Embed Size (px)
Citation preview

Cardiac Arrhythmias
For Pharmacists

Agenda
Overview of the normal
Classification
Management
Therapy
Conclusion

Cardiac arrhythmias
Overview of the normal

Arrhythmia: definition
From the Greek a-, loss + rhythmos, rhythm
= loss of rhythm
Any variation from the normal rhythm of the heartbeat
encompassing abnormalities of:
Rate: too slow (bradycardia) or too fast (tachycardia)
Regularity
Site of impulse origin
Sequence of activation
Any rhythm that is not normal sinus rhythm
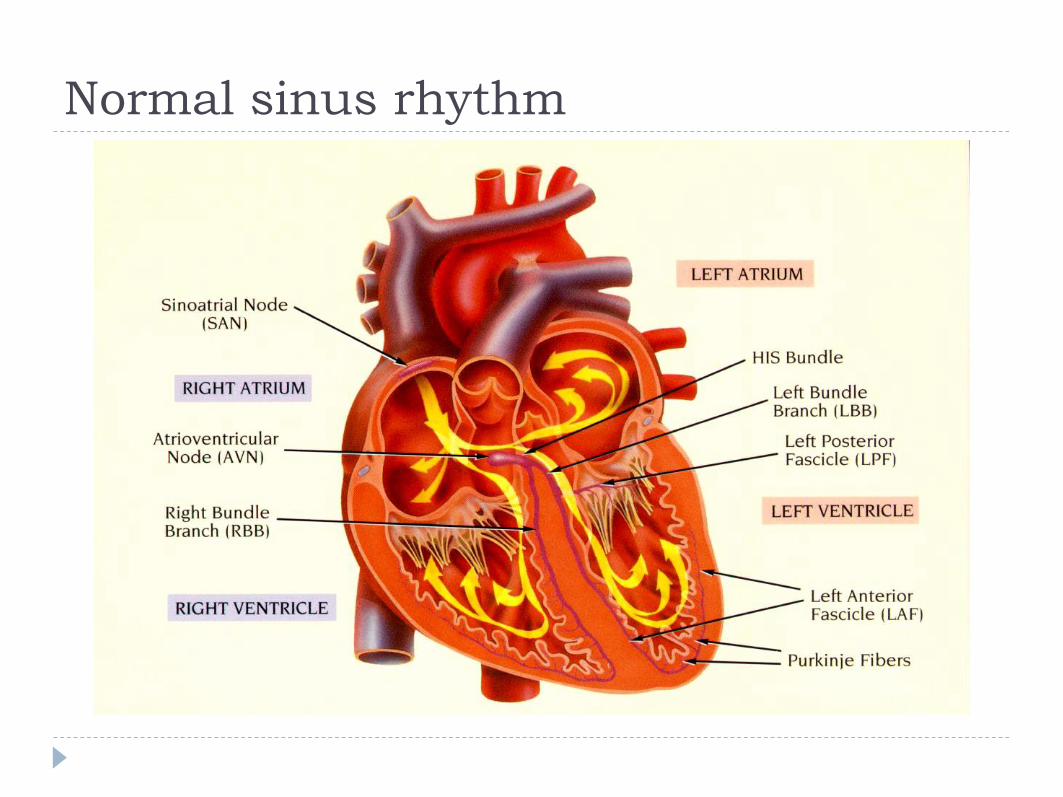
Normal sinus rhythm

Temporal sequence of activation

Temporal sequence of activation

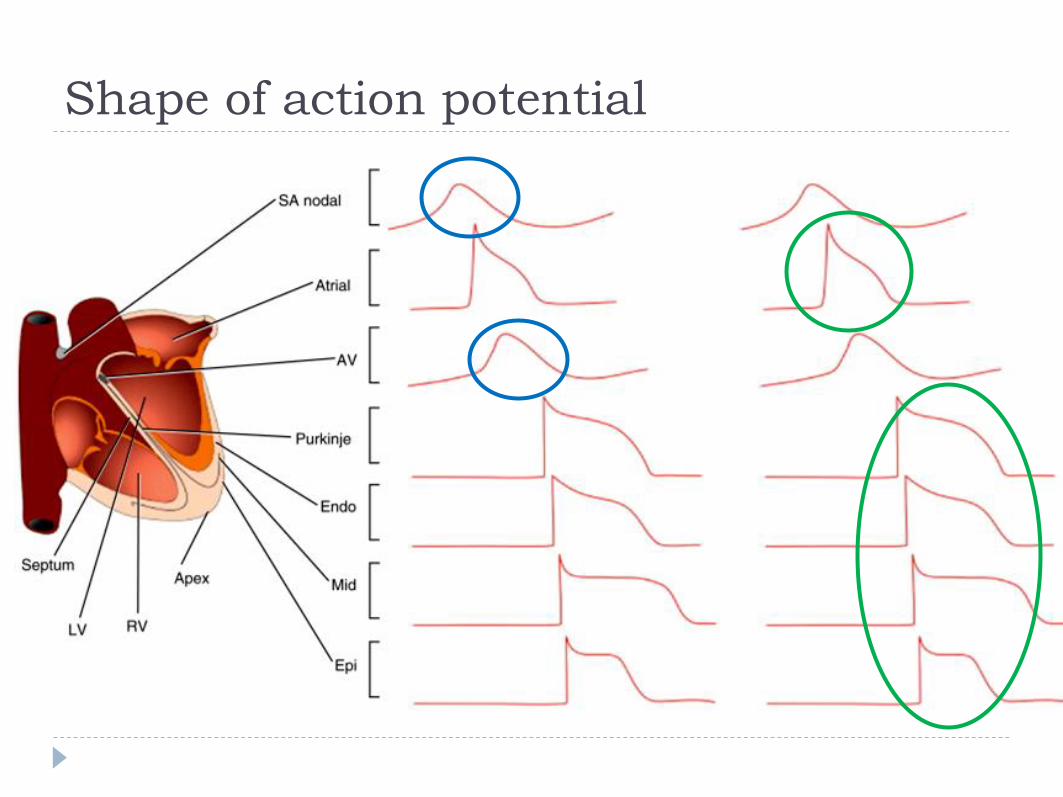
Shape of action potential

Normal cardiac automaticity

Normal cardiac automaticity
All cardiac cells have property of self-excitation ie
INTRINSIC RHYTHMICITY
They can therefore spontaneously depolarize
Pacing of the heart will be carried out by cells with the
fastest natural rate ie OVERDRIVE SUPPRESSION

Currents responsible for ventricular AP.Length of the arrows shows the relative size of each ionic current.
E: Equilibrium potentialECF: extra-cellular fluidICF: intra-cellular fluid.

Cardiac arrhythmias
Classification

Arrhythmias: classification
Site of origin
Mechanism
Duration
Clinical
significance

Site of origin
Supra-ventricular:
Sinus node
Atria
Atrio-ventricular junction
(above bifurcation of HB)
Ventricular:
Bundle branches
Purkinje fibres
Working myocardium

Mechanism
Abnormal impulse initiation
Abnormal automaticity
Triggered activity
Abnormal impulse conduction
Slow or blocked conduction
Re-entry
Most clinically important
arrhythmias are due to re-entry

Re-entry

Re-entry

Duration
Paroxysmal or non-sustained
Persistent or sustained
Permanent or chronic

Clinical significance
Benign
No independent increase in risk
Significant
Independent increase in risk
Potentially lethal
Can lead to proximate fatality if left untreated

Cardiac arrhythmias
Management
Management
1. Precise diagnosis + assessment
Must precede any intervention!!
2. Eliminate precipitants
Drugs: digoxin, beta-blockers
CHF, TTX, anxiety
Hypokalaemia, hypoxia, acidosis

3. Assess risk
High risk
Moderate risk
Low risk
Management

Low risk arrhythmias
Do not have potential to produce death
Need not be suppressed
Treat only if they produce disruptive symptoms

High risk arrhythmias
Potentially life-threatening
Must be suppressed
Treat always even if symptoms are minor
Moderate risk arrhythmias
Problematic!
No clear cut treatment of choice
Amelioration
Prevention
Cure
Management strategies
Termination
• Increasing AVB in AF
• Pacing AVB
• Decrease or abolish
arrhythmia attacks
• Ablation of irritable focus or
accessory pathway
• Conversion of SVT to SR

Amelioration
Prevention
Cure
Management strategies
Termination
• Increasing AVB in AF
• Pacing AVB
• Decrease or abolish
arrhythmia attacks
• Ablation of irritable focus or
accessory pathway
• Conversion of SVT to SR

Amelioration
Prevention
Cure
Management strategies
Termination
• Increasing AVB in AF
• Pacing AVB
• Decrease or abolish
arrhythmia attacks
• Ablation of irritable focus or
accessory pathway
• Conversion of SVT to SR

Amelioration
Prevention
Cure
Management strategies
Termination
• Increasing AVB in AF
• Pacing AVB
• Decrease or abolish
arrhythmia attacks
• Ablation of irritable focus or
accessory pathway
• Conversion of SVT to SR

External electric therapy
Anti-arrhythmic drugs
Non-pharmacologic therapy
Management modalities
Autonomic manoeuvers

External electric therapy
Anti-arrhythmic drugs
Non-pharmacologic therapy
Management modalities
Autonomic manoeuvers

External electric therapy
Anti-arrhythmic drugs
Non-pharmacologic therapy
Management modalities
Autonomic manoeuvers
External electric therapy
Anti-arrhythmic drugs
Non-pharmacologic therapy
Management modalities
Autonomic manoeuvers

Non-pharmacologic therapy
Management modalities
Radio-frequency ablation
Arrhythmia surgery
Implantable devices

Cardiac arrhythmias
Pharmacotherapy

Bradyarrhythmias

Bradyarrhythmias
Identify and treat the cause eg hypothyroidism
Atropine (anti-cholinergic)
Decreases vagal tone
Decreases AV block and increases SA rate
Sympathomimetics: isoprenaline or adrenaline
Increase heart rate and contractility:
ß1 adrenergic effect

Bradyarrhythmias

Bradyarrhythmias

Bradyarrhythmias

Tachyarrhythmias

Aims of drug treatment
1. Afford symptomatic relief
2. Prevent onset of arrhythmias producing
major haemodynamic sequelae
3. Prevent recurrent life-threatening
arrhythymias

Ideal anti-arrhythmic drug
1 Wide range of therapeutic activity against
atrial, junctional and ventricular arrhythmias
2 Available in parenteral and oral form
3 Pharmacokinetic properties to allow predictable long
term plasma level
4 No pro-arrhythmic, no depressant haemodynamic
effects or significant non-cardiac side-effects

Ideal anti-arrhythmic drug
1 Wide range of therapeutic activity against
atrial, junctional and ventricular arrhythmias
2 Available in parenteral and oral form
3 Pharmacokinetic properties to allow predictable long
term plasma level
4 No pro-arrhythmic, no depressant haemodynamic
effects or significant non-cardiac side-effects

Torsades de pointes

http://crediblemeds.org/

Once upon a
time……
Back in 1986……

Back in 1986……

Back in 1986……

CAST
A causes B
PVCs in post-MI patients increase mortality
C reduces A
AAD (encainide, flecainide, and moracizine) can successfully
reduce PVCs
C therefore reduces B
AADs in post-MI patients with PVCs reduces mortality
CAST
“Prophylactic” treatment of
PVCs in post-MI patients

CAST
Drugs used: encainide,
flecainide, and
moracizine
Successful reduction in
the amount of PVCs
BUT: led to more
arrhythmia-related
deaths

CAST
Total mortality was
significantly higher
in actively treated
group compared to
placebo
Excess mortality
was attributed to
proarrhythmic
effects of the agents
AFFIRM
Rate or rhythm control in AF

AFFIRM How do you interpret this?


Classification of AADs
Vaughan Williams (1970)
Effect on the action potential of cardiac cells
Sicilian Gambit (1990)
Effect on the ionic currents of cardiac cells
No good classification scheme exists!!



General considerations
Continuing imperfections of current AADs and rapidly
expanding technologies have led to:
Rapid expansion in use of devices and ablation techniques for
treatment of arrhythmias
Rapid disappearance of many AADs (some of which are no
longer manufactured!!)

Cardiac arrhythmias
Non-pharmacological therapy

EPS

RF Ablation
RF energy is delivered to a
localised area of cardiac tissue
from the tip of a steerable
electrode catheter

RF Ablation
Arrhythmia trigger/substrate is modified:
Initiating foci are destroyed
Conducting pathways are interrupted
No painful skeletal muscle contraction occurs
Can be carried out under LA
Serious complications seldom occur
Non reversible, permanent cure
Uniformly high success rate (depends on arrhythmia type)

RF Ablation lesions

RF Ablation
Useful for:
AVNRT and AVRT
Atrial tachycardia
Atrial flutter
Bundle branch re-entry
VT in normal hearts

Conclusions
Remember…..

Conclusions - 1
An arrhythmia is any rhythm that is not sinus rhythm
Ionic flows through
membrane channels
determine automaticity,
conduction and excitability

Conclusions - 2
Arrhythmias may be classified by:
Site of origin
Mechanism
Duration
Clinical significance

Conclusions - 3
Management depends on:
Precise diagnosis
Elimination of precipitants
Risk assessment

Conclusions - 4
Pharmacotherapy is:
Imperfect
May be dangerous
RF ablation and devices are
rapidly becoming the
mainstay of treatment

Confidential –
for
inte
rnal use o
nly
Thank you for your attention!

Confidential –
for
inte
rnal use o
nly Any
questions?