Embed Size (px)
Citation preview

University of Groningen
Counterregulation to acute and recurrent hypoglycemia in ratsBouman, Stephan Daniël
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2009
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Bouman, S. D. (2009). Counterregulation to acute and recurrent hypoglycemia in rats s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 17-03-2018

RIJKSUNIVERSITEIT GRONINGEN
Counterregulation to acute and recurrent hypoglycemia in rats
Proefschrift
ter verkrijging van het doctoraat in de Wiskunde en Natuurwetenschappen aan de Rijksuniversiteit Groningen
op gezag van de Rector Magnificus, dr. F. Zwarts, in het openbaar te verdedigen op
vrijdag 20 februari 2009 om 16:15 uur
door
Stephan Daniël Bouman
geboren op 5 september 1973 te Nieuw‐Lekkerland

Promotor:
prof. dr. A.J.W. Scheurink Beoordelingscommissie: prof. dr. P.G.M. Luiten
prof. dr. G.J. ter Horst prof. dr. R.J. Vonk ISBN: 978‐90‐367‐3720‐3 (printed version) 978‐90‐367‐3721‐0 (electronic version)

Counterregulation to acute and recurrent hypoglycemia in rats
Tegenregulatie op enkelstaande en herhaalde hypoglycemie in ratten
Stephan D. Bouman
The experiments, the presenting of the results at scientific conferences, and the printing of the thesis have been generously supported by:
Dutch Diabetes Research Foundation
European Association for the Study of Diabetes
Center for Behavioral and Cognitive Neurosciences
Insulin Pharmacology, Novo Nordisk A/S
University of Groningen
The studies have been performed at the Department of Animal Physiology, University of Groningen, The Netherlands, and at the Department of Animal Sciences, University of
Illinois at Urbana‐Champaign, USA.
Printed by Reprocenter, University of Copenhagen, Denmark.
i

ii

From the moment I picked it up until I laid it down, I was convulsed with laughter. Some day I intend reading it.
‐ Groucho Marx
iii

Table of contents
Nederlandse samenvatting.............................................................................................................. vii
English summary ................................................................................................................................ix
Abbreviations and definitions...........................................................................................................xi
Chapter 1 General introduction .........................................................................................................3 Glucose homeostasis .................................................................................................................................... 3 Diabetes and hypoglycemia........................................................................................................................ 4 Counterregulation to hypoglycemia.......................................................................................................... 5 Recurrent hypoglycemia and hypoglycemia unawareness.................................................................... 6 Counterregulation to acute and recurrent hypoglycemia in rats........................................................... 6 References...................................................................................................................................................... 7
Section I – Counterregulation, insulin, and the nutritional state ................................................13
Chapter 2 Insulin levels and fasting independently co‐determine the counterregulatory responses to hypoglycemia...............................................................................................................17
Introduction................................................................................................................................................. 17 Methods ....................................................................................................................................................... 18
Animals and surgery ............................................................................................................................................18 Experimental design .............................................................................................................................................18 Analysis ..................................................................................................................................................................19
Results .......................................................................................................................................................... 19 Experiment 1 – Insulin‐induced hypoglycemia in fed rats..............................................................................19 Experiment 2 – Insulin‐induced hypoglycemia in fasted rats.........................................................................23
Discussion.................................................................................................................................................... 24 Glucose and insulin are independent moderators of the counterregulatory responses..............................25 Fasting enhances all counterregulatory responses ...........................................................................................28 Summary ................................................................................................................................................................29
References.................................................................................................................................................... 31
Chapter 3 Inhibition of fatty acid oxidation strongly potentiates the counterregulatory responses to insulin‐induced hypoglycemia..................................................................................37
Introduction................................................................................................................................................. 37 Methods ....................................................................................................................................................... 38
Animals and surgery ............................................................................................................................................38 Experimental design .............................................................................................................................................38 Determinations and analysis ...............................................................................................................................39
Results .......................................................................................................................................................... 39 Discussion.................................................................................................................................................... 41 References.................................................................................................................................................... 43
Section II – Central nervous mechanisms.......................................................................................47
Chapter 4 Noradrenergic and GABAergic systems in the medial hypothalamus are activated during hypoglycemia ........................................................................................................................51
The ventral hypothalamus ........................................................................................................................ 51 Research design and methods .................................................................................................................. 52
Surgical procedures ..............................................................................................................................................52 Sample collection ..................................................................................................................................................53 Effect of insulin‐induced hypoglycemia on NE and GABA............................................................................53 Sample analysis .....................................................................................................................................................54
iv

Data analysis..........................................................................................................................................................54 Supplies ..................................................................................................................................................................55
Results .......................................................................................................................................................... 55 Discussion.................................................................................................................................................... 58
Perspectives ...........................................................................................................................................................61 References.................................................................................................................................................... 61
Chapter 5 Blockade of paraventricular hypothalamic alpha‐adrenoceptors impairs the counterregulation to hypoglycemia ................................................................................................67
Introduction................................................................................................................................................. 67 Methods ....................................................................................................................................................... 68
Animals and surgery ............................................................................................................................................68 Experimental design .............................................................................................................................................68 Analysis ..................................................................................................................................................................69
Results .......................................................................................................................................................... 70 Discussion.................................................................................................................................................... 72 References.................................................................................................................................................... 73
Section III – Recurrent hypoglycemia .............................................................................................77
Chapter 6 Hypoglycemia‐Associated Autonomic Failure in rats ...............................................81 Introduction................................................................................................................................................. 81 Methods ....................................................................................................................................................... 82
Animals and surgery ............................................................................................................................................82 General protocol....................................................................................................................................................82 Specific protocols ..................................................................................................................................................83
Results .......................................................................................................................................................... 84 Experiment 1 – One antecedent hypoglycemic episode...................................................................................84 Experiment 2 – A higher insulin dose ................................................................................................................86 Experiment 3 – Three times a hypo ....................................................................................................................86 Experiment 4 – Food intake and nutrient preference .......................................................................................87 Experiment 5 – GAAF...........................................................................................................................................89
Discussion.................................................................................................................................................... 90 References.................................................................................................................................................... 92
Chapter 7 General discussion...........................................................................................................99 Section I – Counterregulation, insulin, and the nutritional state......................................................... 99
Insulin.....................................................................................................................................................................99 The nutritional state............................................................................................................................................101
Section II – Central nervous mechanisms ............................................................................................. 102 Activation of noradrenergic pathways.............................................................................................................102 Blockade of noradrenergic pathways ...............................................................................................................103
Section III – Recurrent hypoglycemia.................................................................................................... 104 Rat model for HAAF...........................................................................................................................................104 HAAF is GAAF?..................................................................................................................................................105
Conclusions and perspective .................................................................................................................. 105 References.................................................................................................................................................. 106
Authorʹs papers and published abstracts .....................................................................................112
Dankwoord .......................................................................................................................................114
v

vi

Nederlandse samenvatting Het glucosegehalte van het bloed is erg belangrijk, aangezien glucose voor het grootste deel van de energievoorziening van de hersenen staat. Het is daarom van wezenlijk belang dat er nooit te weinig glucose in het bloed is, zodat de hersenen normaal kunnen functioneren. Daarentegen zijn te hoge glucosespiegels evenmin gezond, aangezien dat tot weefselschade kan leiden. Het lichaam heeft daarom verschillende mechanismen om het glucosegehalte van het bloed te reguleren. Glucose komt via de spijsvertering het lichaam in en wordt via het bloed naar alle weefsels getransporteerd. De meeste organen gebruiken glucose als brandstof, maar de lever kan bovendien glucose opslaan. Veel van de weefsels nemen glucose voornamelijk vanuit het bloed op onder invloed van het hormoon insuline. De stijging in het glucosegehalte na het eten gaat dan ook altijd gepaard met een verhoogde afgifte van insuline door de pancreas. Bovendien verhindert deze insuline de lever in het vrijgeven van opgeslagen glucose. Insuline is vrijwel het enige hormoon dat het glucosegehalte van het bloed kan verlagen en is daarmee dus het belangrijkste mechanisme om een te hoog glucosegehalte tegen te werken. In periodes waar er geen nieuwe glucose het bloed in komt of waar het glucoseverbruik toeneemt, begint het glucosegehalte omlaag te gaan. Het insulinegehalte gaat eveneens omlaag, zodat veel weefsels nu geen glucose meer opnemen maar andere energiesubstraten gebruiken. Bovendien is het nu mogelijk voor de lever om opgeslagen glucose vrij te geven. Op deze manier wordt de energievoorziening van de hersenen gewaarborgd. Als het glucosegehalte van het bloed desondanks te laag wordt (hypoglycemie), zijn er verschillende mechanismen die dit tegengaan. Ten eerste wordt er glucagon afgegeven, wat de lever stimuleert meer glucose vrij te geven. Daarnaast wordt er adrenaline geproduceerd, wat ook het glucosegehalte in het bloed kan verhogen. Verder kunnen ook cortisol en groeihormoon helpen een te laag glucosegehalte tegen te gaan. Samen geven deze mechanismen gezonde mensen een effectieve tegenregulatie tegen lage glucosespiegels. Voor patiënten met diabetes is dit echter niet het geval. Diabetes wordt gekenmerkt door te hoge glucosespiegels en dient daarom te worden behandeld met glucoseverlagende medicijnen, bijvoorbeeld insuline. Dit leidt regelmatig tot hypoglycemie en diabetespatiënten zijn daarom erg afhankelijk van een goede tegenregulatie. Diabetes gaat echter vaak al gepaard met defecten in de glucagonrespons. Daarnaast is gebleken dat herhaalde hypoglycemie leidt tot steeds lagere tegenregulerende responsen – een fenomeen wat Hypoglycemia‐Associated Autonomic Failure wordt genoemd. De reden waarom dit ontstaat is niet bekend, maar het leidt onder andere tot een verlaging van de juist zo belangrijke adrenalinerespons en zorgt er tevens voor dat de patiënt minder goed waarneemt dat het glucosegehalte te laag is. Dit leidt daardoor weer tot meer hypoglycemische episodes – een vicieuze cirkel die het noodzakelijk maakt de insulinedosis te verminderen en daarmee een optimale diabetesbehandeling onmogelijk maakt. Het onderzoek in dit proefschrift had daarom tot doel de mechanismen achter de tegenregulerende responsen op hypoglycemie nader te onderzoeken. Daarnaast werd er onderzocht hoe en waarom deze responsen verminderen bij herhaalde hypoglycemie. Alle experimenten werden uitgevoerd in ratten.
vii

In de eerste experimenten werd er onderzocht hoe de tegenregulerende
mechanismen onderling samenhangen, wat de rol van insuline is en hoe de beschikbaarheid van andere energiebronnen de tegenregulatie beïnvloedt. Het bleek dat de tegenregulatie van glucoseverlaging erg precies is, waarbij de verschillende tegenregulerende responsen ervoor zorgen dat het glucosegehalte altijd boven een bepaald niveau blijft, ongeacht de hoeveelheid toegediende insuline. Een mogelijke verklaring hiervoor is dat een hoger insulinegehalte van het bloed zorgt voor extra stimulatie van de tegenregulerende responsen. Verder bleek het dat een vermindering van andere energiebronnen (zoals na 48 uur vasten, of na toediening van een vetverbrandingsremmer) de tegenregulerende responsen op hypoglycemie veel groter worden – wat er op kan duiden dat het lichaam de grotere afhankelijkheid van glucose erkent.
De volgende experimenten onderzochten de rol van de noradrenerge neuronale signaaloverdracht in de hypothalamus – een hersendeel wat veel van de energiehuishouding stuurt. In experimenten aan de University of Illinois werd onder invloed van hypoglycemie verhoogde afgifte van de neurotransmitter noradrenaline geconstateerd. Deze respons verdween slechts gedeeltelijk onder toediening van glucose, wat er ook op kan duiden dat de toegediende insuline zelf een rol speelt. Daarna vonden we dat deze noradrenalinerespons inderdaad belangrijk is voor het sturen van de tegenregulerende responsen, aangezien een blokkering van de noradrenalinetransmissie leidde tot verminderde responsen op hypoglycemie.
Als laatste werd een aantal experimenten met herhaalde hypoglycemie uitgevoerd. Ten eerste bleek het dat ook in ratten een vermindering van de tegenregulerende responsen optreedt, wat dit dier geschikt maakt voor verder onderzoek naar het ontstaan van Hypoglycemia‐Associated Autonomic Failure. In de daaropvolgende experimenten werd er onder andere aangetoond dat de hypoglycemie‐frequentie en de gebruikte insulinedosis waarschijnlijk van belang zijn. Bovendien leidde herhaald blootstellen aan een remmer van de glucoseverbranding eveneens tot verminderde responsen op hypoglycemie, wat aantoont dat dit een algemene aanpassingsrespons is en niet alleen specifiek voor insuline‐geïnduceerde hypoglycemie.
Samenvattend heeft dit onderzoek geresulteerd in nieuwe inzichten in de
samenhang tussen de tegenregulerende responsen, de neuronale netwerken die hierbij betrokken zijn, en de ontwikkeling van Hypoglycemia‐Associated Autonomic Failure.
viii

English summary The blood glucose levels are of great importance, as glucose is responsible for the major part of the brainʹs energy supply. It is therefore essential to avoid glucose shortage in the blood, to ensure normal brain function. High glucose levels are also undesirable, as those can lead to tissue damage. Therefore the body has multiple mechanisms to regulate blood glucose levels. Glucose enters the body by means of digestion and is transported to all tissues by the blood circulation. Most organs use glucose as fuel, but the liver is in addition capable of storing glucose. Many tissues predominantly take up glucose when stimulated by the hormone insulin. The increase in glucose levels after a meal is therefore always accompanied by increased insulin secretion by the pancreas. This insulin also ensures the liver does not release stored glucose. Insulin is practically the only hormone that is able to lower blood glucose levels, and is thereby the most important mechanism in counteracting too high blood glucose levels. In periods where no new glucose enters the blood, or glucose usage increases, glucose levels will start to decrease. Insulin levels also decrease, so many tissues will stop taking up glucose and use other energy substrates instead. It is now also possible for the liver to release stored glucose. This guarantees the brainʹs energy supply. Should blood glucose levels nevertheless become too low (hypoglycemia), multiple mechanisms exist to counteract this. First glucagon is secreted, stimulating the liver to release more glucose. Next adrenalin is produced, which is also able to raise blood glucose levels. Cortisol and growth hormone can also help counteract low blood glucose. Together these mechanisms provide healthy persons with an effective counterregulation to low blood glucose levels. This is however not the case for diabetic patients. Diabetes is characterized by high blood glucose levels and therefore needs to be treated with glucose‐lowering drugs, such as insulin. This leads occasionally to hypoglycemia, and diabetic patients are therefore very dependent on a well‐functioning counterregulation. Diabetes is however often accompanied by defects in the glucagon response. In addition it has been shown that recurrent hypoglycemia decreases the counterregulatory responses more and more – a phenomenon dubbed Hypoglycemia‐Associated Autonomic Failure. It is not known why this develops, but it leads to a decrease in the important adrenaline response, and also makes the patient less aware of the low glucose levels. This results in even more hypoglycemic episodes – a vicious circle which necessitates a reduction of the insulin dose and thereby prevents an optimal diabetes treatment. The aim of the studies presented in this thesis was therefore to further investigate the mechanisms behind the counterregulatory responses to hypoglycemia. In addition it was investigated how and why these responses decrease with recurrent hypoglycemia. All studies were performed in rats. The first experiments investigated how the counterregulatory responses depend on each other, how insulin plays a role, and what the effect is of a reduced availability of other energy sources on the counterregulatory responses. It was shown that the counterregulation of low blood glucose levels is very accurate, with the different counterregulatory responses
ix

ensuring that glucose levels always stay above a certain threshold level, independent of the amount of insulin administered. A possible explanation for this would be that a higher insulin level in the blood further stimulates the counterregulatory responses. Furthermore it was shown that a reduction of other energy sources (such as after 48 hours of fasting, or after administration of a fat oxidation blocker) markedly enhanced the counterregulatory responses to hypoglycemia – possibly indicating that the body recognizes its increased dependence on glucose. The next studies investigated the role of the noradrenergic signal transduction in the hypothalamus – a brain part controlling much of the energy homeostasis. In studies at the University of Illinois, hypoglycemia was observed to increase secretion of the neurotransmitter noradrenaline. This response did not disappear completely when glucose was administered, which can also indicate a role for the administered insulin itself. Thereafter we discovered that this noradrenaline response is indeed important in activating the counterregulatory responses, since blocking noradrenergic neurotransmission decreased the responses to hypoglycemia. Finally a number of experiments with recurrent hypoglycemia were performed. Importantly we observed that rats also show a reduction of the counterregulatory responses, which makes it possible to use this animal for further research into the development of Hypoglycemia‐Associated Autonomic Failure. In subsequent studies it was shown that the hypoglycemia frequency as well as the insulin dose might be important. Furthermore the counterregulatory responses to hypoglycemia were also reduced after recurrent administration of a glucose oxidation blocker, showing that this is likely to be a general adaptive process and not unique for insulin‐induced hypoglycemia. In conclusion, these investigations have resulted in new insights into the coordination of the counterregulatory responses, the neuronal networks that are involved, as well as in the development of Hypoglycemia‐Associated Autonomic Failure.
x

Abbreviations and definitions 2‐DG (2‐deoxyglucose): drug used to block glucose metabolism, thereby creating
glucoprivation ANOVA (analysis of variance): statistical test method CRs (counterregulatory responses): responses aimed at restoring the normal situation DCCT (diabetes control and complications trial): large trial study which proved that tight
control of blood glucose levels greatly reduces the risk for diabetic long‐term complications, but increases the risk for hypoglycemia
EDTA (ethylenediaminetetraacetic acid): anticoagulant and antioxidant GABA (gamma‐amino butyric acid): principal inhibitory neurotransmitter in the central
nervous system HAAF (hypoglycemia‐associated autonomic failure): reduction in the onset and magnitude
of the counterregulatory responses to hypoglycemia, caused by antecedent hypoglycemic episodes
HPLC (high‐pressure liquid chromatography): analysis technique using chromatography columns to separate sample compounds before electrochemical or photometric detection
i.v. (intravenous): administration directly into the venous system LHA (lateral hypothalamic area): hypothalamic part involved in among others food intake MA (mercaptoacetate): drug used to block fatty acid metabolism, thereby creating
lipoprivation NE (norepinephrine): American name for the key sympathetic neurotransmitter
noradrenaline PVN (paraventricular nucleus): hypothalamic nucleus greatly involved in the autonomic
nervous system; also called PVH PVP (polyvinylpyrrolidone): substance used to increase a solutionʹs viscosity RIA (radioimmunoassay): assay technique using antibodies and radioactive labeled tracer
compound to determine protein quantities SEM (standard error of the mean): statistical parameter U (unit): standardized quantity measure for proteins; for insulin, one unit is defined as
6 nmol, i.e. approximately 35 μg VMH (ventromedial hypothalamus): hypothalamic nucleus containing important glucose‐
sensitive circuits; also called VMN
xi

xii

Chapter 1
General introduction
I think animal testing is a terrible idea; they get all nervous and give the wrong answers.
‐ A Bit of Fry and Laurie
1

2

Chapter 1 – General introduction
Chapter 1 General introduction
Glucose homeostasis Glucose levels in the blood are well‐regulated. Glucose is a vital energy substrate, and it is therefore of paramount importance that its levels are controlled. High glucose levels cost much energy to maintain, and may lead to long‐term complications such as microvascular and macrovascular damage. Low levels will impair energy availability, which is also undesirable – especially for the brain which is predominantly dependent on glucose for its energy. Ideal therefore would be a constant optimal level of glucose in the blood, which moreover can be adjusted in times with changed demand or supply. The body has several mechanisms to ensure this homeostatic situation (5, 9). The supply of glucose to many tissues is regulated by the pancreatic hormone insulin. As a hydrophilic molecule, glucose needs to be transported across the cellular membrane to enter the cells. This is achieved by glucose transporter proteins, and the most sensitive of those is activated by insulin. Other tissues such as the brain have insulin‐independent glucose transporters however, and can thereby always use glucose from the blood independent of the presence of insulin (3). Because of its stimulation of glucose uptake, insulin is the key hormone to counteract high blood glucose levels. During hyperglycemia, insulin release from the pancreatic beta‐cells is stimulated, and the increased insulin levels inhibit glucagon and stimulate uptake of glucose by the tissues that express the insulin‐sensitive glucose transporter (especially muscle and fat) (5). The increased insulin levels also stop the release of glucose from the liver (7). This results in a reduction of blood glucose levels, and storage of energy. In addition, insulin is transported into the brain, where it is thought to increase satiety and thereby decrease food intake (43, 56). In contrast, low blood glucose levels are counteracted by a range of hormones (5, 31, 34, 46, 57). The two major hyperglycemic hormones are glucagon and adrenaline. Glucagon is secreted from the pancreatic alpha‐cells, and its main function is to stimulate glucose production and release by the liver. Adrenaline is released from the adrenal medulla and acts on most of the tissues in the body. Among others it increases glucose production by the liver and kidneys, inhibits glucose uptake by muscle and promotes lactate release, and stimulates glucagon secretion. All these responses seem to be under control of the brain (26, 41, 51). The brain reacts to changes in blood glucose levels (2, 47), and thereby it can regulate the appropriate responses, such as stimulating insulin and inhibiting food intake when glucose levels are high, or stimulating glucagon and adrenaline when glucose levels are low (35, 42). The brain is therefore likely the major player in the control of glycemia. Together these hormonal and neural mechanisms enable healthy organisms to maintain stable blood glucose levels, even in changing environments.
3

Chapter 1 – General introduction
Diabetes and hypoglycemia Diabetes is a chronic disease defined by impaired or absent insulin function. When untreated, this leads to a strongly reduced ability to counterregulate elevated blood glucose levels (hyperglycemia), a reduced ability to use glucose as energy source, and finally ketoacidosis. Hyperglycemia on the long term also leads to microvascular and macrovascular complications, increasing the risk for blindness, kidney failure, neuropathy, and cardiovascular disease (20). Hence, diabetes needs to be treated with therapies aiming to reduce blood glucose levels. Dietary changes and exercise may be sufficient to treat a mild diabetic state, but more pronounced diabetes needs to be treated with hypoglycemic drugs (45, 48). It may be clear that the precise treatment regimen of such drugs is important, because too high or improperly timed dosing may decrease blood glucose too much (hypoglycemia). Drug‐induced hypoglycemia is particularly riskful for several reasons. First, it may come unanticipated. Second, such drugsʹ action often lasts for many hours. Third, the drugʹs effect may occur simultaneously with other factors decreasing glucose levels, such as fasting or physical activity. Finally, diabetes is accompanied by impairment of the normal counterregulatory responses to hypoglycemia (12, 37) – as discussed later. Therefore, while significant hypoglycemia is very rare in healthy persons, it is common for diabetes patients, especially those on insulin therapy. Hypoglycemia poses a considerable problem for the treatment of diabetes. Although its mortality is low (hypoglycemia only rarely results in severe injury or death), it is a profound psychosocial problem, with strong effects on morbidity and quality of life (22, 23). All diabetes patients on insulin therapy fear hypoglycemia; afraid of getting into severe hypoglycemia, being unable to perform normal daily functions, or even losing consciousness. Many patients worry as much about severe hypoglycemia as they do about the serious long‐term complications of diabetes (44). This fear of the incapacitating effect of hypoglycemia results in a non‐optimal treatment of diabetes, because it causes many physicians and patients to shun the insulin doses needed to fully normalize blood glucose levels. This results in chronic hyperglycemia which significantly increases the risk for the long‐term microvascular and macrovascular complications – increasing morbidity and mortality. This reduced compliance is particularly a problem in intensive insulin therapy, which aims specifically at avoiding those long‐term complications. Intensive therapy allows a much tighter glucose control, bringing the daily glucose profile closer to a normal profile. As shown in the Diabetes Control and Complications Trial (DCCT) (20, 38, 40), intensive therapy greatly reduces the incidence of the aforementioned long‐term microvascular and macrovascular complications of diabetes. It does however increase the incidence of hypoglycemia (19, 21), because it is very difficult to regulate glucose levels close to normal without an increased risk of hypoglycemia – which patients and their physicians will try to avoid, at the cost of a suboptimal glucose profile (52). Taken together, it becomes clear that hypoglycemia is the main limitation in the treatment of diabetes (14, 18, 25). In addition, the problem of hypoglycemia is becoming
4

Chapter 1 – General introduction
pertinent for many more patients, because the number of diabetes patients on intensive insulin therapy has greatly increased since the DCCT. It is therefore very important to understand the physiological mechanisms by which hypoglycemia is detected and counteracted.
Counterregulation to hypoglycemia As mentioned before, low glucose levels are counterregulated by a variety of responses, some of which may be impaired in diabetes. In healthy humans or animals, a number of systems respond to hypoglycemia. A hierarchy for these counterregulatory responses has been described (13, 28, 39). Generally, the first response to a decrease in blood glucose levels is the suppression of endogenous insulin production, which happens already after a small decline in blood glucose. When glucose levels drop further, secretion of the most important hyperglycemic hormones starts – first glucagon, followed by adrenaline, while corticosteroids and growth hormone also may respond (5, 33, 55). Low glucose levels will in addition generate a feeling of hunger, and food intake is hence the normal behavioral response to hypoglycemia. These responses are mediated by the autonomic nervous system (30, 31). When glucose levels keep going down, sympathetic activity increases further, and together with the concomitant adrenaline response, this produces the sensations that diabetes patients learn to associate with hypoglycemia (such as sweating and trembling (6, 10)). These sensations are very important, since they signal the upcoming hypoglycemia – enabling the subject to become aware of the situation and take appropriate action (intake of carbohydrates) and perhaps also adjust therapy regimen to avoid repetition of the problem. In diabetes, the counterregulatory responses to hypoglycemia are of even greater importance. Not only do diabetes patients experience many hypoglycemic episodes, but those episodes are also of a serious and longer‐lasting nature. Unfortunately, diabetes is accompanied by several defects in the normal counterregulatory responses (12). Firstly, the pancreatic beta‐cells are malfunctioning, and therefore the important early counterregulatory response to hypoglycemia – inhibition of insulin secretion – is partially or completely impaired. Severe hypoglycemia is indeed less common in diabetes patients who still have some residual beta‐cell functionality (as shown by the presence of C‐peptide in the blood) (21). Furthermore, the glucagon response to hypoglycemia disappears during the first years after the onset of diabetes (37). This means that two of the most important counterregulatory responses to hypoglycemia are impaired in diabetes patients. A proper adrenaline response and an accurate awareness of hypoglycemia are therefore more than crucial for the diabetes patient to recover from a hypoglycemic episode. It is unknown how the different counterregulatory responses are coordinated in relation to each other. The brain is involved in the control of energy metabolism (36, 49, 50) and is known to be involved in the counterregulatory responses to hypoglycemia (4, 47), but detailed information on the areas involved and the neurochemical background of this coordination is scarce. It is also unknown whether the counterregulatory responses adapt to situations with higher energy demand or lower energy availability (such as during exercise
5

Chapter 1 – General introduction
or fasting, situations where diabetes patients have a greatly increased risk of hypoglycemia). Studies suggest that counterregulatory responsivity may increase during fasting (32, 53), but this has not been experimentally studied yet for insulin‐induced hypoglycemia. Thus more investigations into the mechanistic nature of hypoglycemia counterregulation are needed.
Recurrent hypoglycemia and hypoglycemia unawareness As was concluded in the previous paragraphs, hypoglycemia occurs more often in diabetes patients, the hypoglycemic episodes are more severe and longer‐lasting, and essential counterregulatory responses are impaired (12, 37). There is an other negative effect: the more often hypoglycemia occurs, the greater the risk that it happens again (15). An increased frequency of hypoglycemia impairs the counterregulatory responses to hypoglycemia, a phenomenon known as Hypoglycemia‐Associated Autonomic Failure (HAAF) (1, 12, 16). HAAF affects most major counterregulatory responses to hypoglycemia, including adrenaline, meaning that a stronger reduction of blood glucose levels is needed before this important response is triggered. In addition, the feelings associated with hypoglycemia (such as sweating, trembling, increased pulse) are reduced as well, a condition called hypoglycemia unawareness (5, 8, 29). Taken together, patients with HAAF and hypoglycemia unawareness fail to produce the appropriate autonomic counterregulatory responses to counteract hypoglycemia, while at the same time they are less aware of their becoming hypoglycemic. The consequence is that hypoglycemia occurs more and more often, which again further worsens the above mentioned defects – a vicious circle which can only be broken by scrupulously avoiding hypoglycemia (11, 17, 54). It is estimated that 20‐25% of insulin‐treated patients have impaired hypoglycemia awareness, while this increases to around 50% for patients who have been on insulin therapy for 25‐30 years (24, 27, 44). We may therefore conclude that HAAF, the impairment of the autonomic responses to hypoglycemia, is a serious problem associated with intensive insulin therapy. Hypoglycemia in itself is not necessarily dangerous, as long as the patient is aware of the declining blood glucose levels and can take appropriate action (intake of carbohydrates, and avoiding potential dangerous activities such as driving a vehicle); therefore preservation of hypoglycemia awareness is important for every patient on insulin therapy. Intensive insulin therapy has many advantages – and many patients have switched to this therapy form. This increases the occurrence of hypoglycemia unawareness, and it is therefore crucial to understand the problem of recurrent hypoglycemia. However, the underlying mechanisms that cause the development of HAAF and hypoglycemia unawareness is still unclear.
Counterregulation to acute and recurrent hypoglycemia in rats From the previous paragraphs it is clear that we need to obtain more insight in 1) the underlying mechanisms that control the counterregulatory responses to insulin‐induced hypoglycemia, and the factors that may influence this regulation such as nutritional state; 2)
6

Chapter 1 – General introduction
the neurochemical nature and the central nervous pathways controlling these responses; and 3) the development of defects due to recurrent hypoglycemia. The studies described in this thesis are aimed at investigating these three research questions. Due to the fundamental nature of these questions as well as to enable brain investigations, all studies were performed in rats. The first section of this thesis investigates the regulation and adaptation of the counterregulatory responses to insulin‐induced hypoglycemia. We studied these responses by administering different doses of insulin in fed and fasted rats (Chapter 2). Insulin was infused intravenously and the counterregulatory responses were determined in blood samples taken throughout the study period. This study also addressed the question how a change in nutritional state (i.e. fasting) may affect the counterregulation to hypoglycemia. In the next study the effect of another change in energy availability was examined. Here we studied counterregulatory responses when insulin‐induced hypoglycemia was combined with reduced availability of energy from fatty acids (Chapter 3). The second section of this thesis focuses on the brain mechanisms involved in the counterregulation to hypoglycemia. Data from the literature pointed to a possible role for noradrenergic neurotransmission in the hypothalamus in the activation of the counterregulatory responses. To investigate this, noradrenaline release in the hypothalamus during euglycemia and hypoglycemia was measured by means of in vivo microdialysis (Chapter 4), while in another study noradrenergic neurotransmission in the hypothalamus during hypoglycemia was pharmacologically blocked by adrenoceptor antagonists (Chapter 5). The last section of this thesis addresses the issue of recurrent hypoglycemia. Since no established animal model existed for the development of Hypoglycemia‐Associated Autonomic Failure, we performed a number of pilot studies to investigate the development of HAAF in rats, and to characterize some of the associated phenomena, such as the individual differences in susceptibility to HAAF and the importance of the hypoglycemic drug used (Chapter 6).
References 1. S.A. Amiel, R.S. Sherwin, D.C. Simonson, and W.V. Tamborlane; Effect of intensive
insulin therapy on glycemic thresholds for counterregulatory hormone release. Diabetes (1988) 37: 901‐907
2. B.K. Anand, S. Dua, and B. Singh; Electrical activity of the hypothalamic ʹfeeding centresʹ under the effect of changes in blood chemistry. Electroencephalography and Clinical Neurophysiology (1961) 13: 54‐59
3. G.I. Bell, C.F. Burant, J. Takeda, and G.W. Gould; Structure and function of mammalian facilitative sugar transporters. Journal of Biological Chemistry (1993) 268: 19161‐19164
7

Chapter 1 – General introduction
4. W.P. Borg, M.J. During, R.S. Sherwin, M.A. Borg, M.L. Brines, and G.I. Shulman; Ventromedial hypothalamic lesions in rats suppress counterregulatory responses to hypoglycemia. Journal of Clinical Investigation (1994) 93: 1677‐1682
5. P.J. Boyle and J. Zrebiec; Physiological and behavioral aspects of glycemic control and hypoglycemia in diabetes. Southern Medical Journal (2007) 100: 175‐182
6. V.J. Briscoe and S.N. Davis; Hypoglycemia in Type 1 and Type 2 diabetes: physiology, pathophysiology, and management. Clinical Diabetes (2006) 24: 115‐121
7. A.D. Cherrington, D. Edgerton, and D.K. Sindelar; The direct and indirect effects of insulin on hepatic glucose production in vivo. Diabetologia (1998) 41: 987‐996
8. W.L. Clarke, L.A. Gonder‐Frederick, F.E. Richards, and P.E. Cryer; Multifactorial origin of hypoglycemic symptom unawareness in IDDM. Association with defective glucose counterregulation and better glycemic control. Diabetes (1991) 40: 680‐685
9. E.P.M. Corssmit, J.A. Romijn, and H.P. Sauerwein; Regulation of glucose production with special attention to nonclassical regulatory mechanisms: A review. Metabolism: Clinical and Experimental (2001) 50: 742‐755
10. D.J. Cox, L. Gonderfrederick, B. Antoun, P.E. Cryer, and W.L. Clarke; Perceived symptoms in the recognition of hypoglycemia. Diabetes Care (1993) 16: 519‐527
11. I.C. Cranston, J. Lomas, A. Maran, I. Macdonald, and S.A. Amiel; Restoration of hypoglycaemia awareness in patients with long‐duration insulin‐dependent diabetes. Lancet (1994) 344: 283‐287
12. P.E. Cryer; Hypoglycemia‐associated autonomic failure in diabetes. American Journal of Physiology (2001) 281: E1115‐E1121
13. P.E. Cryer; Hierarchy of physiological responses to hypoglycemia: relevance to clinical hypoglycemia in type I (insulin dependent) diabetes mellitus. Hormone and Metabolic Research (1997) 29: 92‐96
14. P.E. Cryer; Hypoglycaemia: The limiting factor in the glycaemic management of Type I and Type II Diabetes. Diabetologia (2002) 45: 937‐948
15. P.E. Cryer; Hypoglycemia begets hypoglycemia in IDDM. Diabetes (1993) 42: 1691‐1693
16. P.E. Cryer; Iatrogenic hypoglycemia as a cause of hypoglycemia‐associated autonomic failure in IDDM. A vicious cycle. Diabetes (1992) 41: 255‐260
17. S. Dagogo‐Jack, C. Rattarasarn, and P.E. Cryer; Reversal of hypoglycemia unawareness, but not defective glucose counterregulation, in IDDM. Diabetes (1994) 43: 1426‐1434
18. S. Davis and M.D. Alonso; Hypoglycemia as a barrier to glycemic control. Journal of Diabetes and Its Complications (2004) 18: 60‐68
19. DCCT Research Group; Epidemiology of severe hypoglycemia in the Diabetes Control and Complications Trial. American Journal of Medicine (1991) 90: 450‐459
20. DCCT Research Group; The effect of intensive treatment of diabetes on the development and progression of long‐term complications in insulin‐dependent diabetes mellitus. New England Journal of Medicine (1993) 329: 977‐986
21. DCCT Research Group; Hypoglycemia in the diabetes control and complications trial. Diabetes (1997) 46: 271‐286
22. B.M. Frier; Morbidity of hypoglycemia in type 1 diabetes. Diabetes Research and Clinical Practice (2004) 65: S47‐S52
23. B.M. Frier; How hypoglycaemia can affect the life of a person with diabetes. Diabetes‐Metabolism Research and Reviews (2008) 24: 87‐92
8

Chapter 1 – General introduction
24. B.M. Frier; Hypoglycaemia‐‐clinical consequences and morbidity. International Journal of Clinical Practice (2000) 112: 51‐55
25. B.M. Frier and B.M. Fisher; Hypoglycaemia in clinical diabetes. Wiley, Chichester, 1999
26. R.T. Frizzell, E.M. Jones, S.N. Davis, D.W. Biggers, S.R. Myers, C.C. Connolly, D.W. Neal, J.B. Jaspan, and A.D. Cherrington; Counterregulation during hypoglycemia is directed by widespread brain regions. Diabetes (1993) 42: 1253‐1261
27. J. Geddes, J.E. Schopman, N.N. Zammitt, and B.M. Frier; Prevalence of impaired awareness of hypoglycaemia in adults with Type 1 diabetes. Diabetic Medicine (2008) 25: 501‐504
28. J.E. Gerich, J. Davis, M. Lorenzi, R. Rizza, N. Bohannon, J. Karam, S. Lewis, R. Kaplan, T. Schultz, and P.E. Cryer; Hormonal mechanisms of recovery from insulin‐induced hypoglycemia in man. American Journal of Physiology (1979) 236: E380‐E385
29. J.E. Gerich, M. Mokan, T.F. Veneman, M.T. Korytkowski, and A. Mitrakou; Hypoglycemia unawareness. Endocrine Reviews (1991) 12: 356‐371
30. P.J. Havel and G.J. Taborsky; The contribution of the autonomic nervous system to increased glucagon secretion during hypoglycemic stress: update 1994. Endocrine Reviews (1994) 2: 201‐204
31. R.P. Hoffman; Sympathetic mechanisms of hypoglycemic counterregulation. Current Diabetes Reviews (2007) 3: 185‐193
32. K. Hojlund, M. Wildner‐Christensen, O. Eshoj, C. Skjaerbaek, J.J. Holst, O. Koldkjaer, D.M. Jensen, and H. Beck‐Nielsen; Reference intervals for glucose, beta‐cell polypeptides, and counterregulatory factors during prolonged fasting. American Journal of Physiology (2001) 280: E50‐E58
33. E.W. Kraegen, L. Lazarus, and L.V. Campbell; Failure of insulin infusion during euglycemia to influence endogenous basal insulin secretion. Metabolism: Clinical and Experimental (1983) 32: 622‐627
34. I. Lager; The insulin‐antagonistic effect of the counterregulatory hormones. Journal of Internal Medicine Supplement (1991) 735: 41‐48
35. B.E. Levin, A.A. Dunn Meynell, and V.H. Routh; Brain glucose sensing and body energy homeostasis: role in obesity and diabetes. American Journal of Physiology (1999) 276: R1223‐R1231
36. B.E. Levin and V.H. Routh; Role of the brain in energy balance and obesity. American Journal of Physiology (1996) 271: R491‐R500
37. M. Lorenzi, N. Bohannon, E. Tsalikian, and J.H. Karam; Duration of type I diabetes affects glucagon and glucose responses to insulin‐induced hypoglycemia. Western Journal of Medicine (1984) 141: 467‐471
38. C.L. Martin, J. Albers, W.H. Herman, P. Cleary, B. Waberski, D.A. Greene, M.J. Stevens, E.L. Feldman, DCCT/EDIC Research Group, and DCCT Research Group; Neuropathy among the diabetes control and complications trial cohort 8 years after trial completion. Diabetes Care (2006) 29: 340‐344
39. A. Mitrakou, C. Ryan, T. Veneman, M. Mokan, T. Jenssen, I. Kiss, J. Durrant, P.E. Cryer, and J. Gerich; Hierarchy of glycemic thresholds for counterregulatory hormone secretion, symptoms, and cerebral dysfunction. American Journal of Physiology (1991) 260: E67‐E74
9

Chapter 1 – General introduction
40. D.M. Nathan, P.A. Cleary, J.Y. Backlund, S.M. Genuth, J.M. Lachin, T.J. Orchard, P. Raskin, B. Zinman, and DCCT/EDIC Research Group; Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. New England Journal of Medicine (2005) 353: 2643‐2653
41. A. Nijima; The nervous mechanisms involved in blood glucose homeostasis. Les mécanismes nerveux de la régulation de la glycémie. Archives Internationales de Physiologie et de Biochimie (1989) 97: A37‐A49
42. L. Penicaud, C. Leloup, A. Lorsignol, T. Alquier, and E. Guillod; Brain glucose sensing mechanism and glucose homeostasis. Current Opinion in Clinical Nutrition and Metabolic Care (2002) 5: 539‐543
43. D. Porte Jr., D.G. Baskin, and M.W. Schwartz; Perspectives in diabetes ‐ Insulin signaling in the central nervous system ‐ A critical role in metabolic homeostasis and disease from C‐elegans to humans. Diabetes (2005) 54: 1264‐1276
44. S. Pramming, B. Thorsteinsson, I. Bendtson, and C. Binder; Symptomatic hypoglycaemia in 411 type 1 diabetic patients. Diabetic Medicine (1991) 8: 217‐222
45. S.A. Raptis and G.D. Dimitriadis; Oral hypoglycemic agents: insulin secretagogues, alpha‐glucosidase inhibitors and insulin sensitizers. Experimental and Clinical Endocrinology & Diabetes (2001) 109 Suppl 2: S265‐S287
46. R.A. Rizza, P.E. Cryer, and J.E. Gerich; Role of glucagon, catecholamines, and growth hormone in human glucose counterregulation. Effects of somatostatin and combined alpha‐ and beta‐adrenergic blockade on plasma glucose recovery and glucose flux rates after insulin‐induced hypoglycemia. Journal of Clinical Investigation (1979) 64: 62‐71
47. V. Routh, Z. Song, and X. Liu; The role of glucosensing neurons in the detection of hypoglycemia. Diabetes Technology and Therapeutics (2004) 6: 413‐421
48. A. Salsali and M. Nathan; A review of types 1 and 2 diabetes mellitus and their treatment with insulin. American Journal of Therapeutics (2006) 13: 349‐361
49. M.W. Schwartz and D. Porte Jr; Diabetes, obesity, and the brain. Science (2005) 307: 375‐379
50. A.B. Steffens, A.J.W. Scheurink, P.G. Luiten, and B. Bohus; Hypothalamic food intake regulating areas are involved in the homeostasis of blood glucose and plasma FFA levels. Physiology & Behavior (1988) 44: 581‐589
51. A.B. Steffens, J.H. Strubbe, B. Balkan, and A.J.W. Scheurink; Neuroendocrine mechanisms involved in regulation of body weight, food intake and metabolism. Neuroscience & Biobehavioral Reviews (1990) 14: 305‐313
52. C.J. Thompson, J.F. Cummings, J. Chalmers, C. Gould, and R.W. Newton; How have patients reacted to the implications of the DCCT? Diabetes Care (1996) 19: 876‐879
53. G. van Dijk, A. Scheurink, S. Ritter, and A. Steffens; Glucose homeostasis and sympathoadrenal activity in mercaptoacetate‐treated rats. Physiology & Behavior (1995) 57: 759‐764
54. T.F. Veneman and D.W. Erkelens; Clinical review 88: hypoglycemia unawareness in noninsulin‐ dependent diabetes mellitus. Journal of Clinical Endocrinology & Metabolism (1997) 82: 1682‐1684
55. W.W. Winder, P.S. MacLean, S.L. Chandler, W. Huang, and R.H. Mills; Role of epinephrine during insulin‐induced hypoglycemia in fasted rats. Journal of Applied Physiology (1994) 77: 270‐276
10

Chapter 1 – General introduction
56. S.C. Woods, E.C. Lotter, L.D. McKay, and D. Porte Jr; Chronic intracerebroventricular infusion of insulin reduces food intake and body weight of baboons. Nature (1979) 282: 503‐505
57. N. Yamaguchi; Sympathoadrenal system in neuroendocrine control of glucose: mechanisms involved in the liver, pancreas, and adrenal gland under hemorrhagic and hypoglycemic stress. Canadian Journal of Physiology and Pharmacology (1992) 70: 167‐206
11

Chapter 1 – General introduction
12

Section I – Counterregulation, insulin, and the nutritional state
Westheimerʹs Discovery: A couple of months in the laboratory
can frequently save a couple of hours in the library.
13

14

Chapter 2
Insulin levels and fasting independently co‐determine the counterregulatory responses to
hypoglycemia
15

16

Chapter 2 – Insulin levels and fasting
Chapter 2 Insulin levels and fasting independently co‐determine the counterregulatory responses to hypoglycemia
These studies were presented at the 1997 IDF Meeting in Helsinki, Finland Diabetologia (1997) volume 40 (Suppl. 1), page A237
Insulin‐induced hypoglycemia elicits a number of counterregulatory responses, including activation of the autonomic nervous system and secretion of hormones. It has been suggested that these responses depend not only on glucose levels but also on insulin levels. The nutritional state of the body may also play a role. In the present study, the hormonal responses to hypoglycemia were studied at different insulin levels and in different nutritional states. Hypoglycemia was induced in normally fed and 48h food deprived rats by intravenous infusion of different insulin doses, ranging from 5.5 to 120 (fed rats) and 0.44 to 22 mU.kg‐1.min‐1 (fasted rats). Blood samples were frequently withdrawn for determination of glucose, insulin, glucagon, adrenaline, noradrenaline and corticosterone. In normally fed rats receiving insulin, the reduction in glucose levels was similar for almost all insulin doses. In contrast, the counterregulatory responses were different between the insulin doses. Low doses of insulin increased only glucagon, higher insulin loads led to dose‐dependent increases in both glucagon and adrenaline levels, and the highest insulin dose was accompanied by increases in glucagon, adrenaline as well as corticosterone. In 48h fasted rats, a similar pattern was observed. Different doses of insulin resulted in similar glucose nadir levels and dose‐dependent responses in glucagon, adrenaline, noradrenaline and corticosterone. However, when compared with normally fed rats, the nadir for glucose was lower and the magnitude of the counterregulatory responses was higher in the fasted rats. Together, these data provide evidence for a tight control of glucose levels during hypoglycemia, and a strong and complex coordination of the different hormonal counterregulatory responses, partly dependent on the ambient insulin levels and the nutritional state.
Introduction Hypoglycemia is a common complication in insulin‐treated diabetes. It is counteracted by counterregulatory responses to restore euglycemia. The counterregulatory responses to insulin‐induced hypoglycemia have been described in humans (5, 7, 8, 19) and in animals such as rats (2, 20, 39) and dogs (13, 15). Several types of counterregulatory responses can be identified: local responses (most notably the immediate changes in glucose production by hepatic autoregulation), endocrine responses (changes in secretion of a range of hormones), and behavioral responses (initiation of food intake). Hierarchical relations have been proposed for the hormonal responses, generally posing that hypoglycemia is initially counteracted by an increase in glucagon secretion, then by activation of the adrenal medulla leading to adrenaline secretion, and finally followed by the release of other counterregulatory hormones such as glucocorticoids and growth hormone (4, 19, 21, 25). There are several factors that may influence the counterregulatory response to hypoglycemia. It may be obvious that the circulating glucose level (i.e. the depth of hypoglycemia) is the primary factor that determines the magnitude of the counterregulatory responses (6, 27). But insulin by itself also seems to have an effect on the counterregulatory responses both in normal subjects (9) and in type 1 diabetes patients (10, 24), although there are some conflicting data (12). Less is known about the influence of the nutritional state of the body on the counterregulatory responses to hypoglycemia. Especially fasting can be of importance, since fasting is associated with many metabolic changes all aiming to spare
17

Chapter 2 – Insulin levels and fasting
glucose for the brain (23, 33). Insulin levels go down, insulin sensitivity increases, and glucose levels decrease. Hepatic glycogen stores will become depleted and gluconeogenesis will become increasingly important in the maintenance of blood glucose levels. These changes may significantly aggravate the threat induced by insulin and at the same time impede the increased endogenous glucose production needed to restore normoglycemia. It might also increase the importance of the level of insulinemia for the counterregulatory responses. The current study was designed to investigate the importance of insulin and of fasting in the counterregulatory responses to hypoglycemia. Therefore, we studied the onset, duration, and magnitude of different counterregulatory responses to insulin‐induced hypoglycemia in rats by varying the ambient insulin levels as well as the nutritional state.
Methods
Animals and surgery Male Wistar rats were used, weighing 300‐330 grams at the beginning of the experiments. They were individually housed in 25*25*30 cm cages with wood shavings bedding. Room temperature was 21 ± 1 °C and the lights were on from 08:00 until 20:00. Food (standard RMH chow, Hope Farms, Woerden, The Netherlands) and water were available ad lib unless otherwise stated. The animals were frequently handled and weighed. Under halothane/N2O inhalation anesthesia, all rats were fitted with two permanent silicone catheters (Medica BV, Den Bosch, The Netherlands), one for i.v. infusions and the other for stress‐free blood sampling. Both catheters were inserted via the jugular vein, according to the principle described by Steffens (31, 37), with the catheter tips ending in the superior vena cava just before the right atrium. In one group of rats, only the catheter for infusions was inserted via the jugular vein; the blood sampling catheter was inserted into the hepatic portal vein, according to the method described by Strubbe et al. (32). The catheter tip ends just downstream of the junction with the pancreatoduodenal vein, so that glucagon secretion dynamics can be studied without the confounding effects of hepatic extraction. The animals were allowed two weeks to recover after the surgery. During the recovery period, they were habituated to the experimental setup conditions (attachment of sampling and infusion tubes, etc.), so that the experiments could be performed with undisturbed freely‐moving animals. The experimental procedures were approved by the Animal Experiments Committee of the University of Groningen.
Experimental design Experiment 1 was designed to study the effects of insulin on the counterregulatory responses in the fed state. In Experiment 1a, hypoglycemia was induced by a 90‐minute intravenous infusion of insulin, at doses of 0, 5.5, 11, 22, 44, 88 or 120 mU.kg‐1.min‐1 (n=5‐8 per group). Blood samples were withdrawn from the jugular vein catheter to determine glucose, insulin, glucagon, adrenaline, noradrenaline, and corticosterone levels. Experiment
18

Chapter 2 – Insulin levels and fasting
1b was similar to Experiment 1a, but the blood samples were now withdrawn from the portal vein to determine glucose, insulin, and glucagon levels. In this experiment only two doses of insulin (11 and 22 mU.kg‐1.min‐1) were used (n=7 in each group). Experiment 2 was designed to study the effects of insulin on the counterregulatory responses in the fasted state. In this experiment, rats were fasted for 48 hours prior to being subjected to hypoglycemia. Hypoglycemia was induced by a 90‐minute intravenous infusion of insulin, at doses of 0.44, 2.2, 5.5, 11 or 22 mU.kg‐1.min‐1 (n=4‐6 per group). Again, blood samples were withdrawn from the jugular vein catheter to determine glucose, insulin, glucagon, adrenaline, noradrenaline, and corticosterone levels. All experiments were performed between 10:00 and 14:00. Food was removed 2 hours (fed state, Experiment 1) or 48 hours (fasted state, Experiment 2) earlier. The rats’ sampling and infusion catheters were connected to polyethylene tubings at least one hour prior to the experiment, to minimize adverse effects due to handling stress. Two blood samples were then taken with a 10‐minute interval, to serve as baseline values. At time point t=0, the 90‐minute infusion of insulin (Velosulin, Novo Nordisk Farma, Alphen a/d Rijn, The Netherlands) or vehicle (0.9% NaCl) was started through the jugular infusion catheter, at an infusion speed of 3.2 ml.kg‐1.min‐1. During the infusion, blood was sampled at time points 2.5, 5, 7.5, 10, 15, 20, 30, 45, 60, 75, and 90 minutes. Immediately after the t=90 sample the infusion was stopped, and a last blood sample was taken another 30 minutes later. Loss of blood volume was compensated by transfusing the same amount of heparinized blood from a donor rat after each blood sample.
Analysis Blood samples were kept chilled at 0 °C during the experiment, in tubes with EDTA and aprotinin (Trasylol). Afterwards 50 μl blood was removed for glucose determination (Hoffmannʹs ferricyanide method (22)), the rest was centrifuged for 15 minutes at 2600 G and 5 °C. Plasma portions were stored at ‐80 °C for determination of glucagon (Glucagon RIA Kit, Linco Research Inc, St. Charles, MO, USA) and catecholamines (HPLC with electrochemical detection (30)), and at ‐20 °C for determination of insulin (Rat Insulin RIA Kit, Linco Research Inc) and corticosterone (HPLC with UV detection (11)). Results are reported as average ± SEM (standard error of the mean). Statistical differences were determined with ANOVA or t‐test (paired where relevant). The significance level was set to p<0.05.
Results
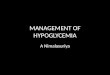
Experiment 1 – Insulin‐induced hypoglycemia in fed rats Figure 1 depicts the blood components that were measured before, during and after infusion of various doses of insulin in normally fed rats. Infusion of different doses of insulin led to a dose‐dependent elevation of plasma insulin during the whole infusion period (t=90 levels p<0.0001). Blood glucose levels decreased in all insulin‐infused groups during the infusion, resulting in a nadir level of 4.2 ±
19

Chapter 2 – Insulin levels and fasting
0.1 mM for the lowest insulin dose, but similar nadir levels of 3.1‐3.4 mM for all other insulin doses (at t=90, there were only significant differences between the 0 dose vs all other doses, and between the lowest insulin dose vs all others). Plasma glucagon responded rapidly and in a dose‐dependent manner to the insulin dose, especially in the first 20 minutes where the rise in glucagon levels was dose‐dependent for the insulin dose (t=20 peak response p<0.0001). During the second part of the infusion period, the glucagon levels were still elevated over baseline, but to the same extent for most insulin doses (t=90 average levels were 96‐109 pg/ml, p=0.733), again except the lowest insulin dose (77 ± 6 pg/ml).
0 30 60 90 120
time (min)
0
10
20
30
40
50
corti
cost
eron
e (µ
g/dl
)
0 30 60 90 120
time (min)
0
50
100
150
200
gluc
agon
(pg/
ml)
0 30 60 90 1200
500
1000
1500
nora
dren
alin
e (p
g/m
l)
0 30 60 90 1200
2
4
6
8
gluc
ose
(mM
)
0 30 60 90 1200
500
1000
1500
2000
2500
3000
adre
nalin
e (p
g/m
l)
0 30 60 90 1200.01
0.1
1
10
100
1000
insu
lin (n
g/m
l)
Figure 1. Circulating insulin, glucose, glucagon, adrenaline, noradrenaline, and corticosterone levels during 90‐minute infusion of insulin in normally fed rats (Experiment 1). Insulin doses were 0 (vehicle, ○), 5.5 (●), 11 (□), 22 (■), 44 (∆), 88 (▲) and 120 ( ) mU.kg‐1.min‐1.
20

Chapter 2 – Insulin levels and fasting
Plasma adrenaline did not change significantly during the insulin infusion period in the rats receiving the two lowest insulin doses (5.5 and 11 mU.kg‐1.min‐1). After t=60, the two highest insulin administrations (88 and 120 mU.kg‐1.min‐1) resulted in significant adrenaline responses (p=0.013 and 0.029 compared to baseline). At t=120 these responses reached their highest levels, and here the two medium insulin infusions (22 and 44 mU.kg‐1.min‐1) also showed an adrenaline response. Plasma noradrenaline levels increased slightly with all insulin doses except the lowest, with t=90 levels being significantly elevated over baseline (p values <0.05 for the 11‐120 mU.kg‐1.min‐1 doses). Corticosterone levels increased significantly only after administration of higher insulin doses (p<0.05 for 22, 88 and 120 mU.kg‐1.min‐1). To study glucagon dynamics more accurately, a group of animals with portal vein catheters had been infused with 11 or 22 mU.kg‐1.min‐1 insulin (doses which as mentioned above did not display a peak in the glucagon response in the general circulation). Glucose, insulin and glucagon measurements in blood samples from the hepatic portal vein during the first 30 minutes of the insulin infusion are depicted in Figure 2, together with the corresponding measurements from the samples from the jugular vein catheter. Insulin and glucose levels in the portal vein were similar to those in the general circulation, but glucagon levels were significantly higher in the portal vein, both in the baseline situation (average baseline level in the general circulation 60 ± 3 vs in the portal vein 89 ± 6 pg/ml, p<0.0001) and during the responses (for the two doses used, t=20 levels in the portal vein were 203 ± 18 and 231 ± 18 pg/ml, whilst in the general circulation 83 ± 6 and 97 ± 8 pg/ml). Glucagon secretion, as indicated by the portal vein samples, started increasing as soon as 5‐10 minutes after the start of the insulin infusion (in both doses, t=7.5 was the first time point to be significantly higher than baseline), and not after 10‐15 minutes as suggested by the data sampled from the jugular vein catheter (for these measurements, the first time points to be significantly different from baseline were t=15 for 11 mU.kg‐1.min‐1, and t=10 for 22 mU.kg‐1.min‐1. This rise within 7.5 minutes in portal glucagon levels occurred when glucose levels were still in the normal range (at t=7.5 still between 5.4 ± 0.2 and 5.6 ± 0.2 mM, both in the general circulation and in the portal vein). Furthermore, the portal venous glucagon response did indeed show a peak response at t=20, followed by a decline; similarly to the response shape seen in the general circulation with the higher insulin doses.
21

Chapter 2 – Insulin levels and fasting
0 30 60 90 120
time (min)
0
100
200
300
gluc
agon
(pg/
ml)
0 30 60 90 1200
2
4
6
8
gluc
ose
(mM
)
0 30 60 90 1200.01
0.1
1
10
100
1000
insu
lin (n
g/m
l)
Figure 2. Insulin, glucose, and glucagon levels in the general circulation (squares □■) and in the portal vein (triangles ∆▲) during 90‐minute intravenous infusion of insulin in normally fed rats (Experiment 1). Insulin doses were 11 (open symbols □∆) and 22 (solid symbols ■▲) mU.kg‐1.min‐1. Portal vein samples were taken up until t=30. In summary, different doses of insulin resulted in similar decreases in glucose levels. The lowest two doses of insulin only affected glucagon release. Higher doses of insulin increased both glucagon and adrenaline levels, and the highest two doses led to increases in glucagon and adrenaline as well as corticosterone.
22

Chapter 2 – Insulin levels and fasting
Experiment 2 – Insulin‐induced hypoglycemia in fasted rats Figure 3 depicts the levels of the blood components that were measured before, during and after infusion of various doses of insulin in 48h food deprived rats. Baseline levels of glucose and insulin were significantly lower than in the normally fed rats (glucose: fed rats overall average 6.14 ± 0.04 mM, fasted rats 4.43 ± 0.09 mM, p<0.0001; insulin: fed rats overall average 2.90 ± 0.20 ng/ml, fasted rats 0.21 ± 0.05 ng/ml, p<0.0001). After the start of the insulin infusions at t=0, plasma insulin levels with the lowest insulin dose (0.44 mU.kg‐1.min‐1) did not change from baseline. In the other groups, plasma insulin reached significantly different steady state levels (p<0.0001) related to the infused amount of insulin. At the two doses which were used in both fed and fasted rats (5.5 and 11 mU.kg‐1.min‐1), the reached plasma insulin levels were comparable to those in the fed state (Figure 1). Blood glucose levels decreased with all insulin doses except the lowest (0.44 mU.kg‐1.min‐1). In the 2.2 mU.kg‐1.min‐1 dose, the response in glucose levels was smaller compared to the other three groups (with 2.2 mU.kg‐1.min‐1 the t=90 nadir level was 3.2 ± 0.2 mM, the nadir levels of the three higher doses were 2.6, 2.3 and 2.8 mM). No detectable plasma glucagon responses occurred with the lowest doses, but there were strong increases in the other groups (at t=30 p=0.047 and 0.010 for 11 and 22 mU.kg‐1.min‐1) which were positively correlated to the insulin dose, throughout the whole infusion period. The same effect was observed for plasma adrenaline, which did not change with the lowest insulin doses, but already after 30 minutes strongly responded in a dose‐dependent manner with the higher doses (t=90 p=0.023 and 0.004 for 11 and 22 mU.kg‐1.min‐1). Plasma noradrenaline levels were also elevated over baseline in the highest insulin doses (t=90 p=0.012 and 0.001 for 11 and 22 mU.kg‐1.min‐1). Corticosterone showed high responses starting after 30 minutes in the three highest insulin administrations (t=90 p=0.008, 0.0004 and 0.001 for 5.5, 11 and 22 mU.kg‐1.min‐1). In summary, in fasting rats different doses of insulin resulted in similar decreases in glucose levels. The nadir for blood glucose was much lower than in Experiment 1 (the fed animals). The two lowest doses of insulin did not result in statistically significant counterregulatory responses. The higher three doses of insulin resulted in strong responses in glucagon, corticosterone, adrenaline, and noradrenaline. When compared to the fed animals, similar insulin doses in the fasted rats led to faster onset as well as a greater magnitude of the counterregulation.
23

Chapter 2 – Insulin levels and fasting
0 30 60 90 120
time (min)
0
25
50
75
100
125
corti
cost
eron
e (µ
g/dl
)
0 30 60 90 120
time (min)
0
200
400
600
800
gluc
agon
(pg/
ml)
0 30 60 90 1200
500
1000
1500
nora
dren
alin
e (p
g/m
l)
0 30 60 90 1200
2
4
6
8
gluc
ose
(mM
)
0 30 60 90 1200
1000
2000
3000
4000
5000
adre
nalin
e (p
g/m
l)
0 30 60 90 1200.01
0.1
1
10
100
1000
insu
lin (n
g/m
l)
Figure 3. Circulating insulin, glucose, glucagon, adrenaline, noradrenaline, and corticosterone levels during 90‐minute infusion of insulin in 48h fasted rats (Experiment 2). Insulin doses were 0.44 (▲), 2.2 (∆), 5.5 (●), 11 (□) and 22 (■) mU.kg‐1.min‐1.
Discussion The current study was undertaken to study the importance of insulin and of fasting in the counterregulatory responses to insulin‐induced hypoglycemia. It was shown that low blood glucose resulted in counterregulatory responses, that blood glucose was maintained at the same level across the different insulin levels by differential action of counterregulatory
24

Chapter 2 – Insulin levels and fasting
responses, and that a fasted state resulted in higher counterregulatory responses for similar insulin and glucose levels. Therefore, glucose levels, insulin levels, and the nutritional state each are important determinants of the counterregulatory responses to insulin‐induced hypoglycemia in rats.
Glucose and insulin are independent moderators of the counterregulatory responses One aim of this study was to investigate the counterregulatory responses to insulin‐induced hypoglycemia in rats at different insulin levels. This was done by infusing groups of rats with different amounts of insulin while monitoring their blood glucose levels and counterregulatory responses. A more than ten‐fold difference in the dose of administered insulin (between the 11 and 120 mU.kg‐1.min‐1 administrations in the normally fed rats, with a resulting more than 30‐fold difference in circulating insulin levels) did not result in differences in glucose levels. Instead there were different magnitudes in counterregulatory responses, with the highest counterregulatory responses at the higher doses of insulin. The seemingly most obvious explanation – that insulin had reached a maximal effect already at the 11 mU.kg‐1.min‐1 dose – is unlikely, for several reasons. Insulin is well able to reduce glucose levels to below 2 mM in non‐fasted rats, for example as injections or rapid infusions – even when plasma insulin peak levels are comparable (26). Similarly, the initial drop in glucose levels did show dose‐dependency, also when plasma insulin levels were already near steady‐state levels (at t=15, see Figure 4). Most importantly, this hypothesis cannot explain the counterregulatory responses reacting differently in the different insulin dose groups.
0 10 20 30
time (min)
4
5
6
gluc
ose
(mM
)
Figure 4. Blood glucose levels during infusion of insulin in normally fed rats. Insulin doses were 0 (vehicle, ○), 5.5 (●), 11 (□), 22 (■), 44 (∆), 88 (▲) and 120 ( ) mU.kg‐1.min‐1. This figure represents time frame t=0‐30 minutes from Figure 1. Hence, the observation that the counterregulatory responses did differ between the different insulin doses implies that higher insulin doses indeed did have stronger effects on glucose disposal, but that the animals used stronger counterregulatory responses to
25

Chapter 2 – Insulin levels and fasting
compensate, resulting in similar glucose nadir levels independent of insulin dose. This is also suggested by the fact that the drop in glucose levels is generally stronger with bolus administrations than with infusions (where animals have more time to produce and adjust counterregulatory responses). If this hypothesis is true, it should result in some specific findings. Glucose levels should be maintained at or above a certain level, and the counterregulatory responses should be stronger when more insulin is administered and glucose levels hence are under a stronger pressure. It may be clear from the data presented in Figure 1 that these conditions are indeed met. Although declining slowly, glucose levels were remarkably similar between the different insulin doses. The counterregulatory responses were not only related to the glucose levels but also to the insulin dose: the more insulin, the more and stronger counterregulatory responses, with adrenaline as clear example, and glucagon as well (especially when keeping in mind that the glucagon dose‐responsivity was underestimated when measured in the general circulation, because of the buffering effect of hepatic extraction; as demonstrated in Experiment 1b; see Figure 2). Adrenaline did not respond at all at the lower insulin doses, even though blood glucose went down to the same level as where adrenaline started responding in the animals receiving the highest insulin doses. The insulin dose cannot be the sole determinant of the counterregulatory responses; otherwise it would be impossible to explain why the adrenaline response did not occur until after 60‐75 minutes, while plasma insulin levels were already in steady state from around t=15‐30. The adrenaline response is therefore determined by at least both blood glucose level and insulin dose, for example by insulin affecting the glucose threshold level for adrenaline secretion. This principle of the counterregulatory responses depending both on glucose and on insulin is further illustrated in Figure 5 where the response levels of glucose, insulin, and counterregulatory responses at the end of the infusion period (t=90) are plotted against the administered insulin dose (on the x‐axis). It can clearly be seen that the doses of 11 and 22 mU.kg‐1.min‐1 already reached 90% of the maximal effect on glucose levels (reducing them to 3.4 mM), with the maximal effect (3.1 mM) equally seen at 44, 88 and 120 mU.kg‐1.min‐1 insulin. In contrast to these similar glucose levels, the t=90 response levels of adrenaline and corticosterone kept increasing with increasing insulin doses. This dual effect of both glucose level and insulin dose results in blood glucose levels being maintained at a similar level, independent of the administered insulin dose. Furthermore, an increase in insulin dose seems to enhance the counterregulatory response magnitude by the appropriate amount to compensate for the increased glucose‐lowering effect, thus maintaining blood glucose at the same level regardless of insulin dose. This suggests that the body might be able to perceive the hypoglycemic effect of the insulin dose, and adjust the counterregulatory responses accordingly – independent of the actual blood glucose level.
26

Chapter 2 – Insulin levels and fasting
0 25 50 75 100 125
insulin dose (mU/kg.min)
0
2
4
6
8
t=90
glu
cose
(mM
)
0
250
500
750
1000
1250
t=90
adr
enal
ine
(pg/
ml)
0 25 50 75 100 1250
2
4
6
8
t=90
glu
cose
(mM
)
0
10
20
30
40
t=90
cor
ticos
tero
ne (µ
g/dl
)
0 25 50 75 100 1250
2
4
6
8
t=90
glu
cose
(mM
)
0
50
100
150
200t=
90 g
luca
gon
(pg/
ml)
0 25 50 75 100 1250
2
4
6
8
t=90
glu
cose
(mM
)
0
250
500
750
1000
t=90
nor
adre
nalin
e (p
g/m
l)
0 25 50 75 100 1250
2
4
6
8
t=90
glu
cose
(mM
)
0
100
200
300
400
t=90
insu
lin (n
g/m
l)
Figure 5. Final levels of glucose, insulin and the counterregulatory responses in normally fed rats at the end of the infusion period (t=90), plotted against the administered insulin dose (x‐axis). Glucose levels (○) are plotted against the left y‐axis, insulin and the counter‐regulatory responses (●) to the right y‐axis. Such a precise regulation of blood glucose independent of the insulin dose requires a fast recognition of an upcoming insulin‐induced hypoglycemia. In the current study it was demonstrated that the glucagon response was very rapid and in the appropriate magnitude to slow down the decline in glucose. It means that the body had somehow activated the counterregulatory responses appropriately already before glucose levels were significantly affected. Such a “feed‐forward” system for the tight regulation of glucose levels during insulin‐induced hypoglycemia needs another factor than blood glucose levels to determine
27

Chapter 2 – Insulin levels and fasting
the magnitude of the required counterregulatory responses. The obvious candidate is plasma insulin, which did reach different levels in the different groups. It has been reported earlier that, at similar glucose levels, higher insulin levels lead to higher responses (18). Also supportive of this is the finding that treatment with an insulin sensitizer increases the counterregulatory responses to hypoglycemia (17). It remains to be resolved if these graded counterregulatory responses are caused by a direct effect of insulin on the counterregulatory response‐producing organs (such as the pancreas (34) or the central nervous system (1, 3, 28)), or by an indirect effect via one of the consequences of high insulin levels (such as the changes in glucose homeostasis, the suppression of endogenous insulin secretion, or a possible sensitization of glucosensing mechanisms (16, 29, 40)). Recent findings in mice lacking brain insulin receptors seem to support the former possibility (14), presumed that peripheral insulin enters the involved brain areas.
Fasting enhances all counterregulatory responses The second aim of this study was to investigate the effect of the nutritional state on the counterregulatory responses to hypoglycemia. In a fasted situation, insulin‐induced hypoglycemia might pose a bigger risk to the organism because of the already decreased glucose levels, the limited glycogen reserves, and the enhanced insulin sensitivity. The role of insulinemia in the regulation of the counterregulatory responses might also be different in the fasted state than in the fed state. These questions were studied by fasting rats for 48 hours before subjecting them to insulin‐induced hypoglycemia. Blood glucose levels were indeed significantly lower in fasted animals compared to normally fed animals. Baseline glucose levels were in the fasted rats in the range of 4‐5 mM (fed rats 6 mM), and the glucose nadir during hypoglycemia levels was around 2.0‐2.5 mM (while in the fed state around 3.5 mM). Baseline insulin levels were lower too after fasting (fasted rats 0.1‐0.4 ng/ml versus fed rats 1.9‐3.5 ng/ml). At similar insulin doses, plasma insulin levels in the fasted rats were comparable to those in the fed rats, with a tendency to being higher (at the 5.5 mU.kg‐1.min‐1 dose, fed rats reached a plasma insulin level of 4.9 ± 1.1 ng/ml while fasted rats reached 6.6 ± 1.4 ng/ml (p=0.34), at the 11 mU.kg‐1.min‐1 dose this was 10.3 ± 0.6 ng/ml versus 15.8 ± 2.8 ng/ml (p=0.07)). The major finding is that the magnitude of the counterregulatory responses was remarkably greater in fasted rats than in fed rats, despite comparable insulin levels. An example is the glucagon response in the 5.5 mU.kg‐1.min‐1 group, where glucagon rose to a peak level of 201 ± 49 pg/ml at t=30, while in the fed rats the same dose of insulin only caused a moderate increase to maximally 76 ± 5 pg/ml at t=45. Such enhanced counterregulatory responses in the fasted state were to be expected. Blood glucose was already decreased before the insulin infusion started and therefore there was a greater risk for glucose becoming so low that it impairs brain functioning. Furthermore insulin sensitivity is increased after fasting so that similar plasma insulin levels could result in stronger glucose disposal in the fasted rats. Glycogen supplies are also limited, therefore more glucagon and adrenaline might be needed to access the remaining glycogen, further stimulate gluconeogenesis, and inhibit glucose disposal. It has been
28

Chapter 2 – Insulin levels and fasting
indicated both for hypoglycemia (38) and for other metabolic challenges (35, 36) that fasting enhances the sympathoadrenal responses as well. The counterregulatory responses started earlier, too. In the fasted rats, adrenaline and corticosterone were already markedly increased within 30 minutes after the onset of insulin‐induced hypoglycemia. This is in sharp contrast to the fed rats where there were no adrenaline or corticosterone responses in the first hour. As a steroid hormone, corticosteroneʹs secretion is not rapid but depends on synthesis of new hormone rather than release of intracellular stores. Furthermore, its production needs activation of the hypothalamo‐pituitary‐adrenal axis first. Therefore the corticosterone response most likely already started when glucose levels were still around 3‐4 mM, a level which in the fed state does not result in a high corticosterone response. Since this corticosterone response in addition also occurred with low insulin doses (which resulted in lower plasma insulin levels than in the fed rats), this implies that the counterregulatory responses to hypoglycemia are not only dependent on the blood glucose levels, or the insulin levels, but that also other factors such as the nutritional state in itself determine the regulation of counterregulatory responses. A third important observation is that just like in the fed rats, different doses of insulin resulted in similar glucose levels, but with clear differences in secretion of e.g. glucagon and adrenaline (Figure 3). Therefore, the phenomenon of similar glucose nadir levels despite different insulin levels, but with different counterregulatory response levels, seems to apply in the fasted state as well. This is also illustrated in Figure 6, where the t=90 levels of glucose, insulin, and counterregulatory responses are plotted against the insulin dose. All counterregulatory responses depended on the dose of insulin (with corticosterone already reaching its maximal response at the dose of 5.5 mU.kg‐1.min‐1). These correlations are very similar to those in the fed state, except that the glucagon and noradrenaline t=90 response levels now kept increasing with increasing insulin dose, again suggesting that hypoglycemia in the fasted state indeed poses a bigger risk to the organism.
Summary In summary, it appears that both in the fed and in the fasted state blood glucose levels are defended at or above a certain level, despite large amounts of infused insulin. The counterregulatory responses are however greater with larger amounts of insulin, and it is suggested that the magnitude of the counterregulatory responses is adjusted to keep blood glucose above this certain level. From the data it appears that the activation and magnitude of the counterregulatory responses controlling glucose levels during hypoglycemia are determined by multiple factors, including at least glucose levels, insulin levels, and the nutritional state. Also the hierarchy between the counterregulatory responses, with glucagon coming first and adrenaline later and/or at higher insulin doses, might be influenced by these factors. Such a complicated regulatory system may also mean that the later responses may serve as backup for the former, and that impairing one counterregulatory response will lead to stronger activation of the others. Combined, these findings suggest that hypoglycemia is not an absolute but a relative state, and its effects and severity depend on several separate factors, including the glucose level, the insulin level, and the availability of other energy sources. It remains to be resolved
29

Chapter 2 – Insulin levels and fasting
how these factors are integrated by the neuronal systems controlling the counterregulatory responses to insulin‐induced hypoglycemia.
0 5 10 15 20 250
2
4
6
8
t=90
glu
cose
(mM
)
0
250
500
750
1000
t=90
nor
adre
nalin
(pg/
ml)
0 5 10 15 20 250
2
4
6
8
t=90
glu
cose
(mM
)
0
25
50
75
100
t=90
insu
lin (n
g/m
l)
0 5 10 15 20 25
insulin dose (mU/kg.min)
0
2
4
6
8
t=90
glu
cose
(mM
)
0
1000
2000
3000
4000
5000
t=90
adr
enal
ine
(pg/
ml)
0 5 10 15 20 250
2
4
6
8
t=90
glu
cose
(mM
)
0
20
40
60
80
100
t=90
cor
ticos
tero
ne (µ
g/dl
)
0 5 10 15 20 250
2
4
6
8
t=90
glu
cose
(mM
)
0
100
200
300
400
500
600
t=90
glu
cago
n (p
g/m
l)
Figure 6. Final levels of glucose, insulin and the counterregulatory responses in 48h fasted rats at the end of the infusion period (t=90), plotted against the administered insulin dose (x‐axis). Glucose levels (○) are plotted against the left y‐axis, insulin and the counterregulatory responses (●) to the right y‐axis.
30

Chapter 2 – Insulin levels and fasting
References 1. J.L. Beverly, M.G. De Vries, S.D. Bouman, and L.M. Arseneau; Noradrenergic and
GABAergic systems in the medial hypothalamus are activated during hypoglycemia. American Journal of Physiology (2001) 280: R563‐R569
2. M.A. Borg, R.S. Sherwin, W.P. Borg, W.V. Tamborlane, and G.I. Shulman; Local ventromedial hypothalamus glucose perfusion blocks counterregulation during systemic hypoglycemia in awake rats. Journal of Clinical Investigation (1997) 99: 361‐365
3. F.T.J. Boyd, D.W. Clarke, T.F. Muther, and M.K. Raizada; Insulin receptors and insulin modulation of norepinephrine uptake in neuronal cultures from rat brain. Journal of Biological Chemistry (1985) 260: 15880‐15884
4. P.J. Boyle and J. Zrebiec; Physiological and behavioral aspects of glycemic control and hypoglycemia in diabetes. Southern Medical Journal (2007) 100: 175‐182
5. V.J. Briscoe and S.N. Davis; Hypoglycemia in Type 1 and Type 2 diabetes: physiology, pathophysiology, and management. Clinical Diabetes (2006) 24: 115‐121
6. P.E. Cryer; Symptoms of hypoglycemia, thresholds for their occurrence, and hypoglycemia unawareness. Endocrinology and Metabolism Clinics of North America (1999) 28: 495‐500
7. P.E. Cryer; Hierarchy of physiological responses to hypoglycemia: relevance to clinical hypoglycemia in type I (insulin dependent) diabetes mellitus. Hormone and Metabolic Research (1997) 29: 92‐96
8. S.N. Davis and A.D. Cherrington; The hormonal and metabolic responses to prolonged hypoglycemia. Journal of Laboratory and Clinical Medicine (1993) 121: 21‐31
9. S.N. Davis, R.E. Goldstein, J. Jacobs, L. Price, R. Wolfe, and A.D. Cherrington; The effects of differing insulin levels on the hormonal and metabolic response to equivalent hypoglycemia in normal humans. Diabetes (1993) 42: 263‐272
10. S.N. Davis, R.E. Goldstein, L. Price, J. Jacobs, and A.D. Cherrington; The effects of insulin on the counterregulatory response to equivalent hypoglycemia in patients with insulin‐dependent diabetes mellitus. Journal of Clinical Endocrinology & Metabolism (1993) 77: 1300‐1307
11. R. Dawson Jr., P. Kontur, and A. Monjan; High‐performance liquid chromatography (HPLC) separation and quantitation of endogenous glucocorticoids after solid‐phase extraction from plasma. Hormone Research (1984) 20: 89‐94
12. M.P. Diamond, L. Hallarman, K. Starick‐Zych, T.W. Jones, M. Connolly‐Howard, W.V. Tamborlane, and R.S. Sherwin; Suppression of counterregulatory hormone response to hypoglycemia by insulin per se. Journal of Clinical Endocrinology & Metabolism (1991) 72: 1388‐1390
13. R.L. Dobbins, C.C. Connolly, D.W. Neal, L.J. Palladino, A.F. Parlow, and A.D. Cherrington; Role of glucagon in countering hypoglycemia induced by insulin infusion in dogs. American Journal of Physiology (1991) 261: E773‐E781
14. S.J. Fisher, J.C. Bruning, S. Lannon, and C.R. Kahn; Insulin signaling in the central nervous system is critical for the normal sympathoadrenal response to hypoglycemia. Diabetes (2005) 54: 1447‐1451
31

Chapter 2 – Insulin levels and fasting
15. R.T. Frizzell, G.K. Hendrick, L.L. Brown, D.B. Lacy, E.P. Donahue, R.K. Carr, P.E. Williams, A.F. Parlow, R.W. Stevenson, and A.D. Cherrington; Stimulation of glucose production through hormone secretion and other mechanisms during insulin‐induced hypoglycemia. Diabetes (1988) 37: 1531‐1541
16. B. Fruehwald‐Schultes, W. Kern, J. Born, H.L. Fehm, and A. Peters; Comparison of the inhibitory effect of insulin and hypoglycemia on insulin secretion in humans. Metabolism (2000) 49: 950‐953
17. I. Gabriely, R. Wozniak, M. Hawkins, and H. Shamoon; Troglitazone amplifies counterregulatory responses to hypoglycemia in nondiabetic subjects. Journal of Clinical Endocrinology & Metabolism (2001) 86: 521‐528
18. P. Galassetti and S.N. Davis; Effects of insulin per se on neuroendocrine and metabolic counter‐regulatory responses to hypoglycaemia. Clinical Science (2000) 99: 351‐362
19. J.E. Gerich, J. Davis, M. Lorenzi, R. Rizza, N. Bohannon, J. Karam, S. Lewis, R. Kaplan, T. Schultz, and P.E. Cryer; Hormonal mechanisms of recovery from insulin‐induced hypoglycemia in man. American Journal of Physiology (1979) 236: E380‐E385
20. P.J. Havel, S.J. Parry, J.S. Stern, J.O. Akpan, R.L. Gingerich, G.J. Taborsky, and D.L. Curry; Redundant parasympathetic and sympathoadrenal mediation of increased glucagon secretion during insulin‐induced hypoglycemia in conscious rats. Metabolism (1994) 43: 860‐866
21. R.P. Hoffman; Sympathetic mechanisms of hypoglycemic counterregulation. Current Diabetes Reviews (2007) 3: 185‐193
22. W.S. Hoffmann; A rapid method for the determination of glucose in blood and urine. Journal of Biological Chemistry (1937) 120: 51‐55
23. K. Hojlund, M. Wildner‐Christensen, O. Eshoj, C. Skjaerbaek, J.J. Holst, O. Koldkjaer, D.M. Jensen, and H. Beck‐Nielsen; Reference intervals for glucose, beta‐cell polypeptides, and counterregulatory factors during prolonged fasting. American Journal of Physiology (2001) 280: E50‐E58
24. D. Kerr, M. Reza, N. Smith, and B.A. Leatherdale; Importance of insulin in subjective, cognitive, and hormonal responses to hypoglycemia in patients with IDDM. Diabetes (1991) 40: 1057‐1062
25. I. Lager; The insulin‐antagonistic effect of the counterregulatory hormones. Journal of Internal Medicine Supplement (1991) 735: 41‐48
26. B.E. Levin and A.C. Sullivan; Glucose, insulin and sympathoadrenal activation. Journal of the Autonomic Nervous System (1987) 20: 233‐242
27. A. Mitrakou, C. Ryan, T. Veneman, M. Mokan, T. Jenssen, I. Kiss, J. Durrant, P.E. Cryer, and J. Gerich; Hierarchy of glycemic thresholds for counterregulatory hormone secretion, symptoms, and cerebral dysfunction. American Journal of Physiology (1991) 260: E67‐E74
28. M.S. Muntzel, D.A. Morgan, A.L. Mark, and A.K. Johnson; Intracerebroventricular insulin produces nonuniform regional increases in sympathetic nerve activity. American Journal of Physiology (1994) 267: R1350‐R1355
29. N.E. Rawson, H. Blum, M.D. Osbakken, and M.I. Friedman; Hepatic phosphate trapping, decreased ATP, and increased feeding after 2,5‐anhydro‐D‐mannitol. American Journal of Physiology (1994) 266: R112‐R117
32

Chapter 2 – Insulin levels and fasting
30. F. Smedes, J.C. Kraak, and H. Poppe; Simple and fast solvent extraction system for selective and quantitative isolation of adrenaline, noradrenaline and dopamine from plasma and urine. Journal of Chromatography (1982) 231: 25‐39
31. A.B. Steffens; A method for frequent sampling of blood and continuous infusion of fluids in the rat without disturbing the animal. Physiology & Behavior (1969) 4: 833‐836
32. J.H. Strubbe, J.E. Bruggink, and A.B. Steffens; Hepatic portal vein cannulation for infusion and blood sampling in freely moving rats. Physiology & Behavior (1999) 65: 885‐887
33. J.H. Strubbe and A.J.A. Prins; Reduced insulin secretion after short‐term food deprivation in rats plays a key role in the adaptive interaction of glucose and free fatty acid utilization. Physiology & Behavior (1986) 37: 441‐445
34. G.J. Taborsky, B. Ahren, and P.J. Havel; Autonomic mediation of glucagon secretion during hypoglycemia. Implications for impaired alpha‐cell responses in type 1 diabetes. Diabetes (1998) 47: 995‐1005
35. G. van Dijk; Central and peripheral mechanisms involved in fuel homeostasis. Febodruk, Enschede, 1995
36. G. van Dijk, A. Scheurink, S. Ritter, and A. Steffens; Glucose homeostasis and sympathoadrenal activity in mercaptoacetate‐treated rats. Physiology & Behavior (1995) 57: 759‐764
37. J.J. van Dongen, R. Remie, J.W. Rensema, and G.H.J. van Wunnik; Manual of microsurgery on the laboratory rat. Part I. Elsevier, Amsterdam, 1990
38. R.R. Vollmer, J.J. Balcita, A.F. Sved, and D.J. Edwards; Adrenal epinephrine and norepinephrine release to hypoglycemia measured by microdialysis in conscious rats. American Journal of Physiology (1997) 273: R1758‐R1763
39. W.W. Winder, P.S. MacLean, S.L. Chandler, W. Huang, and R.H. Mills; Role of epinephrine during insulin‐induced hypoglycemia in fasted rats. Journal of Applied Physiology (1994) 77: 270‐276
40. S.C. Woods, G.J. Taborsky, and D. Porte Jr.; Central nervous system control of nutrient homeostasis. Chapter 7, Handbook of Physiology ‐ The Nervous System IV (1984) 365‐411
33

Chapter 2 – Insulin levels and fasting
34

Chapter 3
Inhibition of fatty acid oxidation strongly potentiates the counterregulatory responses to
insulin‐induced hypoglycemia
35

36

Chapter 3 – Inhibition of fatty acid oxidation
Chapter 3 Inhibition of fatty acid oxidation strongly potentiates the counterregulatory responses to insulin‐induced hypoglycemia
These studies have been presented at the 1997 IDF Meeting in Helsinki, Finland Diabetologia (1997) volume 40 (Suppl. 1), page A237
Insulin‐induced hypoglycemia elicits a number of counterregulatory responses, depending on glucose levels. We hypothesize that the availability of fatty acids also may play a role. In the present study, the effects of inhibited fatty acid oxidation on the counterregulatory responses to insulin‐induced hypoglycemia were investigated. Rats were injected intravenously with the fatty acid oxidation blocker mercaptoacetate and subsequently infused for 90 minutes with insulin. Control animals received either mercaptoacetate or insulin. Blood samples were frequently withdrawn for determination of glucose and the counterregulatory hormones glucagon, adrenaline, noradrenaline, and corticosterone. Insulin infusion resulted in a decrease in glucose (hypoglycemia) and an increase in glucagon and corticosterone levels. Mercaptoacetate injection (lipoprivation) resulted in increases in glucose, glucagon and corticosterone levels. Combining hypoglycemia with lipoprivation decreased glucose levels to a lesser extent than in the insulin‐only control group, but significantly potentiated the glucagon and corticosterone responses and elicited strong adrenaline and noradrenaline responses. These data show that the counterregulatory responses to insulin‐induced hypoglycemia in rats are markedly enhanced when the availability of fatty acids is reduced, suggesting that the severeness of hypoglycemia does not solely depend on glucose levels but is also dependent on the availability of other energy substrates.
Introduction Injection or infusion of insulin can lead to low blood glucose levels (hypoglycemia). This may result in insufficient availability of glucose to the brain, and therefore the body produces counterregulatory responses to restore euglycemia. The counterregulatory responses to insulin‐induced hypoglycemia have been described in humans (3, 5, 6, 16) and in animals such as rats (2, 17, 39) and dogs (9, 14). In short, insulin‐induced hypoglycemia is counteracted by increased secretion of glucagon, adrenaline, noradrenaline, and corticosteroids, which all are factors that can raise glucose levels. The magnitude of these responses is dependent on the decrease in blood glucose levels (4, 24), but the nutritional state of the body has also been indicated to co‐determine the counterregulatory responses to hypoglycemia (Chapter 2). This suggests that the availability of the other key energy substrate, fatty acids, is also important for the counterregulation to hypoglycemia. Also, because most of the body tissues can use both glucose and fatty acids as fuels, it might be argued that low glucose levels are less threatening in a situation with increased fatty acid supply. Indeed it has been shown that infusion of fatty acids markedly attenuated the counterregulatory responses to insulin‐induced hypoglycemia (10). Infusions of other energy substrates such as lactate or ketone bodies also attenuate these counterregulatory responses (38). If this is indeed because excess availability of other energy substrates reduces the risk posed by hypoglycemia (and therefore attenuates the counterregulatory responses), then consequently a reduced availability of other energy substrates should do the opposite and increase the counterregulatory responses to hypoglycemia. We previously showed that a generally reduced nutritional state (48h of fasting) does increase the counterregulatory
37

Chapter 3 – Inhibition of fatty acid oxidation
responses to hypoglycemia, and presently we wanted to investigate whether fatty acids are similarly important. The aim of the present study was therefore to test the hypothesis that a reduction of fatty acid availability increases the counterregulatory responses to hypoglycemia. This was achieved by inducing hypoglycemia in rats that received an inhibitor of the fatty acid beta oxidation, thereby reducing the availability of energy from fatty acids (lipoprivation).
Methods
Animals and surgery Male Wistar rats were used, weighing 341 ± 4 grams (average ± SEM) at the beginning of the experiment. They were individually housed in 25*25*30 cm cages with wood shavings bedding. Room temperature was 21 ± 1 °C and the lights were on from 08:00 until 20:00 h. Food (standard RMH chow, Hope Farms, Woerden, The Netherlands) and water were available ad lib unless otherwise stated. The animals were frequently handled and weighed. For stress‐free blood sampling and i.v. infusions in freely‐moving animals, all rats were fitted under halothane/N2O inhalation anesthesia with two permanent silicone catheters (Medica BV, Den Bosch, The Netherlands), one for blood sampling and one for infusions. The catheters were inserted via the jugular vein, with the catheter tips ending in the superior vena cava just before the right atrium (34, 37). After surgery, the animals were allowed at least two weeks for recovery, and were habituated to the experimental conditions. The experimental procedures were approved by the Animal Experiments Committee of the University of Groningen.
Experimental design To study the importance of fatty acid oxidation during hypoglycemia, the animals were divided into three groups: two control groups, subjected to hypoglycemia alone (group H, n=8) or to lipoprivation alone (group L, n=6), and the experimental group, subjected to hypoglycemia plus lipoprivation (group HL, n=6). All experiments were performed between 10:00 and 14:00 h. Food had been removed between 08:30 and 09:30 h. Thereafter the rats’ sampling and infusion catheters were connected to polyethylene tubings, to enable remote blood sampling and intravenous infusions without disturbing the freely‐moving animals. At least one hour was allowed for the animals to get to rest again. Two blood samples were then taken with a 10‐minute interval to serve as baseline values. At t=0 all groups received a 1 ml/kg injection via the sampling catheter, group H with vehicle (0.9% NaCl), and groups L and HL with 600 μmol/kg of the fatty acid oxidation blocker mercaptoacetate (sodium thioglycolic acid, Sigma‐Aldrich Chemie, Zwijndrecht, The Netherlands) (1). At the same time an infusion was started via the infusion catheter, at a rate
38

Chapter 3 – Inhibition of fatty acid oxidation
of 3.2 ml.kg‐1.min‐1. The infusate was vehicle (0.9% NaCl) for group L, and 22 mU.kg‐1.min‐1 insulin (Velosulin, Novo Nordisk Farma, Alphen a/d Rijn, The Netherlands) for groups H and HL. This insulin dose results in moderate hypoglycemia but does not lead to adrenaline or noradrenaline responses (in this setup, a minimal dose of ~50 mU.kg‐1.min‐1 would be needed to elicit adrenaline and noradrenaline release – see Chapter 2). The mercaptoacetate dose was also based on previous studies in our laboratory (30) (36). The treatment setup is depicted in Table 1. Additional blood sampling time points were 2½, 5, 7½, 10, 15, 20, 30, 45, 60, 75 and 90 minutes, whereafter the infusion was stopped. After each sample, the same amount of heparinized blood from blood donor rats was returned to prevent diminution of blood volume with related changes in hemodynamics. Table 1. The treatment setup for the three groups: group H (hypoglycemia), group L (lipoprivation), and group HL (hypoglycemia in combination with lipoprivation). group injection at t=0 infusion from t=0 to 90 H (hypoglycemia) vehicle (1 ml/kg) insulin (22 mU.kg‐1.min‐1) L (lipoprivation) mercaptoacetate (600 μmol/kg) vehicle (3.2 ml.kg‐1.h‐1) HL (hypoglycemia + lipoprivation) mercaptoacetate (600 μmol/kg) insulin (22 mU.kg‐1.min‐1)
Determinations and analysis Blood samples were kept chilled at 0 °C during the experiment, in tubes with EDTA and aprotinin (Trasylol). Afterwards 50 μl blood was removed for glucose determination (Hoffmannʹs ferricyanide method (20)) and the remainder was centrifuged for 15 min at 2600 G and 4 °C. Plasma aliquots were stored at ‐80 °C for determination of glucagon (Glucagon RIA Kit, Linco Research Inc, St. Charles, MO, USA) and catecholamines (HPLC with electrochemical detection (33)), and at ‐20 °C for determination of corticosterone (HPLC with UV detection (7)). Results are reported as average ± SEM (standard error of the mean). Statistical differences were determined with ANOVA or t‐test (paired where relevant). The significance level was set to p<0.05.
Results Induction of hypoglycemia by intravenous infusion of insulin (group H) resulted in a decrease in blood glucose levels from a baseline level of 6.2 ± 0.2 mM (t=‐1) to a nadir of 3.6 ± 0.1 mM (t=90; p<0.0001). This was accompanied by an increase in plasma glucagon from 51 ± 2 pg/ml to 94 ± 8 pg/ml at t=15 (p=0.004), after which it remained elevated throughout the rest of the experiment (p=0.020 at t=90). Plasma adrenaline and noradrenaline levels did not change significantly. Plasma corticosterone levels increased slightly during the infusion period, from 5 ± 1 μg/dl at baseline to a final level of 12 ± 2 μg/dl (p=0.001).
39

Chapter 3 – Inhibition of fatty acid oxidation
Induction of lipoprivation by intravenous injection of mercaptoacetate (group L) resulted in an immediate increase in glucose levels from 6.2 ± 0.2 mM at baseline to 7.4 ± 0.5 mM at t=2.5 minutes (p=0.041), after which they remained elevated around 7.2 mM for the rest of the test period. Glucagon also rapidly rose, from 48 ± 5 to 83 ± 8 pg/ml at t=5 (p=0.005) and then remained on a level of approximately 70 pg/ml. Plasma adrenaline responded slightly, increasing from 8 ± 4 to a final level of 58 ± 15 pg/ml at t=90 (p=0.039).
0 30 60 900
500
1000
1500
nora
dren
alin
e (p
g/m
l)2
4
6
8
gluc
ose
(mM
)
0 30 60 90
0 30 60 9
time (min)
0
500
1000
1500
adre
nalin
e (p
g/m
l)
0 30 60 900
25
50
75
corti
cost
eron
e (µ
g/dl
)
0
50
100
150
200
gluc
agon
(pg/
ml)
0 30 60 90
0
Figure 1. Responses in blood glucose and plasma glucagon, adrenaline, noradrenaline and corticosterone levels during hypoglycemia (group H, ), lipoprivation (group L, ), or hypoglycemia together with lipoprivation (group HL, ). Hypoglycemia was induced by infusion of 22 mU.kg‐1.min‐1 insulin from t=0 to t=90 minutes, while lipoprivation was induced by injection of 600 μmol/kg of the fatty acid oxidation blocker mercaptoacetate at t=0. For illustrative purposes, the dotted lines represent the combined responses (i.e. increase from baseline) of groups H and L together.
40

Chapter 3 – Inhibition of fatty acid oxidation
Noradrenaline did not show a statistically significant response. Corticosterone increased
The combination of hypoglycemia with lipoprivation (group HL) resulted in a rapid itial i
‐
of 194
ulin and mercaptoacetate also resulted in strong
one end
ypoglycemic omaʺ) .
Discussion
We investigated whether the availability of fatty acids as an energy substrate may lay a r
ile fatty
poglycemia (group H) induced by 22 mU.kg‐1.min‐1 sulin a
to an immediate but modest
ng since
fatty acid availability with insulin‐induced hypoglycemia (group HL) led to a substantial potentiation of the counterregulatory responses: despite
from 9 ± 3 to 38 ± 1 μg/dl at t=45 and slowly fell back to a level of 34 ± 2 μg/dl at t=90 (p=0.0006). in ncrease in glucose levels identical to that of the mercaptoacetate‐group (to 7.3 ± 0.4 mM at t=2.5, p=0.040), followed by a gradual decrease towards the nadir level of the insulingroup (H), reaching 4.1 ± 0.2 mM at t=90 (p=0.0004 vs baseline, p>0.05 vs the insulin‐group). These glucose changes were accompanied by a large and very fast glucagon response, from 48 ± 3 to 90 ± 10 pg/ml within 2.5 minutes (p=0.014) and to a maximum± 14 pg/ml at t=75 (p=0.0001). The increase from baseline levels in group HL was therefore 146 ± 14 pg/ml, which is much more than the combined increases of group H and group L together (47 ± 10 pg/ml and 20 ± 8 pg/ml). The combined administration of insincreases in adrenaline levels (from 28 ± 7 to 754 ± 80 pg/ml at t=90, p=0.0002) and noradrenaline levels (from 299 ± 39 to 638 ± 79 pg/ml at t=90, p=0.0005). Corticosterincreased from 9 ± 3 to 45 ± 3 μg/dl at t=45 (p=0.003) and remained at that level until theof the infusion period. This end level was significantly higher than in the two other groups (p<0.0001 vs the insulin‐group and p=0.005 vs the mercaptoacetate‐group). One animal in this group even showed signs of neuroglycopenia (ʺhc during the experiment, despite that its blood glucose levels did not go below 4 mMIn all our studies with insulin‐induced hypoglycemia in non‐fasted rats, no animal has ever shown such signs, not even with much greater insulin doses. The animal recovered rapidly after i.v. administration of glucose after the last blood sample.
p ole in the counterregulatory responses to insulin‐induced hypoglycemia. We hypothesized that inhibition of fatty acid oxidation would increase the responses to hypoglycemia. To that end, rats were subjected to insulin‐induced hypoglycemia whacid oxidation was inhibited by mercaptoacetate. Animals treated with either insulin or mercaptoacetate served as controls. Moderate insulin‐induced hyin was counteracted by increased secretion of glucagon and a small increase in plasmcorticosterone. The absence of adrenaline and noradrenaline responses is in accordance withprevious studies in our laboratory, in which we found that higher insulin doses are needed to evoke adrenaline or noradrenaline responses (Chapter 2). Lipoprivation induced by mercaptoacetate (group L) ledincrease in glucose levels, confirming earlier studies (8, 30, 36). Lipoprivation was furthermore counteracted by increases in glucagon and corticosterone (a new findithese substances were not analyzed in those earlier studies), without any effect on sympathoadrenal activity. Combining reduced
41

Chapter 3 – Inhibition of fatty acid oxidation
h glucose levels than in the hypoglycemia‐group, it caused a strong activation of thesympathoadrenal system reflected by high plasma levels of noradrenaline and in particuadrenaline. Furthermore the plasma glucagon and corticosterone responses were higher than the sum of the responses to the individual treatments – suggesting that the enhanced responses to hypoglycemia plus lipoprivation are synergistic rather than additive. Taken together, the key finding of this study is that the counterregulatory responsesto insulin‐induced hypoglycemia are directly dependent on the availability of energ
igher lar
y from
tty ac
from the above that lipoprivation will affect the counterregulation to ypoglycemia. It should be noted that the increased counterregulatory responses to
se ffect of
duce
d
two energy sources leads to ynergistically increased responses is not new. Previous data have shown that combining a tty ac ed
s
. Hypoglycemia (or glucoprivation) is detected in everal
increased
duction in both fuels (or total energy status) nd syn ain
fa ids. It is clearhhypoglycemia when accompanied by lipoprivation cannot be explained by blood glucolevels, since these were less reduced than in the hypoglycemia‐only group. A direct emercaptoacetate itself on the pancreatic alpha cells or the adrenal medulla can be excludedtoo, since inhibition of fatty acid oxidation alone did not elicit large responses in glucagon or adrenaline. Our study results thereby support the existence of a link between the counterregulation to hypoglycemia and the counterregulation to lipoprivation. Especially our observation that neither hypoglycemia nor lipoprivation alone were able to insignificant adrenaline or noradrenaline responses – whereas the combination of the two did– is in strong support of this. Also the fact that all counterregulatory hormones respondewith a magnitude greater than the sum of the responses of the two control groups, indicates that the body is able to dissociate hypoglycemia from lipoprivation and adjust counterregulation when both happen simultaneously. The notion that combined reduced availability ofsfa id oxidation inhibitor with a glucose oxidation inhibitor synergistically increasfood intake (13, 27). This synergistic increase in counterregulation has however only been described for the eating response, and not for hormonal counterregulatory responses, as habeen shown now in the present study. The mechanistic basis for where and how this synergy and the integration of the two signals takes place is still to be resolveds sites in the body: the liver and hepatic portal vein area (19, 25), the hypothalamus (2, 23, 29), and the brain stem (15). It is counteracted by increased levels of glucagon, adrenaline, and corticosterone. Lipoprivation is detected in the liver, which then by vagal afferents activates the autonomic nervous system (22, 28, 30). It is counteracted by levels of glucose, glucagon, and corticosterone. The liver may play an essential role in the integration of the glucoprivic and lipoprivic signals, because it may respond to a rea ergistically increase the afferent hepatic vagal signal (12, 21). However the brseems to be the better candidate because it is able to integrate the lipoprivic signal arising from afferent vagal liver nerves with a glucoprivic signal arising from within the brain. Incontrast to the liver, the brain therefore has access to different neuronal networks for different energy substrates (30). In support of the latter, it has been shown that glucoprivation and lipoprivation do activate different neuropeptide systems in the hypothalamus (31).
42

Chapter 3 – Inhibition of fatty acid oxidation
It can also be argued that both the sensory and the integrating processes takethe level of the centr
place at al nervous system, with brain cells that are sensitive to multiple energy
uses d
that one of eiving
acid oxidation synergistically augments the ounterregulatory responses to insulin‐induced hypoglycemia, despite a lesser decrease in lucose to
eferences
he, D. Sabourault, Y. Giudicelli, J. Nordmann, and R. Nordmann; 2‐Mercaptoacetate administration depresses the beta‐oxidation pathway through an
urnal
2. halamus glucose perfusion blocks counterregulation during
361‐
3. iology, pathophysiology, and management. Clinical Diabetes (2006) 24: 115‐121
d
5. e I (insulin dependent) diabetes mellitus. Hormone and
6. Laboratory and Clinical Medicine (1993) 121: 21‐
7. LC) separation and quantitation of endogenous glucocorticoids after solid‐phase
substrates. It is known that both ketone bodies and lactate may serve as fuels for the brain (18, 26), and it has been shown that infusion of these energy substrates can decrease counterregulation to hypoglycemia (11, 35, 38), suggesting that the brain may be less responsive to hypoglycemia when other energy substrates are abundant. If the brain fatty acids as an energy source as well (32), then even lipoprivation may also be sensewithin the brain itself, independently from afferent signals from the liver – and if mercaptoacetate affects fatty acid oxidation in the brain, this could help explain the observations in the present study. This could also be indicated by the observation the rats in the HL group showed signs of neuroglucopenia, while none of the rats recinsulin or mercaptoacetate alone did. In summary, reduction of fattycg levels. From this it may be concluded that the counterregulatory responses hypoglycemia necessary to avoid central energy deficiency are directly dependent on the availability of energy from fatty acids.
R 1. F. Bauc
inhibition of long‐chain acyl‐CoA dehydrogenase activity. Biochemistry Jo(1981) 196: 803‐809 M.A. Borg, R.S. Sherwin, W.P. Borg, W.V. Tamborlane, and G.I. Shulman; Local ventromedial hypotsystemic hypoglycemia in awake rats. Journal of Clinical Investigation (1997) 99: 365 V.J. Briscoe and S.N. Davis; Hypoglycemia in Type 1 and Type 2 diabetes: phys
4. P.E. Cryer; Symptoms of hypoglycemia, thresholds for their occurrence, anhypoglycemia unawareness. Endocrinology and Metabolism Clinics of North America (1999) 28: 495‐500 P.E. Cryer; Hierarchy of physiological responses to hypoglycemia: relevance toclinical hypoglycemia in typMetabolic Research (1997) 29: 92‐96 S.N. Davis and A.D. Cherrington; The hormonal and metabolic responses to prolonged hypoglycemia. Journal of31 R. Dawson Jr., P. Kontur, and A. Monjan; High‐performance liquid chromatography (HPextraction from plasma. Hormone Research (1984) 20: 89‐94
43

Chapter 3 – Inhibition of fatty acid oxidation
8. E. Del Prete, T.A. Lutz, and E. Scharrer; Effects of mercaptoacetate on feeding, circulating glucose and lipids, and gastric emptying in rats fed a carbohydrate‐ free high‐fat diet. Nutritional Neuroscience (2001) 4: 239‐250
9. R.L. Dobbins, C.C. Connolly, D.W. Neal, L.J. Palladino, A.F. Parlow, and A.D. Cherrington; Role of glucagon in countering hypoglycemia induced by insulin infusion in dogs. American Journal of Physiology (1991) 261: E773‐E781
10. M.L. Evans, K. Matyka, J. Lomas, A. Pernet, I.C. Cranston, I. Macdonald, and S.A. Amiel; Reduced counterregulation during hypoglycemia with raised circulating nonglucose lipid substrates: evidence for regional differences in metabolic capacity in the human brain? Journal of Clinical Endocrinology & Metabolism (1998) 83: 2952‐2959
11. J.P. Flatt, G.L. Blackburn, G. Randers, and J.B. Stanbury; Effects of ketone body infusion on hypoglycemic reaction in postabsorptive dogs. Metabolism (1974) 23: 151‐158
12. M.I. Friedman, C.C. Horn, and H. Ji; Peripheral signals in the control of feeding behavior. Chemical Senses (2005) 30: I182‐i183
13. M.I. Friedman, M.G. Tordoff, and I. Ramirez; Integrated metabolic control of food intake. Brain Research Bulletin (1986) 17: 855‐859
14. R.T. Frizzell, G.K. Hendrick, L.L. Brown, D.B. Lacy, E.P. Donahue, R.K. Carr, P.E. Williams, A.F. Parlow, R.W. Stevenson, and A.D. Cherrington; Stimulation of glucose production through hormone secretion and other mechanisms during insulin‐induced hypoglycemia. Diabetes (1988) 37: 1531‐1541
15. R.T. Frizzell, E.M. Jones, S.N. Davis, D.W. Biggers, S.R. Myers, C.C. Connolly, D.W. Neal, J.B. Jaspan, and A.D. Cherrington; Counterregulation during hypoglycemia is directed by widespread brain regions. Diabetes (1993) 42: 1253‐1261
16. J.E. Gerich, J. Davis, M. Lorenzi, R. Rizza, N. Bohannon, J. Karam, S. Lewis, R. Kaplan, T. Schultz, and P.E. Cryer; Hormonal mechanisms of recovery from insulin‐induced hypoglycemia in man. American Journal of Physiology (1979) 236: E380‐E385
17. P.J. Havel, S.J. Parry, J.S. Stern, J.O. Akpan, R.L. Gingerich, G.J. Taborsky, and D.L. Curry; Redundant parasympathetic and sympathoadrenal mediation of increased glucagon secretion during insulin‐induced hypoglycemia in conscious rats. Metabolism (1994) 43: 860‐866
18. R.A. Hawkins and J.F. Biebuyck; Ketone bodies are selectively used by individual brain regions. Science (1979) 205: 325‐327
19. A.L. Hevener, R.N. Bergman, and C.M. Donovan; Portal vein afferents are critical for the sympathoadrenal response to hypoglycemia. Diabetes (2000) 49: 8‐12
20. W.S. Hoffmann; A rapid method for the determination of glucose in blood and urine. Journal of Biological Chemistry (1937) 120: 51‐55
21. H. Ji, G. Graczyk‐Milbrandt, and M.I. Friedman; Metabolic inhibitors synergistically decrease hepatic energy status and increase food intake. American Journal of Physiology (2000) 278: R1579‐R1582
22. W. Langhans and E. Scharrer; Evidence for a vagally mediated satiety signal derived from hepatic fatty acid oxidation. Journal of the Autonomic Nervous System (1987) 18: 13‐18
23. B.E. Levin; Glucosensing neurons: The metabolic sensors of the brain? Diabetes, Nutrition and Metabolism ‐ Clinical and Experimental (2002) 15: 274‐281
44

Chapter 3 – Inhibition of fatty acid oxidation
24. A. Mitrakou, C. Ryan, T. Veneman, M. Mokan, T. Jenssen, I. Kiss, J. Durrant, P.E. Cryer, and J. Gerich; Hierarchy of glycemic thresholds for counterregulatory hormone secretion, symptoms, and cerebral dysfunction. American Journal of Physiology (1991) 260: E67‐E74
25. D. Novin, D.A. Vanderweele, and M. Rezek; Hepatic portal 2‐deoxy‐D‐glucose infusion causes eating: Evidence for peripheral glucoreceptors. Science (1973) 181: 858‐860
26. L. Pellerin; How astrocytes feed hungry neurons. Molecular Neurobiology (2005) 32: 59‐72
27. N.E. Rawson, P.M. Ulrich, and M.I. Friedman; Fatty acid oxidation modulates the eating response to the fructose analogue 2,5‐anhydro‐D‐mannitol. American Journal of Physiology (1996) 271: R144‐R148
28. S. Ritter and J.S. Taylor; Vagal sensory neurons are required for lipoprivic but not glucoprivic feeding in rats. American Journal of Physiology (1990) 258: R1395‐R1401
29. V. Routh, Z. Song, and X. Liu; The role of glucosensing neurons in the detection of hypoglycemia. Diabetes Technology and Therapeutics (2004) 6: 413‐421
30. A. Scheurink and S. Ritter; Sympathoadrenal responses to glucoprivation and lipoprivation in rats. Physiology & Behavior (1993) 53: 995‐1000
31. V.G. Sergeev and I.G. Akmaev; Effects of blockers of carbohydrate and lipid metabolism on expression of mRNA of some hypothalamic neuropeptides. Bulletin of Experimental Biology and Medicine (2000) 130: 766‐768
32. H. Singh, S. Usher, and A. Poulos; Mitochondrial and peroxisomal beta‐oxidation of stearic and lignoceric acids by rat brain. Journal of Neurochemistry (1989) 53: 1711‐1718
33. F. Smedes, J.C. Kraak, and H. Poppe; Simple and fast solvent extraction system for selective and quantitative isolation of adrenaline, noradrenaline and dopamine from plasma and urine. Journal of Chromatography (1982) 231: 25‐39
34. A.B. Steffens; A method for frequent sampling of blood and continuous infusion of fluids in the rat without disturbing the animal. Physiology & Behavior (1969) 4: 833‐836
35. E.M. Stricker, N. Rowland, C.F. Saller, and M.I. Friedman; Homeostasis during hypoglycemia: central control of adrenal secretion and peripheral control of feeding. Science (1977) 196: 79‐81
36. G. van Dijk, A. Scheurink, S. Ritter, and A. Steffens; Glucose homeostasis and sympathoadrenal activity in mercaptoacetate‐treated rats. Physiology & Behavior (1995) 57: 759‐764
37. J.J. van Dongen, R. Remie, J.W. Rensema, and G.H.J. van Wunnik; Manual of microsurgery on the laboratory rat. Part I. Elsevier, Amsterdam, 1990
38. T. Veneman, A. Mitrakou, M. Mokan, P.E. Cryer, and J. Gerich; Effect of hyperketonemia and hyperlacticacidemia on symptoms, cognitive dysfunction, and counterregulatory hormone responses during hypoglycemia in normal humans. Diabetes (1994) 43: 1311‐1317
39. W.W. Winder, P.S. MacLean, S.L. Chandler, W. Huang, and R.H. Mills; Role of epinephrine during insulin‐induced hypoglycemia in fasted rats. Journal of Applied Physiology (1994) 77: 270‐276
45

Chapter 3 – Inhibition of fatty acid oxidation
46

Section II – Central nervous mechanisms
The hypothalamus is one of the most important parts of the brain, involved in many kinds of motivation, among other functions.
It controls the Four Fʹs: 1) fighting; 2) fleeing; 3) feeding; and 4) mating. ‐ unknown psychology professor in neuropsychology intro course
47

48

Chapter 4
Noradrenergic and GABAergic systems in the medial hypothalamus are activated during
hypoglycemia
49

50

Chapter 4 – Noradrenergic responses in the hypothalamus
Chapter 4 Noradrenergic and GABAergic systems in the medial hypothalamus are activated during hypoglycemia J.L. Beverly, M.G. de Vries, S.D. Bouman, L.M. Arseneau; American Journal of Physiology (2001) volume 280, pages R563‐R569 Noradrenergic and GABAergic systems in the medial hypothalamus influence plasma glucose and may be activated during glucoprivation. Microdialysis probes were placed into the ventromedial nucleus (VMH), lateral hypothalamus (LHA), and paraventricular nucleus (PVH) of male Sprague‐Dawley rats to monitor extracellular concentrations of norepinephrine (NE) and GABA. During systemic hypoglycemia, induced by insulin (1.0 U/kg), NE concentrations increased in the VMH and PVH in a bimodal fashion during the first 10 min and 20–30 min after insulin administration. In the VMH, GABA concentrations increased in a similar manner as NE. Extracellular NE concentrations in the LHA were slightly lower, and GABA levels remained at baseline. The increases in NE and GABA in the VMH were absent during euglycemic clamp; however, NE in the PVH still increased, reflecting a direct response to hyperinsulinemia. On the basis of these data, we propose that the activity of noradrenergic afferents to the medial hypothalamus is increased during hypoglycemia and influences the activity of local GABAergic systems to activate appropriate physiological compensatory mechanisms.
The ventral hypothalamus The ventral hypothalamus is a critical brain area for maintaining plasma glucose concentrations. This brain area influences the activity of parts of the sympathetic nervous system that directly affect glycemic state (17, 38). Within the ventromedial portion of the hypothalamus (VMH), the firing rates of some neurons are influenced by glucose availability and affect the activity of the sympathetic nervous system (23, 28). Lesions to the VMH abolished compensatory responses to systemic hypoglycemia (6), and confining glucoprivation to the VMH by direct application of the glucose analog 2‐deoxy‐D‐glucose (2‐DG), increased plasma concentrations of epinephrine, norepinephrine, and glucagon (7). Conversely, maintaining glucose levels within the VMH during systemic hypoglycemia reduced the hypoglycemia‐associated increases in plasma catecholamines and glucagon (5). Noradrenergic systems in the hypothalamus are likely to be involved in compensatory responses to glucoprivation. During hypoglycemia, increased norepinephrine (NE) turnover in the mediobasal hypothalamus, which includes the VMH, has been consistently described (1, 29, 37). The influence of noradrenergic systems in the VMH in glucose regulation is well established. Concentrations of glucose and glucose‐mobilizing hormones in the circulation are increased in response to application of NE into the VMH (8, 30, 38). Studies using microdialysis or push‐pull perfusion to directly measure extracellular NE in the VMH during hypoglycemia are less consistent. Using microdialysis probes in the VMH, Shimizu and Bray (33) reported an increase in extracellular NE 30‐60 min after systemic hypoglycemia, yet no change in NE release to insulin was identified using push‐pull perfusion (18). Several studies measuring tissue content of NE and its metabolites reported increased NE turnover in the VMH after a glucoprivic episode induced by 2‐DG (27, 36, 37). In response to a 2‐DG‐induced glucoprivic challenge, concentrations of the
51

Chapter 4 – Noradrenergic responses in the hypothalamus
neurotransmitter GABA and NE were increased in the VMH (2, 3). The increase in NE was reported to mediate the increase in GABA after 2‐DG (3). The first objective of the present study was to characterize noradrenergic activity and GABAergic activity in discrete hypothalamic areas during a period of hypoglycemia. Microdialysis probes were used to monitor NE or GABA synaptic overflow in the VMH, the adjacent lateral hypothalamic area (LHA), and paraventricular nucleus (PVH) of rats during a period of insulin‐induced hypoglycemia. A euglycemic clamp procedure was used to differentiate the responses to hypoglycemia from hyperinsulinemia. The results were similar to those observed after 2‐DG‐induced glucoprivation. Extracellular NE and GABA concentrations in the VMH were increased during hypoglycemia and followed the same profile measured after 2‐DG.
Research design and methods This study was approved by the Laboratory Animal Care Advisory Committee of the University of Illinois. Male Sprague‐Dawley rats, ~250 g, were housed singly in Plexiglas cages (30 x 30 x 38 cm) in a light (12:12‐h light‐dark cycle; lights on at 0700)‐ and temperature (26 ± 2°C)‐controlled room. Fresh water and rodent diet (Harlan Teklabs, Madison, WI) were available at all times, except during sample collection.
Surgical procedures After a 1‐wk acclimation period, rats were anesthetized with a mixture of ketamine HCl, xylazine HCl, and acepromazine (30:6:1 mg/kg im). The level of anesthesia was monitored and maintained at an appropriate level throughout the surgical procedure. The top of the head and the neck of each rat were shaved, and the skin was washed with povidone‐iodine 10% (Betadine). A jugular vein catheter was aseptically placed through a vertical incision in the neck. The right external jugular vein was isolated, and a 4‐cm segment of Silastic tubing (0.025 in. ID x 0.047 in. OD) was inserted toward the heart. The catheter was secured with 5‐0 suture, tunneled under the skin, and exteriorized through an incision on top of the head before the skin in the neck was closed with wound staples. Some animals also received a femoral vein catheter. A section of the left femoral vein was isolated, and a 1‐cm segment of Silastic tubing (0.020 in. ID x 0.035 in. OD) was inserted into the vein, tunneled under the skin, and exteriorized through the incision on top of the head. The incision on the lower abdomen was closed with wound staples. A piece of 21‐ or 23‐gauge stainless steel tubing was inserted onto the end of each catheter, and the catheters were filled with a 40% polyvinylpyrrolidone (PVP) solution containing 500 U heparin/ml and capped with a sealed piece of Tygon tubing to maintain patency. The rat was placed into a stereotaxic instrument (ASI Instruments, Warren, MI), and a guide cannula was positioned 1 mm dorsal to the sample site using the stereotaxic atlas of Paxinos and Watson (26). Coordinates for sample sites were VMH [anterior‐posterior (AP) = 6.6, lateral (L) = 0.8, dorsal (D) = 9.6 below dura], LHA (AP = 6.6, L = 1.8, D = 8.8 below dura), or PVH (AP = 7.2, L = 0.6, D = 8.2 below dura). In the VMH, probes were placed into the lateral edge of the anterior portion of the VMH immediately anterior to the perifornical nucleus. The same
52

Chapter 4 – Noradrenergic responses in the hypothalamus
rostrocaudal coordinates were used to place probes in the LHA lateral to the fornix. In the PVH, probes were placed to sample from both magnocellular and parvocellular regions. The guide cannula and end of venous catheters were fixed in position with dental acrylic cement and anchored to the skull with four stainless steel screws (Small Parts, Miami Beach, FL). After surgery, rats were monitored until they had completely recovered from the anesthetic. Postsurgical analgesia was provided by butorphanol (0.5 mg/kg sc; Torbuterol).
Sample collection Rats were allowed a 7‐ to 10‐day recovery period after surgery, and only animals with body weights greater than on the day of surgery were used. Blood and dialysate samples were collected from unrestrained animals in their home cages using a weighted counterbalance lever with liquid swivel (Instech, Plymouth Meeting, PA) during the mid‐light phase. Experiments were conducted during the mid‐light phase to minimize possible confounding diurnal‐associated changes in behavior or neurochemical activity in the ventral hypothalamus. Before each experiment, the in vitro recoveries of 0.20 x 1‐mm microdialysis probes were determined before probes were placed into the VMH, LHA, or PVH. To minimize the effect of tissue disruption at the sampling site, probes were in place at least 3 h before samples were collected. The probes were connected through a liquid swivel to a 1‐ml gas‐tight syringe on a microinfusion pump (Bioanalytical Systems, West Lafayette, IN) and continuously perfused with Krebs‐Ringer buffer (in mM: 147 NaCl, 4 KCl, 3.4 CaCl2; pH 6.4) at 1‐2 μl/min. Dialysate was collected into microtubes attached near the swivel and frozen at ‐84°C until assayed for GABA or catecholamines. The PVP‐heparin solution was flushed from catheters before a 30‐ to 40‐cm length of Tygon tubing filled with sterile 0.9% saline was attached to the stainless steel tubing at the end of the catheter. Dialysate samples were collected at 10‐min intervals into microtubes and immediately frozen at the end of each sample period and maintained at ‐84° C until assayed. Samples for catecholamine analysis were collected into microtubes containing 0.2 μl 0.1 N perchloric acid. Blood samples (~20 μl) were collected at regular intervals, and plasma glucose concentration was measured on a handheld glucose monitor (Boehringer Manheim).
Effect of insulin‐induced hypoglycemia on NE and GABA To establish basal concentrations of NE and GABA, three 10‐min dialysate samples were collected before 1.0 U/kg regular insulin (Humulin®, Eli Lilly, Indianapolis, IN) was infused into the jugular vein catheter (n = 6‐8 rats per brain area). The insulin was diluted in sterile saline and delivered at a volume of 1 ml/kg body wt (n = 5 rats per brain area). An equal volume of sterile saline was used as a control. Dialysates were collected at 10‐min intervals over the next 60 min. Blood glucose concentrations were determined at the midpoint of each 10‐min sample. Separate animals were used for analysis of NE and GABA. To distinguish whether the responses in NE and GABA were due to hypoglycemia or hyperinsulinemia, a euglycemic clamp procedure was used. Baseline neurotransmitter and plasma glucose concentrations were determined as in the first experiment. After the third baseline sample was collected and 3‐5 min before administering 1.0 U/kg regular insulin (Humulin®), sterile saline or a 20% glucose solution (in sterile saline) was infused into the
53

Chapter 4 – Noradrenergic responses in the hypothalamus
femoral vein at a constant rate (20 μl/min). Blood glucose levels were checked at 2‐min intervals for the next 30 min, then at 5‐min intervals until the end of the study. The infusion rate of the glucose solution (or saline) was adjusted to maintain blood glucose concentrations near baseline for 60 min after insulin infusion. Dialysate samples were collected at 10‐min intervals for 90 min after insulin administration. At the end of the experiments, rats were anesthetized, and the heart was exposed. The right auricle was punctured, and ~60 ml of chilled saline followed by ~60 ml of 10% formalin solution was perfused through the brain via the left ventricle. The formalin‐fixed brain was removed from the skull, and intrahypothalamic cannula position was verified histologically.
Sample analysis Catecholamines were analyzed on a Dynamax SD‐200 system (Varian Instruments, Woburn, MA) by reverse‐phase HPLC and electrochemical detection. Samples (5‐10 μl) were injected onto a 150 x 2‐mm C18 (3 μm) Hypersil column fitted with a 2‐mm C18 (3 μm) Hypersil javelin guard column (Keystone Scientific, Bellfonte, PA). Mobile phase (pH 3.0) was 75 mM NaH2PO4, 1.7 mM L‐octanesulfonic acid, 25 μM Na2EDTA, 10% (vol/vol) acetonitrile, and 0.1% (vol/vol) tetrahydrofuran. A DECADE electrochemical detector fitted with a VT‐03 glassy carbon electrode (Antec Leyden, Leiden, The Netherlands) set at +0.75 V was used with Dynamax MacIntegrator II and ʺCʺ module programs (Rainin Instruments, Woburn, MA) for peak integration and quantification. With this method, sensitivity for dialysate samples (peak height twice baseline) was 0.1 nM, with an interassay coefficient of variation of ≤3%. GABA was analyzed on a BAS 480 Analyzer (Bioanalytical Systems) by a reverse‐phase HPLC method, using a modified isocratic procedure (2). Sample (20 μl) was mixed with 2.5 μl of derivatization reagent [11 mg O‐phthaldialdehyde in 5 ml of a 0.1 M sodium borate buffer (pH 9.2) containing 5% methanol and 250 μl of 0.03 M sodium sulfite] and heated at 35°C for 5 min before injection onto a 100 x 4‐mm C18 (3 μm) reverse‐phase Microsorb column and 5 x 4‐mm C18 guard column (Varian Instruments). Mobile phase (pH 5.0) was 0.1 M sodium phosphate buffer containing 0.1 mM EDTA and 15% (vol/vol) methanol. Quantitation was by electrochemical detection (BAS LC‐4C, Bioanalytical Systems), using a glassy carbon electrode set at +0.85 V. Sensitivity was 2.5 nM. Data were collected and analyzed using Chromgraph software (Bioanalytical Systems).
Data analysis The effect of hypoglycemia (i.e., saline vs. insulin or clamp vs. non‐clamp) on extracellular neurotransmitter concentration within a brain area was analyzed by repeated‐measures ANOVA. Changes in the response at individual time points, within a treatment, were determined by ANOVA and Schefféʹs multiple‐comparison test. Post hoc analysis of a significant ANOVA was by Schefféʹs multiple‐comparison test. Results are presented as means ± SE. Plasma glucose concentrations were analyzed by repeated‐measures ANOVA and Schefféʹs multiple‐comparison test.
54

Chapter 4 – Noradrenergic responses in the hypothalamus
Supplies Ketamine, acepromazine, and butorphanol were obtained from Aveco (Fort Dodge, IA). Xylazine was obtained from Vedco (St. Joseph, MO). All other reagents were purchased from Sigma Chemical (St. Louis, MO).
Results In response to insulin‐induced hypoglycemia, extracellular NE concentrations changed in the VMH (p=0.02) and PVH (p=0.02) but not the LHA (p=0.16). During hypoglycemia, extracellular NE in both the VMH and PVH were elevated in a bimodal fashion (Figure 1; p<0.01 and p=0.02, respectively). Concentrations of NE in the VMH were increased to 165 ± 27% during the first 10 min after insulin and 165 ± 22% during the 20‐ to 30‐min sample period. In the PVH, NE increased to 148 ± 16 and 146 ± 16% during the 0‐ to 10‐min and 20‐ to 30‐min sample periods, respectively. In the LHA, NE concentrations during hypoglycemia were lower than baseline as extracellular NE was reduced to 79 ± 6% of baseline during the 20‐ to 30‐min collection period after insulin.
Figure 1. Effect of insulin‐induced hypoglycemia on extracellular norepinephrine (NE) in the ventromedial hypothalamus (VMN), lateral hypothalamus (LHA), and paraventricular nucleus (PVN). Insulin (1.0 U regular insulin/kg) or an equal volume of sterile saline was infused into the jugular vein (at time 0) after establishing baseline NE concentrations. Data (means ± SE) are presented as a percent of baseline. *Time points different (p<0.05) from baseline as determined by ANOVA and Schefféʹs multiple‐comparison test.
55

Chapter 4 – Noradrenergic responses in the hypothalamus
Baseline concentrations of NE in dialysates were 0.25 ± 0.10, 0.33 ± 0.15, and 0.74 ± 0.14 nM in the VMH, LHA, and PVH, respectively, after standardizing to in vitro recovery of 5.0% (in vitro recoveries were 4.9 ± 0.4%). Blood glucose concentrations during the baseline period were 6.4 ± 0.3 mM and reached a nadir of 3.0 ± 0.2 mM by 15 min after insulin administration. Changes in GABA concentrations after insulin administration were similar to NE only in the VMH (Figure 2; p<0.01). There were no changes in GABA in the LHA (p=0.35) or PVH (p=0.74) after insulin. Extracellular GABA concentrations increased in a bimodal fashion during the first 30 min after insulin (p<0.01), reaching 151 ± 10% of baseline during the 20‐ to 30‐min period. Baseline concentrations of GABA in dialysates were 177 ± 44, 368 ± 65, and 78 ± 37 nM in the VMH, LHA, and PVH, respectively. Blood glucose concentrations during the baseline period were 6.1 ± 0.4 mM across brain areas and reached a nadir of 2.8 ± 0.4 mM by 15 min after insulin administration.
Figure 2. Effect of insulin‐induced hypoglycemia on extracellular GABA in the VMN, LHA, and PVN. Insulin (1.0 U regular insulin/kg) or an equal volume of sterile saline was infused into the jugular vein (at time 0) after establishing baseline GABA concentrations. Data (means ± SE) are presented as a percent of baseline. *Time points different (p<0.05) from baseline as determined by ANOVA and Schefféʹs multiple‐comparison test.
56

Chapter 4 – Noradrenergic responses in the hypothalamus
There was a significant difference among treatment groups in the NE response in both the VMH (p<0.01) and PVH (p=0.03) in the glucose clamp study. As observed in the first set of experiments, extracellular NE concentrations in the VMH (p<0.01) and PVH (p=0.01) increased in a bimodal fashion (Figure 3) in control animals receiving saline infusions into the femoral vein. When plasma glucose concentrations were maintained at baseline levels, the increase in NE was absent in the VMH (p=0.42) but not the PVN (p=0.07). In the PVH, the initial increase in NE after insulin was still apparent in rats during the euglycemic clamp procedure, although the timing of the changes was different (p<0.01). In this set of animals, the second peak increase in NE (136 ± 14% of baseline) was apparent in the 30‐ to 40‐min sample period and there was a third peak (129 ± 9% of baseline) during the 60‐ to 70‐min time period. The increase in GABA concentrations in the VMH after insulin administration was also absent in animals during the euglycemic clamp procedure (Fig. 4; p= 0.01). There was also a difference among treatment groups (p<0.01) in the euglycemic clamp study when GABA was measured in the VMH (Figure 4). The bimodal increase in GABA concentrations in the VMH was apparent in saline‐infused control animals (p=0.01) but was absent during euglycemic clamp (p=0.42). During euglycemic clamp studies, glucose concentrations were maintained near baseline concentrations (6.2 ± 0.4 mM) for 60 min after insulin (Figure 5). Blood glucose concentrations fell to 45 ± 7% of baseline in saline‐infused animals.
Figure 3. Extracellular NE in the VMN and PVN during euglycemic clamp. A bolus of insulin (1.0 U regular insulin/kg) was infused into the jugular vein at time 0, and sterile saline (Control) or a 20% glucose solution (Euglycemic Clamp) was infused into the femoral vein for 60 min. Data (means ± SE) are presented as a percent of baseline. *Time points different (p<0.05) from baseline as determined by ANOVA and Schefféʹs multiple‐comparison test.
57

Chapter 4 – Noradrenergic responses in the hypothalamus
Figure 4. Extracellular GABA in the VMN during euglycemic clamp. A bolus of insulin (1.0 U regular insulin/kg) was infused into the jugular vein at time 0, and sterile saline (Control) or a 20% glucose solution (Euglycemic Clamp) was infused into the femoral vein for 60 min. Data (means ± SE) are presented as a percent of baseline. *Time points different (p<0.05) from baseline as determined by ANOVA and Schefféʹs multiple‐comparison test.
Figure 5. Blood glucose concentrations during euglycemic clamp studies involving the VMN and PVN. Glucose concentrations were determined at 2‐ to 5‐min intervals before and after a bolus of insulin (1.0 U regular insulin/kg) was infused into the jugular vein (at time 0). Sterile saline (Control) or a 20% glucose solution (Euglycemic Clamp) was infused into the femoral vein for 60 min after insulin administration. Data (means ± SE) are presented as a percent of baseline.
Discussion Noradrenergic and GABAergic activity in the medial hypothalamus are increased during an acute hypoglycemic episode. A bimodal increase in extracellular NE in both the VMH and PVH was consistently recorded during the first 30 min of induced hypoglycemia. The pattern of increased NE release was consistent across experiments, occurring in 80% of
58

Chapter 4 – Noradrenergic responses in the hypothalamus
the rats tested, differing only in the timing of the second peak in the PVH during the euglycemic clamp procedure. The present results differ from earlier reports in either the timing or direction of NE release in medial hypothalamic sites (18, 33). The difference in the timing of the increase in NE concentration may be due to the rate hypoglycemia is induced, inasmuch as the intravenous administration of insulin in the present study would be expected to elicit a quicker decline in plasma glucose than the intraperitoneal route used in the previous reports. There is also disagreement among reports on the NE response in the LHA. During hypoglycemia, there was a slight decrease in NE concentrations in the present study and decreased NE release in a push‐pull perfusion study (18). However, extracellular NE concentrations in the LHA were reported to be higher after insulin administration in a microdialysis study (33). In the present study, the decrease in NE in the LHA was apparent in ~50% of rats tested and occurred during the same time interval as a decrease in extracellular GABA in the LHA after 2‐DG (2). The increases in extracellular GABA and NE in the VMH appear to be common responses to glucoprivation. The bimodal increases during hypoglycemia mirrored those observed in the VMH after cellular glucopenia induced by 2‐DG (2, 3). The increase in extracellular NE concentrations in the VMH and PVH during either glucoprivic episode is consistent with reports of increased NE turnover in the hypothalamus after either insulin (1, 35) or 2‐DG (27, 36). The increased extracellular GABA during hypoglycemia is also in agreement with reports of increased GABA content (15) and increased GABA synthesis (4) in the VMH during hypoglycemia. Of interest is the common observation that NE in the medial hypothalamus remained elevated when animals were not allowed to eat after a glucoprivic episode. Extracellular NE concentrations in the VMH remained above baseline up to 90 min after insulin administration in the present study and were still elevated 6 h after insulin administration in an earlier study (33), returning to baseline when rats were allowed to eat. Extracellular GABA concentrations in the VMH also remained above baseline at least 60 min after insulin (this study) or after 2‐DG administration (2) in animals not allowed to eat. When rats were allowed to eat after 2‐DG, GABA concentrations returned to baseline levels after 30 min (2). Because the pattern of NE and GABA release after both hypoglycemia and 2‐DG was similar, it is unlikely that the increases in either neurotransmitter were due to increased glucose concentrations after 2‐DG administration. The increases in noradrenergic and GABAergic activity in the VMH are consistent with their being involved in the compensatory responses to hypoglycemia. Electrical or chemical stimulation of the VMH increased sympathetic nerve activity (43) and plasma glucose concentrations (40, 41). Conversely, lesions of the VMH reduced the characteristic increases in plasma catecholamines and glucagon in response to hypoglycemia (6). Involvement of NE in the VMH is suggested by reports of increased NE release in the VMH after stimulation of the VMH (41) and increases in the activity of sympathetic efferents (28), plasma glucagon (9), and plasma glucose concentrations (8, 36, 38) after microinjection of NE into the VMH. Increases in blood glucose to a glucoprivic challenge (20, 36) or exercise (30, 38) were also blunted by disruption of NE activity in the medial hypothalamus. In addition, the feeding response to glucoprivation was absent after depletion of NE in the hypothalamus (20, 27, 36). The functional significance of the bimodal pattern in neurotransmitter activity in the medial hypothalamus is unclear. The two peaks may be involved in different aspects of glucose mobilization. Scheurink et al. (30) noted differences in the role of VMH α‐ and β‐adrenoceptors on sympathetic activity during exercise. An exercise‐induced increase in
59

Chapter 4 – Noradrenergic responses in the hypothalamus
plasma epinephrine was reduced by α‐blockade in the VMH, whereas the increase in plasma NE concentration during exercise was reduced when timolol, a β‐adrenoceptor antagonist, was administered into the VMH. The necessity of a functional GABAergic system in the VMH for the feeding response to hypoglycemia was demonstrated when application of the GABA‐receptor antagonist bicuculline into the VMH blocked insulin‐induced feeding (14). Because the increases in extracellular NE and GABA in the VMH were absent during the euglycemic clamp procedure, the increases in these neurotransmitters were due to hypoglycemia. Although it is likely that peripheral glucose‐responsive elements influence hypothalamic activity (13, 21), the increased NE and GABA may be primarily affected by decreased extracellular glucose in the medial hypothalamus. Neural activity in and functional output from the hypothalamus are directly affected by glucose availability. Extracellular glucose concentrations in the brain reflect circulating glucose concentrations, being higher during hyperglycemia and lower during hypoglycemia (34). In the medial and lateral hypothalamus, 20‐40% of isolated neurons were responsive to extracellular glucose concentrations (23), and glucose infusions into the carotid artery affected the activity of neurons in medial hypothalamus (10). Adding glucose to perfusion buffer inhibited NE release in the VMH (19) and reduced GABA release from medial hypothalamic pieces (11). The suppressive effect of glucose on NE release was also apparent in hyperglycemic streptozotocin‐induced diabetic rats (22, 32). The reduced extracellular NE concentration in VMH of diabetic rats was normalized when glucose levels were maintained by supplemental insulin (22). Finally, maintaining extracellular glucose concentrations in the VMH during a glucoprivic challenge blocked the counterregulatory responses to systemic hypoglycemia (5). The relationship between NE and GABA in the VMH during hypoglycemia is likely to be the same as during 2‐DG‐induced glucoprivation. The increase in GABA concentrations in the VMH in response to 2‐DG was promoted by the increase in NE (3). The initial peak in GABA release after 2‐DG was regulated by α‐adrenoceptors, and the second peak in GABA release was regulated by β‐adrenoceptors (3). The noradrenergic nerve terminals in the hypothalamus extend from hindbrain areas (25), whereas GABA is likely to be from local interneurons in postsynaptic contact with NE neurons. Noradrenergic neurons innervating the preoptic hypothalamus have been demonstrated to regulate GABA release by direct synaptic connection (12). It remains to be determined what neurons are immediately postsynaptic to GABA and where these neurons extend. The changes in NE concentrations in the PVH may have been due to a direct effect of insulin and not a response to glucoprivation. Unlike the response in the VMH, the increase in extracellular NE after insulin administration was still apparent during the euglycemic clamp procedure. The increase in NE being due to insulin may explain why there was no increase in extracellular NE in the PVH after 2‐DG administration (3). A direct effect of insulin was also indicated when insulin perfused directly into the medial hypothalamus, during push‐pull perfusion, increased NE release (19), and intracerebroventricular insulin administration increased NE turnover in the hypothalamus (29). In addition, NE release from hypothalamic brain slices was increased when insulin was added to the incubation medium (29). Smythe et al. (35) suggested that the increase in NE turnover in the medial hypothalamus during hypoglycemia was due to a direct effect of insulin. Circulating insulin is taken up into the brain (24, 31, 39) and binds to insulin receptors present throughout the medial hypothalamus (42). Although insulin does have a direct effect on glucose‐responsive neurons in the hypothalamus (23), it is unclear whether the initial increase in NE in PVH in
60

Chapter 4 – Noradrenergic responses in the hypothalamus
the present study was due to the injected insulin. The uptake of insulin from the circulation into the cerebrospinal fluid was reported to be longer than 30 min (31, 39). However, using a sensitive insulin assay and microdialysis probes, Orosco et al. (24) measured insulin in the VMH and PVH during the first 30 min of a meal. In summary, noradrenergic and GABAergic activities in medial hypothalamic areas were activated during hypoglycemia. This response is consistent with in vitro evidence of increased NE turnover (36, 37) and GABA synthesis (4) as well as early in vivo measures of increased NE activity in the medial hypothalamus (18, 33). The bimodal increases in GABA and NE activity in the VMH followed the same pattern previously measured after 2‐DG (2, 3) and is suggestive of a common response to glucoprivic episodes. Because glucoprivation localized to the VMH was sufficient to induce compensatory responses (7), the VMH is a critical site for monitoring glucose status. The changes in activity of these two neurotransmitter systems are likely to be parts of a mechanism by which changes in circulating glucose are translated into neurochemical activity.
Perspectives The mechanisms by which the brain monitors plasma glucose status are unknown. The activity of 30‐50% of the neurons in the VMH is affected by local glucose concentrations (reviewed in Ref. 16). As plasma glucose concentrations decline, glucose concentrations in the hypothalamus and other sensory sites influence the activity of noradrenergic and GABAergic elements in the medial hypothalamus. A role of NE and GABA in the medial hypothalamus in behaviors, endocrine, and autonomic function has been documented and is consistent with our suggestion that increased activity of noradrenergic afferents to the medial hypothalamus work through local GABAergic systems to activate appropriate physiological systems to increase circulating glucose. The nature of the local control in the hypothalamus, the systems activated by GABA, and other modulating factors remain to be determined.
References 1. S.I. Bellin and S. Ritter; Disparate effects of infused nutrients on delayed glucoprivic
feeding and hypothalamic norepinephrine turnover. J Neurosci (1981) 1: 1347‐1353 2. J.L. Beverly, M.F. Beverly, and M.M. Meguid; Alterations in extracellular GABA in
the ventral hypothalamus of rats in response to acute glucoprivation. Am J Physiol (1995) 269: R1174‐R1178
3. J.L. Beverly, M.G. de Vries, M.F. Beverly, and L.M. Arseneau; Norepinephrine mediates glucoprivic‐induced increase in GABA in the ventromedial hypothalamus of rats. Am J Physiol (2000) 279: R990‐R996
4. J.L. Beverly and R.J. Martin; Influence of serum glucose on glutamate decarboxylase activity in the ventromedial nucleus of rats. Am J Physiol (1990) 258: R697‐R703
5. M.A. Borg, R.S. Sherwin, W.P. Borg, W.V. Tamborlane, and G.I. Shulman; Local ventromedial hypothalamus glucose perfusion blocks counterregulation during systemic hypoglycemia in awake rats. J Clin Invest (1997) 99: 361‐365
61

Chapter 4 – Noradrenergic responses in the hypothalamus
6. W.P. Borg, M.J. During, R.S. Sherwin, M.A. Borg, M.L. Brines, and G.I. Shulman; Ventromedial hypothalamic lesions in rats suppress counterregulatory responses to hypoglycemia. J Clin Invest (1994) 93: 1677‐1682
7. W.P. Borg, R.S. Sherwin, M.J. During, M.A. Borg, and G.I. Shulman; Local ventromedial hypothalamus glucopenia triggers counterregulatory hormone release. Diabetes (1995) 44: 180‐184
8. M.D. Chafetz, K. Parko, S. Diaz, and S.F. Leibowitz; Relationships between medial hypothalamic alpha 2‐receptor binding, norepinephrine, and circulating glucose. Brain Res (1986) 384: 404‐408
9. A. De Jong, J.H. Strubbe, and A.B. Steffens; Hypothalamic influence on insulin and glucagon release in the rat. Am J Physiol (1977) 233: E380‐E388
10. A.A. Dunn‐Meynell, E. Govek, and B.E. Levin; Intracarotid glucose selectively increases Fos‐like immunoreactivity in paraventricular, ventromedial and dorsomedial nuclei neurons. Brain Res (1977) 748: 100‐106
11. B.M. Grossman, M.L. Devore, E.W. Kelso, and R.J. Martin; Effect of glucose and 2‐deoxyglucose on hypothalamic GABA release in lactating rats. Physiol Behav (1997) 61: 169‐173
12. A.E. Herbison, R.P. Heavens, and R.G. Dyer; Oestrogen modulation of excitatory A1 noradrenergic input to rat medial preoptic gamma aminobutyric acid neurones demonstrated by microdialysis. Neuroendocrinology (1990) 52: 161‐168
13. T. Himmi, A. Boyer, and J.C. Orsini; Changes in lateral hypothalamic neuronal activity accompanying hyper‐ and hypoglycemias. Physiol Behav (1988) 44: 347‐354
14. G.L. Kamatchi, P. Bhakthavatsalam, D. Chandra, and J.S. Bapna; Inhibition of insulin hyperphagia by gamma aminobutyric acid antagonists in rats. Life Sci (1984) 34: 2297‐2301
15. H. Kimura and K. Kuriyama; Distribution of gamma‐aminobutyric acid (GABA) in the rat hypothalamus: functional correlates of GABA with activities of appetite controlling mechanisms. J Neurochem (1975) 24: 903‐907
16. B.E. Levin, A.A. Dunn‐Meynell, and V.H. Routh; Brain glucose sensing and body energy homeostasis: role in obesity and diabetes. Am J Physiol (1999) 276: R1223‐R1231
17. B.E. Levin and V.H. Routh; Role of the brain in energy balance and obesity. Am J Physiol (1996) 271: R491‐R500
18. M.L. McCaleb and R.D. Myers; 2‐Deoxy‐D‐glucose and insulin modify release of norepinephrine from rat hypothalamus. Am J Physiol (1982) 242: R596‐R603
19. M.L. McCaleb, R.D. Myers, G. Singer, and G. Willis; Hypothalamic norepinephrine in the rat during feeding and push‐pull perfusion with glucose, 2‐DG, or insulin. Am J Physiol (1979) 236: R312‐R321
20. E.E. Muller, D. Cocchi, and P. Mantegazza; Brain adrenergic system in the feeding response induced by 2‐deoxy‐D‐glucose. Am J Physiol (1972) 223: 945‐950
21. A. Niijima; Neurophysiological evidence for hepatic glucose‐sensitive afferents. Commentary on ʺThe current status of hepatic theory of food intake control.ʺ Appetite (1981) 2: 151‐152
22. N. Ohtani, M. Ohta, and T. Sugano; Microdialysis study of modification of hypothalamic neurotransmitters in streptozotocin‐diabetic rats. J Neurochem (1997) 69: 1622‐1628
62

Chapter 4 – Noradrenergic responses in the hypothalamus
23. Y. Oomura and H. Kita; Insulin acting as a modulator of feeding through the hypothalamus. Diabetologia (1981) 20, Suppl: 290‐298
24. M. Orosco, K. Gerozissis, C. Rouch, and S. Nicolaidis; Feeding‐related immunoreactive insulin changes in the PVN‐VMH revealed by microdialysis. Brain Res (1995) 671: 149‐158
25. M. Palkovits, J.S. Baffi, and K. Pacak; The role of ascending neuronal pathways in stress‐induced release of noradrenaline in the hypothalamic paraventricular nucleus of rats. J Neuroendocrinol (1999) 11: 529‐539
26. G. Paxinos and C. Watson; The Rat Brain in Stereotaxic Coordinates. Sydney, Australia: Academic, 1986
27. S. Ritter, N.L. Pelzer, and R.C. Ritter; Absence of glucoprivic feeding after stress suggest impairment of noradrenergic neuron function. Brain Res (1978) 149: 399‐411
28. T. Sakaguchi and G.A. Bray; Effect of norepinephrine, serotonin and tryptophan on the firing rate of sympathetic nerves. Brain Res (1989) 492: 271‐280
29. A. Sauter, M. Goldstein, J. Engel, and K. Ueta; Effect of insulin on central catecholamines. Brain Res (1983) 260: 330‐333
30. A.J. Scheurink, A.B. Steffens, and L. Benthem; Central and peripheral adrenoceptors affect glucose, free fatty acids, and insulin in exercising rats. Am J Physiol (1988) 255: R547‐R556
31. M.W. Schwartz, A. Sipols, S.E. Kahn, D.F. Lattemann, G.J. Taborsky Jr, R.N. Bergman, S.C. Woods, and D. Porte Jr; Kinetics and specificity of insulin uptake from plasma into cerebrospinal fluid. Am J Physiol (1990) 259: E378‐E383
32. H. Shimizu; Alteration in hypothalamic monoamine metabolism of freely moving diabetic rat. Neurosci Lett (1991) 131: 225‐227
33. H. Shimizu and G.A. Bray; Effects of insulin on hypothalamic monoamine metabolism. Brain Res (1990) 510: 251‐258
34. I.A. Silver and M. Erecinska; Extracellular glucose concentration in mammalian brain: continuous monitoring of changes during increased neuronal activity and upon limitation in oxygen supply in normo‐, hypo‐, and hyperglycemic animals. J Neurosci (1994) 14: 5068‐5076
35. G.A. Smythe, J.E. Bradshaw, M.V. Nicholson, H.S. Grunstein, and L.H. Storlien; Rapid bidirectional effects of insulin on hypothalamic noradrenergic and serotoninergic neuronal activity in the rat: role in glucose homeostasis. Endocrinology (1985) 117: 1590‐1597
36. G.A. Smythe and S.R. Edwards; Suppression of central noradrenergic neuronal activity inhibits hyperglycemia. Am J Physiol (1992) 263: E823‐E827
37. G.A. Smythe, H.S. Grunstein, J.E. Bradshaw, M.V. Nicholson, and P.J. Compton; Relationships between brain noradrenergic activity and blood glucose. Nature (1984) 308: 65‐67
38. A.B. Steffens, A.J. Scheurink, P.G. Luiten, and B. Bohus; Hypothalamic food intake regulating areas are involved in the homeostasis of blood glucose and plasma FFA levels. Physiol Behav (1988) 44: 581‐589
39. A.B. Steffens, A.J. Scheurink, D. Porte Jr, and S.C. Woods; Penetration of peripheral glucose and insulin into cerebrospinal fluid in rats. Am J Physiol (1988) 255: R200‐R204
63

Chapter 4 – Noradrenergic responses in the hypothalamus
40. M. Sudo, Y. Minokoshi, and T. Shimazu; Ventromedial hypothalamic stimulation enhances peripheral glucose uptake in anesthetized rats. Am J Physiol (1991) 261: E298‐E303
41. A. Takahashi, E. Kishi, H. Ishimaru, Y. Ikarashi, and Y. Maruyama; Stimulation of rat hypothalamus by microdialysis with K+: increase of ACh release elevates plasma glucose. Am J Physiol (1998) 275: R1647‐R1653
42. M. Van Houten and B.I. Posner; Cellular basis of direct insulin action in the central nervous system. Diabetologia (1981) 20, Suppl: 255‐267
43. H. Yoshimatsu, A. Niijima, Y. Oomura, and T. Katafuchi; Lateral and ventromedial hypothalamic influences on hepatic autonomic nerve activity in the rat. Brain Res Bull (1988) 21: 239‐244
64

Chapter 5
Blockade of paraventricular hypothalamic alpha‐adrenoceptors impairs the counterregulation to
hypoglycemia
65

66

Chapter 5 – Blocking noradrenaline in the hypothalamus
Chapter 5 Blockade of paraventricular hypothalamic alpha‐adrenoceptors impairs the counterregulation to hypoglycemia
These studies have been presented at the 1999 EASD Annual Meeting in Brussels, Belgium Diabetologia (1999) volume 42 (Suppl. 1), page A70
A complicated system of counterregulatory responses exists to detect and counteract insulin‐induced hypoglycemia. These counterregulatory responses are likely to be regulated by the brain in response to changes in blood glucose levels and other factors. It has been shown that noradrenaline levels in the hypothalamus rise during hypoglycemia. To investigate whether this noradrenergic signal is indeed crucial for the activation of the counterregulatory responses, rats received selective antagonists to alpha‐adrenoceptors in the paraventricular hypothalamus, and were subjected to hypoglycemia by intravenous infusion of insulin, while counterregulatory responses were monitored. It was shown that blockade of the noradrenergic signal resulted in impaired counterregulatory responses, in particular the adrenaline and noradrenaline responses. Glucose levels decreased more than in the control rats, and plasma corticosterone levels were increased. The data suggest that noradrenergic neurotransmission through the paraventricular hypothalamus plays an important role in the sympathoadrenal counterregulation to insulin‐induced hypoglycemia.
Introduction Hypoglycemia, a common side‐effect in insulin‐treated diabetes, is counterregulated by a variety of responses, aimed at restoring normoglycemia. There are several lines of evidence that show that the brain is involved in this counterregulation against hypoglycemia. First, the brain – and especially the hypothalamus – is known to regulate energy balance (11, 20, 25, 28). Second, the brain receives information from multiple glucose‐sensitive sites, both inside and outside the brain (4, 14, 18, 29). Third, the hypothalamus is activated during hypoglycemia (13), and both lesions (3), surgical damage (21) and inactivation (7) of hypothalamic nuclei have been shown to attenuate counterregulatory responses to hypoglycemia. From studies about the neurochemical nature of the involved neuronal networks, it appears that in particular the noradrenergic circuits may play an important role in the regulation of metabolism (26) and the counterregulatory responses to hypoglycemia. Noradrenergic projections from the hindbrain to the hypothalamus are involved in the counterregulatory responses (17), and in the previous chapter we showed that noradrenaline levels in the hypothalamus are indeed elevated during hypoglycemia, just as they do during 2‐DG‐induced glucoprivation (1). Within the hypothalamus, especially noradrenergic neurotransmission in the paraventricular hypothalamic nucleus (PVN) may play a major role in regulating the counterregulatory responses to hypoglycemia. The PVN is an important neuronal integration center, with direct connections to the sympathetic nervous system, the parasympathetic nervous system, and the hypothalamo‐pituitary‐adrenal system; and noradrenergic systems in the PVN have been shown to be important in the regulation of blood glucose (7, 24) and food intake (8, 12). The current study was designed to investigate the contribution of noradrenergic neurons projecting to the paraventricular hypothalamus to the counterregulatory responses to hypoglycemia. We focused on the role of α‐adrenergic receptors, based on a pilot study as
67

Chapter 5 – Blocking noradrenaline in the hypothalamus
well as data from the literature (2, 8). Therefore we subjected rats to insulin‐induced hypoglycemia while α1‐ or α2‐adrenergic neurotransmission in the PVN was inhibited, and measured the counterregulatory responses glucagon, adrenaline, noradrenaline, and corticosterone.
Methods
Animals and surgery Male Wistar rats were used, weighing 346 ± 3 gram at the beginning of the experiments, and housed singly under standard conditions (lights on from 08:00‐20:00, temperature 21 ± 1 °C) with ad lib access to water and food (standard RMH chow, Hope Farms, Woerden, The Netherlands) unless otherwise stated. The animals were frequently handled and weighed. For stress‐free blood sampling and i.v. infusions in freely‐moving animals, all rats were fitted under halothane/N2O inhalation anesthesia with two permanent silicone catheters (Medica BV, Den Bosch, The Netherlands), one for blood sampling and one for infusions. The catheters were inserted via the jugular vein, with the catheter tips ending in the superior vena cava just before the right atrium (23). In addition, two stainless steel cannulas (dimensions 0.15 mm ID, 0.30 mm OD) were bilaterally inserted into the brain, aimed at the left and right paraventricular nuclei (stereotactic coordinates: anterioposterior 1.6 mm from bregma, lateral 0.5 mm from midline, and dorsoventral 7.4 mm from dura, according to the brain atlas of Paxinos & Watson (16); see Figure 1), and secured to the skull by screws and dental cement. The cannulas were kept closed by steel wire inserts (0.12 mm OD) and protected by a metal cap. After surgery, the rats were allowed at least two weeks for recovery, and were habituated to the experimental conditions. The experimental procedures were approved by the Animal Experiments Committee of the University of Groningen.
Experimental design On the experiment day, food was removed after the lights went on. The venous catheters and brain cannulas were connected to polyethylene tubings to enable remote venous access and brain infusion in freely‐moving animals. After a resting period of at least one hour, two baseline blood samples were taken, with a 10‐minute interval. Then, a bilateral infusion into the PVN was started, which ran at a rate of 0.15 μl/min over a period of 8 minutes and 20 seconds, resulting in a total volume of 1.25 μl infused into each PVN. Control treatment (n=9) consisted of 1.25 μl sterile artificial cerebrospinal fluid (aCSF; 0.4 mM NaH2PO4, 25 mM NaHCO3, 122 mM NaCl, 3.1 mM KCl, 1.3 mM CaCl2, and 1.2 mM MgCl2; pH 7.4). To inhibit α1‐adrenergic transmission, the selective α1‐adrenoceptor antagonist prazosin (Sigma‐Aldrich Chemie, Zwijndrecht, The Netherlands) was infused in a dose of 0.05 μg in 1.25 μl aCSF (n=8). Inhibition of α2‐adrenergic transmission was achieved by infusion of the selective α2‐adrenoceptor
68

Chapter 5 – Blocking noradrenaline in the hypothalamus
antagonist yohimbine (Sigma‐Aldrich Chemie), infused in a dose of 0.25 μg in 1.25 μl aCSF (n=9). Another blood sample was taken 15 minutes after the start of the PVN infusion, and another five minutes later, at the time point defined as t=0, a 90‐minute intravenous infusion of 120 mU.kg‐1.min‐1 insulin was started (Velosulin, Novo Nordisk Farma, Alphen a/d Rijn, The Netherlands). The dose of insulin was based on the previous studies in our laboratory, where this dose produces significant counterregulatory responses (Chapter 2). Blood samples were regularly taken throughout the infusion period to measure changes in glucose levels and in the counterregulatory responses glucagon, adrenaline, noradrenaline, and corticosterone. After the last sample (at t=90 minutes), the insulin infusion was stopped. Half an hour later, food was returned to the animals, and total food intake during the following hour was determined (i.e., from t=120 to t=180 minutes).
Figure 1. Coronal section of the brain at ‐1.56 mm from bregma, according to the rat brain atlas of Paxinos & Watson (15). The paraventricular hypothalamus is labeled PaMM, PaMP, and PaV.
Analysis The blood samples were collected in tubes containing EDTA and aprotinin, and kept chilled during the experiment. Afterwards, 50 μl blood was removed to determine glucose levels (10), while the remaining blood was centrifuged for 15 minutes at 2600 G and 4 °C. Plasma aliquots were frozen until determination of glucagon (Glucagon RIA Kit, Linco
69

Chapter 5 – Blocking noradrenaline in the hypothalamus
Research, St. Charles, MO, USA), adrenaline and noradrenaline (HPLC with electrochemical detection (22)), and corticosterone (HPLC with UV detection (6)). Results are reported as average ± SEM (standard error of the mean). Statistical differences were determined with ANOVA or t‐test (paired where relevant). The significance level was set to p<0.05.
Results The effects of paraventricular hypothalamic α‐adrenergic blockade on the counterregulatory responses to insulin‐induced hypoglycemia are depicted in Figure 2. In the control experiment (vehicle infusion into the PVN), intravenous infusion of 120 mU.kg‐1.min‐1 insulin during 90 minutes rapidly decreased blood glucose levels, to a final level of 3.1 ± 0.2 mM. This hypoglycemia was accompanied by significant rises in glucagon, adrenaline, and noradrenaline levels (final levels 140 ± 6, 1598 ± 611 and 350 ± 27 pg/ml; p<0.05 vs baseline levels). Glucagon responded first, reaching statistical significance from t=15 minutes after the start of the insulin infusion, while adrenaline and noradrenaline were significantly elevated from t=60 onwards. Corticosterone levels were already increased during vehicle infusion into the PVN, and were also elevated during the i.v. insulin infusion. Blockade of α1‐ or α2‐adrenoceptors in the PVN per se by administration of prazosin or yohimbine had no effect on any of the measured blood parameters compared to vehicle administration. However, subsequent i.v. insulin infusion decreased blood glucose levels to a greater degree. Final glucose levels were 2.5 ± 0.2 mM after α1‐blockade (p=0.03 vs vehicle treatment) and 2.7 ± 0.2 mM after α2‐blockade (p=0.16 vs vehicle treatment). Glucagon responses were similar to the control group, although the final glucagon level after α1‐blockade was slightly higher (162 ± 8 vs 140 ± 6 pg/ml; p=0.04). The adrenaline response was delayed and impaired by α1‐ or α2‐blockade, with adrenaline concentrations in both groups only becoming significantly elevated over baseline at t=90 minutes (in the control group, adrenaline levels were significantly elevated already at t=60) and reaching lower final levels (controls: 1598 ± 611 pg/ml; after α1‐ or α2‐blockade: 785 ± 223 and 860 ± 287 pg/ml). Noradrenaline also showed a delayed and reduced response, although statistical significance was only obtained between control rats and α1‐blockade (p<0.05 at t=60 and t=90), and not between controls and α2‐blockade. Corticosterone levels in plasma increased during the antagonist infusions into the PVN, similarly to the control group. During the insulin infusion corticosterone levels remained elevated also, though at higher concentrations after α‐blockade than after control treatment (final levels: control 23 ± 3 μg/dl, α1‐blockade 32 ± 2 μg/dl (p=0.03 vs control), α2‐blockade 31 ± 2 μg/dl (p=0.07 vs control)).
70

Chapter 5 – Blocking noradrenaline in the hypothalamus
-30 0 30 60 900
250
500
750
1000
nora
dren
alin
e (p
g/m
l)
-30 0 30 60 901
3
5
7gl
ucos
e (m
M)
-30 0 30 60 90
time (min)
0
500
1000
1500
2000
adre
nalin
e (p
g/m
l)
-30 0 30 60 900
20
40
60
80
corti
cost
eron
e (µ
g/dl
)
-30 0 30 60 900
50
100
150
200
250
gluc
agon
(pg/
ml)
Figure 2. Levels of blood glucose and counterregulatory hormones during hypoglycemia with or without blockade of hypothalamic noradrenergic neurotransmission. From t=‐20 to t=‐12, the rats received an infusion into the PVN with vehicle (○), the α1‐antagonist prazosin (●), or the α2‐antagonist yohimbine (■). From t=0 to t=90 all rats were infused intravenously with 120 mU.kg‐1.min‐1 insulin. Half an hour after the end of the insulin infusion, i.e. at t=120 minutes, food was returned to the animals. An hour later the consumed amount of food was recorded, with the results depicted in Figure 3. Animals subjected to hypoglycemia without α‐adrenergic blockade in the PVN consumed 4.0 ± 0.7 grams of food. Animals pretreated with the α1‐antagonist consumed a greater amount of food after hypoglycemia (5.9 ± 0.5 grams; p=0.051
71

Chapter 5 – Blocking noradrenaline in the hypothalamus
vs vehicle), while rats pretreated with the α2‐antagonist consumed a slightly smaller amount of food than controls (3.4 ± 0.8 grams; p=0.58 vs vehicle, p=0.01 vs α1‐antagonist).
Figure 2. Food intake after hypoglycemia with or without blockade of hypothalamic noradrenergic neurotransmission. Rats were injected in the PVN with vehicle, the α1‐antagonist prazosin, or the α2‐antagonist yohimbine, and then subjected for 90 minutes to insulin‐induced hypoglycemia. Food was returned at t=120 minutes and foodintake was measured after 1 hour.
0
2
4
6
food
inta
ke (g
)
control
alpha1
alpha2
p = 0.051 p = 0.011
Discussion The current study was undertaken to determine whether α‐adrenergic neurotransmission in the PVN is involved in the counterregulatory responses to insulin‐induced hypoglycemia. The data revealed that blockade of α‐adrenoceptors indeed reduces the sympathoadrenal counterregulatory responses to hypoglycemia, leading to a further reduction in blood glucose levels which is then counteracted by an increase in other counterregulatory responses such as corticosterone, and in individual cases glucagon and food intake. Intravenous infusion of insulin induced hypoglycemia, which was counteracted by an increase in plasma glucagon and in a later stage by an increase in adrenaline levels. Plasma noradrenaline and corticosterone were also increased but to a lesser extent. The results from the control experiment (where vehicle was infused into the PVN) were similar to our findings in a previous study, in which the same amount of insulin was given to rats without brain cannulas (Chapter 2). Furthermore, when food was returned after the end of the insulin infusion, the animals consumed about four grams of food. Administration of selective α‐adrenoceptor antagonists into the PVN did not by itself affect blood components, except an increase in corticosterone identical to that seen after PVN infusion of vehicle. However, during hypoglycemia clear differences could be observed between treatments. Blood glucose levels decreased more when an α1‐ or α2‐adrenoceptor antagonist had been applied into the PVN. Despite that, the responses in adrenaline and noradrenaline were inhibited, with the strongest inhibition seen after blockade of α1‐adrenoceptors – suggesting a predominant role for this noradrenergic receptor subtype in the sympathoadrenal hormonal responses to changes in glucose homeostasis. In contrast, the glucagon responses were not reduced after PVN α‐adrenergic antagonism. Instead, they were identical to or larger than the glucagon response in the control rats. Corticosterone responses were also larger than in controls – assumedly reflecting a compensation for the insufficient sympathoadrenal responses and the further decreased blood glucose levels. These data are very much in line with literature data where
72

Chapter 5 – Blocking noradrenaline in the hypothalamus
total inactivation of the PVN (by lidocain) did not affect glucagon and corticosterone responses during hypoglycemia, while it reduced the adrenaline and noradrenaline responses (7). From the abovementioned data, it could be concluded that the activation of the glucagon and corticosterone responses during hypoglycemia is either not regulated by neurotransmission in the PVN, or is also mediated by other mechanisms besides this PVN pathway. Indeed, for glucagon it has been shown that during hypoglycemia, glucagon secretion from the pancreatic alpha‐cells is activated via multiple and redundant mechanisms (9, 27). The same might apply for the corticosterone response. In the animals treated with the α1‐antagonist, food intake after hypoglycemia was higher than in the vehicle treated group. This increased response may be considered a compensatory response for the further reduced blood glucose levels after α1‐blockade in the PVN. Animals treated with the α2‐adrenoceptor antagonist failed to compensate with an increased food intake response, despite lower glucose levels. This suggests that the food intake response to hypoglycemia is mediated by α2‐ rather than α1‐adrenoceptors in the PVN, in line with other studies observing that α2‐ but not α1‐adrenoceptors are agonistically involved in the regulation of food intake (5, 8, 12). Taken together, the data reveal that noradrenergic transmission in the PVN plays a role in the counterregulatory responses to insulin‐induced hypoglycemia. This is in agreement with the previous chapter and other studies showing activation of noradrenergic projections to the hypothalamus during glucoprivation (1, 19). This noradrenergic neurotransmission seems to be especially important for the sympathoadrenal counterregulatory responses, as seen from the delayed and reduced plasma adrenaline and noradrenaline responses when this neurotransmission is antagonized – while neither the glucagon response nor the corticosterone response were attenuated. Both subtypes of noradrenaline receptors, α1 and α2, are involved in these sympathoadrenal responses, although the fact that only α2‐antagonism prevented a compensatory increase in food intake might imply that the two receptor subtypes have different roles in the counterregulation, with α1‐adrenoceptors perhaps being more involved in regulation of the hormonal responses, while α2‐adrenoceptors seem to mediate the behavioral food intake response. In conclusion, our data confirm the findings in Chapter 4 that the noradrenergic pathways projecting to the PVN play an important role in the counterregulatory responses to insulin‐induced hypoglycemia in rats.
References 1. J.L. Beverly, M.G. De Vries, M.F. Beverly, and L.M. Arseneau; Norepinephrine
mediates glucoprivic‐induced increase in GABA in the ventromedial hypothalamus of rats. American Journal of Physiology (2000) 279: R990‐R996
2. D.A. Booth; Mechanism of action of norepinephrine in eliciting an eating response on injection into the rat hypothalamus. Journal of Pharmacology and Experimental Therapeutics (1968) 160: 336‐348
73

Chapter 5 – Blocking noradrenaline in the hypothalamus
3. W.P. Borg, M.J. During, R.S. Sherwin, M.A. Borg, M.L. Brines, and G.I. Shulman; Ventromedial hypothalamic lesions in rats suppress counterregulatory responses to hypoglycemia. Journal of Clinical Investigation (1994) 93: 1677‐1682
4. W.P. Borg, R.S. Sherwin, M.J. During, M.A. Borg, and G.I. Shulman; Local ventromedial hypothalamus glucopenia triggers counterregulatory hormone release. Diabetes (1995) 44: 180‐184
5. T. Bungo, T. Higaki, H. Ueda, and M. Furuse; Intracerebroventricular administration of octopamine stimulates food intake of chicks through alpha(2)‐adrenoceptor. Physiology & Behavior (2002) 76: 575‐578
6. R. Dawson Jr., P. Kontur, and A. Monjan; High‐performance liquid chromatography (HPLC) separation and quantitation of endogenous glucocorticoids after solid‐phase extraction from plasma. Hormone Research (1984) 20: 89‐94
7. S.B. Evans, C.W. Wilkinson, P. Gronbeck, J.L. Bennett, G.J. Taborsky, and D.P. Figlewicz; Inactivation of the PVN during hypoglycemia partially simulates hypoglycemia‐associated autonomic failure. American Journal of Physiology (2003) 284: R57‐R65
8. C.K. Goldman, L. Marino, and S.F. Leibowitz; Postsynaptic alpha 2‐noradrenergic receptors mediate feeding induced by paraventricular nucleus injection of norepinephrine and clonidine. European Journal of Pharmacology (1985) 115: 11‐19
9. P.J. Havel, S.J. Parry, J.S. Stern, J.O. Akpan, R.L. Gingerich, G.J. Taborsky, and D.L. Curry; Redundant parasympathetic and sympathoadrenal mediation of increased glucagon secretion during insulin‐induced hypoglycemia in conscious rats. Metabolism (1994) 43: 860‐866
10. W.S. Hoffmann; A rapid method for the determination of glucose in blood and urine. Journal of Biological Chemistry (1937) 120: 51‐55
11. B.E. Levin and V.H. Routh; Role of the brain in energy balance and obesity. American Journal of Physiology (1996) 271: R491‐R500
12. A. Morien, V.M. Cassone, and P.J. Wellman; Diurnal changes in paraventricular hypothalamic alpha1‐ and alpha2‐adrenoceptors and food intake in rats. Pharmacology Biochemistry and Behavior (1999) 63: 33‐38
13. M. Niimi, M. Sato, M. Tamaki, Y. Wada, J. Takahara, and K. Kawanishi; Induction of Fos protein in the rat hypothalamus elicited by insulin‐induced hypoglycemia. Neuroscience Research (1995) 23: 361‐364
14. D. Novin, D.A. Vanderweele, and M. Rezek; Hepatic portal 2‐deoxy‐D‐glucose infusion causes eating: Evidence for peripheral glucoreceptors. Science (1973) 181: 858‐860
15. G. Paxinos and C. Watson; The rat brain in stereotaxic coordinates. The new coronal set ‐ 161 diagrams. 5th ed. Elsevier, Burlington, 2005
16. G. Paxinos and C. Watson; The rat brain in stereotaxic coordinates. Academic, Sydney, 1986
17. S. Ritter, I. Llewellyn‐Smith, and T.T. Dinh; Subgroups of hindbrain catecholamine neurons are selectively activated by 2‐deoxy‐D‐glucose induced metabolic challenge. Brain Research (1998) 805: 41‐54
18. V. Routh, Z. Song, and X. Liu; The role of glucosensing neurons in the detection of hypoglycemia. Diabetes Technology and Therapeutics (2004) 6: 413‐421
19. N.E. Rowland; Effects of glucose and fat antimetabolites on norepinephrine turnover in rat hypothalamus and brainstem. Brain Research (1992) 595: 291‐294
74

Chapter 5 – Blocking noradrenaline in the hypothalamus
20. D. Sandoval, D. Cota, and R.J. Seeley; The integrative role of CNS fuel‐sensing mechanisms in energy balance and glucose regulation. Annual Review of Physiology (2008) 70: 513‐535
21. C. Schoefl, A. Schleth, D. Berger, C. Terkamp, A. von zur Muehlen, and G. Brabant; Sympathoadrenal counterregulation in patients with hypothalamic craniopharyngioma. Journal of Clinical Endocrinology & Metabolism (2002) 87: 624‐629
22. F. Smedes, J.C. Kraak, and H. Poppe; Simple and fast solvent extraction system for selective and quantitative isolation of adrenaline, noradrenaline and dopamine from plasma and urine. Journal of Chromatography (1982) 231: 25‐39
23. A.B. Steffens; A method for frequent sampling of blood and continuous infusion of fluids in the rat without disturbing the animal. Physiology & Behavior (1969) 4: 833‐836
24. A.B. Steffens, A.J.W. Scheurink, P.G. Luiten, and B. Bohus; Hypothalamic food intake regulating areas are involved in the homeostasis of blood glucose and plasma FFA levels. Physiology & Behavior (1988) 44: 581‐589
25. A.B. Steffens, J.H. Strubbe, B. Balkan, and A.J.W. Scheurink; Neuroendocrine mechanisms involved in regulation of body weight, food intake and metabolism. Neuroscience & Biobehavioral Reviews (1990) 14: 305‐313
26. A.B. Steffens, J.H. Strubbe, B. Balkan, and A.J.W. Scheurink; Neuroendocrine factors regulating blood glucose, plasma FFA and insulin in the development of obesity. Brain Research Bulletin (1991) 27: 505‐510
27. G.J. Taborsky, B. Ahren, and P.J. Havel; Autonomic mediation of glucagon secretion during hypoglycemia. Implications for impaired alpha‐cell responses in type 1 diabetes. Diabetes (1998) 47: 995‐1005
28. G. Williams, J.A. Harrold, and D.J. Cutler; The hypothalamus and the regulation of energy homeostasis: lifting the lid on a black box. Proceedings of the Nutrition Society (2000) 59: 385‐396
29. K. Yettefti, J.C. Orsini, and J. Perrin; Characteristics of glycemia‐sensitive neurons in the nucleus tractus solitarii: Possible involvement in nutritional regulation. Physiology & Behavior (1997) 61: 93‐100
75

Chapter 5 – Blocking noradrenaline in the hypothalamus
76

Section III – Recurrent hypoglycemia
The most exciting phrase to hear in science, the one that heralds new discoveries, is not ʺEureka!ʺ but ʺThatʹs funny...ʺ
‐ Isaac Asimov
77

78

Chapter 6
Hypoglycemia‐Associated Autonomic Failure in rats
79

80

Chapter 6 – HAAF in rats
Chapter 6 Hypoglycemia‐Associated Autonomic Failure in rats
Parts of these studies have been presented at the 1998 EASD Annual Meeting in Barcelona, Spain, at the 2000 EASD Annual Meeting in Jerusalem, Israel,
and at the Hypoglycaemia 2001 symposium in Assisi, Italy Diabetologia (1998) volume 41 (Suppl. 1), page A68 Diabetologia (2000) volume 43 (Suppl. 1), page A193
Insulin‐induced hypoglycemia elicits a number of counterregulatory responses, depending on glucose levels. Repeated hypoglycemia leads to a reduction in these responses. This compromises the restoration of normoglycemia and reduces the patientʹs awareness of the low glucose levels, leading to more frequent and more severe hypoglycemic episodes. This phenomenon is called Hypoglycemia‐Associated Autonomic Failure, a serious limitation to the treatment of insulin‐requiring diabetes patients. The causes of HAAF are largely unknown. The aim of the studies presented in this chapter is to develop a rat model for HAAF, and to investigate some of the underlying mechanisms. Rats were subjected to a series of insulin infusions, to mimic the HAAF test protocols in humans. Blood samples were withdrawn for measurement of glucose, glucagon, adrenaline and/or corticosterone responses. Antecedent repeated insulin‐induced hypoglycemia led to reductions in counterregulatory responses to subsequent hypoglycemia, showing that HAAF can be induced in rats. Antecedent repeated glucoprivation also reduced counterregulatory responses to subsequent hypoglycemia, suggesting that HAAF is the result of glucoprivation and not specific for insulin‐induced hypoglycemia. Finally, in a series of behavioral experiments we showed that individual differences (such as food preference) are associated with the susceptibility for developing HAAF.
Introduction Since the initiation of the Diabetes Control and Complications Trial (DCCT) (17), the number of diabetes patients on intensive insulin therapy has greatly increased. Intensive therapy allows a much tighter glucose control than classic insulin therapy, keeping the diurnal blood glucose profile closer to a normal non‐diabetic profile. This markedly reduces the incidence of the long‐term complications of diabetes (microvascular damage due to chronic hyperglycemia, resulting in retinopathy, neuropathy, and nephropathy) (16, 30). It does however considerably increase the incidence of hypoglycemia (18). It is debated how much this incidence is increased – the often cited number from the DCCT (a three‐fold increase in severe hypoglycemia) most likely underestimates the true increase, since those data are from a very select group of patients and under near‐ideal conditions (7). There is no doubt however that hypoglycemia is a major limitation to the intensive treatment of diabetes (9). Not only because of the increased risk of hypoglycemia when regulating glucose levels close to normal, but in particular because of the risk of Hypoglycemia‐Associated Autonomic Failure (HAAF), the condition where an increased frequency of hypoglycemic episodes reduces both the counterregulatory responses to hypoglycemia (2, 8) and the sensations associated with hypoglycemia (3, 5, 22). As a consequence, repeated hypoglycemia is not only accompanied by insufficient counterregulatory responses, but the patients also fail to sense that they are becoming hypoglycemic (called hypoglycemia unawareness). This leads to additional and more severe hypoglycemic episodes (11, 44), which again further worsens the above mentioned defects – a vicious circle which can only
81

Chapter 6 – HAAF in rats
be broken by rigorous avoidance of hypoglycemia (6, 12), at the cost of poorer glycemic control. The underlying mechanisms for the development of HAAF remain unclear, and the lack of an established animal model makes mechanistic investigations difficult. Therefore, the aim of the exploratory studies described in this chapter was to establish a rat model of HAAF, and to characterize some of the associated phenomena. More specifically, we investigated the effect of different amounts of infused insulin and of the number of antecedent hypoglycemic episodes, the individual differences between animals, and the effects of other glucoprivic agents, but also the relationships with food intake and nutrient preference.
Methods
Animals and surgery In all studies, normal male Wistar rats were used, weighing around 350 grams at the beginning of the experiments, and housed singly under standard conditions (lights on from 08:00 to 20:00, temperature 21 ± 1 °C), with ad lib access to water and food (standard RMH chow, Hope Farms, Woerden, The Netherlands) unless otherwise stated. The animals were frequently handled and weighed. Under halothane+N2O anesthesia, the rats were equipped with two permanent silicone catheters (Medica BV, Den Bosch, The Netherlands), inserted via the jugular vein (40). This method enables remote infusions and blood sampling from undisturbed freely‐moving animals. The rats were allowed 1‐2 weeks to recover from the surgery, and were habituated to the experimental conditions, thus excluding undesirable stress effects. The experimental procedures were approved by the Animal Experiments Committee of the University of Groningen.
General protocol Hypoglycemia was in all studies induced by a 90‐minute intravenous infusion of insulin (Velosulin, Novo Nordisk Farma, Alphen a/d Rijn, The Netherlands). Control infusions consisted of vehicle (0.9% NaCl). The infusion speeds were 3.2 ml.kg‐1.min‐1. The animals did not have access to food during the experiment. Blood samples were withdrawn throughout the study period and collected in chilled tubes with aprotinin and EDTA. The samples were used for determination of blood glucose (Hoffmannʹs ferricyanid method (26)) as well as plasma levels of insulin (Rat Insulin RIA Kit, Linco Research, St. Charles, MO, USA), glucagon (Glucagon RIA Kit, Linco Research), adrenaline and noradrenaline (HPLC with electrochemical detection (37)), and/or corticosterone (HPLC with ultraviolet detection (15)). In those experiments where more than 1 ml of blood in total was withdrawn during the experimental period, anemia was avoided by transfusing the same amount of heparinized blood from a blood donor rat after each blood sample. In some of the studies,
82

Chapter 6 – HAAF in rats
food was returned after the hypoglycemic episode and weighed again one hour later, to measure the acute food intake response. Data are expressed as average ± standard error of the mean (SEM). Statistical differences were determined with ANOVA or t‐test (paired where relevant). The significance level was set to p<0.05. Generally, small groups of animals were used, and therefore the statistical power of these exploratory pilot studies is limited.
Specific protocols Different experimental protocols were applied to induce Hypoglycemia‐Associated Autonomic Failure. In Experiment 1, we investigated whether a single antecedent hypoglycemic episode could induce HAAF in rats. After two baseline blood samples, the animals (n=4) were infused for 90 minutes with 88 mU.kg‐1.min‐1 insulin, and this was repeated 24 hours later. During both treatments, blood samples were taken at time points 5, 7.5, 10, 15, 20, 30, 45, 60, 75 and 90 minutes, to determine levels of blood glucose and of the counterregulatory responses adrenaline and corticosterone. In Experiment 2, we studied whether a higher dose of insulin would be better at inducing HAAF. The same protocol as in Experiment 1 was used, but with an insulin dose of 120 mU.kg‐1.min‐1, on both days (n=5). A control group (n=6) was also included, which was infused with vehicle on the first day, and with insulin on the second day. Blood samples were taken at time points 2.5, 5, 7.5, 10, 15, 20, 30, 45, 60, 75 and 90 minutes, to determine levels of blood glucose and of the counterregulatory responses glucagon, adrenaline and corticosterone. In Experiment 3, the effect of two antecedent hypoglycemic episodes (instead of one) on the development of HAAF was investigated. On the first day, the rats (n=5) received two insulin infusions, one in the morning and one in the afternoon. On the second day the rats received an insulin infusion again in the morning. The insulin dose was 120 mU.kg‐1.min‐1 in all cases. Blood samples for measurement of counterregulatory responses were taken at t=0 and t=90 on both mornings, i.e. the beginning and the end of the first and the third hypoglycemic episode. This protocol had been used in human studies (e.g. Refs 14 and 25), and it was thought that such a protocol might be better at inducing HAAF in animals. In Experiment 4, behavioral responses (food intake and nutrient preference) in relation to the development of HAAF were studied. Rats (n=10) were maintained on a freely feeding self‐selection paradigm, where they had permanent access to two enriched chow types, carbohydrate‐enriched chow and fat‐enriched chow. The diets were made of 75% normal chow (RMH chow, Hope Farms, Woerden, The Netherlands), which was enriched with either glucose or fat and re‐pelleted. These diets are chosen because the subtle differences between them better reflect nutrient distribution in a natural setting. After food intake and diet preference were stabilized, each ratʹs diet preference was identified, and they were all subjected to three days with two hypoglycemic episodes (90‐min infusions of 120 mU.kg‐1.min‐1 insulin) on each day. The counterregulatory responses glucagon and adrenaline were measured at the beginning and end of the hypoglycemic episodes, while food intake responses were studied afterwards and during the night. Finally, in Experiment 5 we investigated whether HAAF can only be induced by insulin‐induced hypoglycemia, or whether glucoprivation per se induces HAAF. To this
83

Chapter 6 – HAAF in rats
end, a similar protocol as in Experiment 3 was used. On the first day, rats (n=7) were subjected two times to glucoprivation by means of the glucose antimetabolite 2‐deoxyglucose (200 mg/kg i.v., one injection in the morning and one in the afternoon). Control rats (n=2) received vehicle infusions instead. On the morning of the second day, both groups were subjected to hypoglycemia (insulin infusion of 120 mU.kg‐1.min‐1), while blood samples were taken at time points 5, 15, 30, 60 and 90 minutes to measure blood glucose and the counterregulatory responses glucagon, adrenaline, and noradrenaline.
Results
Experiment 1 – One antecedent hypoglycemic episode In the first study, it was investigated whether one antecedent hypoglycemic episode would change the counterregulatory responses to hypoglycemia. Rats were subjected to a hypoglycemic episode by infusion of 88 mU.kg‐1.min‐1 of insulin, which was repeated the following day. The glucose, adrenaline and corticosterone levels in both episodes are shown in Figure 1.
terone levels during insulin‐induced hypoglycemia on day 1 (open symbols) and
episode (open symbols), blood glucose levels were and an increase in secretion of adrenaline and graphs) as well as glucagon (data not shown) was elicited. During the second hypoglycemic episode (solid symbols), reduced glucose levels and a lower adrenaline response,
ically significant. This is mainly due to considerable inter‐individual ariation in the responses to hypoglycemia, and in the development of HAAF. This is lustra
0 30 60 900
10
20
30
40
50
corticosterone (µg/dl)
0 30 60 900
500
1000
1500
adrenaline (pg/ml)
0 30 60 901
3
5
7
glucose (mM)
Figure 1. Glucose, adrenaline and corticoson day 2 (solid symbols) In the first hypoglycemicsignificantly reduced (left graph),corticosterone (middle and rightNoradrenaline was not affected.there was a tendency for furtherwhile the corticosterone and glucagon responses were unaffected. These differences were however not statistvil ted in Figure 2 which shows the responses of the individual animals.
84

Chapter 6 – HAAF in rats
rat 1:
glucose (mM) adrenaline (pg/ml)
2. Glucose, adrenaline and corticosterone levels of four individual rats during insulin‐induced hypoglycemia on day
From this figure the hypoglycemia are evident. On the second day, for instance, raglucose levels as rat 2, yet it does not display any adrenaline the individual responses leads to the following conclusion: boadrenaline responses are always either similar or reduced compared to the first hypoglycemia: rats 1 and 2 had lower
aline response, rat 3 had lower glucose levels and no adrenaline response, and rat 4 had similar glucose levels but a lower adrenaline response. Therefore it appears that a lower blood glucose level is needed to evoke a given counterregulatory response – or that a given blood glucose level is accompanied by reduced counterregulatory responses. In addition,
rat 2:
rat 3:
rat 4:
0 30 60 90
0
10
20
30
40
50
corticosterone (µg/dl)
0 30 60 900
10
20
30
40
50
corticosterone (µg/dl)
0 30 60 900
10
20
30
40
50
corticosterone (µg/dl)
0 30 60 900
10
20
30
40
50
terone (µg/dl)corticos
Figure1 (open symbols) and on day 2 (solid symbols)
differences between the individual responses to insulin‐induced t 3 reaches the same low response. Detailed analysis of th glucose levels and
during the second hypoglycemia glucose levels and a lower
adren
0 30 60 900
500
1000
1500
adrenaline (pg/ml)
0 30 60 900
500
1000
1500
adrenaline (pg/ml)
0 30 60 900
500
1000
1500
adrenaline (pg/ml)
0 30 60 900
500
1000
1500
0 30 60 901
3
5
7
glucose (mM)
0 30 60 901
3
5
7
glucose (mM)
0 30 60 901
3
5
7
0 30 60 901
3
5
7
glucose (mM)
85

Chapter 6 – HAAF in rats
these individual responses illustrate that there are individual differences in the development of HAAF, in addition to the individual differences to hypoglycemia per se.
Experiment 2 – A higher insulin dose In this study, the same protocol was used as in the previous, but with a higher dose of insulin – 120 mU.kg‐1.min‐1. A control group was also included, which received a vehicle
on the second day.
‐induced hypoglycemia 24 hours after being subjected to antecedent
ypoglycemia (HAAF rats, solid symbols) or vehicle infusion (control rats, open symbols).
at were subjected to hypoglycemia n the s
ced glucagon response lucagon levels in the HAAF group were lower up to time point t=60; p<0.05 at t=45).
There were no reductions in the adrenaline and corticosterone responses between the
occasions instead of two: day 1 in the morning, morning. Blood samples taken at the beginninghypoglycemic episode were used to demonstrate of glucagon, adrenaline and noradrenaline are
infusion on the first day, and an insulin infusion on the second day. The experimental groupeceived insulin both on the first andr Figure 3 shows the differences between those two groups in their glucose and glucagon responses during hypoglycemia on the second day.
Figure 3. Glucose and glucagon levels during insulinh This dose of insulin reduced blood glucose to the same extent as the dose of insulin used in Experiment 1 (88 mU.kg‐1.min‐1). In the animals tho preceding day, induction of HAAF was visible as further reduced glucose level(although not significantly), combined with a delayed and redu(g HAAF‐animals and the control animals.
Experiment 3 – Three times a hypo In this study, animals were subjected to insulin‐induced hypoglycemia on three
day 1 in the afternoon, and day 2 in the and the end of the first and the last the induction of HAAF. The responses
depicted in Figure 4.
0 30 60 900
100
200
glucagon (pg/ml)
0 30 60 901
3
5
7
glucose (mM)control
HAAF
86

Chapter 6 – HAAF in rats
pen sym
Both the glucagon and adrenaline responses were impaired, although the differences did not reach statistical significance. There were no differences between the noradrenaline
nsulin levels nor the food intake response after the ypoglycemic episode were different between the groups (Figure 5).
intake response after the hypoglycemic
episode (right). Open bars: first hypoglycemic episode.
nutrient preference
was performed to investigate the relations between hypoglycemia. During these experiments, the rats had
te‐enriched chow and fat‐enriched chow. consumed about 50% of their total daily food intake from repeated hypoglycemia however (twice daily for three d their diet preference more towards the carbohydrate‐
creased from 52 ± 7 % on the day before the first hypoglycemic episodes to 71 ± 4 % on the ird d
Figure 4. Glucagon, adrenaline and noradrenaline during the first hypoglycemic episode (in the morning of the first day;o bols) and the third (in the morning of the second day; solid symbols)
responses. Likewise, neither plasma ih
Figure 5. Plasma insulin levels at the end of the hypoglycemic episode (left) and food episode; solid bars: third hypoglycemic
Experiment 4 – Food intake and In the next set of experimentsdiet preference and recurrent permanent free access to carbohydra On average, the animalseach of the two food types. Duringconsecutive days), all animals shifteenriched chow, so that the average daily consumption of carbohydrate‐enriched chow inth ay with hypoglycemia (p<0.05). After terminating the exposure to repeated hypoglycemic episodes, average diet preference returned to baseline levels (Figure 6).
0
2
4
6
1h food intake (g)
0
1000
2000
plasma insulin (ng/ml)
0 30 60 900
250
500
noradrenaline (pg/ml)
0 30 60 900
1000
2000
3000
adrenaline (pg/ml)
0 30 60 900
100
200
glucagon (pg/ml)
87

Chapter 6 – HAAF in rats
igure 6. Food preference (left) and total daily food intake (right) before, during, and after three days of repeated hypoglycemia (twice daily)
again at basal
vel on
s always ow.
ome other animals showed in the same way a clear preference for the fat‐enriched food.
pattern. These three categories of animals werepreferenceʺ, and ʺno preferenceʺ. After this classification, the counterregulatoryappeared to be different between these groups.preference seemed to develop HAAF sooner the glucagon and adrenaline responses already(Figure 7). The group without a clear diet day 2, and adrenaline responses on day 2 anddecrease in food intake from day 1 to day 3, groups.
F
Food intake during the first hour after each hypoglycemic episode did not change significantly during the three days. Total daily food intake was significantly increasedduring day 1 (13% higher than basal; p<0.05) but decreased thereafter and was le days 2 and 3, while the animals consumed significantly less than baseline during day 4. As can be seen from Figure 6, the overall average baseline food preference was approximately 50% for each food type. However, detailed analysis of individual data revealed that three different categories of animals could be identified. Some animalconsumed more than 60% of their total food intake from the carbohydrate‐enriched chSThe remaining animals either consumed between 40‐60% of each diet, or had no consistent
labeled as ʺcarbohydrate‐preferenceʺ, ʺfat‐
responses to (recurrent) hypoglycemia The two groups having a consistent diet
than the group without a diet preference, with nearly disappeared at the end of day 2
preference still showed a glucagon response on 3. In contrast, this group showed a stronger
ending below baseline and below the other two
basal day 1 day 2 day 3 day 4 day 50
10
20
30
40total daily food intake (g)
basal day 1 day 2 day 3 day 4 day 50
25
50
75
100carbohydrate-enriched chow intake (% of total)
88

Chapter 6 – HAAF in rats
with or without food preference on total 24h food intake. ls: rats with carbohydrate preference; solid symbols: rats
xperiment 5 – GAAF
whether insulin‐induced hypoglycemia is antecedent glucoprivation also reduce the To this end, two groups of rats were used. day 1, while the experimental group was injection of the glucose antimetabolite 2‐
subjected to insulin‐induced hypoglycemia
Figure 7a. Effects of three days of repeated hypoglycemia in rats with or without food preference on glucagon and adrenalinelevels at the end of the second hypoglycemia on days 2 and 3. Hatched bars: rats without clear diet preference; open bars: ratswith carbohydrate preference; solid bars: rats with fat preference.
Figure 7b. Effects of three days of repeated hypoglycemia in ratsDiamond symbols: rats without clear diet preference; open symbowith fat preference.
E The final set of experiments investigatedrequired to induce HAAF, or if other forms of counterregulatory responses to hypoglycemia. Control rats received two vehicle infusions on subjected twice to glucoprivation by intravenousdeoxyglucose. The next day, both groups were(infusion of 120 mU.kg‐1.min‐1 insulin).
basal day 1 day 2 day 3-5
0
5
ange in total daily food intake (g)10
chcarb-pref
fat-pref
no pref
day 2 day 30
1000
2000
3000adrenaline (pg/ml)
0
100
200
300
glucagon (pg/ml)
day 2 day 3
89

Chapter 6 – HAAF in rats
glucose (mM) glucagon (pg/ml)
Figure 8. Glucose, glucagon, adrenaline and noradrenalinesymbols) and in animals previously exposed to glucoprivationadministrations on the preceding day, while GAAF anima Control animals showed the expected
during insulin‐induced hypoglycemia in control animals (open (solid symbols). Control animals had received vehicle
ls had received two injections with 2‐DG.
responses to insulin‐induced hypoglycemia – y 2‐
DG however significantly impaired the adrenaline response to insulin‐induced hypoglycemia (Figure 8). The glucagon and noradrenaline responses were not affected. In a small pilot study, some animals (n=6) underwent the opposite protocol: they received insulin‐induced hypoglycemia twice on the first day, and 2‐DG on the second day. Control rats (n=2) received vehicle twice on the first day. The animals with HAAF (induced by the antecedent hypoglycemia) tended to have lower adrenaline responses to 2‐DG (peak levels 572 ± 146 vs 828 ± 194 pg/ml, p=0.12). Again, the glucagon response remained unaffected (peak levels 114 ± 14 vs 107 ± 8 pg/ml; p>0.05).
The present studies were undertaken in order to develop an animal model for
er
i.e. significant increases in glucagon and adrenaline levels. Antecedent glucoprivation b
Discussion Hypoglycemia‐Associated Autonomic Failure and get more insight into some of its characteristics. We found that recurrent hypoglycemia does indeed induce defects in the counterregulatory responses in rats. Even one single antecedent hypoglycemia may affect the counterregulatory responses in some animals, as was shown in Experiment 1. A high
0 30 60 900
500
1000
noradrenaline (pg/ml)
0 30 60 900
250
500
adrenaline (pg/ml)
0 30 60 900
100
200
0 30 60 901
control
GAAF
3
5
7
90

Chapter 6 – HAAF in rats
insulin dose (as used in Experiment 2) was more effective, leading to a slightly stronger
ed chow and fat‐enriched chow),
e found that recurrent hypoglycemia shifted the nutrient preference of rats towards carbohydrates: all animals increased their consumption of the carbohydrate‐enriched chow,
eir baseline diet preference. This shift in food preference was seen on all ree days where hypoglycemia was induced, and returned to baseline thereafter. When we ivided ce,
hat the
ific, poglycemia,
aps more orrect
2, er
g response to hypoglycemia is regulated
n e different
nterregulatory esponses to hypoglycemia but especially in the development of HAAF.
to
administration, blood glucose levels are actually elevated). This basically suggests that
decrease in glucose levels and a reduced glucagon response during the second hypoglycemic episode. Still, these HAAF‐effects were not very robust, therefore Experiment 3 was performed. Rats received two antecedent hypoglycemic episodes instead of one, resulting in a nearly abolished adrenaline response to subsequent hypoglycemia. In Experiment 4 focused on the behavioral counterregulatory response, food intake.In rats permanently offered two diets (carbohydrate‐enrichw
regardless of ththd the animals over three different groups (carbohydrate‐preference, fat‐preferenand no preference) based on their baseline consumption of the two diets, we found tʺno preferenceʺ rats showed stronger hormonal responses to hypoglycemia, and were slower to develop HAAF. Thereby these results could suggest individual differences in counterregulatory strategies, at least in rats. The last experiment addressed the question whether HAAF is hypoglycemia‐specor may also develop after other forms of glucoprivation. Instead of recurrent hyrats were subjected to recurrent glucoprivation by 2‐DG, a non‐metabolizable glucose analogue. Antecedent 2‐DG reduced the adrenaline responses to insulin‐induced hypoglycemia – suggesting that glucoprivation may indeed induce HAAF (or perhc ly, GAAF – Glucoprivation‐Associated Autonomic Failure). HAAF may manifest itself in different ways. In some groups of animals, the counterregulatory responses were decreased. In others, the counterregulatory responses remained unchanged, but blood glucose levels were lower. Therefore it is important to evaluate the counterregulatory responses in relation to the blood glucose level (which also implies a potential pitfall with the hypoglycemic clamp technique, because it does not allowglucose levels to be different). HAAF does not always affect the same counterregulatory responses either – e.g. adrenaline in Experiments 1 and 5, and glucagon in Experiment while the food intake response does not seem to be particularly sensitive, in line with othdata (33) (which also suggests that the feedinseparately from the hormonal responses). The degree to which the responses are affected is also different – the adrenaline response was markedly reduced or even completely abolished, while the glucagon response seems to be more resistant to HAAF (as has beereported by others (21, 27, 36, 42)). The latter might be due to the redundancy of thmechanisms regulating glucagon secretion during hypoglycemia (24, 41). Furthermore we observed considerable variation between individuals, both in the cour We found that antecedent 2‐DG administration also can lead to a HAAF‐like phenomenon. This finding that not only hypoglycemia but also other forms of glucoprivation can cause autonomic defects is very important, because it removes some of the confounding factors associated with insulin‐induced hypoglycemia, particularly the concomitant hyperinsulinemia (even though severe hyperinsulinemia has been reported potentiate the development of HAAF (36)) and the low blood glucose levels (during 2‐DG
91

Chapter 6 – HAAF in rats
intracellular glucoprivation, rather than e.g. blood glucose or insulin levels, may be considered as the main factor for the development of HAAF. It has furthermore been sin the literature that repeated administration of 2‐DG impairs the counterregulatory responses to 2‐DG (35), just like repeated administration of insulin impairs the autoresponses to insulin. In the current study we showed that repeated administration of 2‐DGimpairs the autonomic responses to insulin, and our pilot data indicated that repeated administration of insulin may impair the autonomic responses to 2‐DG. We therefore conclude that the autonomic dysfunction known as HAAF can be induced by any forglucoprivation.
hown
nomic
m of
d it is also
er
l ,
he precise reason why the brain changes counterregulatory responses after ecurrent hypoglycemia remains to be resolved.
d
lly, it appears
in the impaired counterregulatory response induced by repetitive neuroglucopenia. Endocrinology (2007) 148: 1367‐1375
Several other factors that may underlie the development of HAAF are alreadyinvestigated. The depth of hypoglycemia contributes to its development (14), anknown that HAAF is not a general effect of autonomic responses, since non‐hypoglycemic forms of autonomic activation do not produce HAAF (32). Evidence exists arguing both for(13, 29, 34) and against (19, 21, 23, 31, 36) the notion that antecedent corticosteroid responsesmay play a role in the development of HAAF. It has furthermore been suggested that the brain somehow ʺadaptsʺ to recurrent hypoglycemia, e.g. by changes in brain glucose transport, supercompensation in glial or hepatic glycogen stores, or switching to othenergy sources (increased availability of other energy sources attenuates the counterregulatory responses to hypoglycemia (4, 43)). Also the central and peripheramechanisms involved in glucosensing may be altered during recurrent hypoglycemia (1, 2839). A review of most of the current hypotheses can be found in Ref. 10. In general, data from the literature point to a major role for the brain in the development of HAAF (20, 38). The brain detects hypoglycemia, it controls the counterregulatory responses, and hypothalamic activation is reduced after recurrent hypoglycemia. Tr In conclusion, it is possible to induce HAAF in rats. This generally impairs the responses of adrenaline and glucagon to glucoprivation, although the exact pattern differs between studies and between individual animals. Food intake responses may also be influenced, but seem to be more resistant to HAAF‐like effects. Furthermore, since food preference influences the hormonal and feeding responses to hypoglycemia, and since repeated hypoglycemia can alter nutrient preference, it is suggested that food intake anindividual phenotypic make‐up may play a role in the development of Hypoglycemia‐Associated Autonomic Failure and thereby hypoglycemia unawareness. Finathat glucoprivation in general seems to be the key factor in the development of this autonomic failure.
References 1. T. Alquier, J. Kawashima, Y. Tsuji, and B.B. Kahn; Role of hypothalamic adenosine 5ʹ‐
monophosphate activated protein kinase
92

Chapter 6 – HAAF in rats
2. S.A. Amiel, R.S. Sherwin, D.C. Simonson, and W.V. Tamborlane; Effect of inteninsulin therapy on glycemic thresholds for counterregulatory hormone release. Diabetes (1988) 37: 901‐907
3. V.J. Briscoe and S.N. Davis; Hypoglycemia in Type 1 and Type 2 diabetes: physiology, pathophysiology, and management. Clinical Diabetes (2006) 24: 115
4. K.P. Briski; Intraventricular lactate infusion attenuates the transactivational effects othe glucose antimetabolite, 2‐deoxy‐D‐glucose, on hypothalamic vasopressinneurons. Bra
sive
‐121 f
ergic in Research (1999) 839: 341‐345
. W.L. Clarke, L.A. Gonder‐Frederick, F.E. Richards, and P.E. Cryer; Multifactorial origin of hypoglycemic symptom unawareness in IDDM. Association with defective
counterregulation and better glycemic control. Diabetes (1991) 40: 680‐685 . I.C. Cranston, J. Lomas, A. Maran, I. Macdonald, and S.A. Amiel; Restoration of
7. atus of
65 8. ssociated autonomic failure in diabetes. American
9.
10. (2005) 54: 3592‐3601
‐
12. 94)
13. F. Costa; Prevention of an increase in plasma
14.
hy coids after solid‐phase
16. es on the
tes mellitus. New England Journal of Medicine (1993) 329: 977‐986 T). Design
18. h Group; Hypoglycemia in the diabetes control and complications
19. z; mia but not antecedent
corticosterone in the rat. American Journal of Physiology (2001) 281: R1426‐R1436
5
glucose6
hypoglycaemia awareness in patients with long‐duration insulin‐dependent diabetes. Lancet (1994) 344: 283‐287 O.B. Crofford; The diabetic control and complications trial (DCCT). Current stprevention and treatment of diabetic complications: proceedings of the Third International Symposium on treatment of Diabetes Mellitus. ICS821 (1990) 159‐1P.E. Cryer; Hypoglycemia‐aJournal of Physiology (2001) 281: E1115‐E1121 P.E. Cryer; Hypoglycaemia: The limiting factor in the glycaemic management of Type I and Type II Diabetes. Diabetologia (2002) 45: 937‐948 P.E. Cryer; Mechanisms of Hypoglycemia‐Associated Autonomic Failure and its component syndromes in diabetes. Diabetes
11. P.E. Cryer; Hypoglycemia begets hypoglycemia in IDDM. Diabetes (1993) 42: 16911693 S. Dagogo‐Jack, C. Rattarasarn, and P.E. Cryer; Reversal of hypoglycemia unawareness, but not defective glucose counterregulation, in IDDM. Diabetes (1943: 1426‐1434 S.N. Davis, C. Shavers, B. Davis, andcortisol during hypoglycemia preserves subsequent counterregulatory responses. Journal of Clinical Investigation (1997) 100: 429‐438 S.N. Davis, C. Shavers, R. Mosqueda‐Garcia, and F. Costa; Effects of differing antecedent hypoglycemia on subsequent counterregulation in normal humans.Diabetes (1997) 46: 1328‐1335
15. R. Dawson Jr., P. Kontur, and A. Monjan; High‐performance liquid chromatograp(HPLC) separation and quantitation of endogenous glucocortiextraction from plasma. Hormone Research (1984) 20: 89‐94 DCCT Research Group; The effect of intensive treatment of diabetdevelopment and progression of long‐term complications in insulin‐dependent diabe
17. DCCT Research Group; The diabetes control and complications trial (DCCand methodologic considerations for the feasibility phase. Diabetes (1986) 35: 530‐545DCCT Researctrial. Diabetes (1997) 46: 271‐286 S.B. Evans, C.W. Wilkinson, K. Bentson, P. Gronbeck, A. Zavosh, and D.P. FiglewicPVN activation is suppressed by repeated hypoglyce
93

Chapter 6 – HAAF in rats
20. S.B. Evans, C.W. Wilkinson, P. Gronbeck, J.L. Bennett, G.J. Taborsky, and D.P. Figlewicz; Inactivation of the PVN during hypoglycemia partially simulates hypoglycemia‐associated autonomic failure. American Journal of Physiology (2003)
21. pairment of
22.
24. . Akpan, R.L. Gingerich, G.J. Taborsky, and D.L.
s to mans.
26. n; A rapid method for the determination of glucose in blood and urine.
27. ffects of ulation in
28. vein
07) 293:
30. S.M. Genuth, J.M. Lachin, T.J. Orchard, P.
53
cemia‐associated autonomic
32. emia and is
33.
ia. Physiology & Behavior (2006) 87: 700‐706
284: R57‐R65 D.E. Flanagan, T. Keshavarz, M.L. Evans, S. Flanagan, X. Fan, R.J. Jacob, and R.S. Sherwin; Role of corticotrophin‐releasing hormone in the imcounterregulatory responses to hypoglycemia. Diabetes (2003) 52: 605‐613 J.E. Gerich, M. Mokan, T.F. Veneman, M.T. Korytkowski, and A. Mitrakou; Hypoglycemia unawareness. Endocrine Reviews (1991) 12: 356‐371
23. P.A. Goldberg, R. Weiss, R.J. McCrimmon, E.V. Hintz, J.D. Dziura, and R.S. Sherwin; Antecedent hypercortisolemia is not primarily responsible for generating hypoglycemia‐associated autonomic failure. Diabetes (2006) 55: 1121‐1126 P.J. Havel, S.J. Parry, J.S. Stern, J.OCurry; Redundant parasympathetic and sympathoadrenal mediation of increased glucagon secretion during insulin‐induced hypoglycemia in conscious rats. Metabolism (1994) 43: 860‐866
25. S.R. Heller and P.E. Cryer; Reduced neuroendocrine and symptomatic responsesubsequent hypoglycemia after 1 episode of hypoglycemia in nondiabetic huDiabetes (1991) 40: 223‐226 W.S. HoffmanJournal of Biological Chemistry (1937) 120: 51‐55 K. Inouye, K. Shum, O. Chan, J. Mathoo, S.G. Matthews, and M. Vranic; Erecurrent hyperinsulinemia with and without hypoglycemia on counterregdiabetic rats. American Journal of Physiology (2002) 282: E1369‐E1379 A.V. Matveyenko, M. Bohland, M. Saberi, and C.M. Donovan; Portalhypoglycemia is essential for full induction of hypoglycemia‐associated autonomic failure with slow‐onset hypoglycemia. American Journal of Physiology (20E857‐E864
29. V.P. McGregor, S. Banarer, and P.E. Cryer; Elevated endogenous cortisol reduces autonomic neuroendocrine and symptom responses to subsequent hypoglycemia. American Journal of Physiology (2002) 282: E770‐E777 D.M. Nathan, P.A. Cleary, J.Y. Backlund,Raskin, B. Zinman, and DCCT/EDIC Research Group; Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. New England Journal ofMedicine (2005) 353: 2643‐26
31. B. Raju, V.P. McGregor, and P.E. Cryer; Cortisol elevations comparable to those that occur during hypoglycemia do not cause hypoglyfailure. Diabetes (2003) 52: 2083‐2089 C. Rattarasarn, S. Dagogo‐Jack, J.J. Zachwieja, and P.E. Cryer; Hypoglycemia‐induced autonomic failure in IDDM is specific for stimulus of hypoglycnot attributable to prior autonomic activation. Diabetes (1994) 43: 809‐818 N.M. Sanders, D.P. Figlewicz, G.J. Taborsky, C.W. Wilkinson, W. Daumen, and B.E. Levin; Feeding and neuroendocrine responses after recurrent insulin‐induced hypoglycem
34. N.M. Sanders and S. Ritter; Acute 2DG‐induced glucoprivation or dexamethasoneabolishes 2DG‐induced glucoregulatory responses to subsequent glucoprivation. Diabetes (2001) 50: 2831‐2836
94

Chapter 6 – HAAF in rats
35. N.M. Sanders and S. Ritter; Repeated 2‐deoxy‐D‐glucose‐induced glucoprivation attenuates Fos expression and glucoregulatory responses during subsequent glucoprivation. Diabetes (2000) 49: 1865‐1874 K. Shum, K. Inouye, O. Chan, J. 36. Mathoo, D. Bilinski, S.G. Matthews, and M. Vranic;
455‐
for
39. es the glucose sensitivity of
40. quent sampling of blood and continuous infusion of 3‐
41. omic mediation of glucagon secretion
42. ‐jade staining and blunted adrenomedullary response to hypoglycemia after
)
43. ffect of
hormone responses during hypoglycemia in normal humans.
44. in l of Clinical Endocrinology &
Effects of antecedent hypoglycemia, hyperinsulinemia, and excess corticosterone on hypoglycemic counterregulation. American Journal of Physiology (2001) 281: EE465
37. F. Smedes, J.C. Kraak, and H. Poppe; Simple and fast solvent extraction systemselective and quantitative isolation of adrenaline, noradrenaline and dopamine fromplasma and urine. Journal of Chromatography (1982) 231: 25‐39
38. D. Smith and S.A. Amiel; Hypoglycaemia unawareness and the brain. Diabetologia (2002) 45: 949‐958 Z.T. Song and V.H. Routh; Recurrent hypoglycemia reducglucose‐inhibited neurons in the ventromedial hypothalamus nucleus. American Journal of Physiology (2006) 291: R1283‐R1287 A.B. Steffens; A method for frefluids in the rat without disturbing the animal. Physiology & Behavior (1969) 4: 83836 G.J. Taborsky, B. Ahren, and P.J. Havel; Autonduring hypoglycemia. Implications for impaired alpha‐cell responses in type 1 diabetes. Diabetes (1998) 47: 995‐1005 N.C. Tkacs, Y. Pan, R. Raghupathi, A.A. Dunn‐Meynell, and B.E. Levin; Cortical Fluorononcoma hypoglycemia in rats. Journal of Cerebral Blood Flow & Metabolism (200525: 1645‐1655 T. Veneman, A. Mitrakou, M. Mokan, P.E. Cryer, and J. Gerich; Ehyperketonemia and hyperlacticacidemia on symptoms, cognitive dysfunction, and counterregulatory Diabetes (1994) 43: 1311‐1317 T.F. Veneman and D.W. Erkelens; Clinical review 88: hypoglycemia unawareness noninsulin‐dependent diabetes mellitus. JournaMetabolism (1997) 82: 1682‐1684
95

Chapter 6 – HAAF in rats
96

Chapter 7
General discussion
The more I learn, the more I realize I donʹt know. The more I realize I donʹt know, the more I want to learn.
‐ Albert Einstein
97

98

Chapter 7 – General discussion
Chapter 7 General discussion The work presented in this thesis focused on the counterregulatory responses to hypoglycemia in rats, and the changes in those due to recurrent hypoglycemia. The first section of the thesis addressed the counterregulatory responses and the importance of insulin (Chapter 2) as well as the role of the nutritional state and other energy substrates (Chapters 2 and 3). The second section focused on the role of the central nervous system in the regulation of these counterregulatory responses, by studying the activation of specific brain areas (Chapter 4) or pharmacological blockade of these areas (Chapter 5). The third and final thesis section described the development of a rat model for recurrent hypoglycemia and the associated autonomic failure (Chapter 6).
Section I – Counterregulation, insulin, and the nutritional state
Insulin In Chapter 2, the counterregulatory responses to insulin‐induced hypoglycemia were investigated at different doses of insulin. The results describe in detail the glucagon, catecholamine, and corticosterone responses in rats subjected to hypoglycemia. One of the most important results is that, both in the fed and in the fasted state, higher insulin doses resulted in similar glucose levels but higher counterregulatory responses. From this we conclude that insulin plays a major role in the regulation of the counterregulatory responses to hypoglycemia, which has already been suggested in studies in humans (12, 21, 31). It is not known whether insulin acts directly on the counterregulatory responses, or whether it affects them indirectly through another mechanism (see below). A direct action of insulin on the regulation of the counterregulatory responses would assume that insulin acts directly on the pancreas (glucagon), the adrenal medulla (catecholamines), and/or the brain centers that control these organs. Since insulin is a potent inhibitor of glucagon release, a direct activation of the glucagon response by exogenous insulin can be ruled out. Similarly there is no evidence that secretion of adrenaline from the adrenal medulla is stimulated by insulin. In contrast, a direct insulin effect on the nervous system seems much more likely. As one of the key centers of the autonomic nervous system, the brain is strongly involved in glucose homeostasis (41, 56), is responsive to insulin (36, 42, 57), and reacts differently to hyperinsulinemic euglycemia and hyperinsulinemic hypoglycemia (Chapter 4)). Furthermore it has been shown that insulin can modify noradrenergic neurotransmission by inhibiting noradrenaline reuptake (5), which could augment noradrenaline‐mediated responses such as those in the hypothalamus (discussed later in this chapter). It is therefore very well possible that insulin directly modulates the counterregulatory responses to hypoglycemia by acting on the neural circuits controlling peripheral hormone secretion. This hypothesis presumes that exogenous insulin during
99

Chapter 7 – General discussion
hypoglycemia enterssupported by thcounterregulation to hypogly
the brain (50, 55) and affects these networks, an assumption now e finding that mice lacking brain insulin receptors show defective
cemia (15).
There are a couple of mechanisms that may underlie a possible indirect action of sulin on the regulation of the counterregulatory responses.
lin
nt for ls
n of n (26, 59), and perhaps not
ue to a direct effect of exogenous insulin on the pancreatic beta cells. its effects
, rterial/venous differences, or the speed of the decline in glucose levels). Some of these parameters may be recognized by the brain and thereby influence the counterregulatory
s to insulin‐induced hypoglycemia. It is for example known that a drug that inhibits lucose utilization (the fructose analogue 2,5‐anhydromannitol) does not decrease blood lucose
al
in
Finally, higher insulin levels might have affected the bodyʹs glucosensors, so that the ame b
d insulin
e a er
,
in One consequence of exogenous administration of insulin is that endogenous insusecretion is inhibited. Reduced endogenous insulin release removes the inhibition of glucagon secretion from the alpha cells and could therefore be an important determinathis counterregulatory response (19). Indeed it is hypothesized that intra‐islet insulin levedrop during insulin‐induced hypoglycemia and thereby allow glucagon to be released (24, 59). It should be noted that estimatedly 75% of the glucagon response to hypoglycemia disappears when both branches of the autonomic nervous system are blocked (25). Hence the major part of the glucagon response seems to be due to a nervous stimulatioglucagon secretion, and/or a nervous inhibition of insulin secretiod Insulin may also indirectly affect the counterregulatory responses throughon peripheral glucose homeostasis parameters (e.g. intracellular glucose levelsa
responsegg levels but leads to counterregulatory responses similar to those during insulin‐induced hypoglycemia. This means that the brain receives information on decreased intracellular energy supply (due to the decreased glucose utilization), resulting in counterregulatory responses to restore energy balance (29, 43). It can be argued that the different insulin doses in studies like the one presented in this thesis may have led to locdifferences in peripheral glucose homeostasis (with hepatic intracellular energy availability as an example, or a factor such as speed of decline in glucose levels (35)), which may explawhy different insulin doses but similar blood glucose levels were still accompanied by different counterregulatory responses. s lood glucose level may result in different counterregulatory responses. Those glucosensors are located in the hepatic portal vein area and in the brain (18, 39), anis known to augment the firing response of ventromedial hypothalamic neurons to glucose levels (for review see Ref. 64), which is in agreement with this hypothesis explaining insulinʹs effect on the counterregulatory responses to hypoglycemia. Our data confirm the observation that different glucose threshold levels exist for activation of glucagon, adrenaline, and other counterregulatory responses (37). This means that a hierarchy exists for the counterregulatory responses to hypoglycemia, whermoderate reduction of glucose levels already elicits a glucagon response, while greatreductions of glucose levels are needed to elicit an adrenaline response. The current studies suggest this hierarchy not only exists for glucose levels, but alsofor insulin. At similar glucose levels, a low dose of insulin elicits a glucagon response onlywhile higher insulin doses are needed to elicit an adrenaline response. This suggests that
100

Chapter 7 – General discussion
ʺinsulin thresholdsʺ may exist as well – or that the known glucose thresholds for counterregulatory responses are not fixed, but depend on the ambient insulin level The activation and magnitude of the
s. counterregulatory responses to insulin‐induced
ypoglycemia therefore appear to be triggered by the decrease in glucose levels combined ith th
e
n t
d corticosterone
te
ter of
e liver , the liver
d y inhibition of fatty acid oxidation). This lipoprivic
id emia, indicates a rapid
nd immediate integration of the information about decreasing blood glucose levels with the
ive to ome
hw e increase in insulin levels.
The nutritional state Chapter 2 also addressed the effects of fasting on the counterregulation to hypoglycemia. Counterregulatory responses were greatly enhanced after fasting, which is inagreement with other studies showing increased responses to metabolic challenges in thfasting state (61, 62). The increased counterregulatory responses observed in our studies cafirst and foremost be linked to the lower glucose levels in the fasted condition, both abaseline and during administration of insulin. However, the reduced nutritional state by itself also plays a role, which is among others reflected by the very rapiresponse, which already started at glucose and insulin levels that do not produce a corticosterone response in the fed condition. The mechanism by which fasting enhances the counterregulatory responses to hypoglycemia in this way is not known. The enhanced insulin sensitivity in the fasted stamight explain the increased stimulatory effect of insulin on the counterregulatory responses (as described in the previous paragraph). It may also be possible that periods of fasting althe sensitivity of the glucosensors that respond to hypoglycemia, so that the magnitudethe counterregulatory responses at a given glucose level is increased. Furthermore, thmight report a decreased combined energy status to the brain. As discussed beforecan give rise to afferent signals about energy content (existing as ATP) (43), and it can behypothesized that the reduced glycogen availability negatively affects ATP availability andthereby further enhances the afferent signaling from the liver to the brain. The latter hypothesized mechanism could also help explain the results described in Chapter 3. In that study, rats were subjected to hypoglycemia in a situation with reduceavailability of energy from fatty acids (bcondition also greatly enhanced the counterregulatory responses to hypoglycemia, at higher blood glucose levels than in the rats receiving hypoglycemia alone. While the fasting described in Chapter 2 started 48 hours before the hypoglycemic episode, the blockade of fatty acid oxidation in Chapter 3 was acute, and gradual adaptations to the reduction in energy availability can therefore be excluded. The fact that this acute effect on fatty acoxidation still enhanced the counterregulatory responses to hypoglycainformation about the changed nutritional state (in this case in the form of reduced fatty acidoxidation). This again could suggest the aforementioned involvement of the liver and brain. Both the brain (18, 32, 45) and the liver (28, 39) are glucose‐sensitive, the liver is sensitlipoprivation (44, 49), and in addition the liver contains the glycogen reserves which becdepleted during fasting.
101

Chapter 7 – General discussion
The signals about glucoprivation and lipoprivation could then be integratepossible sites: the liver or the brain.
d at two
ing in a synergistically increased activity of the afferent epatic vagal nerves. This is supported by data in the literature that have shown that a
combination of glucoprivation and lipoprivation synergistically increased food intake (17) energy status (29). This means that the liver indeed may serve as an
tegration site for the signals about glucoprivation and lipoprivation, reporting a combined ignal t on are
ng
dy
oprivation. The neuronal network involved in tty ac d in
n
ses to hypoglycemia were investigated. It is well‐known that the rain – and especially the hypothalamus – is strongly involved in the control of energy alance (33, 54, 63). This certainly also includes glucose homeostasis, since both endogenous lucose production and the secretion of glucoregulatory hormones are coordinated by the
Firstly, it could be possible that the greatly potentiated responses to the combination of glucoprivation and lipoprivation may have been solely caused by the liver detecting a reduction in both fuel sources, resulth
and decreased hepaticins o the brain. It does not explain however, why the responses to glucoprivatidifferent than those to lipoprivation, which makes it less likely that the liver is the only energy substrate sensing organ. The second possible place for the integration of the two signals is the brain. It is tenable that the brain is the key candidate for this, integrating the lipoprivic signal arisifrom afferent vagal liver nerves with a glucoprivic signal arising from the hypothalamus orthe brain stem. This would imply that different neuronal networks exist for homeostaticcontrol of the different energy substrates (49). This may also help explain why the boreacts differently to glucoprivation than to lipfa id homeostasis would then be interconnected to the neuronal networks involveglucose homeostasis, bidirectionally modulating the responsiveness of each other. It has been indicated that indeed separate neuron populations in the hypothalamus are activated during glucoprivation versus lipoprivation (51), which supports this hypothesis. Additionally or alternatively, the brain itself could be sensitive to both glucoprivation and lipoprivation. It is known that the brain can use other energy substrates than glucose, such as ketone bodies and lactate (27, 40), and there are indications that it can also metabolize fatty acids (53), so it is very well possible that some neurons can react to changes in fat oxidation, perhaps even the same neurons that sense hypoglycemia. It has now become clear that the activation of the counterregulatory responses not only depends on glucose levels and on insulin levels, but also on the availability of other energy sources. The most important conclusion from this section is therefore that the activation and magnitude of the counterregulatory responses to insulin‐induced hypoglycemia appear to be triggered by the decrease in glucose levels, the increase iinsulin levels, and the decrease in other energy sources.
Section II – Central nervous mechanisms
Activation of noradrenergic pathways In the second part of this thesis, the central nervous mechanisms involved in the counterregulatory responbbg
102

Chapter 7 – General discussion
autonomic nervous system (48, 54, 58). As mentioned before, the hypothalamus seems to play a major role in the regulation of the counterregulatory responses to hypoglycemia (4). here a
H
– an
‐
in noradrenaline (and GABA) levels in the VMH
r
y the VN is indeed one of the steps in the activation of the counterregulatory responses to
re ibited the
noradrenergic signal to the PVN
escribed in Chapter 4 is indeed important in the counterregulation to hypoglycemia. This is in agreement with the previously published findings that anesthetizing the whole PVN
refines those findings to α‐noradrenergic athways. PVN administration of the α2‐adrenergic antagonist furthermore prevented the
response, in line with the known role of α2‐drenergic signaling in food intake (6, 23, 38). This again suggests that the counterregulation hypo ses
. gin
(7).
T re several lines of evidence for this. It is well known that the ventromedial hypothalamus (VMH) contains glucosensors, and local glucose administration into the VMduring hypoglycemia abolishes the counterregulatory responses (3). In addition, the hypothalamus receives signals from other glucose‐sensitive areas, such as the hindbrainarea also involved in the counterregulatory responses to hypoglycemia and glucoprivation (2). Noradrenaline is the main neurotransmitter in this neuronal pathway between the hindbrain and the hypothalamus, and we confirmed this in Chapter 4 by the elevation of noradrenaline levels in microdialysis samples from the PVN and the VMH during insulininduced hypoglycemia. As expected, the increasedisappeared when the ratsʹ blood glucose levels were kept normal throughout the experimental period by intravenous infusion of glucose. There was however still a noradrenaline response in the PVN, which therefore likely is due to the increased plasma insulin levels – confirming a possible role for insulin in the activation of the counterregulatory responses, as suggested in the previous paragraphs. It may therefore behypothesized that the VMH is mainly involved in responses to low blood glucose levels (in line with its known glucosensory role (3)), while the PVN is mainly involved in the integration of information on glucose levels with information on insulin and perhaps otheparameters, and the subsequent activation of the appropriate responses (in line with its known integratory and coordinating role (30, 34)).
Blockade of noradrenergic pathways To substantiate the notion that the observed noradrenergic signal received bPhypoglycemia, it was investigated whether inhibition of these signals would affect the counterregulatory responses. As described in Chapter 5, this was indeed the case. Rats received either an α1‐ or an α2‐adrenergic antagonist into the PVN, whereafter they wesubjected to insulin‐induced hypoglycemia. Treatment with these antagonists inhsympathoadrenal counterregulatory responses to hypoglycemia, and resulted in furtherreduced blood glucose levels – together indicating that thed
impedes the counterregulatory responses (14), and p
expected compensatory increased food intakeato glycemia is a complex and tightly‐controlled system, and that the different respon(e.g. adrenaline secretion and food intake initiation) are controlled by different mechanismsCurrent investigations are elucidating more details of these mechanisms, such as the oriof the noradrenergic signals observed in the hypothalamus during hypoglycemia (13, 20) and the different neurotransmitters involved in the different counterregulatory responses
103

Chapter 7 – General discussion
Together these data show that the low glucose levels and the high insulin levels associated with insulin‐induced hypoglycemia lead to distinct noradrenergic signaparaventricular hypothalamus in rats. Blocking these noradrenergic signals impairs counterregulatory responses to insulin‐induced hypoglycemia, showing that they arefunctional part of the mechanisms activating the counterregulatory responses.
Section III – Recurrent hypoglycemia
ls to the
a
at mo
by
)
ponses.
e severe hypoglycemic episodes occur ith almost no warning signals. As a result, patients fear the frequent hypoglycemic
insulin therapy, and do not achieve optimal to find out why and how HAAF
evelops. This requires suitable animal models; and the aim of the studies described in
as
es at
poglycemia. Hypoglycemia by itself induces food intake, and can result in total 4h foo t
en
R del for HAAF The final section of this thesis addressed the issue of autonomic failure causedrecurrent hypoglycemia. Recurrent hypoglycemia decreases the counterregulatory responses tohypoglycemia, a phenomenon called Hypoglycemia‐Associated Autonomic Failure (HAAF(1, 9, 11). HAAF impairs the counterregulatory responses to hypoglycemia, so that a further reduction of blood glucose levels is needed to trigger these important autonomic resAt the same time, the awareness of hypoglycemia (by means of sensations such as sweating,trembling, increased pulse) turns into hypoglycemia unawareness (8, 22). This causes a vicious circle, ultimately leading to a situation wherwepisodes, do not comply with the prescribedglucose control. It is therefore of great importancedChapter 6 was thus to develop and characterize such a model. As described in that chapter, protocols used to induce HAAF in humans – suchone or two antecedent hypoglycemic episodes on the day before the test episode – also induced HAAF in rats. HAAF was either evident as reduced counterregulatory responsa given glucose level, or as unchanged counterregulatory responses but at a lower glucoselevel than in controls. The glucagon response seemed to be somewhat less susceptible to recurrent hypoglycemia than the adrenaline response, which has now also been shown inother studies (16, 52, 60). Finally it was remarkable that there were pronounced differences between individual animals in the development of HAAF. In contrast to the hormonal counterregulatory responses, food intake – the behavioral counterregulatory response to hypoglycemia – was not much affected by recurrent hy2 d intake being greater than on a control day, but recurrent hypoglycemia did noaffect this response, which recently was confirmed by Sanders et al. (46). Interestingly, whanimals could choose between carbohydrate‐ and fat‐enriched chow, hypoglycemia shifted their nutrient preference towards carbohydrates. Again, this response to hypoglycemia did not change after multiple hypoglycemic episodes, confirming the differential and separate organization of the distinct counterregulatory responses to hypoglycemia described in the previous paragraph.
104

Chapter 7 – General discussion
HAAF is GAAF?
ther as
y similar to e responses to hypoglycemia – i.e. secretion of glucagon, adrenaline, and corticosteroids
2‐DG administrations reduce the G administration (47), suggesting that
lucoprivation in general (rather than e.g. insulin‐induced hypoglycemia only) can induce autonomic failure. In the last study described in Chapter 6, it was investigated whether
‐DG administrations reduced the counterregulatory responses to ypoglycemia, just like antecedent recurrent hypoglycemia does (as shown in Experiment 3 Chap ial
of Hypoglycemia‐Associated Autonomic Failure. In other words, AAF
an
e precise
that glucose levels may be own of the
into the ventromedial and paraventricular hypothalamus, and that harmacological blockade of this signal in the paraventricular nucleus impairs the
Finally, the most interesting results described in Chapter 6 addressed the question whether HAAF is only related to insulin‐induced hypoglycemia, or perhaps also to oforms of glucoprivation. Generally, the responses to other forms of glucoprivation (suchby the glucose antimetabolites 2‐deoxyglucose or 2,5‐anhydromannitol) are verth(49). Furthermore, it is known that antecedent counterregulatory responses to subsequent 2‐Dg
antecedent recurrent 2hin ter 6). This was indeed the case – suggesting that glucoprivation might be the crucfactor in the developmentH can probably be induced by any form of glucoprivation, and affects the counterregulatory responses to any form of glucoprivation. It might therefore not only be a Hypoglycemia‐Associated Autonomic Failure, but also more generally a Glucoprivation‐Associated Autonomic Failure. This finding may also help pinpoint the mechanistic background of the development of this autonomic failure. Since 2‐DG can induce this failure as well, exogenous insulin clikely be ruled out as an essential causal factor. The general glucoprivation‐linked nature ofthe defect together with considerations about the likeliness of alternative hypothesis suggestthe brain as the probable site for this defect, as that is the place where all glucose‐related signals are integrated and lead to activation of counterregulatory responses (10). Threason why the brain changes counterregulatory responses after recurrent hypoglycemiaremains to be resolved.
Conclusions and perspective The studies presented in the three sections of this thesis have given several new insights into the counterregulation to insulin‐induced hypoglycemia in rats. It was found that a complex but well‐coordinated control of the individual counterregulatory responses exists, both in time and in required magnitude. It appeared defended above a certain level, independent of the exogenous insulin dose. It was shthat insulin by itself may be a significant contributor to the activation and magnitudecounterregulatory responses. Also, the energetic state of the organism was of importance for these counterregulatory responses to hypoglycemia. These findings support the concept ofʺrelative hypoglycemiaʺ, comprising that the effects and severity of hypoglycemia depend on many separate factors, including glucose levels, (exogenous) insulin levels, and the availability of other energy sources such as glycogen and fatty acids. The brain mechanisms involved in these counterregulatory responses were also subject of investigation. It was shown that insulin‐induced hypoglycemia activates noradrenergic signalsp
105

Chapter 7 – General discussion
counterregulatory responses to hypoglycemia, suggesting that the detection of ypoglycemia is relayed by noradrenergic signals through the paraventricular
more
glucagon secretion. American Journal of Physiology (2007)
urnal of Clinical Investigation (1994) 93: 1677‐1682
. F.T.J. Boyd, D.W. Clarke, T.F. Muther, and M.K. Raizada; Insulin receptors and insulin modulation of norepinephrine uptake in neuronal cultures from rat brain.
ry (1985) 260: 15880‐15884 . T. Bungo, T. Higaki, H. Ueda, and M. Furuse; Intracerebroventricular administration
)
0.
hhypothalamus to the autonomic nervous system. Finally, the issue of recurrent hypoglycemia and the associated autonomic failure was investigated. It was shown that this autonomic failure can be evoked in rats, and that the defect can also be induced by other glucoprivic agents. It is suggested therefore that the defect is a result of alterations in brain areas involved in the counterregulation to glucoprivation. However, a definitive mechanism hasnʹt been identified yet, andresearch will be needed to shed light onto the causes for developing Hypoglycemia‐Associated Autonomic Failure.
References 1. S.A. Amiel, R.S. Sherwin, D.C. Simonson, and W.V. Tamborlane; Effect of intensive
insulin therapy on glycemic thresholds for counterregulatory hormone release.Diabetes (1988) 37: 901‐907
2. S.F. Andrew, T.T. Dinh, and S. Ritter; Localized glucoprivation of hindbrain sites elicits corticosterone and292: R1792‐R1798
3. M.A. Borg, R.S. Sherwin, W.P. Borg, W.V. Tamborlane, and G.I. Shulman; Local ventromedial hypothalamus glucose perfusion blocks counterregulation during systemic hypoglycemia in awake rats. Journal of Clinical Investigation (1997) 99: 361‐365
4. W.P. Borg, M.J. During, R.S. Sherwin, M.A. Borg, M.L. Brines, and G.I. Shulman; Ventromedial hypothalamic lesions in rats suppress counterregulatory responses tohypoglycemia. Jo
5
Journal of Biological Chemist6
of octopamine stimulates food intake of chicks through alpha(2)‐adrenoceptor. Physiology & Behavior (2002) 76: 575‐578
7. O. Chan, W. Zhu, Y. Ding, R.J. McCrimmon, and R.S. Sherwin; Blockade of GABA(Areceptors in the ventromedial hypothalamus further stimulates glucagon and sympathoadrenal but not the hypothalamo‐pituitary‐adrenal response to hypoglycemia. Diabetes (2006) 55: 1080‐1087
8. W.L. Clarke, L.A. Gonder‐Frederick, F.E. Richards, and P.E. Cryer; Multifactorial origin of hypoglycemic symptom unawareness in IDDM. Association with defectiveglucose counterregulation and better glycemic control. Diabetes (1991) 40: 680‐685
9. P.E. Cryer; Hypoglycemia‐associated autonomic failure in diabetes. American Journal of Physiology (2001) 281: E1115‐E1121
1 P.E. Cryer; Mechanisms of Hypoglycemia‐Associated Autonomic Failure and its component syndromes in diabetes. Diabetes (2005) 54: 3592‐3601
11. P.E. Cryer; Iatrogenic hypoglycemia as a cause of hypoglycemia‐associated autonomic failure in IDDM. A vicious cycle. Diabetes (1992) 41: 255‐260
106

Chapter 7 – General discussion
12. S.N. Davis, R.E. Goldstein, J. Jacobs, L. Price, R. Wolfe, and A.D. Cherrineffects of differing insulin levels on the hormonal and metabolic responsequivalent hypoglycemia in normal human
gton; The e to
s. Diabetes (1993) 42: 263‐272 3. gic
f
.P.
(2003)
5. S.J. Fisher, J.C. Bruning, S. Lannon, and C.R. Kahn; Insulin signaling in the central nervous system is critical for the normal sympathoadrenal response to
ycemia. Diabetes (2005) 54: 1447‐1451 6. D.E. Flanagan, T. Keshavarz, M.L. Evans, S. Flanagan, X. Fan, R.J. Jacob, and R.S.
17. f, and I. Ramirez; Integrated metabolic control of food
18. nd A.D. Cherrington; Counterregulation during hypoglycemia is
19.
bolism (2000) 49: 950‐953 gic
:
23. itz; Postsynaptic alpha 2‐noradrenergic
‐19 24. d C.
lin for the glucagon response to
25.
1994. Endocrine
27. dividual brain regions. Science (1979) 205: 325‐327
1 M.G. De Vries, M.A. Lawson, and J.L. Beverly; Hypoglycemia‐induced noradreneractivation in the VMH is a result of decreased ambient glucose. American Journal oPhysiology (2005) 289: R977‐R981
14. S.B. Evans, C.W. Wilkinson, P. Gronbeck, J.L. Bennett, G.J. Taborsky, and DFiglewicz; Inactivation of the PVN during hypoglycemia partially simulates hypoglycemia‐associated autonomic failure. American Journal of Physiology284: R57‐R65
1
hypogl1
Sherwin; Role of corticotrophin‐releasing hormone in the impairment of counterregulatory responses to hypoglycemia. Diabetes (2003) 52: 605‐613 M.I. Friedman, M.G. Tordofintake. Brain Research Bulletin (1986) 17: 855‐859 R.T. Frizzell, E.M. Jones, S.N. Davis, D.W. Biggers, S.R. Myers, C.C. Connolly, D.W. Neal, J.B. Jaspan, adirected by widespread brain regions. Diabetes (1993) 42: 1253‐1261 B. Fruehwald‐Schultes, W. Kern, J. Born, H.L. Fehm, and A. Peters; Comparison ofthe inhibitory effect of insulin and hypoglycemia on insulin secretion in humans. Meta
20. K.R. Fugo, M.A. Lawson, and J.L. Beverly; Ibotenic acid lesions reduce noradreneractivation in ventromedial hypothalamus during hypoglycemia. Brain Research (2006) 1111: 105‐110
21. P. Galassetti and S.N. Davis; Effects of insulin per se on neuroendocrine and metabolic counter‐regulatory responses to hypoglycaemia. Clinical Science (2000) 99351‐362
22. J.E. Gerich, M. Mokan, T.F. Veneman, M.T. Korytkowski, and A. Mitrakou; Hypoglycemia unawareness. Endocrine Reviews (1991) 12: 356‐371 C.K. Goldman, L. Marino, and S.F. Leibowreceptors mediate feeding induced by paraventricular nucleus injection of norepinephrine and clonidine. European Journal of Pharmacology (1985) 115: 11N.R. Gosmanov, E. Szoke, Z. Israelian, T. Smith, P.E. Cryer, J.E. Gerich, anMeyer; Role of the decrement in intraislet insuhypoglycemia in humans. Diabetes Care (2005) 28: 1124‐1131 P.J. Havel, S.J. Parry, J.S. Stern, J.O. Akpan, R.L. Gingerich, G.J. Taborsky, and D.L. Curry; Redundant parasympathetic and sympathoadrenal mediation of increased glucagon secretion during insulin‐induced hypoglycemia in conscious rats. Metabolism (1994) 43: 860‐866
26. P.J. Havel and G.J. Taborsky; The contribution of the autonomic nervous system toincreased glucagon secretion during hypoglycemic stress: update Reviews (1994) 2: 201‐204 R.A. Hawkins and J.F. Biebuyck; Ketone bodies are selectively used by in
107

Chapter 7 – General discussion
28. A.L. Hevener, R.N. Bergman, and C.M. Donovan; Portal vein afferents are critical fothe sympathoadrenal response to hypoglycemia. Diabetes (2000) 49: 8‐12 H. Ji, G. Graczyk‐Milbrandt, and M.I. Friedman; Metabolic inhibitors syne
r
29. rgistically
30. The paraventricular nucleus: An e
31. , hormonal responses to hypoglycemia in patients with IDDM. Diabetes
32. iabetes, rimental (2002) 15: 274‐281
34. ical
35. . Donovan; Portal vein
in
(1979) 236: R312‐R321
mptoms, and cerebral dysfunction. American Journal of
38. amic alpha1‐ and alpha2‐adrenoceptors and food intake in rats.
39. D‐glucose
40.
41. in Clinical Nutrition
42.
43. sbakken, and M.I. Friedman; Hepatic phosphate
44. gal sensory neurons are required for lipoprivic but not 1
decrease hepatic energy status and increase food intake. American Journal of Physiology (2000) 278: R1579‐R1582 M.J. Kenney, M.L. Weiss, and J.R. Haywood;important component of the central neurocircuitry regulating sympathetic nervoutflow. Acta Physiologica Scandinavica (2003) 177: 7‐15 D. Kerr, M. Reza, N. Smith, and B.A. Leatherdale; Importance of insulin in subjectivecognitive, and(1991) 40: 1057‐1062 B.E. Levin; Glucosensing neurons: The metabolic sensors of the brain? DNutrition and Metabolism ‐ Clinical and Expe
33. B.E. Levin and V.H. Routh; Role of the brain in energy balance and obesity. American Journal of Physiology (1996) 271: R491‐R500 Z.L. Liposits; Ultrastructure of hypothalamic paraventricular neurons. CritReviews in Neurobiology (1993) 7: 89‐162 A.V. Matveyenko, M. Bohland, M. Saberi, and C.Mhypoglycemia is essential for full induction of hypoglycemia‐associated autonomic failure with slow‐onset hypoglycemia. American Journal of Physiology (2007) 293: E857‐E864
36. M.L. McCaleb, R.D. Myers, G. Singer, and G. Willis; Hypothalamic norepinephrine the rat during feeding and push‐pull perfusion with glucose, 2‐DG, or insulin. American Journal of Physiology
37. A. Mitrakou, C. Ryan, T. Veneman, M. Mokan, T. Jenssen, I. Kiss, J. Durrant, P.E. Cryer, and J. Gerich; Hierarchy of glycemic thresholds for counterregulatory hormone secretion, syPhysiology (1991) 260: E67‐E74 A. Morien, V.M. Cassone, and P.J. Wellman; Diurnal changes in paraventricular hypothalPharmacology Biochemistry and Behavior (1999) 63: 33‐38 D. Novin, D.A. Vanderweele, and M. Rezek; Hepatic portal 2‐deoxy‐infusion causes eating: Evidence for peripheral glucoreceptors. Science (1973) 181: 858‐860 L. Pellerin; How astrocytes feed hungry neurons. Molecular Neurobiology (2005) 32:59‐72 L. Penicaud, C. Leloup, A. Lorsignol, T. Alquier, and E. Guillod; Brain glucose sensing mechanism and glucose homeostasis. Current Opinionand Metabolic Care (2002) 5: 539‐543 D. Porte Jr.; Central regulation of energy homeostasis ‐ The key role of insulin. Diabetes (2006) 55: S155‐S160 N.E. Rawson, H. Blum, M.D. Otrapping, decreased ATP, and increased feeding after 2,5‐anhydro‐D‐mannitol. American Journal of Physiology (1994) 266: R112‐R117 S. Ritter and J.S. Taylor; Vaglucoprivic feeding in rats. American Journal of Physiology (1990) 258: R1395‐R140
108

Chapter 7 – General discussion
45. V. Routh, Z. Song, and X. Liu; The role of glucosensing neurons in the detection of hypoglycemia. Diabetes Technology and Therapeutics (2004) 6: 413‐421
46. N.M. Sanders, D.P. Figlewicz, G.J. Taborsky, C.W. Wilkinson, W. Daumen, and B.E. Levin; Feeding and neuroendocrine responses after recurrent insulin‐induced hypoglycemia. Physiology & Behavior (2006) 87: 700‐706
n
rgman, ulin uptake from plasma into
51. lockers of carbohydrate and lipid Bulletin
52. tecedent hypoglycemia, hyperinsulinemia, and excess corticosterone on
53. eroxisomal beta‐oxidation of ‐
54. intake the homeostasis of blood glucose and plasma FFA
55. n Journal of Physiology
56. s g blood glucose, plasma FFA and insulin in the development of obesity.
57. orlien, W.P. Bellingham, and G.M. Martin; Localization of CNS
58. u; Ventromedial hypothalamic stimulation
03 tion
47. N.M. Sanders and S. Ritter; Repeated 2‐deoxy‐D‐glucose‐induced glucoprivatioattenuates Fos expression and glucoregulatory responses during subsequent glucoprivation. Diabetes (2000) 49: 1865‐1874
48. D. Sandoval, D. Cota, and R.J. Seeley; The integrative role of CNS fuel‐sensing mechanisms in energy balance and glucose regulation. Annual Review of Physiology (2008) 70: 513‐535
49. A. Scheurink and S. Ritter; Sympathoadrenal responses to glucoprivation and lipoprivation in rats. Physiology & Behavior (1993) 53: 995‐1000
50. M.W. Schwartz, A. Sipols, S.E. Kahn, D.F. Lattemann, G.J. Taborsky, R.N. BeS.C. Woods, and D. Porte; Kinetics and specificity of inscerebrospinal fluid. American Journal of Physiology (1990) 259: E378‐E383 V.G. Sergeev and I.G. Akmaev; Effects of bmetabolism on expression of mRNA of some hypothalamic neuropeptides.of Experimental Biology and Medicine (2000) 130: 766‐768 K. Shum, K. Inouye, O. Chan, J. Mathoo, D. Bilinski, S.G. Matthews, and M. Vranic; Effects of anhypoglycemic counterregulation. American Journal of Physiology (2001) 281: E455‐E465 H. Singh, S. Usher, and A. Poulos; Mitochondrial and pstearic and lignoceric acids by rat brain. Journal of Neurochemistry (1989) 53: 17111718 A.B. Steffens, A.J.W. Scheurink, P.G. Luiten, and B. Bohus; Hypothalamic food regulating areas are involved in levels. Physiology & Behavior (1988) 44: 581‐589 A.B. Steffens, A.J.W. Scheurink, D. Porte, and S.C. Woods; Penetration of peripheralglucose and insulin into cerebrospinal fluid in rats. America(1988) 255: R200‐R204 A.B. Steffens, J.H. Strubbe, B. Balkan, and A.J.W. Scheurink; Neuroendocrine factorregulatinBrain Research Bulletin (1991) 27: 505‐510 L.H. Stglucoregulatory insulin receptors within the ventromedial hypothalamus. BrainResearch (1975) 96: 156‐160 M. Sudo, Y. Minokoshi, and T. Shimazenhances peripheral glucose uptake in anesthetized rats. American Journal of Physiology (1991) 261: E298‐E3
59. G.J. Taborsky, B. Ahren, and P.J. Havel; Autonomic mediation of glucagon secreduring hypoglycemia. Implications for impaired alpha‐cell responses in type 1 diabetes. Diabetes (1998) 47: 995‐1005
60. N.C. Tkacs, Y. Pan, R. Raghupathi, A.A. Dunn‐Meynell, and B.E. Levin; Cortical Fluoro‐jade staining and blunted adrenomedullary response to hypoglycemia after
109

Chapter 7 – General discussion
noncoma hypoglycemia in rats. Journal of Cerebral Blood Flow & Metabolism (200525: 1645‐1655
)
ior
us 3: R1758‐R1763
of
85‐396
System IV
61. G. van Dijk, A. Scheurink, S. Ritter, and A. Steffens; Glucose homeostasis and sympathoadrenal activity in mercaptoacetate‐treated rats. Physiology & Behav(1995) 57: 759‐764
62. R.R. Vollmer, J.J. Balcita, A.F. Sved, and D.J. Edwards; Adrenal epinephrine and norepinephrine release to hypoglycemia measured by microdialysis in consciorats. American Journal of Physiology (1997) 27
63. G. Williams, J.A. Harrold, and D.J. Cutler; The hypothalamus and the regulationenergy homeostasis: lifting the lid on a black box. Proceedings of the Nutrition Society (2000) 59: 3
64. S.C. Woods, G.J. Taborsky, and D. Porte Jr.; Central nervous system control of nutrient homeostasis. Chapter 7, Handbook of Physiology ‐ The Nervous(1984) 365‐411
110

111

Authorʹs papers and published abstracts A.J.W. Scheurink, S.D. Bouman, G. van Dijk, A.B. Steffens and B.E. Levin; Metabolic, hormonal and behavioral responses in obesity‐prone and obesity‐resistant rats. Obesity Research (1995) 3: 374s S.M. Korte, E.R. de Kloet, B. Buwalda, S.D. Bouman and B. Bohus; Antisense to the glucocorticoid receptor in hippocampal dentate gyrus reduces immobility in forced swim test. European Journal of Pharmacology (1996) 301: 19‐25 S.D. Bouman, J.E. Bruggink, A.J.W. Scheurink, J.H. Strubbe and A.B. Steffens; Fatty acid utilization influences the counterregulatory response to insulin‐induced hypoglycemia in rats. Diabetologia (1997) 40: A237 S.D. Bouman, J.E. Bruggink, A.J.W. Scheurink, J.H. Strubbe and A.B. Steffens; Hypoglycemia, glucoprivation and the development of hypoglycemia‐associated autonomic failure. Diabetologia (1998) 41: A68 S.D. Bouman, M. Keitz, J.E. Bruggink, A.J.W. Scheurink, J.H. Strubbe and A.B. Steffens; A role for paraventricular hypothalamic alpha‐adrenoceptors in the counterregulation to hypoglycemia. Diabetologia (1999) 42: A70 J.L. Beverly, M.G. de Vries, S.D. Bouman and L.M. Arseneau; Noradrenergic and GABAergic systems in the medial hypothalamus are activated during hypoglycemia. American Journal of Physiology (2001) 280: R563‐R569 M. de Vries and S. Bouman; Gevaarlijk suikertekort (ʺDangerous lack of sugarʺ). Natuur & Techniek (2001) 69: 54‐59 S.D. Bouman, S. Brugman, J.E. Bruggink, J.H. Strubbe, A.B. Steffens and A.J.W. Scheurink; The role of food intake and nutritional preference in the counterregulation to hypoglycemia in rats. Diabetologia (2000) 43: A193 S.D. Bouman, B.D. Roorda, C.L. Brand and T.B. Bödvarsdóttir; Insulin resistance and glucose intolerance in a rat strain prone to diet‐induced obesity ‐ effects of high‐fat diet and rosiglitazone. Diabetes (2002) 51: A417 S.D. Bouman, C.L. Brand and B.F. Hansen; Insulin sensitivity and glucose turnover are increased 24 hours after a single AICAR administration in normal rats, as measured by euglycemic clamp. Diabetologia (2002) 45: A193 S.D. Bouman, S. Brugman and A.J.W. Scheurink; Measuring food preference may influence energy metabolism. Changed characteristics in food intake, glucose challenge, and fasting in rats on carbohydrate‐ or fat‐enriched chow. Appetite (2003) 40: 319
112

S.D. Bouman, J.H. Strubbe, A.B. Steffens and A.J.W. Scheurink; Acutely neutralizing the sympathetic and
drenocortical counterregulatory responses. Diabetes & Metabolism (2003) 29: 4S239
etic e
(2004) 47: A43
gia (2007) 50: S21
mistry (2007) 102: 119 and Journal of Neurochemistry (2008)
olysis is important for maintenance of glutamate
eoxy‐1,4‐imino‐D‐arabinitol (DAB) as an
: Effects of glutamatergic and adrenergic agents.
lls, A. Schousboe, S.D. Bouman and H.S. Waagepetersen;
Evaluation of the lack of anorectic effect of
glucagon response during hypoglycemia in rats enhances the a S.D. Bouman, B. Ursø, C.L. Brand, B. Rolin, U. Ribel and L. Schäffer; A novel insulin mimpeptide with similar pharmacodynamic action and potency as normal insulin on glucosisposal in rats. Diabetologiad S.D. Bouman, L. Jessen, P.J. Larsen, J. Jelsing, U. Ribel, J. Sturis and C.L. Brand; Intravenousinsulin affects hypothalamic insulin receptor substrates and inhibits appetite‐stimulating europeptides at euglycaemia in normal rats. Diabetolon A.B. Walls, C.M. Heimbürger, H.M. Sickmann, S.D. Bouman, A. Schousboe and H.S. Waagepetersen; One third of glycolytic activity in astrocytes depends on the operation of thelycogen shunt. Journal of Neurocheg
104: 53 H.M. Sickmann, L.K. Bak, A. Schousboe, I. Schousboe, S.D. Bouman and H.S. aagepetersen; A functioning glycW
transport in cultured astrocytes. Journal of Neurochemistry (2007) 102: 285 A.B. Walls, H.M. Sickmann, A. Brown, S.D. Bouman, B. Ransom, A. Schousboe and H.S.aagepetersen; Characterization of 1,4‐didW
inhibitor of brain glycogen shunt activity. Journal of Neurochemistry (2008) 105: 1462‐1470 A.B. Walls, C.M. Heimbürger, S.D. Bouman, A. Schousboe and H.S. Waagepetersen; Robust lycogen shunt activity in astrocytesgNeuroscience (2009) 158: 284‐292 .M. Sickmann, A.B. WaH
Functional significance of brain glycogen in sustaining glutamatergic neurotransmission. Journal of Neurochemistry (accepted for publication) . Jessen, D.J. Clegg and S.D. Bouman;L
intracerebroventricular insulin in rats. American Journal of Physiology (submitted)
113

Dankwoord Het is niet makkelijk om een proefschrift te schrijven als je al aan een nieuwe baan begonnen bent en zelfs in een ander land. Dat is een bekend feit, desondanks valt het toch nog tegen. Maar uiteindelijk is het dan toch klaar. Of het resultaat de moeite waard is, is ae lezer om te beoordelen. Een slecht result
an aat zal echter in ieder geval niet te wijten zijn aan
gemak
kalibermunitie (de praktijk van dat laatste werd daarentegen alleen op de
oeren. Dat dit
die
hen doctoraal‐onderwerpen zijn met verve uitgevoerd door
s die
nk k.
llereerst voor het schrijven van de subsidie‐aanvraag voor dit project. Daarnaast hebben zij de eropvolgende jaren mij met raad en daad bijgestaan en zonodig gecorrigeerd. Veel van
de experimenten waren hun ideeën; en niet alleen de meeste experimenten maar ook veel van de verklaringen en interpretaties hadden er zonder hun heel anders uitgezien, evenals dit proefschrift, en ik denk ook minder interessant. Furthermore I wish to express my gratitude to Dr Lee Beverly for the kind opportunity to work in his lab at the University of Illinois at Urbana‐Champaign, and to Martin de Vries and Linda Arseneau who introduced me into the world of micro‐HPLC and home‐made brain microdialysis cannulas.
dde verzamelde data en resultaten, mede doordat dit voor een groot deel gedaan is door en met hulp van uiterst gemotiveerde en bekwame mensen, die ik dan ook uitermate dankbaar ben. Als eerste wil ik Jan Bruggink noemen, de King of Cannulas, die met evenveeleen rat van drie catheters voorziet als dat hij een pot ijzersterke koffie zet, en in ongeveer evenveel tijd. Afgezien van al het praktische werk dat hij heeft verzet voor mij en anderen, is hij ook de vraagbaak voor assay‐details, weigerachtige HPLCʹs, humor in woord en beeld, en grootschietbaan toegepast). Behalve Jan zijn er ook anderen die bij de experimenten geholpen hebben, onderandere in verband met de fameuze 8‐punts cursus Dierfysiologie, waar de deelnemendetudenten in slechts vier weken tijd een compleet experiment moeten uitvsdesondanks mogelijk is, getuigen de data in dit proefschrift (hoofdstukken 2, 3 en 6 zijn geheel of deels gebaseerd op cursus‐resultaten). Deze data zijn verzameld door Nynke Storm, Ben Lachmann, Paulina Sytsma, Sander Gielen, Sander van der Laan, Esther Streefland, Guido Krenning, Michel Romeijn en Olaf Gorter. Andere hypoglycemie‐data, niet in dit proefschrift beschreven zijn, zijn verzameld door Sylvia Brugman, Marcel Bijman, Rick Maneschijn, Agnes Berendsen, Sandra Henkelman en Jenneke Klunder. Daarnaast heb ik het genoegen gehad verschillende doctoraalstudenten te begeleiden, en samen met xperimenten op te zetten. Deze eNynke Storm, Martijn Keitz, Leonie Kamminga en Sylvia Brugman. Ondanks de streshet soms oplevert om met dertig ratten en twee of drie mensen en een strakke planning ineen klein kamertje te zitten, hoop ik dat jullie met evenveel plezier op deze tijd terugkijkenals ikzelf. Met betrekking tot het wetenschappelijke deel van het project ben ik veel daverschuldigd aan Anton Steffens, Jan Strubbe en in het bijzonder Anton ScheurinAin
114

In addition I wish to thank those of my colleagues at Novo Nordisk who have writing this thesis – especially my team members Merete, Maibritt,
ene, Tobias, and Charlotte – and Richard Carr for his interest not only in my hypoglycemia tudies
ren en voor gezelschap in de soms donkere en verlaten kelder; en Joke Poelstra, voor
financiële er –
supported me whileLs but also in myself, offering me my job already before I finished my PhD project. Er zijn veel meer mensen die dank verdienen, voor hulp bij experimenten en andere praktische zaken, samenwerking in binnen‐ en buitenland, en simpelweg al die dagelijkse contacten op de vakgroep. Op het gevaar af iemand te vergeten – waarvoor bij voorbaat mijn excuses – wil ik sommige personen met name noemen: Gerdien Korte en Debby Otjens, voor onmisbare hulp bij de vele bloedmonsteranalyses; Auke Meinema, voor assistentie bij e died
doeltreffende hulp bij administratieve en logistieke zaken. Niet alleen de resultaten in een proefschrift maar ook de tekst ervan is zoals bekend zelden het werk van slechts één persoon, maar is tot stand gekomen met aanvullingen en verbeteringen van mijn begeleiders. Daarnaast hebben de leden van de leescommissie het geheel doorgelezen en kritisch beoordeeld, waarvoor mijn welgemeende dank. De teun vs oor experimenten, congrespresentaties, reizen, en het proefschrift – in het bijzondvan het Diabetes Fonds Nederland en de European Association for the Study of Diabetes wordt eveneens gewaardeerd. Dankwoorden in proefschriften eindigen vaak met het bedanken van familie en vrienden, waardoor het misschien wat clichématig lijkt. Toch is het bereiken van een mijlpaal als deze ook een gelegenheid om dankbaar te zijn voor dingen die zo vanzelfsprekend lijken, zoals de steun van vrienden, familie en in het bijzonder ouders. Pa en ma, bedankt!
115

116

117
Counterregulation to acute and recurrent hypoglycemia in rats by Stephan D. Bouman The studies presented in this thesis were financed by the Dutch Diabetes Research Foundation and aimed to investigate the counterregulatory responses to hypoglycemia, the mechanisms controlling these responses, and the impairment in these responses after repeated exposure to hypoglycemia. It was found that the counterregulatory mechanisms are coordinated in a very intricate way, aiming to keep glucose levels above a certain minimum level. Furthermore it was shown that a noradrenergic neuronal pathway in the paraventricular hypothalamus plays an essential role herein. Finally it was shown in a number of studies with recurrent hypoglycemia that several factors influence the decrease in the counterregulatory responses. © 2008 ISBN 978‐90‐367‐3720‐3







![Hypoglycemia and Diabetes · hypoglycemia, including severe hypoglycemia, occur in people with type 2 diabetes.[25] There is no doubt that hypoglycemia can be fatal.[26] In addition](https://img.pdfslide.net/doc/110x75/5f0518c07e708231d4113f09/hypoglycemia-and-hypoglycemia-including-severe-hypoglycemia-occur-in-people-with.jpg)