Embed Size (px)
Citation preview

rates of smoking currently prevailing. The new healthwarnings on cigarette packets at least mention the dangersof smoking during pregnancy. These warnings and thelanguage in which they are expressed may not be clearlyunderstood by all pregnant women in South Africa. Finally.effective media programmes directed at the public at largeare required to highlight the dangers of passive smoking.especially to pregnant women and their unborn children.
REFERENCES
1. S,mpson WJ A preliminary report on cIgarette smokIng and tne IncIdence ofpremarunty. Am J Obsrer Gynecol 1957; 73: 808-815.
2. Floyd AI. Zahnlser C, Gunter EP. Kendrick JS. Smoking durm9 pregnancy:Pre~alence. effects and intervention strategies. Birth 1991; 18: 48·53.
3. Klemman JC. Madans JH. The effects ot maternal smoking. physical stature andeducational attainment on the inCidence 01 low birtnwelght. Am J Epidemiol1985: 121: 8':3-855,
.:. UlIas HA. Counsell AM, Oa~id C, Sanders G, Sanders OM. First report from thePunket National Child Health Study: smokmg dunng pregnancy in New Zealand.Peedlatr Pennar Epldemlol1993: 7: 318-333.
5. undqvist A. Aberg H. Smoking habits before. during and aftl!i" pregnancy amongS.... eel:sh women ano lhe,r partners in suburban StOCkholm. Scand J Pnm Hea/tnCare 1992; 10: 12-15.
6. Brooke OG. Anderson HR, Bland JM, Peacock JL. $tewart CM. EffeclS on birthweight of smolung, alcohol, caffell'le. sOClo-econom,c factors. and psycnologicalslress. BMJ 1989: 298: 795-801.
7. Butler NA. Golc!stell'l H. Smo 1'19 in pregnancy and subsequent clulddevelopment. BMJ 1973; 4: 573·575.
8. Rantakallio P. A follow up study up to the age of 1': of chilcren wnose motherssmoked during pregnancy. Acta Paediau Scand 1983: 72, 7~7-753.
9, Ounn GH, McBurney AK. ln9ram S, Hunter CM. Maternal cigarette smokingdUring pregnancy and chIld's subSEquent development. Can J Public Health1976; 67: 499-505.
10, Wingerd J. Schoen EJ. Factors influencing health at birth and neight at liveyears. Pediatrics 1974; !53: 737-7011.
11. Fogelman KR. Manor O. Smoking in pregnancy and development into eatlyadulthOOd. BMJ 1988: 297: 1233-1236.
12. Hardy J6. MeJlits EO. Does maternal smoking during pregnancy hil~e e long termeffect on thech,ld? Lancet 1972; 2; 1332-1336.
13. Lelkowitz MM. Smolting during pregnancy: long tl!f"m effects on offspnng.Development Psycnology 1981; 17: 192-19':.
14. Ferguson OM. Uoyd M. Smoking ouring pregnancy an<:! its effecls OIl cMd cognmveability from ages 8 - 12 yeat'$. Paetfi.au Perinli!t Eplriemioll991; 5: 189-200.
15. Klemrnan JC. Pierre MB jun. Madans JH, land GH. Scnramm WF. The effects ofmaternal smoking on fetal and infant mortality. Am J Epic!emio/198a; 127: 27':-282.
16. MartIn TR. Bracken MB. AsSOCIatIon of low blrthwelght WIth passIve smokeexposure during pregnancy. Am J Epicemlol1986; 124: 633-642.
17, RubIn OH, Krasilnikoff PA, Levenlhal JM, Weile B, Serget A. Effect of passIvesmokIng on bIrth weIght. Lancet 1965; 2: ':t5·':17.
t8. Mau G. Netter P. The effect 01 paternal smokll'lg on perinatal mortality and theIncidence of malformations. Otscfl Med Wocflenscflr 1974; 99: 1113-11 t8.
19. Martin G. Steyn K, Vach O. Beliefs about smokIng and health and atlitudestoward tobacco control measures. S Afr Med J 1992: 82: 2~1-245.
20. Redtly P. Meyer-Weitt A. Yach O. Smoking status, knowledge of health effects andattitudes towards tobacco control in South Africa. S AJr Med J 1996: 86: 1369-1393.
21. National Children'S Rights Committee, UNICEF. Ctu/dren and Women In SouthAfrica: A Situation Analysis. Johannesburg: UNICEF and National Children'sR,ghlS Commlne.e. 1993: 138-148.
22. RothbE!f9 AD, Shuenyane E. l.rts 8. Strebel PM. Medical ...,dlor obstetricproblems and bjrthwe'Qht In twO Johannesburg populations. S AJr J EpldemlolInfect 1990; 5(2): 37-39.
23. Vach 0, Richter L. Camotron N, Von Sch,rnding YEA, De Wet T. Mate-rnaleducation and child health: emetgmg evidence from 6lrth-to-Ten. Ureamsauonand Health Newsletter 1993; 18 (Part 2); 37-~7.
2.:. HauIjI K. Aaro LE., Fugelli P. Pregnancy - a Qolcen opportunity for promotIng thecessauon of smoking? Scand J Prim Health Care 1994; 12(3}: 16~-189.
25. De Vnes H. Sackbier E. Self·efficacy as an important c!etemunant of Quitting amongpre-gnant women who smoke: tne phi-pattern. P~v Med 199~; 23{2}: 167-174.
26. Fingemut tA. Kleinman JC, Kendric'''I JS. Smoking before. dunng and afterpregnancy. Am J Public Healrh 1990; 80: 541 -544.
27, Brenner H. Mielck A. The rOle of child birth in smoking cessation. Prev Med 1993;22(2): 225-236.
28. Olsen J. Predictors of smoking cessation 11'1 pregnancy. Scand J Soc Med 1993:21(3): 197-202.
29, Greenberg RA. Haley NJ. Euel RA, Loda FA. Measunng me exposure 01 infantsto tobacco smoke, nlcotlne and cotinll'le in unne and saliva. N EngJ J Med 1984;310: 1075-1076.
30. Mal$ukura 5, Taminto T, KitanO N. EffeclS of envlfOflmental tooacco smoke onunnary cotitllne excretion In non-smO"lers. evidence of passIve smokmg. N Engl JMer; 1964; 311: 828-032.
31 US Department of Health and Hloman ServIces Promoting HeiIJrn Pre,enl1ngO,sesS4: Y1!!M 2000 ObjectIves for the NalJcn. Washmgion DC: US Go"ernmentPrlnang Office 1989.
32, LJ ca, Winc!sor RA, Lowe J6, Goleenoerg RL Evaluation of the Impact ofdiSHmmallon of smoking cessanon meltlocs on the low tllrmwe,ght rate and enhealtn care costs: achlevmg year 2000 objecllves for the nation. Am J Prev Med1992; 8: 171-177.
33. Windsor RA. U ca. Lowe JB. Perklns LL ErshoH 0, Glynn T. The dIsseminationof smoking cessation methods for pregnant women: achieving the year 2000oblectives. Am J Public Health 1993: 83: 173·178.
3<:. Marks JS, Koplan JP, Hogue CJR. Oalmat ME. A cost-benelitlcost-eHectl~eness
analySIS 01 smoking cessation for pri!"{;nant women. Am J Prey Med 1990; 6: 282289.
AcceptlMi 16 May 1996.
SAMJARTICLES
Cost-effective on-sitescreening for anaemia inpregnancy in primary careclinicsDavid Wilkinson, Martene E Sach
Objective. To determine the feasibility, accuracy and cost
of develop!ng a system of on-site screening for anaemia in
pregnancy in primary care clinics.
Setting. Mobile clinic team in Hlabisa health district,
Kwazulu-Natal.Methods. Four hundred and forty-nine consecutive
women attending antenatal clinics were screened for
anaemia (haemoglobin < 10 g1dl) using copper sulphate
solution; the results were compared with true haemoglobin
levels as determined by an automated analyser. Three
hundred women had haemoglobin concentration
estimated with a portable haemoglobinometer and results
compared with those from the automated analyser.
Results. Screening with copper sulphate solution was
highly sensitive (95.7%) but had low positive predictive
value for anaemia (37.2%). Haemoglobin concentration
estimated by haemoglobinometer correlated highly with
results from the analyser (r =0.82; P < 0.0001), and the
mean difference in concentrations between the two
methods was 1,1 g/dl. The average cost of screening all
women with copper sulphate solution (6 cents/sample)
and determining the true concentration in those screened
as possibly anaemic (R2.64/sample) was 72 cents per
woman. The cost of using an automated analyser was
R6.20 per sample.Conclusion. Combined use of copper sulphate solution
and a haemoglobinometer is a feasible, accurate and
cost-effective way of screening for and diagnosing
anaemia in pregnant women. on-site, in primary care
clinics.
S AIr Med J 1997; 87: 463-465.
Screening for anaemia in pregnancy is integral to antenatalcare, as anaemia contributes to both adverse pregnancyoutcome for the fetus and increased risk of maternal death.'Most women in South Africa receive their antenatal care atclinics that do not have laboratory facilities close by. Manyclinics are rural and isolated, and some mobile clinic points
Centre for Epidemiological Research in Southern Africa, MedicalResearch Council and Hlabisa Hospital, Hlabisa, KwaZulu·Natal
David Wilkinson. 6Se. MS Cl'tS, Dip FEC, OCH, OTM&H, MSc (Epi)
Martene E Sach RGN
SAMJ Volume 8i !to-a, 4 April 1997 _

are only visited monthly. Blood is usually taken at the initialvisit and transported to a laboratory for estimation of thehaemoglobin concentration and to perform Rhesus andsyphilis serology. Results are returned days or weeks laterdepending on local circumstances.2 For some mobile clinicsin rural areas, this delay may be as long as a month.
On-site screening for anaemia in primary care clinics isdesirable, as it would allow therapy to be institutedimmediately. However, on-site screening, as well as beingquick and convenient for the midwife, also needs to beaccurate and reliable. Furthermore, those identified asprobably anaemic still require a diagnostic test to determineactual haemoglobin concentration, because although mildanaemia could be treated at the clinic, more severe anaemiamight require referral. Is there a strategy that allows rapid,accurate and cheap screening for and diagnosis of anaemia,at primary care clinics?
Copper sulphate solution, although routinely used byblood transfusion services to screen for anaemia, does notquantify haemoglobin concentration. Portablehaemoglobinometers, although they quantify haemoglobinconcentration, are expensive, may require a power source(Which many clinics in South Africa do not have) and alsorequire maintenance.
The aim of this study was to determine the feasibility,accuracy and cost of developing a system of on-sitescreening for anaemia in pregnancy that uses a copperSUlphate solution to screen all women, and ahaemoglobinometer to quantify haemoglobin concentrationin those screened as possibly anaemic.
Methods
SettingThe Hlabisa health district of northern Kwalulu-Natal islargely rural and remote. The maternity service comprisesHlabisa Hospital, 8 primary care clinics, and 20 mobile clinicpoints. Antenatal care is provided to around 8 000 womeneach year. A recent community survey estimated that 95%of women in the district had received antenatal care duringtheir previous pregnancy.
Screening with copper sulphateFor this feasibility study one mobile clinic team, serving 14clinic points across the district, was selected. A coppersulphate solution with specific gravity 1.048 (Clinical ScienceDiagnostics, Halfway House, South Africa) was used toscreen 449 consecutive women booking for antenatal care.Venous blood was taken from the antecubital fossa with a5 ml syringe. Prior to storing blood in tubes for transport tothe Hlabisa laboratory, one drop of blood was dropped intothe copper sulphate solution from a height of 1 - 2 cmabove the surface. The momentum of the drop carries itthrough the surface and the drop then gradually slows. If thedrop of blood is more dense (> 10 g/dl haemoglobin) thanthe solution, it will continue to fall; if the drop is less dense« 10 g/dll, it will then rise back through the solution. If thedensity of the blood and the solution are equal (10 g/dl), thedrop will slow, stop for a few seconds and then dispersewhile slowly sinking. Anaemia was defined as a haemoglobin
_ Volume 87 No. ~ April1997 SAMJ
concentration of less than 10 g/dl as determined by anautomated haematology analyser (Sysmex).
HaemoglobinometerA f)-haemoglobin photometer (HemoCue, HemoCue AB,Sweden) was used to estimate the haemoglobinconcentration in 300 different consecutive women attendingthe same clinic. A drop of blood is drawn up by capillaryaction into a microcuvette which is then placed in thehaemoglobinometer. The result, to one decimal place, isdisplayed on the unit 45 seconds later. No technical skillsare required. This unit is battery or mains powered and isquite robust.
Laboratory methodsBlood was placed in an EDTA tube, stored in a cool boxcontaining ice packs and taken to the laboratory the sameday. There it was stored at 4°C until haemoglobinconcentration was estimated with the Sysmex analyser (CAMilsch, Johannesburg) within 48 hours. The concentration ofhaemoglobin determined by the Sysmex was considered the'gold standard' and results obtained from copper sulphatesolution and the haemoglobinometer were compared with it.
Data analysisData entry and analysis were by means of Epi-Info version6.02 (Centers for Disease Control, Atlanta, USAl. Results arereported as sensitiVity, specificity, positive predictive valueand negative predictive value, with their 95% confidenceintervals. The correlation coefficient and scatterplot wereobtained wrth the BMDP package (BMDP StatisticalSoftware, Los Angeles).
Results
Copper sulphate screeningThe prevalence of anaemia among the 449 women screenedwith copper SUlphate (Table I) was 10.5%. This screeningstrategy was sensitive (95.7%) and reasonably specific.However, the predictive value of screening as anaemic(37%) was poor because several samples with a truehaemoglobin ~ 10 g/dl were screened as < 10 g/dl.However, 326 (73%) samples from women with haemoglobin'" 10 g/dl would correctly not have been sent to the districtlaboratory for further examination using this approach. Thetwo samples wrongly screened as > 10 g/dl both had truehaemoglobin concentrations of 9.4 g/dl.
Table J. Copper sulphate screening compared with Sysmexhaemoglobin analyser
Sysmex
Copper sulphate Hb < 10 gldl Hb'" 10 gldl Totals
< 10 gldl 45 76 121
" 10 gldl 2 326 328- -- --Totals 47 412 449
5ensitrvity (95"'0 confidence interval) = 95.7"'0 (84.3 - 99.3%).Speoficity = 81.1% (76.a - 84.7'0).f'osItJve predictive value" 37.2 (28.7·40.5"0).Negati've predictive value = 99.4% (97.6 • 99.9%).

v.a
".".......".".".".
3 "."....~
...••
f ••." ••J~ ••i! ,.-- ,.!!
••
.......It ."
I. ~ •.'
.-' .....:1 !J
• .t-I" ';" ........- .
I
SAMJARTICLES
be done anywhere, offers the opportunity to reduceunnecessary morbidity and mortality. Apart from absolutecost-savings, which are considerable, the opportunity costsof switching to on-site screening are noteworthy. Testingantenatal specimens in this district requires several hours oflaboratory time each week :- time that could probably bemore usefully spent on other tasks.
Antenatal clinics in KwaZulu-Natal currently screen forRhesus antibodies on site, and it is technically quite feasibleto screen for anaemia, as shown here, and for syphilis.s Thisapproach could put an end to delays in receiving results,3the need to retake specimens because of haemolysis anddelays in initiating therapy.s In response to these findings,the mobile clinic team now does on-site screening andtesting for anaemia, syphilis and Rhesus antibodies, and theservice is being expanded across the district.
REFERENCES
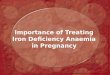
Fig. 1. Scatter plot of haemoglobin concentrations byhaemoglobinometer and Sysmex.
HaemoglobinometerAmong the 300 samples tested with thehaemoglobinometer, the prevalence of anaemia was 5%.The correlation (figure) between the results obtained on siteand in the laboratory was high (r = 0.82, P < 0.0001). Themean haemoglobin concentration estimated on site (11.5g1dl, SO 1.1) was lower than that estimated in the laboratory(12.7 g1dl. SO 1.2). The mean difference between the pairedtests was 1.1 g/dl (SO 0.7) with a range of -1.3 to 5.0; in48% of cases the difference was 1.0 gldl or less and in 88%it was 1.5 gldl or less.
CostsThe cost of estimating haemoglobin concentration with aSysmex analyser is around R6.20 per sample,4 comparedwith 72 cents per sample if all samples are first screenedwith copper sulphate solution (6 cents per sample) and ifthose estimated < 10 g1dl (25% in this study) are then testedwith the haemoglobinometer (R2.64 per sample).
DiscussionThis study shows that the combined use of copper sulphatesolution supplemented with a haemoglobinometer, is afeasible, accurate and cost-effective way of screening forand diagnosing anaemia in pregnancy on site in primarycare clinics.
With this strategy, most women without anaemia will becorrectly screened out by the copper sulphate solution, andthose who are possibly anaemic will have their truehaemoglobin concentration measured. This can then beacted upon, according to local protocols, with only severecases being referred for further examination andinvestigation.
This is not a trivial issue. Anaemia contributes to maternaland perinatal mortality. IOn-site screening ensures thatanaemia is diagnosed at the initial visit, and that therapy orreferral is instituted immediately. On-site testing, which can
1. World Health Organlsauon. Prevention and Marragemenf of Severe Anaemia inPregnancy. Geneva; Wend Health Organisallen. 1993.
2. Fonn S. A blood·result turn-around time survey to improve congenital syphilis ina rural area. S Afr Med J 1996; 86: 67-71.
3. Wilkinson O. Cuns F. Ntuli N, Abdool Karim SS. Maternal and child healthindicators in a rural South African health district, S Afr Med J 1997; 87: 456-459(this issue).
4. Medical Association of South Africa. Guide fO Fees for Medical Services. CapeTown: MASA Publications, 1995.
5. Delport SO. On·site screening for maternal syphHls in an antenatal clinic. S AfrMed J 1993; 83: 723-724
6. Wilkinson 0, Sach M, Connoliy C. Epidemiology of syphilis in pregnancy in ruralSouth Africa: opportunities for control. Trop Med Int Health 1997: 2: 57·62.
Accepted 28 Nov 1996.
SA-MJ Volumt8i No.4 Aprill99i __


![Anaemia in Pregnancy: Prevalence, Risk Factors, and ......Anaemia during pregnancy is a public health problem especially in developing countries and is associated with adverseoutcomesinpregnancy[].WorldHealthOrgani-zation](https://img.pdfslide.net/doc/110x75/60df1f679f6a99520b461cd1/anaemia-in-pregnancy-prevalence-risk-factors-and-anaemia-during-pregnancy.jpg)