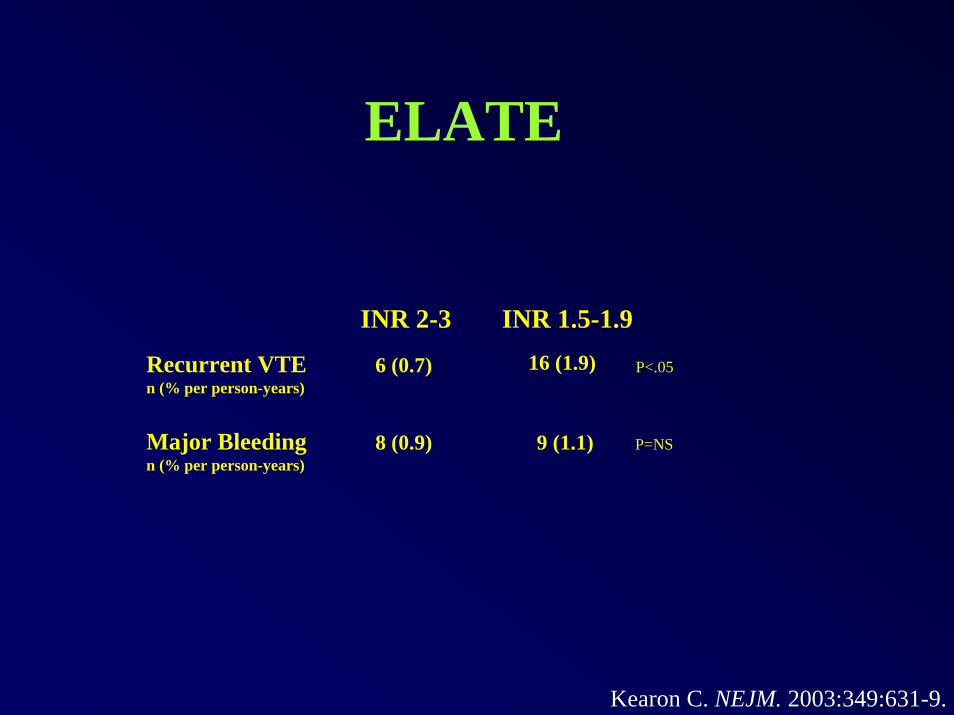
ELATE
INR 2-3 INR 1.5-1.9
Recurrent VTEn (% per person-years)
16 (1.9)6 (0.7) P<.05
Major Bleedingn (% per person-years)
8 (0.9) 9 (1.1) P=NS
Kearon C. NEJM. 2003:349:631-9.
CONCLUSIONS FROM RCTs
• Warfarin works when you are on it
• When you stop warfarin, there is a “catch-up” phenomenon
• If you are treating long-term or indefinite, you are treating lifelong
• If you are going to stop eventually, 6 months reasonable choice
• Major bleeding doesn’t happen in large RCTs
Without OAC, the recurrence rate is ~10% over the first year, then about 5% per year, and starts to wane.
Long-term recurrence rate = 30% over 8 years.
You have a 70% chance of being event free and requiring no medication or monitoring.
You have a 30% chance of a recurrent event, in which case you will need lifelong OAC. Unless you’re dead.
Prandoni P. Annals Intern Med. 1996;125:1-7.
How Often is Recurrent VTE Fatal?
Duration of Anticoagulation Trial Study Group (DURAC)
6 weeks vs 6 months. F/U for 2 years.N = 498.
VTE recurrence 18% vs 9% (6 months superior).
Of 123 recurrences, 5 fatal (4%).
Schulman S. NEJM. 1995;332:1661-5.
Risk of Fatal Recurrent VTE
Long-term follow-up study355 patients with first DVT
9 of 78 (11%) recurrences were fatal.
Prandoni P. Annals Intern Med. 1996;125:1-7.
Risk of Fatal Recurrent VTE
Analysis of California Discharge Database - VTE diagnoses
N = 71,25051,233 DVT21,625 PE
If initial dx DVT, relative risk of hospitalization for DVT = 2.7
If initial dx PE, relative risk of hospitalization for PE = 4.2
Murin S. Thromb Haem. 2002;88:407-14
Risk of Fatal Recurrent VTE
Review of 25 studies of treatment of DVT or PE
Of patients with initial DVT, fatality rate of recurrence 9% (15/171).
Of patients with initial PE, fatality rate of recurrence 26% (19/72).
Douketis JD. JAMA. 1998;279:458-62
IF IT DOESN’T KILL YOU…
IT DOESN’T MAKE YOU STRONGER
Post-thrombotic syndrome at 8 years after DVT - 30%
Best predictor of PTS: Ipsilateral recurrent DVT
Prandoni P. Annals Intern Med. 1996;125:1-7.

Bleeding Risk from OAC
Randomized trials – small (~1%)
Real life – not so small, (range debatable)
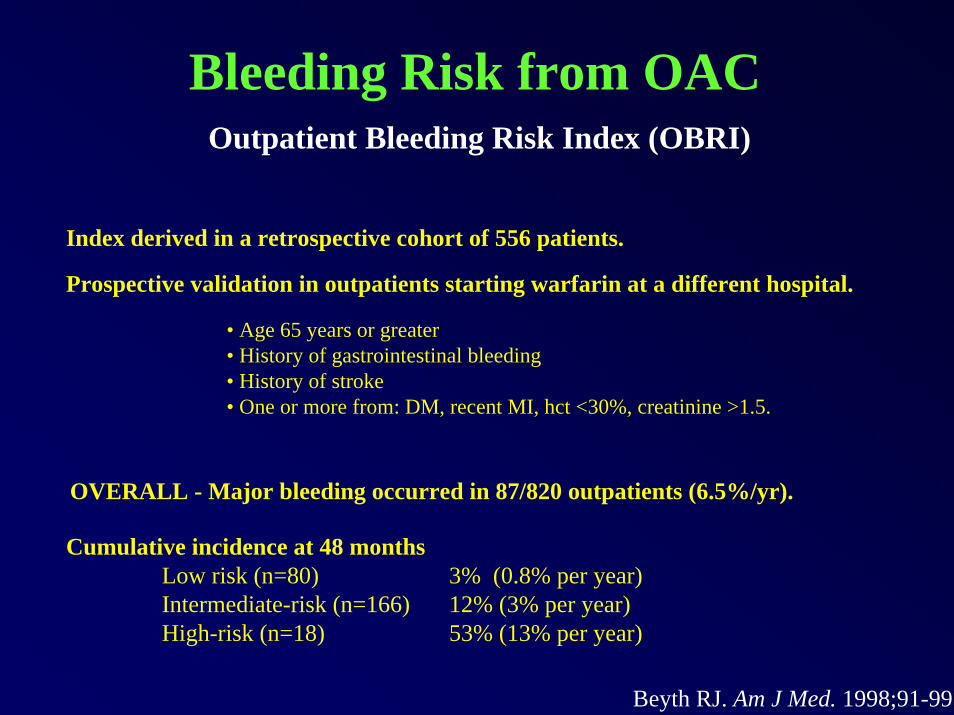
Bleeding Risk from OACOutpatient Bleeding Risk Index (OBRI)
Index derived in a retrospective cohort of 556 patients.
Prospective validation in outpatients starting warfarin at a different hospital.
• Age 65 years or greater• History of gastrointestinal bleeding• History of stroke• One or more from: DM, recent MI, hct <30%, creatinine >1.5.
OVERALL - Major bleeding occurred in 87/820 outpatients (6.5%/yr).
Cumulative incidence at 48 monthsLow risk (n=80) 3% (0.8% per year)Intermediate-risk (n=166) 12% (3% per year)High-risk (n=18) 53% (13% per year)
Beyth RJ. Am J Med. 1998;91-99.
Bleeding from OACHow often is it fatal?
META-ANALYSIS
33 studies examining 4374 patient-years
Case-fatality rate 13.4%
If on OAC >3 months, case fatality rate 9.1%
Linkins L. Ann Intern Med. 2003;139:893-901.
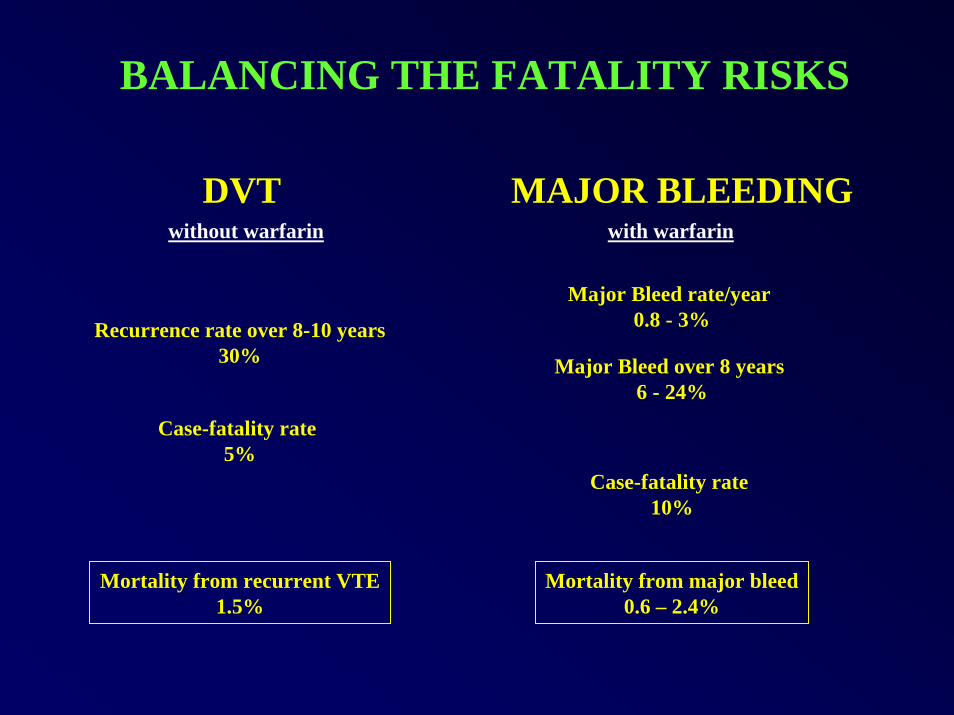
BALANCING THE FATALITY RISKS
DVT MAJOR BLEEDINGwithout warfarin with warfarin
Major Bleed rate/year 0.8 - 3%Recurrence rate over 8-10 years
30% Major Bleed over 8 years 6 - 24%
Case-fatality rate 5%
Case-fatality rate 10%
Mortality from recurrent VTE1.5%
Mortality from major bleed0.6 – 2.4%
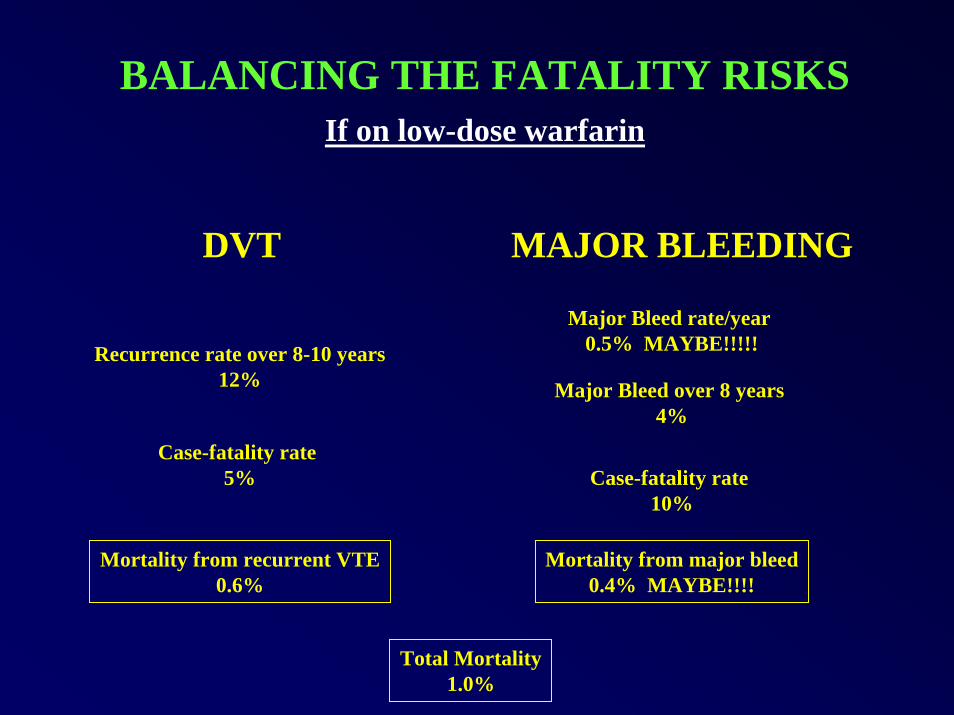
BALANCING THE FATALITY RISKSIf on low-dose warfarin
DVT MAJOR BLEEDING
Major Bleed rate/year 0.5% MAYBE!!!!!Recurrence rate over 8-10 years
12% Major Bleed over 8 years 4%
Case-fatality rate 5% Case-fatality rate
10%
Mortality from recurrent VTE0.6%
Mortality from major bleed0.4% MAYBE!!!!
Total Mortality1.0%
THE BOTTOM LINE48 year-old female first idiopathic DVT
• 30% chance of recurrence long-term
• There is a 70% chance of no recurrence
• If recurs can treat lifelong
• If doesn’t recur, you saved 50 years of warfarin and decreased the risk of fatal and nonfatal bleeding
• A great opportunity to involve the patient in shared decision-making
Should a Patient with Idiopathic DVT Should a Patient with Idiopathic DVT Undergo a Hypercoagulable WorkUndergo a Hypercoagulable Work--Up?Up?
An Argument in Favor of TestingAn Argument in Favor of Testing
Matt Eisen, MDMatt Eisen, MDSGIM 28SGIM 28thth Annual Meeting Annual Meeting
Precourse PM01Precourse PM015/11/055/11/05
Why Test for Thrombophilia?Why Test for Thrombophilia?
ThrombophiliaThrombophilia::•• Is common among patients with VTEIs common among patients with VTE•• Increases the relative risk of recurrent Increases the relative risk of recurrent
VTEVTE•• May influence patient managementMay influence patient management
How Common are How Common are HypercoagulableHypercoagulable Conditions?Conditions?
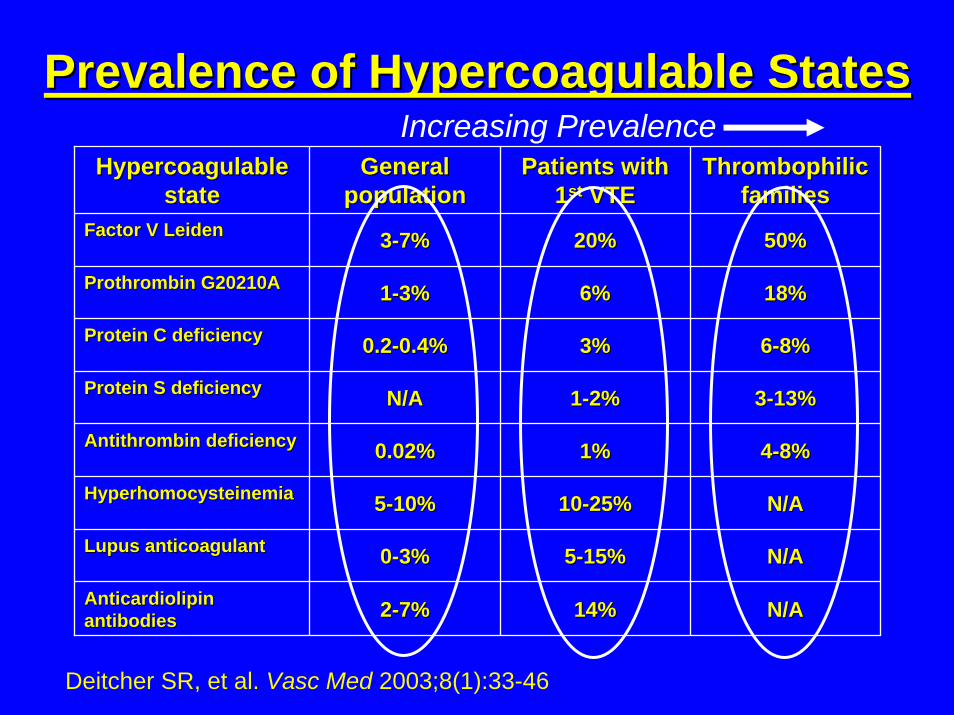
Prevalence of Prevalence of HypercoagulableHypercoagulable StatesStates
HypercoagulableHypercoagulablestatestate
General General populationpopulation
Patients with Patients with 11stst VTEVTE
ThrombophilicThrombophilicfamiliesfamilies
Factor V Factor V LeidenLeiden 33--7%7% 20%20% 50%50%
ProthrombinProthrombin G20210AG20210A 11--3%3% 6%6% 18%18%
Protein C deficiencyProtein C deficiency 0.20.2--0.4%0.4% 3%3% 66--8%8%
Protein S deficiencyProtein S deficiency N/AN/A 11--2%2% 33--13%13%
AntithrombinAntithrombin deficiencydeficiency 0.02%0.02% 1%1% 44--8%8%
HyperhomocysteinemiaHyperhomocysteinemia 55--10%10% 1010--25%25% N/AN/A
Lupus anticoagulantLupus anticoagulant 00--3%3% 55--15%15% N/AN/A
AnticardiolipinAnticardiolipinantibodiesantibodies 22--7%7% 14%14% N/AN/A
Increasing Prevalence
Deitcher SR, et al. Vasc Med 2003;8(1):33-46
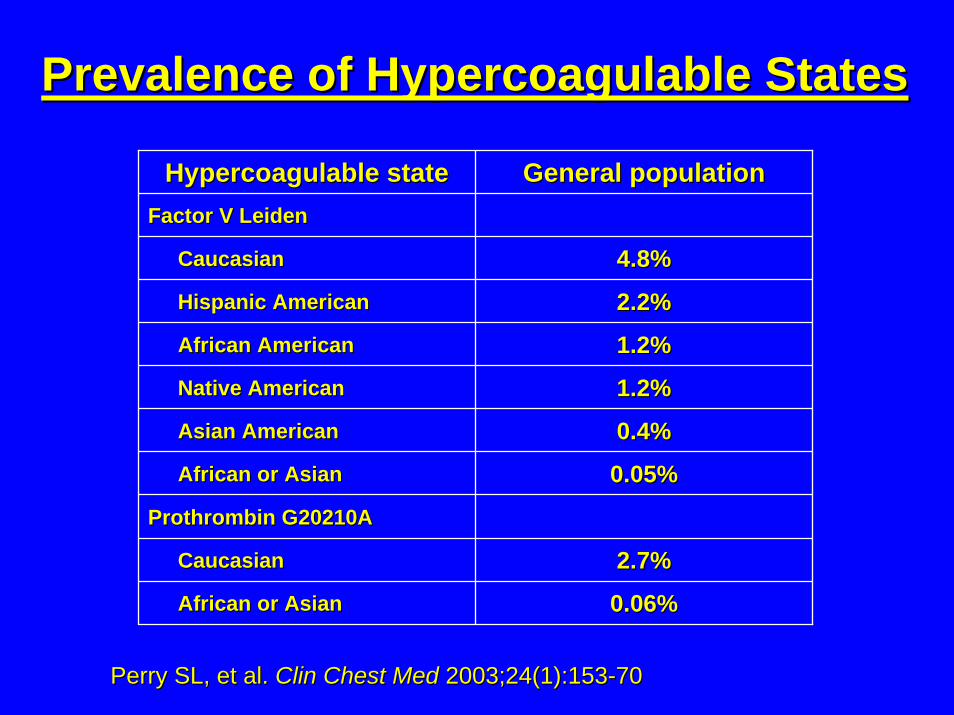
Prevalence of Prevalence of HypercoagulableHypercoagulable StatesStates
HypercoagulableHypercoagulable statestate General populationGeneral populationFactor V Factor V LeidenLeiden
CaucasianCaucasian 4.8%4.8%
Hispanic AmericanHispanic American 2.2%2.2%
African AmericanAfrican American 1.2%1.2%
Native AmericanNative American 1.2%1.2%
Asian AmericanAsian American 0.4%0.4%
African or AsianAfrican or Asian 0.05%0.05%
ProthrombinProthrombin G20210AG20210A
CaucasianCaucasian 2.7%2.7%
African or AsianAfrican or Asian 0.06%0.06%
Perry SL, et al. Perry SL, et al. ClinClin Chest MedChest Med 2003;24(1):1532003;24(1):153--7070
Prevalence ofPrevalence ofHypercoagulableHypercoagulable StatesStates
Key points:Key points:•• Testing will identify Testing will identify thrombophiliathrombophilia in in
2424--37% of patients with VTE37% of patients with VTE•• Selective testing increases the Selective testing increases the
likelihood of positive findingslikelihood of positive findings
How Much Risk is Associated with How Much Risk is Associated with HypercoagulableHypercoagulable Conditions?Conditions?
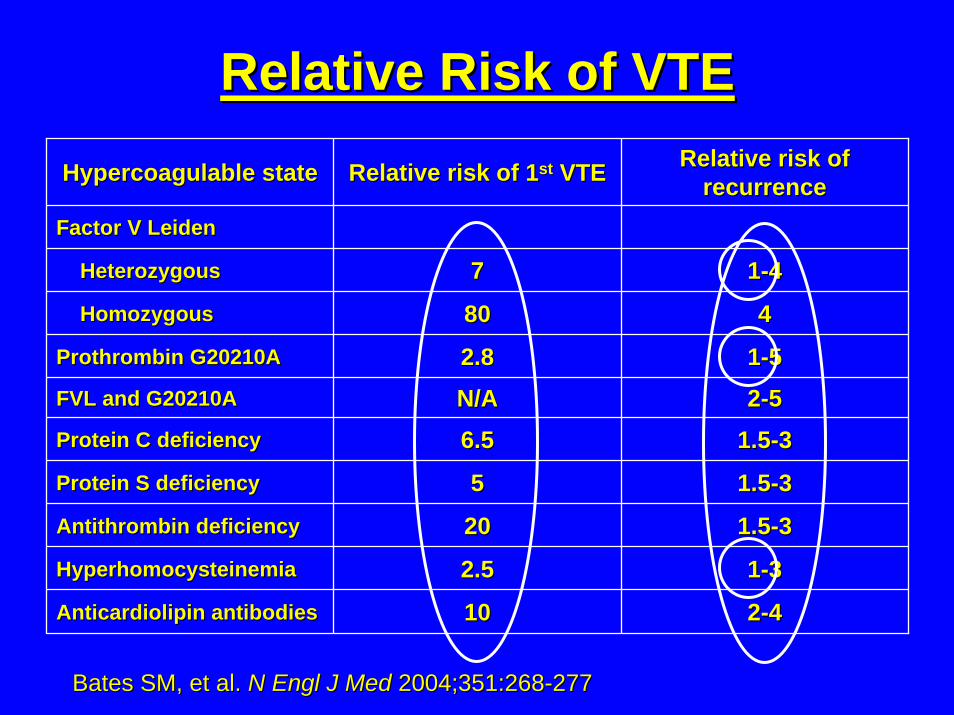
Relative Risk of VTERelative Risk of VTEHypercoagulableHypercoagulable statestate Relative risk of 1Relative risk of 1stst VTEVTE Relative risk of Relative risk of
recurrencerecurrenceFactor V Factor V LeidenLeiden
HeterozygousHeterozygous 77 11--44
HomozygousHomozygous 8080 44
ProthrombinProthrombin G20210AG20210A 2.82.8 11--55
FVL and G20210AFVL and G20210A N/AN/A 22--55
Protein C deficiencyProtein C deficiency 6.56.5 1.51.5--33
Protein S deficiencyProtein S deficiency 55 1.51.5--33
AntithrombinAntithrombin deficiencydeficiency 2020 1.51.5--33
HyperhomocysteinemiaHyperhomocysteinemia 2.52.5 11--33
AnticardiolipinAnticardiolipin antibodiesantibodies 1010 22--44
Bates SM, et al. Bates SM, et al. N N EnglEngl J MedJ Med 2004;351:2682004;351:268--277277
How Might the Presence of How Might the Presence of Thrombophilia Affect Patient Thrombophilia Affect Patient
Management?Management?
Duration of TherapyDuration of Therapy
Consider extended anticoagulation in Consider extended anticoagulation in patients with 1st idiopathic VTE and:patients with 1st idiopathic VTE and:•• Homozygous factor V Homozygous factor V leidenleiden or or
prothrombinprothrombin gene mutationgene mutation•• Combined heterozygous defectsCombined heterozygous defects•• Protein C or S deficiencyProtein C or S deficiency•• AntithrombinAntithrombin deficiencydeficiency•• AntiphospholipidAntiphospholipid antibodiesantibodies
Intensity/Monitoring of TherapyIntensity/Monitoring of Therapy
In patients with In patients with antiphospholipidantiphospholipidantibody syndrome:antibody syndrome:•• Consider higher target INRConsider higher target INR•• Consider monitoring by chromogenic Consider monitoring by chromogenic
factor X assayfactor X assay
Other TherapiesOther Therapies
In patients with In patients with hyperhomocysteinemiahyperhomocysteinemia::•• Consider giving Consider giving folatefolate / B6 / B12 and / B6 / B12 and
monitoring for improvement in serum monitoring for improvement in serum homocysteinehomocysteine

Screening Family MembersScreening Family Members
Finding of Finding of thrombophiliathrombophilia has has implications for:implications for:•• Decision to use Decision to use OCPsOCPs•• Decision to use HRTDecision to use HRT•• Management of pregnancyManagement of pregnancy
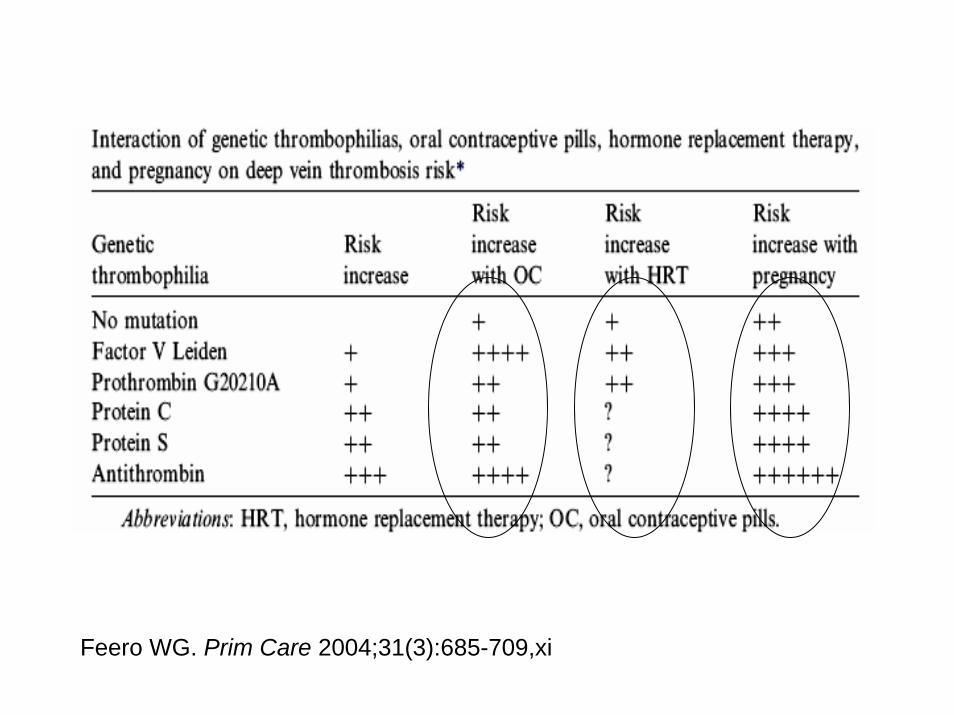
Feero WG. Prim Care 2004;31(3):685-709,xi
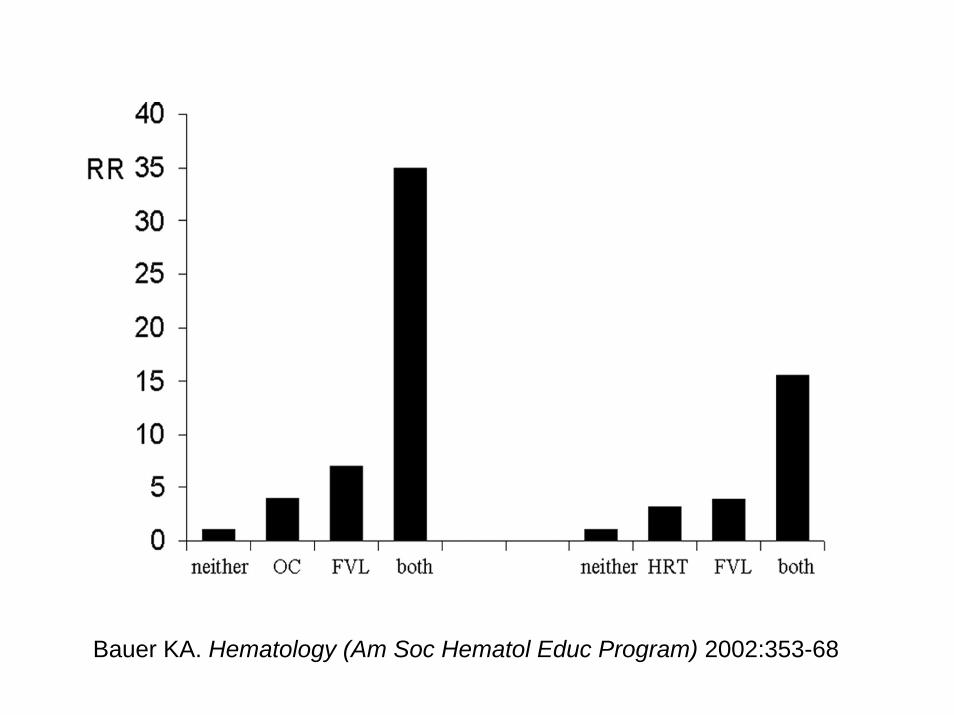
Bauer KA. Hematology (Am Soc Hematol Educ Program) 2002:353-68
What are the Costs of What are the Costs of HypercoagulableHypercoagulable Testing?Testing?

Costs of TestingCosts of Testing
•• Cost estimates range from $250 Cost estimates range from $250 --$1,000 for “standard panel”$1,000 for “standard panel”
•• One published costOne published cost--effectiveness study effectiveness study using Markov modelusing Markov model¹¹ concluded:concluded:
testing for testing for hypercoagulablehypercoagulable disorders in disorders in pts with idiopathic DVT followed by 2 pts with idiopathic DVT followed by 2 years of anticoagulation in affected pts is years of anticoagulation in affected pts is costcost--effectiveeffective
¹Auerbach AD. Am J Med 2004;116(12):816-28
The Case Against Routine The Case Against Routine Testing for HypercoagulabilityTesting for Hypercoagulability
Doug Einstadter, MD, MPHDoug Einstadter, MD, MPHCWRU at MetroHealth Medical CenterCWRU at MetroHealth Medical Center
SGIM 28SGIM 28thth Annual Meeting Annual Meeting New Orleans, LANew Orleans, LA
May 11, 2005May 11, 2005

BackgroundBackground•• A cause of thrombosis can be identified in A cause of thrombosis can be identified in
more than 80% of patients with VTE.more than 80% of patients with VTE.•• From 24 to 37% of all VTE is due to From 24 to 37% of all VTE is due to
inherited inherited thrombophiliathrombophilia..•• Testing for Testing for thrombophilia thrombophilia has become has become
increasingly common.increasingly common.•• Should testing after VTE be routine?Should testing after VTE be routine?
Commonly Requested Tests Commonly Requested Tests •• AntithrombinAntithrombin•• Protein C, Protein SProtein C, Protein S•• Factor V LeidenFactor V Leiden•• Prothrombin 20210AProthrombin 20210A•• DysfibrinogenemiaDysfibrinogenemia•• HyperhomocysteinemiaHyperhomocysteinemia•• Factor VIII, IX, XI, TAFIFactor VIII, IX, XI, TAFI•• APC resistance without Factor V LeidenAPC resistance without Factor V Leiden

Potential Reasons to TestPotential Reasons to Test
•• To determine optimal duration of therapyTo determine optimal duration of therapy•• To determine optimal intensity of therapyTo determine optimal intensity of therapy•• To identify and recommend prophylaxis for To identify and recommend prophylaxis for
asymptomatic family members during:asymptomatic family members during:–– High risk situationsHigh risk situations–– Pregnancy, oral contraceptive use, HRTPregnancy, oral contraceptive use, HRT
•• “Need to know” (intellectual curiosity)“Need to know” (intellectual curiosity)
Assumptions Underlying a Assumptions Underlying a Decision to TestDecision to Test
1.1. Presence of identified Presence of identified thrombophilia thrombophilia predicts greater risk of recurrence.predicts greater risk of recurrence.
2.2. More intense treatment for those with More intense treatment for those with thrombophilia thrombophilia leads to better outcomes.leads to better outcomes.
3.3. Family members of patients with VTE and Family members of patients with VTE and thrombophilia thrombophilia are at increased risk. are at increased risk.
4.4. Prophylactic treatment of family members Prophylactic treatment of family members leads to improved outcomes.leads to improved outcomes.
Does the Literature Support Does the Literature Support the Assumptions for Testing?the Assumptions for Testing?
Is Risk of RecurrentIs Risk of RecurrentVTE Increased?VTE Increased?
•• The overall risk of recurrent VTE in patients The overall risk of recurrent VTE in patients with and without with and without thrombophilia thrombophilia is similaris similar
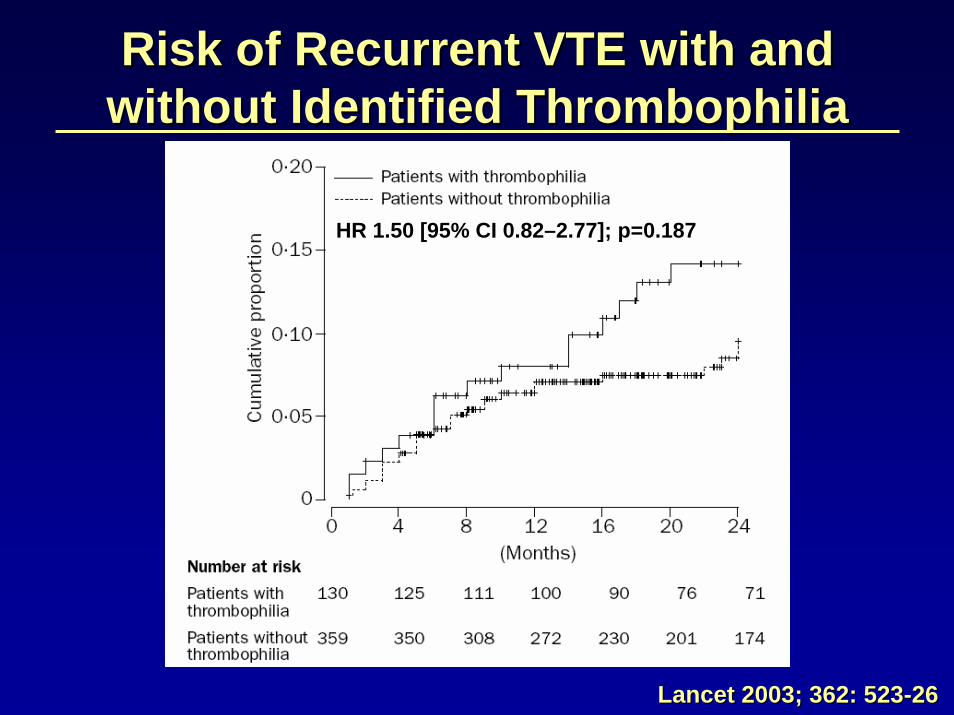
HR 1.50 [95% CI 0.82–2.77]; p=0.187
Risk of Recurrent VTE with and Risk of Recurrent VTE with and without Identified without Identified ThrombophiliaThrombophilia
Lancet 2003; 362: 523Lancet 2003; 362: 523--2626
Is Risk of RecurrentIs Risk of RecurrentVTE Increased?VTE Increased?
•• The overall risk in patients with and without The overall risk in patients with and without thrombophilia thrombophilia is similaris similar
•• Risk for patients with and without Risk for patients with and without heterozygous Factor V Leiden or G20210A heterozygous Factor V Leiden or G20210A is similar; risk in patients with homozygous is similar; risk in patients with homozygous Factor V Leiden probably is increasedFactor V Leiden probably is increased
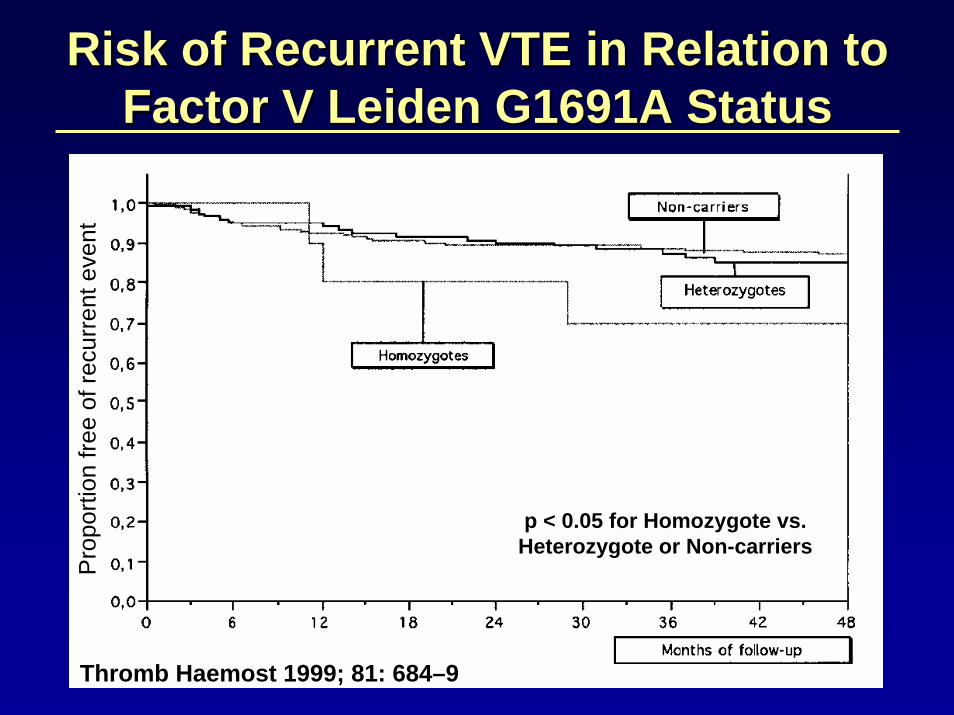
Risk of Recurrent VTE in Relation to Risk of Recurrent VTE in Relation to Factor V Leiden G1691A StatusFactor V Leiden G1691A Status
Thromb Haemost 1999; 81: 684–9
Pro
porti
on fr
ee o
f rec
urre
nt e
vent
p < 0.05 for Homozygote vs. Heterozygote or Non-carriers
Is Risk of RecurrentIs Risk of RecurrentVTE Increased?VTE Increased?
•• The overall risk in patients with and without The overall risk in patients with and without thrombophilia thrombophilia is similaris similar
•• Risk for patients with and without Risk for patients with and without heterozygous Factor V Leiden or G20210A heterozygous Factor V Leiden or G20210A is similar; risk in patients with homozygous is similar; risk in patients with homozygous Factor V Leiden probably is increasedFactor V Leiden probably is increased
•• The risk in patients with combinations of The risk in patients with combinations of thrombophilia thrombophilia is not well definedis not well defined
•• Other, as yet unidentified deficiencies may Other, as yet unidentified deficiencies may also affect riskalso affect risk

Duration of TherapyDuration of Therapy•• Treatment for six months provides a good Treatment for six months provides a good
balance of risks and benefits. balance of risks and benefits. •• Longer duration of treatment (up to 3 Longer duration of treatment (up to 3
years) reduces recurrence, but increases years) reduces recurrence, but increases hemorrhage risk for all patients.hemorrhage risk for all patients.
•• Prolonged duration of treatment for those Prolonged duration of treatment for those with identified with identified thrombophilia thrombophilia alone is not alone is not supported by the literature.supported by the literature.
Intensity of TherapyIntensity of Therapy•• Target INR of 2.5 is recommended for VTETarget INR of 2.5 is recommended for VTE•• Higher intensity indicated in those patients Higher intensity indicated in those patients
with thrombosis despite a therapeutic INR with thrombosis despite a therapeutic INR (regardless of identified thrombophilia)(regardless of identified thrombophilia)
•• There is no evidence to support the routine There is no evidence to support the routine use of higher intensity regimens for use of higher intensity regimens for patients with identified thrombophiliapatients with identified thrombophilia
Thrombosis PreventionThrombosis Prevention
•• There is no evidence to support primary There is no evidence to support primary prophylaxis of asymptomatic family prophylaxis of asymptomatic family members found to have thrombophilia.members found to have thrombophilia.
•• All patients, regardless of thrombophilia All patients, regardless of thrombophilia status, should receive prophylaxis during status, should receive prophylaxis during periods of high risk.periods of high risk.
Effect on Contraceptive, HRT Effect on Contraceptive, HRT and Pregnancy Advice and Pregnancy Advice
•• To prevent 1 oral contraceptive related To prevent 1 oral contraceptive related death due to PE requires screening more death due to PE requires screening more than 2 million women for Factor V Leiden.than 2 million women for Factor V Leiden.
•• There is little evidence to quantitate risk of There is little evidence to quantitate risk of VTE associated with HRT in asymptomatic VTE associated with HRT in asymptomatic women with thrombophilia. women with thrombophilia.
•• No evidence that risk : benefit ratio favors No evidence that risk : benefit ratio favors prophylaxis in pregnant asymptomatic prophylaxis in pregnant asymptomatic carriers of Factor V Leiden, G20210A, or carriers of Factor V Leiden, G20210A, or other deficienciesother deficiencies
SummarySummary
•• The current evidence does not support The current evidence does not support indiscriminate testing for indiscriminate testing for thrombophiliathrombophilia
•• Testing for heritable Testing for heritable thrombophilia thrombophilia is is unlikely to change the clinical unlikely to change the clinical management of individual patientsmanagement of individual patients
•• OverOver--testing may result in increased testing may result in increased anxiety, false reassurance, or treatment anxiety, false reassurance, or treatment related adverse eventsrelated adverse events
Stroke Prevention in AFStroke Prevention in AF
““To To AnticoagulateAnticoagulate or or Not to Anticoagulate”Not to Anticoagulate”
Steven L. Cohn, MD, FACPSteven L. Cohn, MD, FACPChief Chief –– Division of General Internal MedicineDivision of General Internal Medicine
Director Director –– Medical Consultation ServiceMedical Consultation ServiceClinical Professor of MedicineClinical Professor of Medicine
SUNY DownstateSUNY Downstate
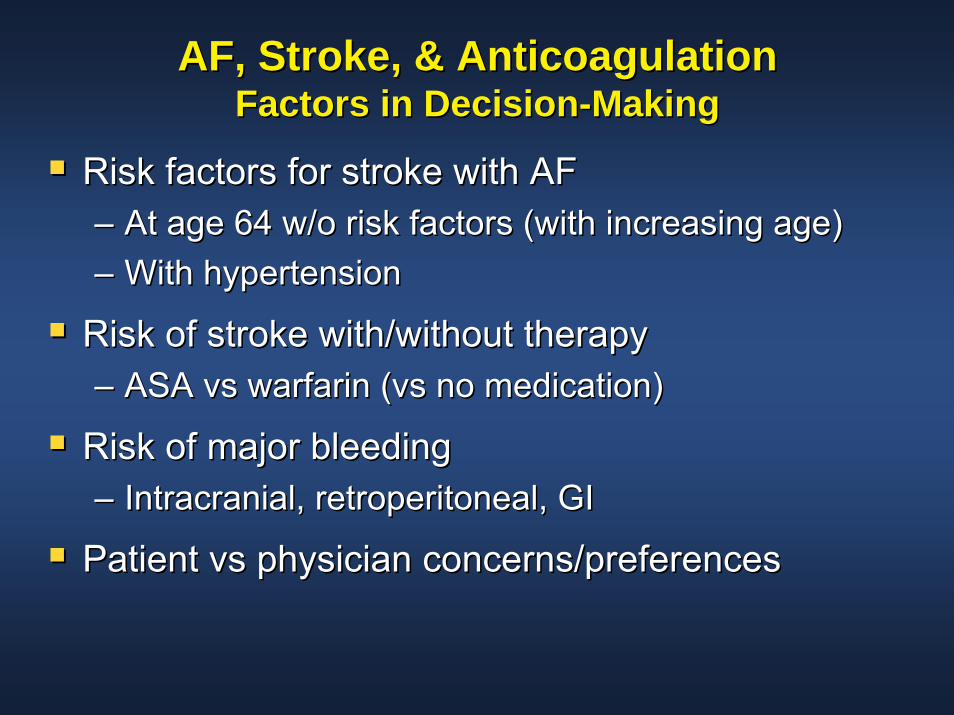
AF, Stroke, & AnticoagulationAF, Stroke, & AnticoagulationFactors in DecisionFactors in Decision--MakingMaking
Risk factors for stroke with AFRisk factors for stroke with AF–– At age 64 w/o risk factors (with increasing age)At age 64 w/o risk factors (with increasing age)–– With hypertensionWith hypertension
Risk of stroke with/without therapyRisk of stroke with/without therapy–– ASA vs warfarin (vs no medication)ASA vs warfarin (vs no medication)
Risk of major bleedingRisk of major bleeding–– Intracranial, retroperitoneal, GIIntracranial, retroperitoneal, GI
Patient vs physician concerns/preferencesPatient vs physician concerns/preferences

Definitions of Stroke RiskDefinitions of Stroke Risk
SourceSource High RiskHigh RiskIntermediate Intermediate
RiskRisk Low RiskLow Risk
Atrial Fibrillation Atrial Fibrillation InvestigatorsInvestigators
Age Age ≥≥6565 years; history of years; history of hypertensionhypertension; CAD; diabetes; CAD; diabetes
Age Age <65 years; <65 years; no highno high--risk featuresrisk features
American College American College of Chest of Chest PhysiciansPhysicians
Age Age >75 years; history >75 years; history of of hypertensionhypertension; LV ; LV dysfunction; more than dysfunction; more than 1 intermediate risk 1 intermediate risk factorfactor
Age Age 6565--75 years; 75 years; diabetes; CAD; diabetes; CAD; thyrotoxicosisthyrotoxicosis
Age Age <65 years; <65 years; no highno high--risk featuresrisk features
Stroke Prevention Stroke Prevention in Atrial in Atrial FibrillationFibrillation
Women age Women age >75 years; >75 years; Systolic BP >160 mm Systolic BP >160 mm HgHg; LV dysfunction; LV dysfunction
History of History of hypertensionhypertension; no ; no highhigh--risk featuresrisk features
No highNo high--risk features; risk features; no history of no history of hypertensionhypertension
Fuster et al. Fuster et al. J Am Coll CardiolJ Am Coll Cardiol. 2001;38:1231. 2001;38:1231--1265.1265.
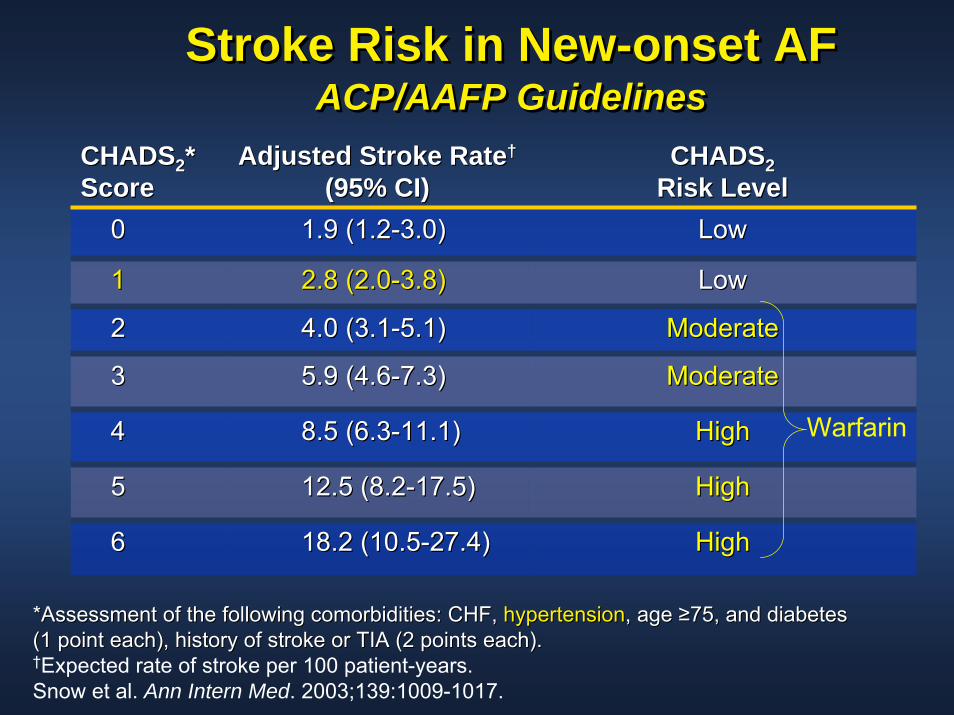
Stroke Risk in New-onset AFACP/AAFP Guidelines
Stroke Risk in NewStroke Risk in New--onset AFonset AFACP/AAFP GuidelinesACP/AAFP Guidelines
CHADSCHADS22**ScoreScore
Adjusted Stroke RateAdjusted Stroke Rate††
(95% CI)(95% CI)CHADSCHADS22
Risk LevelRisk Level00 1.9 (1.21.9 (1.2--3.0)3.0) LowLow
33 5.9 (4.65.9 (4.6--7.3)7.3) ModerateModerate
44 8.5 (6.38.5 (6.3--11.1)11.1) HighHigh
55 12.5 (8.212.5 (8.2--17.5)17.5) HighHigh
66 18.2 (10.518.2 (10.5--27.4)27.4) HighHigh
11 2.8 (2.02.8 (2.0--3.8)3.8) LowLow
22 4.0 (3.14.0 (3.1--5.1)5.1) ModerateModerate
Warfarin
*Assessment of the following comorbidities: CHF, *Assessment of the following comorbidities: CHF, hypertensionhypertension, age , age ≥≥75, and diabetes 75, and diabetes (1 point each), history of stroke or TIA (2 points each). (1 point each), history of stroke or TIA (2 points each). †Expected rate of stroke per 100 patient-years.Snow et al. Ann Intern Med. 2003;139:1009-1017.
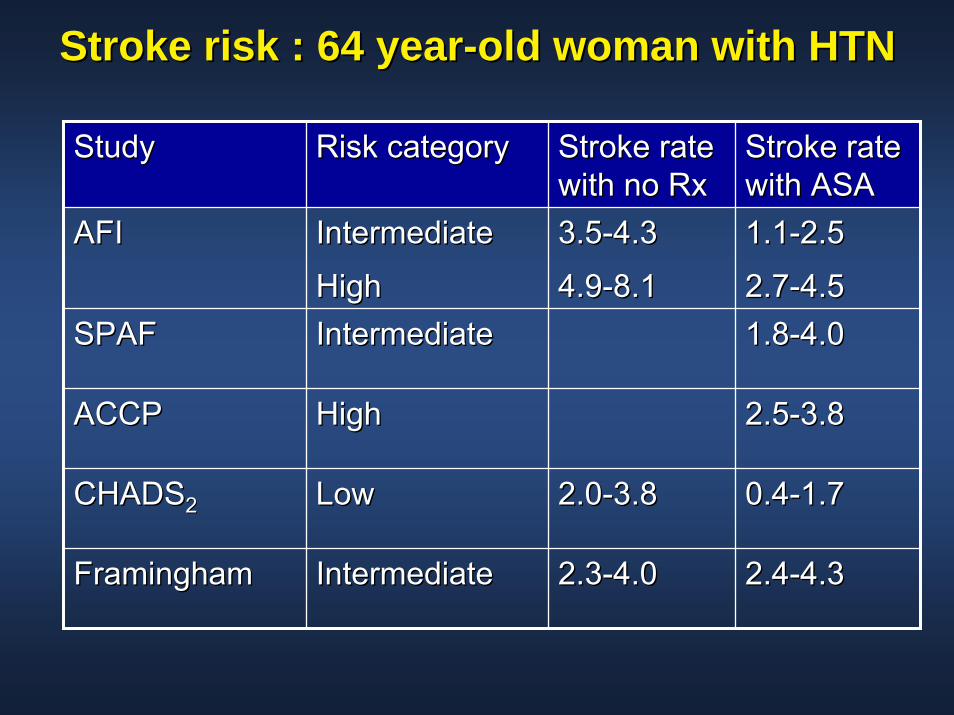
Stroke risk : 64 yearStroke risk : 64 year--old woman with HTNold woman with HTN
StudyStudy Risk categoryRisk category Stroke rate Stroke rate with no Rxwith no Rx
Stroke rate Stroke rate with ASAwith ASA
3.53.5--4.34.3
4.94.9--8.18.11.11.1--2.52.5
2.72.7--4.54.51.81.8--4.04.0
2.52.5--3.83.8
0.40.4--1.71.7
2.42.4--4.34.3
2.02.0--3.83.8
2.32.3--4.04.0
AFIAFI IntermediateIntermediate
HighHighSPAFSPAF IntermediateIntermediate
ACCPACCP HighHigh
CHADSCHADS22 LowLow
FraminghamFramingham IntermediateIntermediate
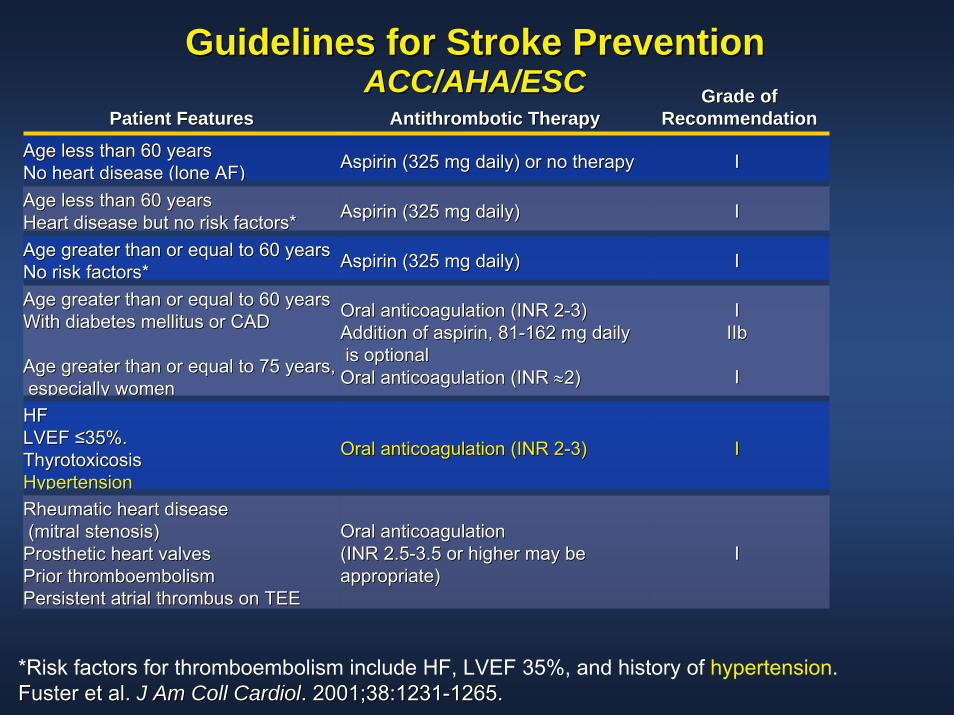
Guidelines for Stroke PreventionGuidelines for Stroke PreventionACC/AHA/ESCACC/AHA/ESC
Patient FeaturesPatient Features Antithrombotic TherapyAntithrombotic TherapyGrade of Grade of
RecommendationRecommendation
Age less than 60 yearsAge less than 60 yearsNo heart disease (lone AF)No heart disease (lone AF) Aspirin (325 mg daily) or no therapyAspirin (325 mg daily) or no therapy II
Age less than 60 yearsAge less than 60 yearsHeart disease but no risk factors*Heart disease but no risk factors* Aspirin (325 mg daily)Aspirin (325 mg daily) II
Age greater than or equal to 60 yearsAge greater than or equal to 60 yearsNo risk factors*No risk factors* Aspirin (325 mg daily)Aspirin (325 mg daily) II
Age greater than or equal to 60 yearsAge greater than or equal to 60 yearsWith diabetes mellitus or CADWith diabetes mellitus or CAD
Age greater than or equal to 75 years,Age greater than or equal to 75 years,especially womenespecially women
Oral anticoagulation (INR 2Oral anticoagulation (INR 2--3)3)Addition of aspirin, 81Addition of aspirin, 81--162 mg daily162 mg dailyis optionalis optional
Oral anticoagulation (INR Oral anticoagulation (INR ≈≈2)2)
IIIIbIIb
II
HFHFLVEF LVEF ≤≤35%.35%.ThyrotoxicosisThyrotoxicosisHypertensionHypertension
Oral anticoagulation (INR 2Oral anticoagulation (INR 2--3)3) II
Rheumatic heart diseaseRheumatic heart disease(mitral stenosis)(mitral stenosis)
Prosthetic heart valvesProsthetic heart valvesPrior thromboembolismPrior thromboembolismPersistent atrial thrombus on TEEPersistent atrial thrombus on TEE
Oral anticoagulationOral anticoagulation(INR 2.5(INR 2.5--3.5 or higher may be 3.5 or higher may be appropriate)appropriate)
II
*Risk factors for thromboembolism include HF, LVEF 35%, and history of hypertension.Fuster et al. Fuster et al. J Am Coll CardiolJ Am Coll Cardiol. 2001;38:1231. 2001;38:1231--1265.1265.

Expected Stroke Rate in AFExpected Stroke Rate in AFEffect of Risk Factors and AgeEffect of Risk Factors and Age
*No data on aspirin therapy.*No data on aspirin therapy.RF = risk factors: RF = risk factors: hypertensionhypertension, diabetes, prior TIA, or stroke., diabetes, prior TIA, or stroke.Ezekowitz et al. Ezekowitz et al. JAMA.JAMA. 1999;281:18301999;281:1830--1835.1835.
0
5
10
15
-- RFRF -- RFRF -- RFRF+ RF+ RF + RF+ RF + RF+ RF
Age (years)Age (years)
Stro
kes
per Y
ear (
%)
Stro
kes
per Y
ear (
%)
WarfarinWarfarinPlaceboPlacebo AspirinAspirin
>75>756565--7575<65<65
10%10%
4%4%
12%12%
**
1.7%1.7%
3.5%3.5%
1.7%1.7%
**
5.7%5.7%
1.4%1.4%1.1%1.1%
4.3%4.3%
1.7%1.7%
**
4.9%4.9%
1%1% 1%1%**
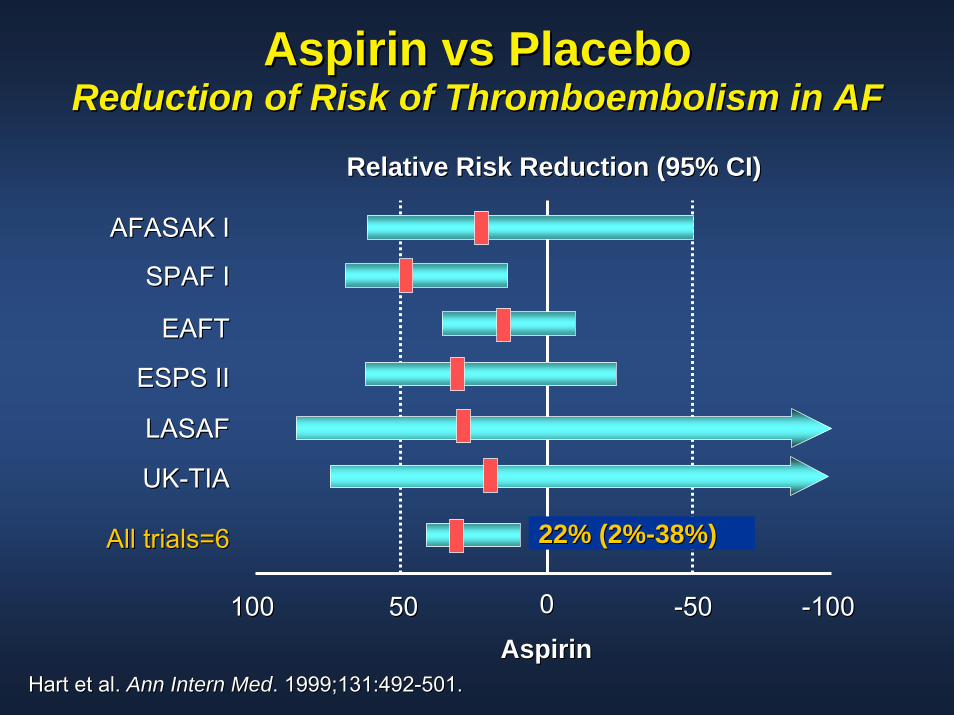
Aspirin vs PlaceboAspirin vs PlaceboReduction of Risk of Thromboembolism in AFReduction of Risk of Thromboembolism in AF
Relative Risk Reduction (95% CI)Relative Risk Reduction (95% CI)
AFASAK IAFASAK I
SPAF ISPAF I
22% (2%22% (2%--38%) 38%)
EAFTEAFT
ESPS IIESPS II
LASAFLASAF
UKUK--TIATIA
All trials=6All trials=6
00
AspirinAspirin100100 5050 --5050 --100100
Hart et al. Hart et al. Ann Intern MedAnn Intern Med. 1999;131:492. 1999;131:492--501.501.
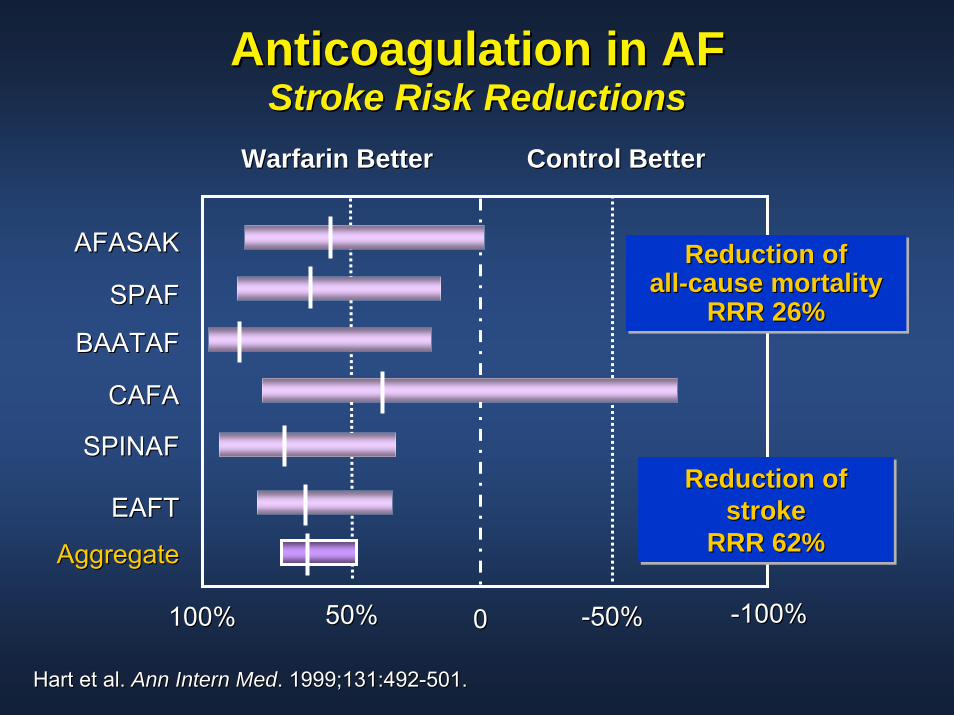
Anticoagulation in AFAnticoagulation in AFStroke Risk ReductionsStroke Risk Reductions
Warfarin BetterWarfarin Better Control BetterControl Better
AFASAKAFASAK
SPAFSPAF
BAATAFBAATAF
CAFACAFA
SPINAFSPINAF
EAFTEAFT
100%100% 50%50% 00 --50%50% --100%100%
AggregateAggregate
Reduction of stroke
RRR 62%
Reduction of Reduction of strokestroke
RRR 62% RRR 62%
Reduction ofall-cause mortality
RRR 26%
Reduction ofReduction ofallall--cause mortality cause mortality
RRR 26%RRR 26%
Hart et al. Hart et al. Ann Intern MedAnn Intern Med. 1999;131:492. 1999;131:492--501.501.
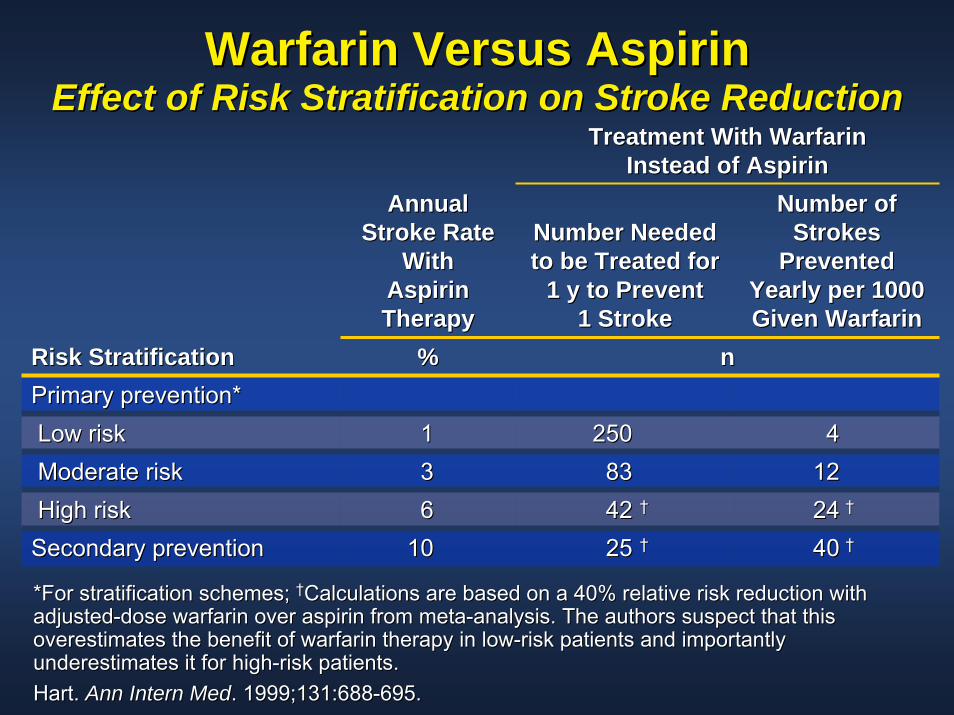
Warfarin Versus AspirinWarfarin Versus AspirinEffect of Risk Stratification on Stroke ReductionEffect of Risk Stratification on Stroke Reduction
Treatment With Warfarin Treatment With Warfarin Instead of AspirinInstead of Aspirin
Number Needed Number Needed to be Treated for to be Treated for
1 y to Prevent 1 y to Prevent 1 Stroke1 Stroke
Number of Number of Strokes Strokes
Prevented Prevented Yearly per 1000 Yearly per 1000 Given WarfarinGiven Warfarin
Risk StratificationRisk Stratification %% nnPrimary prevention*Primary prevention*Low riskLow risk 11 250250 44Moderate riskModerate risk 33 8383 1212High riskHigh risk 66 4242 †† 2424 ††
Secondary preventionSecondary prevention 1010 2525 †† 4040 ††
Annual Annual Stroke Rate Stroke Rate
With With Aspirin Aspirin TherapyTherapy
*For stratification schemes; *For stratification schemes; ††Calculations are based on a 40% relative risk reduction with Calculations are based on a 40% relative risk reduction with adjustedadjusted--dose warfarin over aspirin from metadose warfarin over aspirin from meta--analysis. The authors suspect that this analysis. The authors suspect that this overestimates the benefit of warfarin therapy in lowoverestimates the benefit of warfarin therapy in low--risk patients and importantly risk patients and importantly underestimates it for highunderestimates it for high--risk patients.risk patients.Hart. Hart. Ann Intern MedAnn Intern Med. 1999;131:688. 1999;131:688--695.695.
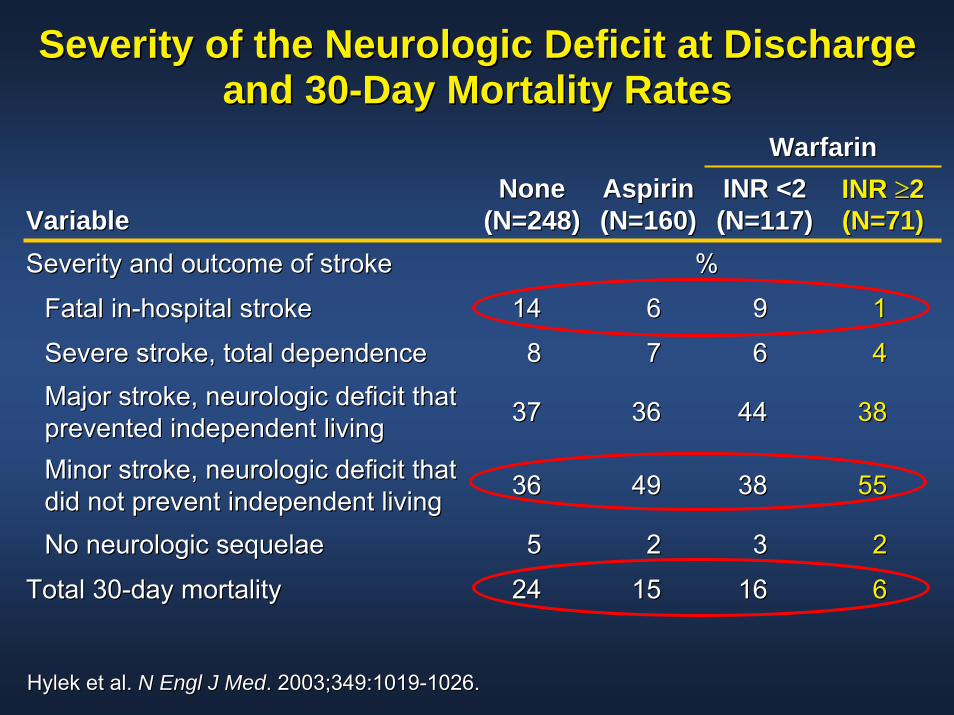
Severity of the Neurologic Deficit at Discharge Severity of the Neurologic Deficit at Discharge and 30and 30--Day Mortality RatesDay Mortality Rates
WarfarinWarfarin
VariableVariableNoneNone
(N=248)(N=248)AspirinAspirin(N=160)(N=160)
INR <2INR <2(N=117)(N=117)
INR INR ≥≥22(N=71)(N=71)
Severity and outcome of strokeSeverity and outcome of stroke %%
Fatal inFatal in--hospital strokehospital stroke 1414 66 99 11
Severe stroke, total dependenceSevere stroke, total dependence 88 77 66 44
Major stroke, neurologic deficit that Major stroke, neurologic deficit that prevented independent livingprevented independent living 3737 3636 4444 3838
Minor stroke, neurologic deficit that Minor stroke, neurologic deficit that did not prevent independent livingdid not prevent independent living 3636 4949 3838 5555
No neurologic sequelaeNo neurologic sequelae 55 22 33 22
Total 30Total 30--day mortalityday mortality 2424 1515 1616 66
Hylek et al. Hylek et al. N Engl J MedN Engl J Med. 2003;349:1019. 2003;349:1019--1026.1026.
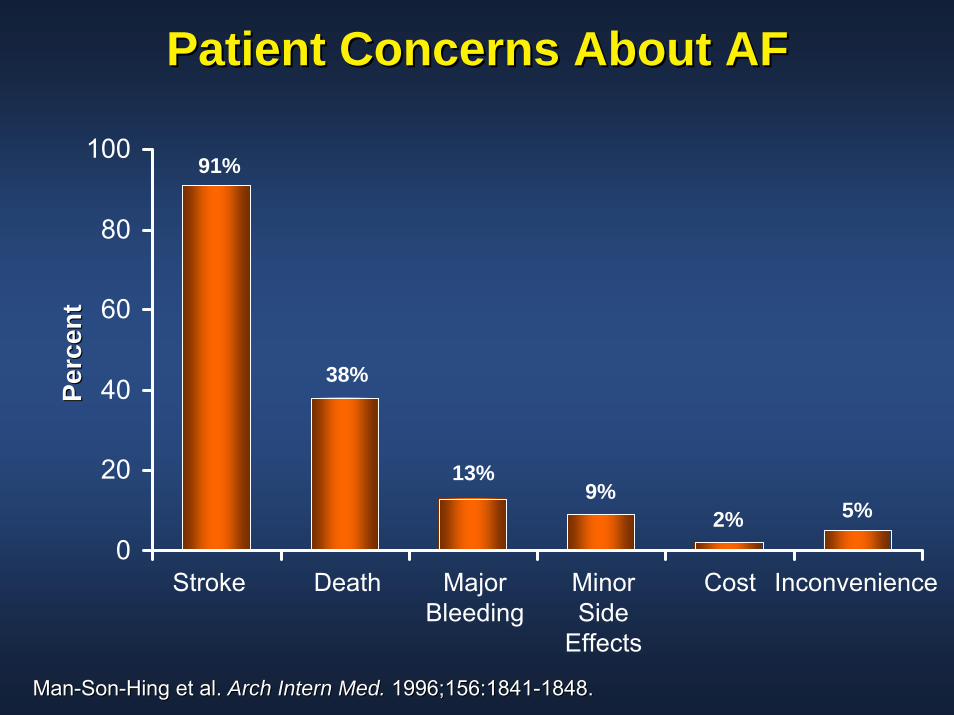
Patient Concerns About AFPatient Concerns About AF
0
20
40
60
80
100
Stroke Death Major Bleeding
InconvenienceMinor Side
Effects
Cost
Perc
ent
Perc
ent
91%
38%
13%9%
2% 5%
ManMan--SonSon--Hing et al. Hing et al. Arch Intern Med.Arch Intern Med. 1996;156:18411996;156:1841--1848.1848.
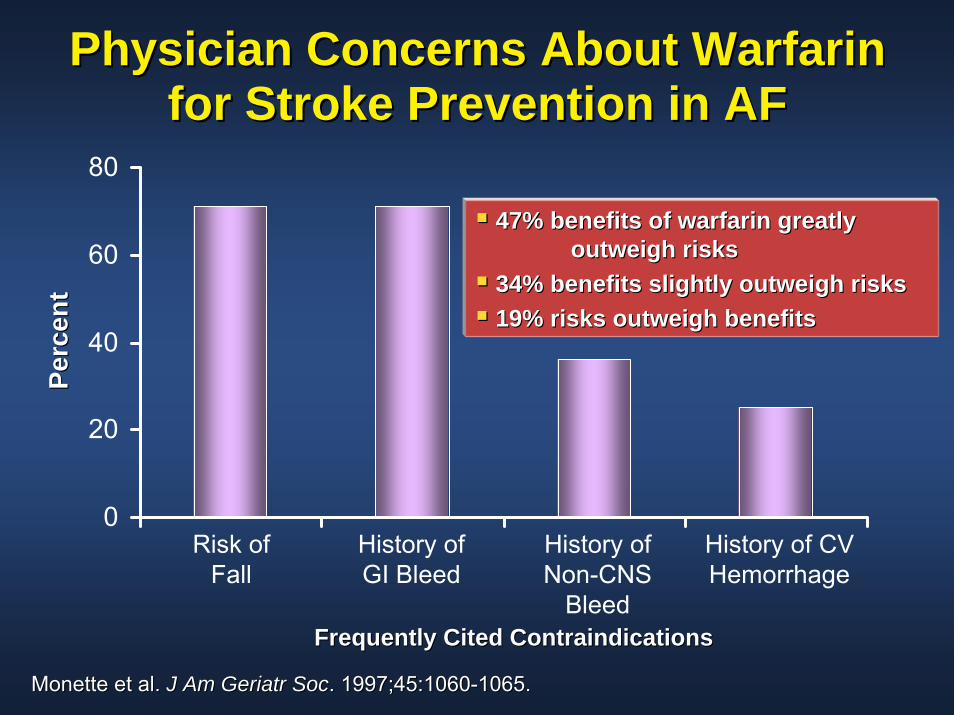
Physician Concerns About Warfarin Physician Concerns About Warfarin for Stroke Prevention in AFfor Stroke Prevention in AF
0
20
40
60
80
Risk of Fall
History of GI Bleed
History of Non-CNS
Bleed
History of CV Hemorrhage
47% benefits of warfarin greatly 47% benefits of warfarin greatly outweigh risksoutweigh risks
34% benefits slightly outweigh risks34% benefits slightly outweigh risks19% risks outweigh benefits19% risks outweigh benefits
Frequently Cited ContraindicationsFrequently Cited Contraindications
Perc
ent
Perc
ent
Monette et al. Monette et al. J Am Geriatr SocJ Am Geriatr Soc. 1997;45:1060. 1997;45:1060--1065.1065.
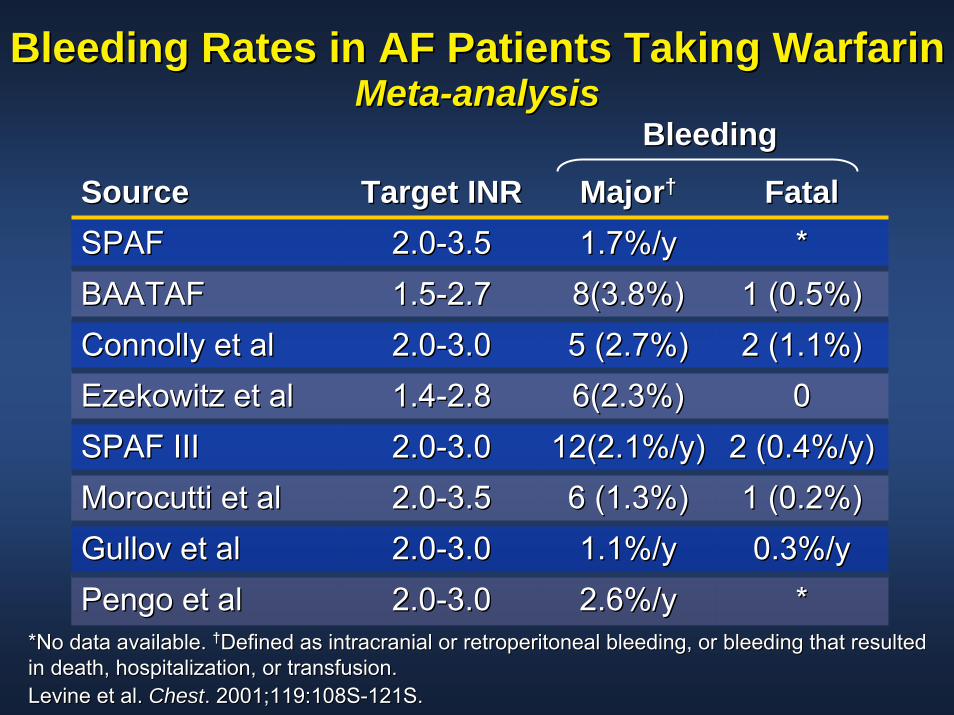
Bleeding Rates in AF Patients Taking WarfarinBleeding Rates in AF Patients Taking WarfarinMetaMeta--analysisanalysis
SourceSource Target INRTarget INR MajorMajor†† FatalFatalSPAFSPAF 2.02.0--3.53.5 1.7%/y1.7%/y **BAATAFBAATAF 1.51.5--2.72.7 8(3.8%)8(3.8%) 1 (0.5%)1 (0.5%)Connolly et alConnolly et al 2.02.0--3.03.0 5 (2.7%)5 (2.7%) 2 (1.1%)2 (1.1%)Ezekowitz et alEzekowitz et al 1.41.4--2.82.8 6(2.3%)6(2.3%) 00SPAF IIISPAF III 2.02.0--3.03.0 12(2.1%/y)12(2.1%/y) 2 (0.4%/y)2 (0.4%/y)Morocutti et alMorocutti et al 2.02.0--3.53.5 6 (1.3%)6 (1.3%) 1 (0.2%)1 (0.2%)Gullov et alGullov et al 2.02.0--3.03.0 1.1%/y1.1%/y 0.3%/y0.3%/yPengo et alPengo et al 2.02.0--3.03.0 2.6%/y2.6%/y **
BleedingBleeding
*No data available. *No data available. ††Defined as intracranial or retroperitoneal bleeding, or bleedingDefined as intracranial or retroperitoneal bleeding, or bleeding that resulted that resulted in death, hospitalization, or transfusion.in death, hospitalization, or transfusion.Levine et al. Levine et al. ChestChest. 2001;119:108S. 2001;119:108S--121S.121S.

Intracranial Hemorrhage During LongIntracranial Hemorrhage During Long--Term Anticoagulation With WarfarinTerm Anticoagulation With Warfarin
0.00.20.40.60.81.01.21.41.61.82.0
*PV=prosthetic valves.*PV=prosthetic valves.Levine et al. Levine et al. ChestChest. 2001;119:108S. 2001;119:108S--121S.121S.
ICH
%/Y
ear
ICH
%/Y
ear
Fihn Fihn (AF)(AF)
INRINR<3.0<3.0
INRINR<3.0<3.0
Fihn Fihn (>75)(>75)
Turpie Turpie (PV*)(PV*)
SPAF SPAF ((≤≤75)75)
SPAF SPAF (AF)(AF)
PengoPengo(PV*)(PV*)
SPAF SPAF ((>>75)75)
SPAF SPAF III (AF)III (AF)
INRINR2.02.0--4.54.5
INRINR2.02.0--3.03.0 INRINR
2.52.5--3.53.5
INRINR3.03.0--4.54.5
INRINR2.02.0--4.54.5
INRINR2.02.0--4.54.5
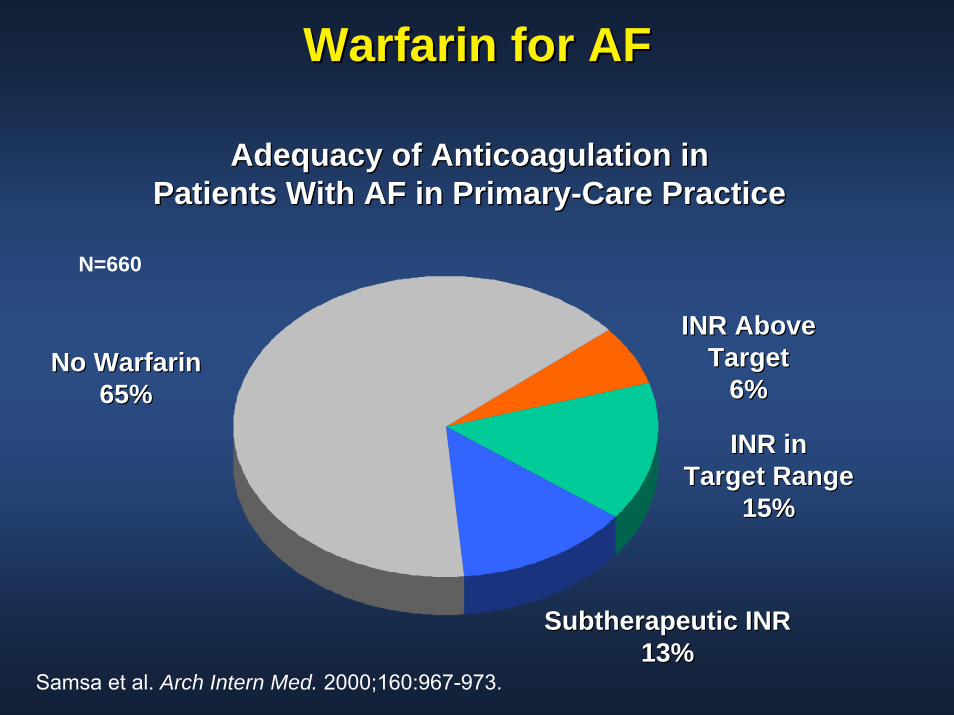
Warfarin for AFWarfarin for AF
Adequacy of Anticoagulation inAdequacy of Anticoagulation inPatients With AF in PrimaryPatients With AF in Primary--Care PracticeCare Practice
Samsa et al. Arch Intern Med. 2000;160:967-973.
INR Above INR Above TargetTarget
6%6%
Subtherapeutic INR Subtherapeutic INR 13%13%
INR inINR inTarget RangeTarget Range
15%15%
No WarfarinNo Warfarin65%65%
N=660
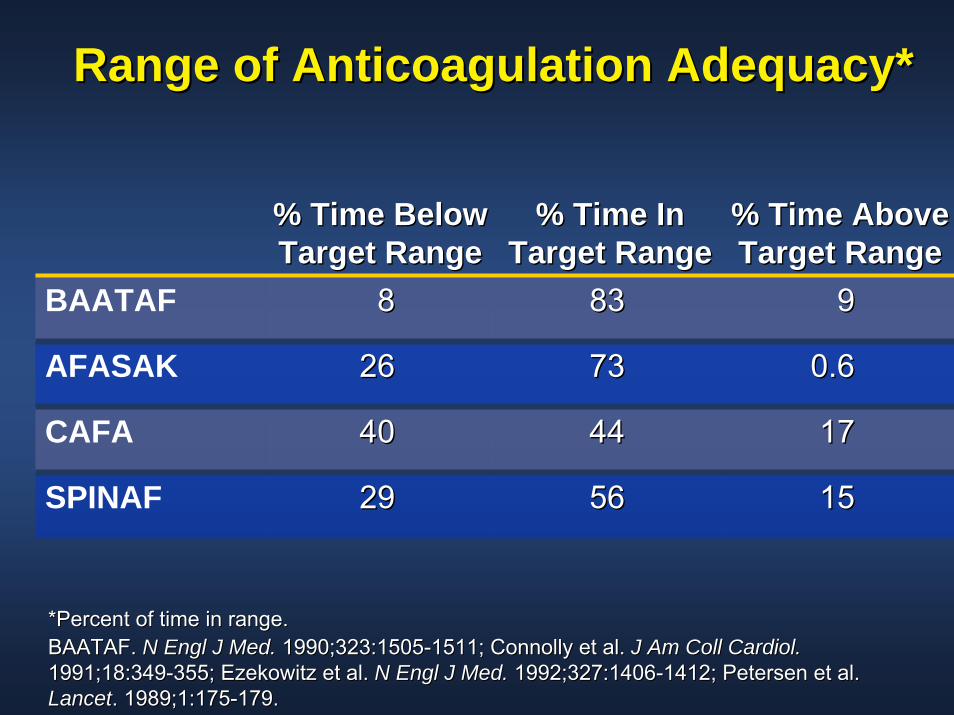
Range of Anticoagulation Adequacy*Range of Anticoagulation Adequacy*
% Time Below % Time Below Target RangeTarget Range
% Time In % Time In Target RangeTarget Range
% Time Above % Time Above Target RangeTarget Range
BAATAF 88 8383 99
AFASAK 2626 7373 0.60.6
CAFA 4040 4444 1717
SPINAF 2929 5656 1515
*Percent of time in range.*Percent of time in range.BAATAF. BAATAF. N Engl J Med.N Engl J Med. 1990;323:15051990;323:1505--1511; Connolly et al. 1511; Connolly et al. J Am Coll Cardiol.J Am Coll Cardiol.1991;18:3491991;18:349--355; Ezekowitz et al. 355; Ezekowitz et al. N Engl J Med.N Engl J Med. 1992;327:14061992;327:1406--1412; Petersen et al. 1412; Petersen et al. LancetLancet. 1989;1:175. 1989;1:175--179.179.
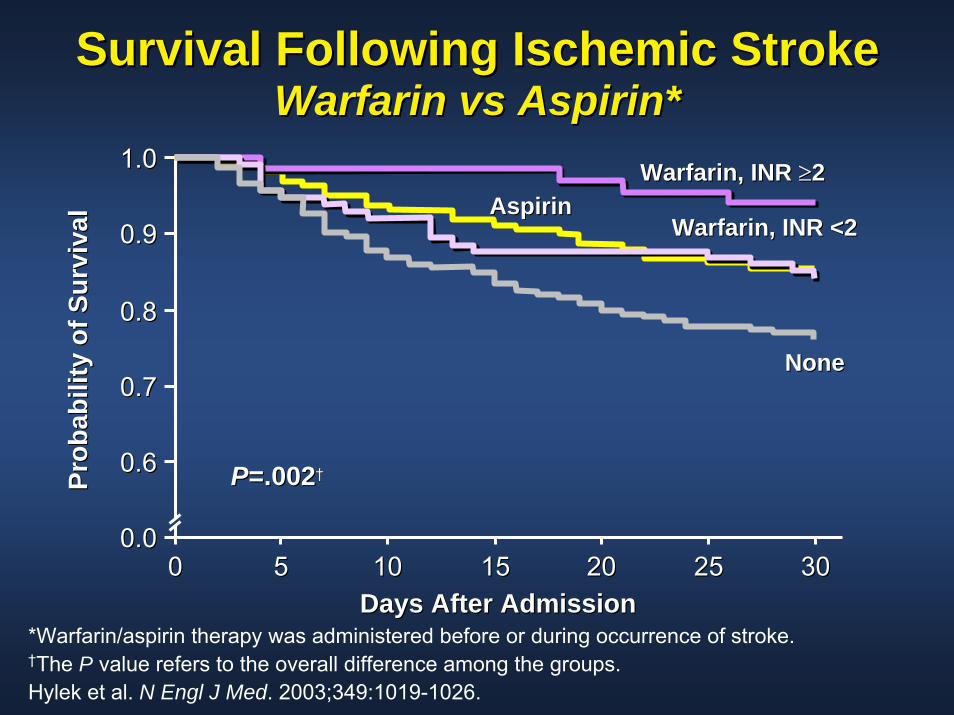
Survival Following Ischemic StrokeSurvival Following Ischemic StrokeWarfarin vs Aspirin*Warfarin vs Aspirin*
1.01.0
Prob
abili
ty o
f Sur
viva
lPr
obab
ility
of S
urvi
val
0.90.9
0.80.8
0.70.7
0.60.6
0.00.000 55 1010 1515 2020 2525
PP=.002=.002††
Warfarin, INR Warfarin, INR ≥≥22AspirinAspirin
Warfarin, INR Warfarin, INR <2<2
NoneNone
3030Days After AdmissionDays After Admission
*Warfarin/aspirin therapy was administered before or during occurrence of stroke.††The P value refers to the overall difference among the groups.Hylek et al. N Engl J Med. 2003;349:1019-1026.
SummarySummaryRisk factors place this patient in an intermediate Risk factors place this patient in an intermediate ––high risk high risk category for risk of stroke.category for risk of stroke.
Stroke risk ranges from 2Stroke risk ranges from 2--5% without therapy.5% without therapy.
Aspirin reduces stroke risk to 0.5Aspirin reduces stroke risk to 0.5--4%.4%.
Warfarin reduces stroke risk to 1.7%.Warfarin reduces stroke risk to 1.7%.
Risk of major bleeding with warfarin is 1Risk of major bleeding with warfarin is 1--3% in general. 3% in general. Risk of ICH in Risk of ICH in thisthis patient is 0.5%. patient is 0.5%.
Risk of major bleeding with ASA is 1Risk of major bleeding with ASA is 1--2% overall.2% overall.
If patient preference favors avoiding stroke despite If patient preference favors avoiding stroke despite inconvenience and risk of bleeding, anticoagulate with inconvenience and risk of bleeding, anticoagulate with warfarin warfarin –– otherwise too close too call. otherwise too close too call.

64 year-old woman w/ Afib and HTN
Brian F. Gage, MD, [email protected]
Associate Professor of Medicine,Washington University, St. Louis

No conflicts of interest
Background
• Over 2 million Americans have atrial fibrillation
• Without antithrombotic therapy their stroke rate is increased 4- to 5-fold
• Stroke is the leading cause of adult disability and the third most common cause of death in Americans

CHADS2
• Congestive Heart Failure (1 pt.)• Hypertension (1 pt.)• Age>75 (1 pt.)• Diabetes (1 pt.)• Stroke History (2 pts.)
With 1 point, expect 2.2 (95% CI: 1.6-3.1) strokes/100 pt-yrs ASA (Gage et al. Circulation 2004)
Efficacy in Clinical Trials• In randomized, controlled trials warfarin reduced
ischemic stroke rate by 65% (hazard ratio 0.35)compared to no antithrombotic therapy
HOWEVER: • Trials excluded over 90% of patients
- Esp. patients with contraindications to warfarin (e.g. neuropsychiatric disease, poor compliance, risk for falls)
• Patients in trials are followed more meticulously than in real-life settings
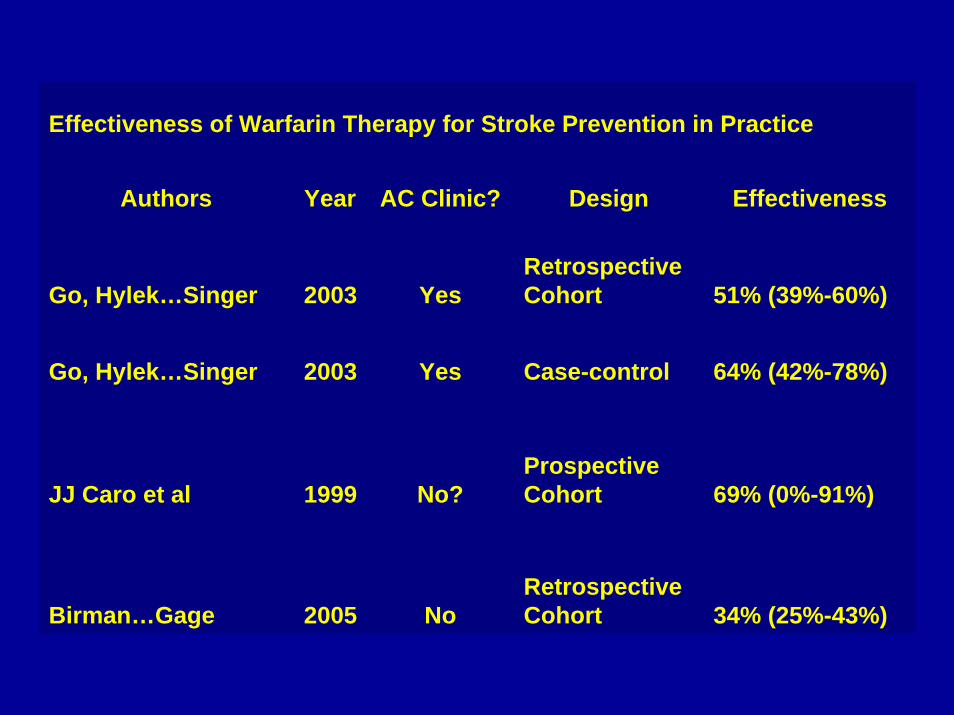
Effectiveness of Warfarin Therapy for Stroke Prevention in Practice
Authors Year AC Clinic? Design Effectiveness
Go, Hylek…Singer 2003 YesRetrospective Cohort 51% (39%-60%)
Go, Hylek…Singer 2003 Yes Case-control 64% (42%-78%)
JJ Caro et al 1999 No?Prospective Cohort 69% (0%-91%)
Birman…Gage 2005 NoRetrospective Cohort 34% (25%-43%)
Subjects and Data Source for Birman-Deych…Gage study
• Subjects: National sample of 23,657 Medicare beneficiaries hospitalized between 04/01/1998 and 03/31/1999 with Atrial Fibrillation
• Data Sources:– Medical chart review (baseline hospitalization) to confirm the
presence of AF and stroke risk factors
– Medicare claims records (baseline and follow-up) for warfarin Rx and validated ICD-9-CM claims for stroke
• For details see poster #23 at session 3, “Real-world effectiveness of warfarin therapy for stroke prevention in Medicare beneficiaries of all races”

0
0.2
0.4
0.6
0.8
1
Go, Hyle
k…Singer
Go, Hyle
k…Singer
JJ Caro
et al
Birman-
Deych…Gage
RR
R W
arfa
rin
for
Stro
ke P
reve
ntio
n
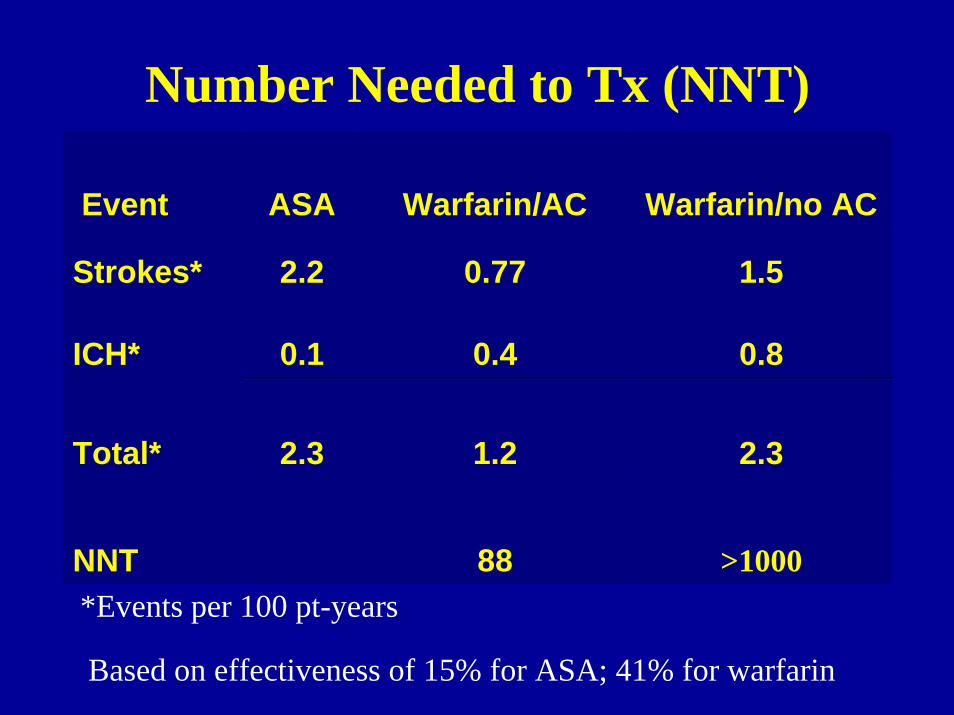
Number Needed to Tx (NNT)
Event ASA Warfarin/AC Warfarin/no AC
Strokes* 2.2 0.77 1.5
ICH* 0.1 0.4 0.8
Total* 2.3 1.2 2.3
NNT 88 >1000*Events per 100 pt-years
Based on effectiveness of 15% for ASA; 41% for warfarin
Conclusions
• For patients with a CHADS2 score of 1, the decision to prescribe warfarin depends on:– The effectiveness of warfarin in the clinical setting– The risk of bleeding (esp. ICH) in the clinical setting– The patient’s preferences for taking warfarin vs. ASA– Possibly other side-effects of these antithrombotic
therapies (e.g. increased osteoporosis?, prevention of MI)