Embed Size (px)
Citation preview
Rethinking prehospital
c-spine immobilization
Terje Sundstrøm MD PhDK. G. Jebsen Brain Tumor Research Center
Department of NeurosurgeryHaukeland University Hospital
Bergen, Norway
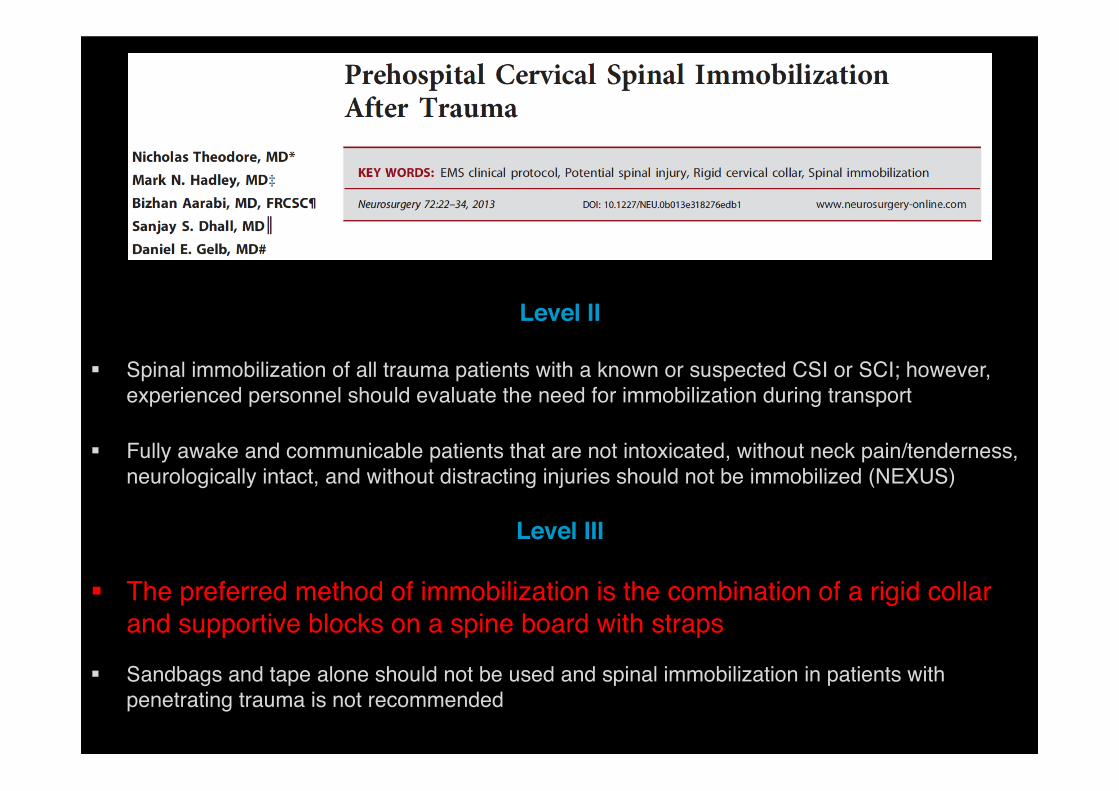
Level II
§ Spinal immobilization of all trauma patients with a known or suspected CSI or SCI; however, experienced personnel should evaluate the need for immobilization during transport
§ Fully awake and communicable patients that are not intoxicated, without neck pain/tenderness, neurologically intact, and without distracting injuries should not be immobilized (NEXUS)
Level III
§ The preferred method of immobilization is the combination of a rigid collar and supportive blocks on a spine board with straps
§ Sandbags and tape alone should not be used and spinal immobilization in patients with penetrating trauma is not recommended
How frequent are cervical injuries?
§ Severe c-spine injury in Norway 2009-2012§ Median age 54§ Incidence 16.5 / 100.000 / year§ Spinal cord injury 13%§ 18% operated
§ 1-4% of major trauma patients§ 1/5 have spinal cord injury§ More common if reduced consciousness
§ Up to 100 patients are immobilized for every patient that has a significant c-spine injury
Ref.: Hasler 2011 & 2012; ATLS 9th ed 2012; Demetriades 2000; Chiu 2001; Deasy 2011; Fredø 2014
Just as important as Airway control?
§ ABCs: Routine application of rigid collars
§ Uncertain effect on mortality, neurological injury, spinal stability, and of adverse effects
§ Growing body of evidence and opinion against this practice
Ref.: Rogers 1957; Bohlman 1979; Gunby 1981; ATLS 9th ed 2012; Kwan 2007; Hauswald 2002; Abram 2010; Deasy 2011; Benger 2009; Abram 2010; Sporer 2012; Sundstrøm 2014
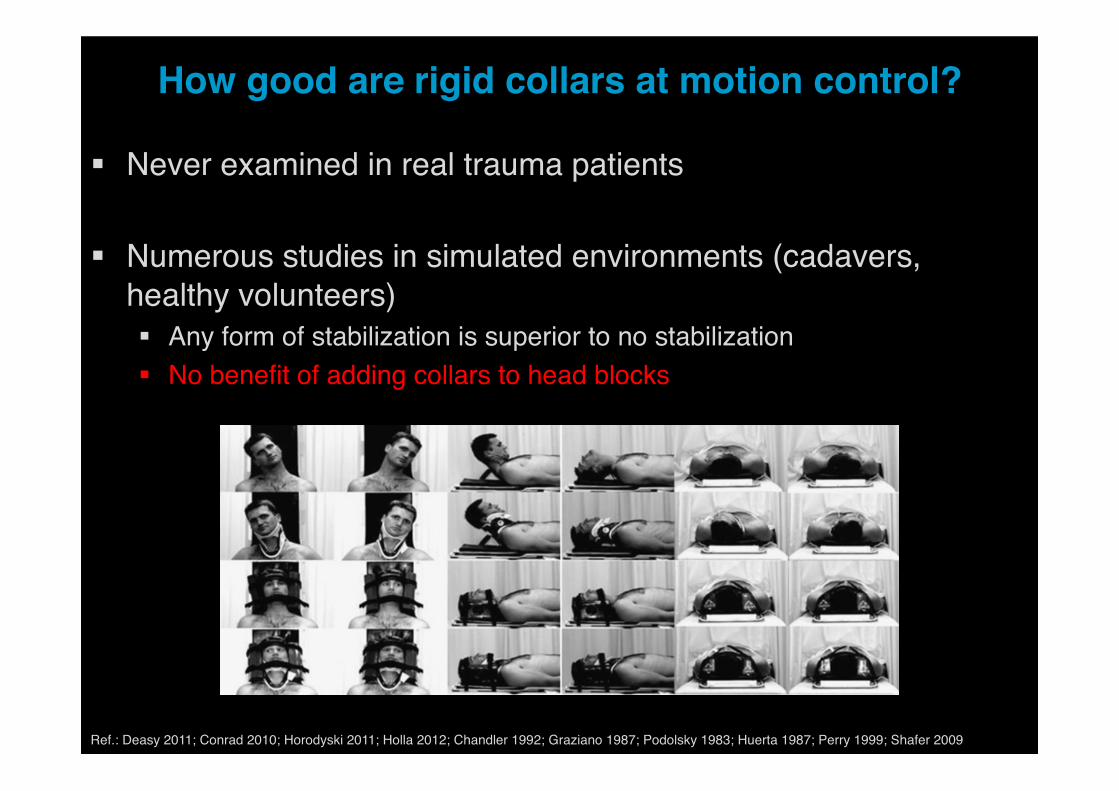
How good are rigid collars at motion control?
§ Never examined in real trauma patients
§ Numerous studies in simulated environments (cadavers, healthy volunteers)§ Any form of stabilization is superior to no stabilization§ No benefit of adding collars to head blocks
Ref.: Deasy 2011; Conrad 2010; Horodyski 2011; Holla 2012; Chandler 1992; Graziano 1987; Podolsky 1983; Huerta 1987; Perry 1999; Shafer 2009
Do collars reduce secondary spinal cord injury?
§ Dubious claim: “3-25% of SCIs are secondary and result from inappropriate management”
§ 5% of patients experience neurological worsening even with proper immobilization
§ New Mexico (collar) vs Malaysia (no collar): More neurological disability with a collar§ Patients maintain a position of comfort with muscle spasm protecting the
spine, and movements during transport are unlikely to generate sufficient energy to result in additional injury
Ref.: Hauswald 2000; Marshall 1987; Huang 2009; Thumbikat 2007; Tator 1991; Hauswald 1998; Sundstrøm 2014
What happens if cervical injuries are overlooked?
§ Five studies: Up to 8% of spinal injuries were missed, but there were no neurological deficits
§ But, delayed diagnosis can result in permanent deficits§ Pooled data: 52 injuries missed, 12 permanent deficits
§ NB! Application & removal of a trauma collar usually spans a couple of hours, whereas the window between trauma and diagnosis for missed injuries can be from days to weeks
Ref.: Armstrong 2007; Brown 1998; Domeier 2005; Domeier 2002; Stroh 2001; Gerrelts 1991; Davis 1993; Platzer 2006
§ Considerable force is required to fracture the cervical spine, and subsequent low-energy movements are unlikely to cause secondary spinal cord injury
§ Most spinal injuries are biomechanically stable in the acute phase, and unstable injuries that have not caused acute, irrevocable injuries are very rare
§ ‘‘It is likely that minor degrees of cervical spine movement are without consequence and more significant movement prevented by common sense”
Ref.: Hauswald 1998; Plumb 2013; Hauswald 2012
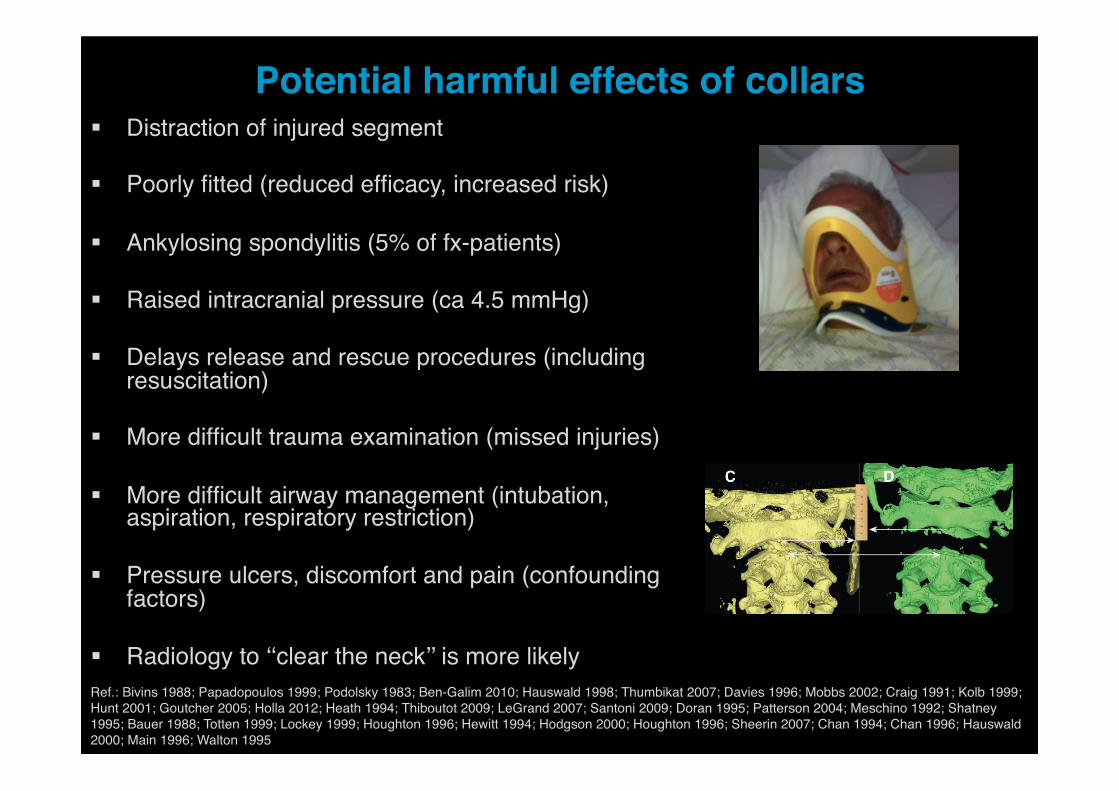
Potential harmful effects of collars§ Distraction of injured segment
§ Poorly fitted (reduced efficacy, increased risk)
§ Ankylosing spondylitis (5% of fx-patients)
§ Raised intracranial pressure (ca 4.5 mmHg)
§ Delays release and rescue procedures (including resuscitation)
§ More difficult trauma examination (missed injuries)
§ More difficult airway management (intubation, aspiration, respiratory restriction)
§ Pressure ulcers, discomfort and pain (confounding factors)
§ Radiology to ‘‘clear the neck’’ is more likelyRef.: Bivins 1988; Papadopoulos 1999; Podolsky 1983; Ben-Galim 2010; Hauswald 1998; Thumbikat 2007; Davies 1996; Mobbs 2002; Craig 1991; Kolb 1999; Hunt 2001; Goutcher 2005; Holla 2012; Heath 1994; Thiboutot 2009; LeGrand 2007; Santoni 2009; Doran 1995; Patterson 2004; Meschino 1992; Shatney 1995; Bauer 1988; Totten 1999; Lockey 1999; Houghton 1996; Hewitt 1994; Hodgson 2000; Houghton 1996; Sheerin 2007; Chan 1994; Chan 1996; Hauswald 2000; Main 1996; Walton 1995
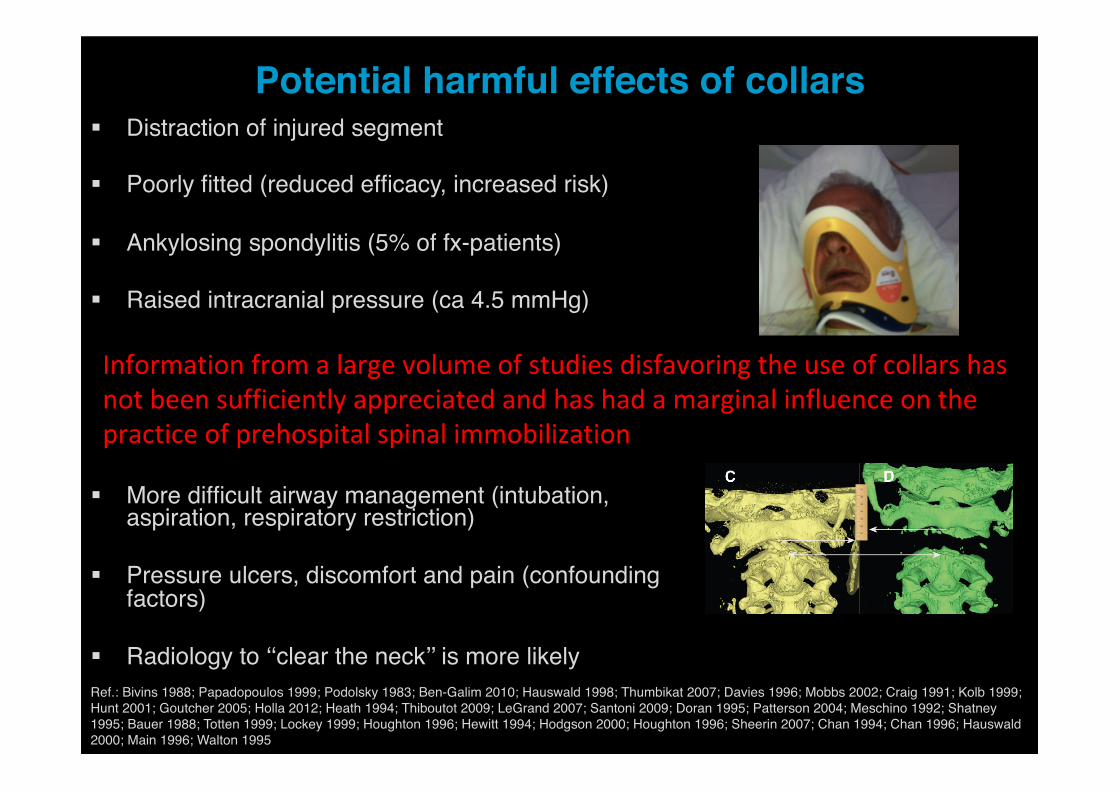
Potential harmful effects of collars§ Distraction of injured segment
§ Poorly fitted (reduced efficacy, increased risk)
§ Ankylosing spondylitis (5% of fx-patients)
§ Raised intracranial pressure (ca 4.5 mmHg)
§ Delays release and rescue procedures (including resuscitation)
§ More difficult trauma examination (missed injuries)
§ More difficult airway management (intubation, aspiration, respiratory restriction)
§ Pressure ulcers, discomfort and pain (confounding factors)
§ Radiology to ‘‘clear the neck’’ is more likelyRef.: Bivins 1988; Papadopoulos 1999; Podolsky 1983; Ben-Galim 2010; Hauswald 1998; Thumbikat 2007; Davies 1996; Mobbs 2002; Craig 1991; Kolb 1999; Hunt 2001; Goutcher 2005; Holla 2012; Heath 1994; Thiboutot 2009; LeGrand 2007; Santoni 2009; Doran 1995; Patterson 2004; Meschino 1992; Shatney 1995; Bauer 1988; Totten 1999; Lockey 1999; Houghton 1996; Hewitt 1994; Hodgson 2000; Houghton 1996; Sheerin 2007; Chan 1994; Chan 1996; Hauswald 2000; Main 1996; Walton 1995
Informationfromalargevolumeofstudiesdisfavoringtheuseofcollarshasnotbeensufficientlyappreciatedandhashadamarginalinfluenceonthepracticeofprehospitalspinalimmobilization
Moving our practice forward
§ Low quality evidence for and against collars
§ Few patients need spinal immobilization, and clearance protocols should be optimized to identify these high-risk patients (NEXUS, CCSR, others)
§ Systematic literature review + Expert consensus
§ Prospective clinical trial unlikely§ ATLS: “... unlikely to occur in North America, but could perhaps be done
elsewhere”
Ref.: Armstrong 2007; Brown 1998; Domeier 2005; Domeier 2002; Stroh 2001; Gerrelts 1991; Davis 1993; Platzer 2006
Recent developments
Application of a cervical collar is not recommended
Manual in-line stabilization is a suitable alternative to a cervical collar
Adequate stabilization can be achieved with manual in-line stabilization or head blocks (full guideline!)
Selective spinal motion restriction protocols are needed...
Ref.: Connor 2013; ACEP 2015; Zideman 2015; Kornhall 2017
Summary
§ Spinal immobilization à Spinal motion restriction
§ Uniform protocols à Triage-based guidelines
§ Rigid collar à Head blocks / Manual in-line stabilization
§ Hard surface stretchers à Soft surface stretchers







![SPINE TRAUMA [Read-Only] - jefferson.edu€¢ Rigid transfer slides Log roll (incorrect) Log roll (correct) Spinal clearance – KEY POINTS 1. Spinal immobilization is a priority in](https://img.pdfslide.net/doc/110x75/5acf9e7a7f8b9a6c6c8d5643/spine-trauma-read-only-rigid-transfer-slides-log-roll-incorrect-log-roll.jpg)