Embed Size (px)
Citation preview
Controversies
in Breast
PathologyELENA PROVENZANO
ADDENBROOKES HOSPITAL, CAMBRIDGE
Neoadjuvant
Chemotherapy
Indications:
• Management of locally advanced invasive breast cancers including inflammatory breast cancer
• ‘Down-staging’ of large inoperable cancers to permit surgical
resection
• Routine management of women with high risk disease who
would require adjuvant chemotherapy based on biological
tumour characteristics and clinical-radiological findings
Prognostic factors post NACT –
Size matters
• Complete pathological response
• Pre treatment histological grade
• Post treatment histological grade
• Residual tumour size
• Residual tumour cellularity
• Lymphovascular space invasion
• Number of lymph nodes containing metastatic carcinoma
• Size of metastases
• Evidence of chemotherapy effect in lymph nodes
• TILs (tumour infiltrating lymphocytes)
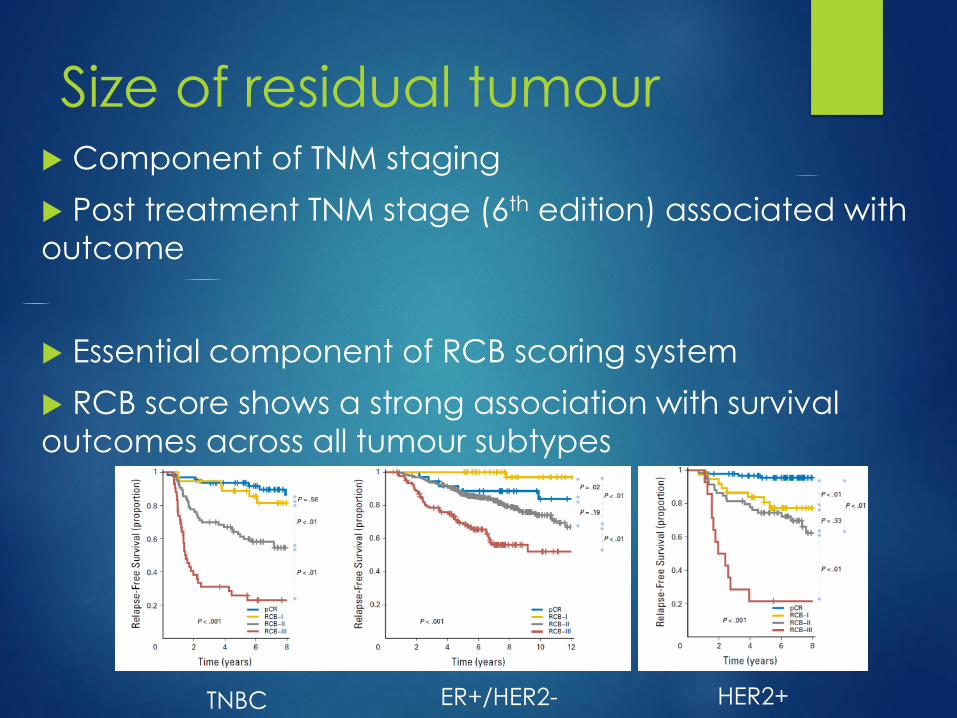
Size of residual tumour Component of TNM staging
Post treatment TNM stage (6th edition) associated with
outcome
Essential component of RCB scoring system
RCB score shows a strong association with survival
outcomes across all tumour subtypes
TNBC HER2+ER+/HER2-
Measuring Size Post NACT
Thorough macroscopic (gross) assessment of the
specimen critical for accurate classification of pCR and
assessment of size post NACT
A multidisciplinary approach with adequate clinical
information and access to imaging results is essential
Close clinical/ radiological correlation to map the
precise location of the tumour bed is preferable to
exhaustive blind sampling
Placement of a marker clip at the time of diagnosis is
very helpful in the event of an excellent response to
treatment
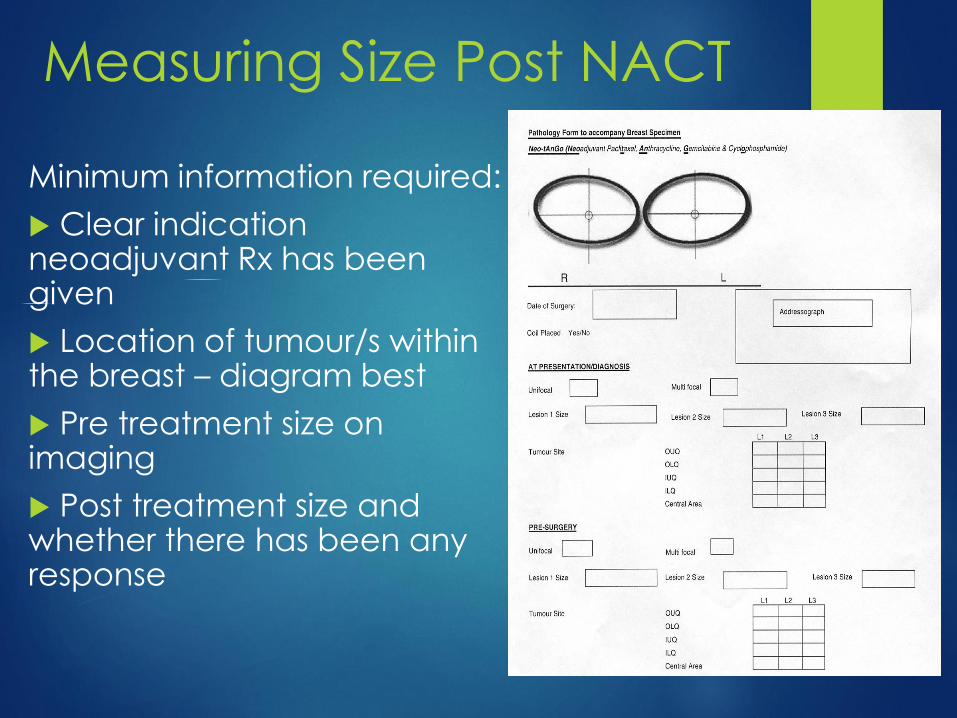
Measuring Size Post NACT
Minimum information required:
Clear indication neoadjuvant Rx has been given
Location of tumour/s within the breast – diagram best
Pre treatment size on imaging
Post treatment size and whether there has been any response
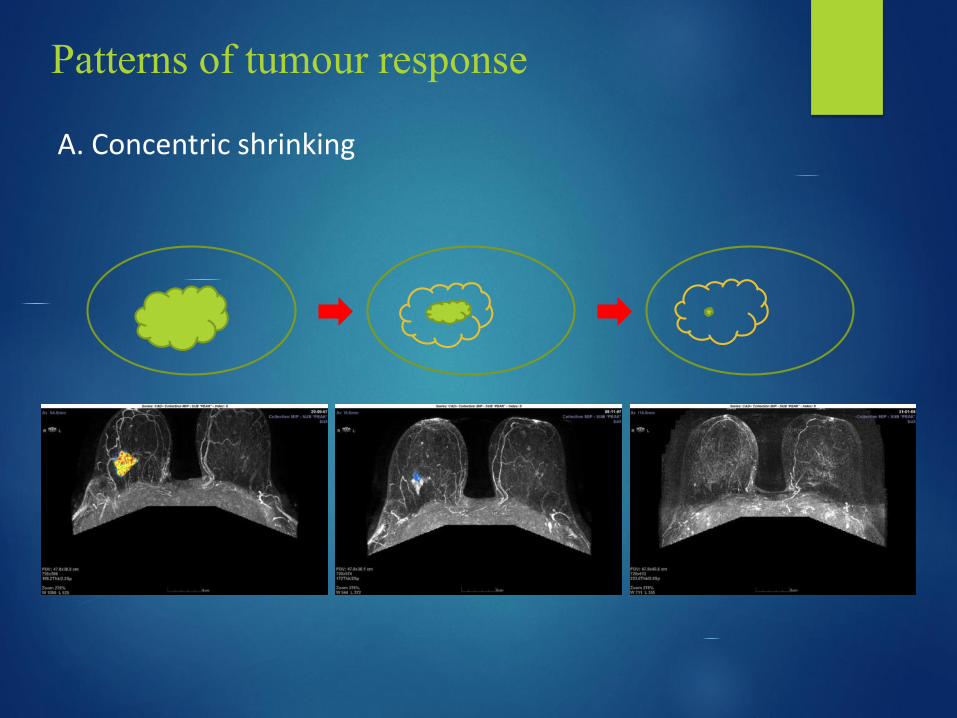
A. Concentric shrinking
Patterns of tumour response
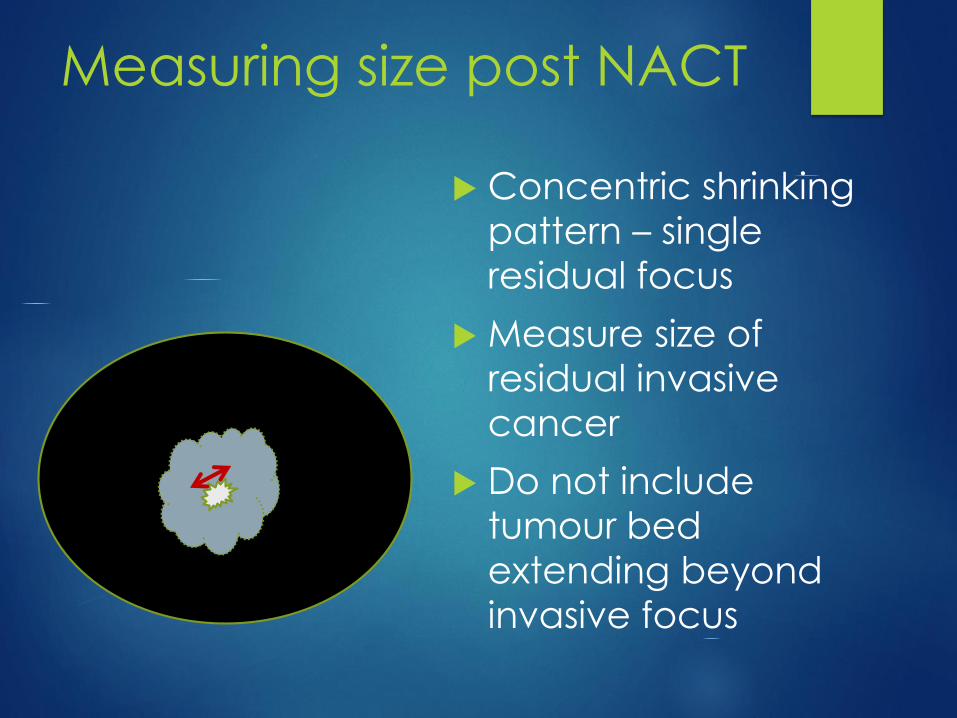
Measuring size post NACT
Concentric shrinking
pattern – single
residual focus
Measure size of
residual invasive
cancer
Do not include
tumour bed
extending beyond
invasive focus
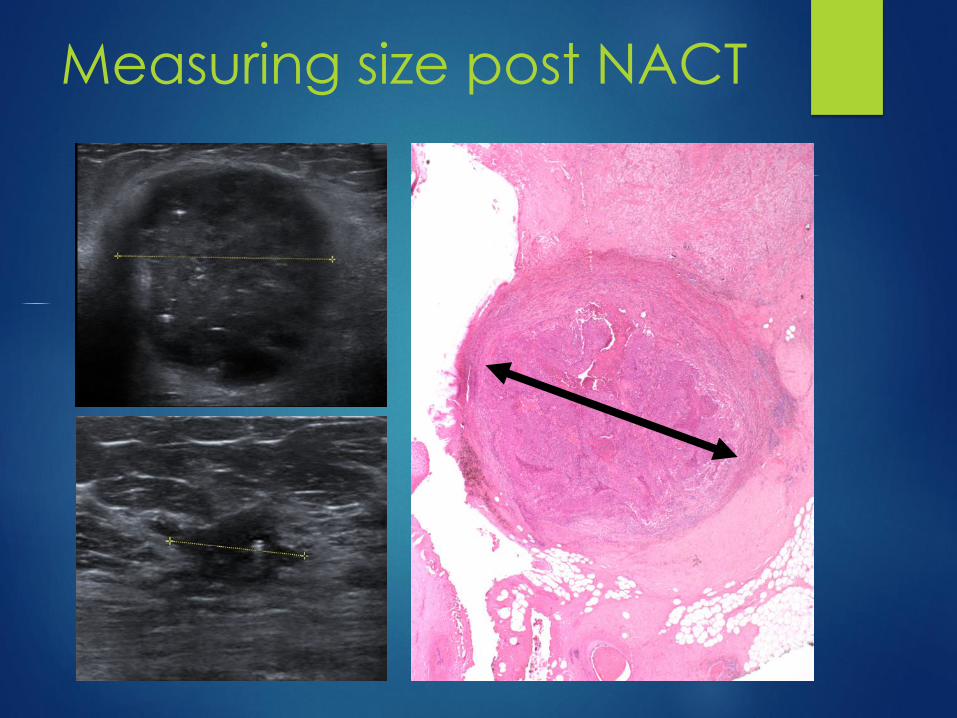
Measuring size post NACT
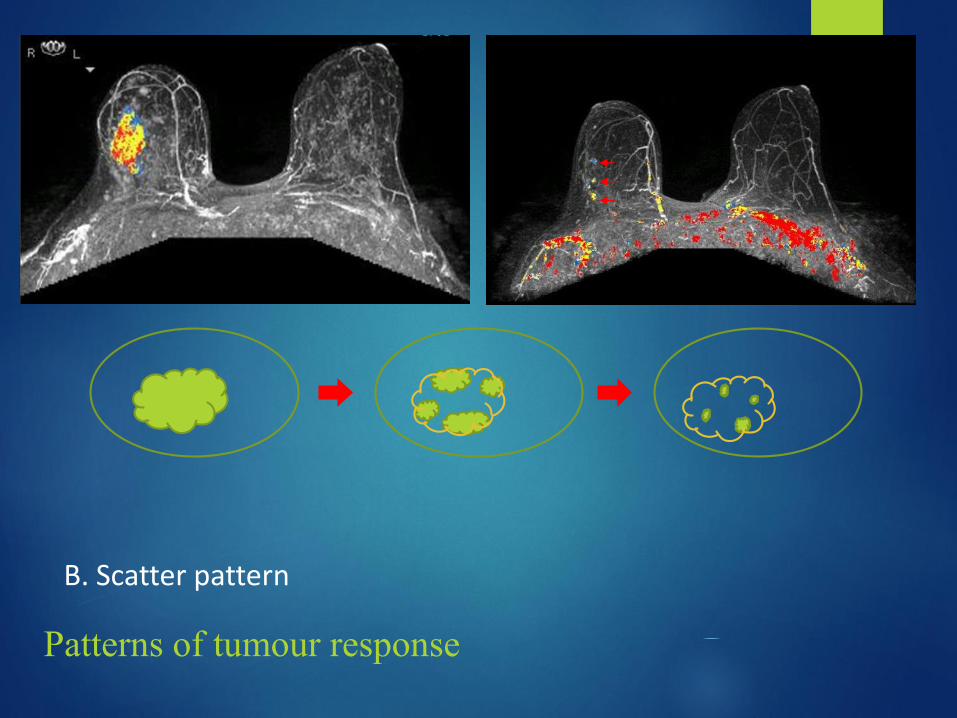
B. Scatter pattern
Patterns of tumour response
Measuring size post NACT
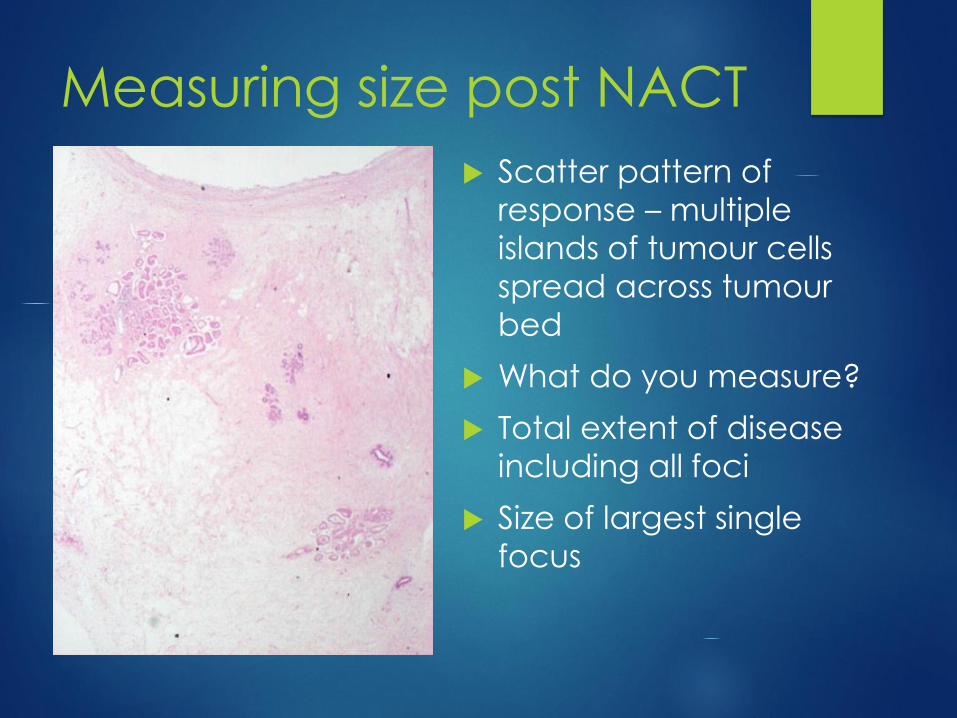
Scatter pattern of
response – multiple
islands of tumour cells
spread across tumour
bed
What do you measure?
Total extent of disease
including all foci
Size of largest single
focus
Measuring size post NACT
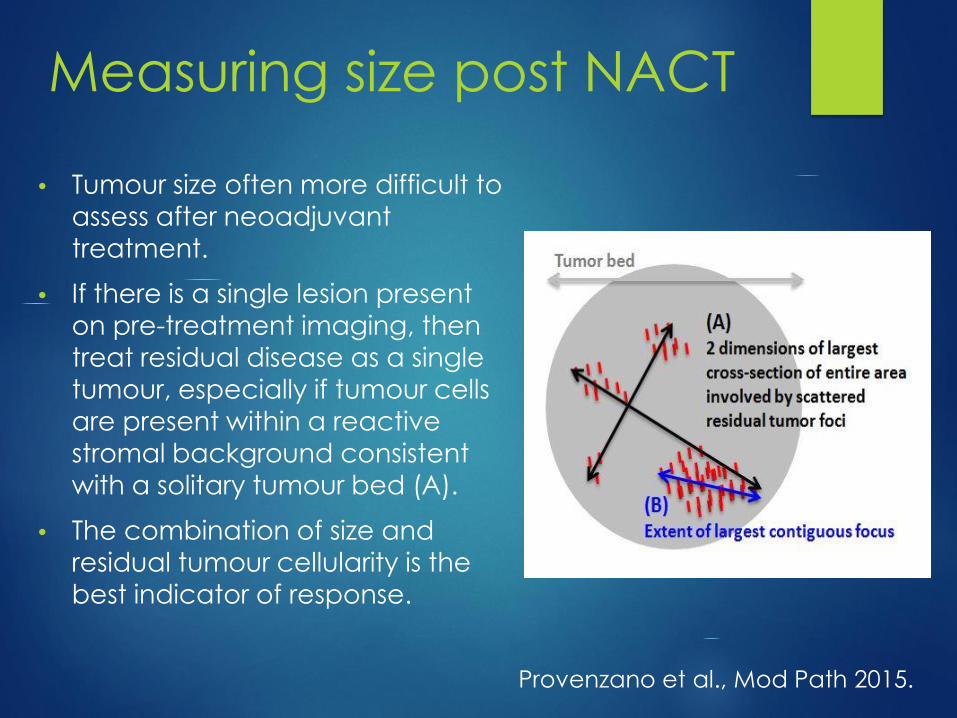
• Tumour size often more difficult to
assess after neoadjuvant
treatment.
• If there is a single lesion present
on pre-treatment imaging, then
treat residual disease as a single
tumour, especially if tumour cells
are present within a reactive stromal background consistent
with a solitary tumour bed (A).
• The combination of size and
residual tumour cellularity is the best indicator of response.
Provenzano et al., Mod Path 2015.
Measuring size post NACT
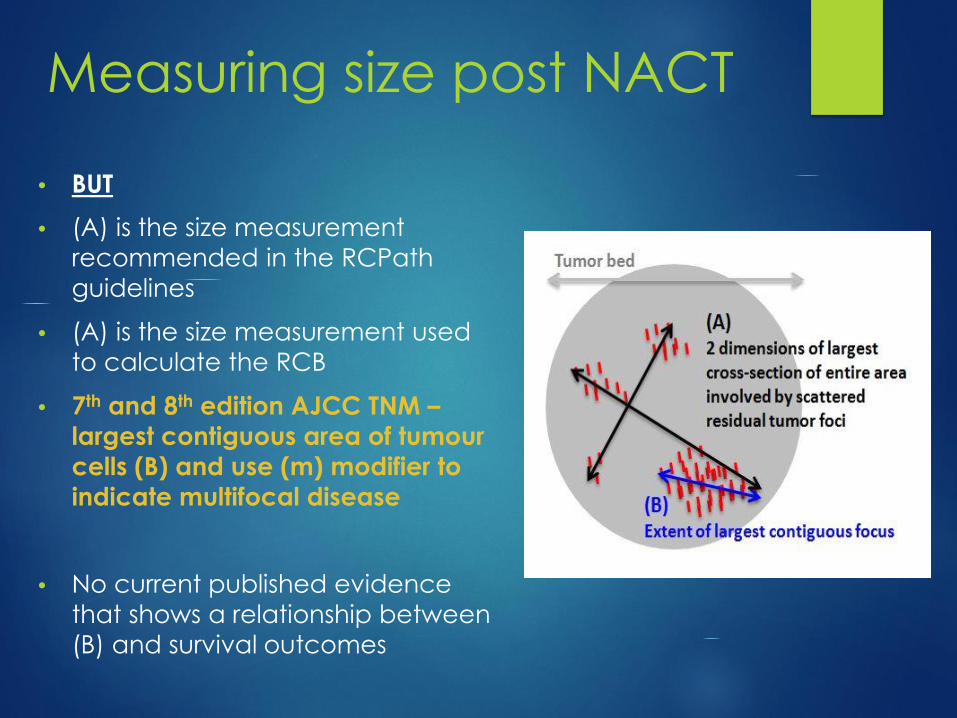
• BUT
• (A) is the size measurement
recommended in the RCPath
guidelines
• (A) is the size measurement used
to calculate the RCB
• 7th and 8th edition AJCC TNM –
largest contiguous area of tumour
cells (B) and use (m) modifier to
indicate multifocal disease
• No current published evidence
that shows a relationship between
(B) and survival outcomes
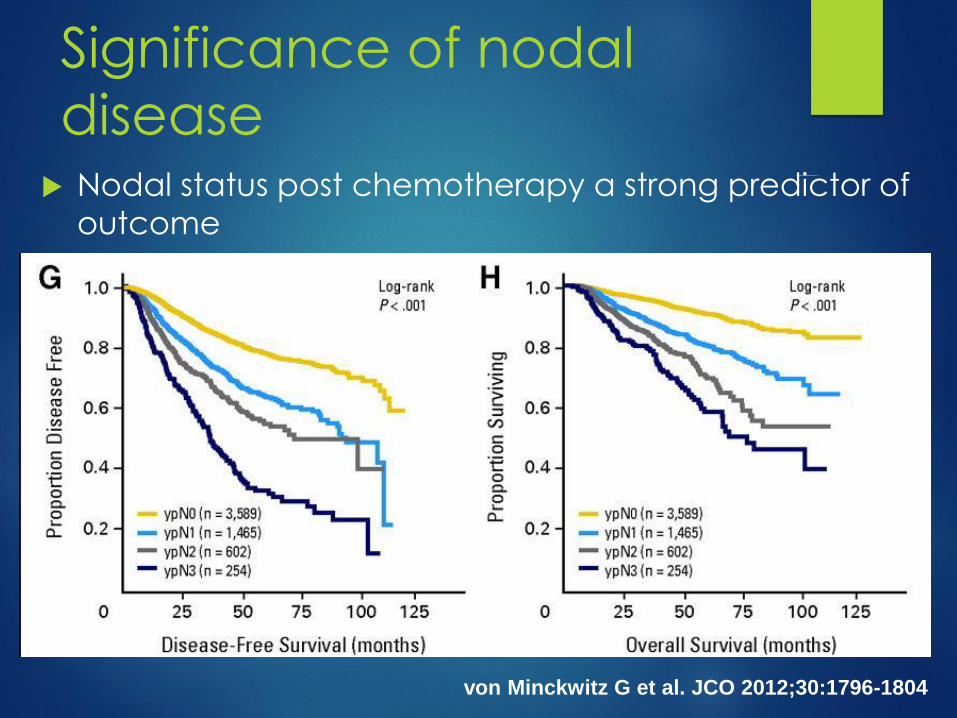
Significance of nodal
disease Nodal status post chemotherapy a strong predictor of
outcome
von Minckwitz G et al. JCO 2012;30:1796-1804
Significance of nodal
disease
Hennessy et al., J Clin Oncol 2005;23:9304-11
403 pts proven node pos
22% axillary pCR, 69% also pCR breast
Axillary conversion the MOST significant predictor of OS
Size of residual breast tumour NOT predictive if residual
nodal disease
No influence of size of metastasis – prognosis still worse if <
0.1 mm
Evidence of nodal response associated with improved DFS

Significance of nodal
disease Cure et al., Breast Ca Res Treatment 2002;76(1):37-45
277 pts, tumours > 3 cm
39% clinically node pos -> ypN0
Number of positive nodes post chemo strongest predictor of survival
Klauber DeMore et al., Ann Surg Oncol 2006;13:685-91
122 pts, 52% node positive pre chemo
Worse DFS/ OS with increased number of nodes and increasing size of metastasis
Size of largest metastasis the strongest predictor of survival on multivariate analysis
ITC’s regarded as node positive

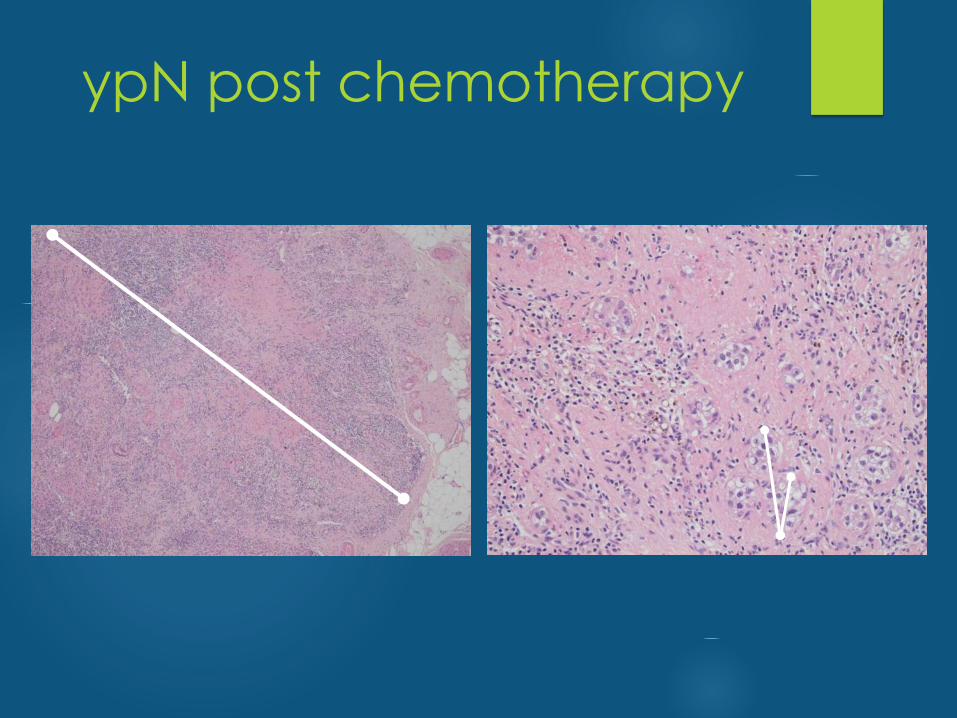
ITC’s post chemotherapy
Presence of isolated tumour cells in lymph nodes
TNM – call ypN0(i) BUT not pCR
WHO/ RCPath – call node positive i.e. NOT pCR
do NOT regard as pCR – nodal equivalent of minimal
residual disease
often background fibrosis indicating previous
macrometastatic disease with regression
measure size of entire deposit including intervening
fibrosis**

ypN post NACTNew definition in 8th edition TNM – introduced beginning 2018
Size of the largest contiguous focus of residual tumour in the node
Any treatment associated fibrosis should NOT be included
A description of number of foci present and total distance over
which they extend may be helpful for clinicians to determine extent
of residual disease
Deposit ≤ 0.2 mm is ypT0(i+); NOT regarded as pCR
This is NOT the measurement of size of metastasis used in the RCB,
which is the largest deposit INCLUDING associated treatment
related fibrosis
No evidence in literature associating nodal status measured in
this way with survival
ypN post chemotherapy
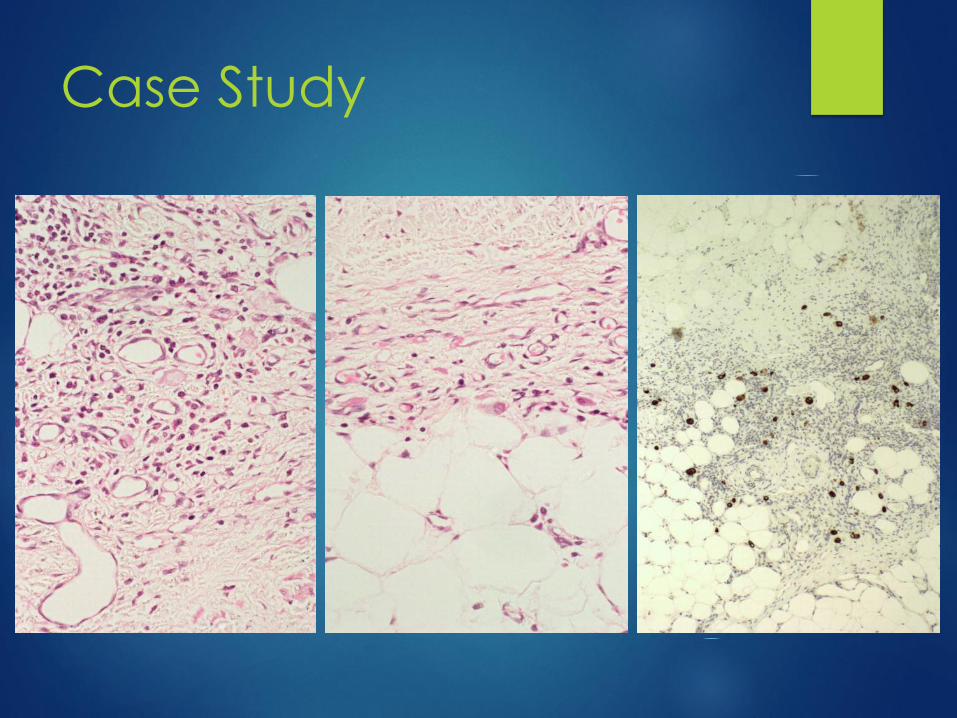
Case study
55 yo female.
Inflammatory breast cancer.
Neoadjuvant chemotherapy on NeotAnGo
trial.
Post treatment mastectomy and axillary
clearance.
Case study
30 mm residual invasive lobular carcinoma
Partial response to neoadjuvant
chemotherapy
7/11 nodes with metastatic carcinoma in
the form of scattered single cells within
background fibrosis
Case Study
How do you report nodal status in this
case?
A. Measure excluding fibrosis = ITCs - Negative
[ypN0(i+)] but not pCR = ypTNM
B. Measure entire deposit including fibrosis -
Positive [ypN2] and not pCR = RCPath/ RCB
Would you recommend regional nodal
irradiation for this patient
Take Home Points
Changes in the way size of tumour and
metastases measured in latest TNM
Size measurement used for TNM not
the same as size measurement used for
RCB or recommended way of
measuring size in RCPath guidelines
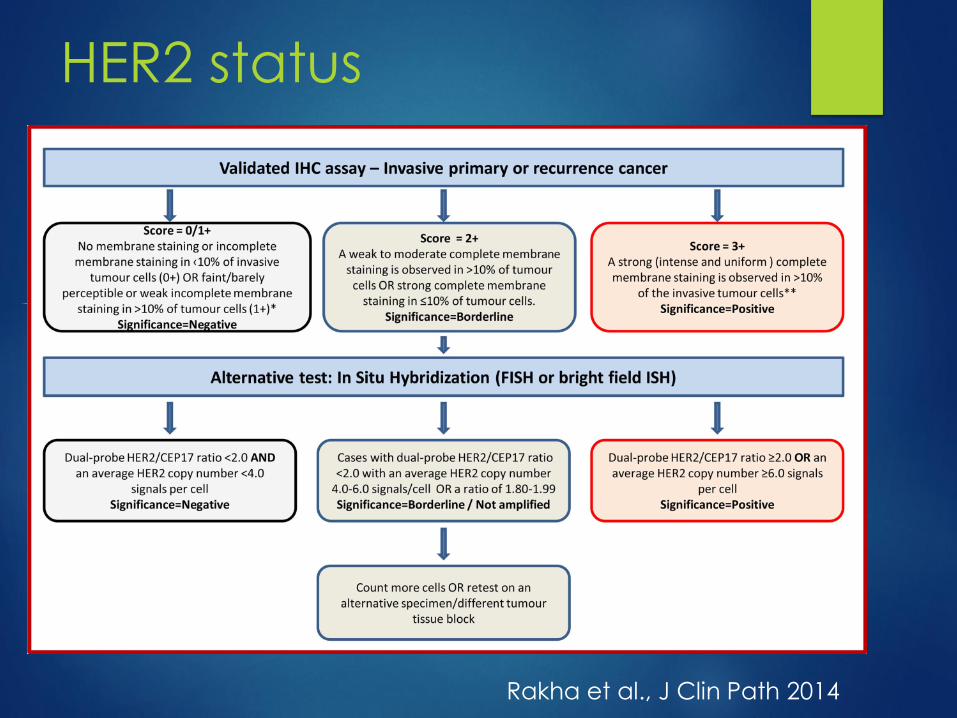
HER2 status
Rakha et al., J Clin Path 2014

HER2 status
3+ 2+
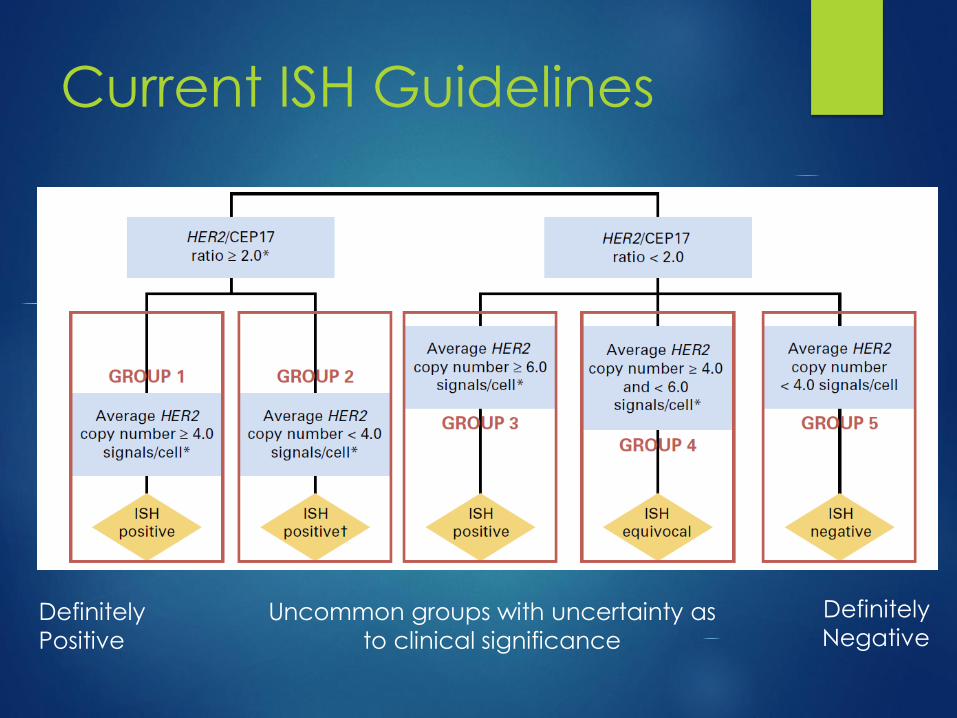
Current ISH Guidelines
Definitely
Positive
Uncommon groups with uncertainty as
to clinical significance
Definitely
Negative
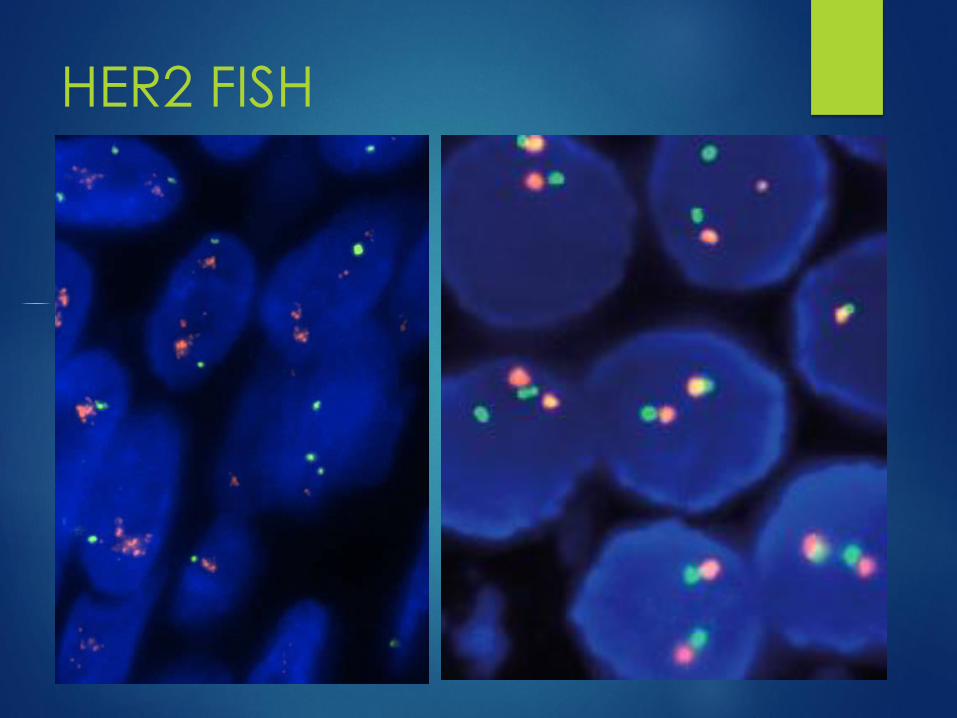
HER2 FISH
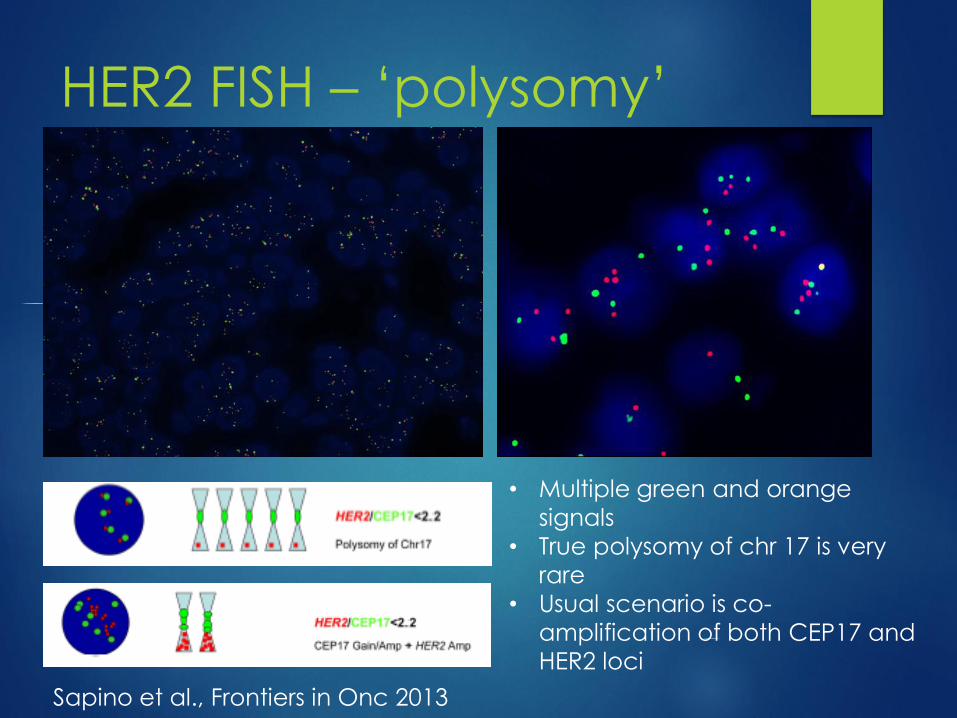
HER2 FISH – ‘polysomy’
• Multiple green and orange
signals
• True polysomy of chr 17 is very
rare
• Usual scenario is co-
amplification of both CEP17 and
HER2 loci
Sapino et al., Frontiers in Onc 2013

HER2 FISH – CEP 17
monosomy
Only one green signal
due to loss of the
CEP17 site
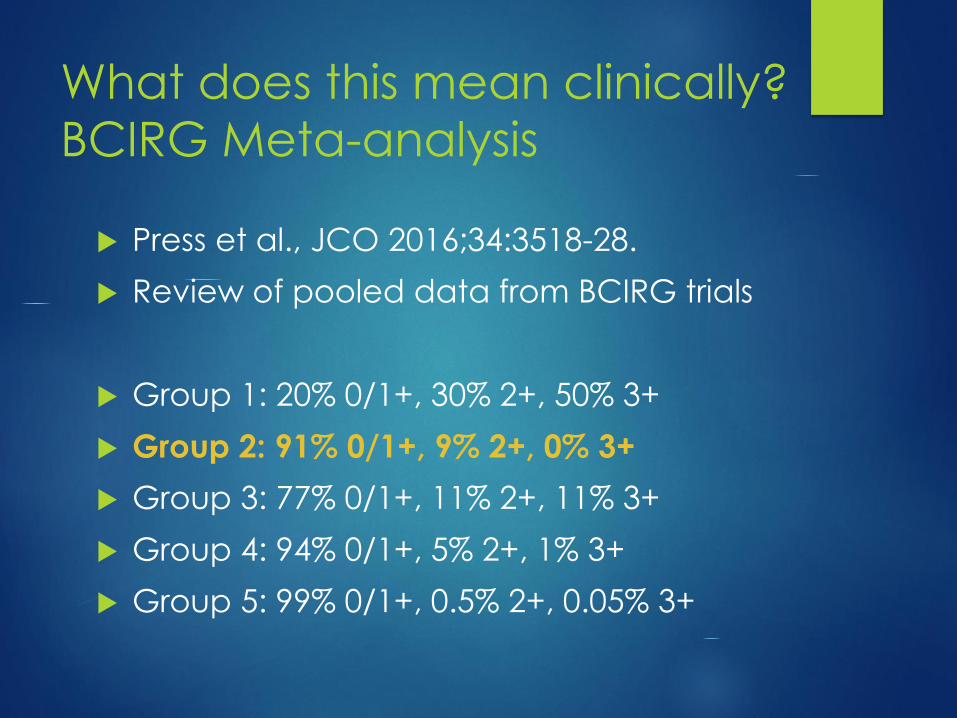
What does this mean clinically?
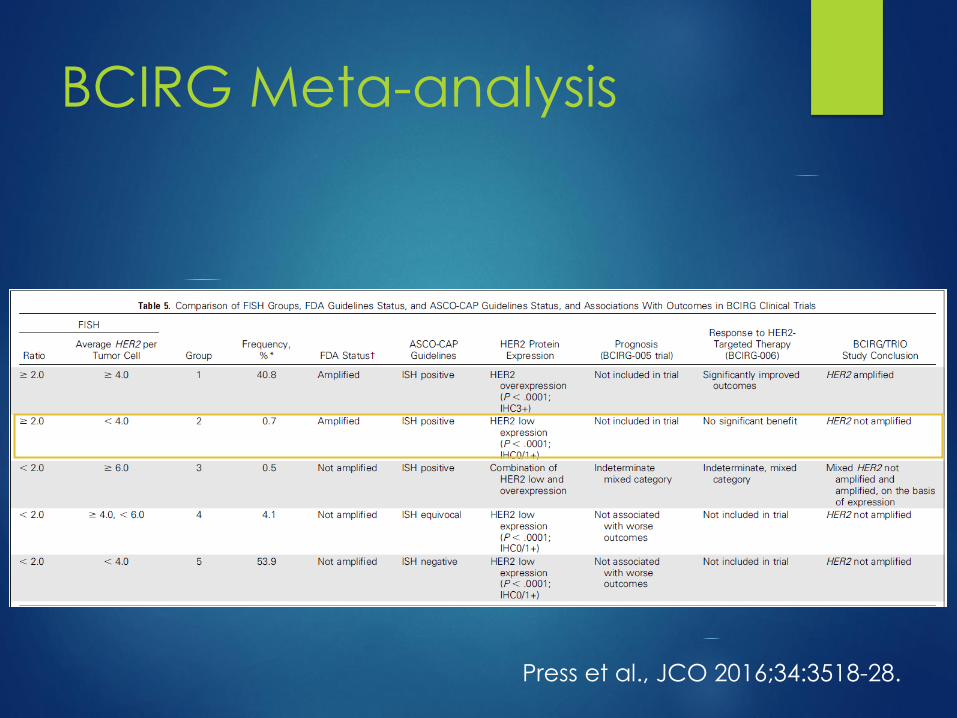
BCIRG Meta-analysis
Press et al., JCO 2016;34:3518-28.
Review of pooled data from BCIRG trials
Group 1: 20% 0/1+, 30% 2+, 50% 3+
Group 2: 91% 0/1+, 9% 2+, 0% 3+
Group 3: 77% 0/1+, 11% 2+, 11% 3+
Group 4: 94% 0/1+, 5% 2+, 1% 3+
Group 5: 99% 0/1+, 0.5% 2+, 0.05% 3+

BCIRG Meta-analysis
BCIRG Meta-analysis
Press et al., JCO 2016;34:3518-28.
Review of ISH Guidelines
Clarify interpretation of ISH to reduce variation
Require concomitant review of IHC AND ISH to arrive at diagnosis
Avoid routine use of alternative chr17 probes
Literature sparse
Variable results depending on probe used
Introduction of statistical error due to multiple testing
HER2 Guidelines – Focused
update (unpublished)
Reflex ISH for IHC 2+
Call HER2 negative if low absolute HER2 copy number
Ratio >2, HER2 < 4
Ratio < 2, copy number 4-6 (= current UK guidelines)
Call HER2 positive if ratio > 2, HER2 4-6
Call HER2 positive if Ratio < 2, HER2 ≥6
Heterogeneous group
Recent data shows some but not all patients respond to HER2 targeted therapy
HER2 Guidelines – Focused
update (unpublished)
Updated guidelines still unpublished
Recommendation is to continue to use 2013 guidelines
NHS BSP Pathology Co-Ordinating Committee is
undertaking a UK based review of these cases prior to
adopting the ASCO CAP Update once it is published
My reports – add a comment
‘This tumour has an elevated HER2:CEP17 ratio due to relative loss of the CEP 17 locus without an increase in HER2 copy number. Whilst regarded as HER2 positive
under current guidelines, this subgroup did not show a benefit from HER2 targeted therapies in the BCIRG analysis.’
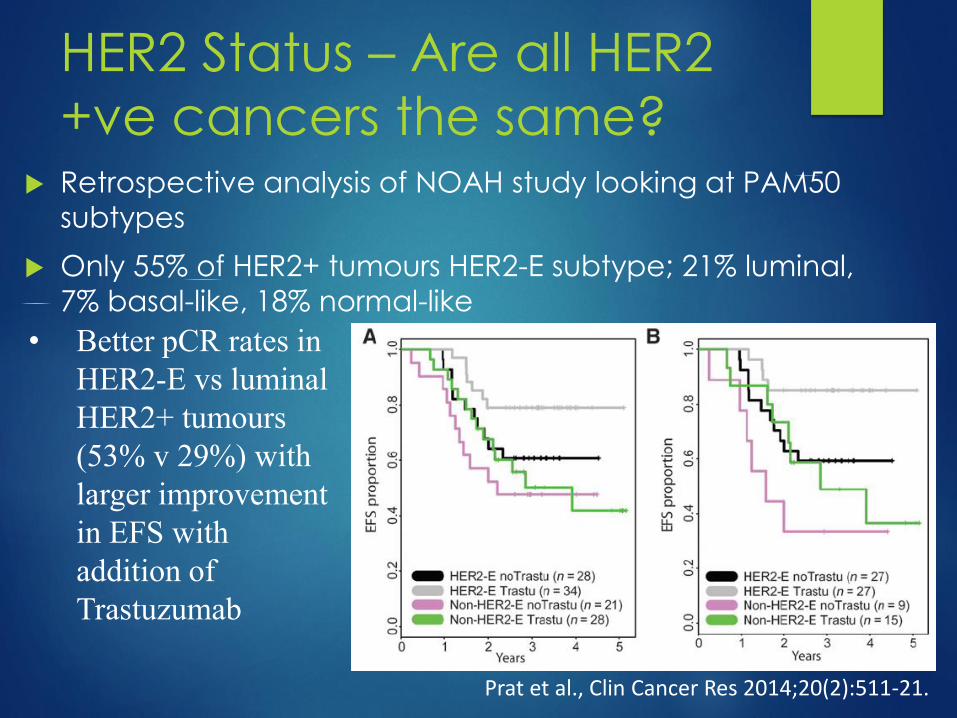
HER2 Status – Are all HER2
+ve cancers the same? Retrospective analysis of NOAH study looking at PAM50
subtypes
Only 55% of HER2+ tumours HER2-E subtype; 21% luminal,
7% basal-like, 18% normal-like
Prat et al., Clin Cancer Res 2014;20(2):511-21.
• Better pCR rates in
HER2-E vs luminal
HER2+ tumours
(53% v 29%) with
larger improvement
in EFS with
addition of
Trastuzumab
HER2 Status – Are all HER2
+ve cancers the same?Predictors of response in HER2 positive cancers
In the NEOSPHERE trial, higher levels of HER2 protein expression
associated with pCR after dual targeted Rx
Bianchini et al., Breast Ca Res 2017;19:16.
FISH:
higher HER2:CEP17 ratio – OR = 2.11, optimum cut off 4.5
higher HER2 copy number – OR = 1.15, optimum cut off 14
Wu et al., Oncotargets and Therapy 2018;11:801-8
Higher pCR rate with high level amplification (copy number >10)
than low level amplification (6-10) – 55% v 24%
No difference in RFS or OS
Guiu et al., BrJC 2010;103:1335-42.