Embed Size (px)
Citation preview

Course : PGPathshala-Biophysics Paper 08 : Medical Physics Module : M 32: Radiation Biology Content Writer: Dr. K. Thayalan, Dr. Kamakshi Memorial Hospital, Chennai-600100.
Quadrant I
1. Introduction
Radiobiology is a scientific discipline that studies the effects of ionizing radiation on living
systems, including cells, normal tissues and malignant cells. It helps to understand the
sequence of events and its nature after the exposure of ionizing radiation. Basically, it is
concerned about biological damage, modification and its repair. The radiobiological
studies contribute to the development of medicine, especially radiotherapy in many
ways.
Objectives
To understand radiobiological principle, which are very much essential, not only
to predict outcome, but also to use effectively a given radiation technique or
procedure.
To understand the radiation interactions with tissue and cells,
To understand radiation damage of DNA
To study survival curves and its modifying agents
To know the biological effects of radiation
2. Interaction of radiation with cell
Radiation can damage cell and result in biological effects in a multi cellular
organism. Therefore, the study of the radiation effects at cellular level is more useful to
know about the radiation damage. The time interval between the radiation exposure and
manifestation of biological effects can be divided into 3 stages namely (i) physical stage,
(ii) chemical stage, and (iii) biological stage.
2.1.Sequence of radiation events
(i).Physical stage
The physical stage refers to the interaction of charged particles and atoms and
molecules of tissues. In this stage, the bio molecules in the environment absorb the
radiation energy and undergo ionization and excitation and release electrons. These
electrons are called secondary electrons and they transfer energy to the surrounding by
further excitation, ionization and thermal heating in the medium. Its duration is about 10-
7 s and the deposition of energy is rapid and random.

(ii).Chemical stage
In the chemical stage, the damaged atoms and molecules further reacts with the
cellular components through chemical reactions. The exposed bio molecules rearrange
themselves, which results in formation of primary lesions in them. Primary lesions are
transformed into bio radicals, resulting molecular alterations. Bio radicals can also be
formed with indirect interaction of radicals with bio molecules. The structural changes
includes (i) hydrogen bond breakage, (ii) molecular degradation and (iii) inter and intra
molecular cross linking. The duration of the above event is about 10-10 s.
(iii).Biological stage
The biological stage starts with enzymatic reactions, which act on the residual
chemical damage. Majority of the lesions are repaired and lesions that are not repaired
result in cellular death or mutations in cells. Cell death may lead to organ death that
appears as clinical changes. The biological effect at cellular level includes lethality,
mitotic inhibition, division delay, chromosome aberration and induction of mutations.
These effects can create radiation sickness, resulting in delayed somatic effects in
humans.
Cell may take time to die and may undergo mitotic division before death. The
death of stem cells appears as early effects in normal tissue. After the cell killing,
compensatory cell proliferation occurs both in normal and tumour cells. At later time late
reactions appear in normal tissues. Mutation can occur in the (i) germ cells and (ii)
somatic cells. The mutation in germ cell may result in hereditary effects, whereas
cancer induction is the outcome in somatic cells. The time schedule for biological effects
is few minutes to several years.
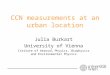
2.2. Direct and indirect action
Biological effects resulting from the direct interaction of radiation with the target
sites is called the direct action. There are critical sites or targets within the cells which
must be damaged in order to kill the cell. DNA, RNA and proteins are the common
critical targets for radiation exposure. In a direct action, the radiation interacts directly
with such critical sites and creates biological effects (Fig.1). The radiation ionizes or
excites the molecules such as DNA, RNA and protein directly. It is a dominant process
with high LET radiations such as alpha, neutrons etc.
It involves rupture of cell membrane and breaking of chromosome structure,
resulting in DNA strand breaks. The fragments of chromosomes produced in a direct
interaction, can join together to form chromosomes with abnormal structures. This is
known as chromosomal aberration. The frequency of chromosomal aberrations
increases with radiation dose and hence the magnitude of aberrations is a biological

indicator of radiation dose absorbed in human body. Chromosomal aberration analysis
(CAA) is useful in determining the radiation dose received by a person who is
accidentally exposed to high radiation dose (>100 mGy).
Fig. 1.Direct and indirect action of radiation on a DNA molecule.
Alternatively, the radiation can interact with other molecules (e.g. water) and
forms free radicals. The interaction of free radicals with critical sites may also result in
biological effects, which is called indirect action. For example, radiation interacts with
oxygen and water molecules present in the cell. These interactions produce a large
number of free radicals, which are atoms or molecules or ions with an unpaired electron
and hence are highly reactive. Since electrons are spinning, a pair of electron spins
both clockwise and anticlockwise, giving stability. Unpaired electron spins in one
direction and is unstable. Free radical has high degree of chemical reactivity and
interacts strongly with bio molecules. This is a major source of radiation damage.
Human body tissue is composed of 80% water, and the major interaction is indirect
action (66%) through water. The effect of x and gamma rays in macromolecules of living
system are mainly due to indirect interactions.
2.3. Radiation damage to DNA

DNA is the largest and most important molecule for radiation damage. Its
damage gives rise to cell killing, carcinogenesis, and mutation. The radiation induced
lesions in the DNA can be repaired successfully.
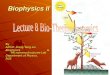
Radiation exposure to DNA gives two major effects namely (i) cross linking and
(ii) strand break (Fig.2). Cross linking may be protein-protein cross link, DNA-protein
cross link, intra strand cross link and inter strand cross link. Intra strand cross linking is
one in which cross linking occurs between bases on the same stand, e.g. formation of
adjacent thymine dimers (TT).Dimerization reduces the distance between the bases
and results in distortion (kink) of sugar–phosphate back bone. The rupture of hydrogen
bond may lead to irreversible changes in the secondary and tertiary structure of DNA
molecule, which may compromise genetic transcription and translation.
Radiation exposure also causes DNA strand break due to loss of viscosity in
DNA solutions, in addition to base change, and the DNA is degraded into smaller
fragments. As a result, there will be a decrease in molecular weight of DNA. The strand
breaks may be single strand break or double strand break. If the break is located on one
of the strand it is referred as single strand break (SSB). If two breaks are located on
opposite strands, separated by 5 bases, then it is called double strand break (DSB).
The SSB between sugar and the phosphate can rejoin, if it is not separated, but takes a
longer time. Presence of oxygen may cause peroxidation of base that prevents
rejoining. The DSB are basically genotoxic lesions that can result in chromosome
alterations. This may activate oncogenes, inactivation of tumour suppression genes or
loss of heterogeneity, resulting carcinogenesis. The SSB are mostly caused by OH
radical and easily repaired compared to DSB.
Fig.2.Radiation damage of DNA: (a) Single strand break, (b) double strand break,
(c) cross linking, and (d) rung breakage

The DSB is the result of sparse ionization pattern of the low LET radiation. A X-
ray dose of 1 Gy, may disturb the mitotic capability in 50 % of the exposed cells. All
ionizing radiations are capable of producing DSB and complex DNA damages. In low
LET radiation, about ¼ of the dose is deposited in tissue via low energy secondary
electrons (0.1-5 keV).These low energy electrons produce dense ionization tracks over
a short range, equal to the diameter of double helix strand. This may result in complex
DNA damages that are less likely to be repaired.
Though the amount of DSB lesions caused by the radiation is more, but the
number giving rise to cell kill is small. The dose of ionising radiation that gives one lethal
event per cell and leave 37% of the viable cell is called D0. The D0 value for low LET X-
ray lies between 1-2 Gy dose, which is sufficient to cause about 1000 base damages,
1000 SSB and 40 DSB per cell. SSB is of little importance, since its damage is mostly
repaired by taking a template from the opposite strand. If incorrect repair takes place in
SSB, it may lead to mutation. If both strands are broken, and are well separated, it can
also be repaired, since the two breaks are handled as two single strand breaks.
DSB is the most important damage in DNA, after radiation exposure. The
interaction of two DSB may lead to cell killing, carcinogenesis and mutation. There are
many kinds of DSB, depending upon the distance between the break and kinds of end
point. The DSB yield out 0.04 times that of SSB and it is induced linearly with dose.
Mostly DSBs are caused by single track of ionizing radiation. DSB result in cleavage of
chromatin into two pieces and is the critical lesion, responsible for cell kill. Experimental
studies reveal that DSB produced initially correlate with radiosensitivity and survival at
low dose. Whereas unrepaired or miss repaired DSB correlate with survival at higher
doses. High LET radiations are capable of producing complex DSB lesions. The
clusters of ionization and excitations that take place at the end of the secondary
electrons tracks are capable of producing multiple lesions within 20 nm range, resulting
cell death.
The DNA damage is a normal event in a cell’s life. Apart from radiation, there are
many more agents that may cause DNA damage. However, the spontaneous mutation
rate is less due to efficient repair mechanism present in the cell. The extent of DNA
damage depends upon the repair mechanism present in the organism. Eukaryotic cells
are equipped with ability to repair DSB, whereas organisms with prokaryotic cells are
not equipped. A single DSB is lethal to bacteria, whereas about 60 DSB are required to
kill a mammalian cell. Similarly, few SSBs are lethal to viruses and micro organisms,
whereas several hundred SSB are required to kill a mammalian cell. The above
difference is due to repair capacity between different organisms.

2.4. Radiation and Chromosome damage
Irradiation can damage chromosomes and delay the cell’s entry into mitosis. This
delay is dose dependent. If the cells are irradiated during the inter phase, they begin to
divide and undergo aberrations. Chromosome aberration refers to their appearance in
the first metaphase after irradiation. The stable aberrations may be carried out through
number of cell divisions, generally called chromosome aberrations. Unstable
aberrations may lead to cell death. If cells are exposed to radiation, DSB occurs in
chromosomes. The broken ends are sticky due to their unpaired bases. These broken
ends may (i) join with their original chromosome, (ii) fail to rejoin, that leads to
aberrations, or (iii) rejoin with other broken ends.
These aberrations may be chromatid or chromosome aberrations. Chromatid
aberrations are due to irradiation of cells, while they are in late interphase (G2). In this,
one arm of the sister chromatid is broken. The DNA has already doubled and the
chromosomes consist of two strands of chromatin, during irradiation. If the cells are
irradiated, while they are in early inter phase (G1) and if unrepaired, that leads to
chromosome aberrations. In this case, the chromosome is not duplicated, and the
damage is a SSB of chromatin. During the S phase an identical strand is synthesized.
This is visible in the mitosis, as identical breaks in the pair of chromatin strands.
Irradiation of cells, while they are in S phase may bring both types of aberrations.
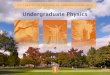
The types of chromosome aberrations that are lethal to cells are (i) dicentric, (ii)
ring, and (iii) anaphase bridge. The first two are chromosome aberrations, whereas
anaphase bridge is chromatid aberration. The types of aberrations that are not lethal to
cells are (iv) symmetric translocation and (v) small interstitial deletion (Fig.3).They are
basically arises from DSB, remains intact with two chromatids and centromere, and
carry out mitosis normally. However, there may be some loss of genetic information,
that may be passed on to the next generations.
(i) Dicentric
Two separate chromosomes undergo breaks at the early inter phase. If the
broken ends are close to each other, they get united illegitimately, and replicated during
the S phase. After the synthesis, a pair of sister chromatids appears with two
centromeres, which is called dicentric. It is an unstable aberration lethal to the cell, not
passed on to the progeny. It decreases slowly over a period of time after radiation
exposure. Since spindle has two centromeres to grab during the meta phase, it get
disturbed while pulling the chromatids during the anaphase.

(ii) Ring
Radiation induces breaks in each arm of a single chromatid, at the early part of
the cell cycle. The breaks may rejoin and form ring and fragments. During synthesis, it
gets replicated and appears as overlapping rings and acentric fragments without
centromere. Since the ring or the acentric fragment do not have properly constructed
centromere for the spindle to attach, chromosomes unable to divide properly. The
fragments will be lost during next mitosis.
Fig.3.Radiation induced chromosome damage: (a) Dicentric, (b) ring
formation,(c) anaphase bridge, (d) symmetric translocation and (e) small
interstitial deletion.
3.CELL SURVIVAL CURVES
3.1.Introduction
Radiation exposure creates two types of population namely (i) dead cells and (ii)
surviving cells. Dead cells are the one which have lost the capacity to divide indefinitely,
i.e. loss of reproductive integrity. Cells which are physically present, synthesize DNA or
make proteins but not able to divide during mitosis are also said to be dead. Cells that
have retained its reproductive capacity and are able to divide indefinitely are called
survived cells. These cells can produce colony and hence said to be cologenic cells. A
cell death in differentiated cells leads to loss of organ function, e.g. nerve, muscle etc.
The cell death in a proliferating cell (stem cell) refers loss of reproductive capacity, e.g.
blood cells, epithelium, etc. Cells may die in two ways: (i) they die when they attempt to

divide, called mitotic death, and (ii) some cells undergo a programmed death called
apoptosis.
The relation between the radiation dose and the number of surviving cells that
form colonies can be plotted in a curve, known as survival curve. The survival curve is a
measure of reproductive death. To conduct the experiment, the cells are seeded in a
petri dish (in vitro) and exposed to varying dose of radiation. Usually multiple petri
dishes with cells are planned. One two dishes are used as control and no irradiation is
given. They are allowed to grow colonies and the same is counted. The irradiated and
the control cells are incubated for same duration of time. Each cell is assumed to make
their respective colony. The fraction of surviving cells are normalised by the fraction of
cells that survive with no radiation exposure.
A graph is plotted between the radiation dose and the survival fraction. The
survival curve of the Mammalian cells are exponential in nature and hence, plot is
usually drawn between of log of survival fraction (Y-axis) vs radiation dose (X-
axis).These curves are useful to understand radiation damage and their nature. The
shape of the curve tells us the radio sensitivity, repair and recovery ability of the cell.
The shape of the cell survival curve gets altered, if the exposure conditions are
changed, during or after the radiation exposure. To quantify the cells the parameters
such as (i) plating efficiency and (ii) survival frcation is used.
3.2. Survival fraction and plating efficiency
The surviving fraction (SF) is given by the relation,
𝑆𝐹 =𝐶𝑜𝑙𝑜𝑛𝑖𝑒𝑠 𝑐𝑜𝑢𝑛𝑡𝑒𝑑
𝐶𝑒𝑙𝑙𝑠 𝑠𝑒𝑒𝑑𝑒𝑑 ×𝑃𝐸
100
− − − − − (1)
Where, PE is the plating efficiency, which refers to the percentage of seeded cells that
survive to form colonies under control conditions:
𝑃𝐸 = 𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑐𝑜𝑙𝑜𝑛𝑖𝑒𝑠 𝑐𝑜𝑢𝑛𝑡𝑒𝑑
𝑁𝑢𝑚𝑏𝑒𝑟 𝑜𝑓 𝑐𝑒𝑙𝑙𝑠 𝑠𝑒𝑒𝑑𝑒𝑑× 100 − − − − − (2)
The PE can be obtained with invitro studies as follows. The cells are prepared in
a culture vessel (dish) with trypsin and the number of cells are counted by an electronic
or hemocytometer. The dish is incubated for 1-2 weeks, during the period the cells
divide and forms colonies. Now, the number of colonies is again counted using the
above formula, to get the PE. The number of colonies are always lesser than the
number of seeded cells due to growth medium, uncertainties of counting and trauma of
trypsinization and handling.

3.3. Survival curve
In vitro studies show that survival curve of each cell line after radiation exposure
can be plotted in a semi-log graph with the surviving fraction in the Y axis and the dose
in the X axis (Fig.4a & b).
Fig.4. Shape of the survival curve for mammalian cells. Survival fraction is plotted
in (a) linear scale and (b) logarithmic scale with dose on a linear scale.
The curve 4a contains two regions namely, region A at low doses and region B at
low survivals, both are important for radiotherapy. However, the curve may not be useful
clinically as it is not giving the true picture of cell survival. In radiotherapy, we use low
dose per fraction (1-3 Gy per fraction) and tumour cure require cell survival of about 10-8
cells. Hence, it is meaningful to plot the curve as shown in 4b, in a semi log scale. This
curve demonstrates the exponential behaviour of region A as straight line. It also
magnifies the region B, which represents the low survival levels of cell (10-8), visualize
tumour cure.
4. BIOLOGICAL EFFECTS OF RADIATION
4.1.Introduction
Radiation exposure can destroy cells ability to reproduce, but may not disturb its
function. Then, there is a chance that cell may not complete the cell cycle and undergo
reproductive death. These cells do not reproduce, but continue its function such as

production of protein, hormones etc. The reproductive death is not related with cancer.
In general the biological damage depends upon the mitotic index of the cell. This means
that cell with higher replication rate and high turnover are more sensitive and exhibits
their damage immediately. The organ response depends upon the mixture of cells by
which it is made up of.
Biological effect of radiation is generally divided into stochastic and deterministic
effects (Fig.5). A stochastic effect is one in which the probability of effect occurring,
increases with dose, rather than its severity, e.g. induction of cancer. A radiation dose of
5 Gy has more probability to induce cancer than 1 Gy dose, even though the severity is
same in both cases. It has no threshold dose; even a small radiation has ability to cause
stochastic effect. The risk increases with increase of dose and there is no dose at which
the risk is zero. Stochastic effects are the principle health risk from low level radiation;
hence it is important in medical exposures of patients and occupational workers.
(A) (B)
Fig.5.The (A) stochastic effect and (B) deterministic effect of radiation
4.2. Stochastic effect
Stochastic effect is observed only in animal experiments. The dose effect
relationship can be studied only in a group of human population. The dose effect
relationship is linear, but its effect <100 mSv (low dose range) is not verified. The
observed dose response at higher doses is extrapolated for low doses. This is

applicable for radiation protection and safety purpose. There is no method to identify
the appearance of effect in an individual. The increase in occurrence of effect can be
proved only by epidemiological studies. The stochastic effects are further classified as
(i) radiation carcinogenesis and (ii) hereditary effects. The stochastic effects usually
appear as late effects
4.3. Deterministic effect
A deterministic effect is one in which the severity of the effect increases with
dose, due to degenerative changes in tissues. It has a threshold dose, below which no
radiation effects is seen. Deterministic effects always occur at high radiation doses.
The threshold dose is higher than the doses from natural radiation or from the
occupational exposure at normal operations. Skin erythema, cataract and hematopoietic
damages fall under this category. Deterministic effects are often known as normal tissue
reactions.
There is a time interval between irradiation and the occurrence of radiation
effects, called latent period. It is the indicator of tissue radiosensitivity and it is
inversely proportional to the dose. This means that lower the dose, and greater the
latent period and appearance the effect. There are two latent periods correspondingly
for the appearance of early and late effects. Of course there is no difference in the
radiation damage in terms of early and late effects, but only difference is the time of
appearance of effect. The acute early effects appear within a month after radiation
exposure, The early effects are further divided into (i) radiation injury in individual
organs or normal tissue reactions and (ii) acute radiation syndrome. The former is the
result of partial body exposure, including radiotherapy treatments and later is the
outcome of whole body exposure, due to accidents. The late effects appear within
months or year after radiation exposure that includes (i) radiation dermatitis,(ii) cataract,
and (iii) teratogenic effects on embryo and fetus.
The basic difference between stochastic and deterministic arises from the
interaction. In the former the radiation interacts with DNA, at the cellular level. This
results in mutation which can be passed to the next generation, leading genetic effects
or induction of cancer. In the later, the interaction is in a group of cells that forms the
tissue or organs. This will end up with loss of tissue function.

Fig.6.The various types of radiation effects after acute and chronic
radiation effects.
Summary
The radiobiological studies contribute to the development of medicine, especially
radiology and radiotherapy. Understanding the interaction of radiation of radiation with
cell or DNA and the resulting damage is very important. Cell survival curves give an idea
about the number of cells (%) remaining after the exposure of ionizing radiation.
Biological effects appear as deterministic and stochastic effects. The Deterministic
effects are possible only at high level radiation, hence, unlikely in a hospital setup.
Stochastic effects are possible in low level radiation, hence, likely to occur at hospital
workers. Therefore, the aim of radiation safety policy is to prevent the deterministic
effects and minimize the stochastic effects. All efforts must be taken to keep the radiation
levels as low as reasonably achievable (ALARA).