Embed Size (px)
Citation preview
Copyright 2012. MGMA-ACMPE. All rights reserved.
Using HIT for Practice Improvement
Rosemarie NelsonPrincipalMGMA Healthcare Consulting Group
October 2013
Derek KosiorekPrincipalMGMA Healthcare Consulting Group
Copyright 2012. MGMA-ACMPE. All rights reserved.
About MGMA-ACMPE
Our mission…
To continually improve the performance of medical group practice
professionals and the organizations they represent• 22,500 members
• Manage and lead 13,200 organizations
• About 280,000 physicians
Copyright 2012. MGMA-ACMPE. All rights reserved.
Abstract
You invest a lot in information technology, but if you're like many practices, you feel like you could be getting more bang for your buck • Take a look at many ways to leverage your existing information technology
infrastructure and help make your practice run more efficiently.
• Wrap-around and bolt-on technology and apps to improve the user experience and deliver operational effectiveness will be highlighted.
• Look at different pitfalls that practices fall into with regard to staffing, training, infrastructure and purchasing to help you avoid the mistakes that medical practices have been making for years.
• Look at innovative ways that practices are using technology to increase revenues, improve quality and make life easier for staff, doctors and even patients.
Copyright 2012. MGMA-ACMPE. All rights reserved.
Objectives
• Analyze ways to gain more efficiency from your practice’s IT systems
• Identify how HIT in medical practices can help increase revenue and improve quality
• Identify how medical practices are using new technologies, such as “the cloud” and mobile apps
• Match the appropriate IT staffing structures to your size practice
• Identify the need for an HIT strategy in your practice
Copyright 2012. MGMA-ACMPE. All rights reserved.
“With the Jan. 1, 2014, deadline for meaningful use (MU)
stage 2 on your doorstep, the conversion to ICD-10 just
down the block, and the demands of value-based
payment, population health management and other payer
initiatives roaming your neighborhood, you might have
decided that your information technology (IT) house isn't
quite in order. You're not alone. Many practices have
taken a long look at their EHRs and practice management
(PM) systems and decided it's time for a change.”
Copyright 2012. MGMA-ACMPE. All rights reserved.
Information Technology is Changing Rapidly
• Virtualization of servers, storage, and workstations
• Remote hosted versus in-house
• Zero tolerance for downtime
• Data network bandwidth and speeds
• Wireless and mobile data and voice
• Explosive demands for medical image storage
• Data security threats and prevention requirements
Copyright 2012. MGMA-ACMPE. All rights reserved.
Leverage existing HIT
• Assumptions:– PM, EHR, patient portal
• Optimize tech > RCM, patient communications
• Wrap around/bolt on > BI reporting, population health management, mobile apps
• Staffing and training
• Infrastructure & purchasing (HW, Cloud, mobile apps) – workstation replacement too
• Innovate to:– Increase revenue– Improve quality– Make life easier for staff, providers, and patients
Copyright 2012. MGMA-ACMPE. All rights reserved.
Study findings
• One IDS claimed to have leveraged PM very well, achieving 95%-97% adjusted collection rate at cost of $.04-$.05 to collect $1.00.– Note: An IDN/IDS may accept 95% adjusted collection from a physician practice within their
organization, but that is below better performer results from private physician-owned practices (an additional 3%-5% in collections can pay for a Medical Assistant in the practice of primary care physician seeing only 25 patients/day).
• Expectations vary significantly: “Great” results with 17 days in AR and 27 days in AR.
• Like many practices, benefits that technology bring via change are difficult to visualize and accept; especially for physicians without data to measure results that are achieved with the application of a technology tool and the associated change.
• Administrators overwhelmed with managing to maintain a flat revenue and various changes (after-effect of 5010, pending ICD-10, electronic prescribing penalties and Meaningful Use incentives, continued HIPAA privacy and security pressures) while implementing technology that they can’t see through the clouds of those changes to anticipate future needs.
Copyright 2012. MGMA-ACMPE. All rights reserved.
More efficiency: Optimize RCM
• Outsource?
• Clearinghouse services
• Charge capture integration with EHR documentation
• Patient portal and/or kiosk
• Real-time claim adjudication
Copyright 2012. MGMA-ACMPE. All rights reserved.
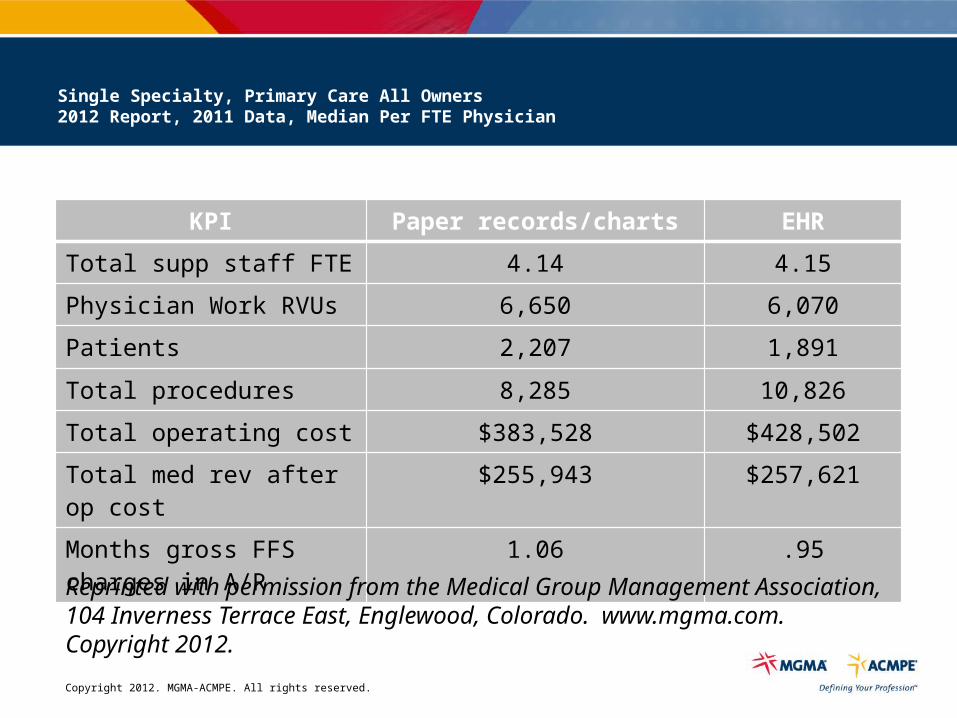
Single Specialty, Primary Care All Owners2012 Report, 2011 Data, Median Per FTE Physician
KPI Paper records/charts EHR
Total supp staff FTE 4.14 4.15
Physician Work RVUs 6,650 6,070
Patients 2,207 1,891
Total procedures 8,285 10,826
Total operating cost $383,528 $428,502
Total med rev after op cost $255,943 $257,621
Months gross FFS charges in A/R
1.06 .95
Reprinted with permission from the Medical Group Management Association, 104 Inverness Terrace East, Englewood, Colorado. www.mgma.com. Copyright 2012.
Copyright 2012. MGMA-ACMPE. All rights reserved.
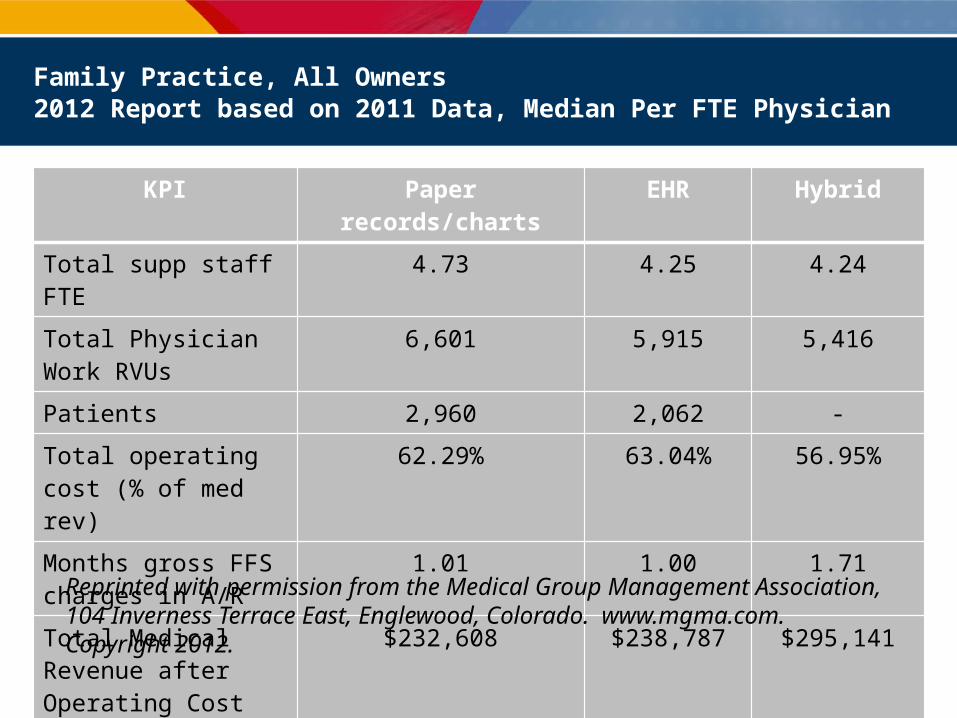
Family Practice, All Owners2012 Report based on 2011 Data, Median Per FTE Physician
KPI Paper records/charts EHR Hybrid
Total supp staff FTE 4.73 4.25 4.24
Total Physician Work RVUs
6,601 5,915 5,416
Patients 2,960 2,062 -
Total operating cost (% of med rev)
62.29% 63.04% 56.95%
Months gross FFS charges in A/R
1.01 1.00 1.71
Total Medical Revenue after Operating Cost
$232,608 $238,787 $295,141
Reprinted with permission from the Medical Group Management Association, 104 Inverness Terrace East, Englewood, Colorado. www.mgma.com. Copyright 2012.
Copyright 2012. MGMA-ACMPE. All rights reserved.
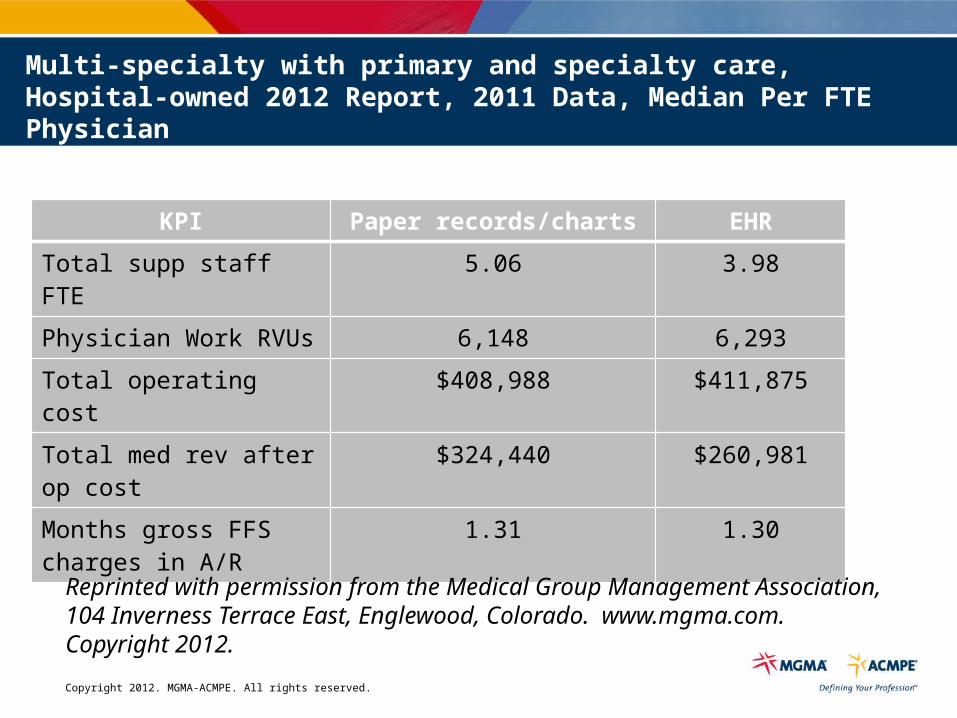
Multi-specialty with primary and specialty care, Hospital-owned 2012 Report, 2011 Data, Median Per FTE Physician
KPI Paper records/charts EHR
Total supp staff FTE 5.06 3.98
Physician Work RVUs 6,148 6,293
Total operating cost $408,988 $411,875
Total med rev after op cost
$324,440 $260,981
Months gross FFS charges in A/R
1.31 1.30
Reprinted with permission from the Medical Group Management Association, 104 Inverness Terrace East, Englewood, Colorado. www.mgma.com. Copyright 2012.
Copyright 2012. MGMA-ACMPE. All rights reserved.
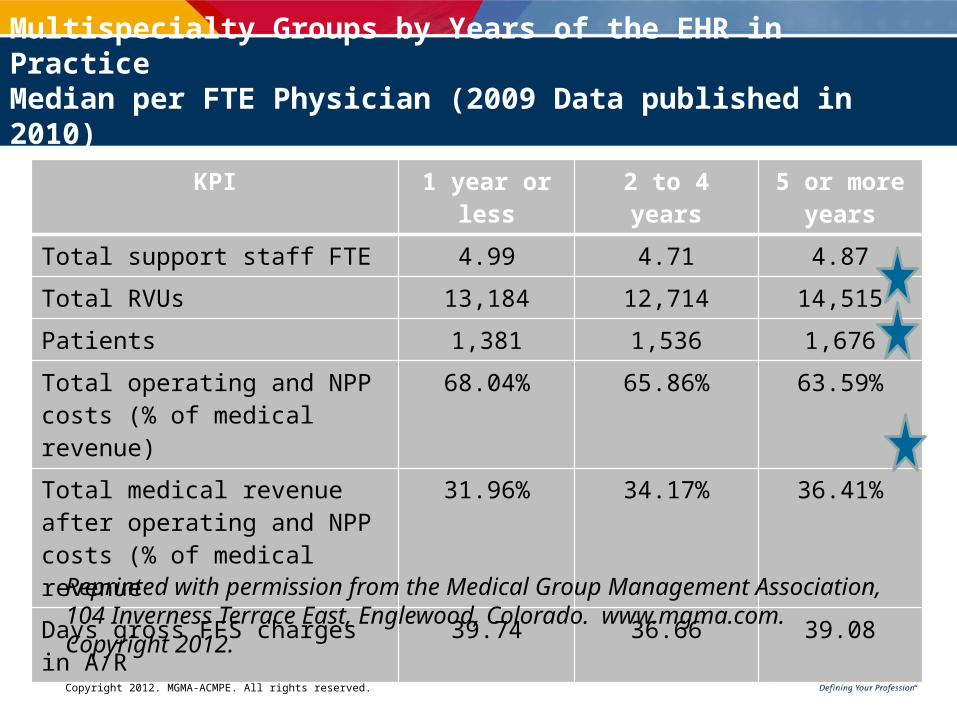
KPI 1 year or less 2 to 4 years 5 or more years
Total support staff FTE 4.99 4.71 4.87
Total RVUs 13,184 12,714 14,515
Patients 1,381 1,536 1,676
Total operating and NPP costs (% of medical revenue)
68.04% 65.86% 63.59%
Total medical revenue after operating and NPP costs (% of medical revenue
31.96% 34.17% 36.41%
Days gross FFS charges in A/R 39.74 36.66 39.08
Multispecialty Groups by Years of the EHR in Practice Median per FTE Physician (2009 Data published in 2010)
Reprinted with permission from the Medical Group Management Association, 104 Inverness Terrace East, Englewood, Colorado. www.mgma.com. Copyright 2012.
Copyright 2012. MGMA-ACMPE. All rights reserved.
Assess EHR utilization
• Patient communications– Integrated portal services
• Information flow during the patient encounter– Physician-nurse communications and encounter documentation
• Charge capture at time of service
• Information flow after patient encounter– Interfaced results tied to interfaced orders delivered to patient portal
Copyright 2012. MGMA-ACMPE. All rights reserved.
Market forces driving physicians
Self-service impact Reduce operational and labor costs Improve efficiency in communications Improve patient satisfaction with self-service capabilities Add new revenue sources
Consumer driven healthcare Patients routinely search for information about their condition
Patients are more involved and educated about their care options Health savings accounts (HSAs) modify patient behavior driving self-service demands
Online Personal Health Record (PHR) use expands Third party payers support online physician-patient communication
HITECH incentives Millions of patients communicate with their physician online
Copyright 2012. MGMA-ACMPE. All rights reserved.
Consumer Demand
Patients want improved communication
79+% of patients have internet access
% of patients wanting the following services: Ask questions where no visit is necessary 77% Fix appointments 71% Get new prescriptions for medications they take 71% Receive the results of medical tests 70% None of the above 6% Don’t know 4%
55% indicated the ability to communicate with their doctors in the above manner would influence their choice of health plans.
-Harris Interactive™
Copyright 2012. MGMA-ACMPE. All rights reserved.
Increase EHR Utilization
• Are only 10% of patients using the portal?–What functionality have you added?
• Are you using a kiosk in the reception area?
• What have you done to increase remote access?–Time patients spend in the reception area
completing forms or even using the kiosk impact the productivity of front staff
17
Copyright 2012. MGMA-ACMPE. All rights reserved.
Increase EHR Utilization
• Refresher Training – EHR compares to any other technology owned; never quite sure
if we are using all the features. – During initial training and the first few weeks of use, users
focused on using the new technology as opposed applying the technology
– Once accustomed to using the technology in the way that feels most comfortable, it is difficult to change behavior
– Beneficial for sub optimal users of the system
• New Users– Assign to super user
18
Copyright 2012. MGMA-ACMPE. All rights reserved.
Increase EHR Utilization
• Software updates– Practices do not fully evaluate new features in updates to
determine which ones will be beneficial and can be incorporated into their workflows
– Train employees on update functionality– Missed opportunity to get more out of your investment
• Updates increase the value of investment
19
Copyright 2012. MGMA-ACMPE. All rights reserved.
Increase EHR Utilization
• “Leaner” Workflows – Re-evaluate people and process – Practices often evaluate process without even knowing that they
are doing so• Can be a formal process - in some cases it comes after a few
days of usage by the staff that suggestions are made “on the fly”• For example, in some practices staff noted that the location of
the printer isn’t optimal. They’ve either repositioned the printer or added another printer to optimize workflow.
20
Copyright 2012. MGMA-ACMPE. All rights reserved.
Increase EHR Utilization
• Shifting Resources– Optimization can be compromised because employees
remain in traditional roles– Employee tasks should be assigned to optimize the
goals for the practice• Enhance the ability to move towards a paperless
system• Evaluate care management opportunities• Build care templates to be used by the nurses and
providers 21
Copyright 2012. MGMA-ACMPE. All rights reserved.
Bottom line
• Delegate all duties that don’t require a physician’s license
• Use patient reminder tools
• Use web/email for patient communications
• How many telephone transactions can you transfer to your web site
• Revamp patient registration – web and EMR and introduce it on the phone scheduling the appointment
• Anticipate needs for visit
Copyright 2012. MGMA-ACMPE. All rights reserved.
BIG Data
• Query/reporting in real time for business intelligence
• Population health management reporting– Integrated to patient communications tools
• Staff analytical skills
Copyright 2012. MGMA-ACMPE. All rights reserved.
Pay for Performance/Quality Reporting: Rationale
• Currently– Healthcare costs an issue for both public and private sector– U.S. spends 15 -18% of GDP on health services (about 12¢
per dollar)– Medicare beneficiaries and private sector face continued
rise in premium payments, doubled from 1998 to 2006, projected to triple from 1998 to 2015
– Dartmouth atlas shows wide variation in Medicare spending per beneficiary among different areas in U.S.
– No correlation in cost variation with quality or outcome
Copyright 2012. MGMA-ACMPE. All rights reserved.
Identify and Manage Patient Populations
• Patient information
• Clinical data
• Comprehensive health assessment
• Use data for population management
Copyright 2012. MGMA-ACMPE. All rights reserved.
Study findings
• Patient population management carries different meanings to many and is not understood to require additional resources.– Believe the EMR vendor solutions are inclusive of patient population care management
functionality. – Very few practices regardless of ownership have ventured this deep into their IT
solutions to identify gaps.
Copyright 2012. MGMA-ACMPE. All rights reserved.
Business Intelligence Reporting
• Add-on tools for reporting from practice management system– www.trellishc.com
• The Diver Solution, Dimensional Insight• www.dimins.com/decisionsupport
– www.bridgeitsolutions.com– www.dashboardMD.com
• Service – runs nightly • Web based – hosted/on your server (data warehouse)• Turn-key enterprise-wide• Custom KPIs
– MGMA DataDive www.mgma.com/datadive
Copyright 2012. MGMA-ACMPE. All rights reserved.
One Health Plan’s Approachto Preventive Measures
Breast Cancer Screening
Colorectal CA Screening
Osteoporosis Screening
Hypertension Screening
Depression Screening
Pneumococcal Vaccine
Influenza Vaccine
Hypertension Control
Smoking Cessation Education
Copyright 2012. MGMA-ACMPE. All rights reserved.
And, Disease Management Measures
Chronic Obstructive Pulmonary Disease (COPD) • Spirometry• Sao2 Measurement• Beta-agonists/Anti-Cholinergic Prescribed
Coronary Artery Disease (CAD)• LDL Screening• LDL Control• Beta Blocker Prescribed (history of MI)• Antiplatelet Therapy Prescribed• Statin Prescribed
Congestive Heart Failure (CHF)• LVF Assessment Completed• ACE or ARB Prescribed • Beta Blocker Prescribed
Diabetes Management
• HbA1c Screening
• HbA1c Control
• LDL Screening
• LDL Control
• Microalbuminuria Testing
• Creatinine Testing
• Eye Exam Screening
• Foot Exam
• Statin Prescribed
• Hypertension Screening
• Hypertension Control
Copyright 2012. MGMA-ACMPE. All rights reserved.
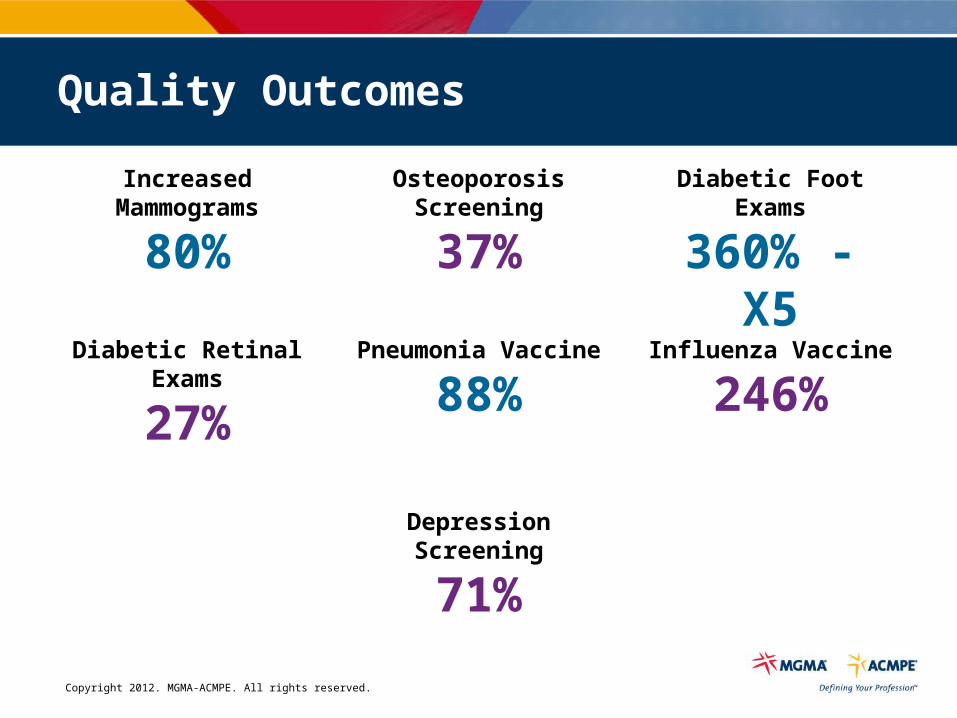
Quality Outcomes
Increased Mammograms
80%
Osteoporosis Screening
37%
Diabetic Foot Exams
360% - X5
Diabetic Retinal Exams
27%
Pneumonia Vaccine
88%Influenza Vaccine
246%
Depression Screening
71%
Copyright 2012. MGMA-ACMPE. All rights reserved.
Improved Efficiency of Care
• Decreased acute care costs
• Decreased outpatient diagnostic testing
• Decreased emergency room costs
• Increased payments to physicians!!
Pilot of 17 Medical Groups
Net: Decreased total expenses
Copyright 2012. MGMA-ACMPE. All rights reserved.
Query and Contact: First 30 Days Results
621 additional appointments
– $65,080 inMonthly Revenue
– $780,960 inAnnualized Revenue
– 15X ROI
Case Study: East Texas Medical Center (First Physicians):Multi-specialty practice employed by Integrated DeliveryHealth System with 200 providers across 12 different specialties.
Compliance Booking Rate
QualityImpact
Financial Impact
Average days since last chronic visit was 235 with a
max of 380 days
Copyright 2012. MGMA-ACMPE. All rights reserved.
Tools support staff
• Online or on the phone?
• 24x7 patient convenience
• Outreach efficiency– Patient management
Copyright 2012. MGMA-ACMPE. All rights reserved.
Apps to help educate patients
• DrawMD (free in Apple app store) – physicians can sketch, stamp or type on detailed anatomic images and then save to EHRs and/or share images with patients
• NumeraNET (free in Apple app store) – patients can share info such as weight, blood pressure, pedometer results with physicians,who can send the info to an EHR
• Survey on the Spot (free in Apple app store) – Gather instant feedback on your practice with custom surveys– See compiled survey results in your account– Get software alerts when a patient rates service as poor
34
Copyright 2012. MGMA-ACMPE. All rights reserved.
Train and support
• Vendor app training
• Practice training on how to apply the tool to the operations
• Dedicated role and/or shared position
• Technical support– Dedicated staff and/or outsource firm
Copyright 2012. MGMA-ACMPE. All rights reserved.
Staff training via online courses
• www.Bridgefront.com – Revenue cycle– Compliance and HIPAA– Medical terminology– Nursing continuing ed
• www.learnthat.com – General computer and Windows basics– Microsoft tools (Excel, Word, Powerpoint, Access)
• www.mgma.com/online – Billing courses
36
Copyright 2012. MGMA-ACMPE. All rights reserved.
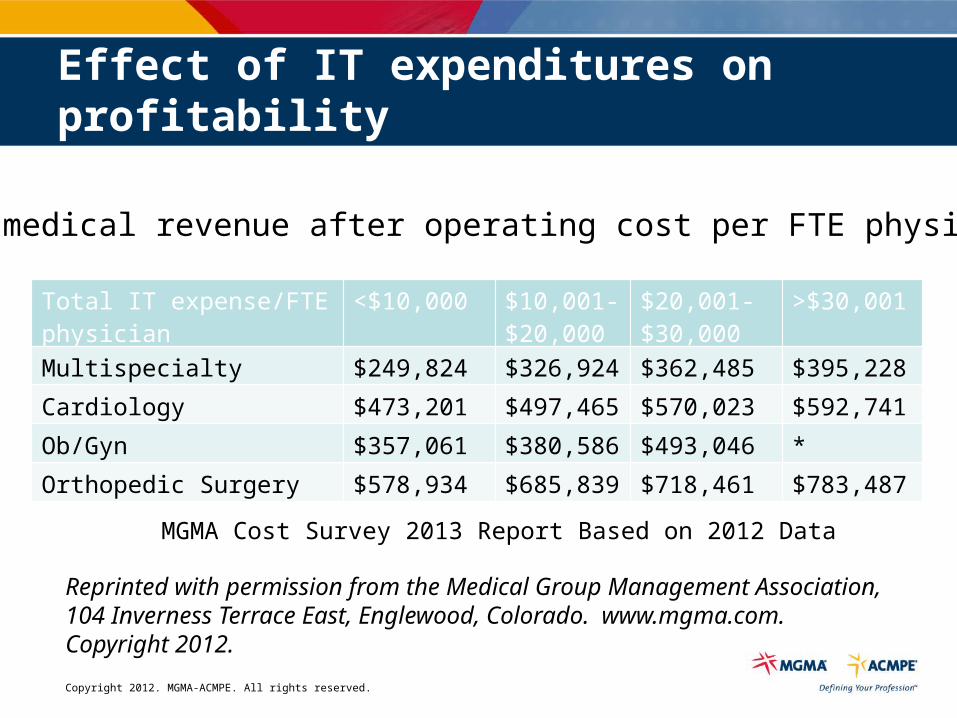
Effect of IT expenditures on profitability
Total medical revenue after operating cost per FTE physician.
MGMA Cost Survey 2013 Report Based on 2012 Data
Total IT expense/FTE physician <$10,000 $10,001-$20,000
$20,001-$30,000
>$30,001
Multispecialty $249,824 $326,924 $362,485 $395,228
Cardiology $473,201 $497,465 $570,023 $592,741
Ob/Gyn $357,061 $380,586 $493,046 *
Orthopedic Surgery $578,934 $685,839 $718,461 $783,487
Reprinted with permission from the Medical Group Management Association, 104 Inverness Terrace East, Englewood, Colorado. www.mgma.com. Copyright 2012.
Copyright 2012. MGMA-ACMPE. All rights reserved.
Infrastructure
Copyright 2012. MGMA-ACMPE. All rights reserved.
Copyright 2012. MGMA-ACMPE. All rights reserved.
Information Technology
Copyright 2012. MGMA-ACMPE. All rights reserved.
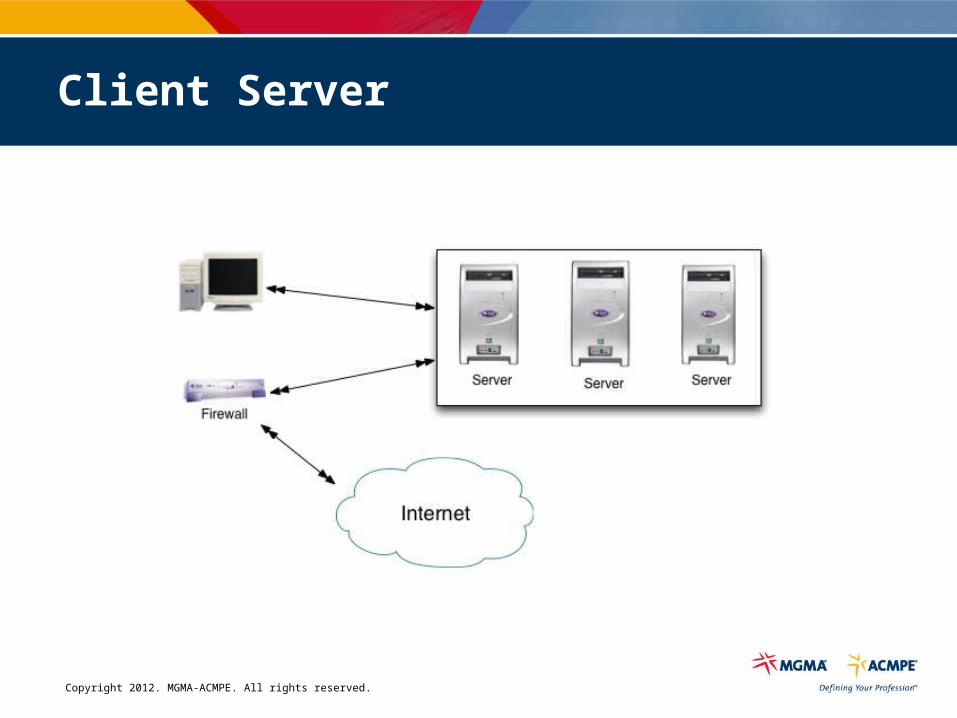
Client Server
Copyright 2012. MGMA-ACMPE. All rights reserved.
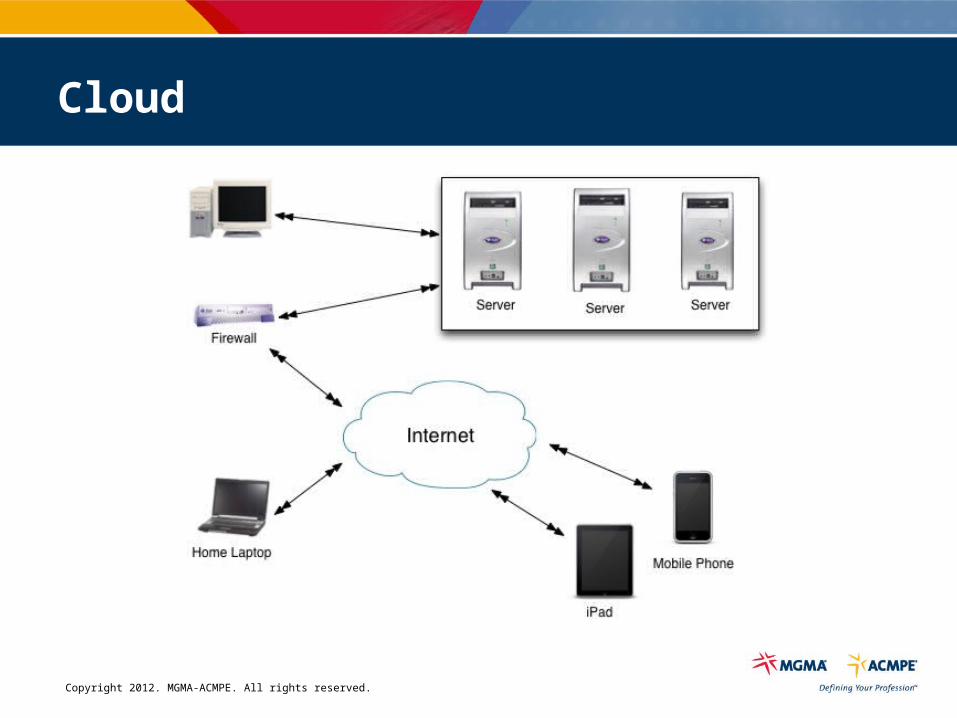
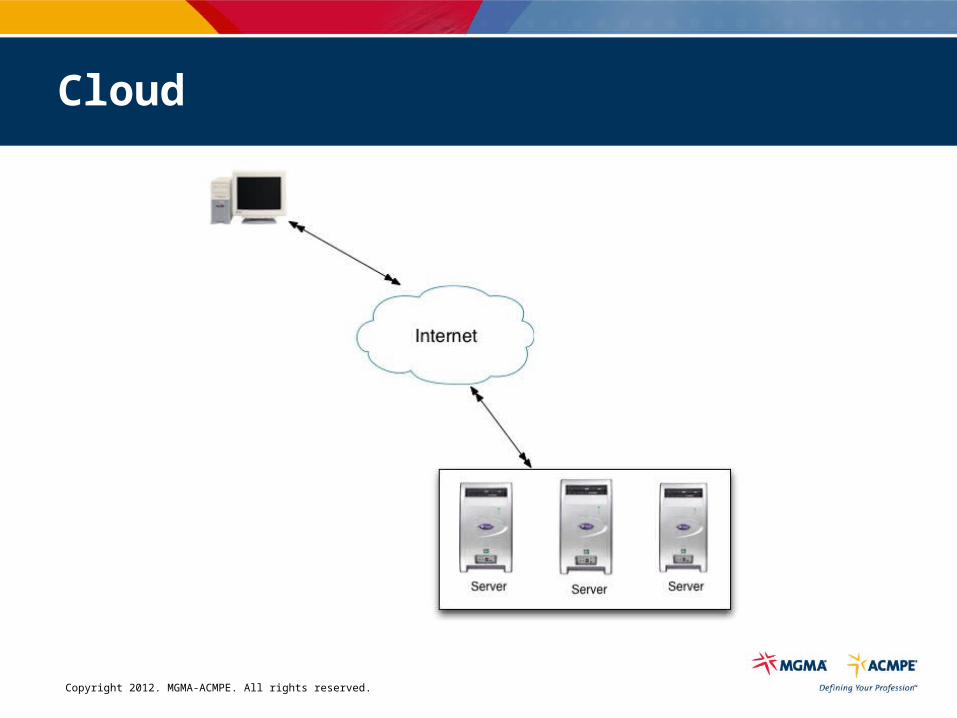
Cloud
Copyright 2012. MGMA-ACMPE. All rights reserved.
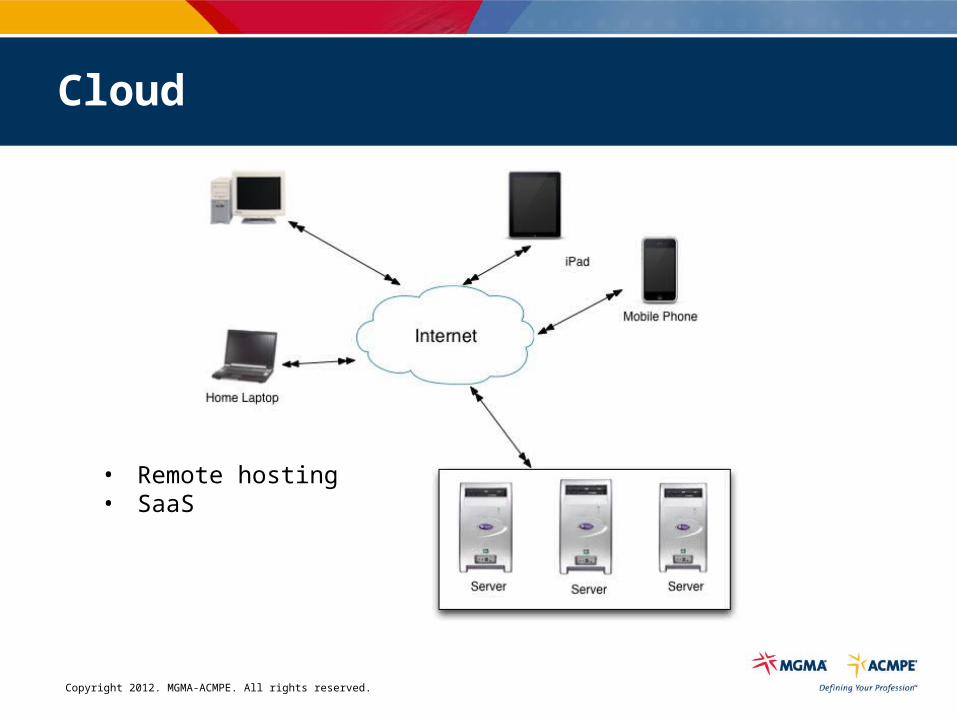
Cloud
Copyright 2012. MGMA-ACMPE. All rights reserved.
Cloud
• Remote hosting• SaaS
Copyright 2012. MGMA-ACMPE. All rights reserved.
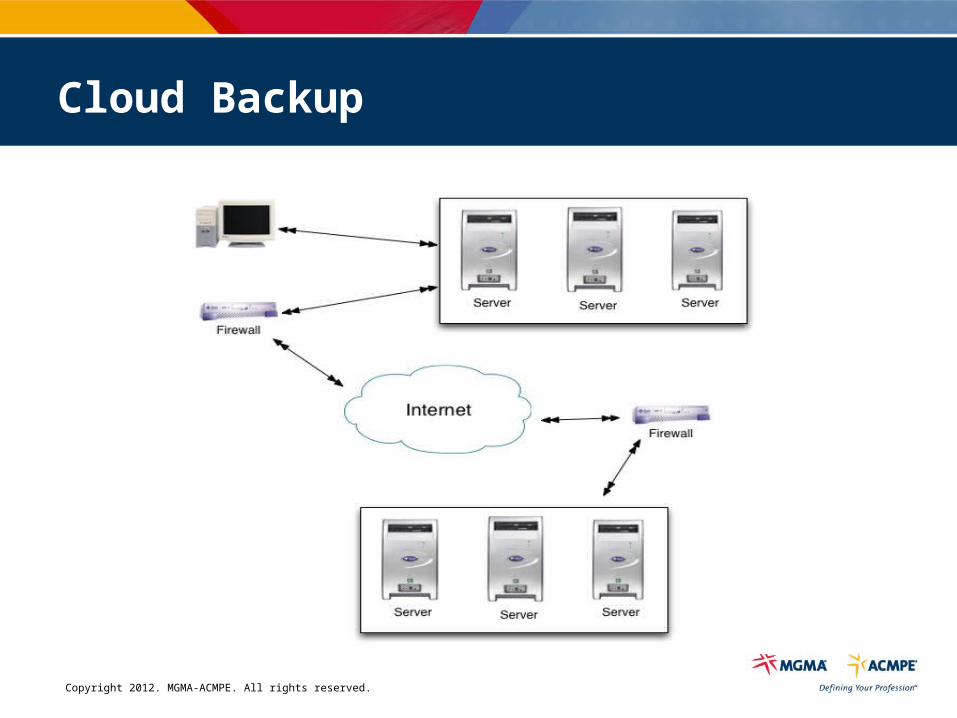
Cloud Backup
Copyright 2012. MGMA-ACMPE. All rights reserved.
Copyright 2012. MGMA-ACMPE. All rights reserved.
Copyright 2012. MGMA-ACMPE. All rights reserved.
Which is the tablet?
Copyright 2012. MGMA-ACMPE. All rights reserved.
Information Security
Copyright 2012. MGMA-ACMPE. All rights reserved.
• Increased connectivity
• Hard to detect loss
• Easy to steal MASSIVE amounts of information
• Increased use of portable devices
• Increasing complexity of systems
Why Worry About Info Security?
Copyright 2012. MGMA-ACMPE. All rights reserved.
• May occur continuously and indefinitely
• Motives of attackers more varied
• Doesn't require physical access to facility
• Low risk of getting caught
Why Worry About Info Security?
Copyright 2012. MGMA-ACMPE. All rights reserved.
Risk =Threat x Vulnerability x Impact
Copyright 2012. MGMA-ACMPE. All rights reserved.
Reducing Vulnerability - Controls
• Technical– Software and hardware tools or products
• Physical– Protecting physical access to information
• Administrative– Policies & procedures, management
Copyright 2012. MGMA-ACMPE. All rights reserved.
Technical Control
• Computer– Username/password
• Server & Local Area Network– Roll based access
• Wide Area Network– Firewalls, Data Encryption
• PDA, Blackberry, Jump drives
– Username/password, Biometric
• Remote Access– VPN (data encryption)
• Wireless– Encryption, Device Filtering
Copyright 2012. MGMA-ACMPE. All rights reserved.
Physical Controls
• Physical access control– Keys, prox cards
• Surveillance and monitoring– Closed circuit TV (CCTV)– Guards or staff watching
• Alarms– Door alarms, motion detectors
• Cable locks on equipment
• Signage
Copyright 2012. MGMA-ACMPE. All rights reserved.
Physical Controls
Environmental Controls
• Power protection– UPS– Backup generators
• Environmental monitoring/detection– Heating, ventilation & air conditioning (HVAC)– Humidity controls– Water detection and alarms
• Fire detection and suppression
Copyright 2012. MGMA-ACMPE. All rights reserved.
Physical Controls
Device and Media Controls
• HIPAA requires proper handling, storage and disposal of media containing PHI
• Includes computers, servers, laptops, USB memory devices, PDAs
• Disposal could include– Overwriting– Demagnetize– Rendering unusable
Copyright 2012. MGMA-ACMPE. All rights reserved.
Administrative Controls
Policies
Effective policies:• Are Enforceable
– If not, it probably won’t be followed
• Are Measurable– Some methodology to know to what extent they are being complied
with
• Are Accessible– communicated, including changes
• Include Sanctions– Consequences for non-compliance that are consistently applied
Copyright 2012. MGMA-ACMPE. All rights reserved.
Administrative Controls
Policies
• Should not be suggestions or guidelines
• Policies, perception, practice need to be in alignment– Gap analysis
Copyright 2012. MGMA-ACMPE. All rights reserved.
Threats to Information
• Insiders making innocent mistakes• Insiders abusing access privileges• Insiders knowingly accessing for spite or profit• Unauthorized physical intruder• Vengeful employees and outsiders who mount attacks to
access information, damage systems and disrupt operations
Copyright 2012. MGMA-ACMPE. All rights reserved.
Staffing
Copyright 2012. MGMA-ACMPE. All rights reserved.
Fundamental Staffing Assumptions
• IT has become essential (IT does matter)• IT has become financially significant• Healthcare IT is different than IT
Copyright 2012. MGMA-ACMPE. All rights reserved.
Why have IT Staff?
• Number of connected sites
• Computers & servers– Quantity & type– Age– Operating systems
• Servers– Quantity & Type– Age
• Age of network
• Applications
• Security
• Staff development
• Tech purchasing
• Other
Factors that impact technology staffing
Copyright 2012. MGMA-ACMPE. All rights reserved.
What is normal?
Multispecialty Staffing per FTE Physician
Median: .11 IT Staff
90th Percentile: .24 IT Staff
Source: 2011 MGMA Cost Survey
Copyright 2012. MGMA-ACMPE. All rights reserved.
What is normal?
Multispecialty IT Operating Cost per FTE Physician
Staff
Median: $5,970
90th Percentile: $13,317
Operating Cost
Median: $10,495
90th Percentile: $29,258
Source: 2011 MGMA Cost Survey
Copyright 2012. MGMA-ACMPE. All rights reserved.
Factors That Impact Technology Staffing
Facilities
– # of facilities– Geographic area - distance between facilities– Age of the facilities – access for cabling and wireless coverage– Electrical Stability
Copyright 2012. MGMA-ACMPE. All rights reserved.
Factors That Impact Technology Staffing
Computers & Servers
– Quantity/type – Desktop, laptop, tablet, PDA – Age – 5 or more years old – Number of manufacturers
• Eg. Apple, HP, Gateway, Dell, ……….– Number of operating systems/versions
• Eg. OS 9.nn, OS 10.nn, Windows 2003, Windows XP , Linux
Copyright 2012. MGMA-ACMPE. All rights reserved.
Factors That Impact Technology Staffing
• Age of network– Quality of the installation– Building network electronics – over 4 years old– Inter-building electronics– Access to Internet
Copyright 2012. MGMA-ACMPE. All rights reserved.
Factors That Impact Technology Staffing
• Quantity and type applications– Mission Critical– Server level databases
• Security– Wireless– Portable memory devices– Portable wireless devices
Copyright 2012. MGMA-ACMPE. All rights reserved.
Factors That Impact Technology Staffing
• Operational processes/documentation– Key processes undocumented– No disaster recovery or IT security plan– No process for deleting staff or students server access rights when they leave
• Staff development– Little or no training of technology staff– No access to peers in other districts
Copyright 2012. MGMA-ACMPE. All rights reserved.
Factors That Impact Technology Staffing
• Other technologies– Copiers/printers– Projectors– Monitors– Security systems
Copyright 2012. MGMA-ACMPE. All rights reserved.
What do they do all day?
• End user support – “Helpdesk”
• Equipment procurement & replacement
• Server management & monitoring
• Network & data connections
• Remote management
• Software upgrades– Desktop software– EHR, PM
• Information Security
• Other equipment (phones, copiers/scanners, printers)
Copyright 2012. MGMA-ACMPE. All rights reserved.
Buy or rent staff?
• In-house staff benefits– Sense of vision– Immediate response– Skin in the game– Institutional knowledge
• Outsourced IT staff benefits– Reduced cost– More all around knowledge– Better ability to keep up with trends
Copyright 2012. MGMA-ACMPE. All rights reserved.
Vendor support of technology
• Tablet rage– Providers and patients
• Mobile apps– Providers and patients
• Integrated reporting tools
• Integrated patient portal and communication– Kiosk functionality
• Cloud support
Copyright 2012. MGMA-ACMPE. All rights reserved.
Where do you find these wonderful people?
• Classifieds are dead
• Job websites– Monster.com, careerbuilder.com, simplyhired.com, indeed.com, dice.com
• Recruiters
• Word of mouth
• HIMSS JobMine– Healthcare Information and Management Systems Society– http://jobmine.himss.org
Copyright 2012. MGMA-ACMPE. All rights reserved.
What do they do all day?
When something works well, there is a perception that it is easy to change without risk of losing what is working well.
Copyright 2012. MGMA-ACMPE. All rights reserved.
Technology Support
Proactive
Vs.
Reactive
Copyright 2012. MGMA-ACMPE. All rights reserved.
Reduce Reactive Support
• Keys to reducing technology support– Implement recommended replacement cycles– Negotiate warrantees to replacement cycle– Limit number computer manufacturers– Implement remote computer support– Implement automated software imaging– Implement server centralization/consolidation– Increase technology staff training– Outsource applications
Copyright 2012. MGMA-ACMPE. All rights reserved.
Tech Staff Development
• Technology support staff development
– Training– Opportunities to network with peers
• User group meetings• Conferences
Copyright 2012. MGMA-ACMPE. All rights reserved.
Tech Staff Development
Credentials
• A+– Hardware technicians– Offered through ComTIA
• MCSE– Microsoft Certified Systems Engineer
• Healthcare IT – CPEHR/CPHIT (http://www.healthitcertification.com)
• Certified Professional Electronic Health Records• Certified Professional Healthcare Information Technology
– CPHIMS/CAHIMS (http://www.himss.org/health-it-certification)• Certified Professional in Healthcare Information & Systems• Certified Associate in Healthcare Information & Management Systems
Copyright 2012. MGMA-ACMPE. All rights reserved.
Metrics
• Support tickets– How many closed?
• Total, average per day by month, current vs. prior year– How many open tickets– Average time to resolve
• Goals (aligned with organization’s business strategy) accomplished
• KPIs– Percentage of up-time (system, workstations)
• Staff survey
• Anecdotal
Copyright 2012. MGMA-ACMPE. All rights reserved.
IT Staff Separation
• Make sure you have an up to date list of all administrator passwords. – This includes passwords to all servers, routers and the firewall(s).
• Deactivate the employee’s account(s). – Including her/his main account and any accounts created for testing or training.
• Audit the membership of the Admin Group on each server and workstation– One of the functions of a server is to maintain a list of users and the
corresponding access granted to each. It does this by maintaining groups of users that share the same permissions. One of these groups is the Admin Group. Also audit the Domain Admins Group.
Copyright 2012. MGMA-ACMPE. All rights reserved.
IT Staff Separation
• Make sure all necessary user account passwords are changed.
• List any equipment and files in the employee’s possession that must be returned.
• Audit all accounts and ways to access the network remotely.– Changing the passwords for authorized employees– If vendor has remote access, determine whether IT can duplicate the access
and make appropriate changes
Copyright 2012. MGMA-ACMPE. All rights reserved.
IT Staff Separation
Notify all external organizations of the new staff member authorized to contact them on your behalf.
This includes:– Domain name listings for website and email (Network Solutions)– Telecom vendors– External IT consultants– Backup tape storage– Practice Management and Development software vendors
Copyright 2012. MGMA-ACMPE. All rights reserved.
Cutting Edge

Copyright 2012. MGMA-ACMPE. All rights reserved.
Wearable Computing
Copyright 2012. MGMA-ACMPE. All rights reserved.
Science and technology
• Telemedicine transforming traditional view of medicine
• Mobile technology untethers healthcare and enables the practice of care anywhere
• DTC market for genetic testing will expand
• Activist disease foundations upending the way scientific research is done and the way academics interact with pharmaceutical and biotech companies– Demands accountability and information sharing – almost unheard of in broad
scientific community
Copyright 2012. MGMA-ACMPE. All rights reserved.
Mobile technology
• Reduces need for hospital admissions and physician office visits
• Improves access – Remote patients– Creates schedule availability
• 40% of physicians say could eliminate 11% to 30% of office visits thru use*
• Contrary to payment mechanisms– Why accept technology that hurts incomes?
• Provides access to more accurate data at decision-making point of care
*PWC Health Research Institute, Sept. 2010
Copyright 2012. MGMA-ACMPE. All rights reserved.
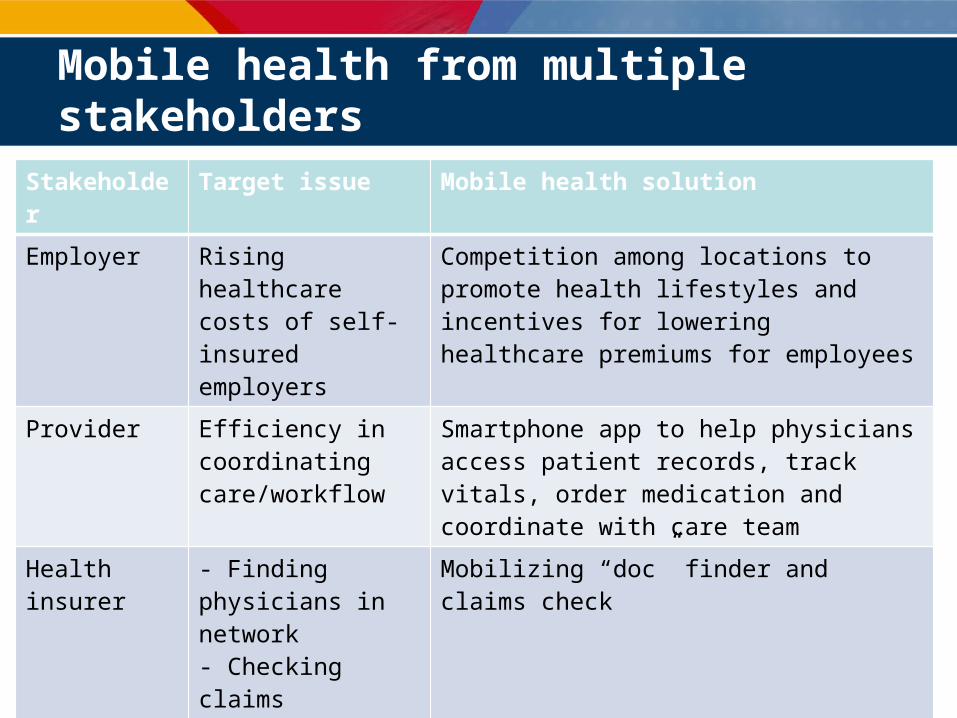
Mobile health from multiple stakeholders
Stakeholder Target issue Mobile health solution
Employer Rising healthcare costs of self-insured employers
Competition among locations to promote health lifestyles and incentives for lowering healthcare premiums for employees
Provider Efficiency in coordinating care/workflow
Smartphone app to help physicians access patient records, track vitals, order medication and coordinate with care team
Health insurer - Finding physicians in network- Checking claims
Mobilizing “doc” finder and claims check
Pharma Patient compliance in diabetes monitoring
Digital glucose monitor that integrates with Nintendo game console
Retail pharma Cost info and Rx management cumbersome to maintain
Smartphone app for Rx drug info and member management of Rx refills, history and retail location finder
Copyright 2012. MGMA-ACMPE. All rights reserved.
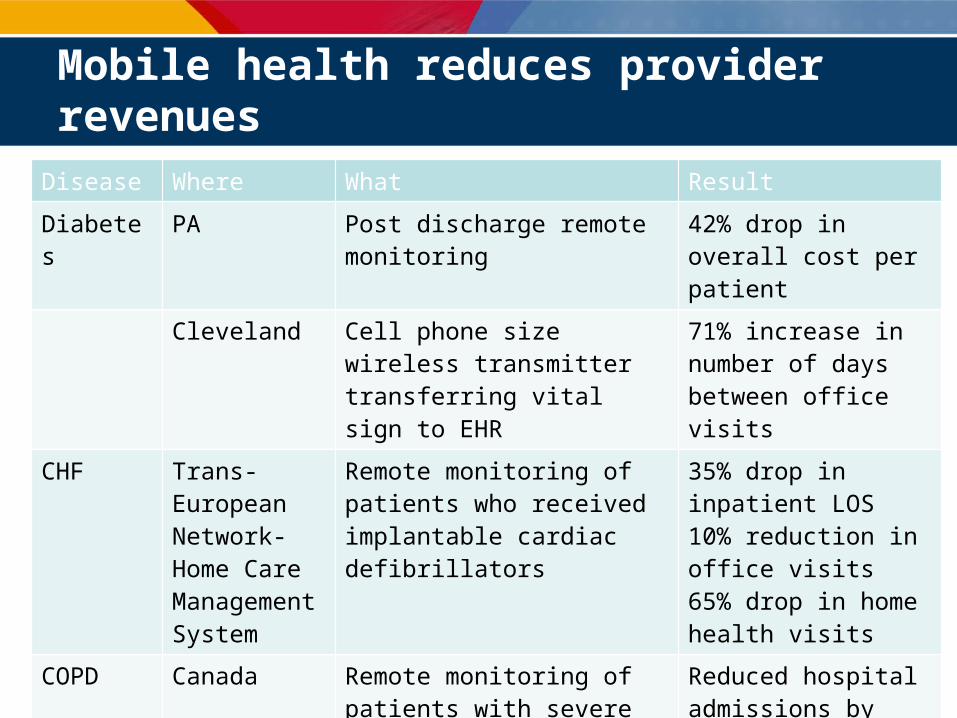
Mobile health reduces provider revenues
Disease Where What Result
Diabetes PA Post discharge remote monitoring 42% drop in overall cost per patient
Cleveland Cell phone size wireless transmitter transferring vital sign to EHR
71% increase in number of days between office visits
CHF Trans-European Network-Home Care Management System
Remote monitoring of patients who received implantable cardiac defibrillators
35% drop in inpatient LOS10% reduction in office visits65% drop in home health visits
COPD Canada Remote monitoring of patients with severe respiratory illness
Reduced hospital admissions by 50%, acute home exacerbations by 55%, hospital costs by 17%
Copyright 2012. MGMA-ACMPE. All rights reserved.
Web sites –daily/weekly feeds
• HITS (HealthIT Strategist) from www.modernhealthcare.com
• www.healthleaders.com
• www.ihealthbeat.org (one of the better ones)
• www.practisinc.com
• www.chcf.org (although named “California” this is a national organization with good credibility)
• www.physicianspractice.com (weekly Pearls)
Copyright 2012. MGMA-ACMPE. All rights reserved.
The New Newspaper
Zite
• Personalized news and features magazine
• An aggregator that collects news and features from other sources
• Socially generates magazines
Copyright 2012. MGMA-ACMPE. All rights reserved.
Copyright 2012. MGMA-ACMPE. All rights reserved.
Questions?
MGMA.org