Embed Size (px)
Citation preview

Regulatory Peptides, 16 (1986) 321-329 321 Elsevier
RPT 00548
Corticotropin-releasing factor receptor antagonist: effects on the autonomic nervous system and
cardiovascular function
Marvin R. Brown 1, Thackery S. Gray 2 and Laurel A. Fisher 3
1Departments of Medicine and Surgery, UCSD Medical Center, San Diego, CA. 2Department of Anatomy, Loyola University, Maywood, IL, and 3Department of Pharmacology, Arizona Health Sciences
Center, Tucson, AZ, U.S.A.
(Received 22 August 1986; revised manuscript received 30 October 1986; accepted for publication 6 November 1986)
Summary
The corticotropin-releasing factor (CRF) receptor antagonist, ~-helical [Glu27] - corticotropin-releasing factor 9-41 (CRF 9-41) has been assessed for its ability to modify plasma concentrations of epinephrine and norepinephrine, mean arterial pres- sure (MAP) and heart rate (HR). Basal concentrations of epinephrine and norepi- nephrine were not altered by lateral ventricular (icv) administration of CRF 9-41. However, this CRF antagonist, given icv, attenuated the rise of plasma epinephrine following 30% hemorrhage and insulin-induced hypoglycemia. CRF 9-41 did not alter the increased plasma concentrations of epinephrine or norepinephrine following icv administration of bombesin. Icv administration of CRF 9-41 blunted CRF-in- duced elevation of MAP and HR in normal animals. However, this CRF antagonist did not modify the MAP or HR in spontaneously hypertensive rats. Similarly, this CRF antagonist administered to Sprague-Dawley rats neither prevented the rise of MAP or HR following electrical stimulation of the central nucleus of the amygdala, nor did it affect nitroprusside-induced hypotension and tachycardia.
CRF; CRF antagonists; adrenal medulla; cardiovascular regulation; spontaneously hypertensive rats; amygdala
Address correspondence to: Marvin R. Brown, M.D., Autonomic Physiology Laboratory, Departments of Medicine and Surgery, T-017, UCSD Medical Center, 225 Dickinson Street, San Diego, CA 92103- 9981, U.S.A.
0167-0115/86/$03.50 © 1986 Elsevier Science Publishers B.V. (Biomedical Division)

322
Introduction
Considerable evidence has accumulated to support the hypothesis that corticotro- pin-releasing factor (CRF) is involved in the integration of the neuroendocrine and autonomic nervous system responses to stressful stimuli. CRF has been demonstrated to be a physiologic regulator of pituitary ACTH secretion following stress [1]. In addition, CRF has been shown to act within the central nervous system (CNS) to elicit a variety of changes in autonomic nervous system functions and in behavior that resemble stress-like or defensive responses [2,3].
We have recently reported that a CRF antagonist, ~-helical-[Glu27]-CRF 9-41 (CRF 9-4 1), inhibits CRF-induced elevation of plasma concentrations of epinephrine and norepinephrine [4]. CRF 9-41 has been demonstrated also to significantly atten- uate the rise of plasma epinephrine following exposure to ether vapor in the rat [4]. The present report describes additional experiments designed to assess the effects of CRF 9-41 on the autonomic nervous system and on mean arterial pressure (MAP) and heart rate (HR) under a variety of other conditions.
Materials and Methods
Male Sprague-Dawley rats (200-250 g) (Holtzman, Madison, Wisconsin) were housed in temperature- and humidity-controlled quarters and received food and water ad libitum. Spontaneously hypertensive rats (SHR), Wistar-Kyoto rats (WKY), were obtained from Charles River Laboratories. Prior to all surgical pro- cedures animals were anesthetized with ether or sodium pentobarbital (40 mg/kg). Two to three days prior to experiments, cannulae (Plastic Products) were stereotax- ically positioned into the lateral ventricle as previously described [5]. Bipolar plati- num electrodes (Plastic Products MS 303/8) were implanted into the central nucleus of the amygdala 4 days prior to experiments. One day prior to the catecholamine sampling experiment, silastic-tipped polyethylene-50 cannulae were inserted through the right jugular vein into the right atrium. In experiments in which cardiovascular measurements were made, right femoral artery catheters were placed 3--4 h prior to the initiation of the experiment. This time period has been found to allow sufficient recovery of cardiovascular function to basal levels following anesthesia and surgery.
All experiments were performed in unanesthetized, unrestrained animals housed in clear plexiglass cages to allow visual monitoring of behavior and activity. 2-3 h prior to each experiment, injection cannulae were inserted into the icv guide cannulae and extension polyethylene tubing was attached to the jugular venous catheters. Icv administration of peptides was made over a 30-s perjod in a 5-10/~1 volume. Blood samples were obtained for determination of plasma concentrations of epinephrine, norepinephrine and glucose at the times indicated in the text. MAP and HR were measured with Gould-Statham P-23Db pressure transducers and monitored with a Beckman R-611 dynograph or a Grass Instruments physiograph. Data were collected and analyzed with a Cyborg Isaac A-D converter interfaced to an Apple II computer programmed with Cyborg software. Electrical stimulation was conducted using a Grass $44 stimulator and a Grass SIU5 stimulus isolation unit. Monophasic pulses,

323
each 0.5 s in duration at 50 Hz and at a current of 75 uA, were delivered over a 30-s period.
Plasma concentrations of catecholamines were assessed using the radioenzymatic method of Peuler and Johnson [6]. S-[methyl-ZH]Adenosyl-l-methionine was pur- chased from New England Nuclear. Plasma glucose concentrations were measured by the glucose oxidase method using a Beckman glucose analyzer.
Verification of ventricular cannulae placement was achieved at the completion of each experiment by injection of pontamine blue dye. Histologic identification of par- enchymal cannulae and electrode placements was made on cresyl violet stained sec- tions of buffered formalin-perfused brain.
Peptides were synthesized and kindly provided by Dr. Jean Rivier of The Salk Institute. CRF 9-41 was found to be readily soluble in water by adjustment of the pH to 6.5 using 1N NaOH. Somatostatin-28 (SS-28) and bombesin were dissolved in distilled water.
Data were subjected to analysis of variance and differences between groups were assessed using the multiple range tests of Dunnett and Duncan.
Results
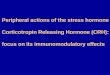
Fig. 1 shows the effects of 30% hemorrhage on plasma concentrations of epine- phrine and norepinephrine. Icv administration of CRF 9-41 resulted in a significant inhibition of hemorrhage-induced epinephrine secretion. Neither hemorrhage nor the CRF antagonist significantly altered plasma concentrations of norepinephrine.
PLASMA NOREPINEPHRINE 3 5 0 -
300- Hem + CRF 9-41 Hem.
_ CRF 9-41 250
200 -
150- ~ . . . . . . . . . .
400- P L A S M A ~ , ~ Hem.
J J
< 01
200-
, ~ T ~ J ~ ~ Hem+CRFg-41 1 0 0 - ~ J- ~ CRF941
O - i . . . . . . . . . . i
0 15 35 55 TIME (min)
Fig. 1. Effects o f CRF 9--41 (50 #g) and 30% hemorrhage (performed immediately after the t = 0) on plasma concentrations of norepinephrine and epinephrine. Hemorrhage (Hem) alone, closed circles; CRF 9--41 alone, open circles; Hem plus CRF 9-41, open triangles. CRF 9-41 was given icv 15 min prior to the t = 0 sample. ** P < 0.01 compared to t = 0. Each group contained six animals.

324
TABLE 1
Effects o f CRF 9-41 on insulin-induced elevation of plasma epinephrine levels
Treatment Plasma epinephrine concentrations (pg/ml)
Time (min): 0 40 60
Control 25 + 5 28 + 4 40 4- 7 Insulin 28 4- 6 228 4- 35** 236 4- 42** Insulin + CRF9-41 ( - 1 5 ) 29 4- 6 71 4- 22 143 4- 29** Insulin + CRF 9-41 ( - 4 5 ) 21 ± 1 175 4- 40 552 4- 139"
CRF 9-41 (50 #g) was given icv 15 or 45 min prior to administration of insulin (1 U, iv). * P < 0.05, • * P < 0.01 compared to t = 0 within each group. P < 0.01 compared to insulin treatment alone. Each group consisted of six animals.
Table I shows the effects of insulin-induced hypoglycemia on plasma concentra- tions of epinephrine and norepinephrine. CRF 9-41 was administered 15 or 45 min prior to iv administration of 1 U of regular insulin. Insulin treatment alone resulted in significant elevation of plasma concentrations of epinephrine, but not norepine- phrine (data not shown). CRF 9-41 given 15 min prior to insulin significantly atten- uated the rise of plasma epinephrine.
2500 1 2000
,~ 1500
1000
500
0
1200 1 1000 - - 8 0 0
600 4O0 200
/~om -Bom + CRF 9-41
Born + SS-28
NOREPINEPHRINE
~ Born + SS-28
"±\Bom + CRF 9-41
300 q GLUCOS___,~E
2 5 0 ** ** Born + CRF 9-41 -'5 Born
~, 200 ** ~ *% .or,', + SS-: 'e
150
100 r i T = 0 20 40 80
TIME (min) Fig. 2. Effects of bombesin (Born, 1 #g) and CRF 9-41 (50 #g) or somatostatin-28 (SS-28, 3 #g) on plasma concentrations of norepinephrine and epinephrine. Born and CRF 9-41 were given icv as a mixture after obtaining the t = 0 sample. * P < 0.05, ** P < 0.01 compared to the t = 0 values. Bona + SS-28 is significantly different (P < 0.01) from Born alone for epinephrine and glucose at all time points. Each group contained six animals.

325
Fig. 2 shows the effects of CRF 9-41 and somatostatin-28 (SS-28) on bombesin- induced elevation of plasma concentrations of catecholamines and glucose. As we have previously observed, SS-28 completely prevented bombesin-induced elevation of plasma epinephrine levels. In contrast, CRF 9-41 did not significantly modify bombesin-induced elevation of plasma epinephrine concentrations.
To determine the effects of CRF 9-41 on cardiovascular function, we assessed the effects of this peptide antagonist on MAP and HR in Sprague-Dawley rats as well as in SHRs with fully developed hypertension and in WKY rats. Fig. 3 shows the effects of CRF 9-41 on CRF-induced elevations of MAP and HR in Sprague-Dawley rats. The antagonist alone did not modify MAP but'produced a transient elevation of HR. CRF-induced elevation of MAP and HR were attenuated by co-administra- tion of the antagonist. In 10-week-old spontaneously hypertensive rats, icv admin- istration of CRF 9-41 did not alter MAP or HR (Table II).
To further assess the possible effects of the C R F gjltagonist on cardiovascular function, experiments were carried out in animals in whom MAP and HR were ele- vated by electrical stimulation of the central nucleus of the amygdala. Stimulation of the amygdala resulted in significant elevation of MAP and HR when the electrode tip was located within the central nucleus. As shown in Table III, icv administration of the CRF antagonist did not significantly attenuate the increase of MAP or HR following amygdala stimulation.
130
~') 120
E: D..
"J ~ ' 110- <
~ N lOO- < Z < uJ 90
500 t
4ooj 35O
.. LJ7 F
ANT
i l l I J * l * l I J
L . ** ** ** • .~. I z T
T
I I I o lo 20 3'o ,'o 6'o 6'0
TIME (min)
Fig. 3. Effects of CRF (10 #g) and CRF 9--41 (ANT, 100 #g) on mean arterial pressure and heart rate. CRF and/or CRF 9-41 was given icv immediately after the t = 0 point. * P < 0.05, ** P < 0.01 compared to the t = 0 values. Each group contained six animals.

326
TABLE II
Effects of CRF 9-41 on MAP and HR in SHR and WKY rats
Treatment Time (min)
0 10 20 30
HR (beats/min)
WKY Control 319 4- 9 329 4- 12 323 4- 13 324 4- 8
WKY + CRF 9-41 307 4- 12 348 4- 11 329 4- 24 311 4- 13
SHR Control 351 4- 9 380 4- 12 360 + 9 351 4- 9
SHR + CRF 9-41 374 4- 13 390 4- 18 391 4- 14 409 4- 23
MAP (mm Hg)
WKY Control 117 4- 3 117 4- 7 120 + 9 120 + 7
WKY + CRF9-41 113 4- 6 117 4- 5 111 4- 4 110 4- 5
SHR Control 166 4- 7 166 + 6 171 4- 8 162 5 : 9
SHR + CRF9-41 159 4- 7 166 4- 6 161 + 3 166 + 9
CRF 9-41 (50 ~g) was given icv after the t = 0 values were obtained. Each group consisted of six animals.
To determine if the CRF antagonist would alter baroreflex-induced changes of HR, animals were given intravenous infusions of nitroprusside (40 ug/kg) after icv administration of the CRF antagonist. As shown in Table IV, the CRF antagonist did not modify the tachycardia or hypotension following nitroprusside infusion.
TABLE III
Effects of CRF 9-41 on central nucleus of the amygdala (CNA) stimulation-induced elevations of MAP and HR
Treatment Time (min)
Pre-stim Post-stim - 1 Post-stim - 2
HR (beats/min)
CNA stim a 376 ± 4 402 4- 4** 404 4- 6**
CNA stim + CRF 9-41 b 374 4- 9 410 ± 15 412 4- 10'
MAP (mm Hg)
CNAs t im a 101 4- 3 115 4- 3* 115 4- 4* CNA stim + CRF 9-41 b 98 4- 4 114 4- 5* 111 4- 3*
a After the pre-stimulation values were obtained, 30 s of electrical stimulation was delivered. Post-stimu- lations 1 and 2 correspond to I0 and 20 s after initiation of the electrical stimulus.
b Following recovery of MAP and HR to baseline, second pre-stimulation values were recorded followed
by icv administration of CRF 9-41 (10 #g) or control injections. 20 min later, a repeat 30-s electrical
stimulation was delivered. Post-stimulation MAP and HR correspond 10 and 20 s after this stimulation. Each group consisted of six animals.

TABLE IV
Effects of CRF 9-41 on MAP and HR in nitroprusside (NP) treated rats
327
Treatment Time (min)
+ Baseline 15' post NP Post-NP CRF 9-41
HR (beats/min) NP 363 + 6 393 4- 20 555 + 21"* 383 -4- 4 NP + CRF9-41 379 + I0 392 + 17 537 + 9** 388 4- 8
MAP (mm Hg) NP 107 4- 4 105 + 3 72 4- 4** 110 + 6 NP + CRF9--41 110 ± 4 102 q- 4 75 4- 3** 107 4- 4
After obtaining baseline values, CRF 9-41 or vehicle was given icy. 15 min after these treatments, NP (40 /~g/kg per min) was infused for 10 min. Post-NP values were obtained 5 min after stopping the NP infusion. ** P < 0.01 compared to the baseline values. Each group consisted of six animals.
Discussion
Similar to previous studies in which it was reported that C R F 9-41 inhibited ether vapor-induced epinephrine secretion [4], the results of the current study indicate that C R F 9-41 is capable of reducing the rise of plasma epinephrine following 30% hem- orrhage and insulin-induced hypoglycemia. Thus, C R F 9-41 supresses adrenal epi- nephrine secretion in three separate animal models. These animal paradigms were
chosen because of the prominent plasma elevations of epinephrine concentration found in each case.
The lack of effect of C R F 9-41 on bombesin-induced elevation of plasma epi- nephrine levels provides evidence that C R F is not involved in mediating this CNS action of this peptide. This finding is not surprising considering the other CNS actions of bombesin that are widely divergent from those of C R F [7].
We have recently reported that C R F produces a profound increase of the concen- trations of epinephrine and glucose in the SHR compared to normotensive W K Y or the Sprague-Dawley rats [8]. Icv administration of C R F has little effect on MAP or H R in the SHR, although C R F does cause a significant increase of M A P and H R in the normotensive W K Y and the Sprague-Dawley rat. It is of interest that the C R F antagonist did not modify the MAP or H R in the SHR. Since these rats are in a fixed hypertensive state, the lack of effect of the C R F antagonist may not be mean- ingful in evaluating the possible function of C R F in the pathogenesis of their hyper- tension. To address this issue similar studies need to be carried out in younger non- hypertensive SHRs.
Central nucleus of the amygdala stimulation has been reported to result in an increase of M A P and H R in the cat and rat [9,10]. The CNA is a source of descending C R F pathways to brainstem autonomic regions and participates in stress-induced

328
alteration of cardiovascular function [9-11,12]. The possible role of CRF in the CNA-induced elevation of MAP and HR was tested using the CRF antagonist. The results demonstrate that the CRF antagonist does not alter amygdala stimulation- induced increase of MAP and HR. These results suggest that endogenous CRF is not necessary for expression of the cardiovascular changes following stimulation of the central nucleus of the amygdala. Participation of CRF in amygdaloid-mediated cardiovascular responses cannot be excluded from these data. CRF-containing path- ways emerging from the CNA could be involved in mediating cardiovascular re- sponses other than those produced by electrical stimulation of this nucleus.
We have recently demonstrated that CRF-induced elevation of HR is accompanied by a resetting of baroreflex gain [2,13]. To test whether a CRF antagonist would interfere with baroreflex-induced changes of HR, studies with nitroprusside were performed. The results of these experiments fail to demonstrate an exclusive role of CRF in mediating the tachycardia following nitroprusside-induced hypotension.
These studies further support the contention that endogenous brain CRF partici- pates in the regulation of adrenal epinephrine secretion. The existence of non-CRF containing neuropathways capable of eliciting adrenal epinephrine secretion is indi- cated by the results of the studies using bombesin. The current studies failed to demonstrate a putative role of CRF in regulation of cardiovascular function under the experimental conditions described. These observations do not exclude a role of CRF in mediating changes of cardiovascular function under different conditions.
Acknowledgements
Research supported by NIH Grants AM26741, HL32008, HL37716 and NS20041. The authors thank Dr. Jean Rivier for generously providing peptides, Karen Carver, Sandra Braun, Winnie Bartholomeus and Marty Mortrud for expert technical as- sistance, and Dorothy Weigand for manuscript preparation.
References
1 Vale, W., Rivier, C., Brown, M.R., Spiess, J., Koob, G., Swanson, L., Bilezikjian, L., Bloom, F. and Rivier, J., Chemical and biological characterization of corticotropin-releasing factor, Rcc. Prog. Hor- mone Res., 39 (1983) 245-270.
2 Brown, M.R. and Fisher, L.A., Corticotropin-releasing factor: effects on the autonomic nervous system and visceral systems, Fed. Proc., 44 0985) 243-248.
3 Sutton, R.F., Koob, G.F., LeMoal, M., Rivier, J. and Vale, W., Corticotropin-releasing factor pro- ducts behavioral activation in rats, Nature, 297 (1982) 331-333.
4 Brown, M.R., Fisher, L.A., Webb, V., Vale, W.W. and Rivier, J.E., Corticotropin-releasing factor: a physiologic regulator of adrenal epinephrine secretion, Brain Res., 328 (1985) 355-357.
5 Brown, M., Tache, Y. and Fisher, D., Central nervous system action of bombesin: mechanism to induce hyperglycemia, Endocrinology, 105 (1979) 660-665.
6 Peuler, J.D. and Johnson, G.A., Simultaneous single isotope radioenzymatic assay of plasma norepi- nephrine, epinephrine and dopamine, Life Sci., 21 (1977) 625~36.
7 Brown, M. and Fisher, L., Regulation of the autonomic nervous system by peptides. In A. Negro-

329
Vilar and P.M. Conn (Eds.), Peptide Hormones: Effects and Mechanisms of Action, CRC Press, Boca Raton, FL, 1986, in press.
8 Brown, M.R. and Fisher, L.A., Autonomic and cardiovascular effects of corticotropin releasing factor (CRF) in the spontaneously hypertensive rat (SHR), Soc. Neurosci. Abstr., (1986) in press.
9 Stock, G., Schmelz, M., Knuepfer, M.M. and Forssmann, W.G., Functional and anatomic aspects of central nervous cardiovascular regulation. In D. Ganlten and D. Pfaff (Eds.), Central Cardiovascular Control, Springer-Verlag, Berlin, 1983, pp. 1-30.
10 Galeno, T.M. and Brody, M.J., Hemodynamic responses to amygdaloid stimulation in spontaneously hypertensive rats, Am. J. Physiol., 14 (1983) R281-R286.
11 Veening, J.G., Swanson, L.W. and Sawchenko, P.E., The organization of projections from the central nucleus of the amygdala to brainstem sites involved in central autonomic regulation: a combined retograde transport-immuno-histochemical study, Brain Res., 303 (1984) 337-357.
12 Moga, M.M. and Gray, T.S., Evidence for corticotropin-releasing factor, neurotensin, and somatos- tatin in the neural pathway from the central nucleus of the amygdala to the parabrachial nucleus, J. Comp. Neurol., 241 (1985) 275-284.
13 Fisher, L.A., Corticotropin-releasing factor: effects on baroreflex control of heart rate, Soc. Neurosci. Abstr., 11 (1985).