Embed Size (px)
Citation preview

Cost-utility analysis of prehospital spine immobilizationrecommendations for penetrating trauma
Arturo Garcia, MD, Terrence H. Liu, MD, MPH, and Gregory P. Victorino, MD, Oakland, California
BACKGROUND: The American College of Surgeons’ Committee on Trauma’s recent prehospital trauma life support recommendations againstprehospital spine immobilization (PHSI) after penetrating trauma are based on a low incidence of unstable spine injuries afterpenetrating injuries. However, given the chronic and costly nature of devastating spine injuries, the cost-utility of PHSI isunclear. Our hypothesis was that the cost-utility of PHSI in penetrating trauma precludes routine use of this prevention strategy.
METHODS: AMarkov model based cost-utility analysis was performed from a society perspective of a hypothetical cohort of 20-year-oldmales presenting with penetrating trauma and transported to a US hospital. The analysis compared PHSI with observationalone. The probabilities of spine injuries, costs (US 2010 dollars), and utility of the two groups were derived from publishedstudies and public data. Incremental effectiveness was measured in quality-adjusted life-years. Subset analyses of isolated headand neck injuries as well as sensitivity analyses were performed to assess the strength of the recommendations.
RESULTS: Only 0.2% of penetrating trauma produced unstable spine injury, and only 7.4% of the patients with unstable spine injurywho underwent spine stabilization had neurologic improvement. The total lifetime per-patient cost was $930,446 for thePHSI group versus $929,883 for the nonimmobilization group, with no difference in overall quality-adjusted life-years.Subset analysis demonstrated that PHSI for patients with isolated head or neck injuries provided equivocal benefit overnonimmobilization.
CONCLUSION: PHSI was not cost-effective for patients with torso or extremity penetrating trauma. Despite increased incidence of unstablespine injures produced by penetrating head or neck injuries, the cost-benefit of PHSI in these patients is equivocal, and furtherstudies may be needed before omitting PHSI in patients with penetrating head and neck injuries. (J Trauma Acute Care Surg.2014;76: 534Y541. Copyright * 2014 by Lippincott Williams & Wilkins)
LEVEL OF EVIDENCE: Economic and value-based evaluation, level II.KEY WORDS: Prehospital spine immobilization; spinal cord injury; penetrating trauma; unstable spine injury; cost-utility analysis.
Spine immobilization in patients with an unstable vertebralinjury can prevent subsequent neurologic deterioration
when the spinal cord is undamaged by the initial trauma. Inblunt trauma, the forces of abrupt deceleration can cause adisruption of the boney and ligamentous structural support,resulting in an unstable spinal injury, which can lead to spinalcord injury when left without immobilization.1 The mechanismof spine injury in penetrating trauma is different from that ofblunt trauma in that the penetrating object itself causes thedamage to the spinal cord.2 Unstable vertebral injuries are lesscommon with penetrating trauma, and patients who experiencethese injuries as the results of penetrating trauma usually havealso sustained permanent irreversible spinal cord injury fromthe initial insult.3 Together, these make spine immobilizationa less effective strategy for spinal cord injury prevention inpenetrating trauma.
The benefit of field interventions such as spine immobili-zation for penetrating trauma patients remains controversial.4 Therehas been a paradigm shift toward minimizing field interventionsand prehospital care by emergency medical service providers toexpedite transport to a trauma center to receive definitive care.5Y7
Procedure-driven, time-intensive approach to emergency medicalservice care with an emphasis on field stabilization needs to bebalancedwith abbreviated scene time and rapid transport time, withthe goal of getting the patient to definitive care in a hospital asquickly as possible. This balance is one of the cornerstones ofprehospital trauma life support (PHTLS).8
In 2011, the PHTLS programVan educational effort foremergency medical technicians, paramedics, and nurses spon-sored by the National Association of Emergency Medical Tech-nicians and the American College of Surgeon’s Committee onTraumaVrevised its recommendations for prehospital spine im-mobilization (PHSI) in cases of penetrating trauma. These newrecommendations stated that there are no data to support routinePHSI in patients with penetrating trauma to the neck, torso, orcranium; PHSI should never be performed at the expense ofaccurate physical examination or identification and correction oflife-threatening conditions; and PHSI may be performed afterpenetrating injury when a focal neurologic deficit is noted onphysical examination, although there is few evidence of benefiteven in these cases.
The new recommendations were based on a literature reviewby the PHTLS Executive Committee that found that the overallincidence of unstable spine injury without spinal cord injury in
ORIGINAL ARTICLE
J Trauma Acute Care SurgVolume 76, Number 2534
Submitted: April 17, 2013, Revised: June 18, 2013, Accepted: September 9, 2013.From the Alameda CountyMedical Center, University of California, San FranciscoYEast
Bay, Oakland, CA.This study was presented at the Academic Surgical Congress, February 5Y7, 2013, in
New Orleans LA.Supplemental digital content is available for this article. Direct URL citations appear
in the printed text, and links to the digital files are provided in the HTML text ofthis article on the journal’s Web site (www.jtrauma.com).
Address for reprints: Arturo Garcia, MD, Department of Surgery, Alameda CountyMedical Center, 1411 East 31st St, QIC 22134, 3rd Floor Oakland, CA 94602-1018; email: [email protected].
DOI: 10.1097/TA.0b013e3182aafe50
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

penetrating trauma is low and often reported as zero.3 However, theprolonged hospitalization, extensive posthospitalization rehabili-tation, and lifelong disability encountered by spinal cord injurypatients are expensive and can range from $3 million to more than$5 million during the life-span of the individual.9 Furthermore,patients with spinal cord injury have a reduced life expectancyalong with varying degrees of disability, leading to personal op-portunity loss and higher societal costs.10When these societal costsare taken into consideration, the relative cost-effectiveness (CE)of PHSI versus nonimmobilization is uncertain.
In light of the chronicity and costs of these devastatingspinal injuries, the objective of this investigation was to comparethe CE of PHSI with no spinal immobilization in patients withpenetrating trauma. Our hypothesis was that the CE of PHSI forisolated penetrating trauma precludes the routine use of thisprevention method.
PATIENTS AND METHODS
Study DesignThisanalysiswasperformedusingastate-transition (Markov)
decisionmodel(SupplementalFigure1,http://links.lww.com/TA/A351)from the society prospective. Penetrating injury ismore commonin the male population and most commonly occurs in the secondand third decade of life;11 therefore, our study population wasa hypothetical cohort of 20-year-old males sustaining penetrat-ing trauma and transported to a US hospital emergency centerby ambulance. Decision software (TreeAge Pro HealthcareModule 2011, TreeAge Software, Inc., Williamstown, MA) wasused in the construction and analysis of our decision model. Thecycle time frame for the analysis was 1 year with an ana-lytic horizon that included the life-span of noninjured in-dividuals, based on a life expectancy of 77 years for 20-year-oldmales.12 This translates to 57 cycles of the Markov model afterwhich all states reached death. Patients reaching the death statebefore the 57th cycle were kept in the model to calculateopportunity loss.
Probabilities of Clinical EventsThe probabilities of events (Table 1) were derived from a
literature review by the PHTLS Executive Committee, whichidentified the incidence and natural history of spine injurycaused by penetrating trauma from a literature search.3
To summarize their methods, the search retrieved English-language articles from 1989 through 2011 relevant to the iden-tification of prehospital management of spine injuries as a resultof penetrating trauma.MeSH search terms includedpre-hospital,cervical spine, spine injury, and penetrating trauma. Lettersto the editor were excluded. The Cochrane Library online da-tabase was also queried for systematic reviews of PHSI andemergency intubations. Bibliographies of all reviewed articleswere cross-referenced to locate any relevant articles not locatedin the MeSH search. Unstable spine injuries were defined asthose identified as unstable or those in which surgical or non-surgical stabilization was instituted.
Cost DeterminationHospital costs of acute management of trauma were
derived from previously published studies examining the costs
of penetrating trauma management.33 Spine immobilizationand imaging costs were based on the reimbursement structureforMedicare as a representative of US payors using actual 2010Medicare reimbursements.34 Total first-year costs and yearlyhealth care and living costs for spinal injury patients wereobtained from the National Spinal Cord Injury StatisticalCenter, which captures approximately 13% of all nationalspinal cord injuries and publishes annual statistical reportsbased on their data collection and follow-up surveys of patientssustaining traumatic spinal cord injuries9 (Table 2). Incomeloss caused by paraplegia and tetraplegia was calculated basedon life expectancies of paraplegia and tetraplegia as well asrates of employment of persons with spinal injury obtainedfrom the National Spinal Cord Injury Statistical Center com-bined with earnings data from the Bureau of Labor StatisticsOccupational Employment Statistics.37 Opportunity loss andcost of living was calculated from published US expectancydata for the dollar value of the day10 and the Bureau of LaborStatistics.35 All costs were presented in US 2010 dollars andwere discounted at a rate of 3% per year.
Utility DeterminationUtilities for individuals with paraplegia and tetraplegia
were obtained from the study of Lin et al.,4 which providesstandard gamble utilities for individuals with traumatic spinalcord injury. Patients who recovered completely following pen-etrating trauma were considered to have a health utility stateof 0.75 for 6 months, thereafter returned to a health utility stateof 1 (Table 2). Patients who sustained spinal cord injury re-sulting in paraplegiawere considered to have a permanent healthutility state of 0.75. Patients who sustained spinal cord injuryresulting in tetraplegia were considered to have a permanenthealth utility state of 0.39. Patients who died were assigned ahealth state of 0. As per the Markov model, health states weresummed over all 57 cycles to obtain quality-adjusted life-years(QALYs). Utilities were discounted at a rate of 3% per year.
Sensitivity AnalysisSubgroup analyses were performed on base-case po-
pulations with different rates of spinal cord injury as a functionof the location of penetrating trauma categorized as (1) pene-trating injury to the head and face or (2) penetrating injury tothe neck. Probabilistic sensitivity analyses were performedusing Monte Carlo simulation consisting of 100,000 first-ordertrials to reflect the sampling uncertainty in the model inputs.One-way sensitivity analyses were also performed on all cost,incidence, and utility variables as well as age and discount ratein the main base-case population as well as the two subgroupanalyses of populations mentioned earlier.
AssumptionsSeveral assumptions were made during the construction
of the analysis. (1) The amount of time it took to place a patientin the field in spine immobilization was considered to be neg-ligible, and the time to intubation as well as the intubationcomplication rate in the PHSI group and the non immobilizationgroup were assumed to be identical. (2) The risk of computedtomography radiation-induced malignancies was not consideredduring this analysis. (3) Patients with spinal cord injury from
J Trauma Acute Care SurgVolume 76, Number 2 Garcia et al.
* 2014 Lippincott Williams & Wilkins 535
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

penetrating neck or head injury were assumed to have tetraplegiaand those with penetrating torso injury were assumed to haveparaplegia. (4) Neurosurgical stabilization procedures and pro-longed spine immobilization with rigid cervical spine collar orspine brace were considered interventions for unstable spineinjury. (5) No penetrating injury recidivism was taken into ac-count in our model.
RESULTS
Base-case analyses of 20-year-old males sustaining pen-etrating trauma demonstrated that only 0.18% of the penetrat-ing trauma patients had unstable spine injuries that may havebenefited from initial spine immobilization (Table 1). In addi-tion, only 7.44% of the patients with unstable spine injury
and who underwent surgical or prolonged nonoperative stabili-zation had neurologic improvement. PHSI had similar overallparaplegia and tetraplegia rates compared with nonimmobili-zation (paraplegia: PHSI, 0.90% vs. no PHSI, 0.91%; relative risk[RR], 0.98; confidence interval [CI], 0.85Y0.99) (tetraplegia:PHSI, 0.38% vs. no PHSI, 0.39%; RR, 0.97; CI, 0.89Y0.99) at1 year. There was no difference in mortality at 1 year between thetwogroups (PHSI, 7.99%vs. noPHSI, 7.99%;RR,1;CI0.99Y1.0;Table 2). The total mean lifetime per-patient cost was $930,446 T$1,253 in the PHSI group versus $929,883 T $1,255 in thenonimmobilization group (Table 3). The mean QALYs gainedper patient by successful surgical stabilization was 12.87, withan average cost-savings of $2,451,379 per patient; however,the mean total health care costs, living costs, and opportunityloss for a patient with spinal injury and neurologic deficits are
TABLE 1. Review of Evidence
References Study PopulationTotal
PatientsSpinal CordInjury, n (%)
Stable Spinal ColumnFracture WithoutCord Injury, n (%)
Unstable Spinal ColumnFracture, n (%)
No SpinalInjury, n (%)
Aryan et al.13 Penetrating bonyspine injury*
60 41 (68.3) 19 (31.7) 0 (0.0) 0 (0.0)
Barkana et al.14 Penetratingneck injury
44 10 (22.7) 1 (2.3) 3 (6.8) 32 (72.7)
Brown et al.15 GSW to the torso 357 17 (4.8) 13 (3.6) 1 (0.3) 324 (90.8)
Any GSW 75,210 1,040 (1.4) 2,176 (2.9) 26 (0.0) 71,994 (95.7)
Chong et al.16 GSW to the head 53 0 (0.0) 0 (0.0) 0 (0.0) 53 (100)
Connell et al.17 GSW to the torso 1,929 12 (0.6) 0 (0.0) 0 (0.0) 1,902 (98.6)
Cornwelletal.18 GSW to the torso 1,000 73 (7.3) 56 (5.6) 2 (0.2) 856 (85.6)
Dubose et al.19 Nonextremity GSW 4,204 150 (3.6) 177 (4.2) 0 (0.0) 3,865 (91.9)
Harrop et al.20 Complete spinalcord injury*
182 182 (100) V V V
Haut et al.21 Any penetratingtrauma**
30,956 86 (0.3) 327 (1.1) 116 (0.4) 30,513 (98.6)
Kaupsand Davis22
GSW to the head 215 1 (0.5) 2 (0.9) 0 (0.0) 199 (92.6)
Kennedyetal.23 GSW to the head 266 4 (1.5) 1 (0.4) 0 (0.0) 261 (98.1)
Klein et al.24 GSW to the head 363 7 (1.9) 5 (1.4) 7 (1.9) 122 (33.6)
GSW to the neck 183 18 (9.8) 16 (8.7) 18 (9.8) 150 (82.0)
GSW to the torso 2,136 126 (5.9) 60 (2.8) 126 (5.9) 2,080 (97.4)
Kupcha et al.25 Penetrating cervicalspinal cord injury*
28 28 (100) 0 (0.0) 0 (0.0) 0 (0.0)
Lanoix et al.26 GSW to the head 151 0 (0.0) 0 (0.0) 0 (0.0) 151 (100)
Lustenbergeret al.27
Penetratingneck injury
1,069 34 (3.2) 61 (5.7) 4 (0.4) 1,004 (93.9)
Medzon et al.28 GSW to thehead or neck
81 15 (18.5) 4 (4.9) 3 (3.7) 62 (76.5)
Ramasamyet al.29
Penetratingneck injury
90 16 (17.8) 3 (3.3) 3 (3.3) 70 (77.8)
Rhee et al.30 Any penetratingtrauma†
20,056 125 (0.6) 54 (0.3) 29 (0.1) V
Vadnerlanet al.31
Penetratingneck injury†
188 V V V V
Vanderlanet al.32
Penetratingneck injury
196 7 (3.6) 13 (6.6) 2 (1.0) 181 (92.3)
Total 107,603 1,647 (1.5) 2,642 (2.5) 192 (0.2) 83,306 (77.4)
*Only identifies patients with spine injury, not used in analysis.**Patient population overlaps other study population in data set, not used in analysis.†Does not identify all spine injuries, not used in analysis.
J Trauma Acute Care SurgVolume 76, Number 2Garcia et al.
536 * 2014 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

$3,304,587 versus $852,332 for a fully recovered trauma pa-tient without neurologic deficits. Lifetime costs per QALY forthe PHSI group are $36,574 T $64 versus $36,552 T $64 inthe nonimmobilization group.
Sensitivity AnalysisSubset analysis of isolated head and isolated neck injuries
demonstrated that 0.7% of isolated head injury and 1.9% ofisolated neck injury patients had unstable spine injury that couldbenefit from initial spine immobilization. The total mean lifetimeper patient cost in isolated head and neck injuries in the PHSIgroup were $953,812 T $1,792 and $1,140,630 T $3,515, re-spectively, versus $954,682 T $1,818 and $1,144,739 T $3,558,respectively, in the nonimmobilization group. For patients withisolated penetrating head or neck injuries, routine PHSI was thedominant strategy over nonimmobilization, but the CIs for theincremental net benefit (INB) indicate equivocal benefit of PHSIeven in these cases (INB head injury: $1,371; CI, j$5,034 to$7,776; INB neck injury: $5,106; CI, j$6,107 to $16,315).
Sensitivity and threshold analyses were then performedon all variables in all three decision trees (all penetratingtrauma, penetrating head trauma, penetrating neck trauma), and
only four variables were found to be sensitive (Figs. 1Y3). Ourfinding that PHSI in penetrating trauma is not advantageous ispredominantly dependent on the incidence of unstable spinalcolumn injury, rate of neurologic recovery after stabilization inpenetrating spine injury, and the cost of routine PHSI (Fig. 1).In patients with penetrating head or neck injury, there are in-creased probabilities of unstable spine injuries; therefore, spinestabilization in these patients may have favorable effects onpatient quality of life and societal burden. Sensitivity analysisin penetrating head and neck injuries found that varying theincidence of unstable spinal column injury and the rate ofneurologic recovery after stabilization in penetrating spineinjury may affect the recommendation regarding omittingPHSI (Figs. 2 and 3). In addition, in penetrating head injury,varying the cost of spine immobilization and the yearly costsof tetraplegia may also affect the recommendation regardingomitting PHSI (Fig. 2).
DISCUSSION
In the current value-based milieu in which medicine ispracticed, CE analyses are becoming increasingly important in
TABLE 2. Incidences, Costs, and Utilities (Includes Living Costs) in US 2010 Dollars
Incidence in No PHSI, % Incidence in PHSI, % First-Year Costs Yearly Costs Opportunity Loss Total Costs Utility4
Parameters
Survive initial trauma35 92.1 92.1
Spinal cord injury* 1.5 1.5 N/A N/A N/A N/A N/A
Unstable spinal injury* 0.2 0.2 N/A N/A N/A N/A N/A
PHSI (direct costs)** 0 100 $876 N/A N/A $876 N/A
Health states
Full recovery10,32 90.7 90.7 $66,316 $29,149 $18,383 $853,208 0.75 (6 mo)
Paraplegia9* 0.91 0.90 $480,431 $63,643 $1,010,290 $3,056,842 0.75
Tetraplegia9* 0.39 0.38 $849,041 $138,098 $1,111,356 $5,056,842 0.39
Death9,10,24,32,36 7.99 7.99 $96,060 $0 $1,298,630 $1,346,563 0
*Incidence calculated from data in Table 1.**Cost of PHSI includes cost of spine imaging33 and cost of cervical collar (estimated from several wholesale options of disposable, adjustable cervical collars).NA, not applicable.
TABLE 3. Expected Costs, Effectiveness, Cost-Utility, and INB
InterventionExpected
Cost (SE), DollarsIncremental Cost(95% CI), Dollars
ExpectedUtility (SE), QALY
Incremental Utility(95% CI), QALY
Cost/Utility(SE), Dollars
INB (95% CI),Dollars*
All penetrating trauma
No PHSI** 929,883 (1,255) V 25.44 (0.01) 0.00 (NA) 36,552 (64) 563.44 (j4,311 to 5,437)
Routine PHSI 930,446 (1,253) 563 (j2,920 to 4,047) 25.44 (0.01) V 36,574 (64) V
Penetratinghead trauma†
No PHSI 954,683 (1,818) 871 (j4,144 to 5,886) 25.32 (0.01) V 37,708 (73) V
Routine PHSI** 953,812 (1,792) V 25.33 (0.01) 0.01 (j0.04 to 0.02) 37,660 (73) 1,371 (j5,034 to 7,776)
Penetratingneck trauma†
No PHSI 1,144,739 (3,558) 4,109 (j5,717 to 13,935) 24.35 (0.01) V 47,014 (165) V
Routine PHSI** 1,140,630 (3,515) V 24.37 (0.01) 0.02 (j0.01 to 0.05) 46,797 (163) 5,109 (j6,107 to 16,325)
*Willingness to pay set at $50,000 per QALY.**dominance.†Sensitivity analysis.NA, not applicable.
J Trauma Acute Care SurgVolume 76, Number 2 Garcia et al.
* 2014 Lippincott Williams & Wilkins 537
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

medical decisionmaking. The question of themost appropriate carein penetrating trauma patients with regard to spinal cord injury isideal for this type of analysis given its low incidence and potentiallydevastating long-term consequences and costs. Initial comparisonsof all patients experiencing penetrating trauma using this Markovmodeled decision analysis suggests that for a cohort of 20-year-oldmales presenting with penetrating injury, routine PHSI is morecostly than no PHSI, without a difference in QALYs; therefore,PHSI is not cost-effective. This is because unstable spine injuriesamenable to surgical or prolonged nonsurgical stabilization aresuch rare occurrences in this patient population3,14Y18,21 that eventhe large, long-term costs of resulting paraplegia, tetraplegia, andpremature death do not justify routine PHSI.
However, with regard to penetrating head and, moreimportantly, neck injuries, there are greater probabilities ofspine injuries than in torso injuries studies.17,20,22,23,29 Thehigher vertebral injury incidence is likely caused by the largercomparative volume of space of the spine compared withthe surrounding tissue creating a proportionally larger at-riskcross-sectional area for spine injury in penetrating trauma.Moreover, cervical spine injuries are more costly than thoracicor lumber spine injuries owing to higher rates of ventilatordependence, higher cost of care for tetraplegic patients, in-creased mortality, and lower rates of subsequent employ-ment and quality of life.4,9 Contrary to our hypothesis, subsetanalyses of patients with isolated penetrating head or neckinjuries showed that routine PHSI was dominant in comparisonwith no PHSI; however, there was no statistically significantincrease in the incremental benefit of PHSI in these patientpopulations.
Upon further analysis, we found that the subset analyses ofisolated head and isolated neck injuries may have been skewed bythe findings of Klein et al.,24 which reviewed 2,450 patients withhead, neck, and torso gunshot wounds (GSWs). This single-centerstudy reported a higher incidence of spinal cord injuries (n = 244,10%), and specifically unstable spine injuries (151 patients,6.2%), than rates reported in other studies.15Y21,23,24,26Y29,32 Theyalso reported many patients requiring prolonged nonsurgicalstabilization for unclear reasons. Although we included thesedata in our analysis in an effort to be unbiased to the availableliterature, if the data from Klein et al. are disregarded, routinePHSI is no longer advantageous in patients with penetratinghead injury; however, it still continues to be the dominant stra-tegy in penetrating neck injury.
There are studies suggesting there is an increased mor-tality associated with spine immobilization in penetrating neckinjuries.20,30 The increasedmortality associated with immobilizedpatients in these studies was attributed to prolonged scene timesand the potential to miss signs of immediate life threat. Unfor-tunately, these immediately life-threatening signs are more com-mon in penetrating neck injuries and include missing expandinghematomas or bleeding, tracheal deviation, and airway compro-mise. Rates of missed life-threatening injuries caused by cervicalspine immobilization are difficult to quantify and are not avail-able in the published literature. Currently, the model shows atrend toward an advantage for PHSI in penetrating neck injury,but the increased rates of complications and mortality with as-sociated PHSI may influence the model such that PSHI is notcost-effective in this subset of patients.
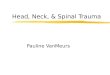
Figure 1. Sensitivity analysis of all penetrating injury. Each linerepresents the expected total cost associated with PHSI(solid line) or no immobilization (dashed line) for the 20-year-oldpatients. The dot indicates the base-case value, and thedotted vertical line indicates the threshold at which the costs ofPHSI and no immobilization are equivalent. In all cases, thedifference in QALYs between PHSI and no immobilization isnegligible, and therefore, for any particular variable, the lowerline represents a lower total cost and therefore the preferredtreatment of choice. A, The base-case value of the probability ofunstable spine injury is 0.2%. Omitting PHSI is preferred forprobabilities below the threshold (0.5%). B, As the probability ofneurologic improvement after stabilization in unstable spineinjury patients increases, the benefit of omitting PHSI afterpenetrating injury decreases with a threshold of 15.6%(base case, 7.4%). C, As the cost of spine immobilizationdecreases, the benefit of omitting spine immobilizationdecreases with a threshold of $407(base case, $876).
J Trauma Acute Care SurgVolume 76, Number 2Garcia et al.
538 * 2014 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

With regard to prolonged scene time from PHSI, incor-porating adverse effects from increasing time to definitivetreatment would only strengthen our conclusion that routinePHSI in all penetrating trauma is not cost-effective and againwould likely not change the outcome of our subset analysis inpenetrating head or penetrating neck injuries. As is the casewith missed injuries, the direct effect and costs of prolongedscene times are difficult to quantify and are not available in thepublished literature.
The average energy involved in stab wounds is 36 J,38
whereas even in a low-velocity (213 m/s), low-caliber (0.22caliber) GSW, the energy involved exceeds 46 J and exceeds450 J in a standard 9-mmGSW.39,40 Given the increased energyof GSWs when compared with stab wounds, it is likely thatGSWs are more likely to cause spinal injury. In fact, in thosestudies that included all penetrating injuries (GSW and stabwounds), the majority indicated that most, if not all, of thespine injuries occurred in patients sustaining a GSW ratherthan stab wounds.14,26,28,31 However, a subset analysis couldnot be performed on spinal injury in patients sustaining stabwounds because this group was not separated in most of the
studies that reported both GSWs and stab wounds. Based onthe studies in our analysis, the incidence of spinal injury inpatients with isolated stab wounds is very low, and it is unlikelythat PHSI in stab wound patients is of any benefit from aclinical and an economic standpoint.
There are limitations to this study. The usefulness of cost-effective analyses are dependent on the available literature re-garding incidence of outcomes from treatments and costs oftreatments and outcomes. Our outcome probabilities are esti-mated from a review of the literature and combined analysis ofthe data contained in 20 studies. These studies are heterogeneousand contribute substantial variability to our data. In addition, asmuch as possible, the types of injuries were categorized, but thiswas difficult to do given the lack of consistent objective defi-nitions of stable and unstable spine injuries in the individualstudies. Moreover, most penetrating trauma patients live in ur-ban areas and have low socioeconomic status that would con-tribute to lower opportunity loss and lower life expectancy thanthat used in the analysis. As is the case with any CE analysis,the costs and other variables assumed in our analysis can beexpected to vary among institutions and regions.
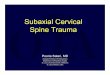
Figure 2. Sensitivity analysis of penetrating head injury. Each line represents the expected total cost associated with PHSI (solid line)or no immobilization (dashed line) for the 20-year-old patients. The dot indicates the base-case value, and the dotted vertical lineindicates the threshold at which the costs of PHSI and no immobilization are equivalent. In all cases, the difference in QALYs betweenPHSI and no immobilization is negligible, and therefore, for any particular variable, the lower line represents a lower total costand therefore the preferred treatment of choice. A, The base-case value of the probability of unstable spine injury is 0.67%. PHSIis preferred for probabilities above the threshold (0.33%). B, As the probability of neurologic improvement after stabilizationdecreases, the benefit of PHSI after penetrating injury decreases with a threshold of 3.7% (base case, 7.4%). C, As the cost ofspine immobilization increases, the benefit of routine spine immobilization decreases with a threshold of $407 (base case, $876).D, Decreasing the yearly cost of tetraplegia (base case, $138,098 per year) decreases the benefit of routine PHSI.
J Trauma Acute Care SurgVolume 76, Number 2 Garcia et al.
* 2014 Lippincott Williams & Wilkins 539
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

CE analyses are becoming increasingly beneficial for theevaluation of treatment strategies given the rising costs of healthcare and increased awareness for outcomes-based practice. Toour knowledge, this is the only decision analysis conductedsurrounding the question of PHSI in penetrating trauma patients.To that end, the present model represents the first attempt toanswer this question from a purely cost-benefit standpoint.
In conclusion, in this CE analysis of PHSI, the recentPHTLS recommendations are substantiated in patients whopresent with penetrating injuries. Despite the increased inci-dence of unstable spine injures produced by penetrating heador neck injuries, subset analyses of the CE of PHSI in thesepatients is still equivocal, and further studies may be neededbefore omitting PHSI in patients with penetrating head andneck injuries.
AUTHORSHIP
A.G. conducted the literature search for this study, which all authorsparticipated in designing. A.G. and T.H.L. contributed to the dataanalysis. A.G. wrote the manuscript. All authors participated in editing.
DISCLOSURE
The authors declare no conflicts of interest.
REFERENCES1. Denis F. The three column spine and its significance in the classification of
acute thoracolumbar spinal injuries. Spine. 1983;8:817Y831.2. Kihtir T, Ivatury RR, Simon R, Stahl WM. Management of transperitoneal
gunshot wounds of the spine. J Trauma. 1991;31:1579Y1583.3. Stuke LE, Pons PT, Guy JS, Chapleau WP, Butler FK, McSwain NE.
Prehospital spine immobilization for penetrating traumaVreview andrecommendations from the PreHospital Trauma Life Support executivecommittee. J Trauma. 2011;71:763Y770.
4. Lin M, Yu W, Wang S. Examination of assumptions in using time tradeoffand standard gamble utilities in individuals with spinal cord injury. ArchPhys Med Rehabil. 2012;93:245Y252.
5. Bickell WH,Wall MJ, Pepe PE, Martin RR, Ginger VF, Allen MK, MattoxKL. Immediate versus delayed fluid resuscitation for hypotensive patientswith penetrating torso injuries. N Engl J Med. 1994;331d:1105Y1109.
6. Shafi S, Gentilello L. Pre-hospital endotracheal intubation and positivepressure ventilation is associated with hypotension and decreased survivalin hypovolemic trauma patients: an analysis of the national trauma databank. J Trauma. 2005;59:1140Y1147.
7. Stiell IG, Nesbitt LP, Pickett W, Munkely D, Spaite DW, Banek J, Field B,Luinstra-Toohey L, Maloney J, Dreyer J, et al., the OPALS Study Group.The OPALS Major Trauma Study: impact of advanced life-support onsurvival and morbidity. CMAJ. 2008;178:1141Y1152.
8. National Association of Emergency Medical Technicians. PrehospitalTrauma Life Support (PHTLS). 7th ed. St. Louis, MO: Mosby Jems/Elsevier; 2011.
9. National Spinal Cord Injury Statistical Center, University of Alabama atBirmingham. 2010 NSCISC Annual Statistical Report. Birmingham 2011.Available at: https://www.nscisc.uab.edu. Accessed March 23, 2012.
10. Expectancy Data. The Dollar Value of a Day, 2010 Edition. ShawneeMission, KS: Expectancy Data; 2010.
11. American College of Surgeons Committee on Trauma. National TraumaData Bank Annual Report 2010. Available at: http://www.facs.org/trauma/ntdb/pdf/ntdbannualreport2010.pdf. Accessed July 20, 2012.
12. Centers for Disease Control and Prevention, National Center for HealthStatistics, Life Expectancy. Available at: http://www.cdc.gov/nchs/faststats/lifexpec.htm. Accessed July 20, 2012.
13. Aryan HE, Amar AP, Ozgur BM, Levy ML. Gunshot wounds to the spinein adolescents. Neurosurgery. 2005;57:748Y752.
14. Barkana Y, Stein M, Scope A, Maor R, Abramovich Y, Friedman Z,Knoller N. Prehospital stabilization of the cervical spine for penetratinginjuries of the neckVis it necessary? Injury. 2000;31:305Y309.
15. Brown JB, Bankey PE, Sangosanya AT, Cheng JD, Stassen NA, GestringML. Prehospital spine immobilization does not appear to be beneficial andmay complicate care following gunshot injury to the torso. J Trauma.2009;67:774Y778.
16. Chong CL, Ware DN, Harris JH. Is cervical spine imaging indicated ingunshot wounds to the cranium. J Trauma. 1998;44:501Y502.
17. Connell RA, Graham CA, Munro PT. Is spinal immobilisation necessary forall patients sustaining isolated penetratin trauma? Injury. 2003;34:912Y914.
18. Cornwell EE, Chang DC, Bonar JP, Campbell KA, Phillips J, Lipsett P,Scalea T, Bass R. Thoracolumbar immobilization for trauma patients withtorso gunshot wounds: is it necessary? Arch Surg. 2001;136:324Y327.
19. Dubose J, Teixeira PGR, Hadjizacharia P, Hannon M, Inaba K, Green DG,et al. The role of routine spinal imaging and immobilisation in asymp-tomatic patients after gunshot wounds. Injury. 2009;40:860Y863.
20. Harrop JS, Sharan AD, Vaccaro AR, Prybylski GJ. The cause of neurologicdeterioration after acute cervical spinal cord injury. Spine. 2001;26:340Y346.
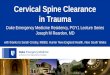
Figure 3. Sensitivity analysis of penetrating neck injury. Eachline represents the expected total cost associated with PHSI(solid line) or no immobilization (dashed line) for the 20-year-oldpatients. The dot indicates the base-case value, and the dottedvertical line indicates the threshold at which the costs of PHSIand no immobilization are equivalent. In all cases, the differencein QALYs between PHSI and no immobilization is negligible, andtherefore, for any particular variable, the lower line representsa lower total cost and therefore the preferred treatment ofchoice. A, The base-case value of the probability of unstablespine injury is 1.89% with a threshold of 0.32%, below whichomitting spine immobilization is preferred. B, As the probabilityof neurologic improvement after stabilization decreases, thebenefit of PHSI after penetrating neck injury decreases with athreshold of 1.2% (base case, 7.4%).
J Trauma Acute Care SurgVolume 76, Number 2Garcia et al.
540 * 2014 Lippincott Williams & Wilkins
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

21. Haut ER, Kalish BT, Efron DT, Haiser AH, Stevens KA, Kieninger AN,Cornwell EE 3rd, Chang DC. Spine immobilization in penetrating trauma:more harm than good? J Trauma. 2010;68:115Y121.
22. Kaups KL, Davis JW. Patients with gunshot wounds to the head do not requirecervical spine immobilization and evaluation. J Trauma. 1998;44:865Y877.
23. Kennedy FR, Gonzalez P, Beitler A, Sterling-Scott R, Fleming AW. In-cidence of cervical spine injury in patients with gunshot wounds to thehead. South Med J. 1994;87:621Y623.
24. Klein Y, Cohn SM, Soffer D, Lynn M, Shaw CM, Hasharoni A. Spineinjuries are common among asymptomatic patients after gunshot wounds.J Trauma. 2005;58:833Y836.
25. Kupcha PC, An HS, Cotler JM. Gunshot wounds to the cervical spine.Spine. 1990;15:1058Y1063.
26. Lanoix R, Gupta R, Leak L, Pierre J. C-spine injury associated withgunshot wounds to the head: retrospective study and literature review.J Trauma. 2000;49:860Y863.
27. Lustenberger T, Talving P, Lam L, Kobayashi L, Inaba K, Plurad D, Branco BC,Demetriades D. Unstable cervical spine fracture after penetrating neck injury:a rare entity in an analysis of 1,069 patients. J Trauma. 2011;70:870Y872.
28. Medzon R, Rothenhaus T, Bono CM, Grindlinger G, Rathlev NK. Stabilityof cervical spine fractures after gunshot wounds to the head and neck.Spine. 2005;30:2274Y2279.
29. Ramasamy A, Midwinter M, Mahoney P, Clasper J. Learning the lessonsfrom conflict: pre-hospital cervical spine stabilization following ballisticneck trauma. Injury. 2009;40:1342Y1345.
30. Rhee P, Kuncir EJ, Johnson L, Brown C, Velmahos G, Martin M, Wang D,Salim A, Doucet J, Kennedy S, Demetriades D. Cervical spine injury ishighly dependent on the mechanism of injury following blunt and pene-trating assault. J Trauma. 2006;61:1166Y1170.
31. Vanderlan WB, Tew BE, McSwain NE. Increased risk of death with cervicalspine immobilisation in penetrating cervical trauma. Injury. 2009;40:880Y883.
32. VanderlanWB, Tew BE, Seguin CY, Mata MM, Yang JJ, Horst HM, ObeidFN, McSwain NE. Neurologic sequelae of penetrating cervical trauma.Spine. 2009;34:2646Y2653.
33. MacKenzie EJ, Weir S, Rivara FP, Jurkovich GJ, Nathens AB, Wang W,Scharfstein DO, Salkever DS. The value of trauma center care. J Trauma.2010;69:1Y10.
34. American Medical Association. CPT code/relative value search. Avail-able at: https://catalog.ama-assn.org/Catalog/cpt/cpt_search.jsp. AccessedJuly 20, 2012.
35. Bureau of Labor Statistics. Consumer Expenditure Survey Tables. Avail-able at: ftp://ftp.bls.gov/pub/special.requests/ce/standard/2010/cusize.txt.Accessed July 20, 2012.
36. Dutton RP, Stansbury LG, Leone S, Kramer E, Hess JR, Scalea TM. Traumamortality in mature trauma systems: are we doing better? An analysis oftrauma mortality patterns, 1997Y2008. J Trauma. 2010;69:620Y626.
37. Bureau of Labor Statisitics. Consumer Expenditure Survey. Available at:http://www.bls.gov/cex/#tables. Accessed July 20, 2012.
38. Chadwick EKJ, Nicol AC, Lane JV, Gray TGF. Biomechanics of knife stabattacks. Forensic Sci Int. 1999;105:35Y44.
39. Robets JC, Ward EE, Merkle AC, O’Connor JV. Asessing behind armorblunt trauma in accordancewith the national institute of justice standard forpersonal body armor protection using finite element modeling. J Trauma.2007;62:1127Y1133.
40. Baik S, Uku JM, Sikirica M. A case of external beveling with an en-trance gunshot wound to the skull made by a small caliber rifle bullet.Am J Forensic Med Pathol. 1993;12:334Y346.
J Trauma Acute Care SurgVolume 76, Number 2 Garcia et al.
* 2014 Lippincott Williams & Wilkins 541
Copyright © 2014 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.