Embed Size (px)
Citation preview

46 MeAd Genet 1994;31:486-489
Costello syndrome: natural history anddifferential diagnosis of cutis laxa
S J Davies, H E Hughes
AbstractCostello syndrome is emerging as a
better delineated condition and should beincluded in the differential diagnosis ofcutis laxa in association with postnatalgrowth retardation and developmentaldelay. We present a further case ofCostello syndrome which illustrates thenatural history of this condition.
(J7 Med Geniet 1994;31:486-489)
Costello first described in 1971, and later in1977, two young children with similar featuresof poor postnatal growth, developmentaldelay, distinctive facies, and papillomata of theanterior nares. 2 There were no further reportsto allow more detailed delineation of the con-
dition until Der Kaloustian et al3 and Martinand Lyons Jones4 described two additionalcases in 1991. Increasing awareness of thissyndrome has led to a number of case reports5-8and has opened debate on whether or not thenew syndrome of multiple congenital anomalywith mental retardation and facio-cutaneous-skeletal involvement described by Boro-chowitz et al9 in 1992 is in fact Costellosyndrome.7 1012
We would like to present a further patientwith Costello syndrome who has been reportedpreviously as case 7 in a series of seven
children with "Congenital cutis laxa withretardation of growth and development" byPatton et al' in 1987. Interestingly, case 5 ofthe same series has independently been re-
assessed and has also been diagnosed as havingCostello syndrome.'4
Institute of MedicalGenetics, Universityof Wales Hospital,Heath Park, CardiffCF4 4XW, UKS J DaviesH E Hughes
Correspondence toDr Davies.
Received 7 December 1993Accepted for publication13 January 1994
Case reportsA female infant was born at 39 weeks byspontaneous vaginal delivery with Apgarscores of 9 at one minute and 10 at fiveminutes. Both parents were healthy and non-
consanguineous with two healthy older sons.
The mother was 24 and the father 32 years ofage at the time of conception. Pregnancy was
complicated by mild hypertension in the thirdtrimester and the mother was aware that fetalmovements were less than in her previouspregnancies. Birth weight was 3950 kg (90thcentile), length 47 cms ( < 10th centile), andhead circumference 35 cm (> 50th centile).Dysmorphic features as well as macroglossiaand lax skin were noted at birth and chromo-some studies showed a normal female karyo-type (46,XX). Hyperbilirubinaemia was pre-
sent with a maximum level of 280 mmol/l on
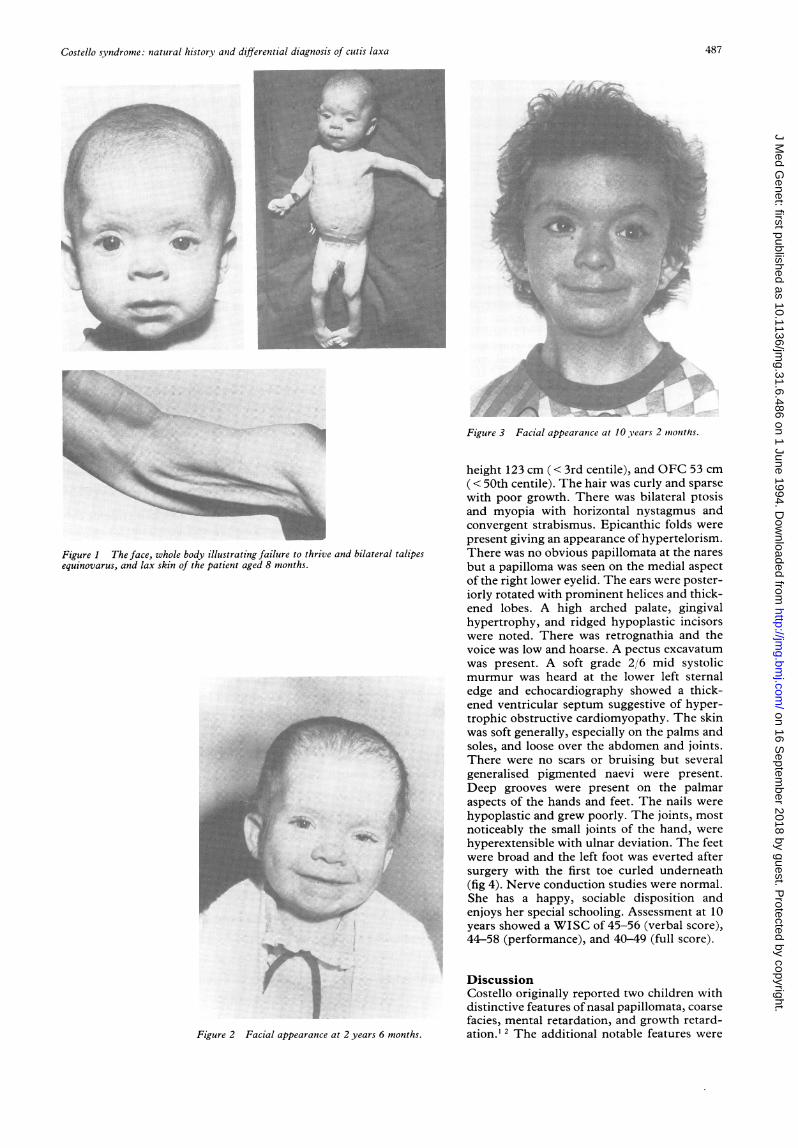
the fifth day. At 6 weeks of age the infant wasinvestigated for failure to thrive. At that time,the head circumference was 37 cm (> 50thcentile), weight 3 48 kg (10th centile), andlength 51 cm (< 10th centile). She was noted tohave a depressed nasal bridge, prominent lowset ears, a large tongue, and bilateral singlepalmar creases. Poor subcutaneous fat withloose folds of skin were apparent and there wasbilateral talipes equinovarus. No obviouscause for her failure to thrive was found otherthan very poor feeding requiring hourly spoonfeeds.At 8 months she was again investigated in
the light of gross failure to thrive, dysmorphicfeatures, and developmental delay (fig 1). Shecould not roll over or lift her head. Weight was45 kg (<3rd centile), height 63 cm (<3rdcentile), while the head circumference was41.5 cm (10th centile). A provisional diagnosisof leprechaunism was made though subse-quently refuted on investigation. Hyperexten-sibility of joints with loose skin were noted (fig1). A diagnosis of the syndrome of cutis laxawith ligmentous laxity and delayed develop-ment was made though it was noted that shehad not had intrauterine growth retardation orcongenital hip dislocation as in the previouslydescribed cases.'5 A skin biopsy showed nor-mal elastic tissue network with Halmi's stainand electron microscopy.The bilateral talipes was treated initially
with passive stretching and plaster of Paris. Agood result was obtained in the right foot butthere was considerable calcaneovarus andmetatarsus varus on the left. When at the ageof 2 years 6 months she was admitted forcorrective surgery, the tight Achilles tendonwas seen to be the major deforming force andelongation of the Achilles tendon and the tibia-lis posterior tendon was performed with split-ing and transfer of the tibialis anterior tendon.Her weight at this time was 7 4 kg (< 3rdcentile), height 75 cm ( < 3rd centile), withrelative macrocephaly, OFC 48 cm (< 50thcentile). Developmental delay was confirmed.Sparse curly hair, ptosis, left facial asymmetry,and delayed hypocalcified carious dentitionwere also noted'3 (fig 2).
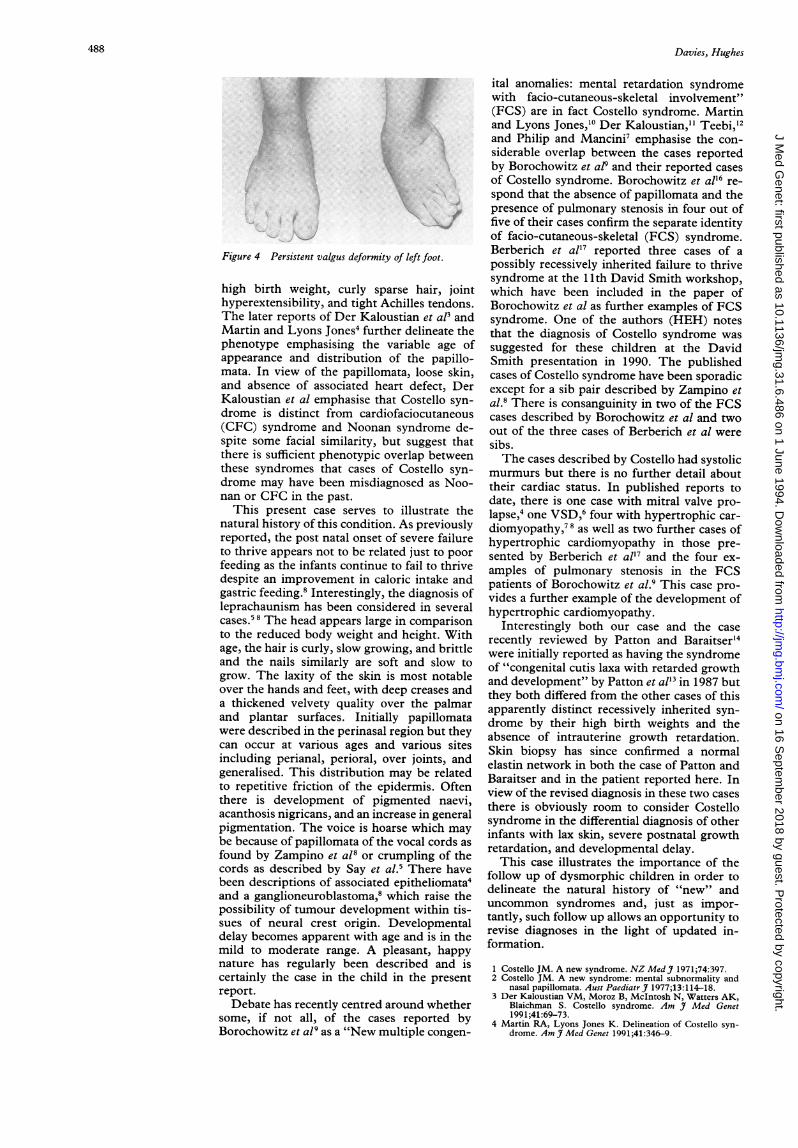
Subsequent development has been slowwith day time continence at 5 years, night timecontinence at 8 years, and walking indepen-dently at 7 years. She attends a special school.The left foot developed a severe valgus defor-mity following surgery and at 8 years of age thetibialis anterior tendon was transferred to itsoriginal attachment.
Referral was made for genetic counselling atthe age of 10 years 2 months (fig 3). Onexamination weight was 18 kg (<3rd centile),
486
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.6.486 on 1 June 1994. D
ownloaded from
Costello syndrome: natural history, and differential diagnosis of cutis laxa
A'
g.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~,,4-''~t
_ _ ~ ~~ ~ ~ ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~-------I-I--
Figure ThfcewolbdIllstaIngfIlueohivadiaerlaie
sequnvrs n a kno teptetae ots
Figure 2 Facial appearance at 2 years 6 months.
Figure 3 Facial appearance at 10 years 2 mtionths.
height 123 cm (< 3rd centile), and OFC 53 cm(< 50th centile). The hair was curly and sparsewith poor growth. There was bilateral ptosisand myopia with horizontal nystagmus andconvergent strabismus. Epicanthic folds werepresent giving an appearance of hypertelorism.There was no obvious papillomata at the naresbut a papilloma was seen on the medial aspectof the right lower eyelid. The ears were poster-iorly rotated with prominent helices and thick-ened lobes. A high arched palate, gingivalhypertrophy, and ridged hypoplastic incisorswere noted. There was retrognathia and thevoice was low and hoarse. A pectus excavatumwas present. A soft grade 2/6 mid systolicmurmur was heard at the lower left sternaledge and echocardiography showed a thick-ened ventricular septum suggestive of hyper-trophic obstructive cardiomyopathy. The skinwas soft generally, especially on the palms andsoles, and loose over the abdomen and joints.There were no scars or bruising but severalgeneralised pigmented naevi were present.Deep grooves were present on the palmaraspects of the hands and feet. The nails werehypoplastic and grew poorly. The joints, mostnoticeably the small joints of the hand, werehyperextensible with ulnar deviation. The feetwere broad and the left foot was everted aftersurgery with the first toe curled underneath(fig 4). Nerve conduction studies were normal.She has a happy, sociable disposition andenjoys her special schooling. Assessment at 10years showed a WISC of 45-56 (verbal score),44-58 (performance), and 40-49 (full score).
DiscussionCostello originally reported two children withdistinctive features of nasal papillomata, coarsefacies, mental retardation, and growth retard-ation.' I The additional notable features were
487
.i0?:,
I'llilm.4
li..1-....'10*.-- AM.-F
oop.:,*;,
M.L.
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.6.486 on 1 June 1994. D
ownloaded from
Davies, Hughes
f.%f..:.1'
Figure 4 Persistent valgus deformity of left foot.
high birth weight, curly sparse hair, jointhyperextensibility, and tight Achilles tendons.The later reports of Der Kaloustian et aP andMartin and Lyons Jones4 further delineate thephenotype emphasising the variable age ofappearance and distribution of the papillo-mata. In view of the papillomata, loose skin,and absence of associated heart defect, DerKaloustian et al emphasise that Costello syn-drome is distinct from cardiofaciocutaneous(CFC) syndrome and Noonan syndrome de-spite some facial similarity, but suggest thatthere is sufficient phenotypic overlap betweenthese syndromes that cases of Costello syn-drome may have been misdiagnosed as Noo-nan or CFC in the past.
This present case serves to illustrate thenatural history of this condition. As previouslyreported, the post natal onset of severe failureto thrive appears not to be related just to poorfeeding as the infants continue to fail to thrivedespite an improvement in caloric intake andgastric feeding.8 Interestingly, the diagnosis ofleprachaunism has been considered in severalcases.5 8 The head appears large in comparisonto the reduced body weight and height. Withage, the hair is curly, slow growing, and brittleand the nails similarly are soft and slow togrow. The laxity of the skin is most notableover the hands and feet, with deep creases anda thickened velvety quality over the palmarand plantar surfaces. Initially papillomatawere described in the perinasal region but theycan occur at various ages and various sitesincluding perianal, perioral, over joints, andgeneralised. This distribution may be relatedto repetitive friction of the epidermis. Oftenthere is development of pigmented naevi,acanthosis nigricans, and an increase in generalpigmentation. The voice is hoarse which maybe because of papillomata of the vocal cords asfound by Zampino et al8 or crumpling of thecords as described by Say et al.S There havebeen descriptions of associated epitheliomata4and a ganglioneuroblastoma,8 which raise thepossibility of tumour development within tis-sues of neural crest origin. Developmentaldelay becomes apparent with age and is in themild to moderate range. A pleasant, happynature has regularly been described and iscertainly the case in the child in the presentreport.Debate has recently centred around whether
some, if not all, of the cases reported byBorochowitz et al9 as a "New multiple congen-
ital anomalies: mental retardation syndromewith facio-cutaneous-skeletal involvement"(FCS) are in fact Costello syndrome. Martinand Lyons Jones,'0 Der Kaloustian," Teebi,"2and Philip and Mancini7 emphasise the con-siderable overlap between the cases reportedby Borochowitz et alP and their reported casesof Costello syndrome. Borochowitz et al'6 re-spond that the absence of papillomata and thepresence of pulmonary stenosis in four out offive of their cases confirm the separate identityof facio-cutaneous-skeletal (FCS) syndrome.Berberich et al'7 reported three cases of apossibly recessively inherited failure to thrivesyndrome at the 11th David Smith workshop,which have been included in the paper ofBorochowitz et al as further examples of FCSsyndrome. One of the authors (HEH) notesthat the diagnosis of Costello syndrome wassuggested for these children at the DavidSmith presentation in 1990. The publishedcases of Costello syndrome have been sporadicexcept for a sib pair described by Zampino etal.8 There is consanguinity in two of the FCScases described by Borochowitz et al and twoout of the three cases of Berberich et al weresibs.The cases described by Costello had systolic
murmurs but there is no further detail abouttheir cardiac status. In published reports todate, there is one case with mitral valve pro-lapse,4 one VSD,6 four with hypertrophic car-diomyopathy,78 as well as two further cases ofhypertrophic cardiomyopathy in those pre-sented by Berberich et al'7 and the four ex-amples of pulmonary stenosis in the FCSpatients of Borochowitz et al.9 This case pro-vides a further example of the development ofhypertrophic cardiomyopathy.
Interestingly both our case and the caserecently reviewed by Patton and Baraitser'4were initially reported as having the syndromeof "congenital cutis laxa with retarded growthand development" by Patton et all' in 1987 butthey both differed from the other cases of thisapparently distinct recessively inherited syn-drome by their high birth weights and theabsence of intrauterine growth retardation.Skin biopsy has since confirmed a normalelastin network in both the case of Patton andBaraitser and in the patient reported here. Inview of the revised diagnosis in these two casesthere is obviously room to consider Costellosyndrome in the differential diagnosis of otherinfants with lax skin, severe postnatal growthretardation, and developmental delay.This case illustrates the importance of the
follow up of dysmorphic children in order todelineate the natural history of "new" anduncommon syndromes and, just as impor-tantly, such follow up allows an opportunity torevise diagnoses in the light of updated in-formation.
1 Costello JM. A new syndrome. NZ MedJ 1971;74:397.2 Costello JM. A new syndrome: mental subnormality and
nasal papillomata. Aust PaediatrJ 1977;13:114-18.3 Der Kaloustian VM, Moroz B, McIntosh N, Watters AK,
Blaichman S. Costello syndrome. Am J Med Genet1991;41:69-73.
4 Martin RA, Lyons Jones K. Delineation of Costello syn-drome. Am J Med Genet 1991;41:346-9.
488
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.6.486 on 1 June 1994. D
ownloaded from

Costello syndrome: natural history and differential diagnosis of cutis laxa
5 Say B, Gucsavas M, Morgan H, York C. The Costellosyndrome. Am Med Genet 1993;47:163-5.
6 Teebi AS, Shabaani IS. Further delineation of Costellosyndrome. Am Med Genet 1993;47:166-8.
7 Philip N, Mancini J. Costello syndrome and facio-cuta-neous-skeletal syndrome. Am 7 Med Genet 1993;47:174-5.
8 Zampino G, Mastroiacovo P, Ricci R, et al. Costello syn-drome: further clinical delineation, natural history,genetic definition, and nosology. Am Med Genet1993;47: 176-83.
9 Borochowitz Z, Pavone L, Mazor G, Rizzo R, Dar H. Newmultiple congenital anomalies: mental retardation syn-drome (MCA/MR) with facio-cutaneous-skeletal involve-ment. Am Med Genet 1992;43:678-85.
10 Martin RA, Lyons Jones K. Facio-cutaneous-skeletal syn-drome is the Costello syndrome. Am Med Genet1993;47:169.
11 Der Kaloustian VM. Not a new MCA/MR syndrome butprobably Costello syndrome? Am Med Genet 1993;47:170-1.
12 Teebi AS. Costello or facio-cutaneous-skeletal syndrome?Am J Med Genet 1993;47:172.
13 Patton MA, Tolmie J, Ruthnum P, Bamforth S, BaraitserM, Pembrey M. Congenital cutis laxa with retardedgrowth and development. J Med Genet 1987;24:556-61.
14 Patton MA, Baraitser M. Cutis laxa and the Costellosyndrome. J Med Genet 1993;30:622.
15 Sakati NO, Nyhan WL, Shear CS, et al. Syndrome of cutislaxa, ligamentous laxity, and delayed development. Pedia-trics 1983;72:850-6.
16 Borochowitz Z, Pavone L, Mazor G, Rizzo R, Dar H.Facio-cutaneous-skeletal syndrome. Am J Med Genet1993;47:173.
17 Berberich MS, Carey JC, Hall BD. Resolution of theperinatal and infantile failure to thrive in a new autosomalrecessive syndrome with the phenotype of a storage dis-order and furrowing of the palmar creases. 11th DWSmith workshop on malformation and morphogenesis,Lexington, Kentucky, 1990. Proc Greenwood GeneticCenter 1991;10:98.
489
on 16 Septem
ber 2018 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.31.6.486 on 1 June 1994. D
ownloaded from





























