Embed Size (px)
Citation preview

TRANSFUSION 1990-Vol. M, No. 4 LETTERS TO THE EDITOR 381
2. Hira PR, Husein SF. Some transfusion-induced parasitic infections in Zambia. J Hyg Epidemiol Microbiol Immunol 1979;23:436-44.
Correction of prolonged bleeding time in von Willebrand’s disease with Humate-P
To the Editor: Patients with moderately severe von Willebrand’s disease
(vWD) frequently fail to respond to desmopressin acetate (DDAVP), and cryoprecipitate is the treatment of choice.’ However, mucosal bleeding requires correction of the bleeding time (BT) as well as correction of coagulation factor levels to stop hemorrhage. Even in patients with mild or moderate vWD, plasma or cryoprecipitate sometimes fails to correct the BT. Czapek2 and others3m4 have described the use of Humate-P (Behringwerke AG, Marburg, FRG), a pasteurized factor VIII concentrate that is available in limited supply in the United States, in patients whose bleeding did not respond to DDAVP. We have reportedS a case of a patient with acquired vWD, whose BT was corrected with Humate-P, at which time his prolonged gastrointestinal bleeding stopped. Recently, we treated a patient with moderately severe vWD whose bleeding did not respond to DDAVP or cryoprecipitate, or a combination of the two, but ceased promptly after the infusion of Humate-P.
A 38-year-old man with known, moderately severe vWD was admitted to the hospital with significant blood loss from prolonged epistaxis that was unresponsive to DDAVP infusion. When tested 2 years previously, the patient’s factor VIII co- agulant (FVIIkC) and von Willebrand factor antigen (vWF:Ag) had been found to respond to DDAVP, although the von Wil- lebrand factor (vWF) and BT showed little change (Table l). On this occasion, cryoprecipitate was administered (10 bags/ 12 hours), and, despite normalization of FVII1:C and vWF, the bleeding time remained prolonged. Because of continued bleeding that required nasal packing, the patient also received an infusion of DDAVP after a dose of cryoprecipitate (Day 2). Again, despite normalization of levels, the BT remained more than 15 minutes. Attempted removal of the nasal packing re- sulted in recurrent hemorrhage that produced a severe anemia (hematocrit, 15). The patient required both anterior and pos- terior packing. The packing was left in place for several days, during which the patient received cryoprecipitate every 12 hours. He was then given an infusion of Humate-P (2600 U = 35 U/ kg) on Day 9 to raise the FVII1:C and vWF to 200 percent. Immediately after this, the BT corrected to 9 minutes and the packing was removed without incident. The patient achieved
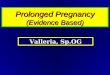
Table 1. Patient response to DDAVP, cryoprecipitafe, and Humate-P
Treatment Baseline (1987) 9 17 el0 <3 After DDAVP (1987) 9.5 99 17 91 Cryoprecipitate alone (Day 2) > 15 85 44 61 Cryoprecipitate + DDAVP >15 87 77 139 Cryoprecipitate alone (Day 9) > 15 85 19 31 Humate-P 9 102 260 222
‘Bleeding time. tFactor Vlll coagulant. won Willebrand factor. Bvon Willebrand antigen.
normal levels of FVIII:C, vWF, and vWF:Ag. Humate-P was then continued every 12 hours for an additional 3 days, at which time the patient was discharged; he has had no further bleeding.
For vWD patients who do not respond to plasma products, the use of Humate-P may well be a life-saving measure. This product has been used extensively in Europe, is pasteurized, and has been considered free of transmission of non-A,non-B hepatitis and HIV.6 That the BT can be corrected with Humate- P in clinical situations in which cryoprecipitate, DDAVP, and cryoprecipitate plus DDAVP replace the deficient factors but do not correct the BT is an interesting observation that may give us an important clue to a definition of those additional factors responsible for correcting the BT. This is in contrast to results recently reported by Cattaneo et al.,’ that the BT often did correct in patients with severe vWD who were given cryoprecipitate followed by DDAVP. These obselvations war- rant further investigation.
ESTHER ROSE, MD ALICE FORSTER, RN
Louis M. ALEDORT, MD Mt. Sinai Hospital
New York, N. Y. 10029
References 1. Mannucci PM. Desmopressin (DDAVP) for treatment of disorders
of hemostasis. Prog Hemost Thromb 1986;8:1945. 2. Czapek E, Gadarowski JJ, Ontiveros JD, Pedraza JL. Humate-P
for treatment of von Willebrand disease (letter). Blood 1988;72:1100. 3. Schaner I. Vigh Z. Comparison between cryoprecipitate and a wet-
heated factor VIII concentrate in the treatmcnt of von Willebrand’s disease (abstract). Ric Clin Lab 1986;16:231.
4. Fukui H, Yoshioka A, Nishino M, Kinoshita S, Niinomi K, Yosh- ioka K. Hemostatic effect of a heat-treated factor VIII concentrate (Humate-P) in von Willebrand’s disease (abstract). Ric Clin Lab 1986;16:238.
5. Uehlinger J. Rose E. Aledort LM, Lemer R. Successful treatmcnt of an acquired von Willebrand factor antibody by extracorporeal immunoadsorption (letter). N Engl J Med 1989;320:254.
6. Schimpf K, Mannucci PM, Kreutz W, et al. Absence of hepatitis aftcr treatment with a pasteurized factor VllI concentrate in patients with hemophilia and no previous transfusions. N Engl J Med 1987;316:918-22.
7. Cattaneo M, Moia M, Della Valle P, Castellana P, Mannucci PM. DDAVP shortens the prolonged bleeding time of patients wilh se- vere von Willebrand disease treated with cryoprecipitate. Blood 1989;74: 1972.
Correlation of IgG subclass with the severity of hemolytic disease of the newborn
To the Editor: We recently published an abstract entitled “Correlation of
IgG subclass with the severity of hemolytic disease of the newborn.”’ An error was made in the calculations in the ab- stract; this error was corrected in the oral presentation at the 42nd Annual Meeting of the American Association of Blood Banks. The abstract stated incorrectly that when IgGl was present without IgG3, 36 percent of the babies needed treat- ment (8% phototherapy [PT], 26% transfusion [Tx], 2% fatal hemolytic disease of the newborn [FHDN]). The figure of 36 percent should have been 56 percent (12% PT, 38% Tx, and 6% FHDN). Unfortunately, the mistake in our calculation led us to conclude incorrectly that severe HDN appeared more